Back to Journals » Breast Cancer: Targets and Therapy » Volume 17
Predicting Axillary Lymph Node Metastasis in Young Onset Breast Cancer: A Clinical-Radiomics Nomogram Based on DCE-MRI
Authors Dong X, Meng J, Xing J, Jia S, Li X, Wu S
Received 19 September 2024
Accepted for publication 10 January 2025
Published 27 January 2025 Volume 2025:17 Pages 103—113
DOI https://doi.org/10.2147/BCTT.S495246
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Robert Clarke
Xia Dong,1 Jingwen Meng,1 Jun Xing,2 Shuni Jia,3 Xueting Li,4 Shan Wu1
1Department of Radiology, Shanxi Bethune Hospital, Shanxi Academy of Medical Sciences, Tongji Shanxi Hospital, Third Hospital of Shanxi Medical University, Taiyuan, 030032, People’s Republic of China; 2Department of Breast Surgery, Shanxi Bethune Hospital, Shanxi Academy of Medical Sciences, Tongji Shanxi Hospital, Third Hospital of Shanxi Medical University, Taiyuan, 030032, People’s Republic of China; 3Department of Ultrasound, Shanxi Bethune Hospital, Shanxi Academy of Medical Sciences, Tongji Shanxi Hospital, Third Hospital of Shanxi Medical University, Taiyuan, 030032, People’s Republic of China; 4Department of Pathology, Shanxi Bethune Hospital, Shanxi Academy of Medical Sciences, Tongji Shanxi Hospital, Third Hospital of Shanxi Medical University, Taiyuan, 030032, People’s Republic of China
Correspondence: Shan Wu, Department of Radiology, Shanxi Bethune Hospital, Shanxi Academy of Medical Sciences, Tongji Shanxi Hospital, Third Hospital of Shanxi Medical University, No. 99, Longcheng Street, Taiyuan, Shanxi Province, 030032, People’s Republic of China, Tel +86 03518368398, Email [email protected]
Background: Young onset breast cancer, diagnosed in women under 50, is known for its aggressive nature and challenging prognosis. Precisely forecasting axillary lymph node metastasis (ALNM) is essential for customizing treatment plans and enhancing patient results.
Objective: This research sought to create and verify a clinical-radiomics nomogram that combines radiomic features from Dynamic Contrast-Enhanced Magnetic Resonance Imaging (DCE-MRI) with standard clinical predictors to improve the accuracy of predicting ALNM in young breast cancer patients.
Methods: We performed a retrospective analysis at one facility, involving the creation and validation of a nomogram in two stages.At first, a medical model was developed utilizing conventional indicators like tumor dimensions, molecular classifications, multifocal presence, and MRI-determined ALN status.A more detailed clinical-radiomics model was subsequently developed by integrating radiomic characteristics derived from DCE-MRI images.These models were created using logistic regression analyses on a training dataset, and their effectiveness was assessed by measuring the area under the receiver operating characteristic curve (AUC) in a separate validation dataset.
Results: The clinical-radiomics nomogram surpassed the clinical-only model, recording an AUC of 0.892 in the training dataset and 0.877 in the validation dataset.Significant predictors included MRI-reported ALN status and select radiomic features, which markedly enhanced the model’s predictive capacity.
Conclusion: Integrating radiomic features with clinical predictors in a nomogram significantly improves ALNM prediction in young onset breast cancer, providing a valuable tool for personalized treatment planning. This study underscores the potential of merging advanced imaging data with clinical insights to refine oncological predictive models. Future research should expand to multicentric studies and include genomic data to boost the nomogram’s generalizability and precision.
Keywords: young onset breast cancer, clinical-radiomics nomogram, axillary lymph node metastasis, dynamic contrast-enhanced MRI
Introduction
Breast cancer is the most prevalent malignancy affecting women worldwide, with a significant trend toward the increasing incidence of early-onset breast cancer—defined as cases diagnosed before the age of 50.1 These early-onset cases often exhibit more aggressive behaviors and have less favorable outcomes compared to later-onset breast cancer.2 This emphasizes the urgent need for improved diagnostic and prognostic methods specifically tailored to this younger demographic, to enhance their clinical management and improve survival rates.
Despite extensive research into breast cancer, the specific challenge of predicting axillary lymph node metastasis (ALNM) in early-onset breast cancer remains inadequately addressed. While numerous studies have developed predictive models for ALNM in the general breast cancer population, there is a notable gap in research focusing exclusively on young women with breast cancer.3–5 This subgroup presents unique biological characteristics and clinical outcomes, necessitating dedicated studies to understand and predict ALNM effectively.6 The use of DCE-MRI and the emerging field of radiomics—which involves extracting large-scale quantitative data from medical images—offer promising tools.7,8 Evidence suggests that younger breast cancer patients exhibit higher rates of ALNM, potentially due to more aggressive tumor phenotypes and distinct tumor biology, highlighting the need for age-specific prediction models.9 However, their potential to specifically forecast ALNM in young breast cancer patients has not been fully explored and leveraged in clinical practice.
This study aims to fill this gap by developing and validating a clinical-radiomics nomogram that integrates DCE-MRI-derived radiomic features with traditional clinical indicators, specifically tailored for predicting ALNM in patients with early-onset breast cancer. By employing a systematic approach that merges advanced imaging analytics with robust clinical parameters, this research seeks to establish a predictive model that is both accurate and practical for clinical use. The model’s efficacy will be rigorously assessed through comprehensive statistical analyses within a training cohort and validated in an independent dataset to ensure its reliability and utility in enhancing decision-making and personalizing treatment strategies for this particularly vulnerable group of patients.
Methods
Participants
A methodology for predicting ALNM in young onset breast cancer using a clinical-radiomics nomogram based on DCE-MRI and clinical risk factors was shown in Figure 1. This retrospective study focused on female patients diagnosed with early-onset breast cancer, defined as a diagnosis before the age of 50. Data collection occurred at a Shanxi Bethune Hospital between March 2020 and February 2024. The study was designed to collect comprehensive patient information and MRI images to develop and validate a clinical-radiomics nomogram for predicting ALNM. Moreover, it was exempt from ethics approval due to its non-interventional design and the use of anonymized data.
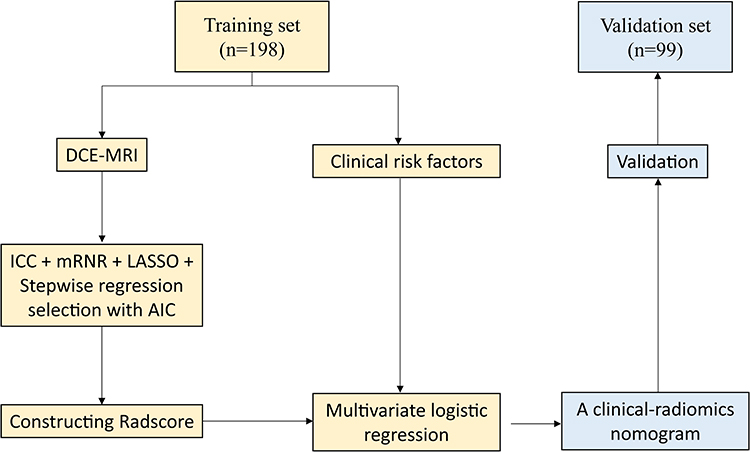 |
Figure 1 Flowchart illustrating the process of clinical-radiomics nomogram modeling for the LNM prediction in patients with PTC. Abbreviations: DCE-MRI, dynamic contrast-enhanced magnetic resonance imaging; GLDM, gray level dependence matrix; GLCM, gray level co-occurrence matrix; GLRLM, gray level run length matrix; GLSZM, gray level size zone matrix; ICC, interclass correlation coefficient; mRMR, minimum redundancy maximum relevance; LASSO, least absolute shrinkage and selection operator; AIC, Akaike information criterion; Radscore, radiomics score. |
Eligible participants included those newly diagnosed with breast cancer, with no prior cancer treatments, no history of recurrent breast cancer, and no metastatic disease at diagnosis. Patients were also required to have complete clinical records and high-quality DCE-MRI scans. Patients who did not meet these criteria were excluded from the study to ensure the reliability of the predictive model.
The study cohort was systematically divided into a training set and a validation set using a 2:1 ratio. This allocation resulted in 198 patients in the training set, used for developing the predictive models, and 99 patients in the validation set, used for testing the models’ performance. Collected data included demographic information, detailed clinical profiles, and radiological imaging. Clinical data encompassed variables such as menopausal status, tumor location, histologic grade, multifocality, molecular subtypes, and receptor statuses (ER, PR, HER2).
Image Acquisition
DCE-MRI scans were conducted using a 3.0 Tesla MRI system (Magnetom Skyra, Siemens Healthineers) equipped with a dedicated breast coil. The imaging protocol included an axial T1-weighted sequence for baseline tissue characterization, a T2-weighted sequence to distinguish fluid from soft tissue, and dynamic sequences post-injection of 0.1 mmol/kg of a gadolinium-based contrast agent (Gadovist, Bayer Healthcare). Parameters for dynamic imaging were set to a repetition time (TR) of 4.45 ms, echo time (TE) of 1.68 ms, a flip angle of 10°, field of view (FOV) of 340×340 mm, a matrix of 512 x 512, and slice thickness of 1.6 mm with no inter-slice gap, achieving a temporal resolution of 7 seconds per phase. Image quality was rigorously controlled by reviewing all scans for artifacts and overall quality by two experienced radiologists, ensuring only high-quality images were included in the study to support the development and validation of the clinical-radiomics nomogram.
Image Segmentation and Feature Extraction
Nodule segmentation was performed using the ITK-SNAP software, and interobserver reproducibility was assessed by two physicians independently segmenting a subset of 30 randomly selected cases. Radiomics feature extraction was conducted using the 3D-Slicer software, with image normalization and resampling to a voxel size of 1 mm × 1 mm × 1 mm. A total of 912 radiomics features were extracted, including first-order statistics, gray level dependence matrix (GLDM), gray level co-occurrence matrix (GLCM), gray level run length matrix (GLRLM), and gray level size zone matrix (GLSZM).
Feature Selection and Radiomics Score Construction
In the development of our clinical-radiomics nomogram for predicting ALNM in young onset breast cancer patients, image segmentation and feature extraction were crucial steps. High-quality DCE-MRI scans were used, with tumor regions of interest (ROIs) meticulously delineated on each image slice by two experienced radiologists independently, resolving any discrepancies through consensus. Using the PyRadiomics software package, version 3.0, a diverse set of radiomic features was extracted from these ROIs, including Gray Level Size Zone Matrix (GLSZM), First-order statistics, GLRLM, GLDM, and GLCM. These features encapsulate various aspects of texture and intensity distribution within the tumors, providing a detailed characterization of tumor phenotype. The features were normalized to minimize variability due to machine settings or patient movement, followed by a rigorous feature selection process. Initial filtering removed features with low interclass correlation coefficients (ICC ≤ 0.75) to ensure reproducibility. The remaining features were then refined through the minimum redundancy maximum relevance (mRMR) technique and finally, the Least Absolute Shrinkage and Selection Operator (LASSO) method was employed to identify the most predictive features for inclusion in the nomogram, thus enhancing its predictive accuracy for lymph node metastasis.
Development of the Clinical Model and the Clinical-Radiomics Nomogram
Initially, we developed a clinical model based solely on patient demographic and tumor characteristics such as age, menopausal status, tumor size, histologic grade, molecular subtypes, and receptor statuses (ER, PR, HER2). Multivariable logistic regression was used to identify significant predictors of lymph node metastasis. The variables that demonstrated statistical significance in predicting lymph node status were incorporated into the clinical model.
Building on the clinical model, we developed the clinical-radiomics nomogram, which integrated the selected radiomics features derived from the DCE-MRI image analysis. The process began with the comprehensive feature selection as described in the previous sections, utilizing LASSO regression to identify the most predictive radiomics features. These features were then integrated with the clinically significant predictors from the initial model using multivariable logistic regression.
The integration aimed to create a more robust predictive tool, the clinical-radiomics nomogram, designed to provide a graphical representation of individual probabilities of ALNM. The discriminative capacity of the nomogram was determined by calculating the area under the receiver operating characteristic (ROC) curve (AUC). Additionally, calibration plots were employed to examine the agreement between the predicted probabilities and observed outcomes, ensuring the model’s accuracy and reliability.
The final nomogram was validated externally in the validation cohort, confirming its predictive performance and utility in clinical settings. This integrated approach not only enhanced the predictive accuracy but also facilitated a more nuanced risk stratification and personalized treatment planning for young onset breast cancer patients.
Statistical Analysis
All statistical analyses were performed using the R software (version 4.0.2). Quantitative data were summarized using descriptive statistics, expressed either as mean ± standard deviation or as median with interquartile ranges. A p-value threshold of less than 0.05 was established for statistical significance across all tests. This criterion was applied to various tests of independence, including chi-square tests for categorical variables and t-tests for continuous variables, utilized during the preliminary data analysis stage.
Results
Patient Characteristics
Table 1 compares patient characteristics between the training set (198 patients) and the validation set (99 patients) in a study, with no statistically significant differences observed across most parameters, indicating well-matched groups. Key characteristics such as menopause status, tumor location, histologic grade, multifocality, MRI-reported axillary lymph node (ALN) status, histologic type, and receptor status (ER, PR, HER2) are reported alongside molecular subtypes and basic demographic data like age and tumor size. The similar distribution of these characteristics between the two groups, reflected in the p-values (all above 0.05 except for a marginally significant difference in ER status with p=0.053), supports the external validity of the findings derived from this dataset.
 |
Table 1 Patients’ Characteristics of Training Set and Validation Set |
Radiomics Score Building
After filtering out features with an ICC of ≤ 0.75, we retained 912 features from the DCE-MRI data (Table S1). The mRMR algorithm then narrowed this selection down to 30 significant features. Subsequently, the LASSO regression analysis, as illustrated in Figure 2, identified 7 pivotal features. These were further refined through backward stepwise logistic regression analysis, which pinpointed 4 essential radiomics features linked to ALNM in young onset breast cancer (Table S2). Utilizing these features, we developed a DCE-MRI radiomics score, formulated as follows:

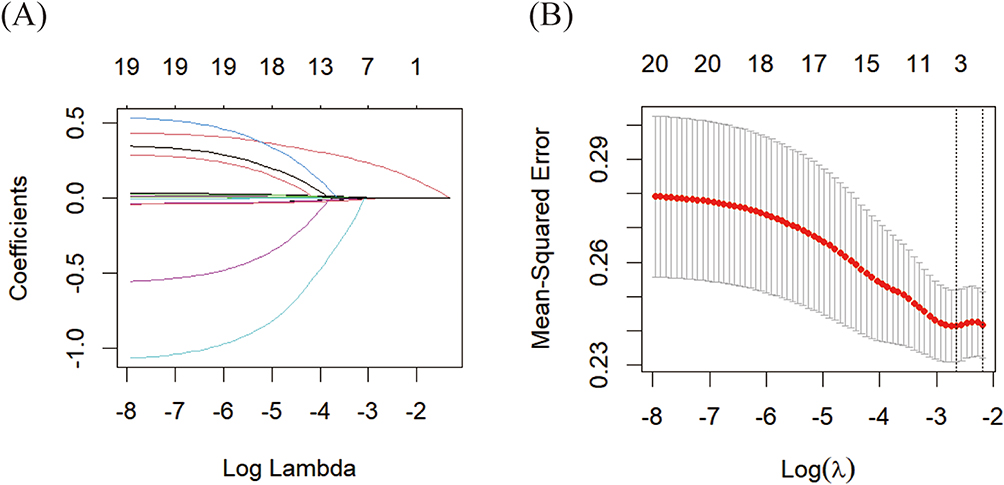 |
Figure 2 LASSO Regression Analysis for Feature Selection in the Training Set. The LASSO regression process used to select features within the training set for predicting axillary lymph node metastasis. (A) displays the trajectories of the coefficients for various predictors across different log(λ) values, demonstrating how each coefficient approaches zero as the regularization penalty increases. (B) shows the mean squared error (MSE) of the model across various log(λ) values, with the continuous red line indicating MSE and dotted vertical lines identifying the optimal λ values that ensure a balance between model accuracy and simplicity. |
Model Building and Validation
Table 2 outlines the results of stepwise multivariate analyses used to predict lymph node metastasis (LNM) in breast cancer, focusing on a clinical model and a clinical-radiomics model. In the clinical model, multifocality, molecular subtypes, tumor size, and MRI-reported axillary lymph node (ALN) status were significant predictors, with MRI-reported ALN status showing a particularly strong association with LNM (OR = 3.17, p = 0.003). Transitioning to the clinical-radiomics model, the inclusion of a radiomics score markedly improved predictive power. The radiomics score itself demonstrated a substantial odds ratio of 2.63 (p = 0.009). This model adjustment not only retained the significance of molecular subtypes and tumor size but also elevated the odds ratio for MRI-reported ALN status to 6.12 (p = 0.024). To further ensure the robustness of the clinical-radiomics nomogram, a 5-fold cross-validation was conducted during the training phase. This yielded a consistent mean cross-validated AUC of 0.884 across folds, demonstrating the stability of the model. In the independent validation cohort, the model achieved a testing accuracy of 87.7%, confirming its reliability in predicting ALNM.
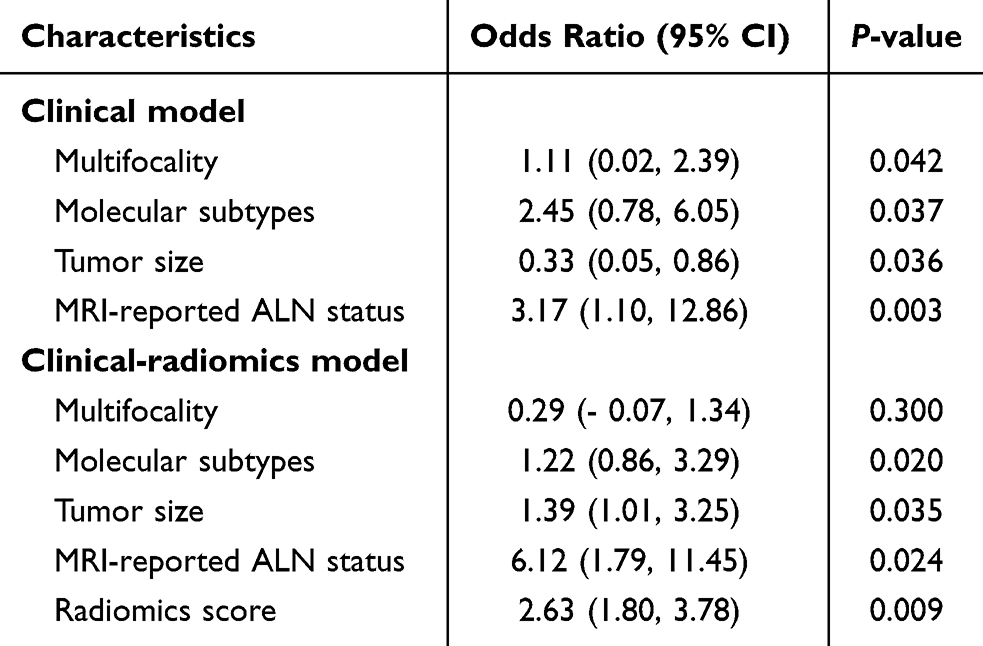 |
Table 2 The Results of Stepwise Multivariate Analyses for Prediction of LNM |
Figure 3 display the ROC curves for two predictive models across the training and validation datasets. In training set (Figure 3A), the clinical-radiomics model significantly outperforms the clinical model with an AUC of 0.892 compared to 0.653. Validation set (Figure 3B) shows a similar trend, where the clinical-radiomics model achieves an AUC of 0.877, vastly superior to the clinical model’s AUC of 0.621.
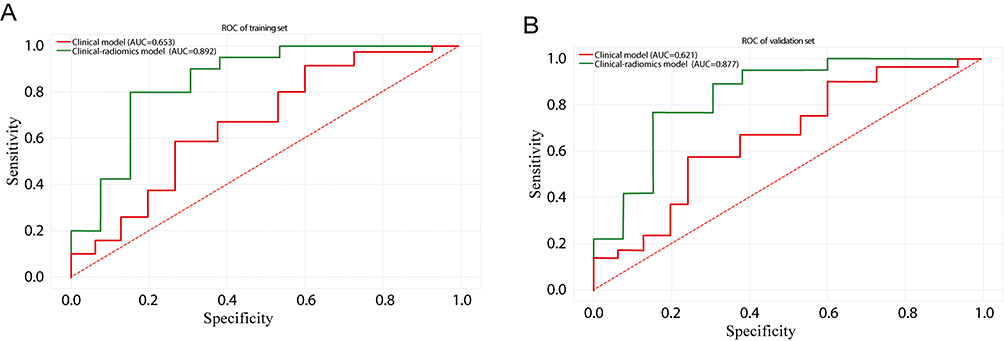 |
Figure 3 ROC Curves Comparing Clinical and Clinical-Radiomics Models on the training set (A) and the validation set (B). Panel A shows the ROC curves from the training set, highlighting the comparative performance of the clinical model against the more advanced clinical-radiomics model. Panel B presents the ROC curves from the validation set, similarly comparing the two models. The curves demonstrate the superior predictive capability of the clinical-radiomics model over the traditional clinical model in both datasets. |
Figure 4 demonstrates the effectiveness of a clinical-radiomics nomogram in predicting ALNM in young onset breast cancer patients. The nomogram effectively integrates clinical and radiomic data to provide a predictive tool (Figure 4A). Calibration curves for both the training set (Figure 4B) and validation set (Figure 4C) show that the nomogram is well-calibrated, indicating its predictions closely match the observed outcomes. This consistency across both datasets underscores the nomogram’s reliability and potential utility in clinical settings, offering a robust method for personalized risk assessment in young onset breast cancer patients. Figure 5 showcases a decision curve analysis (DCA) which confirms that the clinical-radiomics nomogram delivers higher net benefits across various threshold probabilities than standard models.
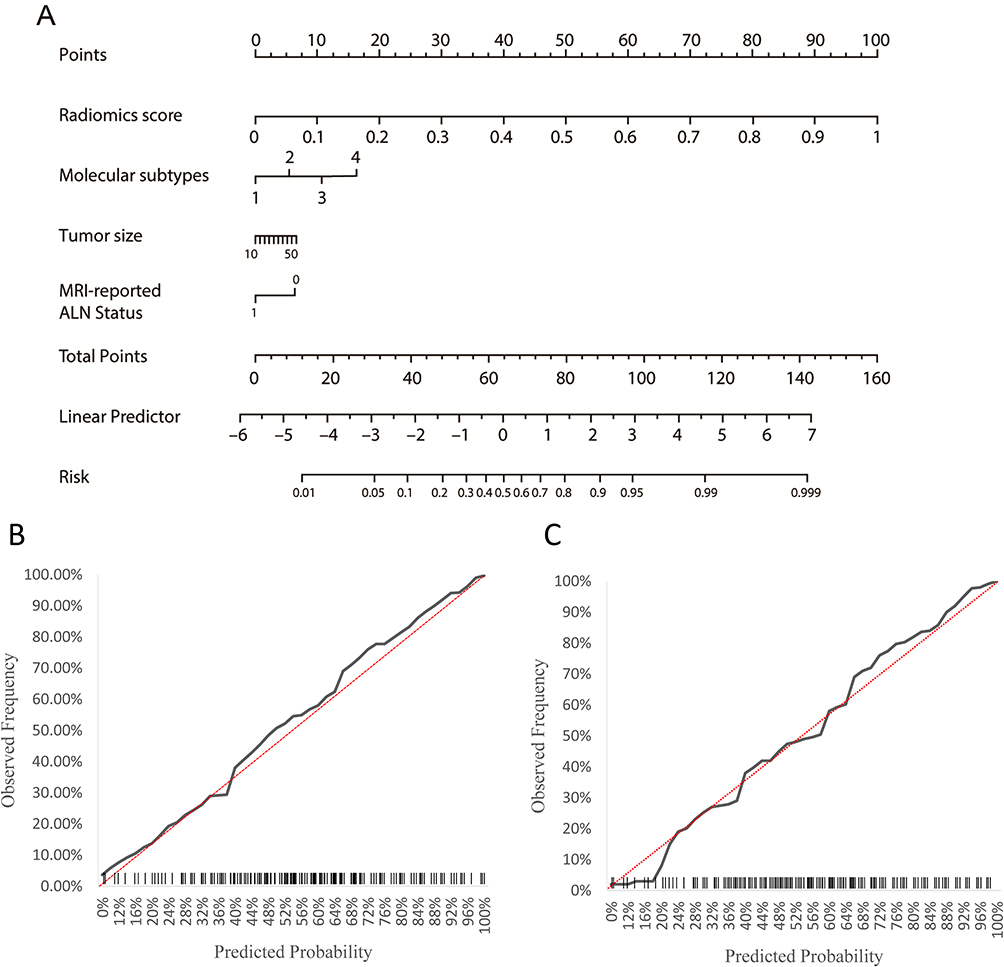 |
Figure 4 Clinical-Radiomics Nomogram and Calibration Curves. The clinical-radiomics nomogram developed for predicting axillary lymph node metastasis in young onset breast cancer patients (A). In the molecular subtypes section, 1, 2, 3, and 4 represent Luminal A, Luminal B, HER2-enriched, and Triple-negative subtypes, respectively. Calibration curves of the clinical-radiomics nomogram in the training set (B) and validation set (C). |
 |
Figure 5 Decision curves were plotted for the clinical model and clinical-radiomics model. The blue line represents the radiomics model, the red line represents the clinical model, and the gray line represents the scenario where all patients are assumed to have the condition. The x-axis indicates the threshold probability, a patient’s risk level at which the expected benefit of treatment equals the expected harm. The y-axis shows the net benefit, calculated by weighing the true positives against the consequences of false positives. |
Discussion
The ability to accurately predict ALNM in young onset breast cancer patients is crucial, given its direct impact on staging, treatment decisions, and prognosis.9,10 For this demographic, characterized by aggressive tumor characteristics and poorer outcomes compared to later-onset cases, early identification of nodal involvement can guide therapeutic strategies, potentially altering the extent of surgical intervention and the need for systemic therapies.11,12 Therefore, enhancing the accuracy of ALNM prediction is paramount for optimizing treatment plans and improving survival rates.
Our study introduced a clinical-radiomics nomogram that integrates DCE-MRI-derived radiomic features with traditional clinical predictors, aimed at refining the prediction of ALNM. The model was rigorously tested across a training set and an independent validation cohort, where it demonstrated high predictive accuracy, reflected by substantial AUC values. The effectiveness of this model underscores the benefits of incorporating radiomic analysis, which extracts a vast array of quantitative data from imaging, into clinical predictive models. This integration offers a more nuanced understanding of tumor behavior, beyond what can be gleaned from traditional imaging assessments alone.13,14
Each predictor included in the nomogram—multifocality, molecular subtypes, tumor size, and MRI-reported ALN status—carries distinct clinical significance. Multifocality suggests a disseminated tumorigenic process within the breast, often correlating with a higher likelihood of systemic spread.15 Different molecular subtypes of breast cancer respond differently to treatment and have varied prognostic outcomes, with some subtypes such as HER2-enriched and triple-negative being associated with a higher propensity for lymphatic spread.16,17 Tumor size has long been recognized as a critical factor in cancer staging; larger tumors have a higher chance of metastasizing due to their increased likelihood of acquiring mutations that facilitate invasion and metastasis.18 MRI-reported ALN status provides a visual assessment of nodal involvement, which can preempt the need for invasive biopsy procedures if predictive accuracy is high.19
The role of radiomics in enhancing ALNM prediction has been increasingly documented. Studies have highlighted how radiomic features can reveal subtle patterns in tissue architecture that are not detectable by the naked eye, providing predictive insights that surpass traditional imaging methods.20,21 These findings suggest that radiomics could play a transformative role in how breast cancer is assessed, moving towards more data-driven, precision-based approaches.
In comparison to existing methods, such as ultrasound-based prediction models, DCE-MRI offers superior soft tissue contrast and spatial resolution, which are advantageous for detecting subtle changes in axillary lymph nodes.22 Ultrasound-based studies have provided valuable insights into ALNM prediction by correlating nodal size, cortical thickness, and vascular patterns with metastatic involvement.23,24 However, these methods are often limited by operator dependency and lower reproducibility compared to radiomics. Incorporating DCE-MRI-derived radiomic features, as demonstrated in our study, offers a more standardized and comprehensive approach, leveraging the wealth of quantitative data extracted from imaging to enhance predictive accuracy. Several studies have also explored the use of ultrasound and radiomic features in predicting ALNM, highlighting their potential in clinical practice. For instance, recent ultrasound-based models have shown promise in identifying nodal metastases but lack the advanced analytical capabilities of radiomics in capturing tumor heterogeneity and microenvironmental features.25 Our study advances this field by specifically tailoring the predictive model to young-onset breast cancer patients, addressing the unique challenges posed by this subgroup.
Despite these advancements, our study has limitations. Notably, the lack of direct pathological correlation in our analysis is a significant constraint, as histological validation remains the gold standard for confirming nodal metastases. Additionally, this study’s retrospective design and confinement to a single institution limit its broader applicability. To address these limitations, future research should focus on multicentric and prospective validations to confirm and possibly enhance the nomogram’s predictive power across diverse populations. The integration of genomic data and other emerging biomarkers into the nomogram could offer deeper insights into the mechanisms driving lymph node metastasis, potentially improving predictive accuracy and clinical utility.26
In summary, our clinical-radiomics nomogram represents a significant step forward in personalizing the management of young onset breast cancer. It provides a scientifically validated, non-invasive tool that enhances the prediction of ALNM, enabling more precise and tailored treatment strategies. This approach not only improves clinical decision-making but also holds the potential to significantly impact patient outcomes by aligning treatment with individual risk profiles, thus embodying the principles of precision medicine in oncology.
Data Sharing Statement
Data are available from the authors upon reasonable request.
Ethics Approval and Informed Consent
This study complies with the principles outlined in the Declaration of Helsinki. It was exempt from ethics approval and patient informed consent due to its non-interventional design and the use of anonymized data, as approved by the Ethics Committee of Shanxi Bethune Hospital.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas, took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Heer E, Harper A, Escandor N, Sung H, McCormack V, Fidler-Benaoudia MM. Global burden and trends in premenopausal and postmenopausal breast cancer: a population-based study. Lancet Glob Health. 2020;8(8):e1027–e1037. doi:10.1016/S2214-109X(20)30215-1
2. He TC, Li JA, Xu ZH, et al. Biological and clinical implications of early-onset cancers: a unique subtype. Crit Rev Oncol Hematol. 2023;190:104120. doi:10.1016/j.critrevonc.2023.104120
3. Yang C, Dong J, Liu Z, et al. Prediction of metastasis in the axillary lymph nodes of patients with breast cancer: a radiomics method based on contrast-enhanced computed tomography. Front Oncol. 2021;11:726240. doi:10.3389/fonc.2021.726240
4. Terada K, Kawashima H, Yoneda N, et al. Predicting axillary lymph node metastasis in breast cancer using the similarity of quantitative dual-energy CT parameters between the primary lesion and axillary lymph node. Jpn J Radiol. 2022;40(12):1272–1281. doi:10.1007/s11604-022-01316-8
5. Yao J, Zhou W, Zhu Y, Zhou J, Chen X, Zhan W. Predictive nomogram using multimodal ultrasonographic features for axillary lymph node metastasis in early‑stage invasive breast cancer. Oncol Lett. 2024;27(3):1–13. doi:10.3892/ol.2024.14228
6. Siddig A, Tengku Din TADAA, Mohd Nafi SN, Yahya MM, Sulong S, Wan Abdul Rahman WF. The unique biology behind the early onset of breast cancer. Genes. 2021;12(3):372. doi:10.3390/genes12030372
7. Nalepa J, Ribalta Lorenzo P, Marcinkiewicz M, et al. Fully-automated deep learning-powered system for DCE-MRI analysis of brain tumors. Artif Intell Med. 2020;102:101769. doi:10.1016/j.artmed.2019.101769
8. Satake H, Ishigaki S, Ito R, Naganawa S. Radiomics in breast MRI: current progress toward clinical application in the era of artificial intelligence. Radiol Med. 2022;127(1):39–56. doi:10.1007/s11547-021-01423-y
9. Lee SY, Yoo TK, Kim J, et al. Characteristics and risk factors of axillary lymph node metastasis of microinvasive breast cancer. Breast Cancer Res Treat. 2024;206(3):495–507. doi:10.1007/s10549-024-07305-x
10. Xiong J, Zuo W, Wu Y, et al. Ultrasonography and clinicopathological features of breast cancer in predicting axillary lymph node metastases. BMC Cancer. 2022;22(1):1155. doi:10.1186/s12885-022-10240-z
11. Basmadjian RB, Chow K, Kim D, et al. The association between early-onset diagnosis and clinical outcomes in triple-negative breast cancer: a systematic review and meta-analysis. Cancers. 2023;15(7):1923. doi:10.3390/cancers15071923
12. Rosa ML, Reinert T, Pauletto MM, Sartori G, Graudenz M, Barrios CH. Implications of tumor-infiltrating lymphocytes in early-stage triple-negative breast cancer: clinical oncologist perspectives. Transl Breast Cancer Res. 2024;5:4. doi:10.21037/tbcr-23-43
13. Horvat N, Papanikolaou N, Koh DM. Radiomics beyond the hype: a critical evaluation toward oncologic clinical use. Radiol Artif Intell. 2024;6(4):e230437. doi:10.1148/ryai.230437
14. Grimm LJ. Radiomics: a primer for breast radiologists. J Breast Imaging. 2021;3(3):276–287. doi:10.1093/jbi/wbab014
15. Tong Y, Sun F, Zhang C, Yang S, Yu Z, Zhao Y. Multifocal/multicentric breast cancer: does each focus matter? Cancer Med. 2023;12(7):8815–8824. doi:10.1002/cam4.5626
16. Hung SK, Yang HJ, Lee MS, et al. Molecular subtypes of breast cancer predicting clinical benefits of radiotherapy after breast-conserving surgery: a propensity-score-matched cohort study. Breast Cancer Res. 2023;25(1):149. doi:10.1186/s13058-023-01747-9
17. Adrada BE, Moseley TW, Kapoor MM, et al. Triple-negative breast cancer: histopathologic features, genomics, and treatment. Radiographics. 2023;43(10):e230034. doi:10.1148/rg.230034
18. Meti N, Saednia K, Lagree A, et al. Machine learning frameworks to predict neoadjuvant chemotherapy response in breast cancer using clinical and pathological features. JCO Clin Cancer Inform. 2021;5:66–80. doi:10.1200/CCI.20.00078
19. Chen ST, Lai HW, Chang JHM, et al. Diagnostic accuracy of pre-operative breast magnetic resonance imaging (MRI) in predicting axillary lymph node metastasis: variations in intrinsic subtypes, and strategy to improve negative predictive value-an analysis of 2473 invasive breast cancer patients. Breast Cancer. 2023;30(6):976–985. doi:10.1007/s12282-023-01488-9
20. Feretzakis G, Juliebø-Jones P, Tsaturyan A, et al. Emerging trends in AI and radiomics for bladder, kidney, and prostate cancer: a critical review. Cancers. 2024;16(4):810. doi:10.3390/cancers16040810
21. Najjar R. Redefining radiology: a review of artificial intelligence integration in medical imaging. Diagnostics. 2023;13(17):2760. doi:10.3390/diagnostics13172760
22. Zheng B, Chen Q. Novel model based on ultrasound predict axillary lymph node metastasis in breast cancer. BMC Med Imaging. 2023;23(1):135. doi:10.1186/s12880-023-01090-7
23. Shao H, Sun Y, Na Z, et al. Diagnostic value of applying preoperative breast ultrasound and clinicopathologic features to predict axillary lymph node burden in early invasive breast cancer: a study of 1247 patients. BMC Cancer. 2024;24(1):112. doi:10.1186/s12885-024-11853-2
24. Duan Y, Zhu Y, Nie F, et al. Predictive value of combining clinicopathological, multimodal ultrasonic characteristics in axillary lymph nodal metastasis burden of patients with cT1-2N0 breast cancer. Clin Hemorheol Microcirc. 2022;81(3):255–269. doi:10.3233/CH-221398
25. Yao Q, Du Y, Liu W, et al. Improving prediction accuracy of residual axillary lymph node metastases in node-positive triple-negative breast cancer: a radiomics analysis of ultrasound-guided clip locations using the SHAP method. Acad Radiol. 2024. doi:10.1016/j.acra.2024.10.039
26. Zeng X, Shi G, He Q, Zhu P. Screening and predicted value of potential biomarkers for breast cancer using bioinformatics analysis. Sci Rep. 2021;11(1):20799. doi:10.1038/s41598-021-00268-9
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.