Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 16
Predicting Re-Exacerbation Timing and Understanding Prolonged Exacerbations: An Analysis of Patients with COPD in the ECLIPSE Cohort
Authors Meeraus WH ![]() , Mullerova H
, Mullerova H ![]() , El Baou C
, El Baou C ![]() , Fahey M, Hessel EM
, Fahey M, Hessel EM ![]() , Fahy WA
, Fahy WA
Received 28 August 2020
Accepted for publication 30 December 2020
Published 5 February 2021 Volume 2021:16 Pages 225—244
DOI https://doi.org/10.2147/COPD.S279315
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Richard Russell
Wilhelmine H Meeraus,1 Hana Mullerova,1 Céline El Baou,2 Marion Fahey,1 Edith M Hessel,2 William A Fahy2
1GlaxoSmithKline plc., Epidemiology – Value, Evidence and Outcomes, Middlesex, UK; 2GlaxoSmithKline plc., Research and Development, Middlesex, UK
Correspondence: Wilhelmine H Meeraus
GlaxoSmithKline plc. House, 980 Great West Road, Brentford, Middlesex, TW8 9GS, UK
Tel +44 208 047 6757
Email [email protected]
Purpose: Understanding risk factors for an acute exacerbation of chronic obstructive pulmonary disease (AECOPD) is important for optimizing patient care. We re-analyzed data from the Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE) study (NCT00292552) to identify factors predictive of re-exacerbations and associated with prolonged AECOPDs.
Methods: Patients with COPD from ECLIPSE with moderate/severe AECOPDs were included. The end of the first exacerbation was the index date. Timing of re-exacerbation risk was assessed in patients with 180 days’ post-index-date follow-up data. Factors predictive of early (1– 90 days) vs late (91– 180 days) vs no re-exacerbation were identified using a multivariable partial-proportional-odds-predictive model. Explanatory logistic-regression modeling identified factors associated with prolonged AECOPDs.
Results: Of the 1,554 eligible patients from ECLIPSE, 1,420 had 180 days’ follow-up data: more patients experienced early (30.9%) than late (18.7%) re-exacerbations; 50.4% had no re-exacerbation within 180 days. Lower post-bronchodilator FEV1 (P=0.0019), a higher number of moderate/severe exacerbations on/before index date (P< 0.0001), higher St. George’s Respiratory Questionnaire total score (P=0.0036), and season of index exacerbation (autumn vs winter, P=0.00164) were identified as predictors of early (vs late/none) re-exacerbation risk within 180 days. Similarly, these were all predictors of any (vs none) re-exacerbation risk within 180 days. Median moderate/severe AECOPD duration was 12 days; 22.7% of patients experienced a prolonged AECOPD. The odds of experiencing a prolonged AECOPD were greater for severe vs moderate AECOPDs (adjusted odds ratio=1.917, P=0.002) and lower for spring vs winter AECOPDs (adjusted odds ratio=0.578, P=0.017).
Conclusion: Prior exacerbation history, reduced lung function, poorer respiratory-related quality-of-life (greater disease burden), and season may help identify patients who will re-exacerbate within 90 days of an AECOPD. Severe AECOPDs and winter AECOPDs are likely to be prolonged and may require close monitoring.
Keywords: observational study, acute exacerbations of COPD, risk factors, regression modeling
Plain Language Summary
Much of the mortality and morbidity associated with chronic obstructive pulmonary disease (COPD) can be attributed to deteriorations in the condition, otherwise known as acute exacerbations of COPD (AECOPD). The risk factors underlying AECOPD have been well described in the literature, as has the impact they can have on patient care. However, the predictive ability of these risk factors in anticipating future re-exacerbations, plus the relationships between these factors and prolonged AECOPD episodes, have not been so well defined – both of which could be of use in guiding healthcare management decisions.
Our study addressed this “knowledge gap” by looking at data from Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE), an international, multicenter, prospective cohort study of patients with COPD conducted from 2005–2010. We developed a predictive model that was capable of identifying potentially predictive factors for early, late, or no re-exacerbations within a 180-day period. We also assessed the data to identify which factors were linked to prolonged episodes of AECOPD.
We found that exacerbation history, impaired lung function, poorer respiratory-related quality-of-life (greater disease burden), and season were all factors with the potential to identify patients most likely to re-exacerbate within 90 days of experiencing an AECOPD. We also found that severe AECOPDs, and AECOPDs occurring in the winter (compared with those in warmer months), are more likely to be prolonged; this suggests that closer monitoring of patients experiencing severe AECOPDs during these months may be required, with subsequent implications for helping physicians optimize patient care.
Introduction
Chronic obstructive pulmonary disease (COPD) is a progressive disease characterized by persistent airflow limitation and respiratory symptoms, which are a result of abnormalities in the airways or alveoli.1 COPD is a leading cause of mortality and morbidity worldwide.2 Much of the mortality and morbidity associated with COPD is driven by acute exacerbations of COPD (AECOPD), which are typically defined as an acute worsening of respiratory symptoms that require additional treatment.3 Systemic and oral corticosteroids are established as the standard-of-care treatment for AECOPD, but their effectiveness may differ between patients, thereby affecting overall recovery time.
Exacerbation symptoms typically last 7–10 days, but some events can last longer, and, at 8 weeks, as many as 20% of patients may not have returned to their pre-exacerbation state.4 Approximately one in two patients with COPD, including those receiving long-term maintenance treatment with an inhaled corticosteroid, experience at least one AECOPD each year, and it is estimated that a single AECOPD event can increase the risk of mortality by 71%.5
Repeated hospitalizations for AECOPD events places a large financial burden on healthcare resources, with some estimates suggesting that hospitalizations for AECOPD account for nearly 70% of COPD-related healthcare expenditure.6,7 Numerous risk factors for moderate and severe AECOPD events have been described in the literature. Prior history of AECOPD events is the most significant risk factor:8 for example, in a large-scale study of patients hospitalized for an AECOPD, the risk of a subsequent exacerbation tripled with a second AECOPD event, and could be up to 24-times higher after a tenth AECOPD event.9 Other established risk factors for an AECOPD include male sex; number of COPD maintenance medications; forced expiratory volume in 1 second (FEV1)/forced vital capacity; and degree of rescue medication use.10–17 It is also unclear how re-exacerbation risk varies over time, although some evidence suggests that this risk is dynamic and subject to fluctuation.18 The risk trajectory of a patient being re-hospitalized following a severe AECOPD has been described,18 and some observational studies have estimated the risk of moderate/severe/moderate-to-severe re-exacerbation within discrete time periods (for example, 90 days after the initial exacerbation).19–23 However, differing study designs and definitions of AECOPD events, as demonstrated in systematic literature reviews,24,25 may mean that comparison of such results is not wholly reliable. Exacerbation history has been identified as a potential predictor of re-exacerbation,26 and a range of comorbidities (including heart disease,21,23 depression, and diabetes)22 may also be involved. Patients may also be at risk of re-exacerbation if they are not prescribed an appropriate treatment following their first AECOPD.27 Understanding the factors behind re-exacerbation, in particular knowledge of those factors which relate to timing of re-exacerbation (ie, early vs late re-exacerbation), is important in optimizing patient care.
Factors that have a causal association with AECOPD duration (including comorbidities;28 laboratory or clinical parameters;29,30 social factors; and prior medication use)28 have been investigated in some small-scale studies of hospitalized patients with COPD. However, such factors overall remain poorly understood and, thus, a more in-depth knowledge of their association with long or prolonged AECOPD duration is needed to help physicians optimize patient care.
Our manuscript reports the results of a re-analysis of data from patients with COPD in the Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE) study.31 The objectives of our analysis were 2-fold. First, we aimed to develop and validate a predictive model capable of identifying factors potentially predictive of experiencing early, late, or no re-exacerbation within 180 days. Second, we aimed to identify patient- and exacerbation-related factors that are potentially associated with prolonged moderate/severe AECOPD duration, ultimately helping to explain why some patients experience longer exacerbations than others. The overall aim of our analysis was to provide data that will have implications for physicians in optimizing care of patients with COPD, based on individual patient needs.
Methods
Study Design, Data Source, and Study Population
We re-analyzed data collected from the ECLIPSE study (NCT00292552).31 ECLIPSE was a large-scale, international, multicenter, prospective cohort study of patients with COPD and both smoking and non-smoking controls. Recruitment into ECLIPSE began in December 2005, with the last patient completing the study in February 2010. Following a baseline visit, patients had a total of seven follow-up visits: one at 3 months, one at 6 months, and then every 6 months thereafter for 3 years. ECLIPSE included 2,164 patients with moderate/severe COPD (Global Initiative for Chronic Obstructive Lung Disease [GOLD]32 airflow limitation stages II, III, and IV) recruited from outpatient clinics at 46 participating study centers in 12 countries.33 ECLIPSE captured a broad range of variables at numerous time points during the 3-year study, which included, amongst others, general demographic variables such as socioeconomic status; self-reported smoking history; vital signs; clinical comorbidities; patient health status and disease burden measured via spirometry, radiography, and patient-reported outcome measures (PROMs) (eg, modified Medical Research Council [mMRC] dyspnea score; Body mass index, airflow Obstruction, Dyspnea and Exercise capacity index; and the Center for Epidemiologic Studies Depression score); respiratory medication use at baseline; and blood and sputum biomarkers (eg, eosinophils, high-sensitivity C-reactive protein).
Eligibility criteria and patient baseline characteristics for the ECLIPSE study have been reported previously.33 The following additional criteria were applied to select patients for inclusion in our analysis: GOLD stage II, III, or IV degree of airflow limitation at baseline visit (note that some patients recruited into ECLIPSE who had GOLD stage I degree of airflow limitation were excluded from our analysis); non-missing information on key variables, including sex, severity of index exacerbation, and GOLD 2017 classification (defined using mMRC dyspnea score and AECOPD history at index date); and ≥1 moderate/severe AECOPD during the ECLIPSE study. AECOPD events were classed as “moderate” if they required treatment with an oral corticosteroid and/or antibiotics, and “severe” if they required hospitalization.
The index date for our analyses was the end date of the first moderate or severe AECOPD event that occurred during study follow-up in ECLIPSE. The end date, rather than the start date of the first AECOPD event, was chosen as the index date to avoid potential immortal time bias (ie, the period in which patients cannot experience a re-exacerbation event due to the fact that they are still exacerbating). Exacerbation duration was assessed in cohort A: this included all patients who had an AECOPD index date, without a requirement for follow-up data. Any patients for whom an index date could not be defined (ie, those without an end date for their first AECOPD event in ECLIPSE) were excluded from cohort A. Re-exacerbation risk was assessed in cohort B, a subset of cohort A that included only patients who had experienced an AECOPD and who had 180 days of follow-up data. Any patients with <180 days’ follow-up data after their index date were excluded from cohort B.
The ECLIPSE study was conducted in accordance with the Declaration of Helsinki and Good Clinical Practice guidelines and was approved by the relevant ethics and review boards at the participating study centers. All participants provided written informed consent. A list of study sites is provided in Supplementary Table 1.
Outcome Variables
ECLIPSE investigators collected detailed information on COPD exacerbations. This included start date, end (resolution) date, treatment (oral corticosteroid/antibiotics), severity (including hospitalization), and outcome (including death). Data was collected at scheduled visits (baseline and 3, 6, 12, 18, 24, 30, and 36 months), using an electronic case-report form and based on either patients’ recall of exacerbation events or available medical records for exacerbation events, and was supplemented by monthly phone calls to ECLIPSE participants.
A re-exacerbation was any new exacerbation event that occurred after the index date, regardless of the number of days between the recorded end date of one exacerbation and the recorded start dates of any subsequent exacerbation. Re-exacerbations were defined a priori as either early (occurring within 1–90 days after the index date) or late (occurring between 91–180 days after the index date). The cut-off point for early and late re-exacerbations was chosen based on clinical judgment, and was informed by an analysis of daily re-hospitalization risk in the US.18 The 90-day cut-off point was also chosen based on clinical development support for an AECOPD therapy. Patients were classed as having no re-exacerbations if they did not re-exacerbate within the 180-day period after the index date.
Exacerbation duration (in days) was calculated as the end date minus the start date for each exacerbation, plus one. Start and end dates were obtained directly from the electronic case-report form source database. For moderate AECOPD events, AECOPD duration represented patient recall of dates and length of time on prescribed therapy (from patient reports or medical records), whereas the duration of severe AECOPD events additionally included information on the duration of hospitalization. For those patients who died during their exacerbation, duration was estimated as the date of death minus the start date of the exacerbation, plus one. Prolonged exacerbations were defined as those exceeding the 75th percentile for exacerbations of the same severity (moderate/severe combined, moderate, and severe), which was consistent with definitions in previous studies of COPD exacerbation duration.28,30
Covariates
All covariates were collected during patient visits. When covariates were measured at multiple time points during ECLIPSE, the covariate recorded nearest to the index date was selected (this may or may not have been at baseline). These included demographic variables; comorbidities; indicators of patient health status and disease burden (PROMs and spirometry); respiratory medications; blood and sputum biomarkers; and exacerbation-related variables (treatment, severity, timing, and seasonality). A full list of covariates is provided in Table 1.
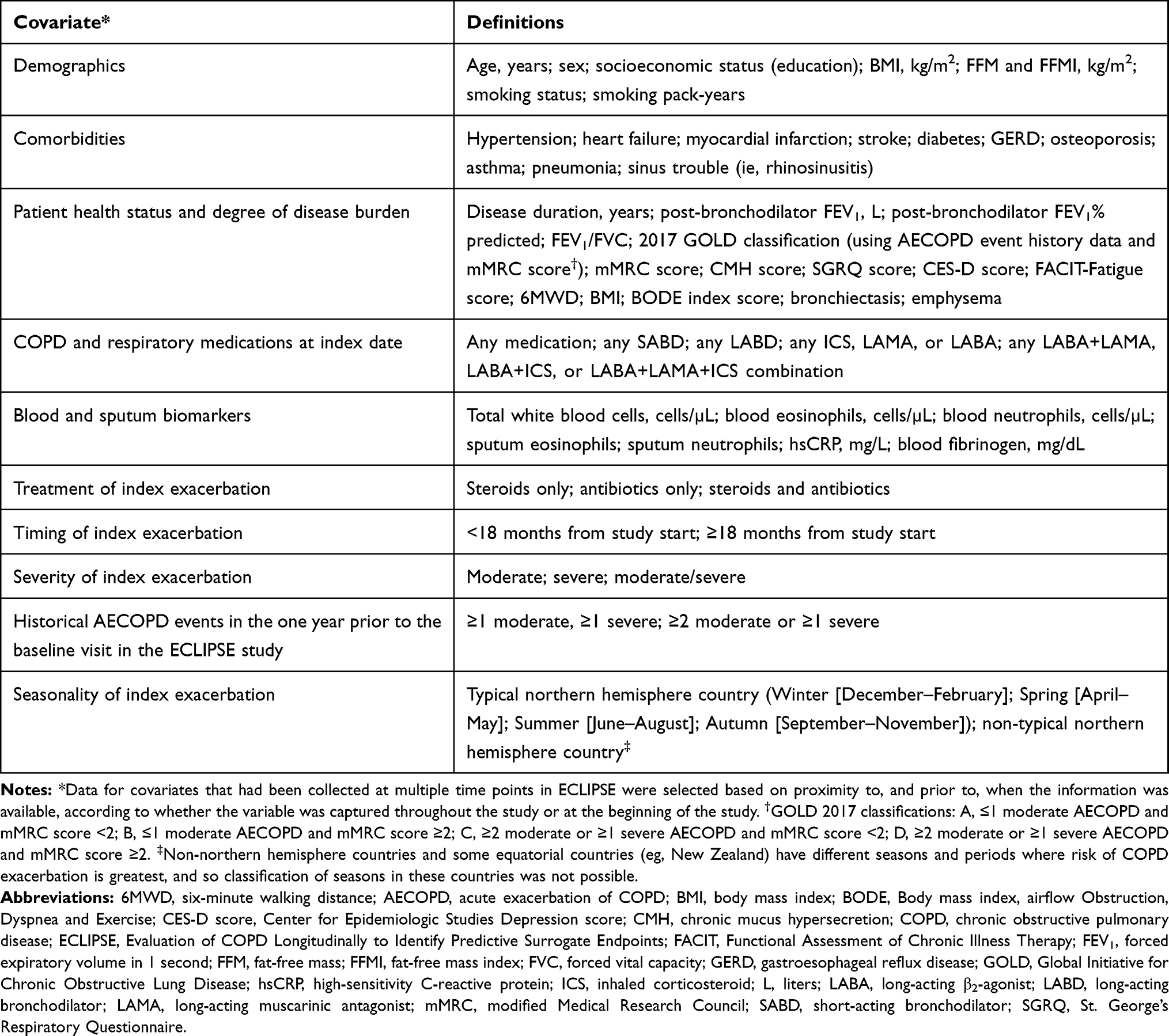 |
Table 1 List of Covariates That Were Defined to Characterize Patients with COPD Who Experienced Re-Exacerbation Events in ECLIPSE (Cohort A), and to Characterize Patients with Prolonged Exacerbation Duration (Cohort B) |
Data Analysis
Timing of Re-Exacerbation Risk
To understand the timing and dynamics of re-exacerbation risk, and to evaluate the choice of cut points for early and late re-exacerbations, Kaplan–Meier cumulative incidence curves of time to first re-exacerbation amongst all patients in cohort A were plotted. Kaplan–Meier curves were stratified by severity of index exacerbation. To further inform dynamics of re-exacerbation risk, monthly conditional risk of first re-exacerbation, stratified by severity of index exacerbation, was estimated in cohort B.
Characteristics of patients with early, late, or no re-exacerbations within 180 days were outlined using descriptive statistics (including, for example, mean, standard deviation, and n [%]). Factors potentially predictive of early, late, or no re-exacerbation within 180 days were identified using a multivariate partial proportional-odds-predictive model.34 This differs from a proportional odds (multinomial/polytomous logistic regression) model in that odds ratios (ORs) are estimated for each comparison, and it does not assume that the OR for each comparison is the same. Re-exacerbation outcome categories were numbered as 1) early re-exacerbation; 2) late re-exacerbation; and 3) no re-exacerbation, thus allowing comparisons to be made between late or no re-exacerbation vs early re-exacerbation, and no re-exacerbation vs early or late re-exacerbation (ie, none vs “any” re-exacerbation). A single set of models was created which considered all moderate and severe index exacerbations together.
Candidate predictor variables were selected for inclusion in the multivariate model according to their clinical and biological plausibility, as assessed by a clinician. Additional variables were considered for inclusion in the final multivariate model when P-values were <0.1 in univariate analysis, and where level of missing data was considered minimal. The univariate models informed which variables should be used in the multivariate model, which considered all moderate/severe index exacerbations together. A full list of factors considered for inclusion in the analysis are listed in Table 1.
The final multivariate model was built using 10-fold cross-validation, and adjusted ORs and 95% confidence intervals (CIs) were determined for all covariates that were included. Stepwise regression was used to select the list of predictors to retain. Proportional odds determination was built into the stepwise regression,35 and different ORs were calculated for variables where the proportional odds assumption was not met. We tested for interactions with key covariates. To achieve as parsimonious a model as possible, we also considered the use of transformed and hybrid variables; however, none were deemed necessary. Performance of our predictive model was assessed using an agreement chart, and was supplemented by conducting a hypothesis test and calculating the kappa co-efficient. Agreement charts present an alternative to receiver-operating characteristic curves and provide a visual representation for comparing the concordance in paired categorical data.
Prolonged AECOPD Events
Median and interquartile range (IQR) exacerbation duration was calculated for moderate and severe exacerbations for all patients in cohort A. Using the 75th percentile as a cut-off point, we reported the proportion of patients who experienced a prolonged AECOPD event (overall and stratified by exacerbation severity). Descriptive statistics were used to describe characteristics of patients identified as having prolonged (based on >75th percentile) and non-prolonged exacerbation durations. Explanatory logistic regression modeling was used to identify patient- and exacerbation-related factors potentially associated with prolonged exacerbation duration, using a composite binary outcome of moderate/severe exacerbations in our analysis (vs continuous outcome variable).
Variables were selected for inclusion in the analysis according to their clinical and biological plausibility, as assessed by a clinician. The final model included all selected variables (a priori) plus any additional variables with a P-value <0.1 in univariate analyses. A full list of factors considered for inclusion in the analysis is available in Table 1.
A complete case analysis, which assumed data were missing at random, was used for the univariate and final multivariate model. For all variables included in univariate models, unadjusted ORs (95% CIs and P-values) were obtained, and adjusted ORs (95% CIs and P-values) were obtained for all variables included in multivariate models. To assess the impact of missing data on the final multivariate model, univariate ORs were calculated in both the full-case population (the population with full data on the variable in question) and the complete-case population (patients with complete data on all variables), as determined by the final model.
Results
Study Population
Of the 2,164 patients with COPD in ECLIPSE, 2,163 were available for re-analysis: 1,554 met the eligibility criteria for inclusion in the final analytical cohort for assessing exacerbation duration (cohort A); and a total of 1,420 patients with 180 days’ follow-up data after their index exacerbation were included in the final analytical cohort for assessing re-exacerbation risk (cohort B) (Figure 1). The proportions of patients who had moderate and severe index exacerbations were similar in cohort A and in cohort B. In cohort A, 1,273 (81.9%) patients had a moderate index exacerbation and 281 (18.1%) patients had a severe index exacerbation. In cohort B, 1,180 (83.1%) patients had a moderate index exacerbation and 240 (16.9%) patients had a severe index exacerbation.
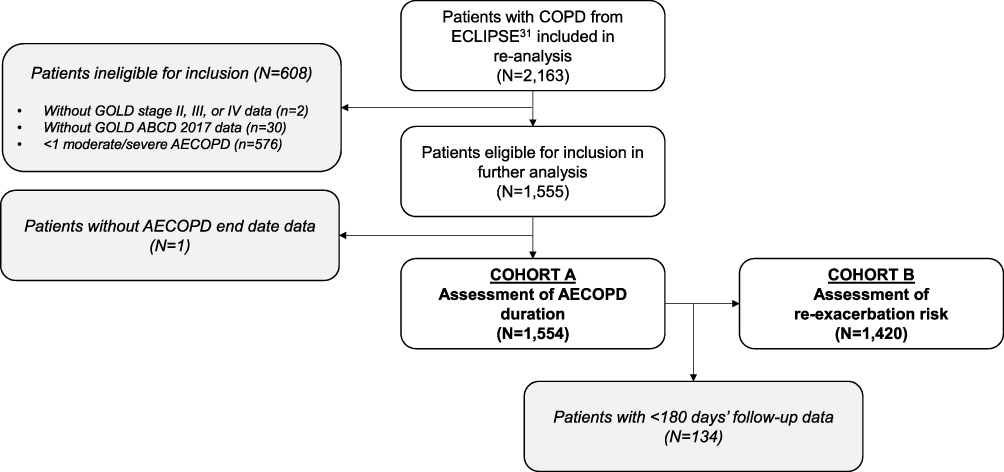 |
Figure 1 CONSORT diagram of patient disposition. Abbreviations: AECOPD, acute exacerbation of COPD; CONSORT, Consolidated Standards of Reporting Trials; COPD, chronic obstructive pulmonary disease; ECLIPSE, Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints; GOLD, Global Initiative for Chronic Obstructive Lung Disease. |
Dynamics of Re-Exacerbation Risk
In cohort A, time to first moderate/severe re-exacerbation after the index exacerbation was similar between patients who experienced a moderate index exacerbation and those who experienced a severe index exacerbation. There was an approximate 70% probability of re-exacerbation in the year following the index exacerbation (Figure 2).
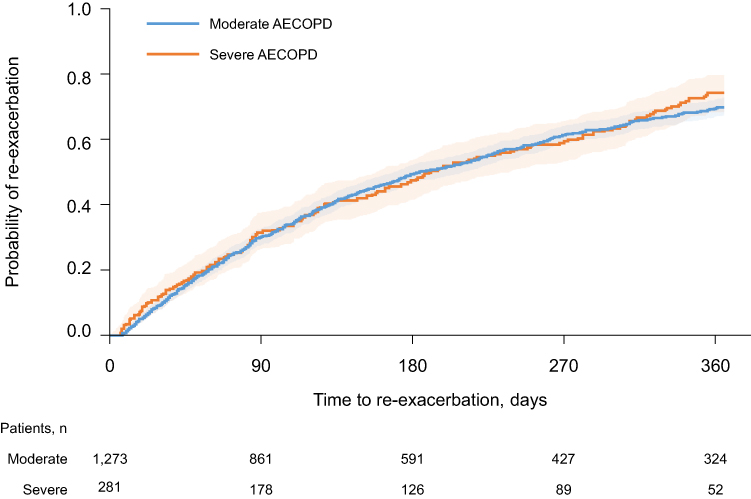 |
Figure 2 Kaplan–Meier cumulative incidence curves for time to first moderate/severe re-exacerbation within 365 days, stratified by severity of index exacerbation (cohort A). N=1,554 (moderate AECOPD n=1,273; severe AECOPD n=281). Abbreviations: AECOPD, acute exacerbation of COPD; COPD, chronic obstructive pulmonary disease. |
In cohort B, 704 (49.6%) patients experienced one or more re-exacerbation events within 180 days. The conditional, monthly risk of first moderate/severe re-exacerbation for these 704 patients was highest in months 1–3 (days 1–90), and subsequently declined from month 4 onwards (days 91–180) (Figure 3). The risk of re-exacerbation in each month (months 1–6) was similar in patients with moderate and severe index exacerbations. For moderate exacerbations, based on 95% CI values, a clear difference in re-exacerbation risk between months 1–3 vs month 6 was observable (approximately 20% vs 10%, respectively).
 |
Figure 3 Conditional, monthly risk of first moderate/severe re-exacerbation within 180 days amongst patients experiencing ≥1 re-exacerbations, stratified by severity of index exacerbation (cohort B). N=704 (moderate re-exacerbation n=590; severe re-exacerbation n=114). Conditional analysis of patients who experienced a moderate or severe re-exacerbation within 180 days. The index date is the end of the index exacerbation. Abbreviations: AECOPD, acute exacerbation of COPD; COPD, chronic obstructive pulmonary disease. |
Factors Predictive of Early, Late, or No Re-Exacerbation Within 180 Days of Index Date
In cohort B, 439 (30.9%) patients experienced an early re-exacerbation and 265 (18.7%) experienced a late re-exacerbation. The remaining 716 (50.4%) patients did not re-exacerbate within 180 days, and so were categorized as having no re-exacerbation (Figure 4). The Kaplan–Meier analysis suggested that overall re-exacerbation risk was independent of index exacerbation severity; it would also appear that timing of re-exacerbation risk is independent of index exacerbation severity, as evidenced by the proportions of patients with early and late re-exacerbations following moderate and severe index exacerbations. Characteristics of patients who experienced early, late, and no re-exacerbations within 180 days are detailed in Table 2 and Supplementary Table 2. The following variables were considered to be potentially predictive based on clinical knowledge and biological plausibility, and were retained by stepwise selection in the final model for predicting the timing of re-exacerbation: post-bronchodilator FEV1, in liters (L); number of moderate or severe exacerbations on or prior to index date; St. George’s Respiratory Questionnaire (SGRQ) total score; and season of index exacerbation (autumn, spring, or summer vs winter). The final partial-proportional-odds-predictive model included data from a total of 1,351 patients (Figure 5). Post-bronchodilator FEV1, L (OR=0.681 per L increase [95% CI=0.535–0.868]; P=0.0019); number of moderate or severe exacerbations on or prior to index date (OR=1.874 [95% CI=1.662–2.112]; P<0.0001); and SGRQ total score (OR=1.050 per 5-unit increase in total score [95% CI=1.016–1.085]; P=0.0035) were identified as predictors of whether a patient would experience an early exacerbation, compared to either a late or no exacerbation. These factors were also predictive of whether a patient would experience any re-exacerbation (early or late) vs no re-exacerbation.
 | 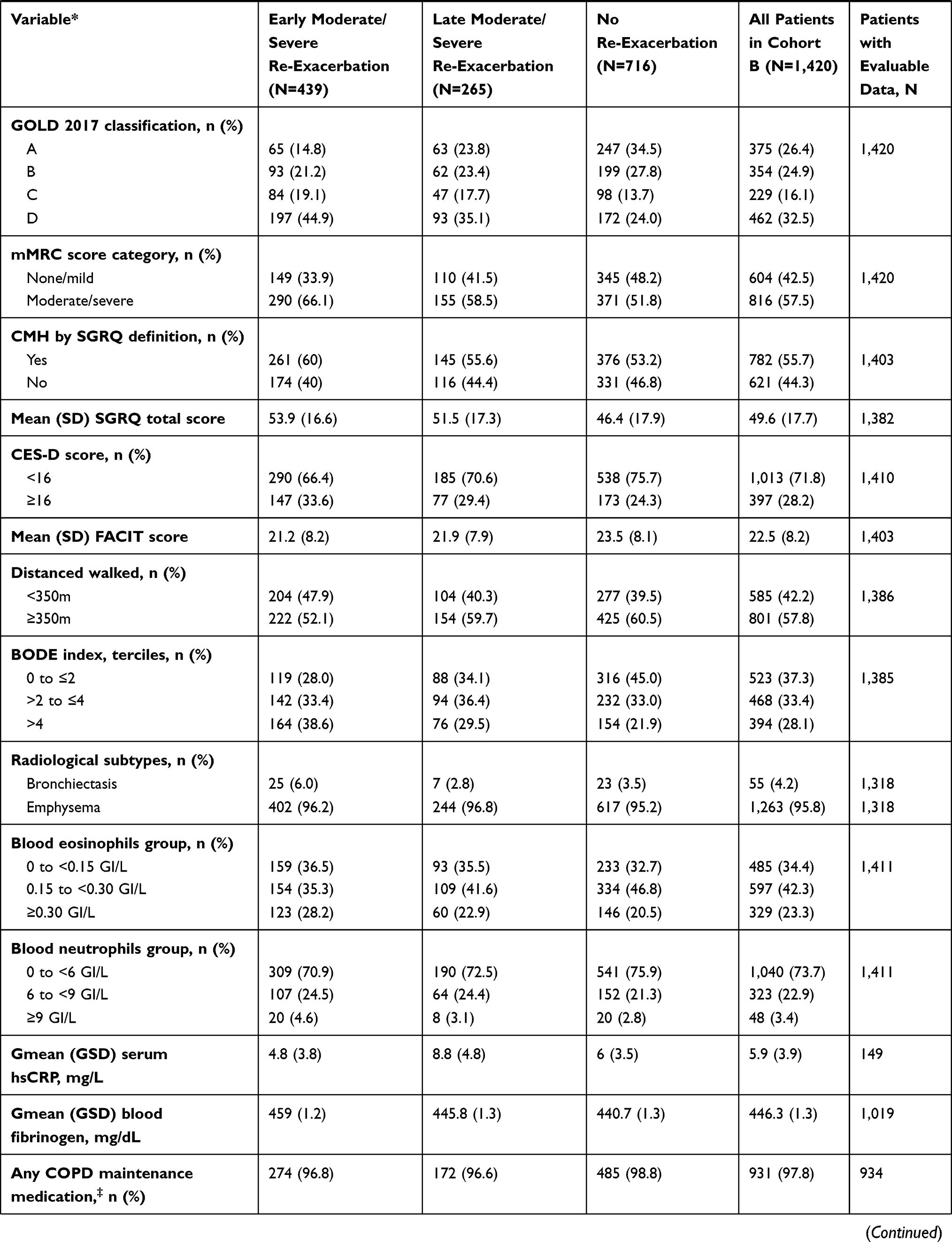 |  |
Table 2 Characteristics of Patients Experiencing Early or Late Moderate/Severe Re-Exacerbation, or No Re-Exacerbation, Following a Moderate/Severe Index Exacerbation (Cohort B) |
 |
Figure 4 Patients who experienced early, late, or no moderate/severe re-exacerbation within 180 days of index date. An early re-exacerbation occurred within 1–90 days from end of index exacerbation; a late re-exacerbation occurred between 91–180 days from end of index exacerbation; no re-exacerbation meant that a patient did not re-exacerbate within 1–180 days from end of index exacerbation. N=1,420 (moderate/severe index exacerbation). N=1,180 (moderate index exacerbation). N=240 (severe index exacerbation). |
 |
Figure 5 Multivariable analysis showing factors potentially predictive of early, late, or no moderate/severe re-exacerbation within 180 days of end of index moderate/severe exacerbation. (A) Proportional-odds-predictive model; (B) Non-proportional odds model. Notes: AECOPD, acute exacerbation of COPD; COPD, chronic obstructive pulmonary disease; CI, confidence interval; FEV1, forced expiratory volume in 1 second; SGRQ, St. George’s Respiratory Questionnaire; OR, odds ratio. |
Seasonality of index exacerbation was also predictive of early, late, or no exacerbation; however, adjusted ORs are provided for both comparisons owing to non-proportionality (early vs late or no exacerbation [OR=1.447; 95% CI=1.070–1.955; P=0.0164]; early or late vs no exacerbation [OR=1.456; 95% CI=1.098–1.930; P=0.0091]). These analyses suggest that with an autumn vs winter index exacerbation, the odds of an early re-exacerbation (vs late or no re-exacerbation) are increased by 45%, and the odds of any re-exacerbation are increased by 46%. Validation suggests the predictive model is internally valid, albeit with low agreement between observed and predicted events.
Partial-Proportional-Odds Model Validation
Our model predicted a larger number of patients with no re-exacerbation than patients with an early re-exacerbation and did not predict any patients with a late exacerbation, indicating potentially poor agreement between observed and predicted outcomes (Supplementary Figure 1). This was possibly due to the choice of an arbitrary 90-day threshold that subsequently hindered discrimination between the three re-exacerbation categories (early, late, and no re-exacerbation). Nevertheless, our model could be considered internally valid for the purposes of our study: hypothesis testing confirmed that we could reject the null hypothesis of no agreement (P<0.001), and the weighted kappa co-efficient of 0.283 (95% CI=0.238–0.239) indicated low agreement between observed and predicted outcomes.
Prolonged AECOPD Exacerbations and Exacerbation Duration
Overall, the median duration of moderate/severe exacerbations was 12 days (IQR=8–22). This was similar for the median duration of moderate (12 days, IQR=8–21) and severe (14 days, IQR=9–24) index exacerbations. The characteristics of patients with prolonged and non-prolonged AECOPD durations are described in Table 3. Of the 1,554 patients in cohort A, 353 (22.7%) experienced a prolonged AECOPD (77.1% moderate and 22.9% severe), and 1,201 (77.3%) experienced a non-prolonged AECOPD (83.3% moderate and 16.7% severe). Overall, no patients died while experiencing a moderate AECOPD, while 2.5% of patients (n=38) died while experiencing a severe AECOPD.
 | | 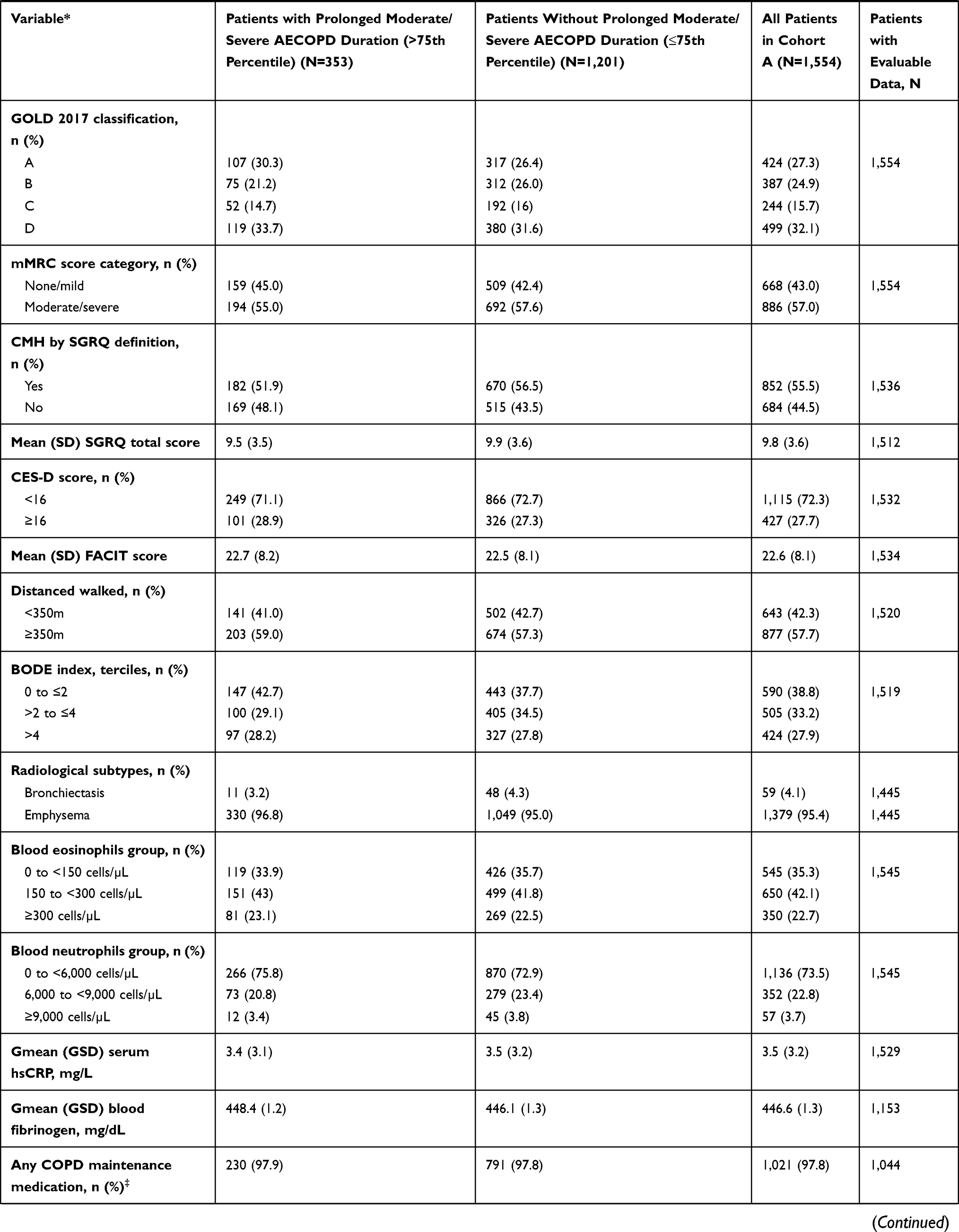 | 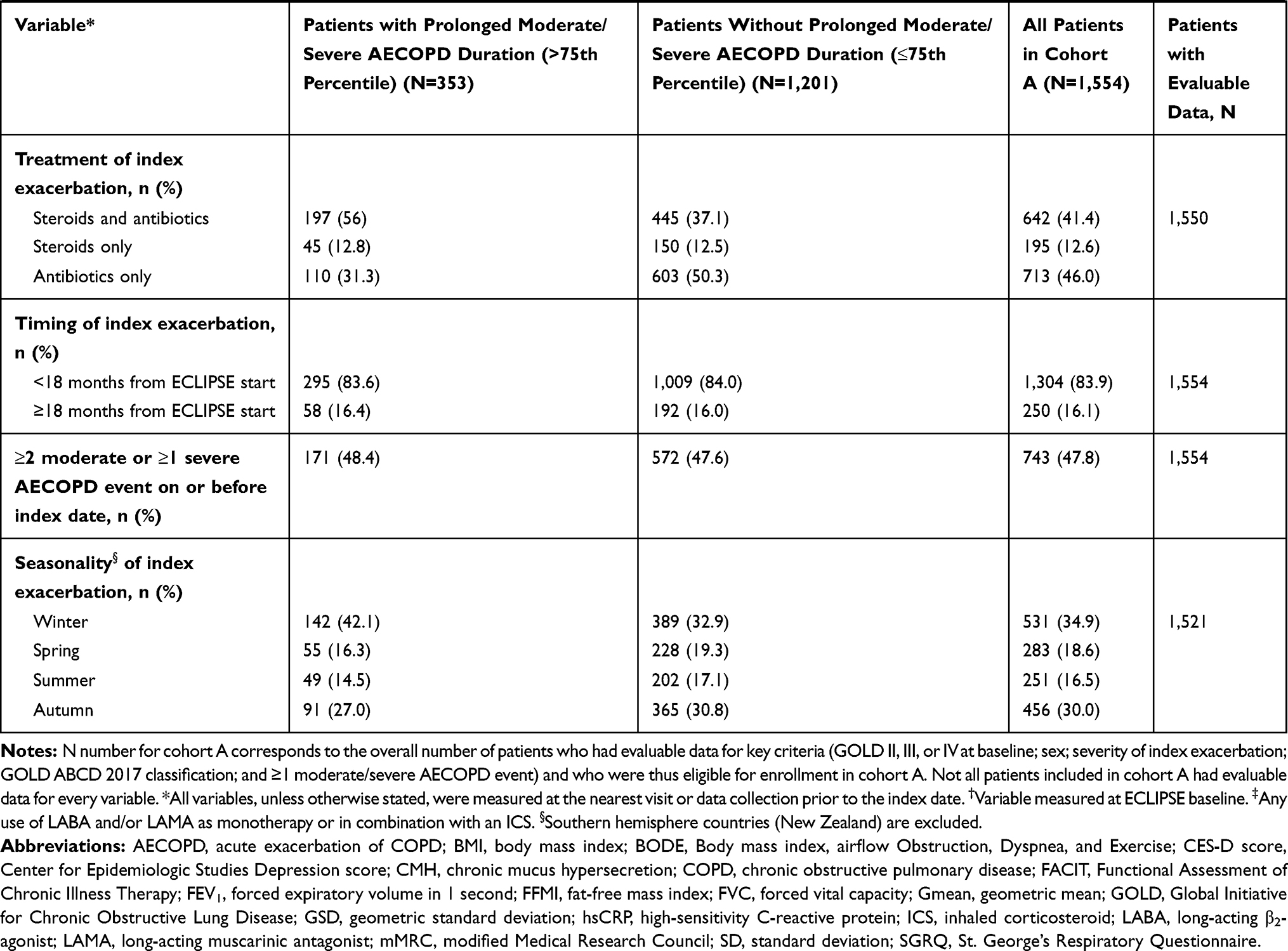 |
Table 3 Characteristics of Patients with Prolonged and Non-Prolonged Moderate/Severe AECOPD Events (Cohort A) |
In univariate analyses, female sex, high fat-free mass index, high mMRC dyspnea score, severe (vs moderate) exacerbation, and winter season had a statistically significant association (all P<0.05) with prolonged AECOPD duration (Table 4). In multivariate analysis, severity of exacerbation had a statistically significant association (P<0.05) with prolonged AECOPD duration. The odds of experiencing a prolonged AECOPD almost doubled for severe vs moderate AECOPD events (adjusted OR=1.917 [95% CI=1.269–2.896]; P=0.002), and the odds of patients experiencing a prolonged AECOPD event were 42% lower with a spring AECOPD event vs a winter AECOPD event (adjusted OR=0.578 [95% CI=0.368–0.906]; P=0.017). There was no evidence of an independent association with AECOPD duration and sex, fat-free mass index, and mMRC in the multivariate model.
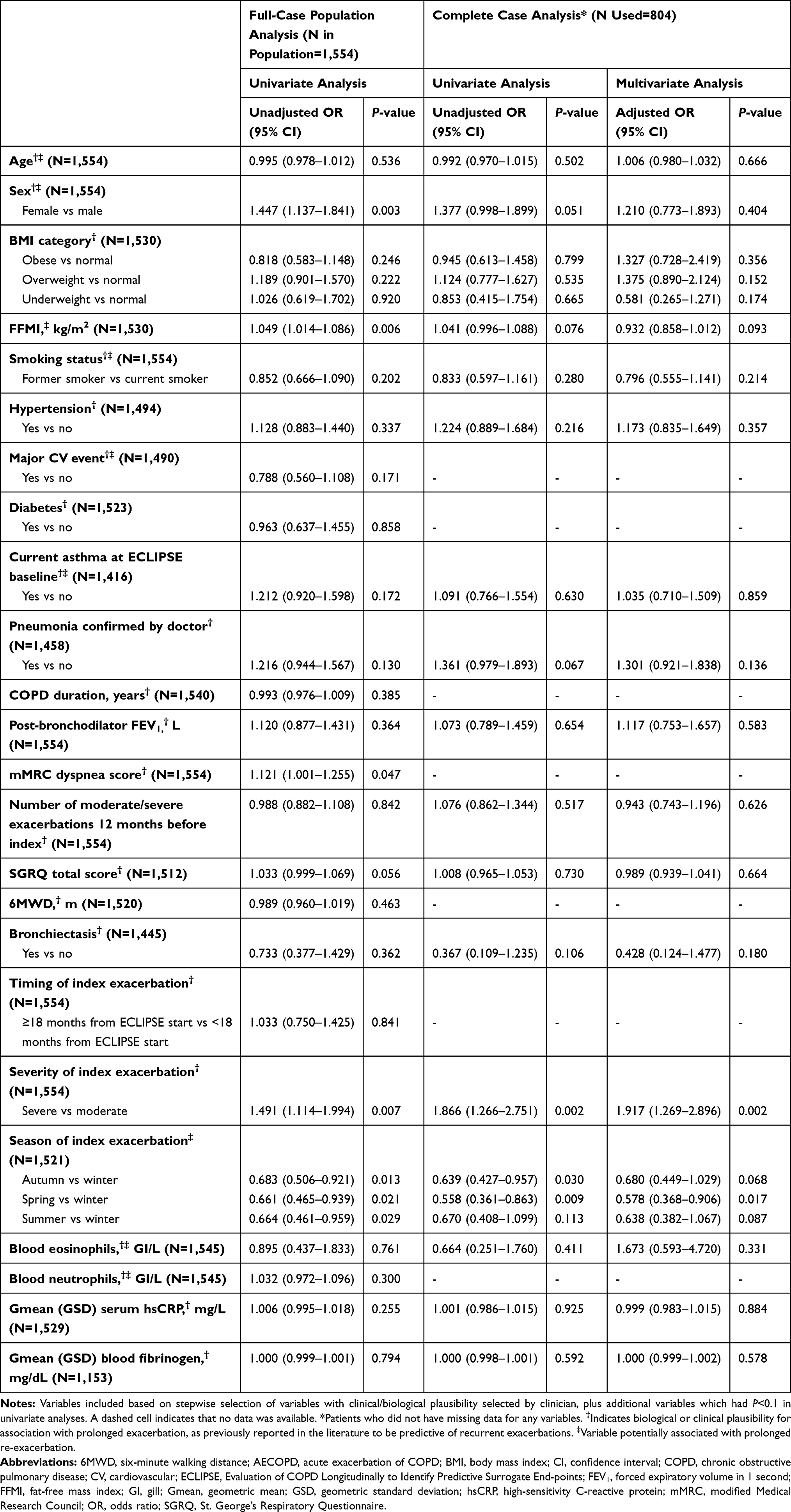 |
Table 4 Univariable and Multivariable Analyses of Factors Potentially Associated with Prolonged Moderate/Severe AECOPD Duration |
Although four variables in our analysis – osteoporosis, asthma, pneumonia, and bronchiectasis – had 9.0% missing data, all other variables had <5% missing data. The final model included only 804 patients with complete data on all variables. To assess the impact of missing data in our analyses, we replicated the univariate analyses using the final multivariate analysis population of 804 patients. There were no clear differences in either the magnitude or direction of the OR for the univariate analyses conducted on the wider and reduced populations (Table 4).
Discussion
An improved understanding of the factors that predict re-exacerbation timing and prolonged AECOPD events has the potential to improve COPD management. Our re-analysis of data from the ECLIPSE study identified factors predictive of early and late re-exacerbations, and also identified independent risk factors for prolonged AECOPD events, with subsequent implications for optimizing patient care.
Our study demonstrated that the risks of re-exacerbation are dynamic and that the timing of re-exacerbation may be affected by multiple factors, including lung function, exacerbation history, respiratory-related quality-of-life (disease burden, as measured with the SGRQ score), and season of index exacerbation. Whilst half of the patients with COPD in our study did not re-exacerbate within 180 days from the end of their index exacerbation, the proportion of patients with an early re-exacerbation within the first 90 days was almost double (30.9%) the proportion of patients with a late re-exacerbation between 91 and 180 days (18.7%). Although validation suggested that the model may not be ideal for predicting early vs late vs no re-exacerbation, the final model indicated that lower FEV1 and higher SGRQ total score were predictive of experiencing an early re-exacerbation. Similarly, index exacerbations occurring in autumn were also predictive of early re-exacerbations, vs index exacerbations occurring in winter. AECOPD severity was a predictor of whether a patient was likely to re-exacerbate early, but was not seen as a predictor of overall re-exacerbation risk based on Kaplan–Meier curves. These observations are consistent with other studies that reported impaired lung function, exacerbation frequency during the prior year (in addition to age, pleural effusion, accessory respiratory muscle use, medication, and hospitalization length),20 or prolonged exacerbation symptoms and poorer health status36 as being associated with re-exacerbation events in general. Evidence is lacking on factors that can predict timing of re-exacerbation. Seasonality is known to affect COPD exacerbations, most frequently occurring in the winter months,37–39 which is likely to reflect an increased prevalence of respiratory infections, reduced immunity, altered environmental conditions, and physiological responses during these months.40,41 Although the factors predictive of re-exacerbation timing require further investigation, our results support the existing body of literature on overall re-exacerbation risk which has subsequent implications for optimizing patient care. Although our study defined an early re-exacerbation/hospital re-admission as that occurring within 1–90 days after the end of the first AECOPD event, understanding which patients are more likely to experience an early re-exacerbation may have implications for helping hospitals in the US reduce their 30-day re-admission rates for patients with COPD, thereby minimizing the risk of financial penalties under the Hospital Readmission Reduction Program.42
Factors that have a causal association with prolonged AECOPD duration and, therefore, extended hospital stays for the most severe AECOPD patients are not well understood. Although some small-scale studies have aimed to explore such factors in hospitalized patients with severe AECOPDs, their usefulness remains limited due to different designs and the limited number of risk factors examined. Factors described in the literature as having an independent association with long or prolonged hospitalizations include comorbidities28 (such as heart failure, diabetes, and stroke); laboratory or clinical parameters (including high partial pressure of carbon dioxide in arterial blood,29,30 low serum albumin level,30 and mMRC dyspnea score);29 social factors (such as living alone); and medication use prior to hospitalization (ie, the use of more than three drugs, or of drugs with respiratory-depressant properties).28 A greater understanding of specific factors associated with prolonged moderate or severe AECOPDs (rather than just the length of a hospital stay, which only describes part of the duration of an AECOPD event and which may exclude less severe AECOPDs) could help physicians identify patients who would benefit from targeted risk-minimization measures, or from future therapies aimed at reducing exacerbation duration. To our knowledge, our study is the first study to explore the characteristics of patients who experienced prolonged moderate and severe AECOPD events (ie, events lasting >22 days), building on a previous study of patients experiencing severe AECOPD events.28 In our study, prolonged AECOPDs were observed in approximately one fifth (22.7%) of patients. After controlling for a wide range of patient- and exacerbation-related factors, our analysis found that only severity and seasonality of the exacerbation was independently associated with prolonged AECOPD duration. Prolonged AECOPD is likely to require more frequent healthcare contacts and may mean longer hospital stays. Our findings support previous studies of exacerbating patients with COPD that have identified factors associated with longer hospital stays: these include older age,43 female sex,44 disease severity,43,45,46 comorbidities, and a low serum albumin level.30
Our large study, which was based on the rich and well-collected demographic, clinical, and patient-reported data from the ECLIPSE study, was able to explore a large number of factors potentially predictive for early or late re-exacerbation, and factors potentially associated with prolonged AECOPD duration. Follow-up of patients in ECLIPSE was prospective, with short intervals between patient visits, thus allowing characteristics potentially associated with AECOPD events to be assigned within a short time of a patient’s index exacerbation.
AECOPD events were collected robustly in ECLIPSE and information on both moderate and severe exacerbations was available, allowing us to explore the impact of exacerbation severity on both exacerbation duration and timing of re-exacerbation risk.
A key limitation of our work relates to the thresholds for distinguishing between early and late re-exacerbations, and prolonged and non-prolonged AECOPD events. Although our visualization of the dynamic risk of re-exacerbation supports a 90-day threshold for defining early and late re-exacerbations, a distinct cut-off point applicable across studies of re-exacerbation timing may not exist. We used the 75th percentile as a cut-off for prolonged exacerbations. Although this threshold has been used in other studies,28,30 it may not be the optimal threshold. Use of an incorrect threshold diminishes our ability to identify predictors of early vs late re-exacerbation and our ability to understand factors (potentially) causally associated with prolonged duration.
Although the level of missing data in the ECLIPSE study is low, our final model to explore factors associated with prolonged exacerbation only retained half of the patients. Our hypothesis that data were missing at random was confirmed in our comparison of the strength and magnitude of association in univariate analyses in the full-case and complete-case populations, but it is possible that this level of missing data may have reduced our ability to identify all potential risk factors for prolonged exacerbation duration.
Although the ECLIPSE cohort was large, sample size may have constrained our predictive model on re-exacerbation risk. It is general practice to limit the number of predictors in a predictive model to one per every ten events. However, we identified a multitude of demographic, clinical, and exacerbation-specific factors and may have benefited from a larger cohort to fully explore the predictive nature of these factors. Further, our internal validation of the predictive model suggests that agreement between observed and predicted outcomes in cross-validation was sub-optimal. Other studies of COPD risk factor models that have been developed and validated in internal datasets without external validation are available;47–49 however, we do acknowledge that lack of external validation in our study is a potential limitation, and that future work to validate our model externally would subsequently be beneficial.
Conclusions
This study adds to existing knowledge of our ability to predict timing of future re-exacerbation outcomes for patients who experience an AECOPD event, and improves our understanding of the causal relationships between specific risk factors and prolonged exacerbation duration, with subsequent implications for optimizing patient care.
In this analysis, exacerbation history, impaired lung function, poorer respiratory-related quality-of-life (greater disease burden), and season of index exacerbation were identified as significant predictors of early re-exacerbation. Although risk of re-exacerbation is dynamic and likely to be influenced by multiple factors, optimizing medication regimens for patients more likely to experience an early re-exacerbation may improve patient outcomes. Severe AECOPDs and AECOPDs occurring in the winter are likely to be prolonged, relative to those occurring in the warmer months, and may therefore require closer monitoring.
Abbreviations
6MWD, six-minute walking distance; AECOPD, acute exacerbation of chronic obstructive pulmonary disease; BMI, body mass index; BODE, Body mass index, airflow Obstruction, Dyspnea and Exercise capacity; CES-D, Center for Epidemiologic Studies Depression score; CI, confidence interval; CMH, chronic mucus hypersecretion; COPD, chronic obstructive pulmonary disease; ECLIPSE, Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints; eCRF, electronic case-report form; FACIT, Functional Assessment of Chronic Illness Therapy; FEV1, forced expiratory volume in 1 second; FFM, fat-free mass; FFMI, fat-free mass index; FVC, forced vital capacity; GI, gill; GERD, gastroesophageal reflux disease; Gmean, geometric mean; GOLD, Global Initiative for Chronic Obstructive Lung Disease; GSD, geometric standard deviation; hsCRP, high-sensitivity C-reactive protein; ICS, inhaled corticosteroid; IQR, interquartile range; L, liter; LABA, long-acting β2-agonist; LABD, long-acting bronchodilator; LAMA, long-acting muscarinic antagonist; mMRC, modified Medical Research Council; OR, odds ratio; PROM, patient-reported outcome measure; SABD, short-acting bronchodilator; SGRQ, St. George’s Respiratory Questionnaire.
Data Sharing Statement
Anonymized individual participant data and study documents can be requested for further research from www.clinicalstudydatarequest.com.
Acknowledgments
Medical writing support (including manuscript development, collating author comments, and grammatical editing) was provided by Joanna Wilson, PhD of Gardiner–Caldwell Communications (Glasgow, UK) and was funded by GlaxoSmithKline plc. The studies in our analysis (study numbers 209217 and 210008) and the ECLIPSE study (NCT00292552) were funded by GlaxoSmithKline plc.
Author Contributions
All authors made substantial contributions to the study conception and/or design, and data analysis and/or interpretation. All authors critically reviewed the manuscript for important intellectual content and gave final approval for its submission and publication. All authors agree to be fully accountable for all aspects of the work.
Disclosure
Wilhelmine H Meeraus and William A Fahy are employees of, and hold shares in, GlaxoSmithKline plc. Hana Mullerova was an employee of GlaxoSmithKline plc. at the time the study was conducted, and is now an employee of AstraZeneca. Céline El Baou was an employee of GlaxoSmithKline plc. at the time the study was conducted, and is now the owner of CEBSTAT Consultancy Ltd. Marion Fahey was an employee of GlaxoSmithKline plc. at the time the study was conducted, and is now an employee of Pfizer. Edith M Hessel was an employee of and shareholder in GlaxoSmithKline plc. at the time the study was conducted, and is now an employee of Mestag Therapeutics, Ltd. The authors report no other conflicts of interest in this work.
References
1. Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease; 2021. Available from: https://goldcopd.org/wp-content/uploads/2020/11/GOLD-REPORT-2021-v1.1-25Nov20_WMV.pdf.
2. GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. The Lancet. 2018;392(10159):1789–1858. doi:10.1016/S0140-6736(18)32279-7
3. Wedzicha JA, Seemungal TA. COPD exacerbations: defining their cause and prevention. Lancet. 2007;370(9589):786–796. doi:10.1016/S0140-6736(07)61382-8
4. Seemungal TA, Donaldson GC, Bhowmik A, et al. Time course and recovery of exacerbations in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2000;161(5):1608–1613. doi:10.1164/ajrccm.161.5.9908022
5. Rothnie KJ, Mullerova H, Smeeth L, et al. Natural history of chronic obstructive pulmonary disease exacerbations in a general practice-based population with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2018;198(4):464–471. doi:10.1164/rccm.201710-2029OC
6. Ramsey SD, Sullivan SD. The burden of illness and economic evaluation for COPD. Eur Respir J Suppl. 2003;41:29s–35s. doi:10.1183/09031936.03.00078203
7. Strassels SA, Smith DH, Sullivan SD, et al. The costs of treating COPD in the United States. Chest. 2001;119(2):344–352. doi:10.1378/chest.119.2.344
8. Hurst JR, Vestbo J, Anzueto A, et al. Susceptibility to exacerbation in chronic obstructive pulmonary disease. N Engl J Med. 2010;363(12):1128–1138. doi:10.1056/NEJMoa0909883
9. Suissa S, Dell’Aniello S, Ernst P. Long-term natural history of chronic obstructive pulmonary disease: severe exacerbations and mortality. Thorax. 2012;67(11):957–963. doi:10.1136/thoraxjnl-2011-201518
10. Erdal M, Johannessen A, Eagan TM, et al. Incidence of utilization- and symptom-defined COPD exacerbations in hospital- and population-recruited patients. Int J Chron Obstruct Pulmon Dis. 2016;11:2099–2108. doi:10.2147/COPD.S108720
11. Halpin DM, Miravitlles M, Metzdorf N, et al. Impact and prevention of severe exacerbations of COPD: a review of the evidence. Int J Chron Obstruct Pulmon Dis. 2017;12:2891–2908. doi:10.2147/COPD.S139470
12. Han MK, Quibrera PM, Carretta EE, et al. Frequency of exacerbations in patients with chronic obstructive pulmonary disease: an analysis of the SPIROMICS cohort. Lancet Respir Med. 2017;5(8):619–626. doi:10.1016/S2213-2600(17)30207-2
13. Hartley BF, Barnes NC, Lettis S, et al. Risk factors for exacerbations and pneumonia in patients with chronic obstructive pulmonary disease: a pooled analysis. Respir Res. 2020;21(1):5. doi:10.1186/s12931-019-1262-0
14. Jinjuvadia C, Jinjuvadia R, Mandapakala C, et al. Trends in outcomes, financial burden, and mortality for acute exacerbation of chronic obstructive pulmonary disease (COPD) in the United States from 2002 to 2010. COPD. 2017;14(1):72–79. doi:10.1080/15412555.2016.1199669
15. Make BJ, Eriksson G, Calverley PM, et al. A score to predict short-term risk of COPD exacerbations (SCOPEX). Int J Chron Obstruct Pulmon Dis. 2015;10:201–209. doi:10.2147/COPD.S69589
16. Stanford RH, Korrer S, Brekke L, et al. Validation and assessment of the COPD treatment ratio as a predictor of severe Exacerbations. Chronic Obstr Pulm Dis. 2020;7(1):38–48. doi:10.15326/jcopdf.7.1.2019.0132
17. Worth H, Buhl R, Criee CP, et al. GOLD 2017 treatment pathways in ‘real life’: an analysis of the DACCORD observational study. Respir Med. 2017;131:77–84. doi:10.1016/j.rmed.2017.08.008
18. Lindenauer PK, Dharmarajan K, Qin L, et al. Risk trajectories of readmission and death in the first year after hospitalization for chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2018;197(8):1009–1017. doi:10.1164/rccm.201709-1852OC
19. Seymour JM, Moore L, Jolley CJ, et al. Outpatient pulmonary rehabilitation following acute exacerbations of COPD. Thorax. 2010;65(5):423–428. doi:10.1136/thx.2009.124164
20. Liu D, Peng SH, Zhang J, et al. Prediction of short term re-exacerbation in patients with acute exacerbation of chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2015;10:1265–1273. doi:10.2147/COPD.S83378
21. Almagro P, Cabrera FJ, Diez J, et al. Comorbidities and short-term prognosis in patients hospitalized for acute exacerbation of COPD: the EPOC en servicios de medicina interna (ESMI) study. Chest. 2012;142(5):1126–1133. doi:10.1378/chest.11-2413
22. Johannesdottir SA, Christiansen CF, Johansen MB, et al. Hospitalization with acute exacerbation of chronic obstructive pulmonary disease and associated health resource utilization: a population-based Danish cohort study. J Med Econ. 2013;16(7):897–906. doi:10.3111/13696998.2013.800525
23. Baker CL, Zou KH, Su J. Risk assessment of readmissions following an initial COPD-related hospitalization. Int J Chron Obstruct Pulmon Dis. 2013;8:551–559. doi:10.2147/COPD.S51507
24. Meeraus W, Benson V, Tabberer M, et al. How are recovery and recurrence of COPD exacerbations defined in observational studies? A systematic review. Eur Respir J. 2018;52:PA1167.
25. Meeraus W, Mullerova H, Tabberer M, et al. Systematic review of COPD re-exacerbation and exacerbation treatment failure definitions used in randomised controlled trials (RCTs). Eur Respir J. 2018;52:PA1171.
26. Donaldson GC, Wedzicha JA. COPD exacerbations.1: epidemiology. Thorax. 2006;61(2):164–168. doi:10.1136/thx.2005.041806
27. Bollmeier SG, Hartmann AP. Management of chronic obstructive pulmonary disease: a review focusing on exacerbations. Am J Health Syst Pharm. 2020;77(4):259–268. doi:10.1093/ajhp/zxz306
28. Incalzi RA, Pedone C, Onder G, et al. Predicting length of stay of older patients with exacerbated chronic obstructive pulmonary disease. Aging (Milano). 2001;13(1):49–57.
29. Crisafulli E, Ielpo A, Barbeta E, et al. Clinical variables predicting the risk of a hospital stay for longer than 7 days in patients with severe acute exacerbations of chronic obstructive pulmonary disease: a prospective study. Respir Res. 2018;19(1):261. doi:10.1186/s12931-018-0951-4
30. Wang Y, Stavem K, Dahl FA, et al. Factors associated with a prolonged length of stay after acute exacerbation of chronic obstructive pulmonary disease (AECOPD). Int J Chron Obstruct Pulmon Dis. 2014;9:99–105. doi:10.2147/COPD.S51467
31. Vestbo J, Anderson W, Coxson HO, et al. Evaluation of COPD longitudinally to identify predictive surrogate end-points (ECLIPSE). Eur Respir J. 2008;31(4):869–873. doi:10.1183/09031936.00111707
32. Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease; 2009.
33. Agusti A, Calverley PM, Celli B, et al. Characterisation of COPD heterogeneity in the ECLIPSE cohort. Respir Res. 2010;11(1):122. doi:10.1186/1465-9921-11-122
34. Peterson B, Harrell JF. Partial proportional odds models for ordinal response variables. J Royal Stat Soc. 1990;39(2):205–217.
35. Derr B. Ordinal response modeling with the LOGISTIC procedure. SAS Global Forum; 2013. San Francisco. Available from: https://support.sas.com/resources/papers/proceedings13/446-2013.pdf.
36. Donaldson GC, Law M, Kowlessar B, et al. Impact of prolonged exacerbation recovery in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2015;192(8):943–950. doi:10.1164/rccm.201412-2269OC
37. Wise RA, Calverley PM, Carter K, et al. Seasonal variations in exacerbations and deaths in patients with COPD during the TIOSPIR® trial. Int J Chron Obstruct Pulmon Dis. 2018;13:605–616. doi:10.2147/COPD.S148393
38. Rabe KF, Fabbri LM, Vogelmeier C, et al. Seasonal distribution of COPD exacerbations in the prevention of exacerbations with tiotropium in COPD trial. Chest. 2013;143(3):711–719. doi:10.1378/chest.12-1277
39. Jenkins CR, Celli B, Anderson JA, et al. Seasonality and determinants of moderate and severe COPD exacerbations in the TORCH study. Eur Respir J. 2012;39(1):38–45. doi:10.1183/09031936.00194610
40. Ko FW, Chan KP, Hui DS, et al. Acute exacerbation of COPD. Respirology. 2016;21(7):1152–1165. doi:10.1111/resp.12780
41. Hicks A, Healy E, Sandeman N, et al. A time for everything and everything in its time – exploring the mechanisms underlying seasonality of COPD exacerbations. Int J Chron Obstruct Pulmon Dis. 2018;13:2739–2749. doi:10.2147/COPD.S146015
42. McIlvennan CK, Eapen ZJ, Allen LA. Hospital readmissions reduction program. Circulation. 2015;131(20):1796–1803. doi:10.1161/CIRCULATIONAHA.114.010270
43. Roberts CM, Lowe D, Bucknall CE, et al. Clinical audit indicators of outcome following admission to hospital with acute exacerbation of chronic obstructive pulmonary disease. Thorax. 2002;57(2):137–141. doi:10.1136/thorax.57.2.137
44. Säynäjäkangas O, Kinnunen T, Tuuponen T, et al. Length of stay and interval to readmission in emergency hospital treatment of COPD. Age Ageing. 2004;33(6):567–570. doi:10.1093/ageing/afh188
45. Wong AW, Gan WQ, Burns J, et al. Acute exacerbation of chronic obstructive pulmonary disease: influence of social factors in determining length of hospital stay and readmission rates. Can Respir J. 2008;15(7):361–364. doi:10.1155/2008/569496
46. Ruparel M, Lopez-Campos JL, Castro-Acosta A, et al. Understanding variation in length of hospital stay for COPD exacerbation: European COPD audit. ERJ Open Res. 2016;2(1):1. doi:10.1183/23120541.00034-2015
47. Kotz D, Simpson CR, Viechtbauer W, et al. Development and validation of a model to predict the 10-year risk of general practitioner-recorded COPD. NPJ Prim Care Respir Med. 2014;24(1):14011. doi:10.1038/npjpcrm.2014.11
48. Himes BE, Dai Y, Kohane IS, et al. Prediction of chronic obstructive pulmonary disease (COPD) in asthma patients using electronic medical records. J Am Med Inform Assoc. 2009;16(3):371–379. doi:10.1197/jamia.M2846
49. Annavarapu S, Goldfarb S, Gelb M, et al. Development and validation of a predictive model to identify patients at risk of severe COPD exacerbations using administrative claims data. Int J Chron Obstruct Pulmon Dis. 2018;13:2121–2130. doi:10.2147/COPD.S155773
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.