Back to Journals » Journal of Inflammation Research » Volume 19
Predictive Value of Inflammatory Burden Index for Sepsis in Critically Ill Patients with Extensive Burns: A Decade-Long Cohort Study
Authors Zhou S, He X, Huang Y, Zhu W, Song H ![]()
Received 22 October 2025
Accepted for publication 24 January 2026
Published 4 February 2026 Volume 2026:19 574776
DOI https://doi.org/10.2147/JIR.S574776
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Anh Ngo
Songwei Zhou,* Xin He,* Yuqun Huang,* Wei Zhu, Huapei Song
Institute of Burn Research, The First Affiliated Hospital of Army Medical University, State Key Laboratory of Trauma and Chemical Poisoning, Chongqing, 400038, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Huapei Song, Institute of Burn Research, The First Affiliated Hospital of Army Medical University, 30 Gaotanyan Street, Chongqing, 400038, People’s Republic of China, Email [email protected]
Objective: We aimed to explore the correlation between the inflammatory burden index (IBI) and the development of sepsis in critically ill patients with extensive burns.
Methods: This retrospective cohort study included extensively burned patients who were admitted to the First Affiliated Hospital of Army Medical University from January 1, 2014, to December 31, 2023. These patients were divided into two groups based on the presence or absence of sepsis within 28 days after burns (the sepsis group and the nonsepsis group). Furthermore, the patients’ basic information, burn severity, blood parameters in the early post-burn period (within 48h after burns), mechanical ventilation, ICU length of stay and the outcome were collected. Independent samples Mann–Whitney U-tests and chi-square tests were performed with respect to the indicators between the groups. Univariate and multivariate logistic regression analyses were conducted on the basis of indicators that exhibited statistically significant differences to identify independent risk factors pertaining to sepsis occurrence. Receiver operating characteristic (ROC) curves were plotted to evaluate the predictive efficacy of indicators such as the IBI and determine optimal cutoff values.
Results: A total of 178 critically ill patients with extensive burns were enrolled in this study. Significant differences were observed in the total body surface area (TBSA), burn index (BI), C-reactive protein (CRP) level and neutrophil-to-lymphocyte ratio (NLR), IBI, revised Baux score (rBaux), mechanical ventilation and ICU length of stay between the sepsis group and the nonsepsis group (P < 0.05). Logistic regression analysis identified the IBI in the early post-burn period as an independent risk factor for sepsis (P < 0.05), and its predictive performance surpassed that of the CRP level. The optimal cut-off value of the IBI was 695.01, and combination of the IBI with the BI led to further improvements in predictive performance.
Conclusion: The IBI in the early post-burn period offers good predictive value for the development of sepsis in critically ill patients with extensive burns, which is helpful for formulating treatment strategies, including early surgical intervention, antibiotic application, and early enteral nutrition, etc. to reduce the incidence of sepsis.
Keywords: inflammatory burden index, sepsis, extensive burns, C-reactive protein, burn index
A Letter to the Editor has been published for this article.
Introduction
The critically ill patients with extensive burns often face a significantly increased risk of infection because of skin barrier destruction, homeostatic imbalance, immunosuppression, and systemic inflammation. Sepsis is a common complication of severe burns and is the leading cause of death in patients.1,2 Studies have shown that the incidence of sepsis in patients with total body surface area (TBSA) burns greater than 20% is 3%-30%,3,4 while the mortality of burned patients with sepsis complications is 20.3%.5 Therefore, early prediction of sepsis by biomarkers and timely treatments for reducing the incidence of sepsis are critical for improving prognoses in this context. Immune and metabolic disorders caused by severe burns can lead to changes in the levels of some biomarkers, which are helpful for assessing infection risk, identifying physiological dysfunction and monitoring treatment efficacy. Common biomarkers include C-reactive protein (CRP), procalcitonin (PCT), inflammatory cytokines, etc.6 CRP is an acute phase protein that is closely related to systemic inflammation. Neutrophils and lymphocytes are major components of white blood cells (WBC), participating in the body’s immune and inflammatory responses. Studies have revealed that the neutrophil to lymphocyte ratio (NLR) is increased during bacterial or fungal infection and is correlated with death in septic patients.7 The inflammatory burden index (IBI) is a novel inflammation indicator that combines the CRP and NLR (IBI=CRP × NLR), which reflect body inflammation and immune status more comprehensively. IBI is generally used for the first assessment of the inflammatory load and death risk of tumour patients, and multiple studies have shown that IBI exhibits superior predictive performance for mortality compared to a single inflammatory marker.8–10 Nevertheless, the correlation between IBI in the early post-burn period and the development of sepsis in critically ill patients with extensive burns remains unclear and has not been reported.
Methods
This retrospective cohort study was conducted in accordance with the basic principles of the Declaration of Helsinki. The data are anonymous, and the requirement for informed consent was therefore waived, which was approved by the Ethics Committee of the First Affiliated Hospital of Army Medical University (KY2025168). The study was conducted and reported in accordance with the RECORD guidelines.
Inclusion Criteria and Exclusion Criteria
Inclusion criteria: age ≥18 years, admission to the hospital within 24 hours after burn injury, and burn size ≥50% TBSA. Exclusion criteria: special types of burns (electrical burns, radiation burns, chemical burns, etc).; patients with serious heart, brain, liver, kidney comorbidities, immunodeficiency diseases, and malignant tumours before burns; patients who were self-discharged from the hospital within 4 weeks after injury or who did not cooperate with treatment, and patients whose data were incomplete or missing.
Clinical Data
Severely burned patients admittied between January 1, 2014, and December 31, 2023, were identified from the database of the First Affiliated Hospital of Army Medical University and divided into a sepsis group and a nonsepsis group according to whether sepsis occurred within 28 days after burn injury. The demographic and clinical data of the patients in the two groups were collected, including age, sex, time of admission, cause of burn, TBSA, burn index (BI), revised Baux score (rBaux), WBC count, NLR, CRP level, PCT level, IBI, haemoglobin (Hb) level, albumin (Alb) level, globulin (Glb) level, serum creatinine (SCr) level, blood urea nitrogen (BUN) level, inhalation injury, mechanical ventilation and mortality. All of the blood parameters were collected at admission within 24 hours after burn injury in both two groups. If some parameters were collected more than twice, the average was used.
Diagnosis of Sepsis
In this retrospective study, the diagnostic criteria of sepsis was as follows: positive microbiological tissue or blood culture, antibiotic therapy was effective, and met 3 out of 6 of the following items: (1) temperature>39.0 °C or <36.5 °C; (2) progressive tachycardia>110 beats/minute; (3) respiratory rate>25 breaths/min when not ventilated (12 L/minute when ventilated); (4) thrombocytopenia (only applicable after 3 days during the recovery period)<100×109/L; (5) blood glucose (without pre-existing diabetes mellitus)>20 mg/dL or insulin resistance; and (6) inability to continue enteral nutrition>24 hours.11
Treatments
After admission, the patients were given intensive care, fluid resuscitation, analgesia, maintenance of internal environmental stability, maintenance of organ function, nutritional support, and early rehabilitation. The burn wounds were treated with dressing changes and skin grafting.
Data Analysis
SPSS 26.0 software was used to facilitate the data analysis conducted for this research. The measurement data were tested for normality using the Shapiro–Wilk test, and the normally distributed measurement data were expressed as  , and two independent samples t tests were used for pairwise comparisons; measurement data that did not fit a normal distribution were expressed as the median and quartile M(P25, P75), and intergroup comparisons were performed using the Mann–Whitney U-test. The count data were expressed as percentages, and comparisons of the two sample rates were performed using the χ2 test. Owing to the large difference in the order of magnitude of the original variable IBI, some continuous variables were standardized to prevent variables with large numerical values from dominating the model results. Variance-influencing factors and collinearity tests were performed on all the variables. Moreover, variables for which P <0.05 were screened on the basis of a univariate regression analysis and input to multivariate logistic regression analysis to identify independent risk factors associated with adverse outcomes. The receiver operating characteristic (ROC) curves used to predict sepsis in severely burned patients were plotted using independent risk factors. All statistical significance levels were set at 0.05.
, and two independent samples t tests were used for pairwise comparisons; measurement data that did not fit a normal distribution were expressed as the median and quartile M(P25, P75), and intergroup comparisons were performed using the Mann–Whitney U-test. The count data were expressed as percentages, and comparisons of the two sample rates were performed using the χ2 test. Owing to the large difference in the order of magnitude of the original variable IBI, some continuous variables were standardized to prevent variables with large numerical values from dominating the model results. Variance-influencing factors and collinearity tests were performed on all the variables. Moreover, variables for which P <0.05 were screened on the basis of a univariate regression analysis and input to multivariate logistic regression analysis to identify independent risk factors associated with adverse outcomes. The receiver operating characteristic (ROC) curves used to predict sepsis in severely burned patients were plotted using independent risk factors. All statistical significance levels were set at 0.05.
Results
A total of 178 critically ill patients with extensive burns who met the inclusion and exclusion criteria were included in this research; the sample featured 143 males and 35 females. The mean age of the participants was 43 years, the median TBSA was 70%, and the median BI was 56.00. There were 82 patients in the sepsis group and 96 patients in the nonsepsis group (Table 1).
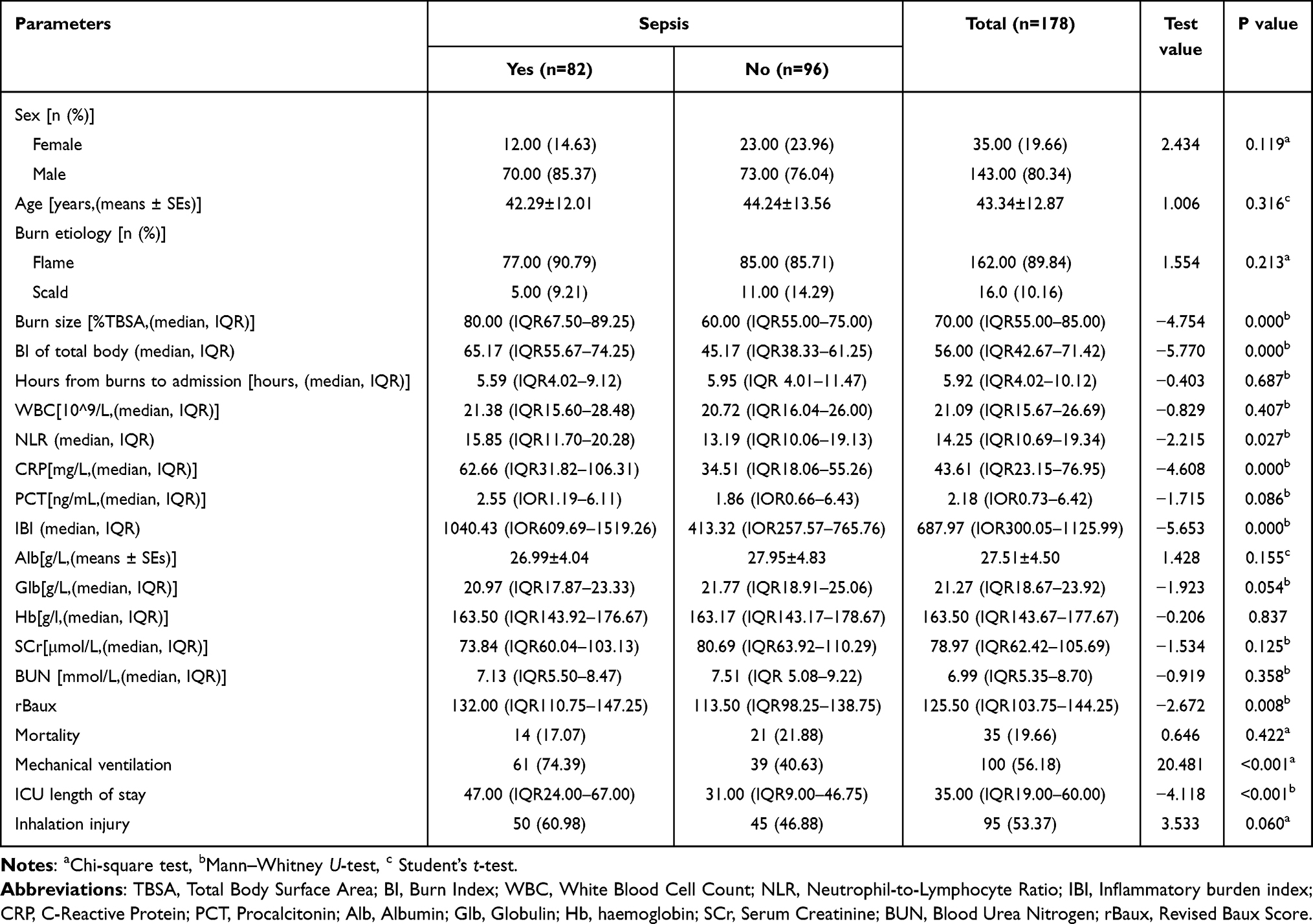 |
Table 1 Baseline Characteristics of Subjects Between the Sepsis and Non-Survival Groups |
Comparison of the Basic Information of Patients with Sepsis and Without Sepsis
Significant differences were observed in the TBSA, BI, CRP, NLR, IBI, rBaux, the proportion of mechanical ventilation and ICU length of stay between sepsis group and nonsepsis group (P < 0.05); while sex, age, cause of burn, time of admission after injury, WBC, PCT, ALB, Glb, Hb, SCr, BUN, the proportion of inhalation injury and mortality were not significantly different (P>0.05) (Table 1). Meanwhile, the IBI showed no correlation with the rBaux, ICU length of stay, mechanical ventilation or mortality in this study (P>0.05).
Factors Predicting the Development of Sepsis in Burned Patients
Univariate logistic regression analysis revealed TBSA, BI, CRP, and IBI in the early post-burn period as risk factors for the development of sepsis in severely burned patients (P <0.01), and there was no significant collinearity in these indicators (Figure 1). Multivariate logistic regression analysis revealed that TBSA (odds ratio (OR): 1.552; 95% confidence interval (CI): 1.004–2.398; P=0.048), BI (OR: 1.871; 95% CI: 1.198–2.923; P=0.006), CRP (OR: 1.950; 95% CI: 1.243–3.061; P=0.004), and IBI (OR: 2.250; 95% CI: 1.367–3.704; P=0.001) were independent risk factors with regard to the development of sepsis in severely burned patients (P<0.05) (Table 2).
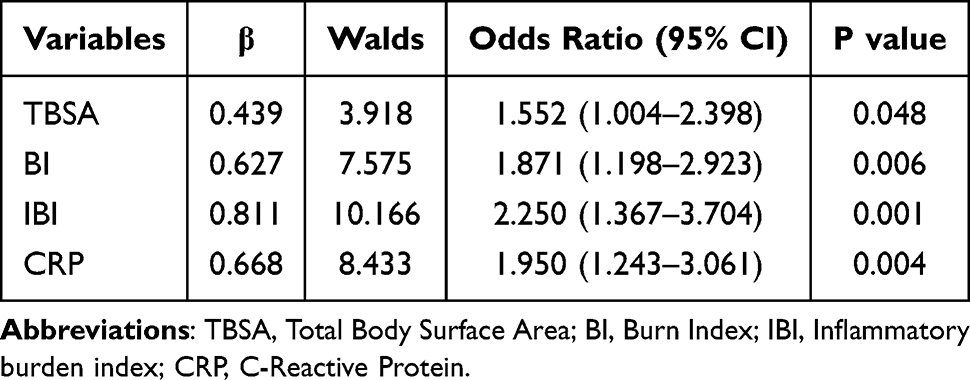 |
Table 2 Risk Factors for Sepsis of Severe Burn Patients Analyzed by Logistic Regression |
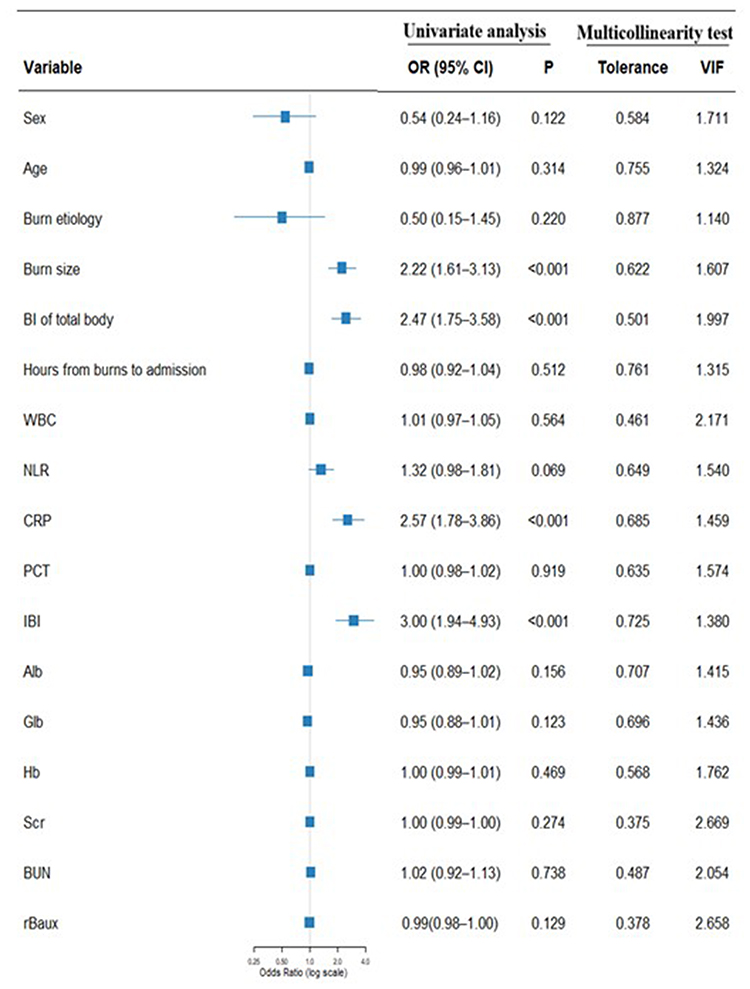 |
Figure 1 Forest plot of risk factors for sepsis determined by the univariate logistic regression analysis and multicollinearity test. TBSA: Total body surface area. Abbreviations: BI, Burn index; WBC, White blood cell count; NLR, Neutrophil-to-lymphocyte ratio; IBI, Inflammatory burden index; CRP, C-reactive protein; PCT, Procalcitonin; Alb, Albumin; Glb, Globulin; Hb, Haemoglobin; SCr, Serum creatinine; BUN, Blood urea nitrogen; rBaux, Revised Baux score. |
Prediction of Sepsis Risk in Severely Burned Patients
ROC curves were used to evaluate the predictive performance of the predictors for the development of sepsis in severely burned patients, and the optimal cut-off values were determined (Figure 2). The results revealed that BI exhibited the largest area under the curve (AUC: 0.751; 95% CI: 0.678–0.825; P=0.000) value, followed by IBI (AUC: 0.746; 95% CI: 0.671–0.821; P=0.000), TBSA (AUC: 0.709; 95% CI: 0.630–0.787; P = 0.000) and CRP (AUC: 0.701; 95% CI: 0.621–0.780; P = 0.000). The optimal cutoff value for the IBI to distinguish whether patients would develop sepsis was 695.01. ROC curves were constructed using the BI combined with the IBI, and the analysis results revealed that the AUC for BI combined with IBI was significantly greater than that for BI alone and IBI alone (AUC: 0.831; 95% CI: 0.770–0.892; P = 0.000) (Figure 3).
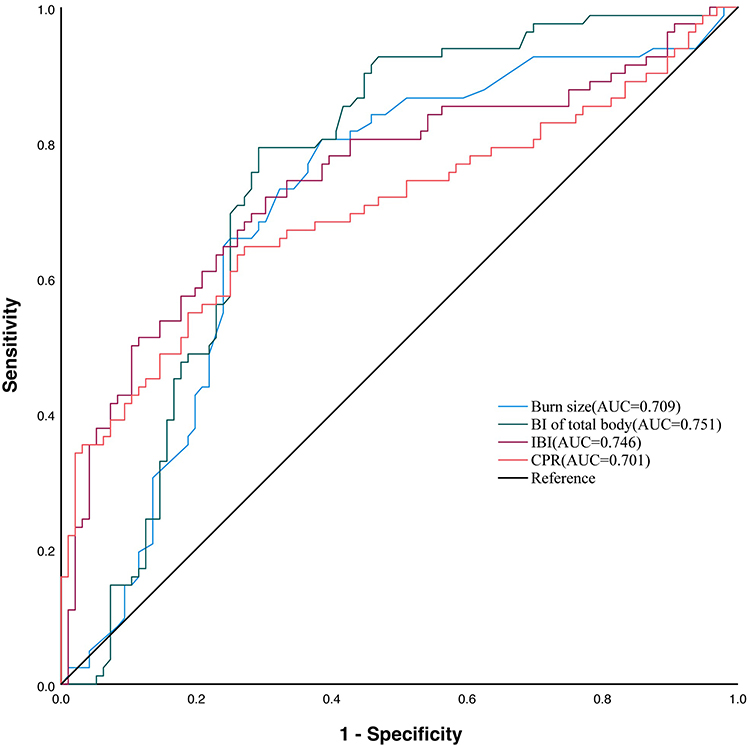 |
Figure 2 Evaluation of the predictive value of predictors for sepsis development in severe burn patients via the ROC curve. The ROC curves illustrate the predictive performance of TBSA (AUC = 0.709), BI (AUC = 0.751), IBI (AUC = 0.746), and CRP (AUC = 0.701) for sepsis in severe burn patients. Abbreviations: BI, Burn Index; IBI, Inflammatory burden index; CRP, C-reactive protein. |
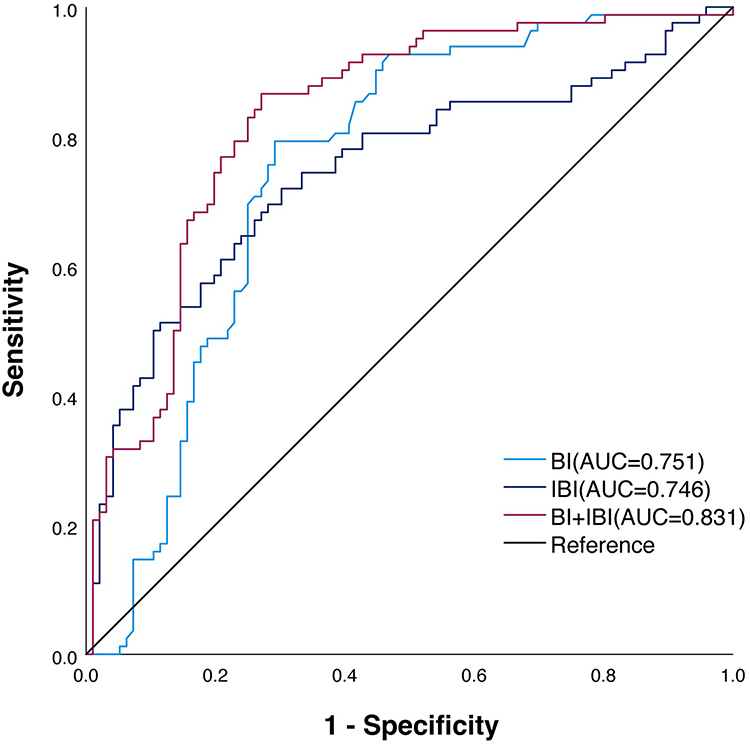 |
Figure 3 ROC curve analysis of the combined burn index and IBI. The ROC curves illustrate the predictive performance for sepsis in severe burn patients using BI (AUC = 0.751), IBI (AUC = 0.746), and their combination (BI + IBI, AUC = 0.831). Abbreviations: BI, Burn index; IBI, Inflammatory burden index. |
Comparison of Clinical Data Between the High IBI and Low IBI Group
In accordance with the IBI cut-off value, the patients were divided into a high IBI group and a low IBI group, with 88 patients in the high IBI group and 90 patients in the low IBI group. The results revealed that the incidence of sepsis was significantly different between the two groups of patients (P <0.05), and the serum ALB level in the low-IBI group was greater than that in the high-IBI group (P <0.05). No significant differences were observed between the two groups of patients in terms of sex, age, cause of burn, time of admission after injury, or WBC, PCT, Glb, Hb, SCr, and BUN levels (P>0.05) (Table 3).
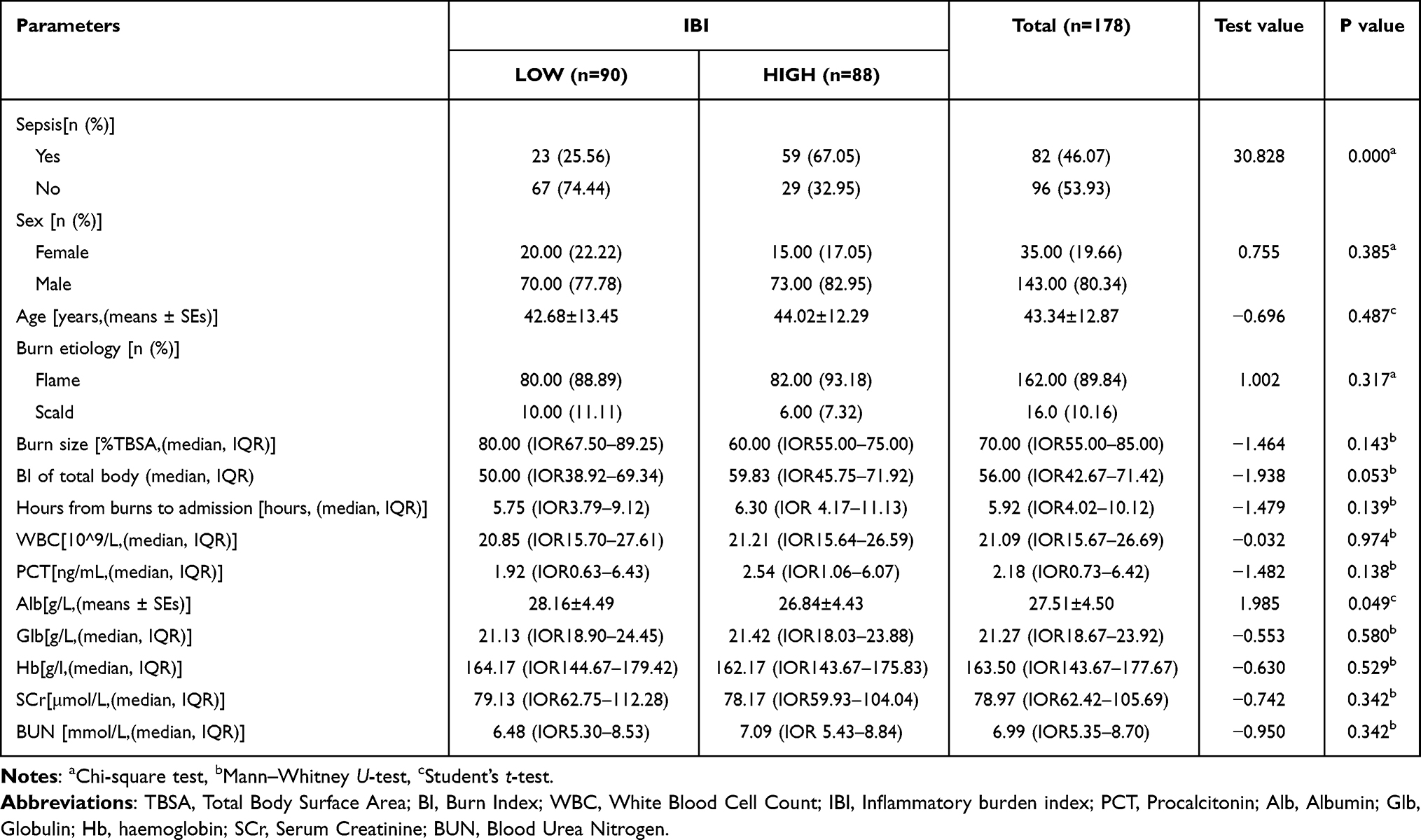 |
Table 3 Clinical Characteristics of Subjects Grouped by IBI |
Discussion
Sepsis is the leading cause of death in severely burned patients. Previous studies have reported that the mortality of critically ill patients with extensive burns suffering from complications with sepsis can reach 58.9%.12,13 In patients with extensive burns, the body’s homeostasis is disrupted, leading to severe complications and physiological conditions. Sepsis is typically correlated with burn severity and subsequent cascade of immune and inflammatory responses. Early determination of burn severity and treatment is vital for prognosis. Recent studies have shown that some biomarkers during the early post-burn phase can predict the onset of sepsis. Xu et al found that increased serum PCT concentrations in the early post-burn period could predict the onset of sepsis within 60 days of the burn, which may serve as an early indicator of burn severity.14 Pileri et al showed that as early as hospital admission, serum IL-6 and IL-10 levels have been found to be higher in septic burn patients than their non-septic counterparts. Meanwhile, levels of these cytokines were found to correlate with the severity of sepsis.15 Moreover, these predictive indicators can assist in formulating treatment strategies, including early surgical intervention, antibiotic application, and enteral nutritionet al, to reduce the incidence of sepsis. However, the clinical significance of IBI levels during the early phase of extensive burns have rarely been reported. This study indicated that the IBI in the early post-burn period was an independent risk factor for sepsis, which can be used to predict burn sepsis in clinical practice.
CRP is a classic clinical nonspecific inflammatory marker, and its abundance is usually significantly increased when the body is infected, especially in sepsis.16,17 PCT is also widely used as a biomarker in clinical practice and plays a certain role in the early diagnosis of sepsis. When the body suffers from sepsis, PCT increases obviously, even thousands of times higher than the baseline level.17–19 The NLR is an inflammatory indicator reflecting the comprehensive influence of innate immunity mediated by neutrophils and adaptive immunity mediated by lymphocytes, which is associated with disease-specific mortality, including heart disease, chronic lower respiratory disease, pneumonia, and kidney disease.20,21 The IBI is a new inflammation indicator that combines the levels of CRP, neutrophils, and lymphocytes to assess inflammation more comprehensively, stably and accurately, which not only distinguishes the prognosis of patients with different inflammation levels but also provides significant prognostic stratification for cancer, respiratory diseases, heart failure and sepsis.22–24 In this study, the results identified IBI and CRP as independent risk factors for sepsis in severely burned patients. The ROC curves revealed that the predictive value of the IBI for sepsis was better than that of the CRP, and the combination of the IBI and BI could further increase the predictive value. The IBI outperformed CRP, likely due to its integration of multiple inflammatory and immune response markers to provide a more complete picture of the patient’s status, which is closely related with subsequent systemic inflammation and organ dysfunction caused by sepsis.25,26 This study further used the best cut-off value for the IBI (695.01) to divide the patients into a high IBI group and a low IBI group for comparison. The incidence of sepsis in the high IBI group was significantly greater than that in the low IBI group. Differences in Alb levels between the two groups may be related to the reduced Alb production and increased leakage from blood vessels, which are due to more intense inflammatory responses in the high IBI group. In this study, no significant difference in PCT levels was observed between the sepsis group and the nonsepsis group, which may be attributed to the significant influence of noninfectious factors, such as traumatic stress and inadequate tissue perfusion, during the early post-burn period.
This study also has limitations. First, due to the single-centre design and its retrospective nature, inherent biases were inescapable. Second, the mean age of the patients is low compared to other studies. The influence of age and concomitant pathologies on the prognosis should be taken into account. Third, the sequential organ failure assessment (SOFA) score was not utilized in the study. Since this study is a retrospective analysis conducted from 2014 to 2023, some early patients did not undergo Glasgow Coma Scale assessments, and the mean arterial pressure (MAP) or vasoactive agents were not provided in some medical records. Therefore, accurate SOFA scores cannot be determined. Nevertheless, the SOFA score and Sepsis 3.0 will be applied in our further prospective study. Moreover, dynamics of the biomarkers can provide more reliable information to clinicians, and the combination of repeated measurements together with other laboratory biomarkers can strengthen sepsis diagnosis.
Conclusions
The IBI in the early post-burn period offers good predictive value for the development of sepsis in critically ill patients with extensive burns. High level of the IBI, especially more than 695.01, indicates the increased risk of sepsis, which means that the early intervention treatments should be initiated to reduce the incidence of sepsis. Moreover, combination of IBI with BI can improve the predictive performance.
Data Sharing Statement
The data are available from the corresponding author on reasonable request.
Ethical Approval Statement
Ethical approval was obtained from the Institutional Review Board.
Author Contributions
Songwei Zhou: Conceptualization, Methodology, Writing-Original draft creation.
Xin He: Data collection, Writing-Original draft preparation.
Yuqun Huang: Data collection, Writing-Original draft preparation.
Wei Zhu: Investigation, Validation.
Huapei Song: Supervision, Writing- Reviewing and Editing.
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by grants from Chongqing Science and Health Joint Medical Research Project (2026DBXM003).
Disclosure
The authors declare no conflict of interest.
References
1. Jeschke MG, van Baar ME, Choudhry MA, Chung KK, Gibran NS, Logsetty S. Burn injury. Nat Rev Dis Primers. 2020;6(1):11. doi:10.1038/s41572-020-0145-5
2. Manning J. Sepsis in the burn patient. Crit Care Nurs Clin North Am. 2018;30(3):423–10. doi:10.1016/j.cnc.2018.05.010
3. Bang RL, Sharma PN, Sanyal SC, Bang S, Ebrahim MK. Burn septicaemia in Kuwait: associated demographic and clinical factors. Med Princ Pract. 2004;13(3):136–141. doi:10.1159/000076952
4. Stanojcic M, Vinaik R, Jeschke MG. Status and challenges of predicting and diagnosing sepsis in burn patients. Surg Infect. 2018;19(2):168–175. doi:10.1089/sur.2017.288
5. Yoon J, Kym D, Hur J, et al. Comparative usefulness of sepsis-3, burn sepsis, and conventional sepsis criteria in patients with major burns. Crit Care Med. 2018;46(7):e656–e662. doi:10.1097/CCM.0000000000003144
6. Khalaf F, Touma D, Pappas A, Hatim L, Wojtowicz-Piotrowski S, Jeschke MG. Decoding burn trauma: biomarkers for early diagnosis of burn-induced pathologies. Biomark Res. 2024;12(1):160. doi:10.1186/s40364-024-00707-5
7. Zhang J, Zhao Q, Hu Z. Clinical predictive value of the initial neutrophils to lymphocytes and platelets ratio for prognosis of sepsis patients in the intensive care unit: a retrospective study. Front Med Lausanne. 2024;11:1351492. doi:10.3389/fmed.2024.1351492
8. Deng J, Hua J, Zeng T, et al. Associations between inflammatory burden index, prostate cancer, and mortality among middle-aged and elderly individuals. World J Urol. 2024;42(1):538. doi:10.1007/s00345-024-05241-5
9. Xiong Z, Xu W, Wang Y, Cao S, Zeng X, Yang P. Inflammatory burden index: associations between osteoarthritis and all-cause mortality among individuals with osteoarthritis. BMC Public Health. 2024;24(1):2203. doi:10.1186/s12889-024-19632-1
10. Xie H, Ruan G, Ge Y, et al. Inflammatory burden as a prognostic biomarker for cancer. Clin Nutr. 2022;41(6):1236–1243. doi:10.1016/j.clnu.2022.04.019
11. Greenhalgh DG, Saffle JR, Holmes JH, et al. American Burn Association consensus conference to define sepsis and infection inburns. J Burn Care Res. 2007;28(6):776–790. doi:10.1097/BCR.0b013e3181599bc9
12. Xu Y, Jin X, Shao X, Zheng F, Zhou H. Valuable prognostic indicators for severe burn sepsis with inhalation lesion: age, platelet count, and procalcitonin. Burns Trauma. 2018;6:29. doi:10.1186/s41038-018-0132-1
13. Yao YM, Sheng ZY, Chai JK. The pathogenesis and management of severe sepsis after burns. Zhonghua Shao Shang Za Zhi. 2008;24(5):337–339.
14. Xu L, Jin J, Wu G, et al. Elevated serum procalcitonin early after extensive burn: influencing factors and clinical significance. Burns J Int Soc Burn Inj. 2021;47(6):1399–1407. doi:10.1016/j.burns.2020.12.010
15. Pileri D, Accardo Palombo A, D’Amelio L, et al. Concentrations of cytokines IL-6 and IL-10 in plasma of burn patients: their relationship to sepsis and outcome. Ann Burns Fire Disasters. 2008;21(4):182–185.
16. Aggarwal N, Karki D, Gaind R, Matlani M, Muthukumar V. Serum procalcitonin and C-reactive protein as indices of early sepsis and mortality in North Indian pediatric burn injuries: a prospective evaluation and literature review. Acute Crit Care. 2024;39(3):350–358. doi:10.4266/acc.2023.00759
17. Gülhan B, Kanık Yüksek S, Hayran M, et al. Infections in pediatric burn patients: an analysis of one hundred eighty-one patients. Surg Infect. 2020;21(4):357–362. doi:10.1089/sur.2019.010
18. Li AT, Moussa A, Gus E, et al. Biomarkers for the early diagnosis of sepsis in burns: systematic review and meta-analysis. Ann Surg. 2022;275(4):654–662. doi:10.1097/SLA.0000000000005198
19. Tan J, Li N, Gong Y, Yuan L, Zhou J, Luo G. Procalcitonin kinetics early after severe burn injury and its value in diagnosis of sepsis. Burns. 2021;47(8):1802–1809. doi:10.1016/j.burns.2021.02.024
20. Song M, Graubard BI, Rabkin CS, Engels EA. Neutrophil-to-lymphocyte ratio and mortality in the United States general population. Sci Rep. 2021;11(1):464. doi:10.1038/s41598-020-79431-7
21. Li F, He Q, Peng H, et al. The systemic inflammation indexes after admission predict in-hospital mortality in patients with extensive burns. Burns. 2024;50(4):980–990. doi:10.1016/j.burns.2024.01.020
22. Xie H, Ruan G, Wei L, et al. Comprehensive comparative analysis of prognostic value of serum systemic inflammation biomarkers for colorectal cancer: results from a large multicenter collaboration. Front Immunol. 2022;13:1092498. doi:10.3389/fimmu.2022.1092498
23. Zhu N, Lin S, Wang L, Kong X, Huang W, Cao C. Elevated inflammatory burden index increases mortality in adults with chronic inflammatory airway diseases: a nationwide cohort study. BMC Pulm Med. 2024;24(1):399. doi:10.1186/s12890-024-03211-6
24. X YL, Z HW, He C, et al. Association between inflammatory burden index and risk of heart failure: evidence from NHANES 2003–2017. BMC Cardiovasc Disord. 2025;25(1):318. doi:10.1186/s12872-025-04781-x
25. Zhong Z, Fan M, Lv L, Long Q, Li K, Xu P. Inflammatory burden index as a predictor of mortality in septic patients: a retrospective study using the MIMIC-IV database. BMC Infect Dis. 2025;25(1):552. doi:10.1186/s12879-025-10936-0
26. Song Z, Lin F, Chen Y, et al. Inflammatory burden index: association between novel systemic inflammatory biomarkers and prognosis as well as in-hospital complications of patients with aneurysmal subarachnoid hemorrhage. J Inflamm Res. 2023;16:3911–3921. doi:10.2147/JIR.S416295
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Marked Non-Infectious Elevation of Procalcitonin in a Hemodialysis Patient with Bladder Cancer: A Case Report
Yan YC, Guo Q, Xu J, Wei Z, Li J
Infection and Drug Resistance 2026, 19:569356
Published Date: 17 January 2026