Back to Journals » Infection and Drug Resistance » Volume 16
Predicting Antibiotic Resistance in ICUs Patients by Applying Machine Learning in Vietnam
Authors Tran Quoc V ![]() , Nguyen Thi Ngoc D
, Nguyen Thi Ngoc D ![]() , Nguyen Hoang T
, Nguyen Hoang T ![]() , Vu Thi H, Tong Duc M
, Vu Thi H, Tong Duc M ![]() , Do Pham Nguyet T, Nguyen Van T
, Do Pham Nguyet T, Nguyen Van T ![]() , Ho Ngoc D
, Ho Ngoc D ![]() , Vu Son G, Bui Duc T
, Vu Son G, Bui Duc T ![]()
Received 5 April 2023
Accepted for publication 16 August 2023
Published 22 August 2023 Volume 2023:16 Pages 5535—5546
DOI https://doi.org/10.2147/IDR.S415885
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Suresh Antony
Viet Tran Quoc,1 Dung Nguyen Thi Ngoc,2,3 Trung Nguyen Hoang,4 Hoa Vu Thi,4 Minh Tong Duc,4 Thanh Do Pham Nguyet,2 Thanh Nguyen Van,5 Diep Ho Ngoc,2 Giang Vu Son,6 Thanh Bui Duc7
1Intensive Care Unit, Military Hospital 175, Ho Chi Minh City, Vietnam; 2Department of Military Science and Training, Military Hospital 175, Ho Chi Minh City, Vietnam; 3Hanoi University of Public Health, Hanoi, Vietnam; 4Department of Military Hygiene, Vietnam Military Medical University, Hanoi, Vietnam; 5Department of General Planning, Military Hospital 175, Ho Chi Minh City, Vietnam; 6Department of Personnel, Military Hospital 175, Ho Chi Minh City, Vietnam; 7Institute of Trauma and Orthopedics, Military hospital 175, Ho Chi Minh City, Vietnam
Correspondence: Thanh Bui Duc, Military Hospital 175, 786 Nguyen Kiem, 3 Ward, Go Vap District, Ho Chi Minh City, Vietnam, Tel +84 975 430 258, Email [email protected]
Introduction: Artificial Intelligence (AI) and machine learning (ML) are used extensively in HICs to detect and control antibiotic resistance (AMR) in laboratories and clinical institutions. ML is designed to predict outcome variables using an algorithm to enable “machines” to learn the “rules” from the data. ML is increasingly being applied in intensive care units to identify AMR and to assist empiric antibiotic therapy. This study aimed to evaluate the performance of ML models for predicting AMR bacteria and resistance to antibiotics in two Vietnamese hospitals.
Patients and Methods: A cross-sectional study combined with retrospective was conducted from 1st January 2020 to 30th June 2022. Five models were developed to predict antibiotic resistance of bacterial infections of ICU patients. Two datasets were prepared to predict AMR bacteria and antibiotics with ML models. The performance of the prediction models was evaluated by various indicators (sensitivity, specificity, precision, accuracy, F1-score, PRC, AuROC, and NormMCC) to determine the optimal time point for data selection. Python version 3.8 was used for statistical analyses.
Results: The accuracy, F1-score, AuROC, and normMMC of LightGBM, XGBoost, and Random Forest models were higher than those of other models in both datasets. In both datasets 1 and 2, accuracy, F1-score, AuROC and normMCC of the XGBoost model were the highest among five models (from 0.890 to 1.000). Only Random Forest models had specificity scores higher than 0.850. High scores of sensitivity, accuracy, precision, F1-score, and normMCC indicated that the models were making accurate predictions for datasets 1 and 2.
Conclusion: XGBoost, LightGBM, and Random Forest were the best-performed machine learning models to predict antibiotic resistance of bacterial infections of ICUs patients using the patients’ EMRs.
Keywords: antibiotic resistance, machine learning, XGBoost, LightGBM, random forest
Introduction
Antibiotic resistance (AMR) is one of ten major global health challenge facing both high-income countries (HICs) and low- and middle-income countries (LMICs).1 Two main factors, included the inappropriate use of antibiotics in the community and the misprescription of broad-spectrum antibiotics in health-care settings, are contributing to the development of AMR.2,3 In hospitals, intensive care units (ICUs), where the mortality rate of infections could be as high as 80%, and the overuse of antibiotics is common, are the greatest threat of AMR.4 In previous study conducted in 1265 ICUs from 75 countries, nearly half of the patients admitted to these units found hospital-acquired infections.5 In Vietnam, a high incidence of nosocomial infections and AMR were found among hospitalized patients, especially in ICUs.6–8 Antibiotic susceptibility tests in hospitals usually require 36–72 hours for sample cultivation and identification of bacteria.9 Therefore, ICU physicians often prescribe antibiotics for prophylaxis based on their experience and the patient’s clinical symptoms rather than laboratory test results as known as empiric therapy.10 However, during empiric therapy, two main types of errors might occur, including the prescription of inefficient antibiotics and the prescription of antibiotics with coverage that is too broad.
In recent years, artificial Intelligence (AI) and machine learning (ML) are used extensively in HICs to detect and control AMR in laboratories and clinical institutions.11 ML is designed to predict outcome variables using an algorithm to enable “machines” to learn the “rules” from the data.12–14 The parameters of the models are first customized with a training dataset and then applied to the test dataset to evaluate the prediction performance.14 ML is increasingly being applied in ICUs to identify AMR and to assist empiric antibiotic therapy. In a review of 60 clinical decision support systems using machine learning, 24 systems (or 40%) were applied in ICUs for diagnosing or treating infectious diseases.12 However, few studies have been conducted in LMICs using ML to detect AMR and prescribe antibiotics in ICUs.11
The present study used electronic medical records (EMR) of ICU patients at Phu Tho Hospital and Military Hospital 175 (Vietnam). Then, different machine learning algorithms were used to develop AMR prediction models of target bacteria for the most frequently used antibiotic families in AST results in two Vietnamese hospitals. This study aimed to evaluate the performance of ML models for predicting AMR bacteria and resistance to antibiotics in two Vietnamese hospitals. Findings from this study are expected to assist clinicians in making better choices of empiric antibiotic therapy for ICU patients in Vietnam and other LMICs.
Materials and Methods
Study Area
The study was implemented at Phu Tho Hospital (Phu Tho province) and 175 Hospital (Ho Chi Minh City) in Vietnam. These two hospitals were selected based on purposive sampling. Phu Tho Hospital is a provincial-level hospital, whereas 175 Hospital is a central level hospital. The first one is in a rural, mountainous, and midland province; the second is in an urban, populated, and delta city in Vietnam.
Study Design
This study applied the retrospective cross-sectional design. The data were extracted from the EMRs of patients admitted to the ICUs of Phu Tho Hospital and 175 Hospital in Vietnam between January 1st, 2020, and June 30th, 2022. The criteria for selection were the medical records of all patients who were 18 years of age or older on admission (in 175 Hospital) or at the time of taking the AST test (in Phu Tho Hospital) and had positive bacterial cultures.
Data Collection
We retrieved EMRs of patients who had positive bacterial culture results from the ICUs in Phu Tho Hospital (Phu Tho province) and Military Hospital 175 (Ho Chi Minh City) in Vietnam between January 1st, 2020, and June 30th, 2022. The total of 3326 specimens were positive for bacteria in the two hospitals (1121 in Phu Tho Hospital and 2205 in Military Hospital 175). After checking for duplicates, 2432 specimens, of which 856 were from Phu Tho Hospital, and 1576 were from Military Hospital 175, were included in the final data analysis of the present study. 1625 medical records were collected, of which 643 were from Phu Tho Hospital and 982 from Military Hospital 175. The patients from both hospitals were 1296 people, including 600 patients in Phu Tho Hospital and 696 in Military Hospital 175.
The demographic and clinical information (age, gender, place of residence (province and town/district), occupation, having insurance or not, diagnosis at admission by the International Code of Diseases (ICD-10), dates of admission and discharge, treatment results, and complication) were collected from the patient’s medical history.
Antimicrobial Resistance Patterns of Isolated Bacteria
Different types of specimens, such as blood, cerebrospinal fluid (CSF), tracheobronchial/bronchoalveolar fluid, urine, skin/wound/tissue specimens, catheters, pleural and peritoneal fluid, were collected and used for the Antimicrobial Susceptibility Testing (AST). The antibiotic susceptibility of isolated bacteria was detected by VITEK 2 Compact System (bioMérieux) at the Testing Center in Phu Tho Hospital and BD Phoenix 100 system (Becton Dickinson, USA) at the Department of Microbiology in the Military Hospital 175. All tests were standardized and performed following the criteria of the Clinical and Laboratory Standards Institute (CLSI).15
Development and Evaluation of ML Models
At first, all input data were preprocessed to be compatible with machine learning models by addressing issues of variations in data format and high dimensionality. The data, then, were split into a training set (80% of the data) to fit the model to the data and a testing set (20% of the data) to evaluate the model’s ability to predict new data accurately, using k-fold cross-validation.16 The training set was used to fit the model to the data, while the test set was used to evaluate the model’s ability to predict new data accurately. This process helps to prevent overfitting, where the model is overly tailored to the training data and may not generalize extensively to new data. In the present study, we developed five models using five supervised ML algorithms, including regularized logistic regression (Ridge logistic regression), adaptive boosting decision trees (AdaBoost), random forest, XGBoost, and LightGBM.
Development and evaluation of a predictive model were performed on a three-phase process. The initial phase determined the presence of five targeted bacterial strains. The second phase predicted the top six antibiotic families most used in AST tests and prescriptions in the hospital, specifically, aminoglycosides, fluoroquinolones, polymyxins, carbapenem, fourth-generation cephalosporin, and trimethoprim derivatives. Finally, the combination of bacterial strains and the corresponding antibiotic resistance profiles were identified.
Eleven combinations were selected based on the prevalence of antibiotics used in AST and the resistance level of each kind of bacteria, including (i) four bacteria against aminoglycosides (Klebsiella spp, Pseudomonas aeruginosa, Escherichia, Staphylococcus aureus), (ii) one bacterium against polymyxins (Klebsiella spp), (iii) one bacterium against fluoroquinolones (Staphylococcus aureus), (iv) one bacterium against carbapenems (Escherichia coli), (v) two bacteria against fourth-generation cephalosporin (Escherichia coli and Pseudomonas aeruginosa), and (vi) two bacteria against trimethoprim derivatives (Staphylococcus aureus and Escherichia coli). Each dataset was run and evaluated for 22 targeted variables (including five bacteria, six antibiotics, and eleven combinations).
The performance of the various machine learning models was evaluated using a range of metrics, including sensitivity, specificity, precision, accuracy, the area under the receiver operating characteristic curve (AuROC), the harmonic mean of precision and recall (F1-score), normalized Matthew Correlation Coefficient (normMCC), Precision–Recall Curve (PRC). For binary classification and imbalanced datasets, norm MCC and PRC are more informative and valuable besides the indicators of accuracy, F1-score, and AuROC Plot. SHAP (SHApley Additive Explanations) package was also used to assess the impact of each feature on the final prediction of the machine learning models. This allowed the contribution of each variable to the model’s output to be determined.
Two datasets were prepared to predict AMR bacteria and antibiotics with ML models. The first dataset (dataset 1) included demographic information, clinical diagnoses, treatment results, and AST results, and complete blood count data. The second dataset (dataset 2) included demographic information, clinical diagnoses, treatment results, and AST results, complete blood count and biochemical data. The performance of the prediction models was evaluated by various indicators (sensitivity, specificity, precision, accuracy, F1-score, PRC, AuROC, and NormMCC) to determine the optimal time point for data selection.17–20 A reference dataset was created by combining the data from Military Hospital 175 and Phu Tho Hospital based on available standard variables.
Statistical Analysis
The data were cleaned and checked for missing values, then reshaped and analyzed using Python 3.8 with various packages, including Pandas, Numpy, Statsmodels, Matplotlib, and Seaborn.
Results
The Performance of the Predictive Model of the Five Targeted Bacteria in the Dataset 1 and Dataset 2
Table 1 presents summary statistics of the datasets used for machine learning predictive models. In the dataset 1 (without biochemical test results), 684 patients were selected. A total of 953 health records, 1537 AST results, and 7538 complete blood tests were included (Table 1). In dataset 2 (with biochemical test results), 560 patients with 755 health records were selected. A total of 1182 AST test, 5924 complete blood count test and 4058 biochemical test results were analyzed (Table 1). In the reference dataset, all patients and health records of two hospitals were included in the predictive models.
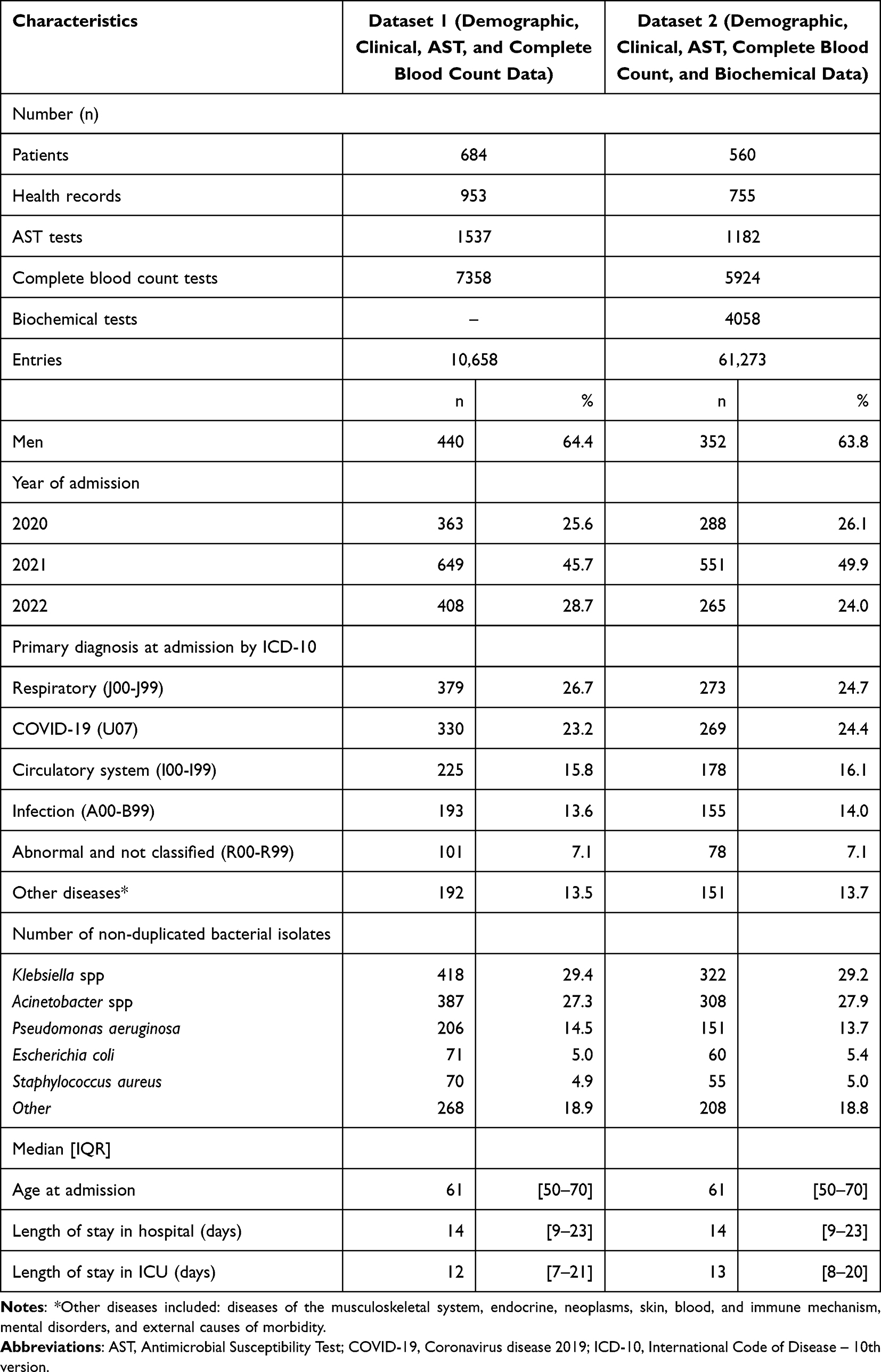 |
Table 1 Description of Datasets Used for Machine Learning Predictive Models |
The sensitivity, specificity, precision, accuracy, F1-score, AuROC, PRC, and normMCC were compared among the five machine learning models in the dataset 1 and dataset 2 and shown in Table 2 and Table 3, respectively. The accuracy, F1-score, AuROC, and normMMC of LightGBM, XGBoost, and Random Forest models were higher than those of other models in both datasets. In both datasets 1 and 2, accuracy, F1-score, AuROC and normMCC of the XGBoost model were the highest among five models (from 0.890 to 1.000). For database 1, XGBoost was the most accurate model in predicting all five targeted bacteria except Pseudomonas aeruginosa (Table 2). Random Forest models gave the highest specificity score for predicting Escherichia coli (0.941) and Staphylococcus aureus (0.932). In dataset 2, the high sensitivity and precision were determined for all the models, but the specificity was still low, particularly for predicting Escherichia coli and Staphylococcus aureus (Table 3). Only Random Forest models had specificity scores higher than 0.850 (Table 3).
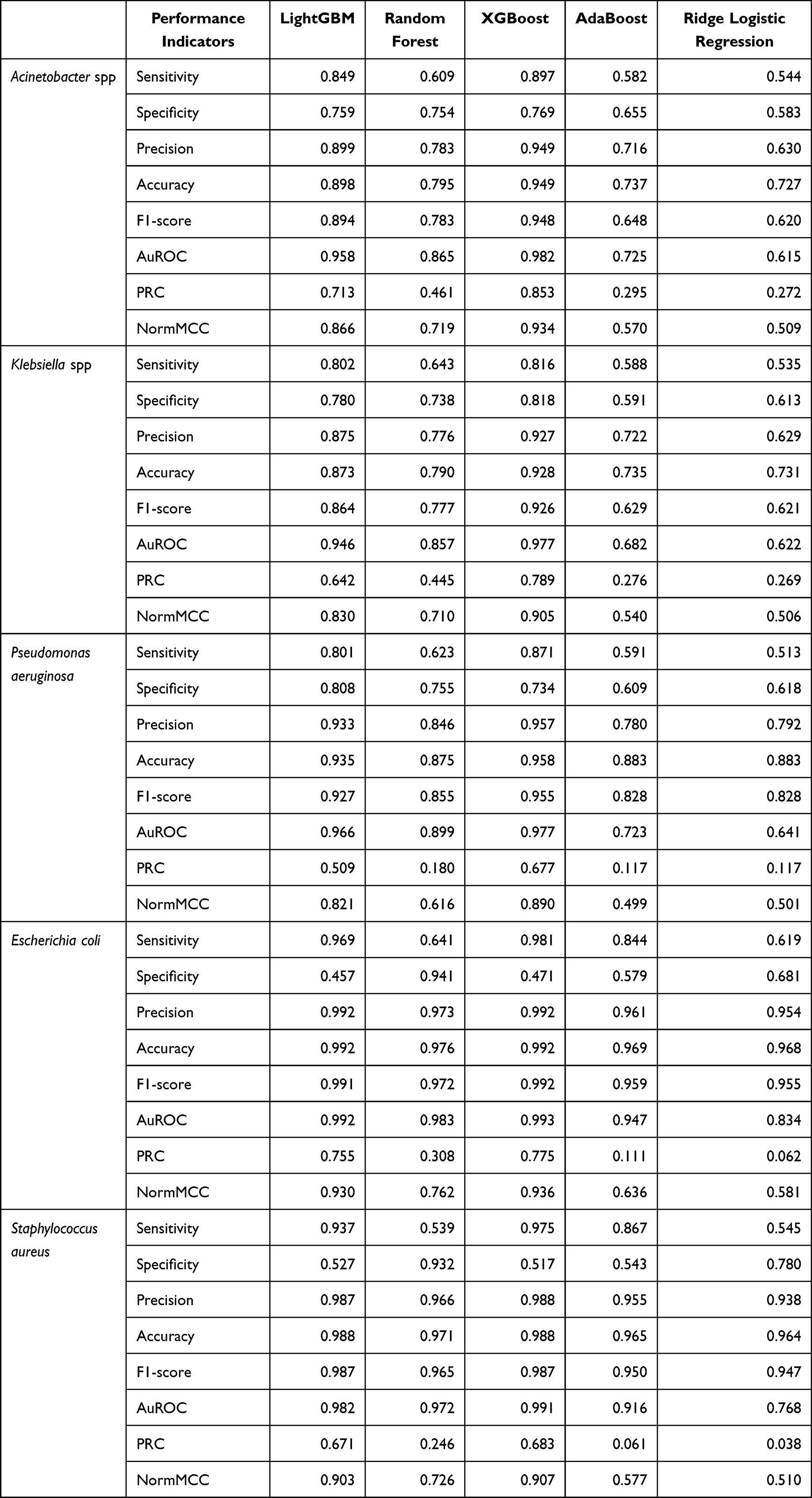 |
Table 2 Comparing the Performance of Different Machine Learning Algorithms on the Dataset 1 |
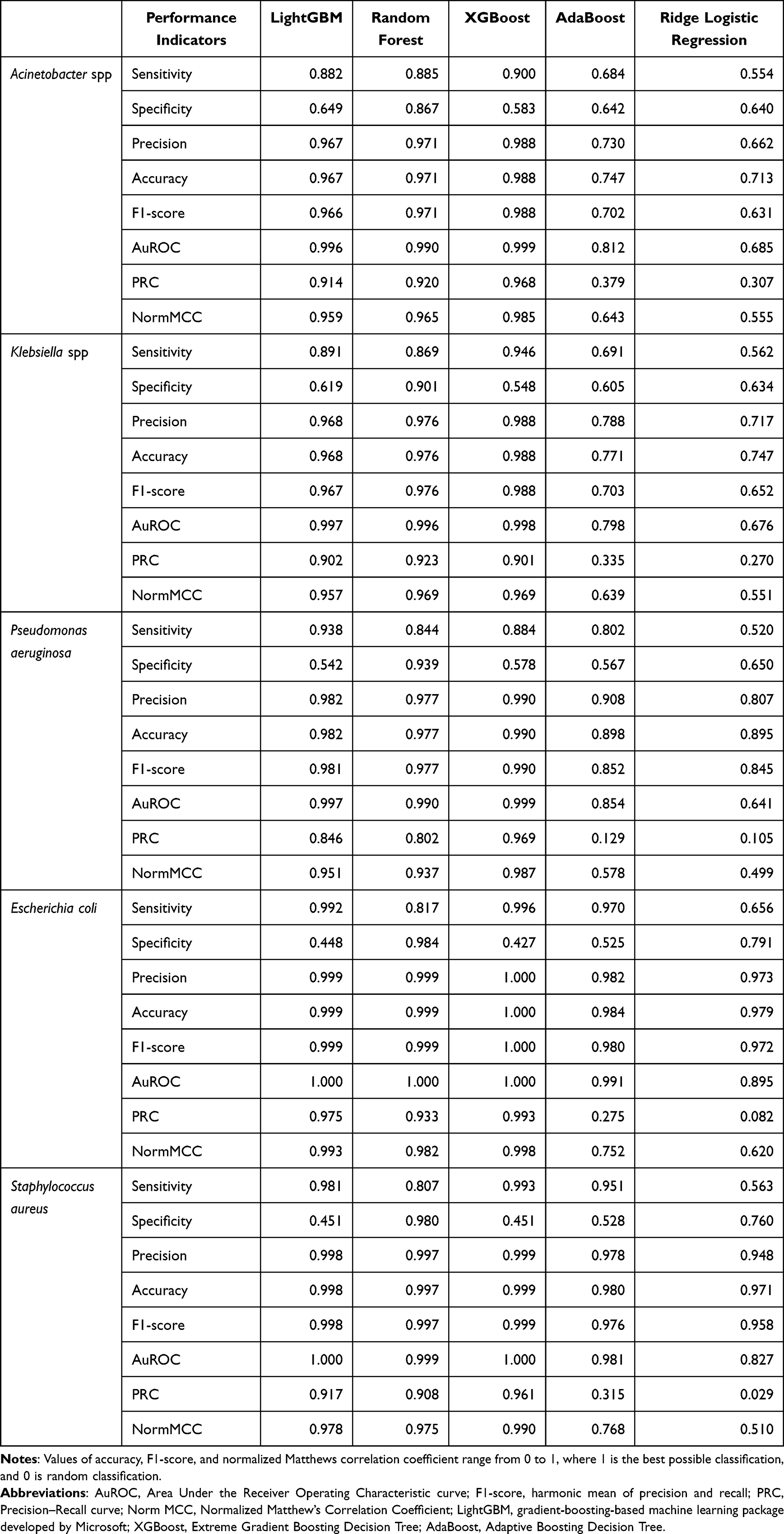 |
Table 3 Comparing the Performance of Different Machine Learning Algorithms on the Dataset 2 |
The Performance of the Predictive Model of the Resistance to Antibiotic Families and Its Combinations of Bacteria
The predictive model of the resistance to antibiotic families was performed with the isolated bacterial species. Overall, high scores of sensitivity, accuracy, precision, F1-score, and normMCC indicated that the models were making accurate predictions for datasets 1 and 2. Tables 4–6 showed the sensitivity, specificity, precision, accuracy, F1-score, AuROC, PRC, and normMCC of the performance of LightGBM model to predict resistance to antibiotic families and the combinations between selected bacteria and antibiotic families in the dataset 1, 2, and reference, respectively.
 |
Table 4 Performance of LightGBM Model (5-Fold Cross-Validation) to Predict Resistance to Antibiotic Families and Between Bacteria and Antibiotic Families in Dataset 1 |
 |
Table 5 Performance of LightGBM Model (5-Fold Cross-Validation) to Predict Resistance to Antibiotic Families and Between Bacteria and Antibiotic Families in Dataset 2 |
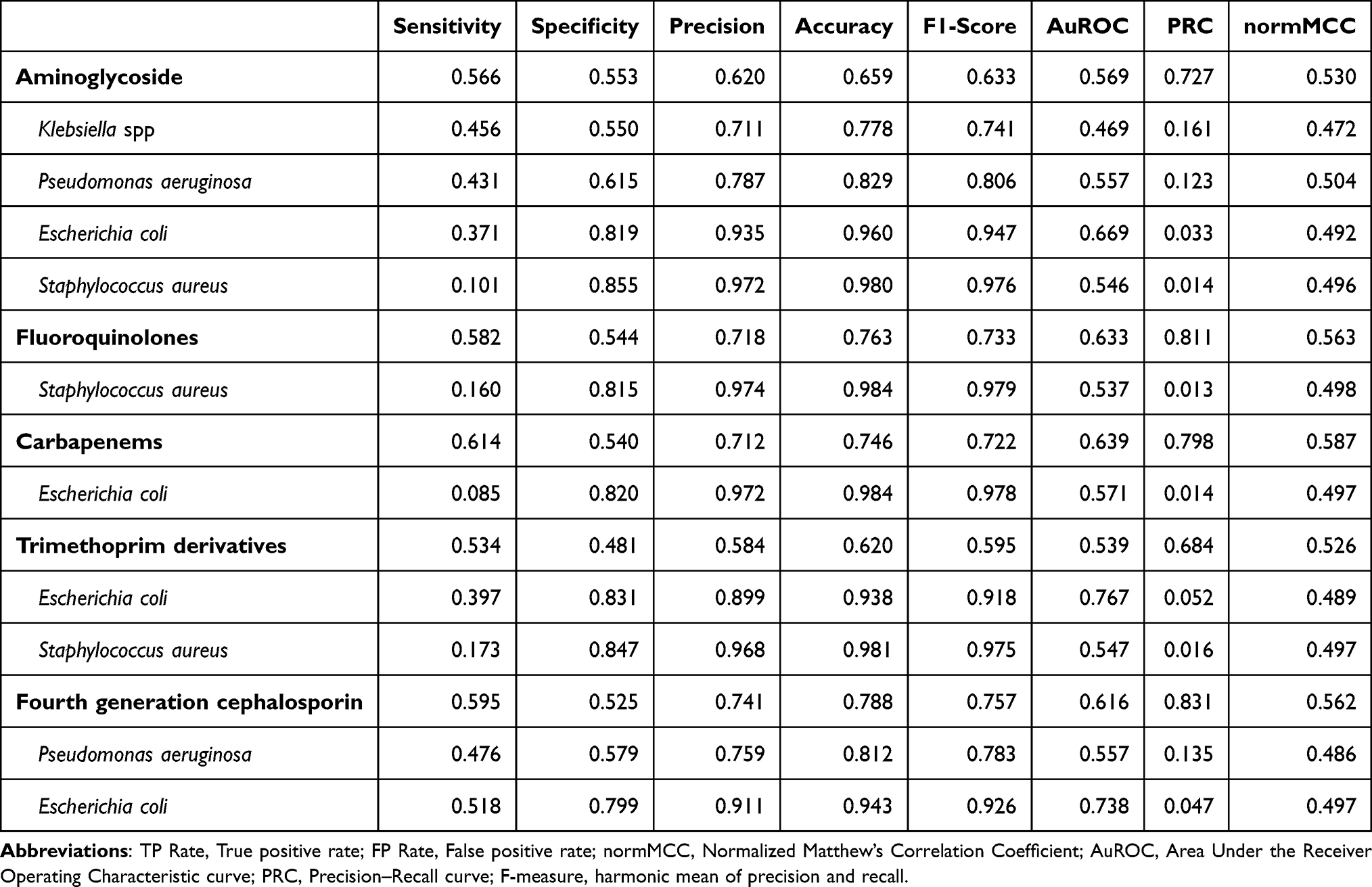 |
Table 6 Performance of LightGBM Model (5-Fold Cross-Validation) to Predict Resistance to Antibiotic Families and Between Bacteria and Antibiotic Families in Reference Dataset |
Discussion
In the present study, we used five machine learning models across three datasets with more than 110 variables to predict the AMR of bacteria and antibiotic families. Although no single model showed superiority for all bacteria or performance metric, the study yielded highly reliable results with AUROC scores of over 0.850 in 3 algorithms LightGBM, XGBoost, and Random Forest, which were higher than the results of the recent studies in Greece and Israel on the prediction of AMR of bacteria, antibiotics, or bloodstream infection.4,21–23 The normMCC value reached above 0.750 for the LightGBM algorithm in predicting bacteria and AMR and predicting combinations of bacteria against antibiotic families. All machine learning models in this study were evaluated using this indicator, which is more reliable and informative than accuracy or F1-score for the binary classification.20 LightGBM model was fast and gave high-performance results,21,24 but its specificity score was not as high as those of other algorithms like Random Forest and XGBoost.
In the two datasets, Random Forest showed the highest specificity results for minority bacterial incidences (Pseudomonas aeruginosa, Escherichia coli, and Staphylococcus aureus). In dataset 2, XGBoost and LightGBM generated results with high sensitivity (0.950) but average specificity (0.650), whereas Random Forest produced high sensitivity and specificity results (0.840 to 0.990). Although no studies on AMR prediction showed the excel of Random Forest in specificity index, the application of k-fold validation when preparing data may have significantly increased accuracy, reliability, and specificity compared to ordinary Random Forest alone.25 The limitations and advantages of the LightGBM, XGBoost, and Random Forest algorithms should be considered in clinical applications and specific cases. The selection of models should depend on whether clinicians prioritize detecting more positive cases or limiting false positives.
Clinical patient evaluation indicators such as Acute Physiology and Chronic Health Evaluation (APACHE II), Simplified Acute Physiology Score (SAP) 3, or indicators of catheter transmission use, surgical, or comorbidities,4,24 were not used in our study. However, the performance of predictive models was still high with dataset 2, which contained complete blood tests and biochemical tests results. This result suggests other hospitals to determine the most appropriate model and indicators for their facilities. In addition, several potentially important predictors for resistance, such as residency location,26 antibiotic use outside the hospital,27–29 microbiome composition, diet, and exercise,30–33 which were not included in the present study, should be consider in future studies.
Limitations
Although the study obtained high-performing machine learning models, some limitations must be addressed. The first limitation was related to the data availability and the period when data were selected. In this study, there was only one hospital with enough data on blood tests and biochemical tests. The extrapolation to other hospitals or other departments should be done with caution. Because the data were collected during the COVID-19 pandemic in Vietnam (from 2020 to 2022), they could be analyzed and interpreted with bias when extrapolated to other periods or hospitals. Furthermore, this study did not distinguish bacterial infections based on the time they occurred after admission, so it was impossible to determine whether the infections were nosocomial. The second limitation was that no algorithm was better than another, and every algorithm had its trade-offs. The results from machine learning will not be optimal and effective without the coordination among clinicians, hematology and biology technicians, and information technology staff. The interdisciplinary collaboration will ensure that professional requirements are evaluated and fully reflected in the choice of algorithms. Lastly, many recommended features in the previous study were not considered, which may influence current output values if included. Machine learning is driven by data; therefore, it is crucial to be cautious and prepare sufficient data for different objects. Data cannot be arbitrarily applied from one department to another, from one hospital to another, or from one group of patients to another without considering scientific evidence and comprehensive protocols.
Conclusion
In the present study, we present machine learning models to predict antibiotic resistance of bacterial infections of ICUs patients using the patients’ EMRs. The best-performed machine learning models were achieved using XGBoost, LightGBM, and Random Forest, and the dataset included complete blood count and biochemical test results (accuracy, F1-score, AUROC, normMCC ≥ 0.90). The performance of machine learning models varied depending on the data set, selected variables, and algorithms.
Research Ethics
The study was approved by the Institutional Research Board of Ethic Committee of the Hanoi University of Public Health (approval number 022-357 DD/YTCC on August 2nd, 2022). The study was conducted based on data on electronic medical records, so the Institutional Research Board of Ethics Committee of the Hanoi University of Public Health did not require the patient’s consent to review their medical records. The patient’s data is confidential, used for research purposes only, and in compliance with the Declaration of Helsinki. All patients were informed and consented to data collection for this study.
Acknowledgments
We thank all the staffs in the Phu Tho Hospital and Military Hospital 175 for supporting the study.
Funding
There was no financial support for the research, and publication of this article.
Disclosure
The authors declare that they have no conflicts of interest for this work.
References
1. Thangaraju P, Venkatesan S. WHO Ten threats to global health in 2019: antimicrobial resistance. Cukurova Med J. 2019;44(3):1150–1151. doi:10.17826/cumj.514157
2. Gebeyehu E, Bantie L, Azage M, Ciccozzi M. Inappropriate use of antibiotics and its associated factors among Urban and Rural Communities of Bahir Dar City Administration, Northwest Ethiopia. PLoS One. 2015;10(9):e0138179. doi:10.1371/journal.pone.0138179
3. Chowdhury AS, Lofgren ET, Moehring RW, Broschat SL. Identifying predictors of antimicrobial exposure in hospitalized patients using a machine learning approach. J Appl Microbiol. 2020;128(3):688–696. doi:10.1111/jam.14499
4. Martinez-Aguero S, Mora-Jimenez I, Lerida-Garcia J, Alvarez-Rodriguez J, Soguero-Ruiz C. Machine learning techniques to identify antimicrobial resistance in the Intensive Care Unit. Entropy. 2019;21(6):603. doi:10.3390/e21060603
5. Vincent JL, Rello J, Marshall J, et al. International study of the prevalence and outcomes of infection in intensive care units. JAMA. 2009;302(21):2323–2329. doi:10.1001/jama.2009.1754
6. Nguyen KV, Thi Do NT, Chandna A, et al. Antibiotic use and resistance in emerging economies: a situation analysis for Viet Nam. BMC Public Health. 2013;13(1):1158. doi:10.1186/1471-2458-13-1158
7. Kinh NV, Wertheim HFL, Thwaites GE, et al. Developing an antimicrobial resistance reference laboratory and surveillance programme in Vietnam. Lancet Glob Health. 2017;5(12):e1186–e1187. doi:10.1016/S2214-109X(17)30370-4
8. Tvd V, Ttn D, Rydell U, et al. Antimicrobial susceptibility testing and antibiotic consumption results from 16 hospitals in Viet Nam: the VINARES project 2012–2013. J Global Antimicrob Resist. 2019;18:269–278. doi:10.1016/j.jgar.2019.06.002
9. Vasala A, Hytonen VP, Laitinen OH. Modern tools for rapid diagnostics of antimicrobial resistance. Front Cell Infect Microbiol. 2020;10:308. doi:10.3389/fcimb.2020.00308
10. Thu TA, Rahman M, Coffin S, Harun-Or-Rashid M, Sakamoto J, Hung NV. Antibiotic use in Vietnamese hospitals: a multicenter point-prevalence study. Am J Infect Control. 2012;40(9):840–844. doi:10.1016/j.ajic.2011.10.020
11. Lv J, Deng S, Zhang L. A review of artificial intelligence applications for antimicrobial resistance. Biosafety and Health. 2021;3(1):22–31. doi:10.1016/j.bsheal.2020.08.003
12. Peiffer-Smadja N, Rawson TM, Ahmad R, et al. Machine learning for clinical decision support in infectious diseases: a narrative review of current applications. Clin Microbiol Infect. 2020;26(5):584–595. doi:10.1016/j.cmi.2019.09.009
13. Anahtar MN, Yang JH, Kanjilal S, McAdam AJ. Applications of machine learning to the problem of antimicrobial resistance: an emerging model for translational research. J Clin Microbiol. 2021;59(7):e0126020. doi:10.1128/JCM.01260-20
14. Deo RC. Machine learning in medicine. Circulation. 2015;132(20):1920–1930. doi:10.1161/CIRCULATIONAHA.115.001593
15. Clinical and Labortory Standard Institute. Performance Standards for Antimicrobial Susceptibility Testing.
16. McHugh ML. Interrater reliability: the kappa statistic. Biochem Med. 2012;22(3):276–282. doi:10.11613/BM.2012.031
17. Oonsivilai M, Mo Y, Luangasanatip N, et al. Using machine learning to guide targeted and locally-tailored empiric antibiotic prescribing in a children’s hospital in Cambodia. Wellcome Open Res. 2018;3:131. doi:10.12688/wellcomeopenres.14847.1
18. Janitza S, Celik E, Boulesteix A. A computationally fast variable importance test for random forests for high-dimensional data. Adv Data Anal Classif. 2018;12(4):885–915. doi:10.1007/s11634-016-0276-4
19. Feretzakis G, Sakagianni A, Loupelis E, et al. Using machine learning to predict antimicrobial resistance of Acinetobacter baumannii, Klebsiella pneumoniae and Pseudomonas aeruginosa strains. Stud Health Technol Inform. 2021;281:43–47. doi:10.3233/SHTI210117
20. Chicco D, Jurman G. The advantages of the Matthews correlation coefficient (MCC) over F1 score and accuracy in binary classification evaluation. BMC Genomics. 2020;21(1):6. doi:10.1186/s12864-019-6413-7
21. Zoabi Y, Deri-Rozov S, Shomron N. Machine learning-based prediction of COVID-19 diagnosis based on symptoms. NPJ Digit Med. 2021;4(1):3. doi:10.1038/s41746-020-00372-6
22. Lewin-Epstein O, Baruch S, Hadany L, Stein GY, Obolski U. Predicting antibiotic resistance in hospitalized patients by applying machine learning to electronic medical records. Clin Infect Dis. 2021;72(11):e848–e855. doi:10.1093/cid/ciaa1576
23. Tzelves L, Lazarou L, Feretzakis G, et al. Using machine learning techniques to predict antimicrobial resistance in stone disease patients. World J Urol. 2022;40(7):1731–1736. doi:10.1007/s00345-022-04043-x
24. Zoabi Y, Kehat O, Lahav D, Weiss-Meilik A, Adler A, Shomron N. Predicting bloodstream infection outcome using machine learning. Sci Rep. 2021;11(1):20101. doi:10.1038/s41598-021-99105-2
25. Adeshina YO, Deeds EJ, Karanicolas J. Machine learning classification can reduce false positives in structure-based virtual screening. Proc Natl Acad Sci U S A. 2020;117(31):18477–18488. doi:10.1073/pnas.2000585117
26. Low M, Neuberger A, Hooton TM, et al. Association between urinary community-acquired fluoroquinolone-resistant Escherichia coli and neighbourhood antibiotic consumption: a population-based case-control study. Lancet Infect Dis. 2019;19(4):419–428. doi:10.1016/S1473-3099(18)30676-5
27. Yelin I, Snitser O, Novich G, et al. Personal clinical history predicts antibiotic resistance of urinary tract infections. Nat Med. 2019;25(7):1143–1152. doi:10.1038/s41591-019-0503-6
28. Costelloe C, Metcalfe C, Lovering A, Mant D, Hay AD. Effect of antibiotic prescribing in primary care on antimicrobial resistance in individual patients: systematic review and meta-analysis. BMJ. 2010;340:c2096. doi:10.1136/bmj.c2096
29. Pouwels KB, Freeman R, Muller-Pebody B, et al. Association between use of different antibiotics and trimethoprim resistance: going beyond the obvious crude association. J Antimicrob Chemother. 2018;73(6):1700–1707. doi:10.1093/jac/dky031
30. Sommer MO, Church GM, Dantas G. The human microbiome harbors a diverse reservoir of antibiotic resistance genes. Virulence. 2010;1(4):299–303. doi:10.4161/viru.1.4.12010
31. Baron SA, Diene SM, Rolain J-M. Human microbiomes and antibiotic resistance. Hum Microbiome J. 2018;10:43–52. doi:10.1016/j.humic.2018.08.005
32. Corpet DE. Antibiotic resistance from food. N Engl J Med. 1988;318(18):1206–1207. doi:10.1056/nejm198805053181818
33. Van TT, Moutafis G, Tran LT, Coloe PJ. Antibiotic resistance in food-borne bacterial contaminants in Vietnam. Appl Environ Microbiol. 2007;73(24):7906–7911. doi:10.1128/AEM.00973-07
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prediction of Acute Kidney Injury in Intracerebral Hemorrhage Patients Using Machine Learning
She S, Shen Y, Luo K, Zhang X, Luo C
Neuropsychiatric Disease and Treatment 2023, 19:2765-2773
Published Date: 11 December 2023
Enhancing Prediction of Myocardial Recovery After Coronary Revascularization: Integrating Radiomics from Myocardial Contrast Echocardiography with Machine Learning
Huang D, Yang X, Ruan H, Zhuo Y, Yuan K, Ruan B, Li F
International Journal of General Medicine 2024, 17:2539-2555
Published Date: 31 May 2024
Early Warning of Axillary Lymph Node Metastasis in Breast Cancer Patients Using Multi-Omics Signature: A Machine Learning-Based Retrospective Study
Ke Z, Shen L, Shao J
International Journal of General Medicine 2024, 17:6101-6114
Published Date: 12 December 2024
Machine Learning Based Prediction of Postoperative Acute Kidney Injury Risk in Coronary Artery Bypass Grafting Patients
Zhang Y, Cai D, Deng Y, Wang Z, Zhang Z, Zhang H, Wang Q, Feng S, Sun L, Wei J
Clinical Interventions in Aging 2025, 20:2033-2048
Published Date: 15 November 2025
Machine Learning Models for Identifying the Risk of Chronic Kidney Disease in Patients with Coronary Heart Disease: A Retrospective Study
He T, Zhao J, Hou L, Su K, Li Y
International Journal of General Medicine 2025, 18:7327-7340
Published Date: 5 December 2025