Back to Journals » Journal of Pain Research » Volume 19
Predictive Value of Epidural Gas Spread Pattern Following Transforaminal Ozone Injection for Clinical Outcomes in Cervical Radiculopathy: A Prospective Cohort Study
Authors Yang M, Qiong X, Xu X, Abdullah Al-Goshae HA
Received 23 December 2025
Accepted for publication 16 March 2026
Published 21 March 2026 Volume 2026:19 591176
DOI https://doi.org/10.2147/JPR.S591176
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Andrea Tinnirello
Maojiang Yang,1,2,* Xian Qiong,1,* Xiaoxue Xu,1 Husni Ahmed Abdullah Al-Goshae2
1Department of Pain, Affiliated Hospital of North Sichuan Medical College, Nanchong, Sichuan, 637000, People’s Republic of China; 2School of Graduate Studies, Management and Science University (MSU), Shah Alam, Selangor, 40100, Malaysia
*These authors contributed equally to this work
Correspondence: Xiaoxue Xu, Department of Pain, Affiliated Hospital of North Sichuan Medical College, Nanchong, Sichuan, People’s Republic of China, Email [email protected] Husni Ahmed Abdullah Al-Goshae, School of Graduate Studies, Management and Science University, Shah Alam, Selangor, Malaysia, Email [email protected]
Background: Percutaneous interventions for cervical radiculopathy (CR) show variable efficacy, lacking reliable prognostic predictors. We hypothesized that epidural gas spread patterns during CT-guided ozone injection—using ozone as a native contrast agent—can functionally assess epidural adhesions and predict clinical outcomes.
Methods: This prospective, observational cohort study enrolled 185 patients with single-segment CR completing a 6-month follow-up. During CT-guided transforaminal ozone injection, epidural gas spread was evaluated before administering the therapeutic dose. Patients were classified into Good Spread (GS; n=98) or Poor Spread (PS; n=87) groups. Primary (Neck Disability Index, NDI) and secondary (Visual Analog Scale, VAS) outcomes were assessed at baseline and multiple post-intervention time points up to 6 months.
Results: Both groups showed significant NDI and VAS improvements from baseline (p< 0.001). However, the GS group exhibited significantly greater improvement at all follow-ups (p< 0.01). At 6 months, treatment success (≥ 50% NDI reduction) was 89.8% in the GS group versus 44.8% in the PS group (p< 0.001). Multivariate analysis identified a good spread pattern (OR=9.80, 95% CI: 4.51– 21.30; p< 0.001) and shorter symptom duration (OR=4.50, p=0.004) as independent predictors of treatment success.
Conclusion: This study suggests that the epidural diffusion pattern of ozone gas during CT-guided transforaminal injection may be a useful predictor for clinical outcomes in CR. These findings highlight the potential role of epidural adhesions in treatment response. However, due to the single-center observational design, our findings may lack broad generalizability, and future randomized controlled trials are necessary to confirm these results.
Keywords: cervical radiculopathy, ozone therapy, CT-guided, transforaminal injection, gas spread, prognostic prediction, epidural adhesion
Introduction
Degenerative cervical spondylosis (DCS) encompasses a spectrum of subdiseases, including cervical radiculopathy (CR) and cervical spondylotic myelopathy (CSM). CR represents a prevalent clinical entity, accounting for 60–70% of all DCS cases.1–3 The primary therapeutic goals for CR are pain alleviation and functional restoration. Among diverse treatment modalities, percutaneous targeted injections have gained widespread clinical adoption due to their minimally invasive nature and precision.4 In particular, CT-guided transforaminal injections leverage unparalleled anatomical resolution and three-dimensional localization capabilities, ensuring precise needle placement within target regions while maximizing therapeutic targeting and avoiding critical structures.5
Despite technological advancements, substantial interindividual variability in treatment efficacy remains a central challenge in CR interventions. Clinicians frequently encounter the perplexing phenomenon of imaging-symptom mismatch: asymptomatic individuals may exhibit disc herniations on MRI, while patients with severe symptoms might display minimal radiographic abnormalities.6,7 This discrepancy complicates clinical decision-making, rendering it difficult to prognosticate outcomes or select optimal therapies based solely on herniation size.
The traditional “mechanical compression” theory—which posits a direct correlation between symptom severity and nerve root compression—fails to fully explain this clinical complexity. Recent pathophysiological research has shifted focus from pure mechanical compression to chemical inflammation and secondary changes triggered by herniated disc material.8 Herniated nucleus pulposus acts as a “foreign body”, releasing inflammatory mediators such as tumor necrosis factor-α (TNF-α) and interleukins (ILs), which incite aseptic inflammation in the epidural space.9–11 This chronic inflammation drives epidural adhesions (or epidural fibrosis), which tether nerve roots, restrict physiological gliding within the spinal canal, and subject neural structures to repetitive microtrauma during neck movement, ultimately manifesting as intractable pain and dysfunction.12,13 We postulate that adhesive pathology is the core mechanism underlying imaging-symptom mismatch.
Consequently, we hypothesize that the success of injective therapies hinges fundamentally on the ability of therapeutic agents to penetrate adhesive barriers and reach affected spinal nerves. Thus, real-time assessment of drug distribution during injection may hold greater prognostic value than static preoperative imaging. Recent studies have well-documented the clinical utility of ozone-related interventions; for instance, previous research has demonstrated the safety and efficacy of CT-guided pulsed radiofrequency combined with steroid and ozone injections for treating cervical herpes zoster neuralgia.14 However, while existing literature primarily focuses on the ultimate therapeutic outcomes of ozone, its potential as an intraoperative prognostic indicator remains unexplored.
To address this gap, the novelty of the present study lies in utilizing medical ozone (O3) not only as a therapeutic agent but functionally as an excellent native negative contrast medium on CT imaging due to its gaseous state.15 This unique property offers an opportunity to dynamically evaluate epidural patency and adhesion severity by directly visualizing the spread pattern of the ozone gas itself, without the need for additional contrast agents. To rigorously investigate our central hypothesis—that the epidural spread pattern of ozone gas can effectively predict clinical outcomes—a prospective cohort study design was specifically chosen. This approach allowed us to systematically standardize the real-time evaluation of the gas dispersion pattern during CT-guided transforaminal injections and accurately track these cohorts. By correlating these intraoperative spread patterns with 6-month clinical outcomes, this study aims to validate its prognostic predictive value, thereby pioneering a novel pathway for individualized management and prognostic stratification in patients with cervical radiculopathy.
Methods
Study Design and Ethics
This prospective, single-center, observational cohort study adhered to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines. Importantly, all CT-guided transforaminal ozone injections evaluated in this study were performed strictly as part of routine clinical practice and the standard of care for managing cervical radiculopathy, entirely independent of this observational research protocol. The study protocol was reviewed and approved by the Institutional Review Board (IRB) of the Affiliated Hospital of North Sichuan Medical College (Ethics Approval No: 2024ER95-1) and was conducted in strict accordance with the ethical principles of the Declaration of Helsinki. All participants provided written informed consent after receiving comprehensive explanations of the observational procedures.
Study Population
Between January 2024 and December 2024, patients with cervical radiculopathy were consecutively enrolled from the Department of Pain Medicine and Interventional Radiology at our institution.
Inclusion Criteria
- Age 18–70 years;
- Clinical and MRI-confirmed single-level disc bulging/protrusion with symptom-imaging concordance;
- Symptom duration >3 months and suboptimal response to standard conservative therapy (eg., pharmacotherapy, physical therapy);
- Willingness and ability to complete all follow-ups.
Exclusion Criteria
- Clinical signs of spinal cord compression;
- Multilevel or bilateral symptoms;
- Disc extrusion or sequestration;
- Cervical spine tumors, infection, fracture, severe instability, or prior surgery;
- Severe cardiopulmonary disease, coagulopathy, or immune disorders;
- Known ozone intolerance or glucose-6-phosphate dehydrogenase (G6PD) deficiency;
- Pregnancy or lactation.
CT-Guided Interventional Procedure
All procedures were performed by the same team of physicians with extensive expertise in CT-guided interventions using a 128-slice spiral CT scanner (Siemens Somatom Definition AS).
Preparation and Positioning
Patients were placed in the supine position, secured to the CT table, with the head slightly rotated toward the symptomatic side. Initial axial thin-slice scanning of the target segment was performed to determine the optimal puncture trajectory, avoiding vascular/bony structures while achieving the shortest path to the anterolateral aspect of the target intervertebral foramen.
Puncture Technique
Under CT laser guidance, the skin was sterilized and draped. Local anesthesia was administered along the puncture path using 1% lidocaine. A 22-gauge, 10-cm coaxial introducer needle was advanced along the predetermined trajectory using an iterative scan-advance-rescan technique. Final needle tip position was confirmed by CT to reside within the intervertebral foramen adjacent to the nerve root sleeve. This approach leverages CT’s superior soft-tissue/vascular resolution for millimeter-level precision.
Gas Spread Assessment and Group Stratification
After confirming optimal needle placement, 10 mL of medical ozone (30 μg/mL; Ozonosan® generator, Germany) was slowly injected as a negative contrast agent. Immediate volumetric CT scanning (1-mm slice thickness) was performed. Axial reconstructions were analyzed on a dedicated workstation to evaluate gas dispersion patterns. Patients were classified as:
Good Spread (GS) Group
Gas (appearing as hypodense black shadows) flowed medially along the nerve root sleeve into the anterior epidural space, forming a well-defined crescent-shaped silhouette around the dural sac (Figure 1A). Concurrent circumferential perineural spread within the foramen was observed.
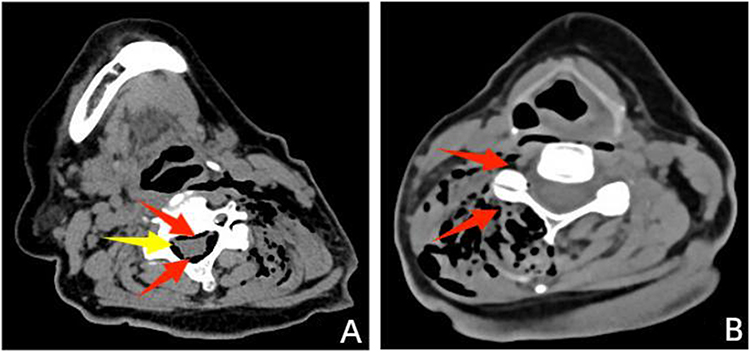 |
Figure 1 CT-guided transforaminal ozone injection. (A) Good Spread (GS) Pattern: Hypodense gas (black shadow) forms a distinct crescent-shaped silhouette surrounding the dural sac (red arrowhead), with circumferential dispersion along the nerve root within the intervertebral foramen (yellow arrowhead). (B) Poor Spread (PS) Pattern: Gas exhibits restricted dispersion, appearing as clustered accumulation around the facet joint (red arrowhead) and absent distribution near the dural sac, indicating adhesive obstruction. |
Poor Spread (PS) Group
Gas dispersion was restricted, manifesting as: (a) Clustered accumulation around facet joints; (b) Isolated lateral spread without medial flow; (c) Irregular dispersion with abrupt termination at invisible tissue barriers (Figure 1B). These patterns indicated epidural adhesions impeding gas distribution.
Therapeutic Completion and Postprocedural Care
Therapeutic Injection
Following group stratification, a 5-mL therapeutic cocktail was slowly injected: Compound Betamethasone: (1 mg total dose (0.4 mg betamethasone dipropionate + 0.6 mg betamethasone sodium phosphate), Lidocaine: 12.5 mg (0.25% solution)), diluted to 5 mL volume with 0.9% physiological saline.
The needle was then withdrawn, the puncture site compressed, and an aseptic dressing applied.
Postprocedural Management
Patients were monitored in the recovery area for 1 hour to assess for immediate complications. Upon confirming absence of adverse events (eg., neural irritation, vasovagal reactions), then returned to the ward.
Data Collection and Outcome Assessment
Baseline data included demographic characteristics, clinical features, MRI-based disc pathology grading (bulging/protrusion), and pretreatment clinical scores. The primary outcome was the Neck Disability Index (NDI),16 with the Visual Analog Scale (VAS) for neck/arm pain as the secondary outcome.17 Follow-up assessments occurred at baseline, 1 week, 1 month, 3 months, and 6 months post-intervention, conducted by an independent researcher blinded to group allocation via outpatient visits or structured telephone interviews. Treatment success was defined a priori as ≥50% improvement in NDI score from baseline at the 6-month endpoint.
Statistical Analysis
Statistical analyses were performed using SPSS 26.0 (IBM Corp., USA). Baseline characteristics were compared between groups via independent samples *t*-test or Mann–Whitney-U test, as appropriate for data distribution. Longitudinal changes in clinical scores were analyzed using repeated-measures ANOVA with assessment of group-by-time interaction effects. Treatment success rates were compared using Pearson’s chi-square test. Binary logistic regression identified independent predictors of treatment success, with spread pattern (GS/PS) and baseline variables included as covariates. A two-tailed p-value <0.05 defined statistical significance.
Results
Patient Baseline Characteristics
A total of 210 patients were enrolled during the study period, with 185 (88.1%) completing the 6-month follow-up and included in the final analysis (Good Spread [GS] group:n=98; Poor Spread [PS] group: n=87). Baseline characteristics—including age, sex, symptom duration, and affected level—were well-balanced between groups. Critically, no significant differences were observed in pretreatment NDI or VAS scores, nor in MRI-based adhesion and herniation grading, confirming robust comparability (Table 1).
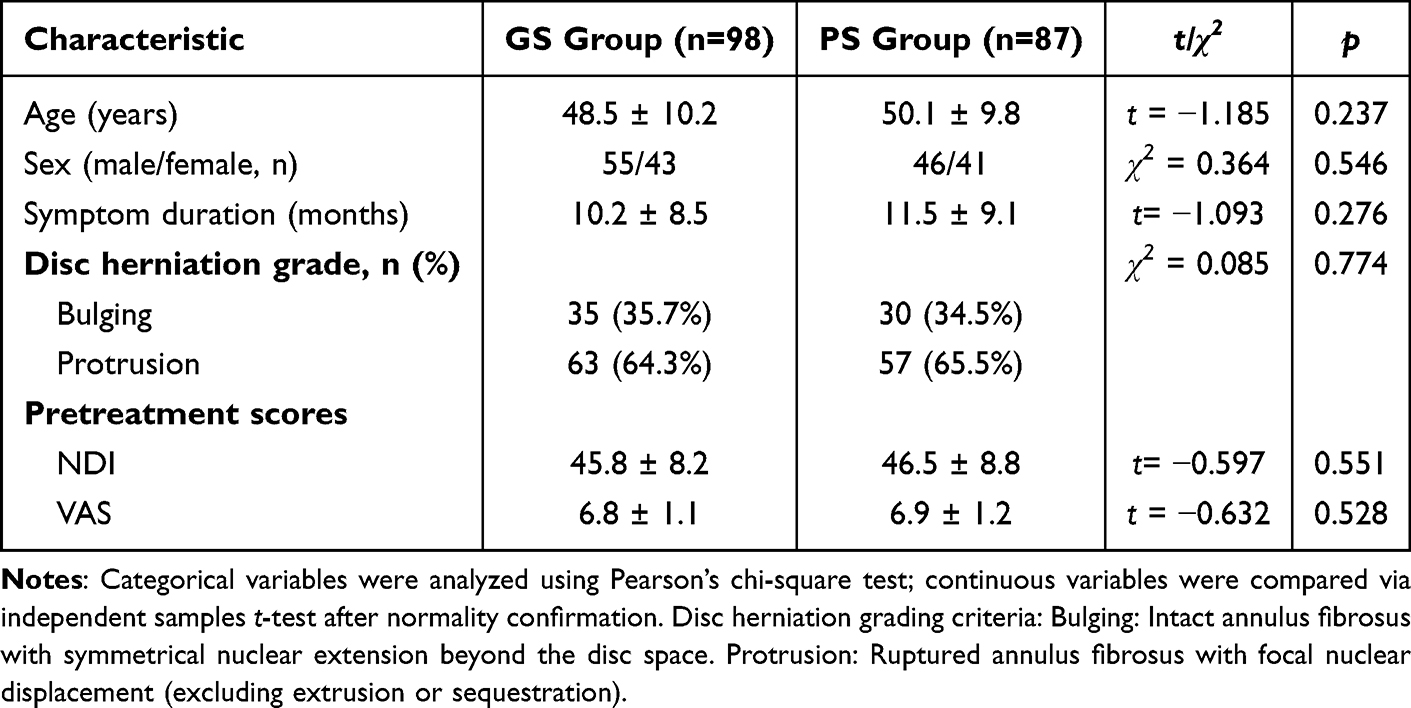 |
Table 1 Comparison of Baseline Characteristics Between Groups |
Longitudinal Comparison of Clinical Outcomes
Repeated-measures ANOVA revealed highly significant main effects of time (p < 0.001p<0.001) and group-by-time interactions for both outcomes (NDI: F=48.7, p<0.001; VAS: F=38.2, p<0.001), indicating divergent clinical trajectories between groups.
Both groups exhibited declining NDI and VAS scores post-intervention. The GS group demonstrated sustained and substantial improvement, with NDI decreasing to 10.2±4.1 at 6 months. While the PS group showed significant improvement, its magnitude was markedly smaller (6-month NDI: 25.1±7.9). Critically, the GS group achieved significantly superior NDI and VAS scores at all postoperative follow-ups (p < 0.01) (Table 2 and Figure 2).
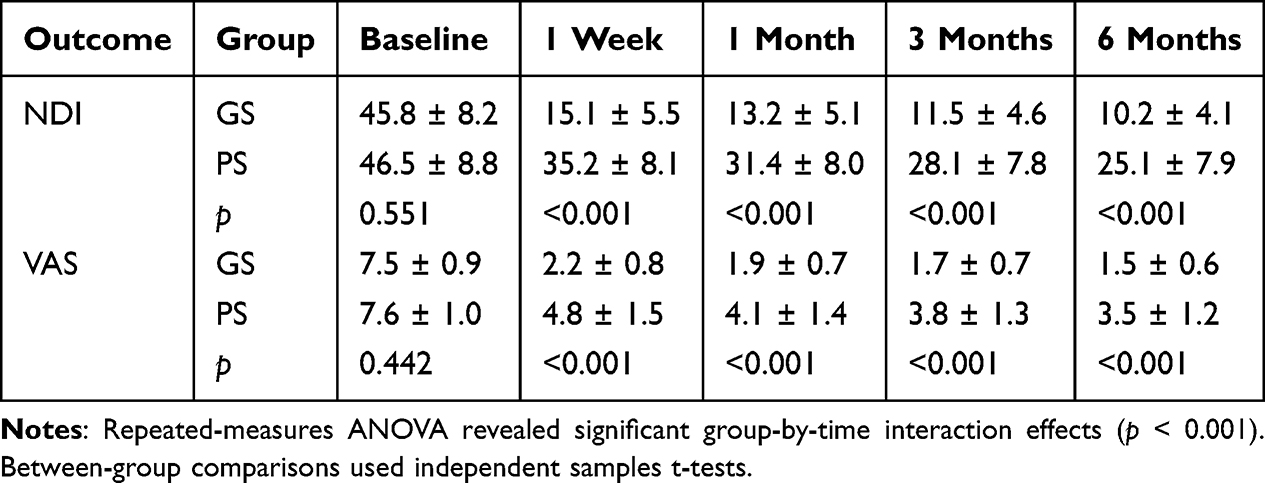 |
Table 2 Comparison of Clinical Scores at Follow-Up Timepoints |
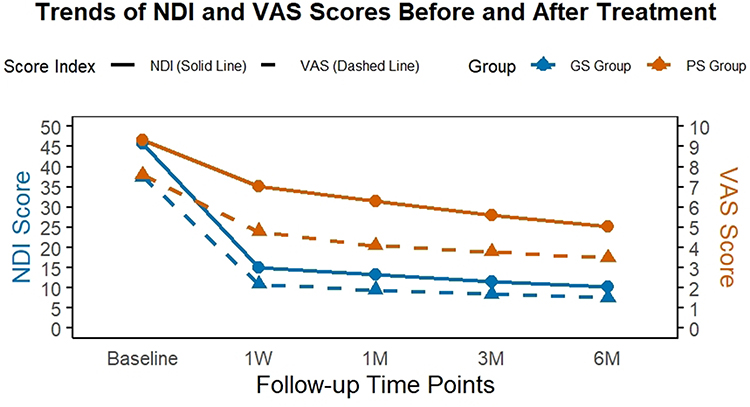 |
Figure 2 Longitudinal Trends in NDI and VAS Scores. Solid lines: Neck Disability Index (NDI); Dashed lines: Visual Analog Scale (VAS). Error bars denote SD. Abbreviations: GS, Good Spread; PS, Poor Spread. |
Treatment Success Rates and Predictor Analysis
Using the predefined success criterion (≥50% improvement in NDI at 6 months), the GS group achieved a significantly higher success rate of 89.8% (88/98) compared to 44.8% (39/87) in the PS group. Despite partial efficacy in the PS cohort, this represented a striking between-group difference (χ2 = 42.1, p < 0.001) (Table 3).
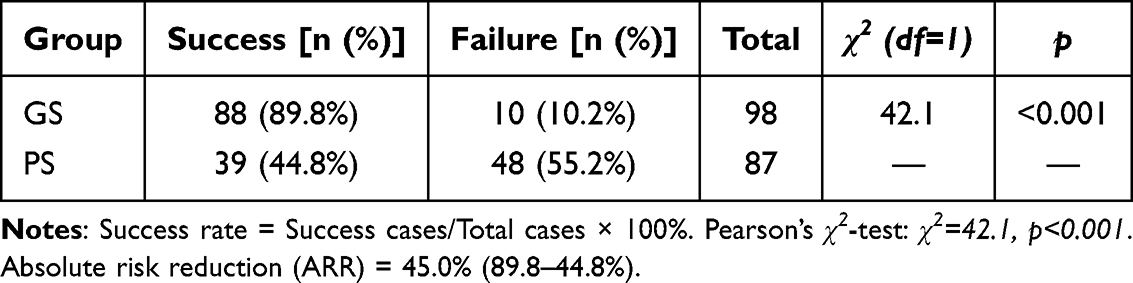 |
Table 3 Treatment Success Rates Based on ≥50% NDI Improvement |
Binary Logistic Regression Analysis
Multivariable analysis incorporating all potential predictors identified favorable gas spread (GS group) and symptom duration as independent predictors of treatment success. Optimal dispersion pattern emerged as the strongest predictor, with GS patients exhibiting 9.80-fold higher odds of success versus PS (OR = 9.80, 95% CI: 4.51–21.30; p < 0.001). Symptom duration demonstrated significant but lesser predictive value (OR = 4.50, 95% CI: 1.78–11.37; p = 0.004). Age, sex, and MRI grading showed no independent associations (Table 4 and Figure 3).
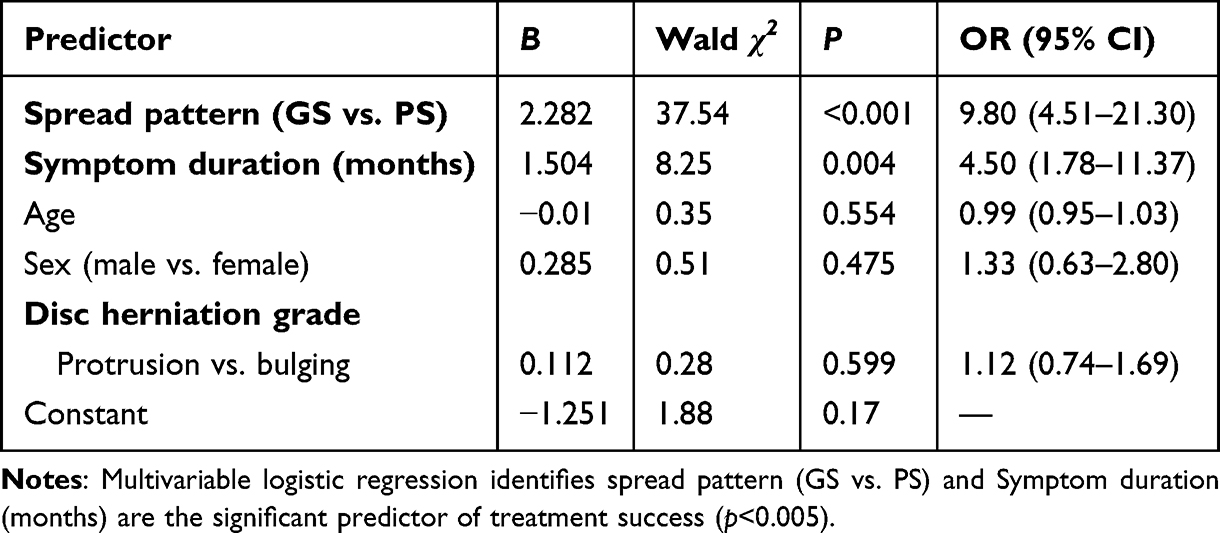 |
Table 4 Multivariable Logistic Regression Analysis for Treatment Success at 6 Month |
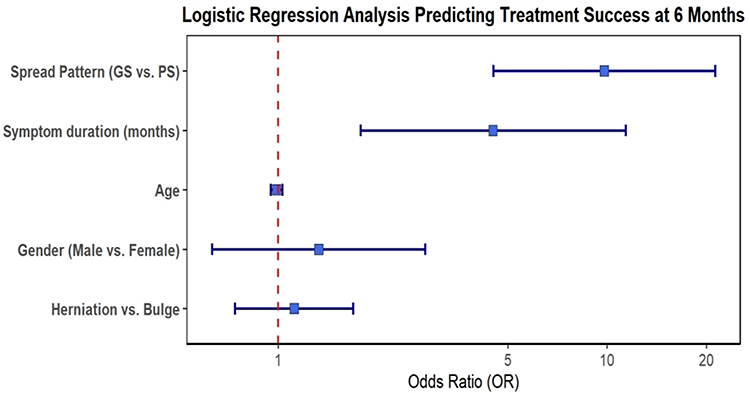 |
Figure 3 The forest plot shows the results of a multivariate logistic regression analysis to predict treatment success at 6 months. The squares and horizontal lines represent the odds ratios (OR) and 95% confidence intervals (CI), respectively. A vertical dashed line at OR=1 indicates no effect. As the CIs for both spread pattern and symptom duration do not cross this line, they are identified as significant independent predictors of treatment success. |
Adverse Events
All procedures were successfully completed under precise CT guidance, with no occurrence of severe complications such as vascular injury, permanent nerve damage, or infection. A total of 15 patients (8.1%) reported transient distending pain during the injection, which was similar to their original symptoms. These symptoms were well-tolerated after slowing the injection rate.No participants withdrew from the study due to adverse events.
Discussion
This prospective cohort study provides compelling evidence that the epidural gas spread pattern, visualized on CT during transforaminal ozone injection, is a decisive factor in predicting clinical outcomes for patients with cervical radiculopathy. The principal finding is that patients exhibiting good epidural spread of the gas achieve dramatically better functional improvement and higher rates of treatment success compared to those with poor spread. This finding not only introduces a novel prognostic tool but also offers significant insights into the underlying pathophysiology of CR and has direct implications for refining clinical practice.
Methodological Innovation: A Paradigm for Functional Assessment
The methodology employed in this study represents a dual innovation. First, the exclusive use of high-precision CT guidance for all procedures is a critical strength. Unlike conventional fluoroscopy, CT provides superior cross-sectional visualization of soft-tissue anatomy, enabling sub-millimeter needle tip accuracy and ensuring the definitive avoidance of the vertebral artery and other vital structures.5 This precision effectively eliminates suboptimal needle placement as a potential confounding factor, allowing for a more pure and direct investigation into the relationship between drug distribution and clinical efficacy.
Second, and more fundamentally, this study pioneers the use of the therapeutic agent itself—ozone gas—as an intrinsic negative contrast agent. This approach is innovative for several reasons. It is inherently safe, completely avoiding the risks of allergic reaction and nephrotoxicity associated with iodinated contrast media.18–21 Moreover, it provides a uniquely authentic assessment. Rather than observing the spread of a surrogate substance, we visualized the distribution of the actual treatment agent. This directly addresses the most clinically relevant question: did the medication reach the target pathological site? The high sensitivity of CT to gas density provides excellent delineation of the spread, making this a reliable and high-resolution method for functionally assessing the patency of the epidural space.22
Pathophysiological Interpretation: Vindicating the Adhesion Theory
The results of this study offer strong functional validation for the theory that epidural adhesions are a central element in the pathophysiology of chronic CR and a primary determinant of treatment failure. In the GS group, the unimpeded flow of gas signifies a patent epidural space, allowing the anti-inflammatory and analgesic ozone to comprehensively bathe the inflamed nerve root and surrounding tissues, resulting in excellent clinical outcomes.15,23–25 Conversely, the restricted gas spread observed in the PS group serves as direct, in-vivo evidence of a physical barrier, which we interpret as epidural fibrosis or adhesions. These adhesions effectively sequester the nerve root, preventing the therapeutic agent from reaching the critical neuro-inflammatory interface and thus limiting its efficacy.
An important and nuanced finding is that nearly 45% of patients in the PS group still achieved treatment success. Several mechanisms may account for this. The localized injection of gas, even if contained, may exert a “hydro-dissection” or pressure effect, leading to some degree of mechanical lysis of finer adhesions.26 More plausibly, the needle tip’s proximity to the dorsal root ganglion (DRG) within the foramen is key. The DRG is a critical hub for pain signal generation and transmission.27,28 A concentrated local effect of ozone on the DRG could modulate its excitability and inhibit nociceptive signaling, producing significant pain relief even in the absence of widespread medial epidural spread.29 However, despite this potential for localized benefit, the vast and statistically significant chasm in success rates between the GS (89.8%) and PS (44.8%) groups provides an unequivocal conclusion: while a localized effect on the DRG may be beneficial, achieving broad and thorough coverage of the inflamed nerve root within the epidural space is paramount for maximizing the probability of a robust, durable, and successful clinical outcome.
Clinical Implications and Future Directions
The findings of this study have immediate and significant implications for clinical practice and future research.
First, the gas spread pattern offers a tool for intraoperative prognostication. Clinicians can use this real-time functional information to provide patients with a more accurate, evidence-based prognosis immediately following the diagnostic phase of the injection. For patients with poor spread, expectations can be managed appropriately, and discussions regarding alternative or subsequent treatment strategies can be initiated much earlier in the care pathway.
Second, this technique provides a clear trigger for individualized treatment decision-making. A finding of poor spread should not be viewed as a treatment failure, but rather as a diagnostic finding that necessitates a change in strategy. It provides a powerful, evidence-based rationale to escalate care. This could involve intra-procedural adjustments, such as attempting a different needle trajectory, or it could identify the patient as an ideal candidate for more advanced interventions specifically designed to address adhesions, such as targeted percutaneous epidural adhesiolysis.12,30 This transforms a standard injection from a one-size-fits-all therapy into a diagnostic-therapeutic procedure that can guide a more precise and personalized treatment algorithm.
Third, this method has the potential to refine the design of future clinical trials. A major limitation of many studies in interventional pain medicine is the heterogeneity of the patient population, which can dilute treatment effects and lead to inconclusive results. The gas spread assessment provides a robust method for patient stratification. Future randomized controlled trials could, for example, enroll only patients with poor gas spread to compare the efficacy of standard injection versus targeted adhesiolysis. Such a design would test the intervention in the precise population it is intended to benefit, reducing heterogeneity and increasing the likelihood of generating definitive evidence to guide clinical practice. Future research should focus on validating these findings in a multicenter setting, developing automated software for the quantitative analysis of gas volume and distribution to improve objectivity, and conducting long-term follow-up studies to assess the durability of the observed outcomes.
Limitations
Nevertheless, several limitations of this study should be acknowledged. First, due to the single-center, prospective cohort design, our findings may be influenced by local patient demographics and practice patterns, which inherently limits their broad generalizability. Furthermore, while our results demonstrate a strong prognostic association, this observational design cannot establish definitive causality. If the study had been conducted as a randomized controlled trial (RCT), the results could be considered more definitive. Therefore, future large-scale, multicenter RCTs are imperative to externally validate and confirm these findings. Second, the classification of gas spread was based on a qualitative visual assessment by the performing physicians. Although the criteria were defined a priori, this method retains an element of subjectivity. The development of quantitative, software-based analysis of gas volume and distribution would enhance the objectivity and reproducibility of the grouping. Third, this study did not include a head-to-head comparison with traditional iodinated contrast agents. Finally, the 6-month follow-up period, while appropriate for assessing mid-term outcomes, does not provide information on the long-term durability of the treatment effects or the predictive value of the gas spread pattern beyond this time frame.
Conclusion
In conclusion, this prospective study suggests that the epidural diffusion pattern of ozone gas, assessed intraoperatively during CT-guided transforaminal injection, may be a useful predictor of short- and mid-term treatment outcomes for patients with cervical radiculopathy. This real-time, native contrast assessment could assist in clinical decision-making and patient stratification. However, given the inherent limitations of a single-center prospective cohort design, our findings may lack broad generalizability. Future large-scale, multicenter randomized controlled trials (RCTs) are warranted to confirm these findings and provide more definitive evidence.
Institutional Review Board Statement
The protocol was approved by the Institutional Review Board (IRB) of the Affiliated Hospital of North Sichuan Medical College (Ethics Approval No.: 2024ER95-1) and conducted in accordance with the ethical principles of the Declaration of Helsinki.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Informed Consent Statement
All participants provided written informed consent after receiving comprehensive explanations of the study procedures.
Acknowledgments
Maojiang Yang and Xian Qiong are co-first authors for this study. The authors would like to express their sincere gratitude to the Sichuan Provincial Medical Association and the Affiliated Hospital of North Sichuan Medical College for their financial support and resources. We also extend our appreciation to professor Yang Hanfeng and Xu Xiaoxue for technical assistance and to the patients who participated in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Special Fund of Sichuan Provincial Medical Association (Grant No. 2024HR132) and the Special Fund of Affiliated Hospital of North Sichuan Medical College (Grant No. 2024LC006).
Disclosure
The authors report no relevant conflicts of interest.
References
1. Theodore N. Degenerative cervical spondylosis. New Engl J Med. 2020;383(2):159–10. doi:10.1056/NEJMra2003558
2. Editorial Board of Chinese Journal of Surgery. The experts consensus on the classification, diagnosis and non-surgical treatment of cervical spondylisis (2018). Zhonghua Wai Ke Za Zhi. 2018;56(6):401–402. doi:10.3760/cma.j.issn.0529-5815.2018.06.001
3. Rao R. Neck pain, cervical radiculopathy, and cervical myelopathy: pathophysiology, natural history, and clinical evaluation. J Bone Joint Surg AM. 2002;84(10):1872–1881. doi:10.2106/00004623-200210000-00021
4. Lv J, Mei J, Feng X, et al. Clinical efficacy and safety of posterior minimally invasive surgery in cervical spondylosis: a systematic review. J Orthop Surg Res. 2022;17(1):389. doi:10.1186/s13018-022-03274-3
5. Solberg A, Akle N, Gavito J, et al. The use of cone beam CT in image guided pain management. J Vasc Interv Radiol. 2016;27(3):S265. doi:10.1016/j.jvir.2015.12.674
6. Yang X, Arts MP, Bartels RHMA, et al. The type of cervical disc herniation on MRI does not correlate to clinical outcomes. Bone Joint J. 2022;104-B(11):1242–1248. doi:10.1302/0301-620X.104B11.BJJ-2022-0657.R2
7. Mostofi K, Khouzani RK. Reliability of cervical radiculopathy, its congruence between patient history and medical imaging evidence of disc herniation and its role in surgical decision. Eur J Orthop Surg TR. 2016;26(7):805–808. doi:10.1007/s00590-016-1801-z
8. Lipetz JS. Pathophysiology of inflammatory, degenerative, and compressive radiculopathies. Phys Med Reh Clin N. 2002;13(3):439–449. doi:10.1016/s1047-9651(02)00005-0
9. Omoigui S. The biochemical origin of pain: the origin of all pain is inflammation and the inflammatory response. Part 2 of 3 - inflammatory profile of pain syndromes. Med Hypotheses. 2007;69(6):1169–1178. doi:10.1016/j.mehy.2007.06.033
10. Takahashi N, Yabuki S, Aoki Y, et al. Pathomechanisms of nerve root injury caused by disc herniation: an experimental study of mechanical compression and chemical irritation. Spine. 2003;28(5):435–441. doi:10.1097/01.BRS.0000048645.33118.02
11. Ye F, Lyu FJ, Wang H, et al. The involvement of immune system in intervertebral disc herniation and degeneration. Jor Spine. 2022;5(1):e1196. doi:10.1002/jsp2.1196
12. Trescot AM, Chopra P, Abdi S, et al. Systematic review of effectiveness and complications of adhesiolysis in the management of chronic spinal pain: an update. Pain Physician. 2007;10(1):129–146. PMID: 17256027.
13. Helm Ii S, Noe C, Racz GB.Epidural lysis of adhesions: what every interventional pain physician needs to know. Pain Physician. 2025;28(3):249–257. PMID: 40464890.
14. Ma L, Yao M. Safety and efficacy of CT-Guided pulsed radiofrequency combined with steroid and ozone injection-treated cervical 3-8 herpes zoster neuralgia using a posterior and upper quarter of the cervical foramina puncture approach. J Pain Res. 2022;15:23–32. doi:10.2147/JPR.S333481
15. Hidalgo-Tallón FJ, Torres-Morera LM, Baeza-Noci J, et al. Updated review on ozone therapy in pain medicine. Front Physiol. 2022;13(840623). doi:10.3389/fphys.2022.840623
16. Widbom-Kolhanen S, Pernaa KI, Saltychev M. Reliability and validity of the neck disability index among patients undergoing cervical surgery. Int J Rehabil Res. 2022;45(3):273–278. doi:10.1097/MRR.0000000000000540
17. Delgado DA, Lambert BS, Boutris N, et al. Validation of digital visual analog scale pain scoring with a traditional paper-based visual analog scale in adults. J Am Acad Orthop Surg Glob Res Rev. 2018;2(3):e088. doi:10.5435/JAAOSGlobal-D-17-00088
18. Hosoya T, Yamaguchi K, Akutsu T, et al. Delayed adverse reactions to iodinated contrast media and their risk factors. Radiat Med. 2000;18(1):39–45. PMID: 10852654.
19. An J, Jung H, Kwon OY, et al. Differences in adverse reactions among iodinated contrast media: analysis of the kaers database. J Aller Clin Imm Pract. 2019;7(7):2205–2211. doi:10.1016/j.jaip.2019.02.035
20. Lin X, Yang J, Weng L, et al. Differences in hypersensitivity reactions to iodinated contrast media: analysis of the US food and drug administration adverse event reporting system database. J Aller Clin Imm Pract. 2023;11(5):1494–1502.e6. doi:10.1016/j.jaip.2023.01.027
21. Alkhalifah B. Contrast-Induced acute kidney injury in radiology: recent insights and advances. J Pharm Bioallied Sci. 2024;16(Suppl 4):S3862–S3864. doi:10.4103/jpbs.jpbs_1299_24
22. Lusic H, Grinstaff MW. X-ray-computed tomography contrast agents. CHEM REV. 2012;113(3):1641–1666. doi:10.1021/cr200358s
23. Bocci V, Borrelli E, Zanardi I, et al. The usefulness of ozone treatment in spinal pain. Drug Des Devel Ther. 2015;9:2677–2685. doi:10.2147/DDDT.S74518
24. Serra MEG, Baeza-Noci J, Mendes Abdala CV, et al. The role of ozone treatment as integrative medicine. An evidence and gap map. Front Public Health. 2023;10:1112296. doi:10.3389/fpubh.2022.1112296
25. Zhuang ZG, Lu LJ, Peng BG, et al. Expert consensus of Chinese Association for the Study of Pain on the application of ozone therapy in pain medicine. World J Clin Cases. 2021;9(9):2037–2046. doi:10.12998/wjcc.v9.i9.2037
26. Simonetti L, Raffi L, Cenni P, et al. Pharmacological mechanisms underlying oxygen-ozone therapy for herniated disc. Riv Neuroradiol. 2017;16(2_suppl_part2):201–204. doi:10.1177/1971400903016sp250
27. Berger AA, Liu Y, Possoit H, et al. Dorsal root ganglion (DRG) and chronic pain. Anesth Pain Med. 2021;11(2):e113020. doi:10.5812/aapm.113020
28. Krames ES. The dorsal root ganglion in chronic pain and as a target for neuromodulation: a review. Neuromodulation. 2014;18(1):24–32. doi:10.1111/ner.12247
29. Lin SY, Zhang SZ, An JX, et al. The effect of ultrasound-guided percutaneous ozone injection around cervical dorsal root ganglion in zoster-associated pain: a retrospective study. J Pain Res. 2018;11:2179–2188. doi:10.2147/JPR.S163340
30. Urits I, Schwartz RH, Brinkman J, et al. An evidence based review of epidurolysis for the management of epidural adhesions. Psychopharmacol Bull. 2020;50(4 Suppl 1):74–90. PMID: 33633419.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.