Back to Journals » Cancer Management and Research » Volume 12
Predictive Value of Postoperative Peripheral CD4+ T Cells Percentage in Stage I–III Colorectal Cancer: A Retrospective Multicenter Cohort Study of 1028 Subjects
Authors Li Z ![]() , Li S
, Li S ![]() , Liang Y, Pu H
, Liang Y, Pu H ![]() , Tu C, Wu Z
, Tu C, Wu Z ![]() , You D
, You D
Received 28 April 2020
Accepted for publication 11 June 2020
Published 7 July 2020 Volume 2020:12 Pages 5505—5513
DOI https://doi.org/10.2147/CMAR.S259464
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Eileen O'Reilly
Zhenhui Li,1,* Shaoyou Li,2,* Yun Liang,3,* Hongjiang Pu,4 Changling Tu,5 Zhenyu Wu,6 Dingyun You7,8
1Department of Radiology, The Third Affiliated Hospital of Kunming Medical University, Yunnan Cancer Hospital, Yunnan Cancer Center, Kunming 650118, People’s Republic of China; 2Department of Medical Oncology, The First Affiliated Hospital of Kunming Medical University, Kunming 650032, People’s Republic of China; 3Department of Hepatobiliary Surgery, The First Affiliated Hospital of Kunming Medical University, Kunming 650032, People’s Republic of China; 4Department of Colorectal Surgery, The Third Affiliated Hospital of Kunming Medical University, Yunnan Cancer Hospital, Yunnan Cancer Center, Kunming 650118, People’s Republic of China; 5Department of Cadres Medical Oncology, The Third Affiliated Hospital of Kunming Medical University, Yunnan Cancer Hospital, Yunnan Cancer Center, Kunming 650118, People’s Republic of China; 6Department of Biostatistics, School of Public Health, Key Laboratory of Public Health Safety and Collaborative Innovation Center of Social Risks Governance in Health, Fudan University, Shanghai 200032, People’s Republic of China; 7The Department of Epidemiology & Biostatistics, School of Public Health, Kunming Medical University, Kunming, Yunnan 650500, People’s Republic of China; 8Yunnan Key Laboratory of Laboratory Medicine, Kunming Medical University, Kunming, Yunnan 650500, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Dingyun You
Yunnan Key Laboratory of Laboratory Medicine, Kunming Medical University, No. 1168 Chunrongxi Road, Chenggong District, Kunming, Yunnan 650500, People’s Republic of China
Tel/ Fax +86 871-5922935
Email [email protected]
Zhenyu Wu
Department of Biostatistics, School of Public Health, Key Laboratory of Public Health Safety and Collaborative Innovation Center of Social Risks Governance in Health, Fudan University, 130 Dongan Road, Shanghai, People’s Republic of China
Tel/ Fax +86 21‐33563913
Email nc.ude.naduf@wyz
Objective: Association of postoperative peripheral CD4+ T cells percentage and recurrence in colorectal cancer (CRC) remains to be explored. Therefore, we aimed to investigate the association between the postoperative peripheral CD4+ T cells percentage and recurrence in CRC patients.
Patients and Methods: Consecutive stage I–III CRC patients without neoadjuvant treatment undergoing curative resection from January 2010 to July 2016 were identified in two Chinese centers. The association between the postoperative CD4+ T cells percentage, measured within 12 weeks after surgery, and recurrence-free survival (RFS) was analyzed.
Results: A total of 1028 patients were identified (training set: 913 patients, validation set: 115 patients). In the training set, the 5-year RFS rate of the 441 patients with abnormal postoperative CD4+ T cells percentage was significantly lower than that of those with normal percentage (70.3% [95% CI 65.7– 75.2%] vs 77.6% [95% CI 73.7– 81.7%] and unadjusted hazard ratio [HR] 1.36 [95% CI 1.04– 1.78], P= 0.02). The result was confirmed in the validation set. Multivariable Cox regression analysis demonstrated that the association of postoperative CD4+ T cells percentage with 5-year RFS was independent both in the training and validation sets. In propensity score matching analysis, patients with normal postoperative CD4+ T cells percentage were found to have a favourable response to adjuvant chemotherapy (HR 0.29 [95% CI 0.12– 0.72], P=0.008).
Conclusion: Postoperative peripheral CD4+ T cells percentage is a predictive biomarker for RFS in patients with CRC, which can identify those who will benefit from adjuvant chemotherapy.
Keywords: recurrence, peripheral CD4+ T cells, colorectal cancer, adjuvant chemotherapy, propensity score matching analysis
Introduction
Among men and women across the world, colorectal cancer (CRC) is the fourth and third leading cause of cancer-related death, respectively,1 even though the survival rate has improved with early diagnosis and multiple therapies.2 For the standard treatment of CRC, adjuvant chemotherapy after surgery may be required depending on the tumor stage.3,4 However, the TNM stage fails to provide complete prognostic information, and clinical outcomes vary significantly among patients with the same tumor stage.5 Thus, there is an urgent need for a new prognostic tool to determine the risk of CRC recurrence and develop personalized treatments for patients with a high probability of recovery, such as intensified local or systemic treatment.
The host local and systemic immunity is significantly associated with tumor response to treatment and prognosis.6–13 The local tumor-infiltrating lymphocytes (TILs) represent the local immunity in the tumor microenvironment. Multiple studies confirmed that TILs in the tumor played a prominent role in the prognosis of patients with CRC, and some investigators suggested that the immunoscore should be a new component in the classification of colon cancer according to the TNM classification system.6–9 However, these studies focused only on local immunity and ignored the systemic immunity.
The systemic immunity is constituted by the immune cells in the peripheral blood except for the spleen, lymph node, and bone marrow.12 Some studies suggested that the peripheral subsets of immune cells may play a more important and effective antitumour role than that of TILs in the tumor region.12,14 For example, anti-PD-1 therapy in patients with basal or squamous cell carcinoma mainly relied on recruitment of novel T cells from peripheral sources rather than on reinvigorating pre-existing intratumoural TILs.14 There is a strong evidence from murine studies that an emergent population of peripheral CD4+ T cells primed by a subtype of conventional dendritic cells, cDC2, contribute to the systemic immunity with effective antitumour capabilities, as a difference to CD8+ T cells.10,12 Additionally, peripheral CD4+ T cells were significantly expanded in patients responding to immunotherapy.12 Hence, peripheral CD4+ T cells may be a marker for predicting treatment response and prognosis in cancer; however, there is controversy in this regard.15–18 One study stated that peripheral CD4+ T cells percentage had a predictive value of anti‐PD‐L1/PD‐1 immunotherapy response in lung cancer patients,15 while another study reported no significant predictive value for progression-free survival (PFS) in metastatic breast cancer and prostate cancer with metastatic bone lesions.16 For CRC, one study of a small cohort (N = 40) with advanced stages stated that the counts of peripheral СD4+ T cells ≥300 cells/ul before surgery had a beneficial effect on overall survival (OS) by using an univariate analysis,17 while another study reported that the preoperative peripheral CD4+ T cell counts did not have prognostic value on OS.18
Hence, the value of peripheral CD4+ T cells on the clinical outcome is not clear in cancer. Thus, the current study aims to analyse the influence of postoperative peripheral CD4+ T cells on the recurrence in patients with CRC in a retrospective multicenter cohort.
Patients and Methods
This retrospective study was approved by the institutional review boards of Yunnan Cancer Hospital and the First Affiliated Hospital of Kunming Medical University. The requirement for informed consent was waived by the board, due to the nature of the retrospective study. All of the patient data in the survey was anonymized.
Patients
We retrospectively identified 1028 consecutive patients who underwent surgical resection for stage I to III colorectal adenocarcinoma between January 2010 and July 2016 at 2 centers of Yunnan Province in China. Figure 1 demonstrates the study flowchart, which includes the inclusion and exclusion criteria. The patients were grouped into two sets: one training set (n=913 from center 1) and one validation set (n=115 from center 2).
 |
Figure 1 Study flow chart. |
Specimen Collection
After admission, the patients who met the inclusion criteria were collected 2 mL of fasting venous blood with heparin anticoagulant tube at 6:00–8:00 in the morning. The blood was mixed upside down, and sent for examination within 2 hrs.
Postoperative Peripheral CD4+ T Cells Determination
Postoperative CD4+ T cells were defined as the circulating CD4+ T cells, including absolute count and percentage value, and were measured within 12 weeks after surgery by using flow cytometry-based method. Detailed description of the CD4+ T cell absolute count and percentage determination procedure by flow cytometry, and the formulation method of the reference range are shown in the Supplementary Methods text sections and Table S1. Patients were grouped by CD4+ T cells percentage status compared to healthy Yunnan population as follows: patients with normal postoperative CD4+ T cells percentage (31.4% to 43.8%) and patients with abnormal postoperative CD4+ T cells percentage (>43.8% or <31.3%), while patients were also grouped by CD4+ T cells count status compared to healthy Yunnan population as follows: patients with normal postoperative CD4+ T cells count (345 to 1402 cells/ul) and patients with abnormal postoperative CD4+ T cells count (>1402 cells/ul or <345 cells/ul).19
Adjuvant Chemotherapy Protocol
Partial patient with stage II–III CRC received the adjuvant chemotherapy according to the National Comprehensive Cancer Network (NCCN) clinical practice guidelines in the CRC.3,4 Adjuvant chemotherapy protocol included FOLFOX, CapeOX, Capecitabine, or 5-FU/leucovorin.
Surveillance Protocol
The clinical evaluation included physical examination, measurement of serum carcinoembryonic antigen (CEA) level, imaging, and colonoscopy. CEA levels were tested at 3- to 6-month intervals for the first 2 years and at 6-month intervals for >2-5 years. Imaging, including contrast-enhanced computed tomography (CT) of the chest, abdomen, and pelvis was performed at a minimum of every 12 months for at least 3 years. Colonoscopy was performed 1 year after surgery and then repeated every 2–5 years unless advanced adenomas were identified. All recurrent cases were confirmed via histology or imaging.
Outcomes
The recurrence-free survival (RFS) time was calculated from the date of surgery to the date of recurrence, death, or the last follow-up. Patients who were alive without recurrence or died before the last follow-up were censored.
Statistical Analysis
All statistical analyses were done with the R software (version 3.4.0; http://www.R-project.org). The statistical significance levels reported in the findings were all two-sided, with statistical significance set at a P-value <0.05. Mean values ± standard deviations (SD) (normal distribution) or median (quartile) (skewed distribution) were provided for continuous variables, whereas frequencies and percentages were provided for categorical variables. Assessment of the correlation between the CD4+ T cells percentage and different clinicopathologic parameters was analysed using the Mann–Whitney U-test or chi-square test.
Kaplan-Meier method was used to analyse the correlation between variables and RFS, and the Log-rank test (univariate analysis) to compare survival curves.
Univariate and multivariable Cox regression model evaluated the associations of CD4+ T cells percentage and count with RFS, and the hazard ratios (HR) and 95% confidence interval (CI) were calculated.6 The multivariable Cox regression model was re-developed with the significant variables, and all predictors still contributed significantly to the reduced model.20
To confirm the predictive contribution of postoperative CD4+ T cells percentage to RFS with adjuvant chemotherapy, propensity score matching was used to select the cases for further analysis because the baseline characteristics were significantly different between the patients who received adjuvant chemotherapy and the patients who did not receive the adjuvant chemotherapy. The propensity score model was used to minimize the potential bias caused by confounding covariates.21 A multivariable logistic regression model was constructed to generate propensity scores. The clinicopathologic factors included in the model were age at diagnosis, sex, body mass index (BMI), pathological T stage, pathological N stage, histologic grade (high, moderate, poor differentiation, or undifferentiated), and Histological type (mucinous type, yes or no). Patients who received adjuvant chemotherapy were matched to those who did not receive adjuvant chemotherapy at a 1:1 using a greedy nearest neighbor matching algorithm with no replacement. A caliper width equal to 0.1 of the standard deviation was used as the logit of the propensity score.22 Patient characteristics between the propensity score-matched groups were compared using Mann–Whitney U-test or chi-square test. Further details on the PSM methods can be found in the Supplementary Table S1.
Results
Patient Characteristics
The cohort of 1028 patients (607 men and 421 women with a mean age of 57.64 years) was followed-up for a long term (median intervals: 52 months, interquartile range [IQR]: 40–70 months). Tumors were located in the colon in 492 patients (47.86%) and in the rectum in 536 patients (52.14%). All patients had undergone surgical resection with histological negative resection margins, and 816 (79.38%) were treated with adjuvant chemotherapy. A total of 258 patients experienced tumor recurrence. Supplementary Table S2 shows detailed clinicopathological characteristics of the training and validation sets. There were significant differences in the clinical characteristics including age, tumor differentiation, T stage, and tumor deposit between the training and the validation sets (Table S2). Median intervals (IQR) of the follow-up of the training and validation sets were 53 months (IQR: 42–71 months) and 51 months (IQR: 39–70 months), respectively.
Association of Postoperative CD4+ T Cells Percentage with Clinicopathologic Characteristics
Table 1 shows the clinicopathological characteristics of patients with normal, or abnormal postoperative CD4+ T cells percentages. The postoperative CD4+ T cells percentages were correlated with sex, age, and the postoperative CD4+ T cells count. No association was noted between postoperative CD4+ T cells percentages and other clinicopathological characteristics including BMI, surgical approach, primary site, tumor differentiation, histologic type, T stage, N stage, and tumor deposit.
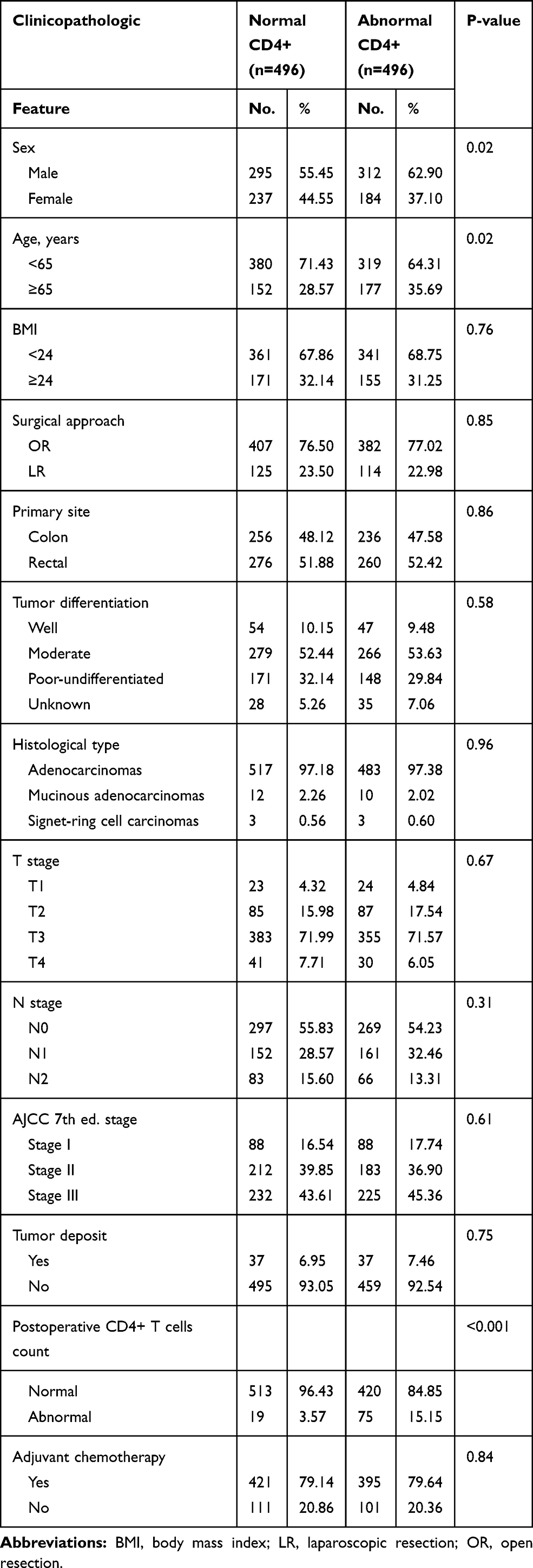 |
Table 1 Correlation Between Postoperative CD4+ T Cells Percentage and Clinicopathologic Features in Colorectal Cancer Patients |
Association of Postoperative CD4+ T Cells Percentage with 5-Year RFS
The 5-year RFS rate of the 441 patients with abnormal postoperative CD4+ T cells percentage was 70.3% (95% CI, 65.7–75.2%), which was significantly lower than the 77.6% (95% CI, 73.7–81.7%) 5-year RFS in the 472 patients with normal postoperative CD4+ T cells percentage (unadjusted HR, 1.36; 95% CI, 1.04–1.78; P = 0.02) in the training set (Figure 2A). The result was confirmed in the validation set (Figure 2B). The 55 patients with the abnormal postoperative CD4+ T cells percentage had the lower 5-year RFS rate than that of 60 patients with the normal postoperative CD4+ T cells percentage (unadjusted HR, 2.27; 95% CI, 1.06–4.89; P = 0.04) in the validation set (Figure 2B).
 |
Figure 2 Kaplan-Meier estimates of recurrence-free survival according to the postoperative CD4+ T cells percentage. (A) In the training set. (B) In the validation set. |
Applying univariate Cox regression analysis to the training set, the abnormal postoperative peripheral CD4+ T cells percentage was associated with significantly shorter RFS, while the postoperative peripheral CD4+ T cells count was not significantly associated with RFS. Multivariate analysis in the training set showed that the abnormal postoperative peripheral CD4+ T cells percentage was independently associated with shorter RFS (HR, 1.35; 95% CI, 1.03–1.77; P = 0.03; Table 2) as well as with higher TNM stage in a model that included sex, age, BMI, surgical approach, primary site, tumor differentiation, histologic type, TNM stage, the postoperative CD4+ T cells count, and tumor deposit. Similar results were obtained in the validation set (Table 2).
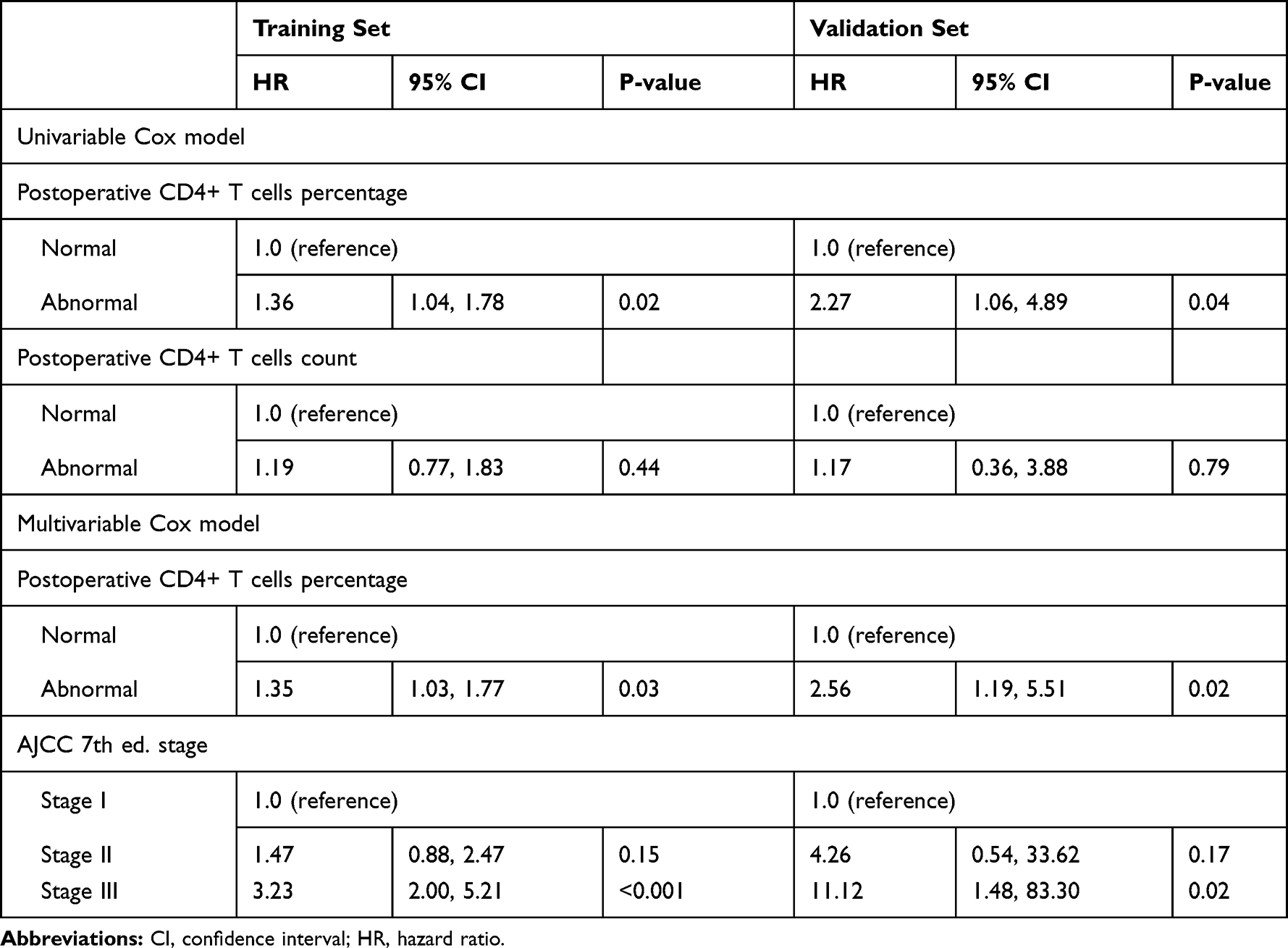 |
Table 2 Cox Proportional Hazard Model Showing Hazard Ratios for 5-Year Recurrence-Free Survival by Variables |
Propensity Score Matching of Adjuvant Chemotherapy
In total, 816 patients receiving adjuvant chemotherapy were matched to 212 patients who did not receive adjuvant chemotherapy. After propensity score matching, 185 pairs of patients were 1:1 matched in the two groups, and all baseline characteristics were well balanced (Supplementary Table S3).
Predictive Contribution of Postoperative CD4+ T Cells Percentage to RFS with Adjuvant Chemotherapy
In the matched population, adjuvant chemotherapy significantly enhanced 5-year RFS relative to no adjuvant chemotherapy (HR 0.29, 95% CI 0.12–0.72; P = 0.008; Figure 3A) in patients with normal postoperative CD4+ T cells percentage, but did not provide a statistically significant benefit in patients with abnormal postoperative CD4+ T cells percentage (HR 0.81, 95% CI 0.39–1.43; P = 0.47; Figure 3B).
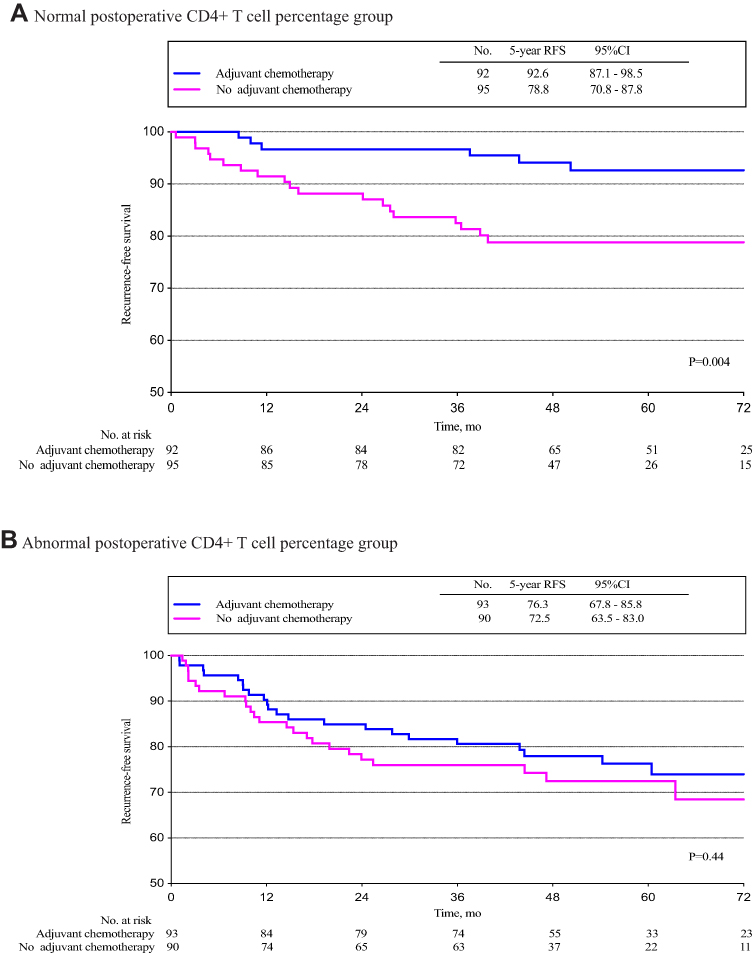 |
Figure 3 Kaplan-Meier estimates of recurrence-free survival according to the postoperative CD4+ T cells percentage and treatment arm. (A) In normal postoperative CD4+ T cells percentage group. (B) In abnormal postoperative CD4+ T cells percentage group. |
Discussion
Our study evidenced that the postoperative peripheral CD4+ T cells percentage was predictive for RFS with adjuvant chemotherapy after propensity score-matched analysis in a large cohort of CRC patients. To our knowledge, no large cohort studies previously investigated the predictive value of peripheral CD4+ T cells in CRC. Our results suggested that the postoperative peripheral CD4+ T cells constitute a predictive biomarker in CRC, unlike the tumor-infiltrating CD3+ and CD8+ T cells as prognostic biomarkers described in the previous studies.6–9
Our result was different from the previous studies.17,18 We systematically reviewed the published literature and performed database queries between 2005 and July 2019 with a focus on the effect of T cells on the prognosis in CRC (Table S4). We observed that the majority of these studies evaluated the prognostic impact of TILs, while only two studies focused on the peripheral T cells in a CRC setting. However, these two studies were performed with relatively small sample sizes and did not indicate the peripheral CD4+ T cells percentage as a predictive biomarker.17,18
Our study findings have important clinical value. Whether chemotherapy is needed for CRC patients is mainly based on TNM staging according to the current guidelines.3,4 But adjuvant chemotherapy had different effect on the CRC patient with the same tumor stage.5 This means administration of adjuvant chemotherapy to all patients with the same tumor stage is unnecessary for partial patients who are cured with surgery alone.23 Hence, it is important to find a predictive biomarker identifying those CRC patients who are more likely to benefit from adjuvant chemotherapy. Our result showed that adjuvant chemotherapy provided a survival benefit to patients with normal postoperative CD4+ T cells percentage, but did not show a statistically significant benefit to patients with abnormal postoperative CD4+ T cells percentage. Therefore, postoperative CD4+ T cells percentage for CRC patients is a predictive biomarker rather than a prognostic biomarker,24 and might allow for better identification of patients who are most likely to benefit from adjuvant chemotherapy.23,24
The present study confirmed prior controversy over the prognostic or predictive value of peripheral CD4+ T cells in cancer patients, as stated in the “Introduction” section. This may be related to the research design. In our research design, all patients were divided into normal and abnormal groups by two cut-off values, which is different from the research design of previous studies that only divided the peripheral CD4+ T cells percentage into two groups by one cut-off value in lung cancer,15 or into three groups according to the linear relationship between peripheral CD4+ T cells percentage and PFS in metastatic breast cancer, and prostate cancer patients with metastatic bone lesions.16
This study has two main limitations. Firstly, our study did not include TIL as an adjust parameter which may affect the independent prognostic effect of the peripheral CD4+ T cells percentage in CRC. However, one study confirmed that the prevalence of some T cell subsets in the tumor was not associated with their frequency in peripheral blood.25 Secondly, genomic characteristics including microsatellite instability, KRAS, NRAS, and BRAF, which are proposed as predictors of CRC patient outcomes,26 were not considered in this study due to the lack of identification method for these characteristics in the hospitals before 2016.
In conclusion, our study demonstrates that postoperative peripheral CD4+ T cells percentage is a predictive biomarker for RFS in patients with CRC, which can identify the patients who will benefit from adjuvant chemotherapy.
Data Sharing Statement
After de-identification, individual participant data will be made available to investigators who provide a methodologically sound proposal for meta-analyses. Proposals should be directed to Dingyun You ([email protected]).
Disclosure
The authors declare that they have no potential conflicts of interest.
References
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. doi:10.3322/caac.21492
2. Boland PM, Ma WW. Immunotherapy for colorectal cancer. Cancers (Basel). 2017;9(5):E50. doi:10.3390/cancers9050050
3. Network NCCN. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines): Colon Cancer. (Version 2.2018). Fort Washington, PA: National Comprehensive Cancer Network; 2018.
4. National-Comprehensive-Cancer-Network. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines): Rectal Cancer. (Version 3.2018). Fort Washington, PA: National Comprehensive Cancer Network; 2018.
5. Konishi T, Shimada Y, Hsu M, et al. Association of preoperative and postoperative serum carcinoembryonic antigen and colon cancer outcome. JAMA oncol. 2018;4(3):309–315. doi:10.1001/jamaoncol.2017.4420
6. Pagès F, Mlecnik B, Marliot F, et al. International validation of the consensus immunoscore for the classification of colon cancer: a prognostic and accuracy study. Lancet. 2018;391(10135):2128–2139. doi:10.1016/S0140-6736(18)30789-X
7. Mlecnik B, Tosolini M, Kirilovsky A, et al. Histopathologic-based prognostic factors of colorectal cancers are associated with the state of the local immune reaction. J Clin Oncol. 2011;29(6):610–618. doi:10.1200/JCO.2010.30.5425
8. Pages F, Kirilovsky A, Mlecnik B, et al. In situ cytotoxic and memory T cells predict outcome in patients with early-stage colorectal cancer. J Clin Oncol. 2009;27(35):5944–5951. doi:10.1200/JCO.2008.19.6147
9. Sinicrope FA, Rego RL, Ansell SM, Knutson KL, Foster NR, Sargent DJ. Intraepithelial effector (CD3+)/regulatory (FoxP3+) T-cell ratio predicts a clinical outcome of human colon carcinoma. Gastroenterology. 2009;137(4):1270–1279. doi:10.1053/j.gastro.2009.06.053
10. Binnewies M, Mujal AM, Pollack JL, et al. Unleashing type-2 dendritic cells to drive protective antitumor CD4(+) T cell immunity. Cell. 2019;177(3):556–571 e516. doi:10.1016/j.cell.2019.02.005
11. Dijkstra KK, Cattaneo CM, Weeber F, et al. Generation of tumor-reactive T cells by co-culture of peripheral blood lymphocytes and tumor organoids. Cell. 2018;174(6):1586–1598 e1512. doi:10.1016/j.cell.2018.07.009
12. Spitzer MH, Carmi Y, Reticker-Flynn NE, et al. Systemic immunity is required for effective cancer immunotherapy. Cell. 2017;168(3):487–502.e415. doi:10.1016/j.cell.2016.12.022
13. Kamphorst AO, Pillai RN, Yang S, et al. Proliferation of PD-1+ CD8 T cells in peripheral blood after PD-1-targeted therapy in lung cancer patients. Proc Natl Acad Sci U S A. 2017;114(19):4993–4998. doi:10.1073/pnas.1705327114
14. Yost KE, Satpathy AT, Wells DK, et al. Clonal replacement of tumor-specific T cells following PD-1 blockade. Nat Med. 2019;25(8):1251–1259. doi:10.1038/s41591-019-0522-3
15. Zuazo M, Arasanz H, Fernández‐Hinojal G, et al. Functional systemic CD4 immunity is required for clinical responses to PD‐L1/PD‐1 blockade therapy. EMBO Mol Med. 2019;11(7):e10293. doi:10.15252/emmm.201910293
16. Farsaci B, Donahue RN, Grenga I, et al. Analyses of pretherapy peripheral immunoscore and response to vaccine therapy. Cancer Immunol Res. 2016;4(9):755–765. doi:10.1158/2326-6066.CIR-16-0037
17. Milasiene V, Stratilatovas E, Norkiene V, Jonusauskaite R. Lymphocyte subsets in peripheral blood as prognostic factors in colorectal cancer. J BUON. 2005;10(2):261–264.
18. Qiu H, Xiao-Jun W, Zhi-Wei Z, et al. The prognostic significance of peripheral T-lymphocyte subsets and natural killer cells in patients with colorectal cancer. Hepatogastroenterology. 2009;56(94–95):1310–1315.
19. Jin CG, Chen XQ, Li J, Wu ZP, Liu X, Wang XC. Moderating effects and maintenance of lung cancer cellular immune functions by CIK cell therapy. Asian Pac J Cancer Prev. 2013;14(6):3587–3592. doi:10.7314/APJCP.2013.14.6.3587
20. Li ZH, Xie PY, Zhang DF, et al. Nomogram for predicting disease-free survival among a multicenter cohort of Chinese patients with locally advanced rectal cancer. Cancer Manag Res. 2019;11:2471–2483. doi:10.2147/CMAR.S196614
21. Renehan AG, Malcomson L, Emsley R, et al. Watch-and-wait approach versus surgical resection after chemoradiotherapy for patients with rectal cancer (the OnCoRe project): a propensity-score matched cohort analysis. Lancet Oncol. 2016;17(2):174–183. doi:10.1016/S1470-2045(15)00467-2
22. Li X, Zhang C, Sun Z, et al. Propensity-matched analysis of adjuvant chemotherapy for completely resected stage IB non-small-cell lung cancer patients. Lung Cancer. 2019;133:75–82. doi:10.1016/j.lungcan.2019.04.024
23. Zhang JX, Song W, Chen ZH, et al. Prognostic and predictive value of a microRNA signature in stage II colon cancer: a microRNA expression analysis. Lancet Oncol. 2013;14(13):1295–1306. doi:10.1016/S1470-2045(13)70491-1
24. Ballman KV. Biomarker: predictive or prognostic? J Clin Oncol. 2015;33(33):3968–3971. doi:10.1200/JCO.2015.63.3651
25. E J, Yan F, Kang Z, Zhu L, Xing J, Yu E. CD8(+)CXCR5(+) T cells in tumor-draining lymph nodes are highly activated and predict better prognosis in colorectal cancer. Hum Immunol. 2018;79(6):446–452. doi:10.1016/j.humimm.2018.03.003
26. Amin MB, Edge S, Greene F, et al. AJCC Cancer Staging Manual.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.