Back to Journals » Infection and Drug Resistance » Volume 16
Prediction of 30-Day Mortality Using the Quick Pitt Bacteremia Score in Hospitalized Patients with Klebsiella pneumoniae Infection
Authors Su C, Tsai IT, Lai CH, Lin KH ![]() , Chen CC
, Chen CC ![]() , Hsu YC
, Hsu YC ![]()
Received 9 May 2023
Accepted for publication 20 July 2023
Published 25 July 2023 Volume 2023:16 Pages 4807—4815
DOI https://doi.org/10.2147/IDR.S420569
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Ching Su,1 I-Ting Tsai,1,2 Chung-Hsu Lai,2,3 Kuo-Hsuan Lin,1 Chia‐Chi Chen,2,4 Yin-Chou Hsu1,2,5– 7
1Department of Emergency Medicine, E-Da Hospital, I-Shou University, Kaohsiung City, 82445, Taiwan; 2School of Medicine, College of Medicine, I-Shou University, Kaohsiung, Taiwan; 3Division of Infectious Diseases, Department of Internal Medicine, E-Da Hospital, I-Shou University, Kaohsiung City, 82445, Taiwan; 4Department of Pathology, E-Da Hospital, I-Shou University, Kaohsiung City, 82445, Taiwan; 5School of Chinese Medicine for Post Baccalaureate, I-Shou University, Kaohsiung, Taiwan; 6School of Medicine for International Student, I-Shou University, Kaohsiung, Taiwan; 7Graduate Institute of Clinical Medicine, College of Medicine, Kaohsiung Medical University, Kaohsiung, Taiwan
Correspondence: Yin-Chou Hsu, Department of Emergency Medicine, E-Da Hospital, No. 1, Yida Road, Jiao-Su Village, Yan-Chao District, Kaohsiung City, 82445, Taiwan, Tel +886-7-615-0011, Fax +886-7-615-5352, Email [email protected]
Purpose: Klebsiella pneumoniae is an important causative pathogen of nosocomial infections, resulting in poor prognosis owing to its hypervirulence and antibiotic resistance. A simplified quicker version of the Pitt bacteremia score (PBS) (qPitt) for acute illness severity measurement was developed recently. The goal of this study was to explore the prognostic value of qPitt in patients with K. pneumoniae infection.
Patients and Methods: Demographic information and management strategies were retrospectively collected from the records of all adult patients who visited the emergency department between January 1, 2021, and December 31, 2021, with culture-positive K. pneumoniae. The qPitt score was calculated based on: temperature < 36°C, systolic blood pressure ≤ 90 mmHg or vasopressor administration, respiratory rate ≥ 25 times/min or need of mechanical ventilation, altered mental status, and cardiac arrest event. The 30-day mortality prediction abilities of the qPitt were compared with the PBS, the sequential organ failure assessment (SOFA), and the quick sequential organ failure assessment (qSOFA) using receiver operating characteristic curves.
Results: Data from 867 patients (57.8% men) with a mean age of 66.9 were compiled. The 30-day mortality rate of the enrolled patients was 13.4%, and the area under the curve (AUC) of the scoring systems were as follows: SOFA, 0.91 (95% confidence interval [CI]=0.89– 0.93), qPitt, 0.87 (95% CI=0.84– 0.89), PBS, 0.87 (95% CI=0.85– 0.89), and qSOFA, 0.73 (95% CI=0.70– 0.76). The AUC of qPitt was significantly higher than that of qSOFA (p< 0.01) and similar to that of PBS (p=0.65).The qPitt also demonstrated excellent mortality discrimination ability in non-bacteremic patients, AUC= 0.85 (95% CI=0.82– 0.88).
Conclusion: The qPitt revealed excellent 30-day mortality prediction ability and also predicted mortality in non-bacteremic patients with K. pneumoniae infection. Clinicians can use this simplified scoring system to stratify patients earlier and initiate prompt treatment in high-risk patients.
Keywords: Klebsiella pneumoniae, organ dysfunction scores, bacteremia, prognosis
A Letter to the Editor has been published for this article.
A Response to Letter by Mrs Yang has been published for this article.
Introduction
Klebsiella pneumoniae is a gram-negative, encapsulated bacterium that usually colonizes the human gastrointestinal tract mucosal surface, but may cause extraintestinal opportunistic infections in the urinary tract, lung, brain, or bloodstream, especially in immunocompromised status.1,2 K. pneumoniae is an important causative pathogen in approximately 10% of nosocomial infections, resulting in poor prognosis owing to its hypervirulence and antibiotic resistance.3,4 It has been estimated that the mortality rate of patients with K. pneumoniae infection ranged from 5–30% and up to 29–54% in those with bloodstream infection.5–7 The World Health Organization recently included K. pneumoniae in list of critical microorganisms, which pose a significant threat and major burden to global public health.2
The Pitt bacteremia score (PBS) has been a widely used scoring system for disease severity stratification in patients with bacteremia for decades and has recently been validated for its prognostic role in patients with nonbacteremic infections.8–10 Recently, a simplified quicker version of the PBS (qPitt) using binary variables for acute illness severity measurement was developed, including body temperature, blood pressure, respiratory rate, cardiac arrest event, and mental status.11 qPitt was investigated as an outcome prediction tool in patients with Staphylococcus aureus bloodstream infection,12 and bloodstream infection secondary to urinary tract infection in recent studies.13 Both studies revealed that qPitt has excellent mortality discrimination ability in these patients.12,13 As PBS was originally derived from patients with gram-negative bloodstream infection,14 and qPitt has not been validated in patients with single causative gram-negative pathogen, the goal of this study was to explore the prognostic value of qPitt in patients with K. pneumoniae infection. Furthermore, we tested the mortality discrimination ability of qPitt in subgroups of patients with nonbacteremic infections.
Materials and Methods
Study Design and Patient Enrollment
This retrospective observational cohort study was conducted at a tertiary medical center located in Kaohsiung, Taiwan. There are approximately 1100 licensed bed and 53,000 emergency department (ED) visits annually. The institutional review board waived the requirement for informed consent because of the retrospective and observational nature of the study. The study followed the principles of the Declaration of Helsinki and STROBE guidelines.
Inclusion Criteria
We enrolled all adult patients (aged ≥18 years) who visited the ED between January 1, 2021, and December 31, 2021, and underwent blood or other site-specific cultures which yield K. pneumoniae in this study. If a patient had multiple ED visits during the study period, only the first visit was included.
Exclusion Criteria
To avoid selection bias and heterogeneity, we excluded patients with bloodstream infection from site-specific infection at another body site (ie, secondary bloodstream infection).15 We also excluded non-hospitalized patients and those with unrelated diagnoses (the cultured bacteria was not related to the cause of patient’s infection. eg, the urine specimen yield K. pneumoniae but the principal diagnosis was biliary tract infection not yield K. pneumoniae).
Data Collection and Study Definitions
All eligible patients and their relevant data, including demographic, clinical, microbiological information and management strategies, were collected from an anonymized electronic medical record system. The patients were divided into survivor and non-survivor groups according to their 30-day survival status for further comparison and analysis. The systemic inflammatory response syndrome (SIRS), quick sequential organ failure assessment (qSOFA), and sequential organ failure assessment (SOFA) scores were calculated based on their original definition using the initial ED physiological and laboratory parameters.16 A qSOFA score ≥ 2 points was used as the prognostic cutoff value.17 The PBS, ranging from 0 to 14, was obtained based on the following five variables: temperature, altered mental status, blood pressure, need for mechanical ventilation, and cardiac arrest event.8 The qPitt score was calculated based on five scoring items: temperature <36°C, systolic blood pressure ≤90 mmHg or vasopressor administration, respiratory rate ≥25 times/min or need of mechanical ventilation, altered mental status, and cardiac arrest event.11 Each variable was assigned one point, with a maximum score of 5. The sources of K. pneumoniae infection was stratified as primary bacteremia, urinary tract infection, respiratory tract infection, intra-abdominal infection, skin/soft tissue infection, and others (minor infection sites, such as catheter-related infection).15 The administered antibiotic was considered appropriate if it was active in vitro against the cultured K. pneumoniae (eg, blood, urine, sputum, or bronchoalveolar lavage) by susceptibility testing. The implementation of source control (measures to eliminate the source of infection) was determined by the treating physician’s judgement and recorded according to medical records.
Outcome Measurement and Statistical Analysis
The primary outcome of this study was to compare the 30-day mortality prediction ability of qPitt and other commonly used sepsis severity scoring systems, including qSOFA, SOFA, and PBS, in patients with K. pneumoniae infection. The secondary outcome was the mortality discrimination ability of qPitt in nonbacteremic patients. Quantitative variables were expressed as mean ± standard deviation or median (interquartile range) and were compared using a two-sample t-test or Mann–Whitney U-test, depending on whether they were normally distributed. Qualitative variables were expressed as percentages and compared using the Chi-square or Fisher’s exact test. The mortality discriminative ability of qPitt and other scoring systems was tested using the area under the receiver operating characteristic (ROC) curve. The DeLong method was used to compare the area under the curve (AUC) of these variables.18 The significance level for statistical testing was defined as two-tailed p < 0.05. All statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS, IL, USA), version 25.0, and MedCalc Statistical Software version 18.2.1 (MedCalc Software bv, Ostend, Belgium). Figures were drafted using GraphPad Prism version 8.4.3 (GraphPad Software, CA, USA).
Results
Initially, 1569 patients with K. pneumoniae infection met the inclusion criteria. After excluding repetitive patients (N = 88), non-hospitalization (N = 378), secondary bacteremia (N = 90), and unrelated diagnoses (N = 146), the remaining 867 patients were included in the final analysis (Figure 1).
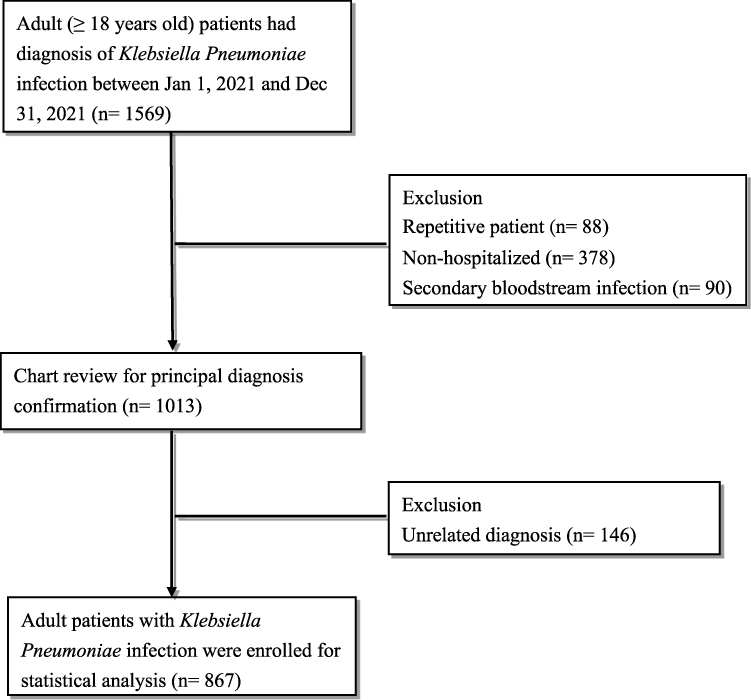 |
Figure 1 Flowchart of patient enrollment. |
As shown in Table 1, the total 30-day mortality rate of the enrolled patients was 13.4% (116/867). The mean age of the patients was 66.9±15.8 years, and more than half (57.8%) were male patients. Compared with survivor group, patients in the non-survivor group had significantly higher proportion of chronic liver disease (12.9% vs 5.6%, p<0.01), chronic kidney disease (50.0% vs 30.6%, p<0.01), and malignancy (37.1% vs 22.6%, p<0.01) comorbidities. The non-survivor group also had significantly lower hemoglobin (10.3 [8.7–12.9] g/dL vs 11.8 [9.9–13.6] g/dL, p<0.01) and platelet (158 [97–244] ×109/L vs 218 [159–289] ×109/L, p<0.01) level, longer international normalized ratio (1.24 [1.13–1.46] vs 1.07 [1.02–1.18], p<0.01), higher lactate (3.6 [2.1–7.6] mmol/L vs 1.7 [1.1–2.7] mmol/L, p<0.01), c-reactive protein (108.5 [40–203.9] mg/dL vs 64.4 [20–150.7] mg/dL, p<0.01), and creatinine levels (1.7 [1.0–2.3] mg/dL vs 0.7 [1.0–1.4] mg/dL, p<0.01) than the survivor group (Table 1).
 |
Table 1 Baseline Characteristics of Patients with Klebsiella pneumoniae Infection |
Regarding the sepsis severity scoring systems, it was not surprising that patients in the non-survivor group had a significantly higher proportion of SIRS criteria (81.9% vs 66.0%, p<0.01), high qSOFA category (39.7% vs 13.3%, p<0.01), and higher SOFA scores (9 [7–11] vs 2 [0–4], p<0.01). Furthermore, the non-survivor group had significantly higher PBS (5 [3–8] vs 0 [0–2], p<0.01) and qPitt (3 [2–3] vs 0 [0–1], p<0.01) scores than the survivor group (Table 2).
 |
Table 2 Sepsis Severity, Source and Management of Patients with Klebsiella pneumoniae Infection |
The most common infection source in the enrolled patients was the urinary tract (32.9%), followed by the bloodstream (26.0%) and skin/soft tissue (17.3%). Approximately three-fourths (71.7%) of the patients in this study received appropriate antibiotic administration (Table 2). The patients in the non-survivor group had a significantly higher proportion of bloodstream infections (33.6% vs 24.8%, p<0.01) and a lower proportion of urinary tract infections (19.0% vs 35.0%, p<0.01) than those in the survivor group. There were comparable proportion of appropriate antibiotic administration between the survivor and non-survivor groups (p=0.85).
The 30-day mortality prediction abilities of the scoring systems were compared. As shown in Figure 2, the AUC of each scoring system was as follows: SOFA, 0.91 (95% confidence interval [CI] = 0.89–0.93), qPitt, 0.87 (95% CI = 0.84–0.89), PBS, 0.87 (95% CI = 0.85–0.89), and qSOFA, 0.73 (95% CI = 0.70–0.76). Moreover, the AUC of qPitt was significantly higher than that of qSOFA (p<0.01) and similar to that of PBS (p=0.65).
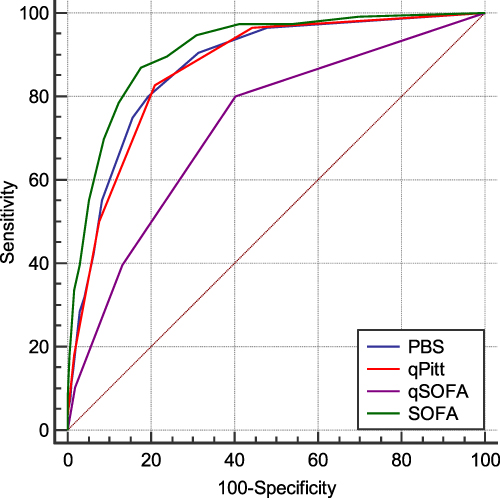 |
Figure 2 The AUC of each scoring system. |
We further examined the mortality discriminative performance of the qPitt score, which ranged from 0 to 5. As shown in Figure 3, the 30-day mortality rates in the qPitt group were 0.9% (4/422), 8.4% (16/191), 27.3% (38/139), 45.1% (37/82), 60.7% (17/28), and 80.0% (4/5), respectively. The mortality risk increased significantly in a stepwise manner as qPitt increased (p<0.01). Finally, we tested the ability of qPitt to predict mortality in nonbacteremic patients. As shown in Figure 4, qPitt also demonstrated excellent mortality discrimination ability in these patients (AUC= 0.85, 95% CI = 0.82–0.88, p<0.001).
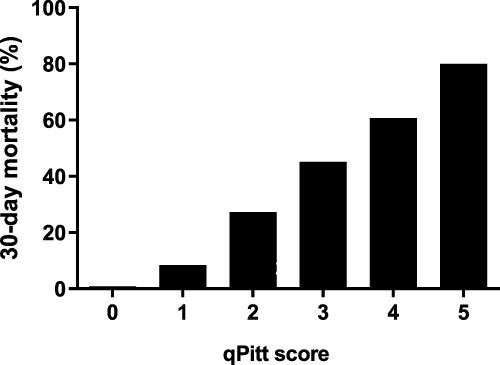 |
Figure 3 30-day mortality rates in the qPitt score groups. |
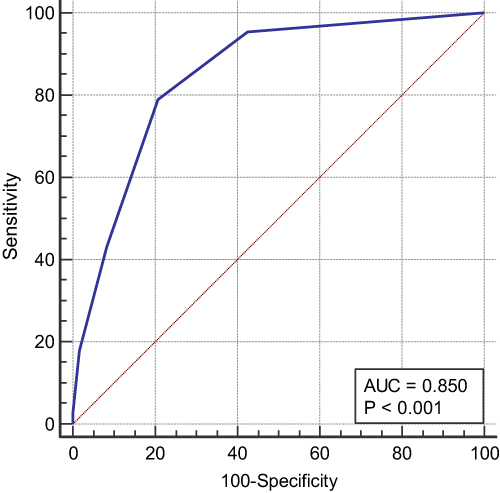 |
Figure 4 The ability of the qPitt to predict mortality in patients without bacteremia. |
Discussion
In this single-center, ED-based, retrospective observational study, we evaluated the predictive performance of qPitt for the 30-day mortality risk of patients with K. pneumoniae infection and compared it with other widely used scoring systems, including SOFA, PBS, and qSOFA. We demonstrated that qPitt had a mortality discriminative ability comparable to that of PBS and was superior to that of the qSOFA score. Furthermore, we revealed that qPitt has an excellent mortality prediction ability in nonbacteremic patients with K. pneumoniae infection. To the best of our knowledge, this is the first study to investigate the prognostic role of qPitt in patients with a single causative gram-negative pathogen, including both bloodstream and non-bloodstream infections.11–13,19
Susceptibility to K. pneumoniae infection is determined by various factors, including pathogen virulence, host defense, and extrinsic stress.1–3 It was studied that individuals with advanced age or other chronic illness, such as diabetes, malignancy, liver disease, chronic obstructive lung disease, renal failure, or malnutrition, are more vulnerable to K. pneumoniae infections and have a poorer prognosis.1,3 In patients with K. pneumoniae bloodstream infection, anemia, thrombocytopenia, coagulation disorders, renal failure, hypoalbuminemia, elevated c-reactive protein levels, and hyperlactatemia have been reported to be associated with mortality risk.20–22 The comorbidities and laboratory results of the non-survivors in our study were consistent with these findings, further strengthening their prognostic significance in patients with K. pneumoniae infections.
The proportion of infection source distribution in our patient groups was also consistent with previous studies.5 Patients have bloodstream infections due to their chronic illness and are prone to undergo surgical procedures, immunosuppressant agents, and invasive devices, all of which contribute to their poor physical condition and higher mortality risk.3,5 In contrast, the urinary tract is a relatively minor infection site, which may slightly influence the patient’s condition, thus providing a better survival chance.5 The escalating prevalence of multidrug-resistant bacteria is another global issue, and was estimated to account for one-third of all K. pneumoniae pathogens in a recent meta-analysis.4 Fortunately, the relatively low mortality rate of bloodstream infections in our study may be attributed to the low prevalence of antibiotics resistance (ie, a high proportion of appropriate antibiotics administration).
The SOFA score was developed to quantitatively describe the degree of organ dysfunction/failure and complications of critical illness in individuals or groups of patients and is one of the most widely used scoring systems in adult intensive care settings, including sepsis.23 Although the SOFA score was originally designed to evaluate the extent of organ dysfunction rather than outcome prediction, it has been well validated as a good prognostic discrimination tool in patients with infectious disease.16,24,25 Therefore, it is reasonable that the SOFA score had the highest prognostic accuracy in our study. Nevertheless, the need for laboratory parameter measurements and a slightly complex calculation process sometimes makes the SOFA score not readily available for risk stratification of these patients.25 Moreover, the iatrogenic confounders, inter-patient variability, and the introduction of new intervention strategies all possibly promote the need for SOFA score update.23,25
PBS has been used for three decades to stratify acute illness severity and predict mortality in various patient populations with bloodstream infections.14,26,27 Similar to PBS, qPitt is a more simplified scoring system consisting of five binary variables that retain hypothermia but exclude fever from PBS.11 Hypothermia is deemed a late phase of acute illness and a more severe stage of endotoxic shock in animal experimental studies; thus, it is more strongly correlated with mortality in patients with infectious diseases.28,29 Another advantage of qPitt variables is the respiratory rate, which is based on the number of breaths/min rather than the oxygen concentration, and the need for mechanical ventilation may allow earlier detection of respiratory failure in these patients.12 The comparable mortality prediction ability of PBS and qPitt in our study strengthens the value of outcome prediction. Larger prospective studies are required to validate these findings.
Both the qPitt and qSOFA scores were developed to identify high-risk patients based solely based on vital signs and other readily available clinical variables during an initial physical examination, and the absence of laboratory parameters allows making clinical decision more quickly.12,14 Although they share some similar parameters, the slightly higher threshold in respiratory rate and systolic blood pressure parameters in qPitt may improve its specificity and positive predictive value without the expense of sensitivity or negative predictive value.11 Notably, qPitt outperformed qSOFA in mortality prediction in patients with Staphylococcus aureus bloodstream infection in a previous study, whereas another study in patients with urinary tract infection revealed converse results.12,19 The significantly superior prognostic value of qPitt in our study encourage future studies to compare both scoring systems in other cohorts, further extending the application potential of qPitt to a wide variety of infections.
Another novel finding of our study is that qPitt predicted mortality in nonbacteremic patients with K. pneumoniae infection, as well as in those with bacteremia. A recent multicenter prospective study investigated the prognostic role of qPitt in patients with nonbacteremic carbapenem-resistant Enterobacteriaceae infections and demonstrated the strong mortality prediction ability of qPitt in these patients.10 These findings may allow the broader use of this simple score for risk stratification in clinical infectious diseases, even prior to the identification of the microbiological profile or site of infection.10,12
The main strength of this study was the inclusion of all patients with K. pneumoniae infection, regardless of the infection site, which is more practical for clinical applications. The exclusion of patients with secondary bloodstream infections also avoided misclassification of these patients. Nevertheless, this study also shares the common limitations of a retrospective observational cohort design, which is mostly subject to inherent recall bias. Although we thoroughly reviewed the electronic medical records to obtain detailed information on our enrolled patients, some unknown and unmeasured confounders may still bias the results. Other important elements of sepsis management, including the amount of fluid or vasopressors administered to patients, were not calculated or controlled in this study. The single-center nature of this study warrants future multicenter prospective studies to validate our findings.
Conclusion
In conclusion, in patients with K. pneumoniae infection, qPitt revealed excellent 30-day mortality prediction ability, similar to PBS, and outperformed the qSOFA score. The qPitt also exhibited mortality discrimination ability in nonbacteremic patients with K. pneumoniae infections. Clinicians can use this simplified scoring system to stratify patients earlier and initiate prompt treatment in high-risk patients.
Abbreviations
AUC, area under the curve; ED, emergency department; PBS, Pitt bacteremia score; qPitt, quick version of the PBS; qSOFA, quick sequential organ failure assessment; SIRS, systemic inflammatory response syndrome; SOFA, sequential organ failure assessment.
Ethic Approval and Informed Consent
This study was approved by the ethics committee of the E-Da hospital (EMRP-111-081). All data were anonymized and obtained from electronic medical record systems to maintain participant’s privacy. The ethics committee did not require written informed consent due to the retrospective nature of the study.
Acknowledgments
This study was supported by funding from the E-Da Hospital, Kaohsiung, Taiwan, (Grant no. EADHP109026).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Paczosa MK, Mecsas J. Klebsiella pneumoniae: going on the offense with a strong defense. Microbiol Mol Biol Rev. 2016;80(3):629–661. doi:10.1128/MMBR.00078-15
2. Bengoechea JA, Sa Pessoa J. Klebsiella pneumoniae infection biology: living to counteract host defences. FEMS Microbiol Rev. 2019;43(2):123–144. doi:10.1093/femsre/fuy043
3. Chang D, Sharma L, Dela Cruz CS, Zhang D. Clinical epidemiology, risk factors, and control strategies of Klebsiella pneumoniae infection. Front Microbiol. 2021;12:750662. doi:10.3389/fmicb.2021.750662
4. Mohd Asri NA, Ahmad S, Mohamud R, et al. Global prevalence of nosocomial multidrug-resistant Klebsiella pneumoniae: a systematic review and meta-analysis. Antibiotics. 2021;10(12):1508. doi:10.3390/antibiotics10121508
5. Xu L, Sun X, Ma X. Systematic review and meta-analysis of mortality of patients infected with carbapenem-resistant Klebsiella pneumoniae. Ann Clin Microbiol Antimicrob. 2017;16:1–12. doi:10.1186/s12941-017-0191-3
6. Hu Y, Anes J, Devineau S, Fanning S. Klebsiella pneumoniae: prevalence, reservoirs, antimicrobial resistance, pathogenicity, and infection: a hitherto unrecognized zoonotic bacterium. Foodborne Pathog Dis. 2021;18(2):63–84. doi:10.1089/fpd.2020.2847
7. Zhang J, Dan L, Xiangning H, et al. Klebsiella pneumoniae bacteremia mortality: a systematic review and meta-analysis. Front Cell Infect Microbiol. 2023;13:469. doi:10.3389/fcimb.2023.1157010
8. Paterson DL, Ko W-C, Von Gottberg A, et al. Antibiotic therapy for Klebsiella pneumoniae bacteremia: implications of production of extended-spectrum β-lactamases. Clin Infect Dis. 2004;39(1):31–37. doi:10.1086/420816
9. Rhee J-Y, Kwon KT, Ki HK, et al. Scoring systems for prediction of mortality in patients with intensive care unit-acquired sepsis: a comparison of the Pitt bacteremia score and the Acute Physiology and Chronic Health Evaluation II scoring systems. Shock. 2009;31(2):146–150. doi:10.1097/SHK.0b013e318182f98f
10. Henderson H, Luterbach CL, Cober E, et al. The Pitt bacteremia score predicts mortality in nonbacteremic infections. Clin Infect Dis. 2020;70(9):1826–1833. doi:10.1093/cid/ciz528
11. Battle SE, Augustine MR, Watson CM, et al. Derivation of a quick Pitt bacteremia score to predict mortality in patients with gram-negative bloodstream infection. Infection. 2019;47(4):571–578. doi:10.1007/s15010-019-01277-7
12. Battle SE, Shuping M, Withers S, Justo JA, Bookstaver PB, Al-Hasan MN. Prediction of mortality in Staphylococcus aureus bloodstream infection using quick Pitt bacteremia score. J Infect. 2022;84(2):131–135. doi:10.1016/j.jinf.2021.12.002
13. Li C, Wang J, Wang Q, et al. Predictive value of a quick Pitt bacteremia score for prognosis of patients with bloodstream infection secondary to urinary tract infection: a retrospective cohort study. Infect Drug Resist. 2022;Volume 15:4381–4391. doi:10.2147/IDR.S373998
14. Al-Hasan MN, Baddour LM. Resilience of the Pitt bacteremia score: 3 decades and counting. Clin Infect Dis. 2020;70(9):1834–1836. doi:10.1093/cid/ciz535
15. Sante L, Aguirre-Jaime A, Miguel MA, Ramos MJ, Pedroso Y, Lecuona M. Epidemiological study of secondary bloodstream infections: the forgotten issue. J Infect Public Health. 2019;12(1):37–42. doi:10.1016/j.jiph.2018.08.011
16. Raith EP, Udy AA, Bailey M, et al. Prognostic accuracy of the SOFA score, SIRS criteria, and qSOFA score for in-hospital mortality among adults with suspected infection admitted to the intensive care unit. JAMA. 2017;317(3):290–300. doi:10.1001/jama.2016.20328
17. Marik PE, Taeb AM. SIRS, qSOFA and new sepsis definition. J Thorac Dis. 2017;9(4):943. doi:10.21037/jtd.2017.03.125
18. DeLong ER, DeLong DM, Clarke-Pearson DL. Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics. 1988;44:837–845. doi:10.2307/2531595
19. Madrazo M, Piles L, López-Cruz I, et al. Comparison of quick Pitt to quick sofa and sofa scores for scoring of severity for patients with urinary tract infection. Intern Emerg Med. 2022;17(5):1321–1326. doi:10.1007/s11739-022-02927-9
20. Ramirez-Alfaro C, Villalobos-Vindas J. Analysis of Klebsiella pneumoniae bacteremia in patients from Mexico hospital. Acta Médica Costarricense. 2016;58(2):62–68.
21. Li L, Huang H. Risk factors of mortality in bloodstream infections caused by Klebsiella pneumonia: a single-center retrospective study in China. Medicine. 2017;96(35):145. doi:10.1097/MD.0000000000007924
22. Li S, Liu J, Chen F, et al. A risk score based on pediatric sequential organ failure assessment predicts 90-day mortality in children with Klebsiella pneumoniae bloodstream infection. BMC Infect Dis. 2020;20(1):1–12. doi:10.1186/s12879-020-05644-w
23. Lambden S, Laterre PF, Levy MM, Francois B. The SOFA score—development, utility and challenges of accurate assessment in clinical trials. Crit Care. 2019;23(1):1–9. doi:10.1186/s13054-019-2663-7
24. Liu Z, Meng Z, Li Y, et al. Prognostic accuracy of the serum lactate level, the SOFA score and the qSOFA score for mortality among adults with Sepsis. Scand J Trauma Resusc Emerg Med. 2019;27:1–10. doi:10.1186/s13049-019-0609-3
25. Moreno R, Rhodes A, Piquilloud L, et al. The Sequential Organ Failure Assessment (SOFA) score: has the time come for an update? Crit Care. 2023;27(1):1–5. doi:10.1186/s13054-022-04291-8
26. Vaquero‐Herrero MP, Ragozzino S, Castaño‐Romero F, et al. The Pitt Bacteremia Score, Charlson Comorbidity Index and Chronic Disease Score are useful tools for the prediction of mortality in patients with Candida bloodstream infection. Mycoses. 2017;60(10):676–685. doi:10.1111/myc.12644
27. Lee -C-C, Wang J-L, Lee C-H, et al. Age-related trends in adults with community-onset bacteremia. Antimicrob Agents Chemother. 2017;61(12):e01050–01017. doi:10.1128/AAC.01050-17
28. Rumbus Z, Matics R, Hegyi P, et al. Fever is associated with reduced, hypothermia with increased mortality in septic patients: a meta-analysis of clinical trials. PLoS One. 2017;12(1):e0170152. doi:10.1371/journal.pone.0170152
29. Shimazui T, Nakada T-A, Walley KR, et al. Significance of body temperature in elderly patients with sepsis. Crit Care. 2020;24:1–9. doi:10.1186/s13054-020-02976-6
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Extended-Spectrum β-Lactamase-Producing Escherichia coli and Klebsiella pneumoniae: Risk Factors and Economic Burden Among Patients with Bloodstream Infections
Chen J, Allel K, Zhuo C, Luo W, He N, Yang X, Guo Y, Wang J, Yao L, Li J, Lin Y, Tu R, Yakob L, Zhuo C
Risk Management and Healthcare Policy 2024, 17:375-385
Published Date: 28 February 2024
Prognostic Factors and Nomogram for Klebsiella pneumoniae Infections in Intensive Care Unit
Du C, Zhang H, Zhang Y, Zhang H, Zheng J, Liu C, Lu F, Shen N
Infection and Drug Resistance 2025, 18:1237-1251
Published Date: 1 March 2025
Necrotizing Myositis Caused by Enterococcus faecium with Concurrent Klebsiella pneumoniae Bacteremia: A Rare Case Report
Niu X, Ji H, Wang S, Wang G, Wang Y, Liu Y, Kong L
Infection and Drug Resistance 2026, 19:591080
Published Date: 27 April 2026
Comparative Analysis of Clinical Characteristics and Antimicrobial Resistance of IA-BSI Caused by Escherichia coli and Klebsiella pneumoniae
Huang X, Huang L, Xiao M, Zhou X
International Journal of General Medicine 2026, 19:593975
Published Date: 24 June 2026