Back to Journals » Advances in Medical Education and Practice » Volume 13
Preclinical and Clinical Medical Students’ Perception of the Learning Environment: A Reference to the Forensic Medicine and Clinical Toxicology Course
Authors Fayed MM, Abdo SA ![]() , Sharif AF
, Sharif AF ![]()
Received 2 January 2022
Accepted for publication 7 April 2022
Published 23 April 2022 Volume 2022:13 Pages 369—406
DOI https://doi.org/10.2147/AMEP.S354446
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Manar M Fayed,1 Sanaa A Abdo,2 Asmaa F Sharif1
1Forensic Medicine and Clinical Toxicology Department, Faculty of Medicine, Tanta University, Tanta, Egypt; 2Public Health and Community Medicine Department, Faculty of Medicine, Tanta University, Tanta, Egypt
Correspondence: Asmaa F Sharif, Forensic Medicine and Clinical Toxicology Department, Faculty of Medicine, Tanta University, El Geish Street, Tanta, Gharbia, 31527, Egypt, Tel +966581639317, Email [email protected]
Purpose: Understanding learning environments is vital for developing curricula. This study aims to evaluate medical students’ achievements and perception of learning environments considering the Forensic Medicine and Clinical Toxicology course as an analog for the curricular transition process.
Methods: A cross-sectional study was conducted among undergraduate medical students at the Faculty of Medicine, Tanta University, from August 2020 to October 2021. Using the Dundee Ready Education Environment Measure (DREEM) questionnaire, the perception of 621 students (of which 307 were enrolled in the integrated curriculum and 314 in the traditional curriculum) were compared. Furthermore, the appropriate tests of significance and correlations were used to compare students’ perception according to their enrollment, age, gender, and previous year grade point average.
Results: The mean overall DREEM score was 121.04 ± 22.35, implying a more positive than negative learning environment, that is, a more positive learning perception, with students’ perceptions of teachers moving in the right direction, students’ academic self-perceptions getting more on the positive side, more positive attitudes regarding student’s perceptions of the learning environment, and not-too-bad student’s social self-perception. Medical students enrolled in the integrated curriculum showed higher DREEM scores, with significantly better learning and academic self-perceptions (p < 0.05). Knowledgeable, qualified faculties are the most significant characteristic feature in both systems. A significant number of students achieved excellent grades in the integrated curriculum (n = 740 out of 1076, 68.8%) than in the traditional one (n = 470 out of 961, 48.9%) (p < 0.0001).
Conclusion: This study revealed a smooth, successful transition from the traditional to integrated curriculum among Egyptian medical students. The main areas for improvements are focusing on factual teaching, implementing student-centered teaching activities, promoting students’ memorizing, and engaging students in activities that may help them enjoy learning.
Keywords: learning, education, self-perception, achievement, curriculum, competency-based education
Introduction
Learning environment is a collective term that covers every aspect related to a specific educational program. It includes, but is not limited to, teaching strategies, course syllabi, assessment modalities, teaching faculties, and learning resources.1 Students in different learning contexts are influenced by the various learning environments in terms of perception, understanding of learning practices, and achieving learning objectives and planned outcomes.2
Understanding the learning environment is vital for developing curricula. It helps in exploring a program’s strengths that can be capitalize on and in outlining improvement areas for the purpose of reorganization. Questionnaires are among the appropriate methods proposed to explore the learning environment from student perspectives, which aid in optimizing different aspects of the learning context.3
The Dundee Ready Education Environment Measure (DREEM) questionnaire is one of the most valid and reliable recommended tools for assessing learning environments, especially among healthcare professions.4 The DREEM questionnaire assists in describing different learning domains, outlining problematic issues, and solving emerging problems to enhance a learning process’s efficiency. It can be used to compare learning experiences in diverse settings with each other and with ideal ones proposed in similar settings.5
In Egypt, and up to recent years, most medical schools adopted the French model: a 6-year program followed by 1 year of internship. After completion, the graduate earns a Bachelor of Medicine and Surgery (MBBCH) degree. The French model deploys a traditional subject-based, teacher-centered curriculum where all students attend theoretical lectures as one batch and are only divided into subgroups for practical and clinical purposes. The gradual shift toward integrated curricula started in various medical schools in 2009, except for the Suez-Canal University, which started earlier than 2009.6
The Faculty of Medicine, Tanta University, was first established in 1962 and subsequently recognized by the World Directory of Medical Schools. In 2018, major curricular changes were deployed, and the curriculum for the Medicine and Surgery Bachelor Program (MSBP-CB) was changed to the integrated system-based credit point (282 credit hours) system. The MSBP-CB program is divided into three phases: Phase I (basic preparatory modules taught during first and second years), Phase II (preclinical modules taught during the third year), and Phase III (clinical courses taught during the fourth, fifth, and sixth years). Problem-based, student-centered educational approaches with early exposure to some clinical practices were the primary learning strategies that were adopted. Additionally, different levels of integration (vertical and horizontal) were adopted during the program’s different phases.
In the traditional program, the Forensic Medicine and the Clinical Toxicology course is scheduled for the fourth-year students as a clinical course. In the integrated program, despite the clinical nature of the course, it is delivered to second-year students as a means of vertical integration.
Global studies were carried out to address medical students’ perception toward the curricular reform. These studies were carried out in European countries like Sweden,7 in the Middle East like Saudi Arabia and Kuwait and in other developing countries like Chile and Turkey.8–11 To the best our knowledge, although there is a simultaneous change toward the integrated curricula in Egyptian universities, no previous work had been conducted in Egypt that examines medical students’ perception toward these changes in the different learning phases. Therefore, and because of the critical medicolegal importance of the Forensic Medicine and Clinical Toxicology course, our study aims to evaluate medical students’ perception of learning environments wherein the course is delivered in two different learning contexts (traditional subject-based curriculum versus the integrated system-based curriculum). Moreover, this study aims to compare students’ achievements in the MBBCH program—where the course is taught in clinical phases—with the integrated MSBP-CB program—where the same course is delivered in basic phases.
Materials and Methods
Study Design and Setting
This research is a cross-sectional study that was conducted among two cohorts of undergraduate medical students at the Faculty of Medicine, Tanta University, from August 2020 to October 2021.
Sample Size
The total number of students enrolled in traditional and integrated systems was 2037 students (961 enrolled in the MBBCH program and 1076 enrolled in the MSBP-CB program). As the difference in perception of DREEM scale between the two systems was unknown, so considering occurrence equaled no occurrence=50% with a margin of error of 0.04, and confidence level 95%, the sample size has been calculated and it was 464 students. Accounting for a drop-out of 20%, the minimal sample size was estimated to be 557 students. The questionnaire was distributed to all students. Out of them, 715 consented to participate. However, 621 responses were included (distributed as 307 students in the MBBCH program and 314 students in the MSBP-CB program) after excluding incomplete responses with a response rate of 86.9% (621/715).
Participants and Grouping
The study participants were divided into two groups according to their program enrollment. The first group comprised students enrolled in the MBBCH program (traditional curriculum, fourth-year students in the clinical phase), while the second group comprised those in the MSBP-CB program (integrated curriculum, second-year students in the basic phase). Both groups attended lectures on the same campus, and the same instructors provided the same learning material for both groups.
Inclusion Criteria
Students who had completed the Forensic Medicine and Clinical Toxicology course were allowed to participate, provided that they were registered as regular students who successfully completed all previous courses.
Exclusion Criteria
Students who had withdrawn from or were denied exam entry were excluded from the study, and those who did not complete previous years’ modules before joining the course and those with incomplete questionnaires were also excluded.
Ethical Considerations
Data collection commenced after the study was approved by the Research Ethical Committee of the Faculty of Medicine, Tanta University (number 34379/1/21). Following the recommendations of the 1964 Declaration of Helsinki and its subsequent amendments, the collected data and students’ records were handled anonymously to maintain the confidentiality of the participants. Moreover, all participants gave their written informed consent before their inclusion in the study. The students were free to participate. Besides, a statement that clearly stated the study’s objectives and procedures was added at the beginning of the questionnaire.
Data Collection Tools and Instruments
The DREEM Questionnaire
In the final weeks of the semester, after finalizing students’ assessments, they were briefed regarding the contents of the questionnaire and how to fill it. Then, the online questionnaire was distributed as a link through email and paper-based questionnaires were provided to those without email access. Students were briefed on the items and read the questionnaire carefully before responding on a 5-point Likert scale, where responses ranged from strongly agree to strongly disagree. An English version of the questionnaire was adopted given that all students had passed the placement test for language before joining the Faculty of Medicine.
The DREEM questionnaire is a 50-item questionnaire distributed under 5 main domains: Student’s Perceptions of Learning (SPL), Student’s Perceptions of Teachers (SPT), Student’s Academic Self-Perceptions (SAP), Student’s Perceptions of Atmosphere (SPA), and Student’s Social Self-Perception (SSP) as follows:8
- Domain 1: SPL [(items: 1, 7, 13, 16, 20, 22, 24, 25, 38, 44, 47, and 48) 12 items/max score 48].
- Domain 2: SPT [(items: 2, 6, 8, 9, 18, 29, 32, 37, 39, 40, and 50) 11 items/max score 44].
- Domain 3: SAP [items: 5, 10, 21, 26, 27, 31, 41, and 45) 8 items/max score 32].
- Domain 4: SPA [(Items: 11, 12, 17, 23, 30, 33, 34, 35, 36, 42, 43, and 49) 12 items/max score 48].
- Domain 5: SSP [Items: 3, 4, 14, 15, 19, 28, and 46) 7 items/max score 28].
Scoring of the DREEM Questionnaire
All items were scored as follows: 4 for strongly agree, 3 for agree, 2 for uncertain, 1 for disagree, and 0 for strongly disagree. Nine out of the fifty items (items 4, 8, 9, 17, 25, 35, 39, 48, and 50) were scored in negatively: 0 for strongly agree, 1 for agree, 2 for uncertain, 3 for disagree, and 4 for strongly disagree. The overall scoring was interpreted according to McAleer and Roff,9 as follows:
- 0–50: Very poor;
- 51–100: Plenty of problems;
- 101–150: More positive than negative; and
- 151–200: Excellent.
Additionally, each domain was analyzed, and each item’s response was checked to ascertain if they were above 3 and 3.5, which is considered positive, while items sored less than 2 were considered problematic. Items scored between 2 and 3 required educational climate enhancement. After completing the DREEM questionnaire items, the respondents answered questions related to age, gender, and previous years’ grade point averages (GPAs).
Students’ Achievements
The achievements of all students registered in both programs, regardless of their participation in our study, were obtained from the Assessment and Evaluation Center of the Faculty of Medicine, Tanta University. These achievements include the results of summative assessments and the average of formative assessments for every student. Results were categorized as excellent (85–100%), very good (70–84%), good (55–69%), fair (40–54%), fail (<40%), and absent. This grading system is adopted by Tanta University, Faculty of Medicine, and is aligned with General Egyptian Universities Guidelines which might vary between different Egyptian schools and even in the same Faculty running two different programs. Brief modifications were conducted to compare the studied groups using a unified scale.10
Rigor
To ensure robustness of the current study, A pilot study was carried out before starting data collection including 40 participants of the target population with the following objectives:1. to test and evaluate the adequacy of the questionnaire, 2. to estimate the time needed for filling the questionnaire and 3. to determine the potential obstacles that might be met with during execution of the study. Pilot study was carried out using online and paper-based questionnaires.
Feedback of pilot study revealed that no questions have to be added, deleted or rephrased so the tool was adopted as it is. Moreover, the time needed for filling the questionnaire ranged from 15–20 minutes.
To assess reliability, the study tool was tested by the pilot subjects at first session and the calculated Cronbach’s Alpha was 0.831. Moreover, the internal consistency reliability was calculated using Spearman- Brown Prophecy formula (r1=2 (r) /1+r) where r estimated correlation coefficient computed on the split halves and r1 estimated reliability of the entire test and it was 0.814.11 The results of the pilot were included in the final results as there were no changes or modifications done to the tool of the study.
Statistical Data Analysis
Data were analyzed using SPSS version 27 (SPSS Inc., Chicago, IL, USA). Quantitative data were presented as mean ± SD, and qualitative data were presented as frequencies and percentages. The chi-square test and Fischer’s exact test were used to assess associations between qualitative variables, while the Mann–Whitney U-test and the Kruskal–Wallis H-test were conducted to compare the DREEM scores among the different groups. Spearman correlation was used for investigating correlation between the DREEM score and its subscales among the studied groups. A Z-score test was used to compare students’ achievements in the two groups. The level of significance was considered to be P < 0.05.
Results
The DREEM questionnaire was distributed to 2037 medical students (961 enrolled in the MBBCH program and 1076 in the MSBP-CB program). Overall, females (n = 319, 51.4%) slightly outnumbered males (n = 302, 48.6%). However, for those enrolled in the traditional program, males slightly outnumbered females (52.1% and 47.9%, respectively). The age of the included participants ranged from 19 to 24 years, with a mean age of 21.71 ± 5.12 years. Significant variations of the enrolled students in terms of age were noticed, as 97.1% of those enrolled in traditional programs were aged 20 years and above, while 98.4% of students enrolled in the integrated curriculum were aged less than 20 years. Table 1 presents previous years’ GPAs, with no significant variations between the study groups.
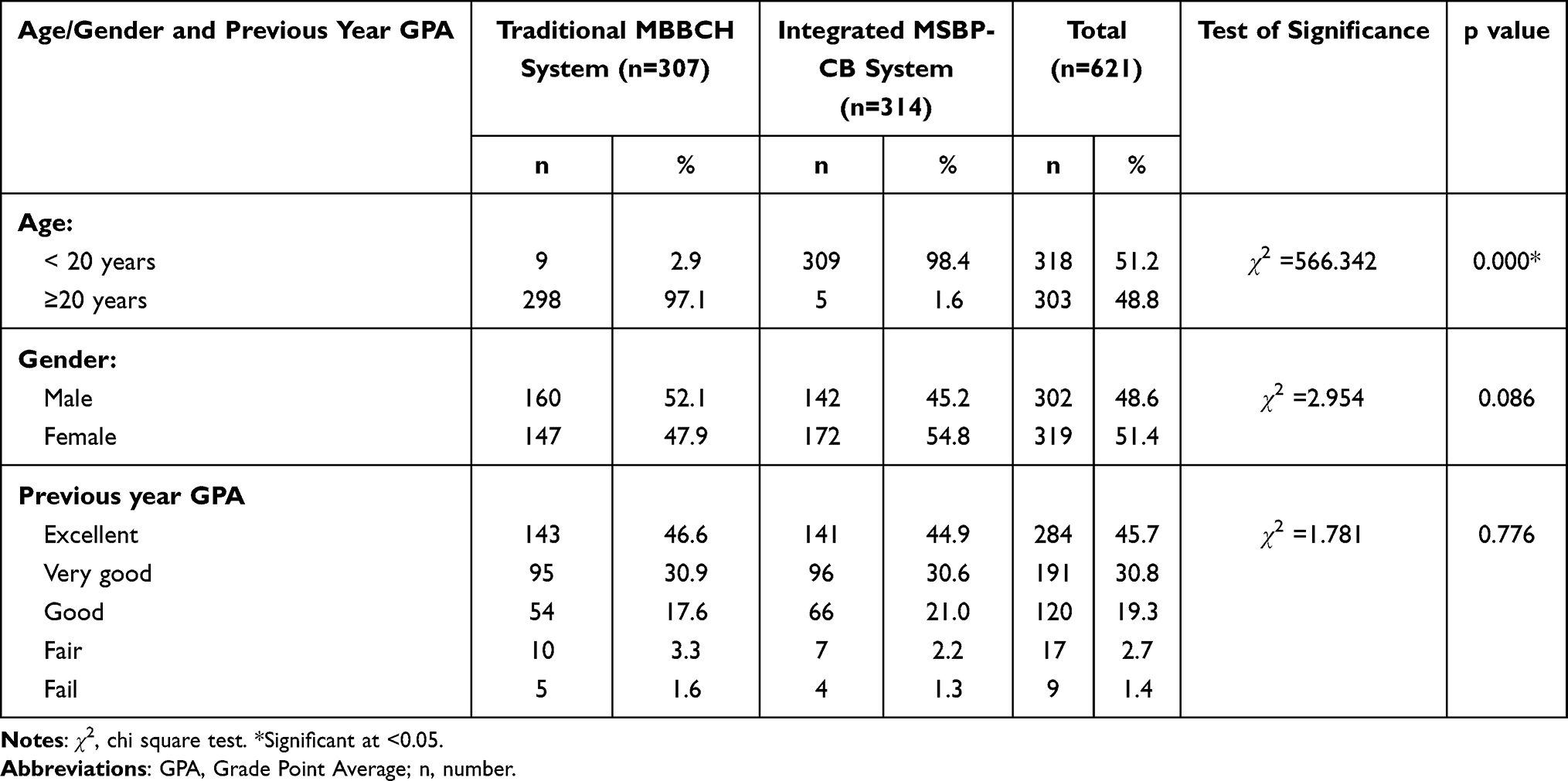 |
Table 1 Demographic and Educational Profiles of the Respondents Who Participated in the Current Study |
As depicted in Table 2 and Figure 1, this study revealed a mean overall DREEM score of 121.04 ± 22.35 among the study participants, implying a more positive than negative learning environment and no difference the type of the program. Regarding DREEM subscales, this study conveys a more positive learning perception, with SPT moving in the right direction, SAPs being more on the positive side, there being more positive attitudes regarding student’s perceptions of the learning environment, and not-too-bad students’ SSP. Students enrolled in the integrated program showed significantly higher means of learning perception and academic self-perceptions (p < 0.05) compared to those enrolled in the traditional program. Table 3 presents the interpretation of the DREEM questionnaire and its subscales in both study groups; as can be seen, there were no significant variations.
 |
Table 2 Comparison Between the Traditional MBBCH and Integrated MSBP-CB Systems Regarding Mean Total DREEM and Its Subscales’ Scores |
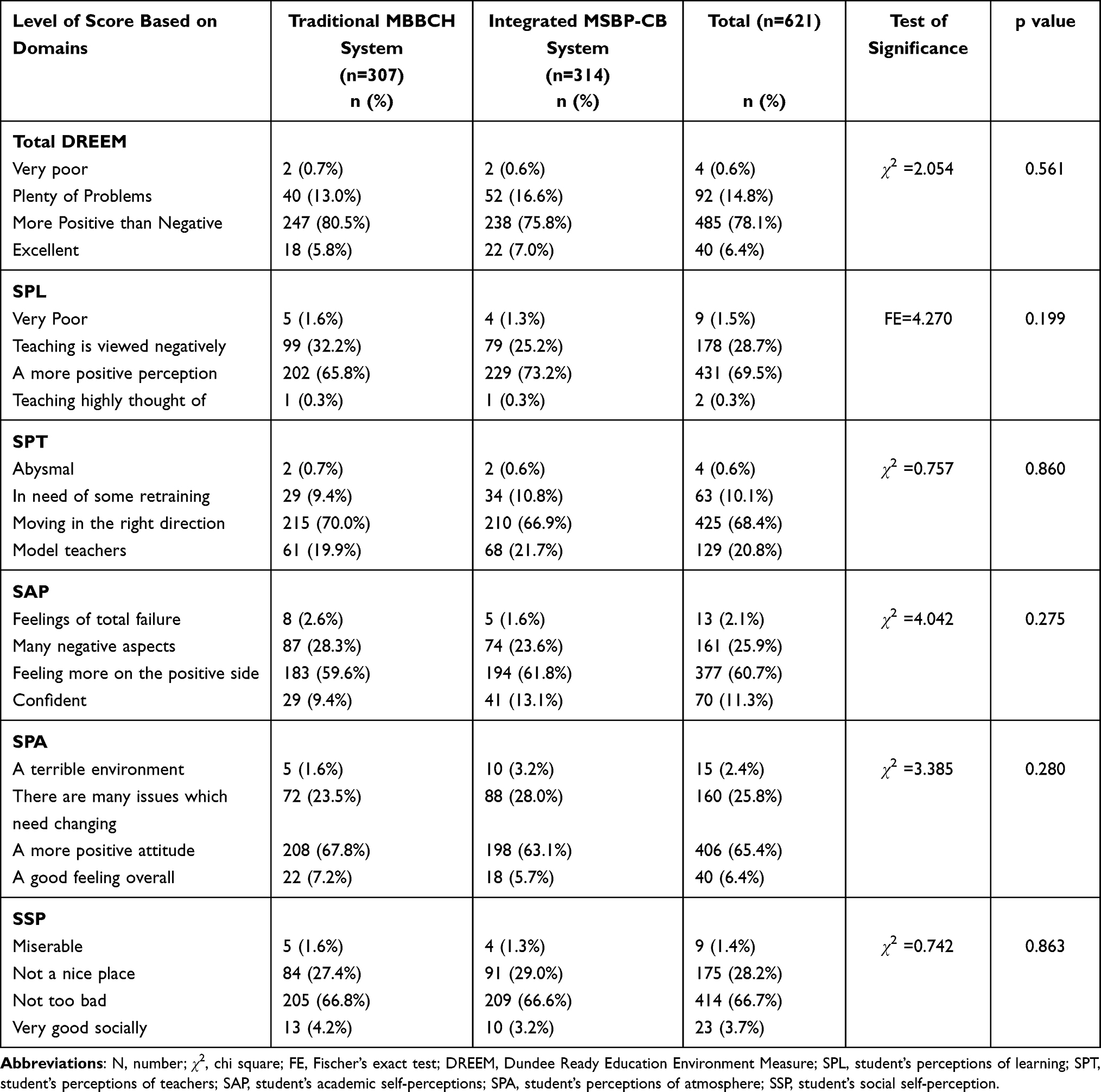 |
Table 3 Level of Scores of the DREEM Inventory and Its Subscales Among Participants Enrolled in Both Systems and Recruited in the Current Study |
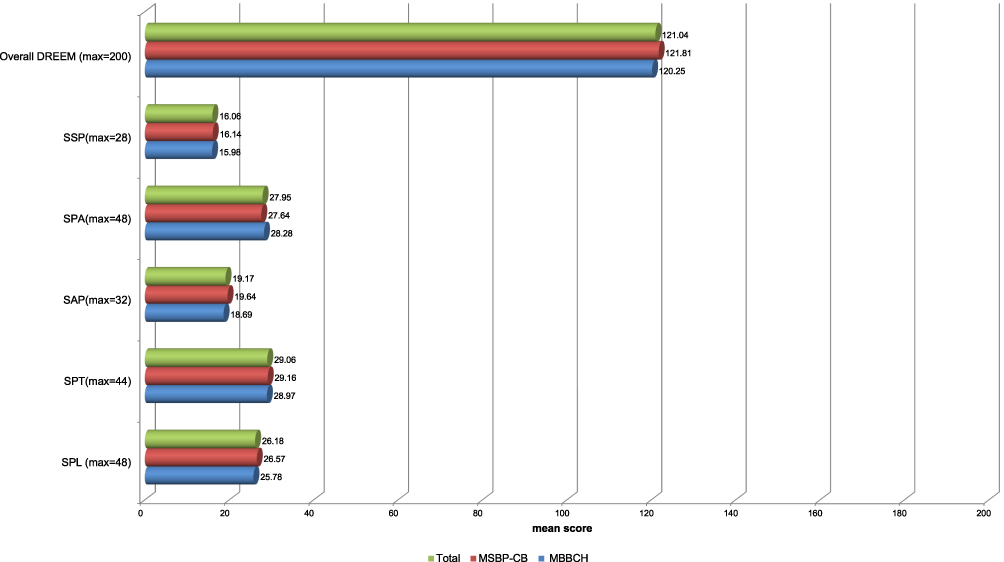 |
Figure 1 Comparing the traditional MBBCH and the integrated MSBP-CB systems regarding mean total DREEM and its subscale scores. |
Examining DREEM subscales on discrete bases yielded valuable findings, as shown in Table 4 and Figure 2. Regarding students’ perceptions of learning, a significant number of students enrolled in the integrated program perceived teaching as more simulating (2.68) than those enrolled in the traditional program (2.51) (p = 0.025). Similarly, a significant number of students enrolled in the integrated program perceived the teaching as less teacher centered compared to those in the traditional program (p = 0.002). Conversely, a significant number of students enrolled in the traditional program showed a better perception of the teaching time as put to good use than integrated program students (p = 0.001).
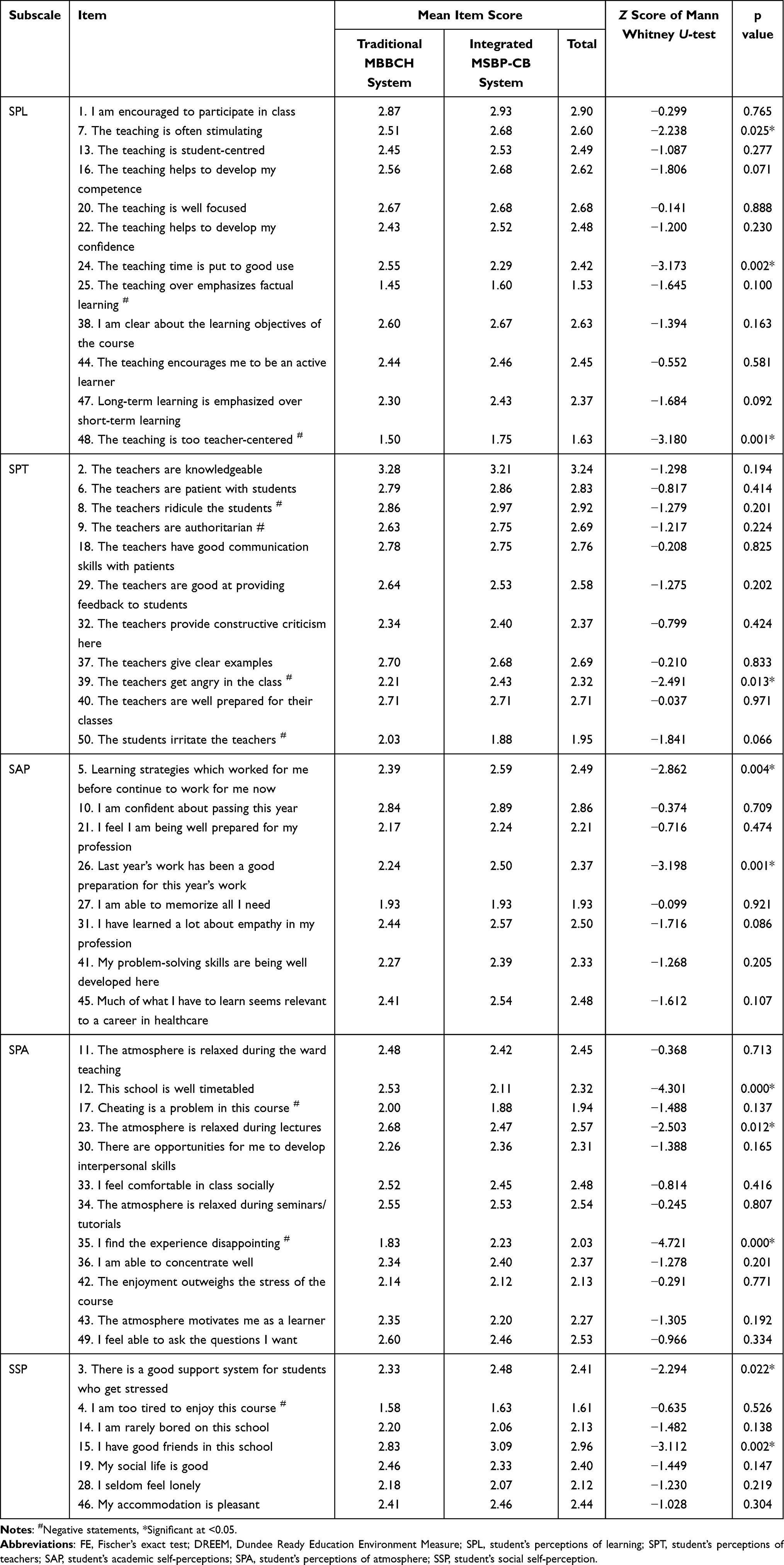 |
Table 4 Comparison Between the Traditional MBBCH and Integrated MSBP-CB Systems Regarding the Mean Item Scores |
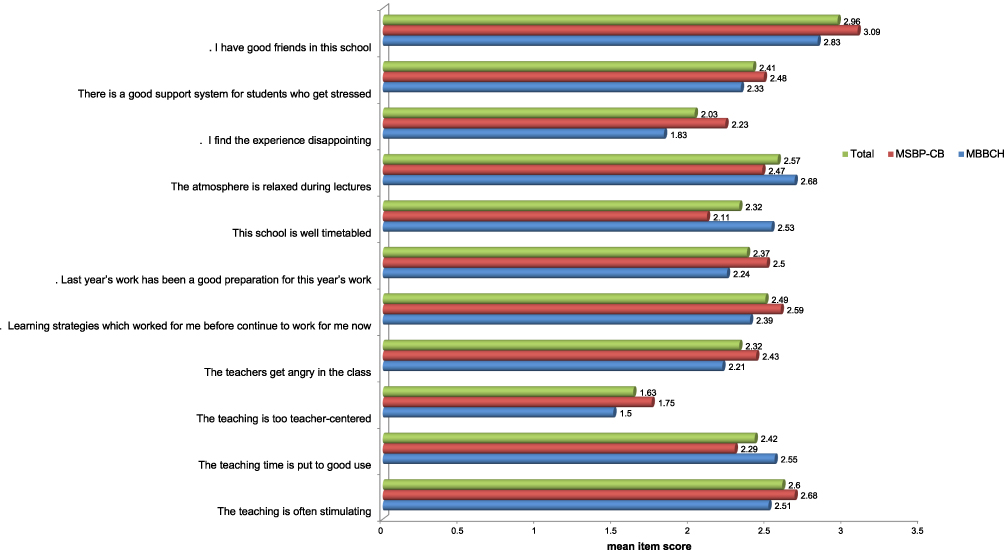 |
Figure 2 Items that differed significantly between the traditional MBBCH and the integrated MSBP-CB systems in terms of mean item scores. |
Concerning students’ perception of teachers, those in the integrated program showed significantly higher mean scores for the item “the teachers get angry in the class” (2.43) than those in the traditional program group (2.21). Significantly better perceptions among students in the integrated program compared to those enrolled in the traditional program were noticed in the academic self-perception and students’ SSP domains. This includes higher mean values of the perception of learning strategies that continue to work, previous years’ proper preparation for the current year, good support systems for stressed students, and making good friends inside the school (p < 0.05). Similarly, the students in the integrated program perceived the learning environment as less disappointing compared to those in the traditional system (mean = 2.23 versus 1.83, respectively). Paradoxically, other items were significantly better perceived by students enrolled in the traditional program compared to those enrolled in the integrated one, which includes a proper timetable and a relaxing atmosphere during lectures (p < 0.05).
Table 5 presents the variations between male and female students’ perceptions of the learning environment in both programs. The overall DREEM scores were higher for females than males; however, the difference was not statistically significant. The mean overall mean DREEM was (122.7 ± 20.4) for females and (119.3 ± 24.1) for males. Among the DREEM subscales, females had higher scores than males enrolled in the same program in all subscales, except for SSP where male had higher mean scores in both groups. However, gender variations were statistically significant (p < 0.05) only in the perceptions of teachers’ domain. Figure 3 highlights these variations.
 |
Table 5 Mean Score of DREEM Inventory and Its Subscales Based on Gender in Both Study Groups |
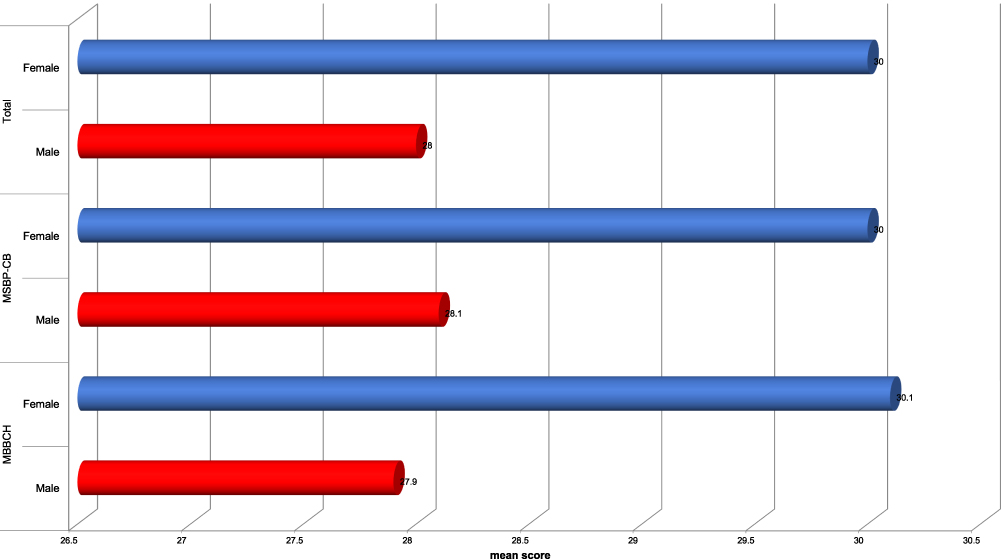 |
Figure 3 Comparing the traditional MBBCH and the integrated MSBP-CB systems regarding the mean student’s perceptions of teacher (SPT) score based on gender. |
Considering the study participants’ age, our study found nonsignificant differences in the overall DREEM scores between the two groups (p > 0.05). However, and as Figure 4 illustrates, younger students aged less than 20 years showed significantly higher SPL mean values (26.5 ± 5.1) compared to students aged 20 years and above (25.8 ± 4.8), (p = 0.012). Conversely, students aged 20 years and above showed higher SPT mean values among those enrolled in the traditional program. Moreover, the mean SAP value was significantly higher in students aged less than 20 years (19.6 ± 4.9) than in older students (18.7 ± 4.7), (p < 0.05), as shown in Table 6.
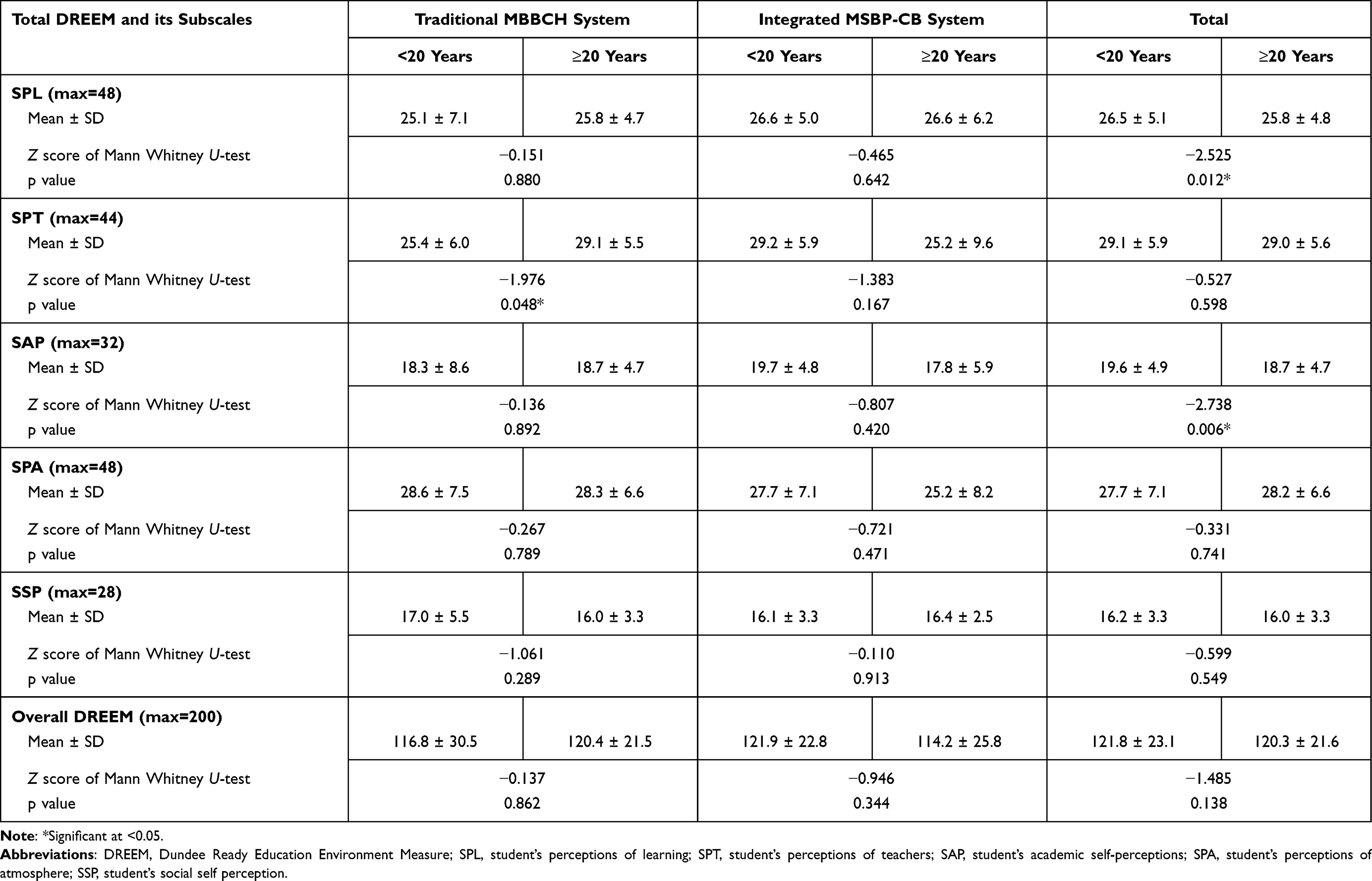 |
Table 6 Mean Score of DREEM Inventory and Its Subscales Based on Age in Both Study Groups |
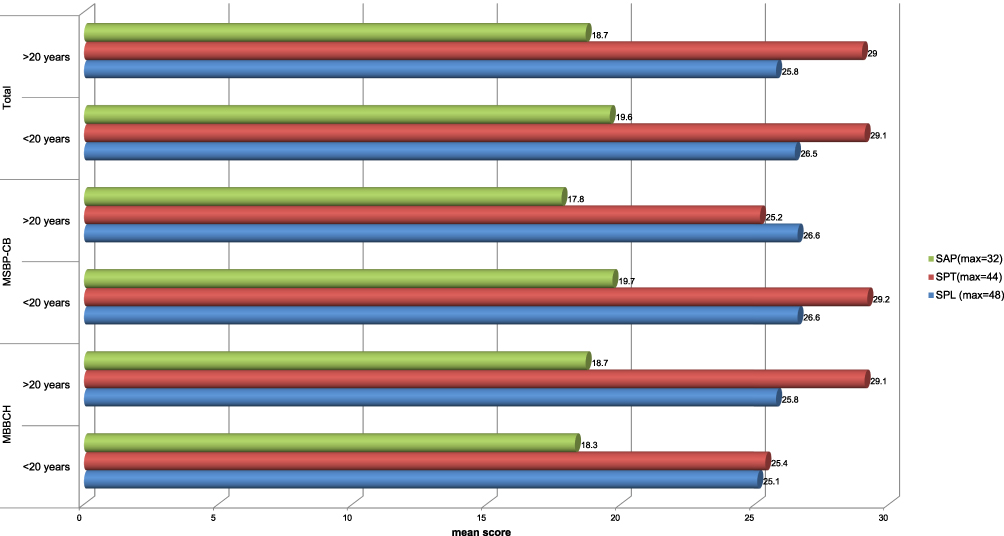 |
Figure 4 Comparing the traditional MBBCH and the integrated MSBP-CB systems regarding the mean scores of SAP, SPT, and SPL based on age. |
Table 7 and Figure 5 show the mean DREEM score and its subscales among participants according to their previous GPAs. Among them, students with higher GPAs (Excellent) showed significantly higher mean values in terms of overall DREEM, SPL, SPT, and SAP scores (p < 0.05). A similar finding had been obtained among students enrolled in the traditional curriculum, where students with higher GPAs (Excellent) showed significantly higher mean values in terms of overall DREEM, SPL, and SPT scores (p < 0.05). The variations in the overall DREEM scores (including those of its subscales) between students enrolled in the integrated curriculum were not statistically significant. Table 8 shows a significant positive correlation between Overall DREEM, SPL, SPT, SAP, SPA and the previous year GPA among students enrolled in the traditional program. Moreover, there was a significant negative correlation between SPL, SAP and students age among all studied participants.
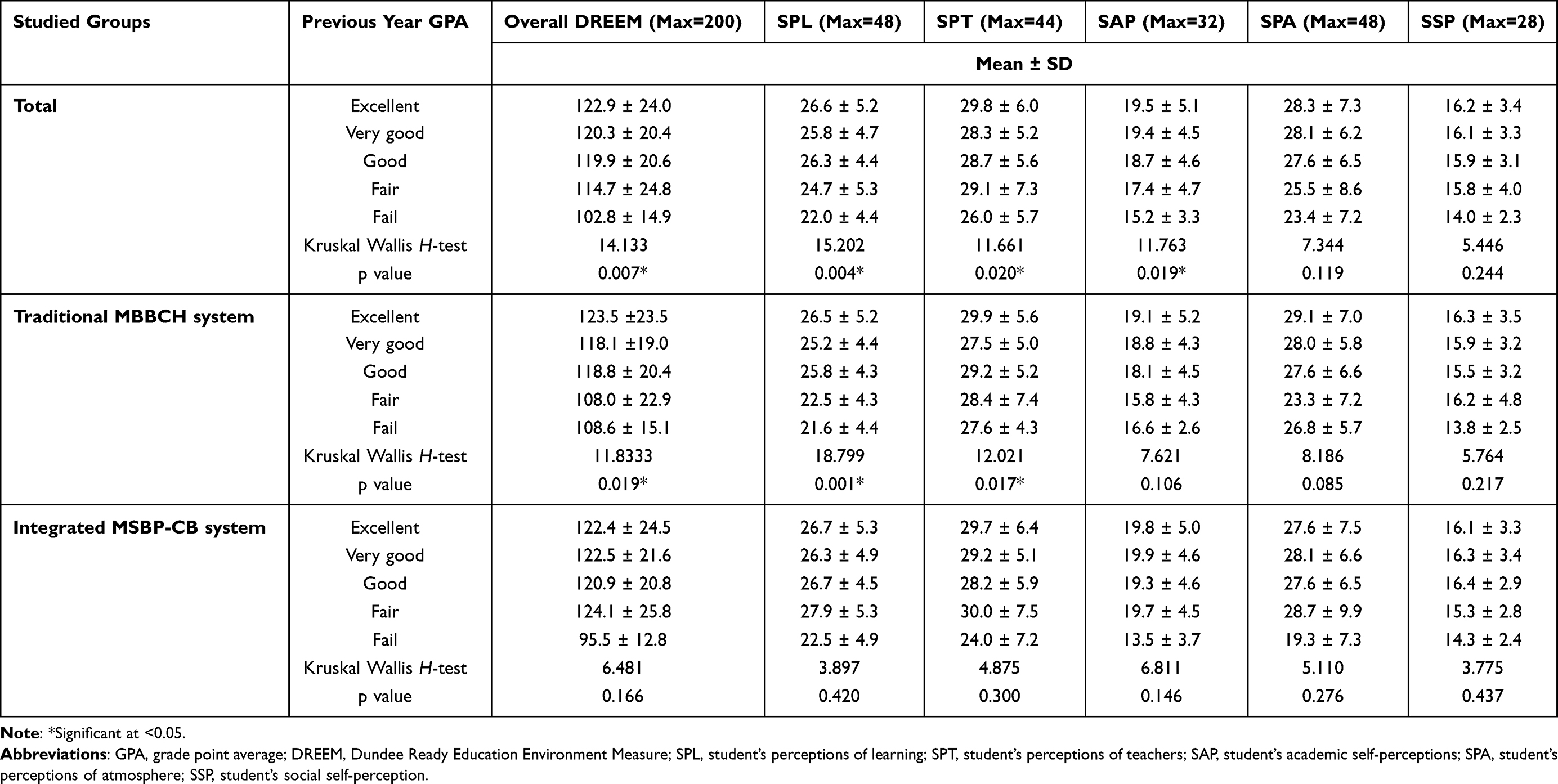 |
Table 7 Mean Score of DREEM Inventory and Its Subscales Based on the Previous Year’s GPA in Both Study Groups |
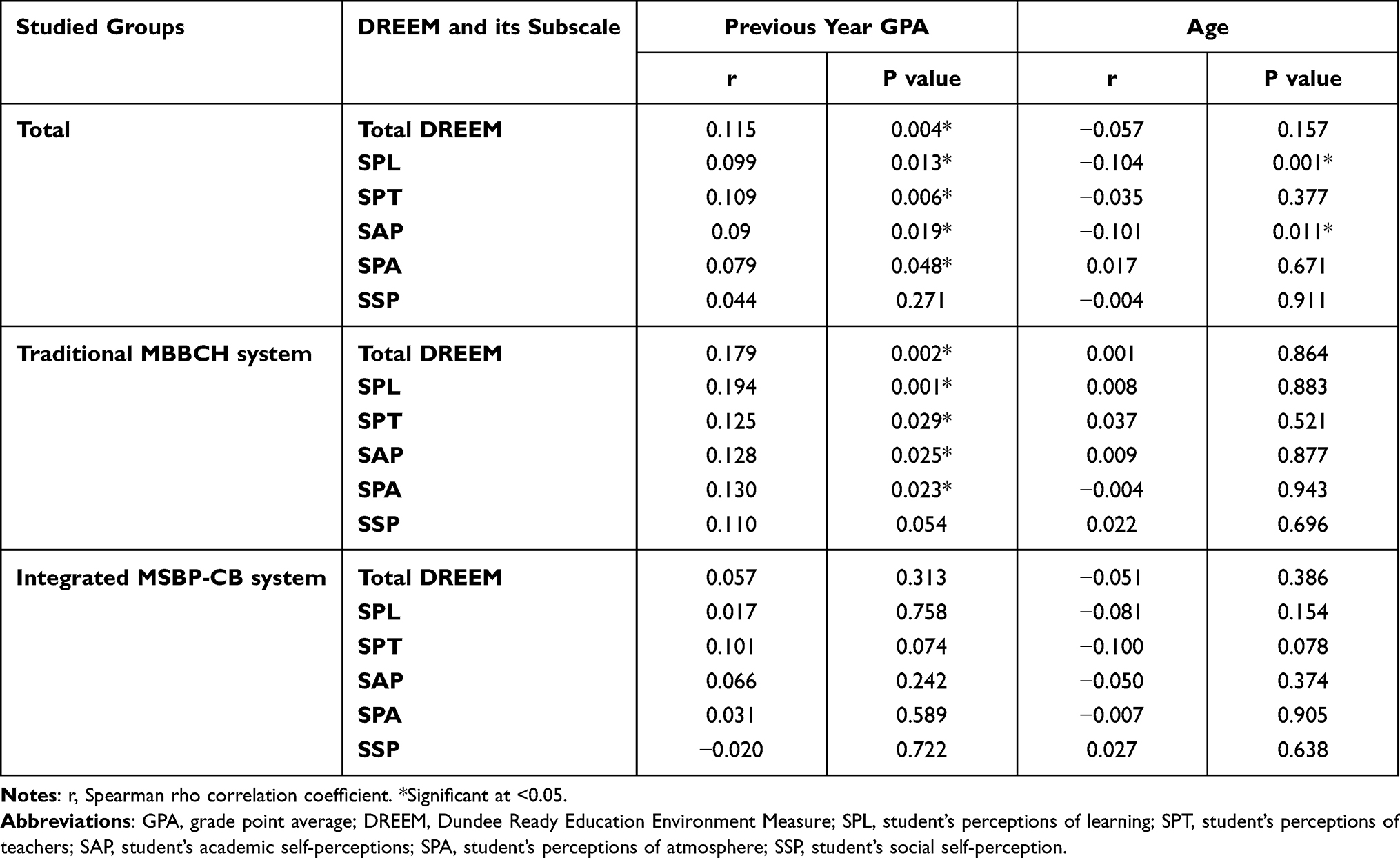 |
Table 8 Correlation Between Score of DREEM and Its Subscales, Age and Previous Year GPA in Both Studied Groups |
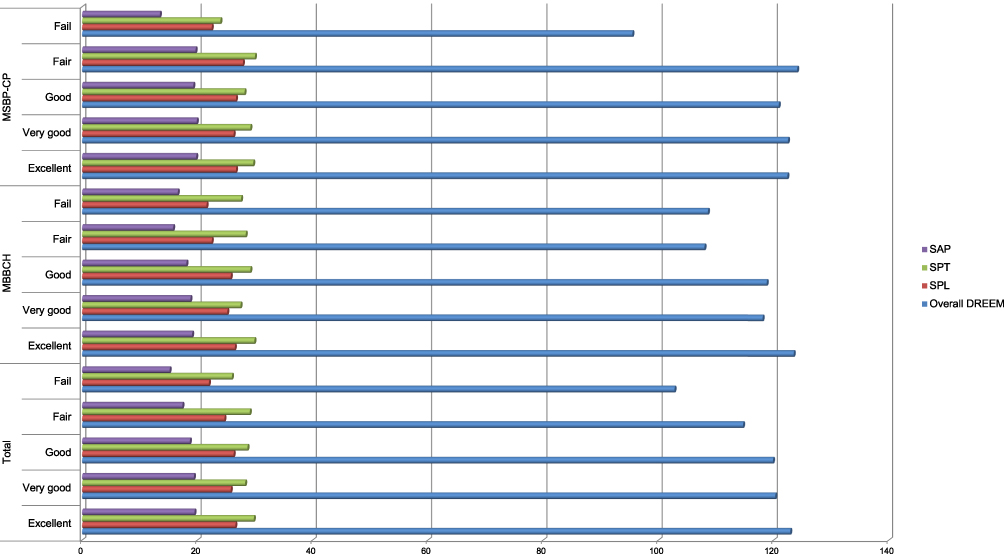 |
Figure 5 Comparing the traditional MBBCH and the integrated MSBP-CB systems regarding the mean score of SAP, SPT, SPL, and overall DREEM based on the previous year’s GPA. |
Table 9 summarizes the areas of weakness and strength between the study groups. Four areas were problematic in both groups: teaching over-emphasizes factual learning, teaching is too teacher centered, I am able to memorize all that I need, and I am too tired to enjoy this course. In the integrated curriculum, two additive items were considered weak areas, including “the students irritate the teachers” and “cheating is a problem in this course.” However, the student’s perception of the atmosphere in a traditional program needs improvement, especially in their evaluation of their learning experience as disappointing. We could not find any items ranked >3.5. However, the highest-ranked item was the students’ perception of teachers, where the mean of the response to the item “the teachers are knowledgeable” was 3.24 out of 4. Centralization of the teaching and feeling disappointing were significantly more reported among students enrolled in traditional program. Table 10 shows moderate to strong positive correlation between Overall DREEM, and its subscales among all students and among every group according to the program of enrollment (p < 0.001).
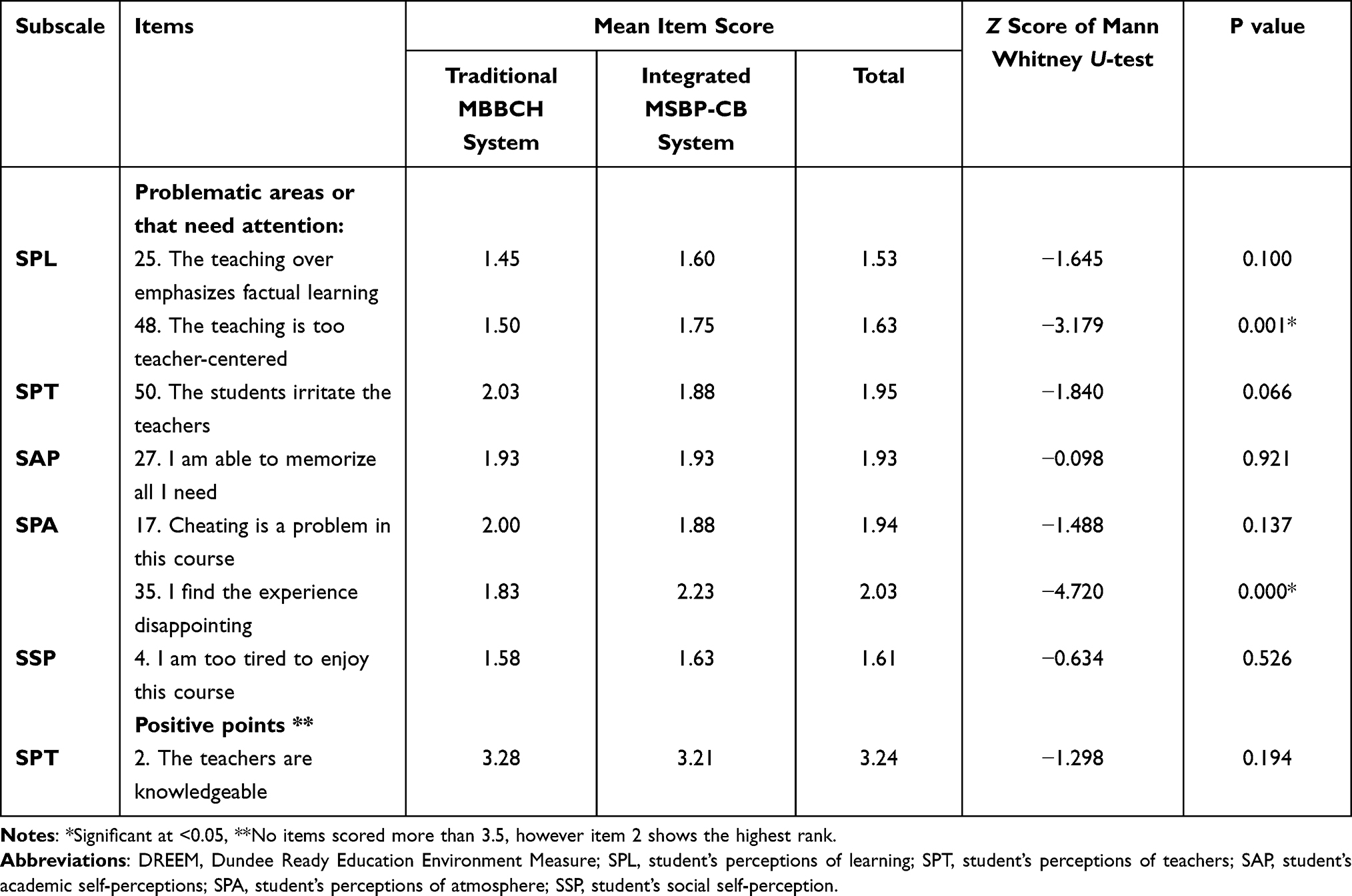 |
Table 9 Positive Points and Problematic Areas in the Learning Environment as Illustrated by the Mean Item Scores |
 |
Table 10 Spearman Correlation Coefficients Between Score of DREEM and Its Subscales, Among Studied Groups |
Regarding students’ performances in both programs, our study revealed a significant finding. As Table 11 and Figure 6 show, a significant number of students in the integrated curriculum achieved excellent grades (n = 740 out of 1076, 68.8%) compared to those in the traditional program (n = 470 out of 961, 48.9%), (p < 0.0001). Comparable proportions of students (25.5% for the traditional program versus 23.7% for the integrated one) got “Very Good” with no significant variations between the study groups (p = 0.4009). However, a significant number of students scored “Good,” “Fair,” “Fail,” and “Absent” among those enrolled in the traditional program, a with p values of <0.001.
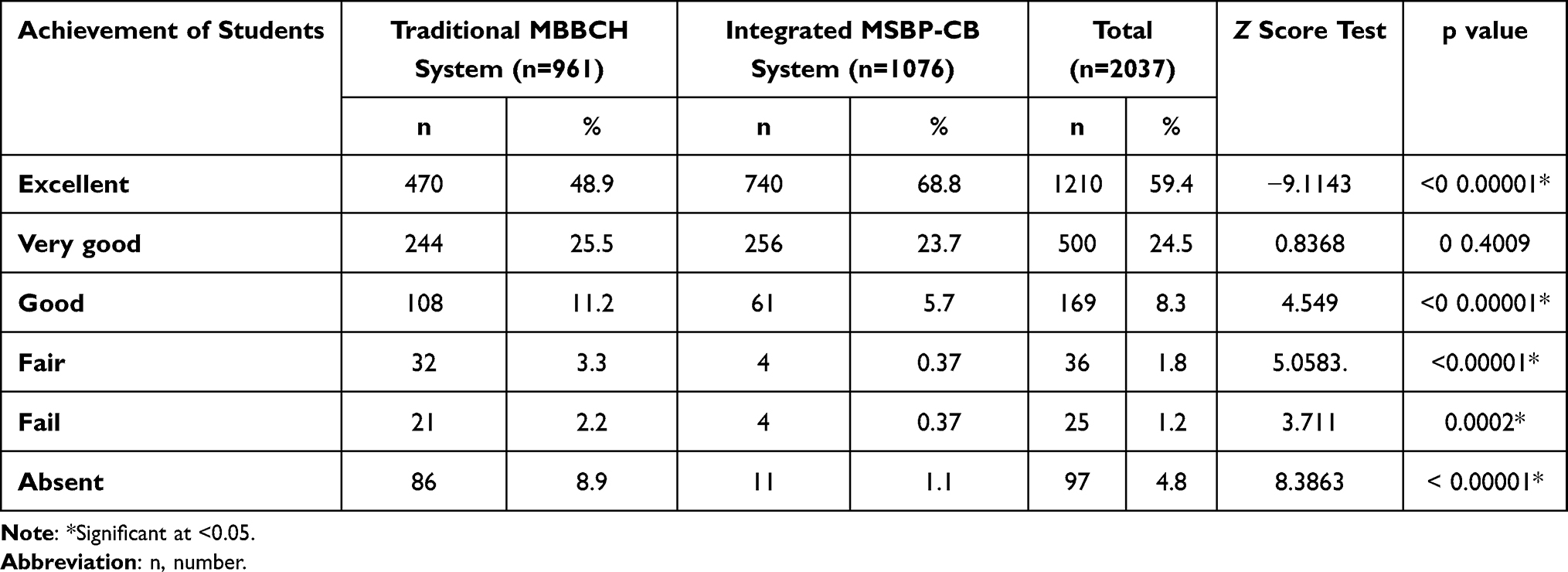 |
Table 11 Comparison Between the Traditional MBBCH and Integrated MSBP-CB Systems Regarding the Achievements of Students |
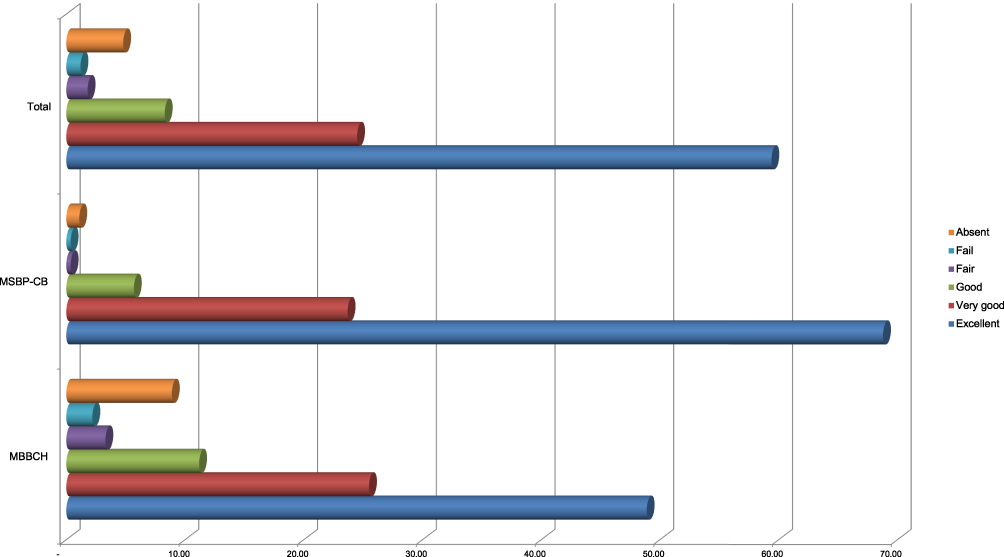 |
Figure 6 Comparing the traditional MBBCH and the integrated MSBP-CB systems regarding the achievements of students. |
Discussion
This study was conducted to evaluate medical students’ achievements and perceptions of learning environments in traditional and integrated curricula considering the Forensic Medicine and Clinical Toxicology course as an analog for the reformed learning context. Although the transition from a traditional to an integrated curriculum is a worldwide phenomenon that has been implemented for years in different medical colleges, such a transition should be carefully considered in terms of perceived and associated benefits and deficiencies (for students and faculties).
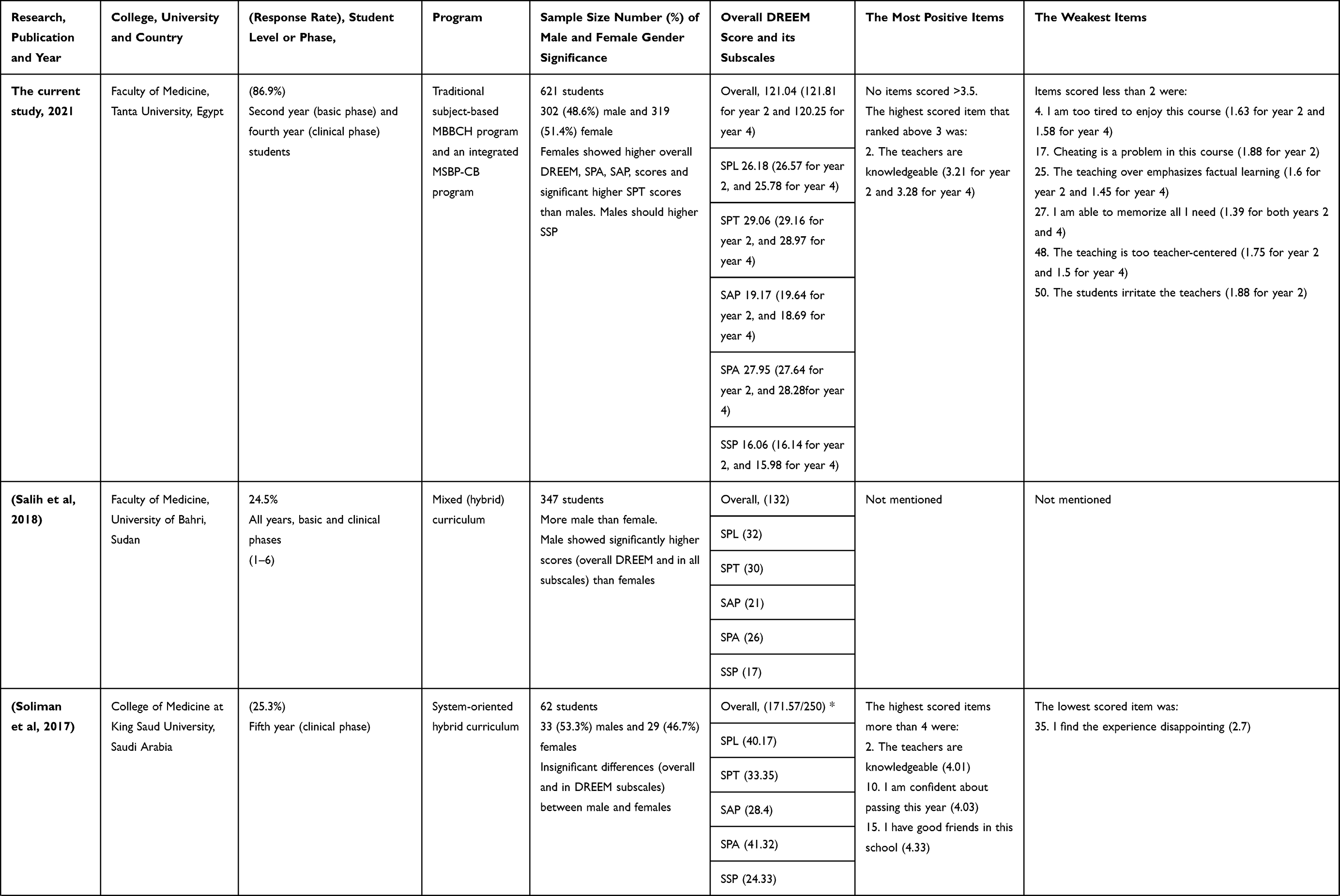
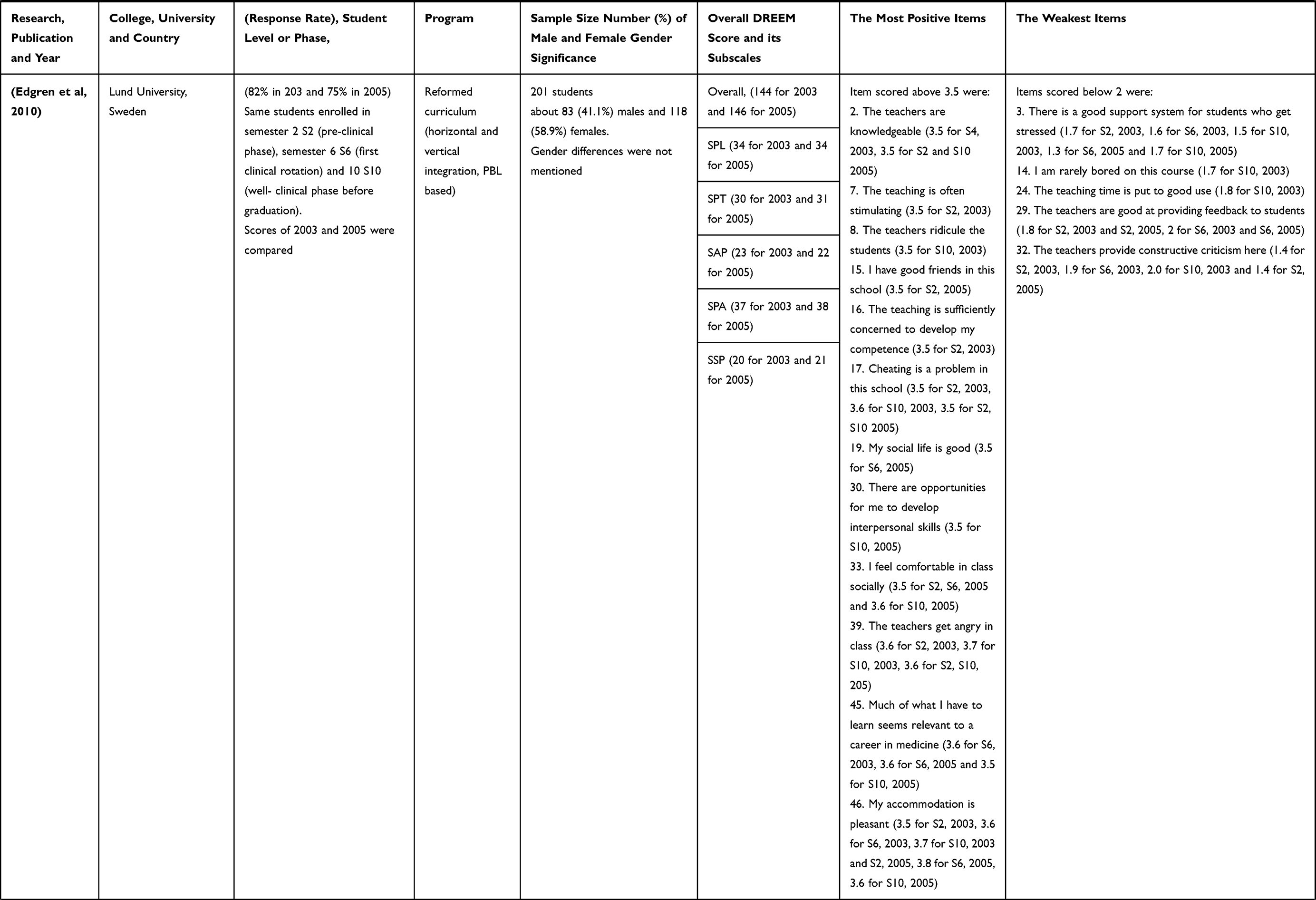
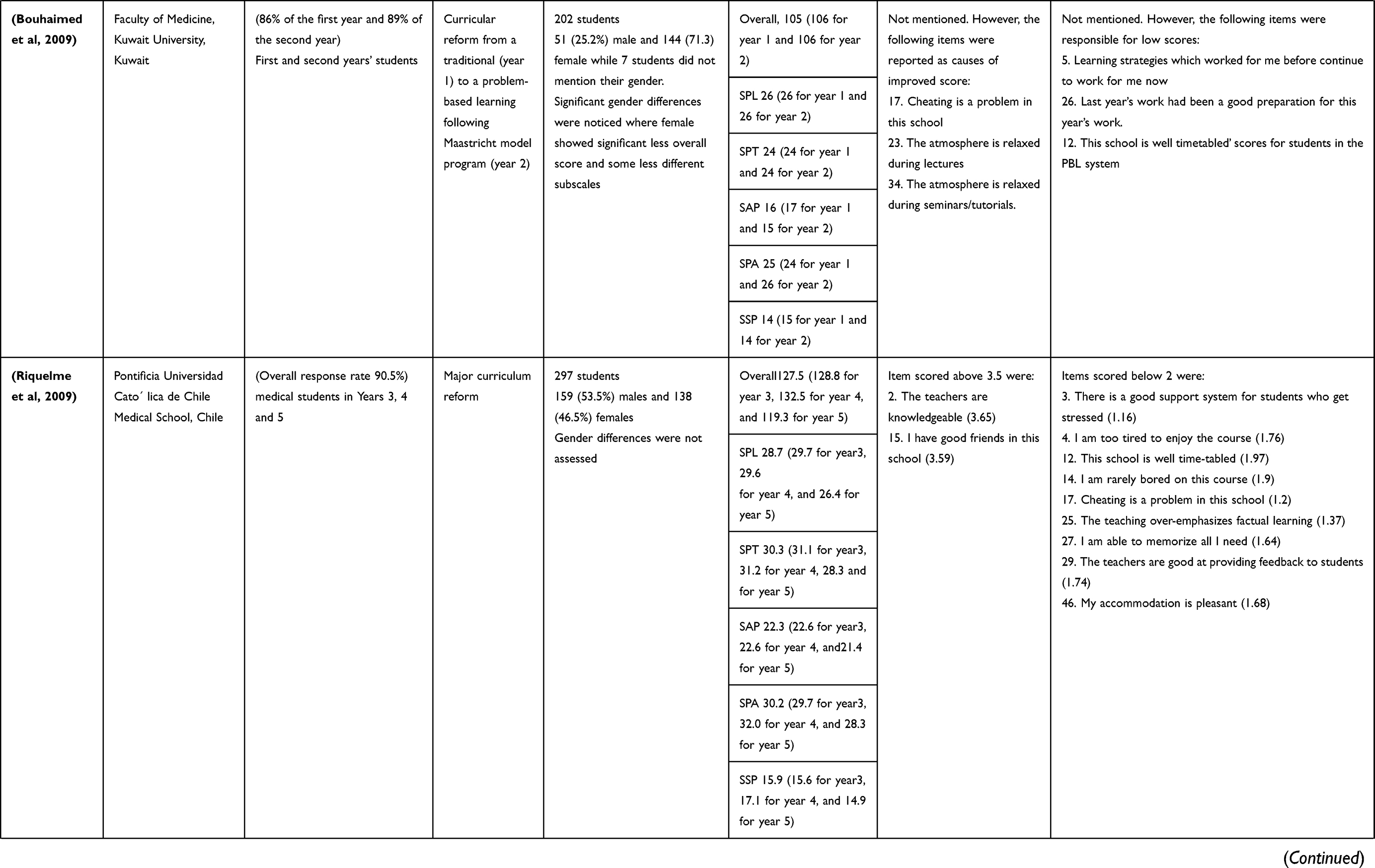
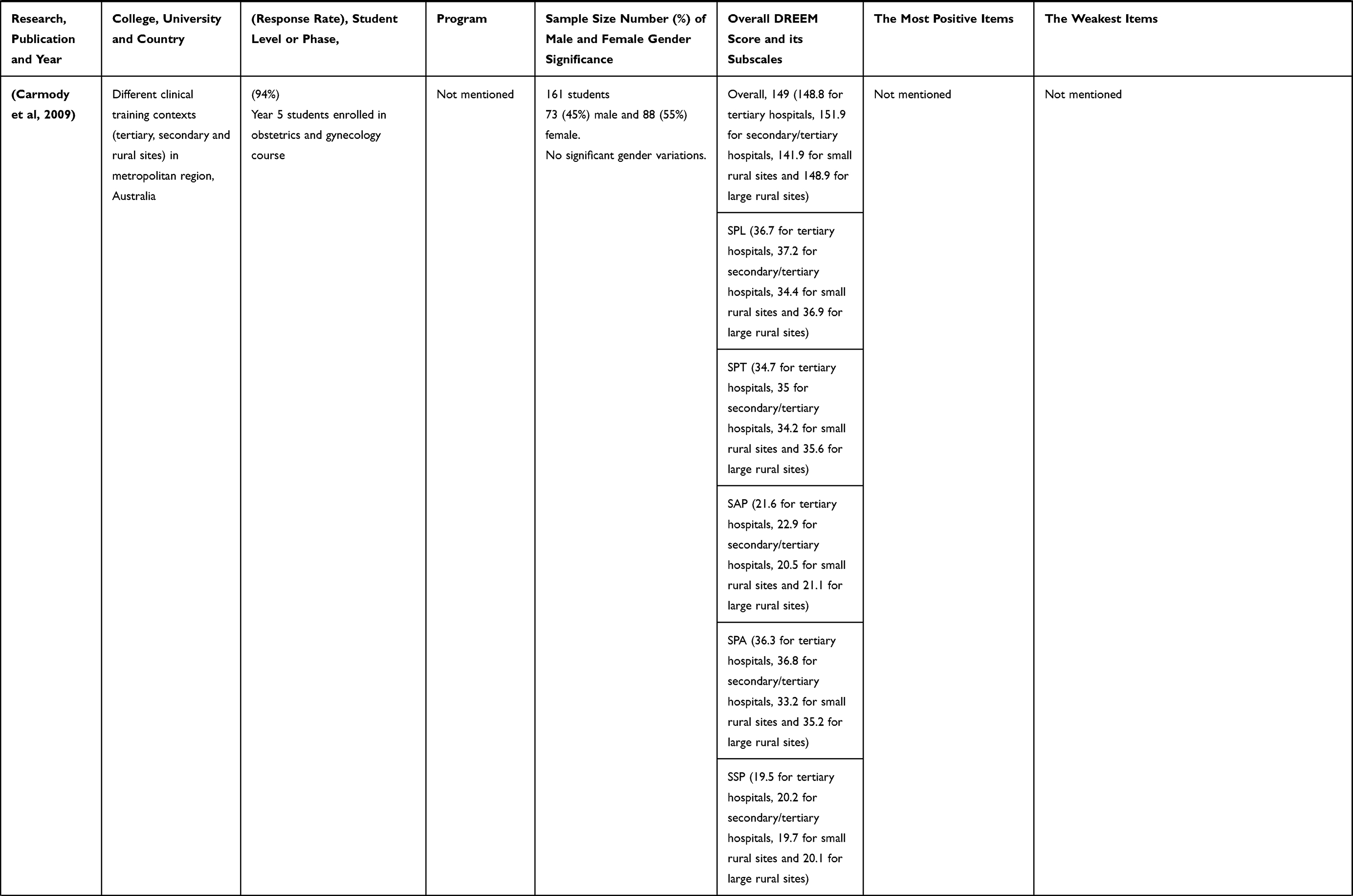
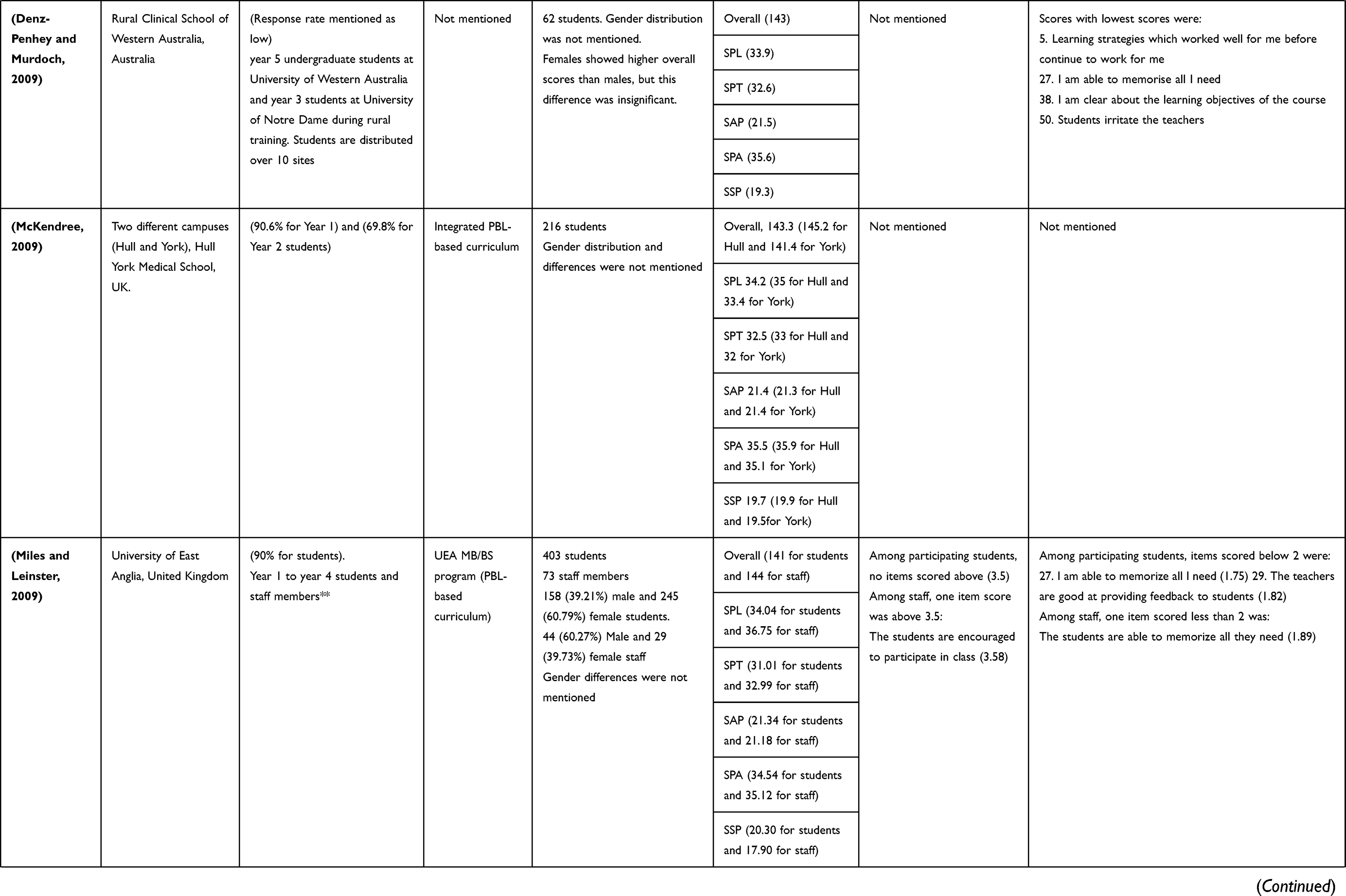
This study analyzed the achievements of 2037 students and the responses of 621 medical students, a relatively high number compared to previous studies, as highlighted in Table 12. The number of females in this study was greater than that of males; however, the difference was not statistically significant. As illustrated in Table 12, several previous studies revealed different patterns of male and female students’ distribution, reflecting gender distribution variations among different populations. Conversely, the reported significant variations in age distribution between the study participants in both groups are a reflection of the time schedule of running programs. Students enrolled in the integrated curriculum were younger (year two) than those in the traditional program (year four).
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
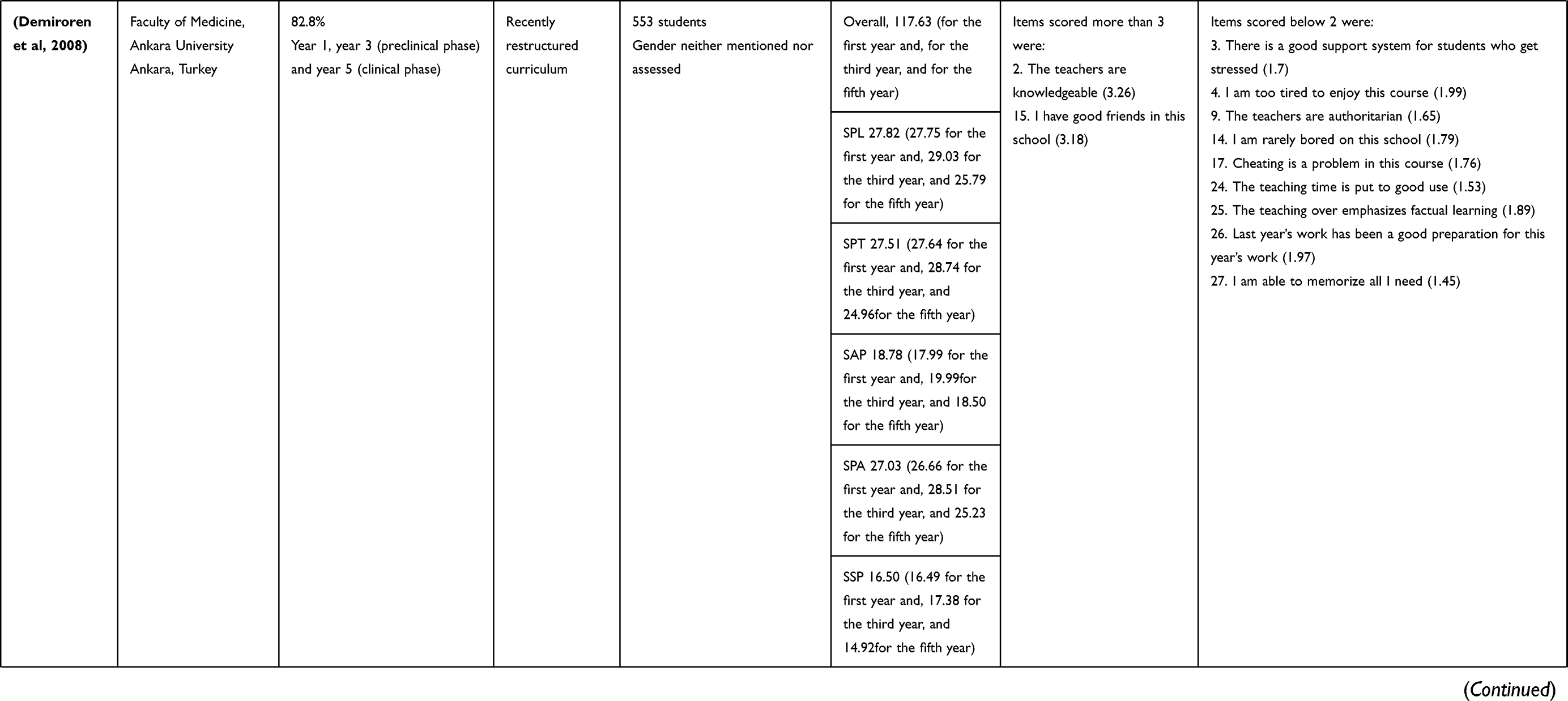 |
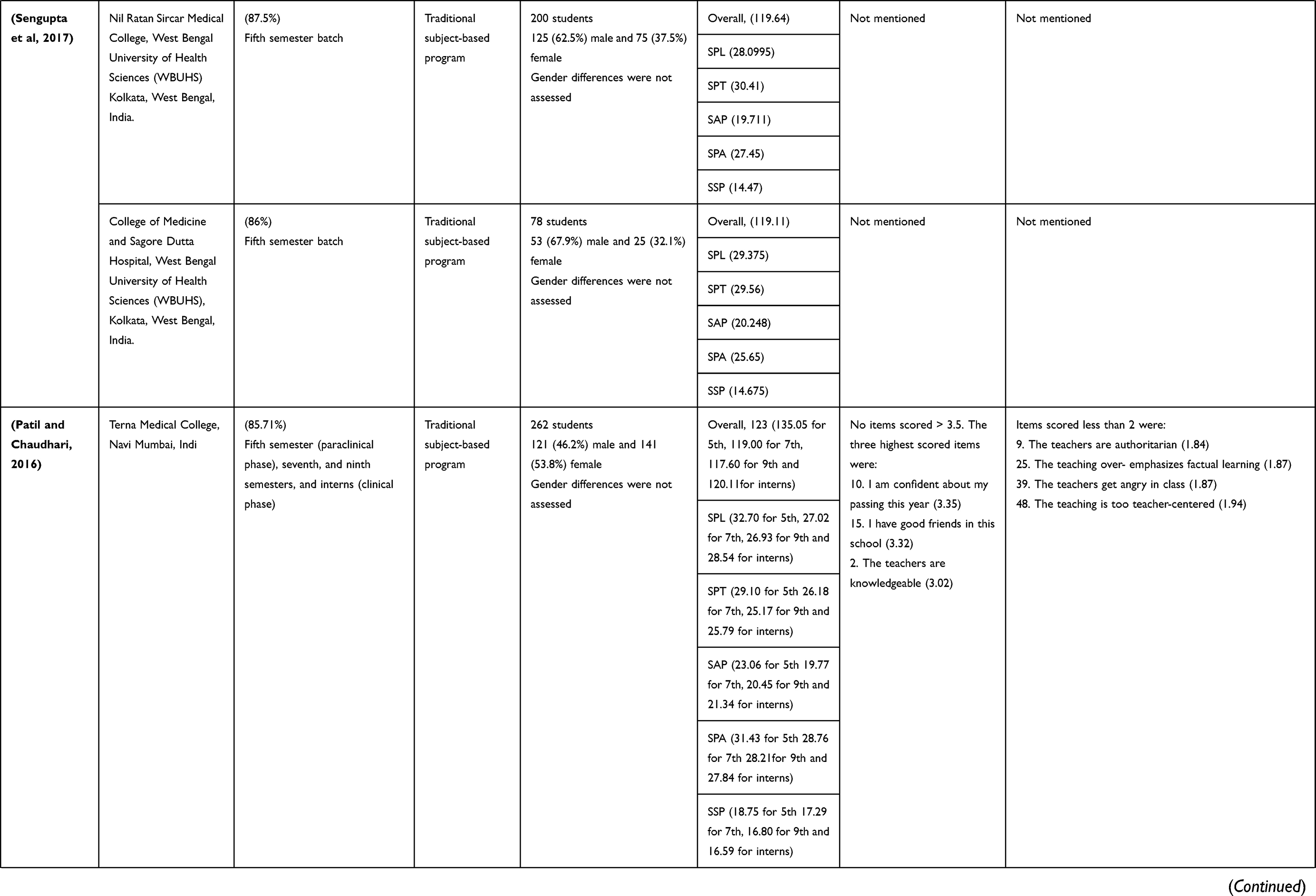
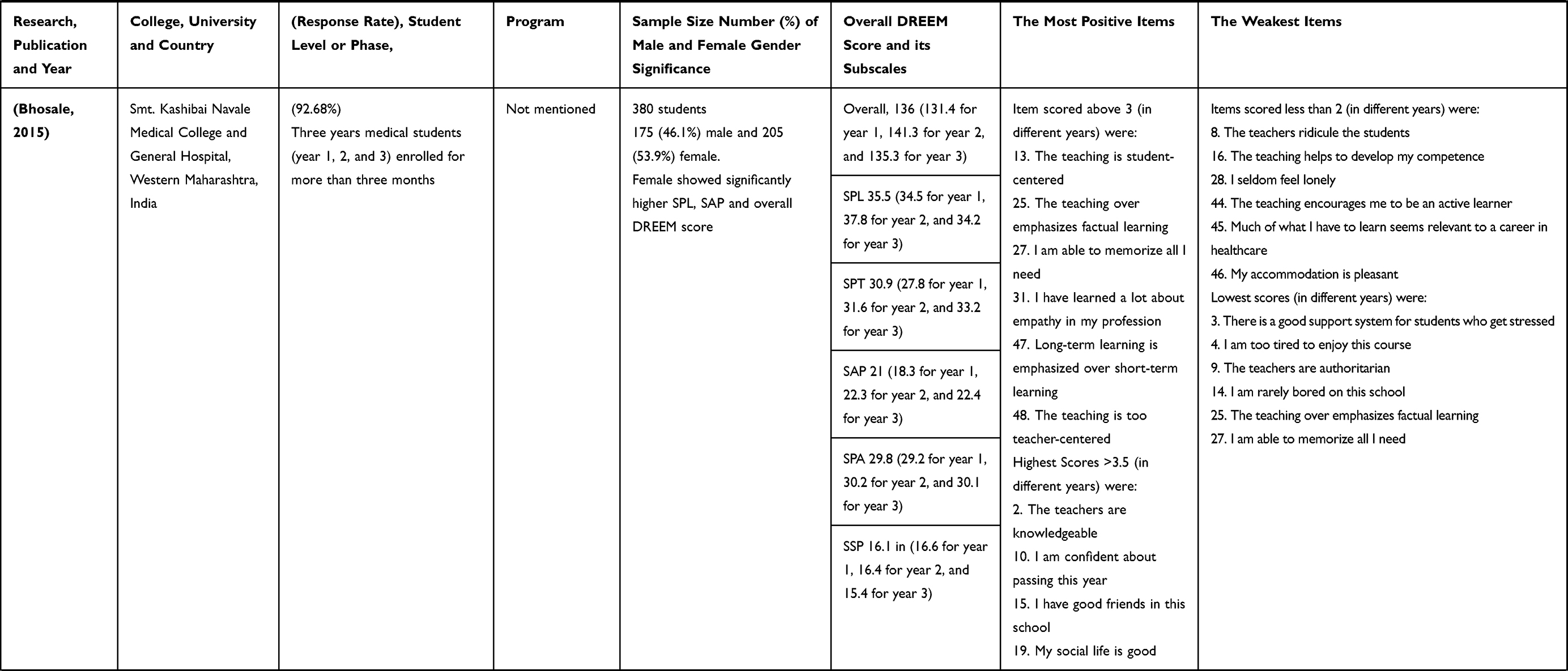
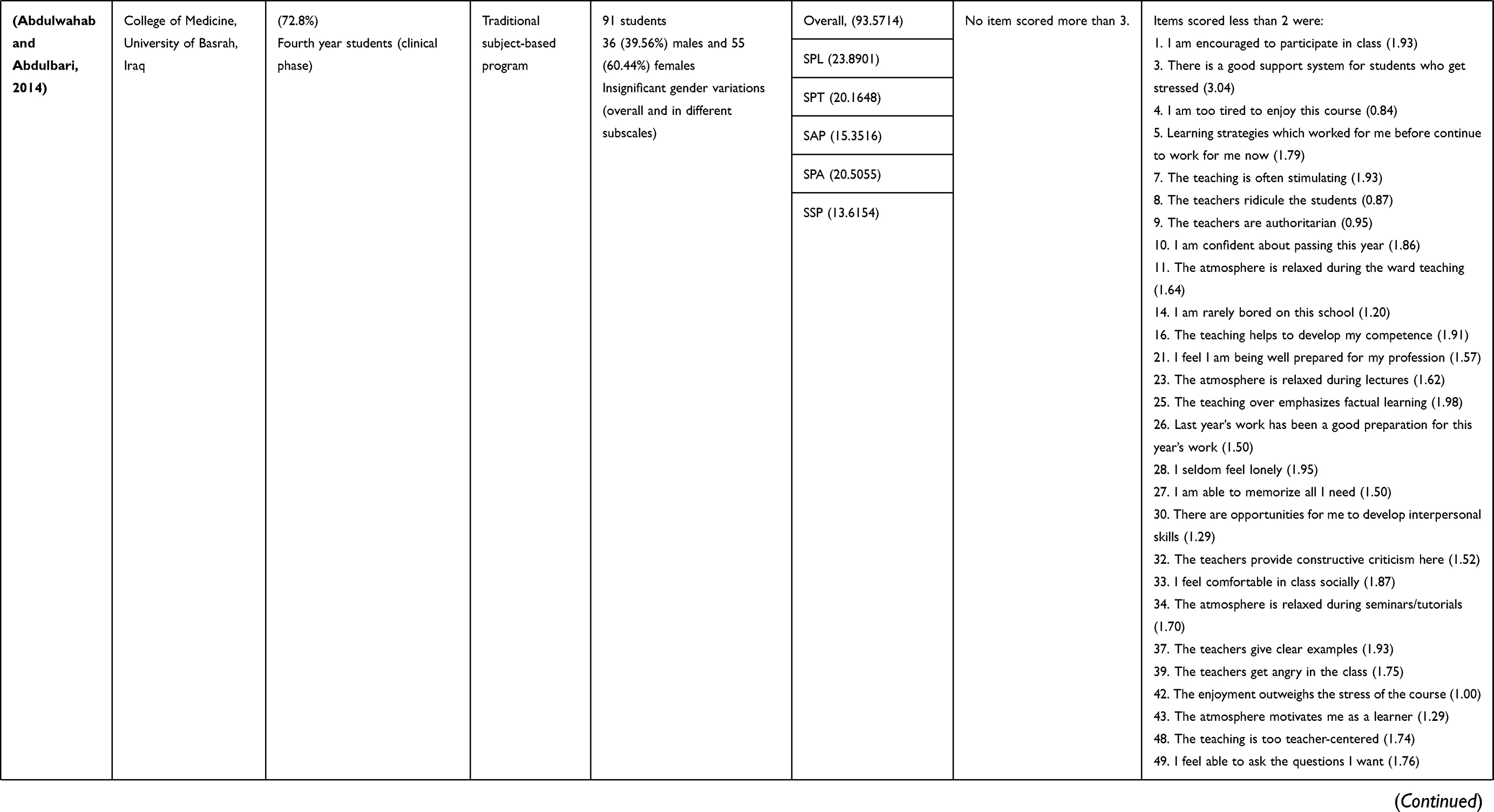
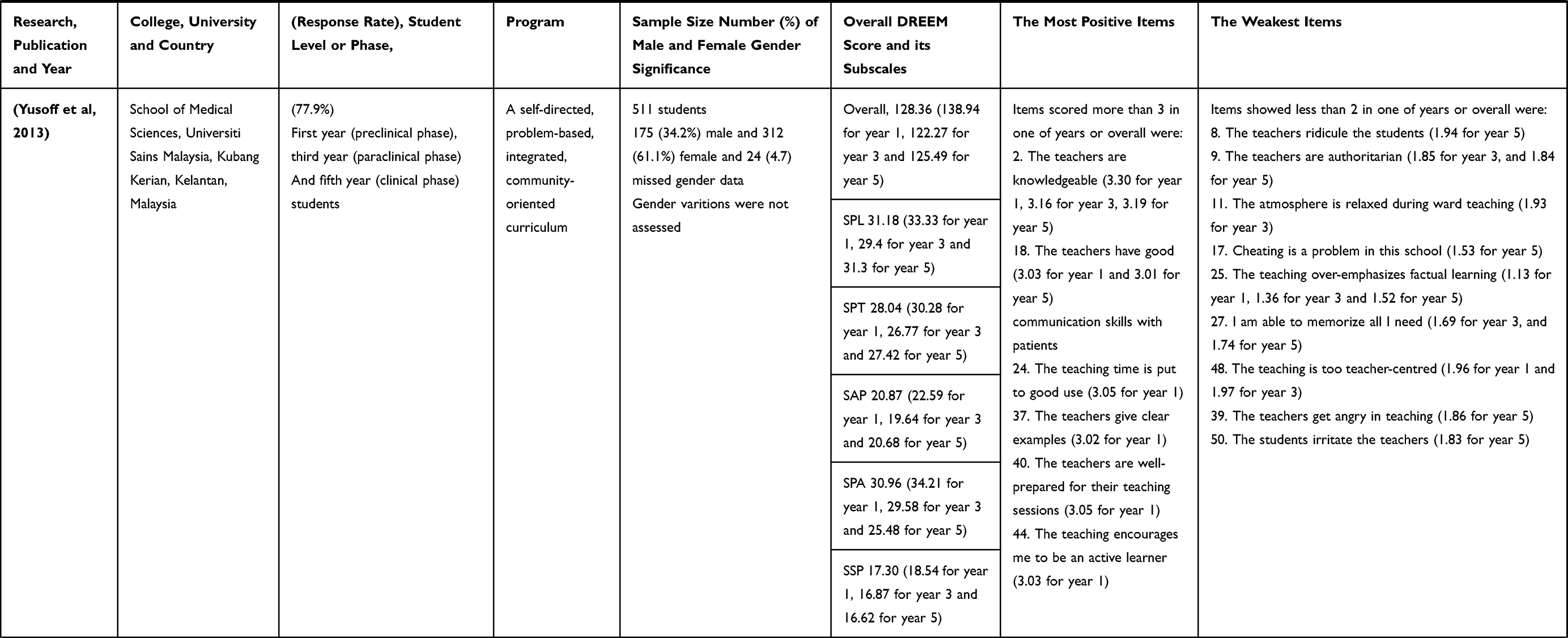
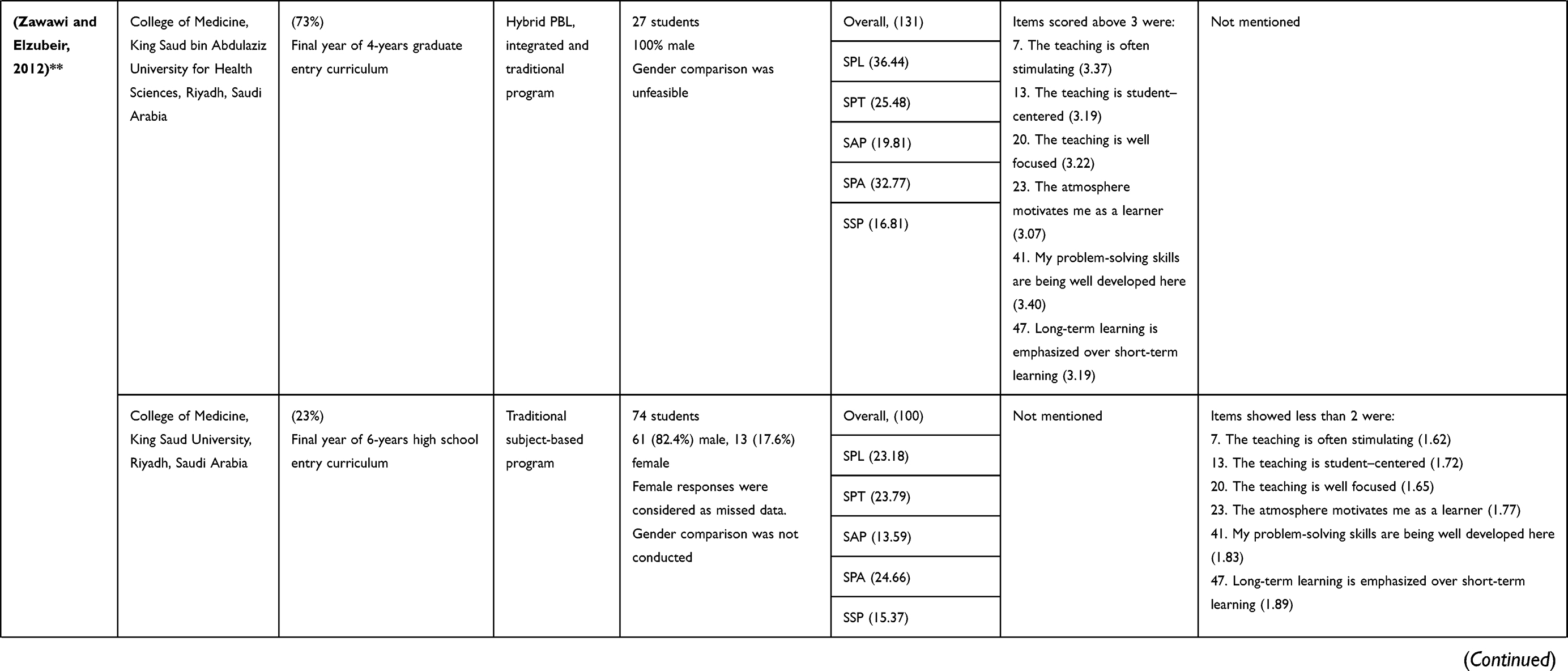
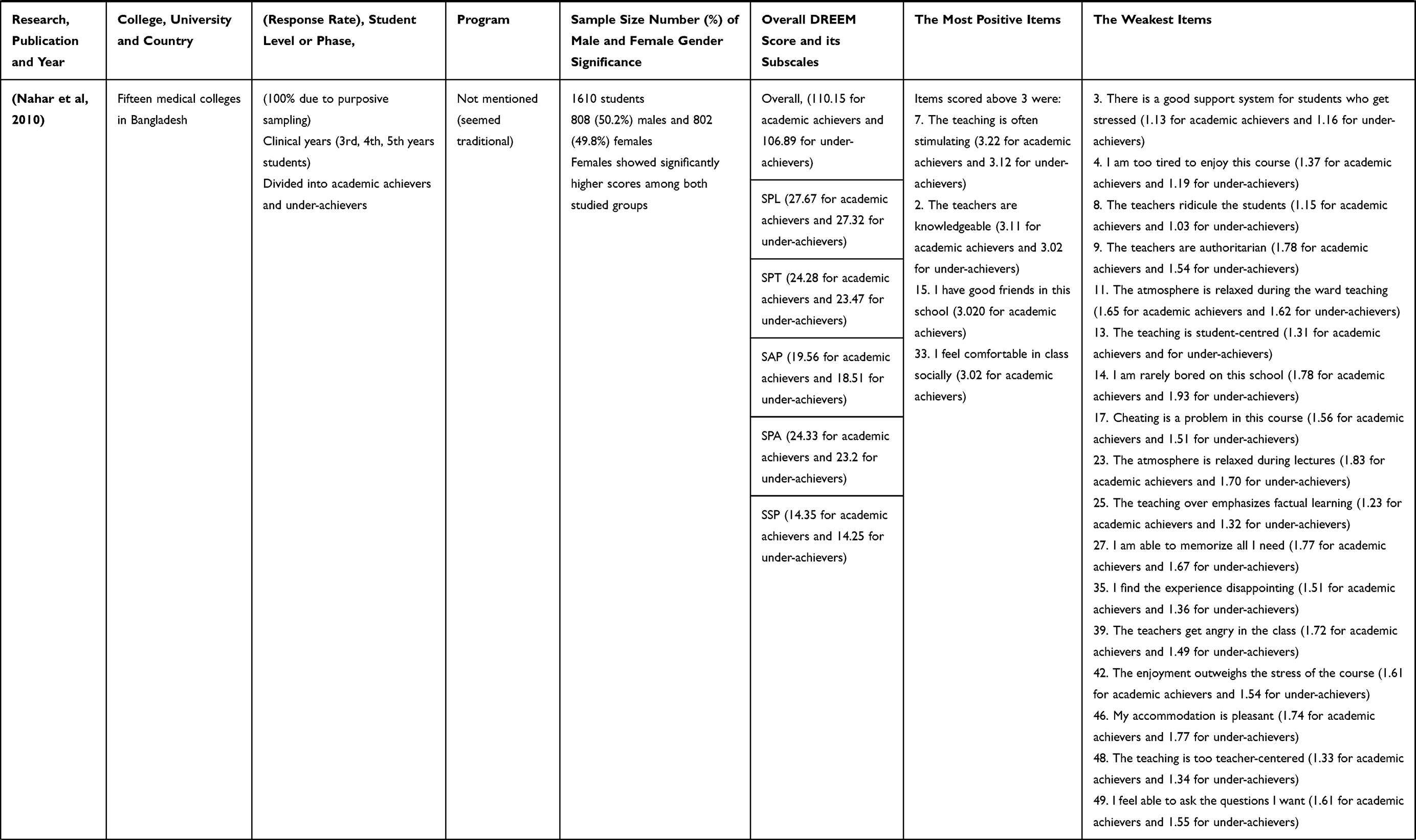
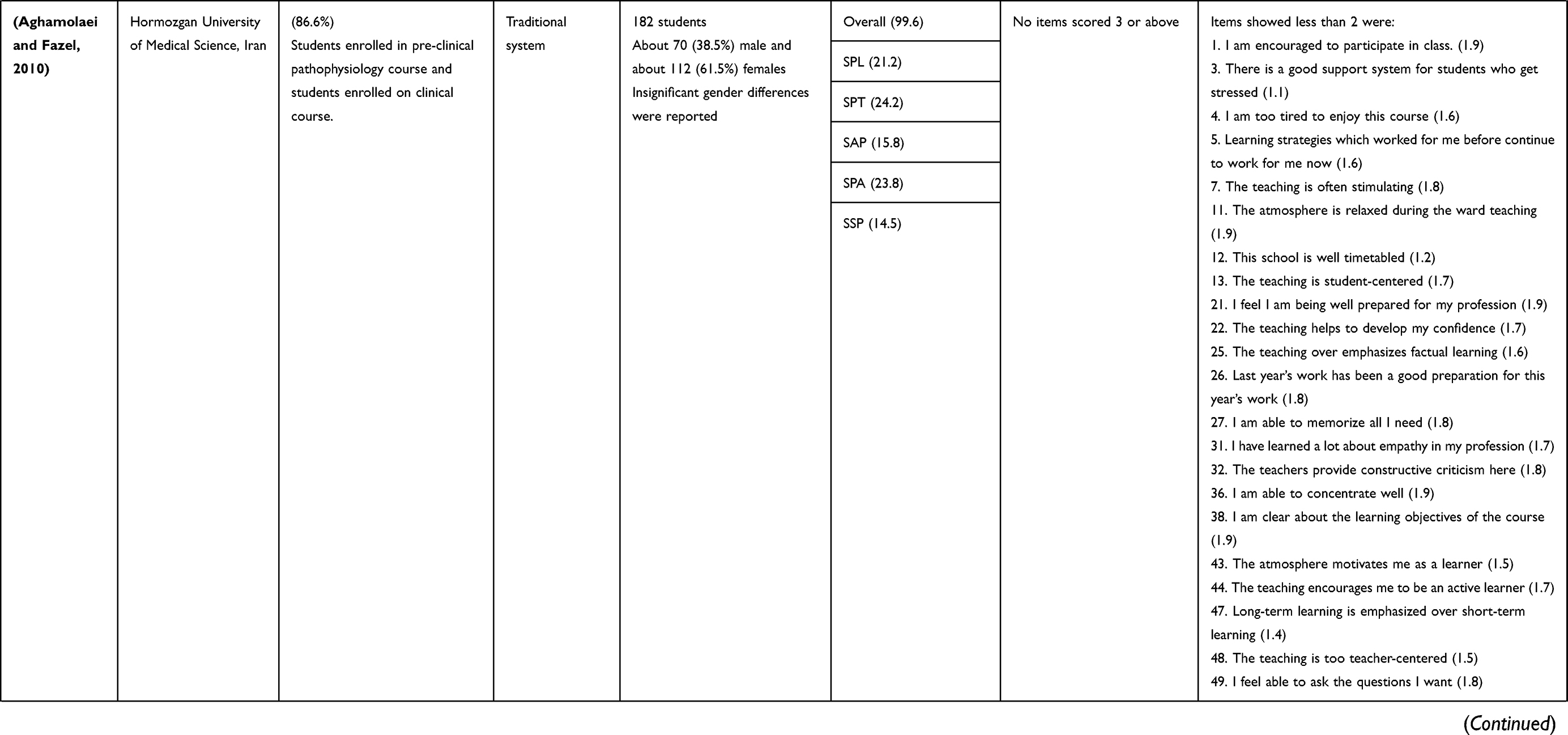
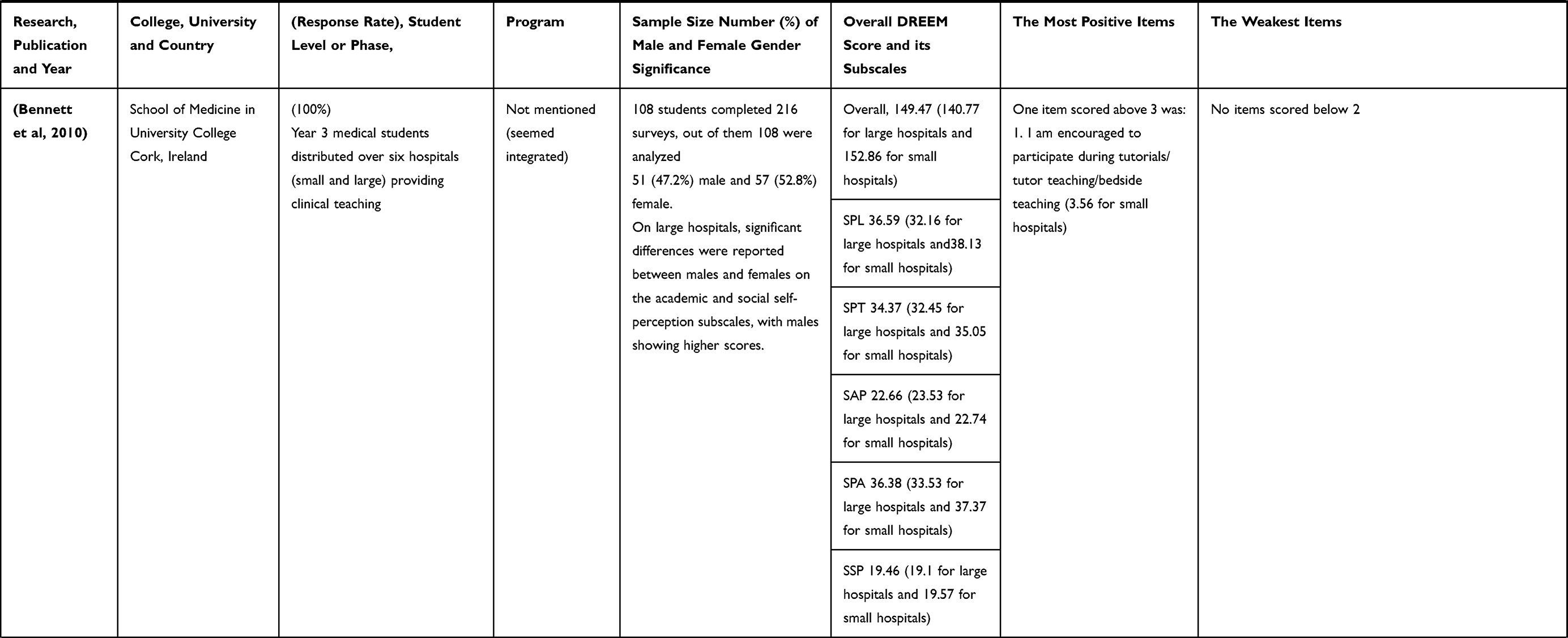
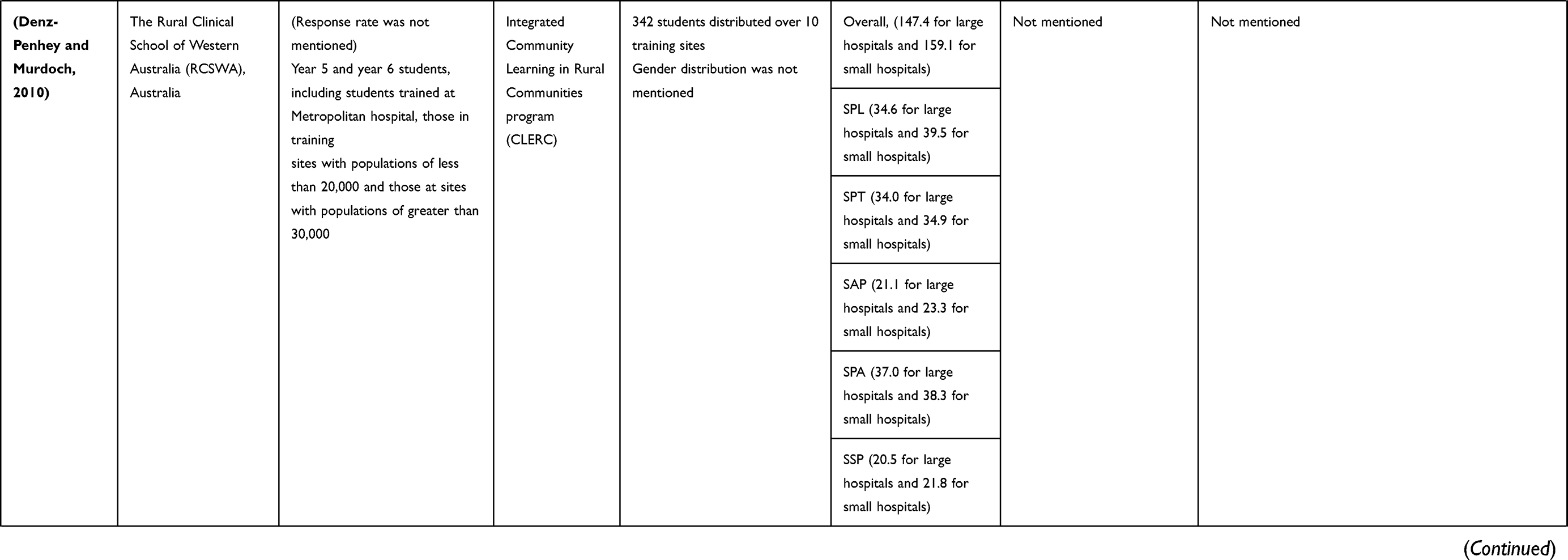
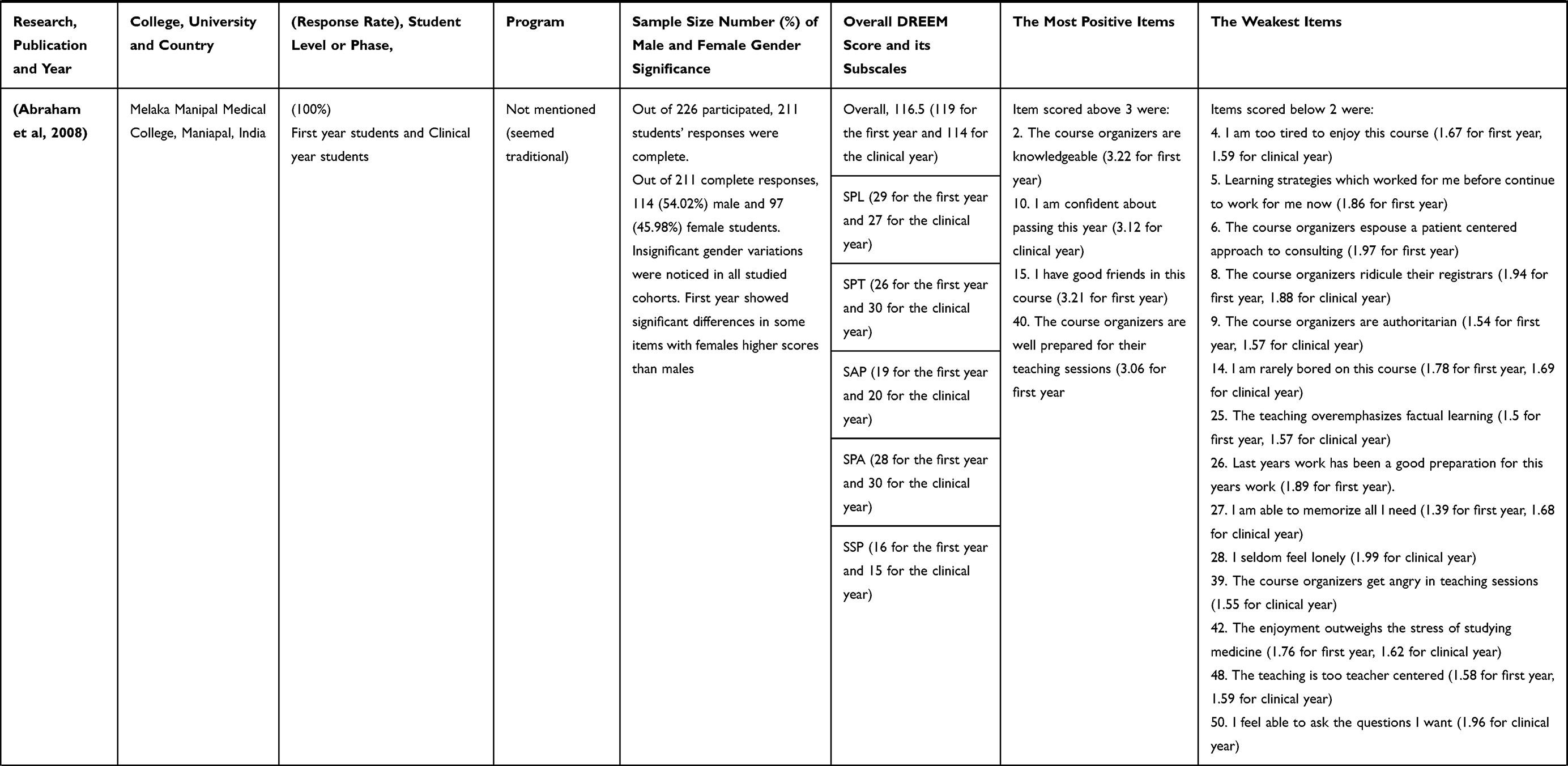
Table 12 Summary of the Selected Studies Showing Medical Students’ Perceptions Using the DREEM Inventory at National and Worldwide Levels from 2008 to 2021 |
This study conveyed more positive than negative learning environments, with slightly higher overall DREEM scores for students in the integrated program than those in the traditional program (121.81 and 120.25, respectively). The reported overall score was similar to scores of students in the School of Medical Sciences, University Sains, Malaysia, enrolled in preclinical, paraclinical, and clinical years (128.36, 122.27, and 125.49, respectively).12 Medical students enrolled in traditional systems in different learning contexts showed similar or even much lower scores than those in our study.13–15 Conversely, students enrolled in hybrid or integrated student-centered curricula exhibited significantly higher scores.13,16,17 The significant improvement in students’ perceptions of the learning environment following curricular reforms is not incidental and is related to the root causes that impel most medical schools to reform their curricula to be integrated, student-centered, problem-based, and socially accountable.18
However, when moving more in-depth, our study yielded significant variations between students’ perceptions of different score subscales in both study groups. Students enrolled in the integrated curriculum showed significantly better perceptions of learning and better academic self-perceptions, as can be demonstrated by more stimulating teaching, less teacher-centered teaching, and less angry teachers in comparison with students of the traditional system. The fact regarding students’ perceptions of learning and teaching being better because of integration is consistent with the results of a previous study conducted in Saudi Arabia.13 A higher perception of learning and teaching upon integration is an encouraging finding. The main goals of program integration are increasing dependence on self-learning and active participation and improving autonomy in thinking and reasoning. Traditional curricula that employ teacher-centered educational strategies typically depend on providing students with readymade opinions and judgments, which some scholars have described as spoon-feeding.13
Additionally, our study reveals some bright points in the form of significant improvements in students’ perception of aspects related to academic self-perceptions following curriculum integration. Students enrolled in the integrated system described the previous learning strategies as continuing to work and the previous year’s work as sufficient preparation for the current year’s work had significantly higher scores than their peers in the traditional curriculum. This finding is consistent with those of Zawawi and Elzubeir, where the mean score of students’ academic self-perception reported for the traditional curriculum was 13.95 compared to 19.81 for the reformed curriculum.13 Similarly, another study reported that students in basic years exhibited better academic self-perception than those in paraclinical and clinical years (22.59, 19.64, and 20.68, respectively).12 However, contrary to the current findings, in Kuwait, Bouhaimed et al reported a deterioration of academic self-perception during the transition from traditional to problem-based learning.19 It is worth mentioning that the deterioration of the academic self-perception score after curricular changes among Kuwaiti students was primarily because of the poor perception of learning strategies and the students’ belief that the previous year’s work had no role in the preparation for the current year. These two items were the same that showed significant improvement among students enrolled in the integrated system in this study. This discrepancy could be related to the different nature of the transition between the two studies. In Egypt, students enrolled in the new curriculum were novices and had no previous experience with the traditional curriculum in contrast to Kuwaiti students, who were part of the traditional system before being involved in the reformed curriculum, which highlights the necessity of students’ preparation before deciding to transition. However, changes in the academic potentials between students in different programs might be another justification.19
This study revealed more positive attitudes regarding students’ perceptions of the learning environment and not-too-bad students’ SSP. Students enrolled in the integrated system, although their experience is less disappointing and they appreciate a good support system for students who have stress, could make good friends significantly more easily than those in the traditional curriculum. These findings are consistent with those of previous studies.19 Similarly, it was reported that SPA and SAP were better in students enrolled in paraclinical years than in those in clinical years.20 It is well known that medical students in all programs are more prone than other students to face stress, develop anxiety and depression symptoms, and lack appropriate strategies for coping with stress. Fear of failure, unsuitable learning environments, and unsatisfactory teaching strategies are among the most common causes of physical and mental disorders in medical students.21 Well-designed curricula can enable appreciating the role of mentorship, student counseling, and guidance such that students are eligible to approach faculties periodically. Moreover, studying in small groups, such in Problem-Based Learning (PBL), or in teams and participating in community-based activities, which are characteristic features of integrated curricula, enable academic advisors to tackle students who need help, thus assisting and offering them scaffolds to bridge problems.22 Additionally, the design of the integrated curriculum helps social interaction between students and promotes their communication skills.
However, our study reported three items that were perceived better by students in the traditional program, that is, that the course was well timetabled and that the teaching time was put to good use, in addition to enjoying a more relaxing atmosphere. These results are partially consistent with those of a study conducted in Kuwait, which revealed that timetable is one weak point presented by students enrolled in the PBL-adopting curriculum. Nevertheless, this study demonstrated an improvement in students’ perceptions of the learning environment upon curricular transition, and students reported that the learning environment was more relaxed than before.19
In this study, the most positively reported item was “the teachers are knowledgeable” as it had scores of >3 in both systems. This is a strong point for the institution, and as we mentioned before, both programs share the same resources, including tutors. Good, qualified faculties are one of the cardinal pillars that support and positively influence learning environments. The role of knowledgeable faculties in improving a learning environment has been thoroughly reported in different contexts.7,23,24
Our study also reported weaknesses that are common to both systems, including the overemphasis on factual learning and learning that is too teacher centered. These two weaknesses, with similar scores, were reported in other studies where traditional curricula were delivered.25,26 However, recently-structured curricula also suffer from a lack of emphasis on factual teaching, which might explain the poor perception of this item among students in the integrated curriculum in this study.27 These findings require that more attention be paid to social accountability when designing curricula and endorsing community-based activities as integral components of an integrated system, besides periodic program monitoring and development. The other important point is the faculty development that should be run parallel to the transition process. Faculties should be trained to utilize innovative teaching strategies and assessment tools to allow students to practice Self Directed learning along with proper tutor guidance.28
Other weaknesses reported in our study were the poor abilities of students to memorize information and the feeling of being too tired to enjoy a course. These results are consistent with those of previous studies.14,26,29 Utilizing multiple instructional designs may solve the poor memorization problem. Additionally, periodic assessments of mental and physical health and involvement in extracurricular activities would bring more pleasure and enjoyment during the arduous journey of medical studies.30
Another aim of this study was to assess if students’ perceptions of their learning environments were influenced by gender, age, or previous GPAs. It was reported that females showed higher overall DREEM scores than males, although the difference was not statistically significant. Furthermore, females showed higher scores than males in all subscales except SSP. These variations were only significant in SPT. Higher perception by females has been thoroughly reported in similar medical schools that implement different programs worldwide.2,26,31 Other studies have reported variations that were not statistically significant between males and females perception.17,32 Paradoxically, males in other studies showed a higher perception of their learning environment. A study conducted in Irish large hospitals revealed that academic and SSP subscale scores of males were significantly higher than those of females.33 A study on Kuwaiti medical students of two different systems (traditional and integrated) also found that female’s perceptions of their learning environments were significantly poorer than those of males.19 Although some studies may attribute gender variations to the segregation of students according to their gender in some countries, which is not the case in Egypt, it is not well known why female’s perceptions are better than those of males, and the inconsistent gender variations between this and other studies should be investigated in future studies.1
This study also found that younger students had higher perceptions of their learning environments (overall DREEM), which was significant in the learning and student academic perception subscales. However, the perceptions of teachers were significantly better in older students enrolled in the traditional program. In our study, younger students enrolled in basic and preclinical years at King Saud University, Saudi Arabia, showed higher perceptions than older students.29 Conversely, students in the first year of study showed lower perceptions of their learning environments than those in advanced levels.27 These variations are intimately related to the curriculum design and the way in which the transition to integration was conducted.
This study expanded on the influence of previous students’ achievements (GPAs) on learning environment perception. It was concluded that students with higher GPAs (Excellent) showed significantly higher mean overall DREEM, SPL, SPT, and SAP scores. Moreover, a positive correlation was found between overall DREEM, as well as its subscales, and previous year GPA. These findings are consistent with those of Nahar et al, who reported higher scores among high achievers compared to underachievers.26 Moreover, our results are partially consistent with those of Mayya and Roff, who reported that higher achievers had better academic self-perceptions and SSP.34 Thus, efforts should be directed to improving the perceptions of low achievers, which is evidently linked to their academic performances.35
The association between students’ perceptions of their learning environments and their academic performances became more obvious when the performances of the two cohorts of students (in integrated and traditional programs) were compared. This study reported that students enrolled in the integrated curriculum achieved significantly more excellent grades than those in the traditional program. Moreover, good and fair grades were significantly more common among students of the traditional system, besides the additional cases of failure and higher absence rates. Our findings are consistent with those of Hong-yan et al, who compared the achievements of medical students in the traditional system with those of others who used new integrated techniques and reported significantly higher grades among students who utilized the new techniques.36
Consistent with the discussion so far, integration itself is not the aim. Instead, the process of integration aims to enhance students’ competencies and upgrade their skills, which is partially reflected in their performances on different assessment platforms. Implementing student-centered, PBL, community-based activities as well as acquiring knowledge in a system-based manner are reflected as a significant decline in the absence and failure rates among students enrolled in the integrated program.
Our study revealed that the integration of medical curricula in Egypt, as a developing country, seems to be on its way to success. Considering the weaknesses and running faculty development programs alongside the transition process will guarantee a smooth, successful transition. Continuous monitoring and improvement of the learning environment are needed to achieve desired outcomes. Although our study elaborated on various important constituents of the learning environment, some other factors should be addressed in future studies, including the effect of the clinical training resources on students’ perceptions.37,38 Moreover, future studies should assess the faculties’ perceptions of their learning environments.39
Limitations and Recommendations
Compared to the total number of students enrolled in both programs, the number of participants was, to some extent, low. This may be attributed to the adoption of a hybrid online system (online lectures and on-campus attendance only for practical sessions) as a measure of limiting the spread of COVID-19. This made it somewhat difficult to meet students. Another possible limitation is that the English version of the survey was administered because the validated Arabic version was not accessible. However, the authors translated a few strange expressions for the students, and both groups study medicine in the English language and are required to pass a placement test with good scores before joining the faculty. Nonetheless, we recommend, where possible, administering the questionnaire in the students’ first language to reduce potential misinterpretation of items.
Conclusion
This study revealed a smooth, successful transition from the traditional to the integrated curriculum among Egyptian medical students. This success is evidenced by the significant improvement in the perception of the learning environment following the aforementioned transition and the significantly higher achievement found among students enrolled in the integrated program. This study conveys more positive than negative perceptions of the learning environment, with more positive learning perceptions, SPT moving in the right direction, SAP being more on the positive side, more positive attitudes regarding students’ perceptions of the learning environment, and not-too-bad students’ SSPs. Medical students enrolled in the integrated curriculum showed higher DREEM scores, with significantly better learning and academic self-perceptions. Knowledgeable, qualified faculties are the most significant characteristic feature of both systems. Females with high GPAs in previous years showed higher perceptions. Areas for improvements include focusing on factual teaching, implementing student-centered teaching activities, promoting students’ ability to memorize, and engaging students in activities that may help them enjoy the learning process.
Abbreviations
AEC, Assessment and Evaluation Center; DREEM, Dundee Ready Education Environment Measure; GPA, grade point average; MBBCH, Bachelor of Medicine, Bachelor of Surgery; MSBP-CB, Medicine and Surgery Bachelor Program-Credit Points; PBL, problem based learning; REC, Research Ethical Committee; SD, standard deviation; SDL, self directed learning; SAP, student’s academic self-perceptions; SPA, student’s perceptions of atmosphere; SPL, student’s perceptions of learning; SPT, student’s perceptions of teachers; SSP, student’s social self-perception.
Institutional Review Board Statement
The current study was carried out after being approved by the Research Ethical Committee (REC) of the Faculty of Medicine, Tanta University (number 34379/1/21).
Data Sharing Statement
The data analyzed in the current study are available upon reasonable request from the corresponding author.
Informed Consent Statement
Written informed consent was obtained from every participant prior to their inclusion in the current study.
Acknowledgments
The authors extend their appreciation for undergraduate medical students of the Faculty of Medicine, Tanta University.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
The authors did not receive any support from funding or nonprofit agencies for this study.
Disclosure
The authors report no competing interests (financial or non-financial) related to this work.
References
1. Vaughan B, Carter A, Macfarlane C, The MT. DREEM, part 1: measurement of the educational environment in an osteopathy teaching program. BMC Med Educ. 2014;14(1):1–11. doi:10.1186/1472-6920-14-99
2. Bhosale U. Medical students’ perception about the educational environment in western Maharashtra in medical college using DREEM scale. J Clin Diagnostic Res. 2015;9(11):JC01–JC04. doi:10.7860/JCDR/2015/15094.6809
3. Genn JM. AMEE medical education guide no. 23 (part 1): curriculum, environment, climate, quality and change in medical education - A unifying perspective. Med Teach. 2001;23(4):337–344. doi:10.1080/01421590120063330
4. Bakhshialiabad H, Bakhshi M, Hassanshahi G. Students’ perceptions of the academic learning environment in seven medical sciences courses based on DREEM. Adv Med Educ Pract. 2015;195. doi:10.2147/amep.s60570
5. Soemantri D, Herrera C, Riquelme A. Measuring the educational environment in health professions studies: a systematic review. Med Teach. 2010;32(12):947–952. doi:10.3109/01421591003686229
6. Abdelaziz A, Kassab SE, Abdelnasser A, Hosny S. Medical education in Egypt: historical background, current status, and challenges. Heal Prof Educ. 2018;4(4):236–244. doi:10.1016/j.hpe.2017.12.007
7. Edgren G, Haffling AC, Jakobsson U, McAleer S, Danielsen N. Comparing the educational environment (as measured by DREEM) at two different stages of curriculum reform. Med Teach. 2010;32:6. doi:10.3109/01421591003706282
8. Finn Y, Avalos G, Dunne F. Positive changes in the medical educational environment following introduction of a new systems-based curriculum: DREEM or reality? Curricular change and the Environment. Ir J Med Sci. 2014;183(2):253–258. doi:10.1007/s11845-013-1000-4
9. McAleer S, Roff S. A practical guide to using the Dundee Ready Education Environment Measure (DREEM) 2003. Creative Educ. 2016;4(5):29–33.
10. Faculty of medicine. Available from: https://med.tanta.edu.eg/en/default.aspx.
11. Trapp RG, Dawson B. Basic & Clinical Biostatistics. McGraw-Hill Education LLC; 2001.
12. Yusoff MSB, Jaa’far R, Arzuman H, Arifin WN, Mat PMN. Perceptions of medical students regarding educational climate at different phases of medical training in a Malaysian medical school. Educ Med J. 2013;5(3). doi:10.5959/eimj.v5i3.146
13. Zawawi AH, Elzubeir M. Using DREEM to compare graduating students′ perceptions of learning environments at medical schools adopting contrasting educational strategies. Med Teach. 2012;34(SUPPL. 1):25–31. doi:10.3109/0142159X.2012.656747
14. Abdulwahab H, Abdulbari A. Validation of dundee ready education environment measure (DREEM) in Basrah college of medicine. Med J Basrah Univ. 2014;32(2):63–69. doi:10.33762/mjbu.2014.103861
15. Sengupta P, Sharma A, Das N. Perception of learning environment among undergraduate medical students in two different medical schools through DREEM and JHLES questionnaire. J Clin Diagnostic Res. 2017;11(2):JC01–JC04. doi:10.7860/JCDR/2017/23810.9248
16. Salih KMA, Idris MEA, Elfaki OA, et al. Measurement of the educational environment in MBBS teaching program, according to DREEM in college of medicine, university of Bahri, Khartoum, Sudan. Adv Med Educ Pract. 2018;9:617–622. doi:10.2147/AMEP.S160218
17. Soliman MM, Sattar K, Alnassar S, et al. Medical students’ perception of the learning environment at king saud university medical college, Saudi Arabia, using dreem inventory. Adv Med Educ Pract. 2017;8:221–227. doi:10.2147/AMEP.S127318
18. RM Harden, Sowden S, WR Dunn. Educational strategies in curriculum development: the SPICES model. Med Educ. 1984;18(4):284–297. doi:10.1111/j.1365-2923.1984.tb01024.x
19. Bouhaimed M, Thalib L, Doi SAR. Perception of the educational environment by medical students undergoing a curricular transition in Kuwait. Med Princ Pract. 2009;18(3):204–208. doi:10.1159/000204351
20. Patil AA, Chaudhari VL. Students’ perception of the educational environment in medical college: a study based on DREEM questionnaire. Korean J Med Educ. 2016;28(3):281–288. doi:10.3946/kjme.2016.32
21. Al-Dabal BK, Koura MR, Rasheed P, Al-Sowielem L, Makki SM. A comparative study of perceived stress among female medical and non-medical university students in Dammam, Saudi Arabia. Sultan Qaboos Univ Med J. 2010;10(2):231–240.
22. Harden RM, Crosby J. AMEE guide no 20: the good teacher is more than a lecturer - The twelve roles of the teacher. Med Teach. 2000;22(4):334–347. doi:10.1080/014215900409429
23. Abraham RR, Ramnarayan K, Pallath V, Torke S, Madhavan M, Roff S. Perceptions of academic achievers and under-achievers regarding learning environment of Melaka Manipal Medical College (Manipal campus), Manipal, India, using the DREEM Inventory. South East Asian J Med Educ. 2007;1:18–24.
24. Riquelme A, Oporto M, Oporto J, et al. Measuring students’ perceptions of the educational climate of the new curriculum at the Pontificia Universidad Católica de Chile: performance of the Spanish translation of the Dundee Ready Education Environment Measure (DREEM). Educ Heal Chang Learn Pract. 2009;22(1):1–11.
25. Aghamolaei T, Fazel I. Medical students’ perceptions of the educational environment at an Iranian Medical Sciences University. BMC Med Educ. 2010;10(87):1–7. doi:10.1186/1472-6920-10-87
26. Nahar N, Talukder H, Khan TH. PErceiption of acdemic acheivers and under acheivers regarding educational environment of medical colleges in Bangladesh. Bangladesh Med J. 2010;39(2):2–10. doi:10.3329/bmj.v39i2.7029
27. Demiroren M, Palaoglu O, Kemahli S, Ozyurda F, Ayhan IH. Perceptions of students in different phases of medicai education of educational environment: Ankara university faculty of medicine. Med Educ Online. 2008;13(1):4477. doi:10.3402/meo.v13i.4477
28. Al-eraky MM, Donkers J, Wajid G, et al. Faculty development for learning and teaching of medical professionalism Faculty development for learning and teaching of medical professionalism. Med Teach. 2015;37:S40–S46. doi:10.3109/0142159X.2015.1006604
29. Al-Ayed IH, Sheik SA. Assessment of the educational environment at the College of Medicine of King Saud University, Riyadh. East Mediterr Heal J. 2008;14(4):953–959.
30. Kim SH. Extracurricular activities of medical school applicants. Korean J Med Educ. 2016;28(2):201. doi:10.3946/kjme.2016.25
31. Denz-Penhey H, Murdoch JC. A comparison between findings from the DREEM questionnaire and that from qualitative interviews. Med Teach. 2009;31(10):e449–e453. doi:10.3109/01421590902849552
32. Carmody DF, Jacques A, Denz-Penhey H, Puddey I, Newnham JP. Perceptions by medical students of their educational environment for obstetrics and gynaecology in metropolitan and rural teaching sites. Med Teach. 2009;31(12):e596–e602. doi:10.3109/01421590903193596
33. Bennett D, Kelly M, O’Flynn S. Are the bigger hospitals better: DREEM on? Ir J Med Sci. 2010;179(4):515–519. doi:10.1007/s11845-010-0551-x
34. Sarwar S, Tarique S. Perception of educational environment: does it impact academic performance of medical students? J Pak Med Assoc. 2016;66(10):1210–1214.
35. Mayya SS, Roff S. Students’ perceptions of educational environment: a comparison of academic achievers and under-achievers at Kasturba Medical College, India. Educ Heal. 2004;17(3):280–291. doi:10.1080/13576280400002445
36. Hong-yan W, Ling-na HAN, Hong-mei MA, Ya-ping PAN. The improvement of periodontal teaching mode based on PDCA theory. Shanghai J Stomatol. 2016;25(4):504.
37. Denz-Penhey H, Murdoch JC. Is small beautiful? Student performance and perceptions of their experience at larger and smaller sites in rural and remote longitudinal integrated clerkships in the Rural Clinical School of Western Australia. Rural Remote Health. 2010;10(3):1470. doi:10.22605/rrh1470
38. Lai NM, Nalliah S, Jutti RC, Hla YY, Lim VKE. The educational environment and self-perceived clinical competence of senior medical students in a Malaysian medical school. Educ Heal Chang Learn Pract. 2009;22(2):1–15.
39. Miles S, Swift L, Leinster SJ. The Dundee Ready Education Environment Measure (DREEM): a review of its adoption and use. Med Teach. 2012;34(9):e620–e634. doi:10.3109/0142159X.2012.668625
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.