Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 16
Precision Medicine in Type 2 Diabetes Mellitus: Utility and Limitations
Authors Galiero R, Caturano A ![]() , Vetrano E, Monda M, Marfella R, Sardu C, Salvatore T, Rinaldi L, Sasso FC
, Vetrano E, Monda M, Marfella R, Sardu C, Salvatore T, Rinaldi L, Sasso FC ![]()
Received 14 April 2023
Accepted for publication 27 October 2023
Published 16 November 2023 Volume 2023:16 Pages 3669—3689
DOI https://doi.org/10.2147/DMSO.S390752
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Juei-Tang Cheng
Raffaele Galiero,1,* Alfredo Caturano,1,* Erica Vetrano,1 Marcellino Monda,2 Raffaele Marfella,1 Celestino Sardu,1 Teresa Salvatore,3 Luca Rinaldi,1 Ferdinando Carlo Sasso1
1Department of Advanced Medical and Surgical Sciences, University of Campania “Luigi Vanvitelli”, Naples, Italy; 2Department of Experimental Medicine, University of Campania “Luigi Vanvitelli”, Naples, Italy; 3Department of Precision Medicine, University of Campania “Luigi Vanvitelli”, Naples, Italy
*These authors contributed equally to this work
Correspondence: Ferdinando Carlo Sasso, Department of Advanced Medical and Surgical Sciences, University of Campania “Luigi Vanvitelli”, Naples, Italy, Tel/Fax +39 0815665010, Email [email protected]
Abstract: Type 2 diabetes mellitus (T2DM) is one of the most widespread diseases in Western countries, and its incidence is constantly increasing. Epidemiological studies have shown that in the next 20 years. The number of subjects affected by T2DM will double. In recent years, owing to the development and improvement in methods for studying the genome, several authors have evaluated the association between monogenic or polygenic genetic alterations and the development of metabolic diseases and complications. In addition, sedentary lifestyle and socio-economic and pandemic factors have a great impact on the habits of the population and have significantly contributed to the increase in the incidence of metabolic disorders, obesity, T2DM, metabolic syndrome, and liver steatosis. Moreover, patients with type 2 diabetes appear to respond to antihyperglycemic drugs. Only a minority of patients could be considered true non-responders. Thus, it appears clear that the main aim of precision medicine in T2DM is to identify patients who can benefit most from a specific drug class more than from the others. Precision medicine is a discipline that evaluates the applicability of genetic, lifestyle, and environmental factors to disease development. In particular, it evaluated whether these factors could affect the development of diseases and their complications, response to diet, lifestyle, and use of drugs. Thus, the objective is to find prevention models aimed at reducing the incidence of pathology and mortality and therapeutic personalized approaches, to obtain a greater probability of response and efficacy. This review aims to evaluate the applicability of precision medicine for T2DM, a healthcare burden in many countries.
Keywords: type 2 diabetes mellitus, precision medicine, risk factors, genomic, environmental factors, drugs
Introduction
Type 2 diabetes mellitus (T2DM) is one of the most widespread diseases in Western countries, and its incidence is constantly increasing. Epidemiological studies have shown that in the next 20 years, the number of subjects affected by T2DM will double. This expected increase in incidence is likely associated with several causes. Among them, a sedentary lifestyle, an unbalanced diet due to an increase in the percentage of daily carbohydrate intake, the absence of robust screening and public health information programs, and the lack of simple access to specialized healthcare could represent some of these reasons. Thus, a great challenge for the healthcare system is to reduce the incidence of the disease and its complications to improve the prognosis and quality of life of the patients.
Precision medicine is a discipline that evaluates the applicability of genetic, lifestyle, and environmental factors to disease development. In particular, it evaluated whether these factors could affect the development of diseases and their complications, response to diet, lifestyle, and use of drugs (Table 1). Consequently, the clinician could identify groups of subjects at higher risk for the development of some diseases or groups of individual responders or non-responders to lifestyle modifications and use of drug classes. Thus, the goal is to find prevention models aimed at reducing the incidence of pathology and mortality and therapeutic personalized approaches to obtain a greater probability of response and efficacy.
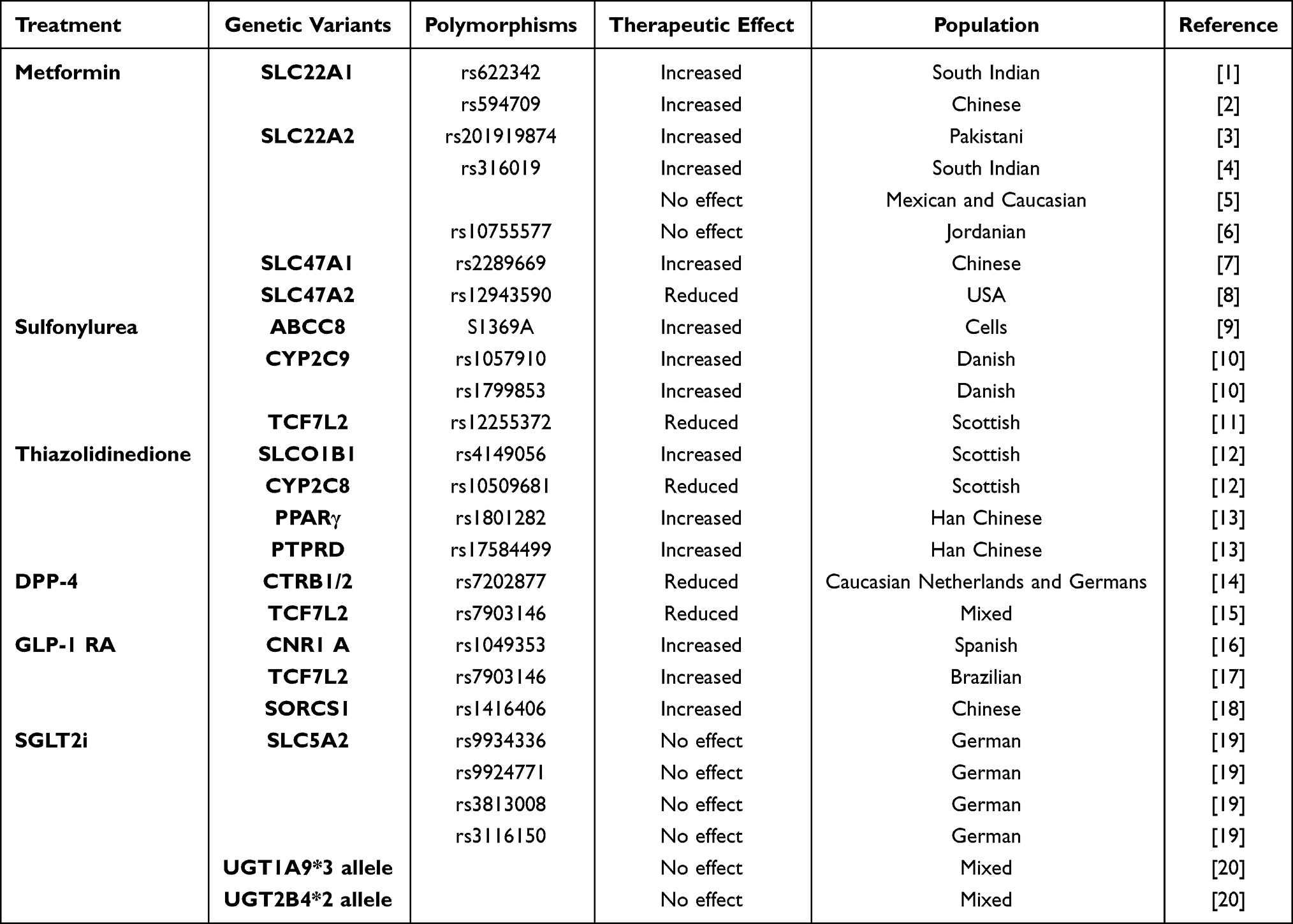 |
Table 1 Main Genetic Variants Influencing Glycaemic Response |
This review aims to evaluate the applicability of precision medicine for T2DM, a healthcare burden in many countries.
Role of Genomic
In recent years, owing to the development and improvement in methods for studying the genome, several authors have evaluated the association between monogenic or polygenic genetic alterations and the development of metabolic diseases and complications. Furthermore, these studies investigated the association between diabetes, development of complications and response to treatments.
Monogenic Diabetes
Monogenic diabetes accounts for almost 3% of all diabetes cases and mainly involves a mutation in the transcription factor gene HNF1A or GCK.21,22 Subjects with these mutations develop diabetes at an age lower than 25 years, are negative for autoimmunity, and have phenotypic characteristics similar to those of individuals with type 1 diabetes (T1DM). Individuals with mutations in the GCK gene do not usually need any treatment, whilst HNF1A mutated patients are particularly responsive to sulfonylureas, probably through a mechanism that involves an increase in insulin secretion compared to normal responders. The authors observed an association between the pharmacodynamic effects of sulfonylureas and the Kir6.2 mutation.23 A similar mechanism of drug sensitivity has been observed in neonatal diabetes caused by mutations in the KCNJ11 and ABCC8 genes.23–25
For what concerns T2DM, still today there are little data on the association between monogenic mutations and the development of the disease.26,27
Polygenic Diabetes
Research on multiple genes or variants, together with increasing the risk of developing diabetes or its complications, is object of precision medicine studies.28 Genome-wide association studies (GWAS) have identified about a hundred loci associated with the development of T2DM. In a cohort study on French subjects with T2DM, approximately 300,000 single-nucleotide polymorphisms were evaluated. By comparing the results of both study populations with the development of high-density arrays, four loci containing variants associated with an increased risk of T2DM were identified.29
Accordingly, another study evaluated 386,731 common single-nucleotide polymorphisms (SNPs) in a population of approximately 3000 subjects equally distributed between diabetic and healthy control individuals. At the end of the study, three loci were identified as associated with T2DM in non-coding regions, specifically in introns of IGF2BP2, CDKAL1, and SLC30A8.30 Results of similar studies on northern European and Chinese populations described new diabetes susceptibility loci and variants, and confirmed those previously identified, for a total of about 10 genomic loci associated with the development of T2DM.31–33 More recently, the results of DIAGRAM and MAGIC meta-analyses, through the evaluation of genetic studies on European populations, have led to the identification of new loci (99), for a total of about 200 loci associated with insulin resistance, rise in HbA1c, fasting 2-hr glucose, and fasting insulin.34–36
Another study on the gene polymorphisms of approximately 800 subjects from North India with and without T2DM evaluated the role of the mitochondrial uncoupling protein 2 (UCP2) gene polymorphism −866 G/A. UCP2 is a mitochondrial protein that plays a modulatory role in oxidative stress reactions, insulin sensitivity, and fatty acid metabolism.37–39 As previously highlighted, this study confirmed that UCP2 locus is associated with the development of obesity and T2DM.40,41 In particular, it has been highlighted that the 866 G/A SNP of UCP2 may be associated with the development of T2DM, both in homozygosis and heterozygosis. Furthermore, this association was more evident in subjects aged >50 years and in those with BMI > 25.42
Recently, based on genetic discoveries and improved computational algorithms, some authors have evaluated whether novel clusters of genetic loci allow to identify subsets of individuals with T2DM.43 In particular, Udler et al, through data from GWAS, have identified five clusters of T2DM loci and traits associated with beta cell function and insulin resistance.43 At the end of the study, the authors identified cluster genetic risk scores associated with distinct clinical outcomes (eg stroke, hypertension, and myocardial infarction).
Similar results have been reported for other datasets in genomic, transcriptomic, and epigenetic categories.44,45 Some authors have identified 10 key drivers associated with T2DM. Of these, COL5A1, IRF7, CD74, and HLA-DRB1 may play diagnostic roles, whereas others (PSMB9, COL1A1, and COL4A1) were presented at high levels in subjects with T2DM.46 These key drivers (hub genes) are the immune system and inflammatory response modulators, particularly associated with the activity of factors such as chemokines and cytokines, growth factor 19/21, TNF-α, Interleukin-1 beta (IL-1β), Interleukin-6 (IL-6), Interleukin-18 (IL-18), adiponectin and C-reactive protein.46 The authors refer to the thesis through which T2DM appears due to the action of these factors, thereby hypothesizing a diagnostic and potentially useful role for susceptibility to some drugs on these key drivers.
In conclusion, discovery of those loci could allow identifying potential causal and tissue-specific regulatory mechanisms associated with pathways associated with insulin resistance and insulin deficiency. Moreover, by clustering the population of T2DM subjects, it will be possible to obtain precision surveillance and clinical response to different treatment regimens.
Epigenetic Changes
Epigenetics is a discipline that studies the role of environmental and non-environmental factors (eg, diet, chemical agents, physical activity, and age) in modulating gene expression, without modifying DNA sequences. The main mechanisms of epigenetic regulation are DNA methylation, histone tails, and chromatin structure modifications.47
DNA methylation involves the addition of a methyl group to DNA molecules, often occurring at cytosine residues in a CpG dinucleotide context. Usually, the result of methylation is to silence some promoters, thus inhibiting the transcription. This process can influence gene expression and has been linked to various metabolic disorders, including obesity and T2DM48–50 In particular, DNA methylation and gene expression analyses have been performed in the adipose tissue of subjects with T2DM and obesity. The authors observed many methylations associated with these pathologies, 11120 differentially methylated CpG sites (DMCs) and 96 differentially methylated regions (DMRs). Furthermore, the correlation between differences in DNA methylation and changes in gene expression profiles was evaluated. Sixteen genes encoding DMCs, including ATP11A, LPL, and EHD2, were also significantly correlated with fasting glucose and HbA1c levels. These observations led authors to hypothesize that these loci with methylated DNA could be considered markers of disease.51 In this regard, the association between methylated DNA sequences obtained from the white blood cells of Indian subjects with diabetes was evaluated. In almost 1300 patients enrolled in the study, methylated positions (DMPs) associated with T2DM were 49. The observed genes with these methylations were associated with insulin sensitivity (SREBF1), cholesterol, and phospholipid transport (ABCG1), as indicated for the development of complications (HDAC). However, these results were not confirmed by multiple comparisons correction.52
Further studies are needed to better define the roles of genomic, epigenomic, and transcriptomic analyses, in terms of their diagnostic and prognostic roles. The variability in response to environmental factors, object of study of precision medicine and epigenetics, will be discussed in the subsequent sections.
Role of Metabolomics
Metabolomics is a comprehensive analysis of metabolites in a biological specimen and is an emerging discipline that could be strictly associated with precision medicine.53 Through new methods for detecting biomarkers in body fluids (eg, serum and urine), it is possible to identify and define the role of multiple metabolomics. Liquid chromatography mass spectrometry (LC-MS), the most common profiling technology used for detecting biomarkers, could show changes in the metabolic profile and particular metabolic abnormalities, by quantifying and specifying the number of modified biomarkers.53 More recently, some authors have evaluated whether known metabolomics or new metabolomics could have not only a role in describing metabolic status of subjects but also in predicting the development of T2DM. In this regard, a study on a population of about 2500 subjects without diabetes followed for about 12 years, showed that some amino acids (isoleucine, leucine, valine, tyrosine, phenylalanine, and 2-aminoadipic acid) were significantly associated with the development of T2DM.54,55 Results from a retrospective cohort study on 100 subjects showed other biomarkers associated with the development of T2DM. At the end of the study, about 10 new metabolites were significantly associated with the development of the disease.56
Some investigators then evaluated whether the intake of food and probiotics could be associated with a modification of the metabolomics and alterations of the intestinal microbiome. Furthermore, it was evaluated whether these changes could have a role in the development or progress of diabetic disease. For example, Bifidobacterium longum, which is normally part of the intestinal microbiota, showed positive effects after the assumption for 5 weeks on the progression of T2DM and obesity in diabetes model mice.57 In another population of hypercholesterolemia hamsters, a diet with addition of hawthorn seed oil decreased plasma cholesterol and favorably modulated gut microbiota composition and gut-derived metabolites associated with cholesterol regulation.58 More recently, some authors have demonstrated that lipid extract of foxtail millet (LEFM) feeding in diabetic mice could modify gut microbiota composition, reduce harmful bacteria, and induce a bloom of probiotics. In particular, they observe a reduction in Escherichia-Shigella, Peptococcus, and norank_f_Oscillospiraceae, an increase of short-chain fatty acid producing bacteria (Adlercreutzia, Faecalibaculum, and Bifidobacterium). Moreover, LEFM treatment altered serum concentration of some metabolites by increasing the levels of L-carnitine and L-glutamine and reducing S-acetyl dihydrolipoamide-E and sphingosine.59 Briefly, it seems that some modifications of the intestinal microbiome could not only modify the amount of serum metabolites but also have a positive impact on the progression of the diabetic disease.
Other studies on adults with T2DM then evaluated whether some biomarkers could be predictive of T2DM complications. In particular, it seems that phosphocreatine and cyclic guanosine monophosphate could be associated with coronary heart disease.60 Moreover, propionic acid, oxoadipic acid, leucine, isovaleric acid, isobutyric acid, and indole-3-carboxylic acid seem markedly and independently associated with diabetic kidney disease, while fatty acid desaturase 2 (FADS2) seems an important potential contributor to the pathogenesis of proliferative diabetic retinopathy.61,62
Lifestyle and Environmental Factors
Over the last 20 years, the incidence of both diabetes and obesity has significantly increased. Some authors describe a real pandemic, especially in Western countries, and agree that unbalanced lifestyles and environmental factors are responsible. There has been a spread of a predominantly energy-rich diet with an increased consumption of refined carbohydrates at the expense of a more varied diet. Moreover, a sedentary lifestyle, which is widespread due to various environmental, socio-economic, and pandemic factors, has a great impact on the habits of the populations and, first of all, on their food lifestyle.63,64 These factors have significantly contributed to an increase in the incidence of metabolic disorders, such as obesity, T2DM, metabolic syndrome, liver steatosis.65–71
In this context, for the clinician, it is crucial to identify the “tailored” diet for each subject. Among hundreds of genes associated with T2DM, the main genomic, lifestyle, and environmental factors linked to this disease are summarized in Figure 1.
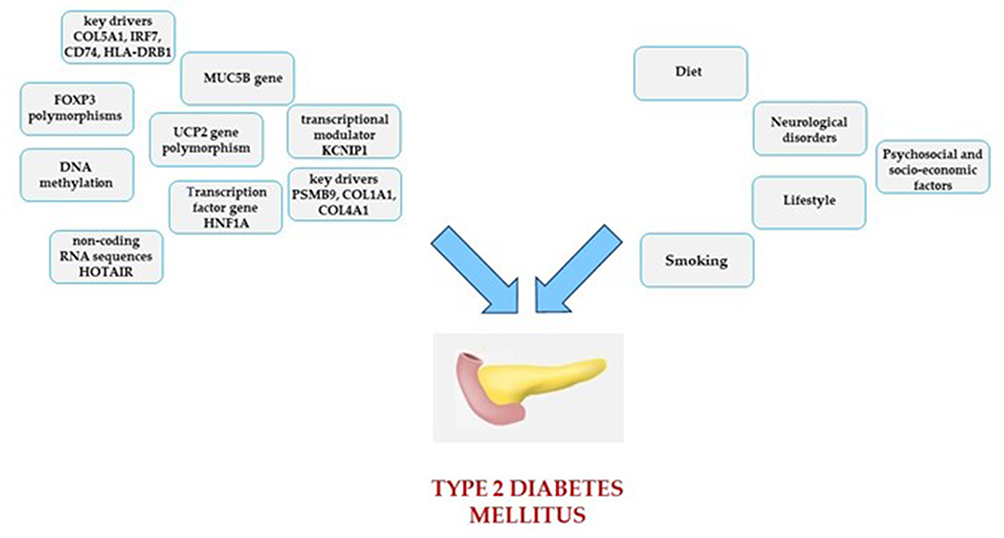 |
Figure 1 An example of main genomic, lifestyle and environmental factors linked to type 2 Diabetes Mellitus. |
Diet
The influence of diet is fundamental, not only to the development of the disease but also to the development of cardiovascular complications. In this regard, the most recent European Society of Cardiology (ESC) guidelines demonstrate, with an I B level of evidence, that a healthy diet is essential for the prevention of cardiovascular risk in all individuals.72
It is suitable to follow a Mediterranean diet and consume plants, including whole grains, fruits, vegetables, pulses, and nuts. In addition, subjects should prefer unsaturated fats to saturated fats, fish a couple of times a week rather than meat, to minimize alcohol and free sugar consumption.73–76
Many trials have demonstrated the effectiveness of the Mediterranean diet in reducing the risk of developing metabolic, cardiovascular, and other diseases (relative risk (RR) for comparing extreme quantiles: 0.87; 95% confidence interval (CI):0.82, 0.93). Diet patterns characterized by legumes, vegetables, poultry, fruits, and fish (“mainly healthy”) were inversely associated with T2DM (RR:0.84; 95% CI:0.77, 0.91). On the other hand, a diet with high consumption of processed meat, high-fat dairy, refined grains, fried products, and eggs (“mainly unhealthy”), seems positively associated with the development of T2DM (RR:1.44; 95% CI:1.27, 1.62).77–83
More recently, the ketogenic diet has stimulated the interest of many authors and nutritionists, also in subjects affected by T2DM. This diet has already been used in the past and even nowadays for the treatment of epilepsy. Ketogenic diet is based on the principle of reducing the consumption of a certain amount of carbohydrates, to a maximum of 50 g daily, and high fat content, moderate protein content, with the formation of ketone bodies as a source of energy.84–91
Some authors therefore suggest that a personalized approach could be useful, especially in those with visceral obesity, dyslipidemia, and high levels of transaminases.92
Intermittent Fasting is another type of diet characterized by two different phases. In one, the subject practices a low-calorie diet and, during the second, the subject eats without specific limitations. There are several types, mainly differentiated according to the duration of each phase.93 Some studies demonstrate that intermittent fasting can improve glycemic control in individuals with T2DM, while others fail to demonstrate such efficacy.94–98
In addition, many people around the world observe a month of Ramadan fasting during their life, according to their religious custom. For this reason, some authors have evaluated the impact of this kind of Intermittent Fasting on glycemic control in patients with T2DM. As a result, it has been observed that people observing a period of pre‐Ramadan assessment with clinicians, as a personalized approach, could improve metabolic balance and also prevent acute complications during and after Ramadan period.99,100
Nutrigenetics studies the role of genetic variants in the modulation of response to diet and the implications in the development, or prevention, of diseases. In particular, some genetic variants seem associated with diet response for what concerns the development of cardiovascular diseases, mainly obesity and diabetes.101 A study described a gene–diet interaction with the Mediterranean diet for both the FTO rs9939609 and for the MC4R rs17782313. People with these variant alleles showed a higher T2DM risk, as compared to wild-type subjects, when the Mediterranean diet was not followed. However, the association does not seem to be observed when subjects support a Mediterranean diet.102 Other studies have also described the interactions between different alleles and diet in modulating T2DM risk. In particular, for what concerns TCF7L2 rs7903146, wholegrain intake seems inversely associated with T2DM risk among CC carriers, whereas this protective effect comes lost in presence of the T-allele.103
Nutrition also seems to influence epigenetic modulation, especially through DNA methylation. In particular, early life nutritional experience, both during pre- and post-natal life, could seriously induce metabolic and physiological changes through altered offspring epigenetic profile. Maternal malnutrition can lead to different susceptibilities to various chronic diseases in subsequent years.104
Lifestyle
As recommended by the most recent guidelines, physical activity is one of the main therapeutic measures for both the general population and particularly for subjects with T2DM.72,105 It is recommended to practice 150–300 min of moderate-intensity aerobic activity per week. In elderly patients and those with chronic diseases, it is advisable to practice physical activity, as allowed by the underlying pathology.72 These measures can determine an improvement in metabolic parameters, HbA1c, and weight, and a reduction in the risk of micro and macrovascular complications.106 Some trials enrolling individuals at high cardiovascular risk have demonstrated that the risk of coronary heart disease can be reduced by 14–20%, as well as the risk of developing diabetes by 6% after approximately 10 years of follow-up.107–109 Exercise may also be favorable for pregnant women to preventing excessive weight and reduce the risk of developing gestational diabetes (6.8% vs 2.6%; odds ratio, 0.363; 95% confidence interval, 0.138–0.953; p=0.033).110
In presence of complications, it seems that personalized physical exercise can determine beneficial effects. Individuals with peripheral neuropathy can benefit from an exercise program with both aerobic and strengthening components showing, after 10 weeks of personalized training, reductions in pain, neuropathic symptoms, and increased intraepidermal nerve fiber branching (−18.1±35.5 mm on a 100 mm scale, P=0.05; −1.24±1.8 on MNSI, P=0.01; +0.11±0.15 branch nodes/fiber, P=0.008).111 Even individuals with diabetic nephropathy seem to benefit from physical exercises, both aerobic and anaerobic, as well as from aerobic exercises only. Although few trials are dedicated to this topic, those available have shown how home training can determine decreased urinary albumin-to-creatinine ratio, serum urea nitrogen, urinary protein-to-creatinine ratio, and urinary protein excretion.112 However, diet and lifestyle seem ineffective on other renal function outcomes (eg eGFR) and the sample size across randomized controlled trials is quite small. As a consequence and as limitations of studies, it is hard to identify subjects with different responses to the same interventions, thus the authors argue that in the future, new trials with large sample sizes will be required to better define the role of lifestyle in populations with diabetic nephropathy.
More recently, a study on subjects with non-proliferative diabetic retinopathy showed that after 12 weeks of a 45-min aerobic exercise program, 3 times a week, a lower fasting glycemia and central macular thickness could be observed.113 However, also here, it is not possible to identify different subgroups of diabetic subjects with different responses to the intervention, due to the small sample size and the endpoint of the study.
As above described, some literatures have identified different genetic clusters of T2DM subjects and associated genetic risk scores for developing cardiovascular diseases.43 Based on previous literature, other authors have thus evaluated the effects of lifestyle associated with genetic risk scores on a population of almost 35,000 individuals naïve for cardiovascular diseases.114 At the end of almost 20 years follow-up, 4,433 participants were diagnosed with type 2 diabetes. Subsequently, the authors identified a global polygenic score and different pathway associated scores (particularly describing insulin impaired secretion and insulin impaired sensitivity). The observed relative risk of T2DM for global polygenic score was 1.29 (95% confidence interval [CI] 1.25, 1.32; P < 0.001), while different risks were associated with pathway-specific polygenic scores (ranging from 1.26 [95% CI 1.22, 1.30; I 2 = 55.5%; P < 0.001] for the beta-cell dysfunction polygenic score to 1.09 [95% CI 1.05, 1.12; I 2 = 49.1%; P < 0.001] for the obesity-mediated insulin resistance polygenic score). Moreover, the population was also subdivided according to the genetic risk (low, intermediate, and high) and the quality of diet and lifestyle (low, intermediate, and high). At the end of the study, low-quality diet was associated with higher T2DM risk, independently from genetic risk. Moreover, high-quality diet and lifestyle was associated with lower T2DM risk across all classes of genetic risk.114 However, the efficacy of high-quality diet and lifestyle comes progressively lost proceeding from the low genetic risk subgroup to the high. The authors argue that this observation underlines the potential of genetic risk assessment for future risk stratification and surveillance.114
Neurological Disorders
T2DM is a chronic disease that affects patients from the time of diagnosis to exitus.115–119 In addition, T2DM can contribute to the development of anxious depressive conditions and is often associated with chronic neurological diseases.30,120
T2DM is associated with a 73% higher risk of developing all types of dementia, 56% of developing Alzheimer’s disease, and more than double the risk of developing vascular dementia compared to the general population.121,122 Moreover, women with diabetes seem to have a higher risk to develop vascular dementia than men. Accordingly, other authors showed a greater risk of cognitive decline of approximately 1.2-fold (95% CI 1.05–1.4) and 1.7-fold (95% CI 1.3–2.3) in the T2DM population compared to the healthy subjects. In addition, the same authors observed an almost doubled risk of developing future dementia (95% CI 1.4–1.8).123
Owing to the development of complications, T2DM is often a cause of disability, which greatly influences the patient’s quality of life.124 Furthermore, subjects with T2DM and disabilities are not able to maintain physical activity; therefore, their sedentary lifestyle does not allow them to obtain adequate glycemic control.124 Consistently, in a study of approximately 7000 elderly people with overweight/obesity and metabolic syndrome, executive functions were directly and negatively associated with T2DM, high BMI, and depressive symptoms. In addition, participants with good glycemic control (HbA1c<53 mmol/mol) showed better cognitive performance, treatment adherence, and quality of life.121,125
Insulin resistance, oxidative stress, inflammation, glycated end-products, and autophagy seem to be pathophysiological common mechanisms underlying the association between mental/neurological disorders and diabetes.126 This evidence has led several authors to evaluate whether antidiabetic drugs could have a positive role in the progression of cognitive impairment.127,128 It seems that some of them, especially metformin and glucagon-like peptide-1 receptor agonists (GLP-1 RA), could have a beneficial effect, not only on HbA1c and other metabolic factors but also on neurological functions.127,128 In particular, these drugs play neurotrophic and neuroprotective roles in central nervous system, by exerting anti-inflammatory effect and reducing Aβ aggregation/deposition and hyperphosphorylation of tau protein.127–129 Clinical consequences seem to be a reduction in cognitive impairment, improvement of cognitive subdomains of delayed memory, attention, and executive function in subjects who have assumed those drugs vs placebo. Consistently, literature provides evidence that treating some mental disorders could improve diabetes outcomes and contribute to the prevention of diabetes.130 However, a number of studies in this field are lacking, and sample size is often very small, with sometimes evidence inconsistent. For this reason, it is difficult to generalize those results and identify subgroups of subjects with different prognoses or different responses to anti-diabetic treatments, in order to stratify treatment recommendations based on mental disorders.130
More recently, some devices can support subjects affected by complicated T2DM and affected by disabilities and mental disorders. For example, role of telemedicine has spread in recent years, especially during the COVID-19 Pandemic.131 Thanks to the use of digital smart ophthalmoscope devices, it was possible to carry out remote retinal evaluation, also in subjects who could not refer to specialist centres, both for physical disabilities and long distances from the hospital care unit domicilio.132 Other recent examples of a technological device, which has allowed a personalized and therapeutic approach through telemedicine include the insulin pump and the blood sugar sensor.133,134 In subjects with T2DM, educational programs through optimal diabetes self-management education via telemedicine, have demonstrated good compliance and good glyco-metabolic compensation in enrolled populations.135,136 In this context, some authors have proposed a web-mediated approach to perform cognitive-behavioral therapy in patients with diabetes and depression. In the experimental arm, a significant reduction of depressive symptoms (41% vs 24%; p<0.001) but no effect on glyco-metabolic compensation was found.137 Therefore, the use of technological devices could favor a personalized approach in people who present neurological disorders and diabetes. However, to date, no such studies have enrolled subjects with T2DM and diagnosed mental disorders, in order to better confirm this hypothesis.130
Psychosocial and Socio-Economic Factors
Socioeconomic status (SES) describes the social condition of the participants based on their income, education, and occupation.138 Several studies have evaluated the association between SES, the prevalence of T2DM, and the prognosis of these patients. It can be argued that low SES is associated with a greater risk of developing diabetes [relative risk (RR) = 1.41, 95% confidence interval (CI):1.28–1.51], (RR = 1.31, 95% CI:1.09–1.57) and (RR = 1.40, 95% CI:1.04–1.88)].64,139 Moreover, subjects with low SES had worse glycol-metabolic control than those with high SES. Some results demonstrated that the pooled mean difference in HbA1c levels among the groups was 0.26% (95% CI, 0.09–0.43) or 3.12 mmol/mol (95% CI, 1.21–5.04) for education and 0.20% (95% CI, 0.05 to 0.46) or 2.36 mmol/mol (95% CI, 0.61 to 5.33) for income. A recent trial of almost 2000 subjects demonstrated a greater risk of developing T2DM (OR:1.48) and its complications (OR:0.71 and 0.88) in individuals with low SES, while higher education was associated with a 53–69% decreased risk of diabetic retinopathy.140,141
Precision Medicine to Address a Tailored Drug Intervention
Treatment Selection Approach in Diabetes
Treatment tailoring dates to the time of Hippocrates. In fact, Hippocrates’ hypothesis was “It is more important to know what sort of person has a disease than to know what sort of disease a person has”.142 However, the role of precision medicine has only increased in recent years owing to the growth of both new diagnostic and informatics tools, which has widened our understanding of the molecular basis (Figure 2).142
Most patients with T2DM respond to antihyperglycemic drugs. Only a minority of patients could be considered true non-responders. Thus, it appears clear that the main aim of precision medicine in T2DM is to identify patients who can benefit most from a specific drug class more than from the others.26 To achieve this, it is crucial to detect markers that can robustly predict a greater or lesser response to each drug class. However, among the single markers, none has emerged, presenting a huge effect. Thus, the use of a combination of these markers for personalized treatment has been proposed.
Metformin is widely acknowledged as the primary treatment choice for T2DM.143 However, there is growing evidence supporting the potential of Sodium-Glucose Cotransporter 2 inhibitors (SGLT2i) and GLP-1 RA as first-line therapies for type 2 diabetes, given their ability to enhance treatment outcomes. Despite the promising effects of SGLT2i and GLP-1 RA, the issue of cost-effectiveness remains a significant consideration. To achieve cost-effectiveness, a substantial reduction in the current costs of these treatments, amounting to at least 70%, would be necessary. Indeed, it would be worth exploring the possibility that in patients with genetically determined low responsiveness to metformin, the cost-effectiveness landscape might change. The main genetic variants influencing glycaemic response are summarized in Table 1. Nevertheless, further research and studies are required to better understand this aspect.144
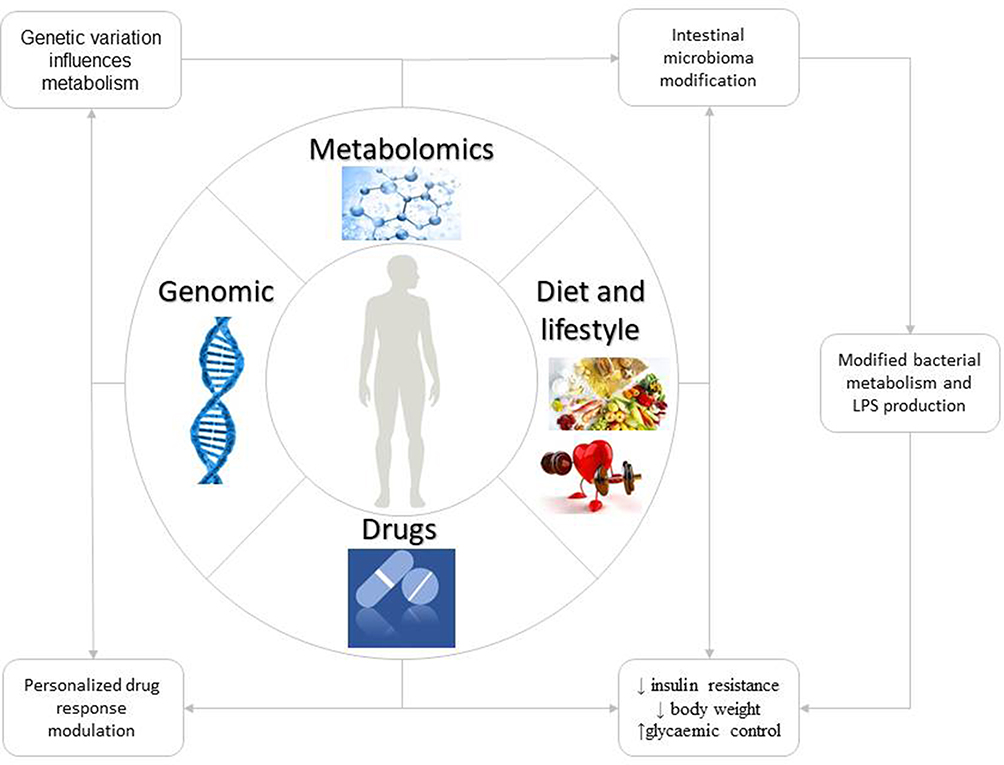 |
Figure 2 Potential applications of Precision Medicine. |
Metformin
Metformin primary actions include increasing glucose uptake by muscles, liver, and adipose tissues, as well as reducing hepatic glucose output, which results in improved insulin resistance. Moreover, metformin may influence the gut by promoting the release of incretins, enhancing insulin secretion, and improving glucose homeostasis.145 In addition, the insulin sensitizer effect seems to be beneficial for weight loss in obese patients (−0.62 [−1.00 to −0.25] kg vs placebo).146
As metformin is cleared through renal filtration, one of the primary concerns regarding its prescription is kidney insufficiency. In such cases, metformin blood levels may rise due to reduced excretion, leading to the risk of lactic acidosis. However, it is noteworthy that this complication is rare and has shown a decreasing trend over time.145–147 Moreover, the FDA has revised the metformin label to reflect its safety use in patients with an estimated glomerular filtration rate (eGFR) of 30 mL/min/1.73 m2.143
Studies on metformin have also made considerable progress in understanding the genetic basis underlying its therapeutic response. In a Genome-Wide Association Study (GWAS) analysis, researchers estimated the heritability of glucose response to metformin to be up to 34% (for the absolute reduction in HbA1c adjusted for pretreatment HbA1c) in patients with type 2 diabetes.148 Metformin is transported across cellular membranes via different isoforms of organic cation transporters (OCTs). These transporters are involved in the uptake of metformin into cells. The primary transporter involved in hepatic uptake is OCT1, which is encoded by the solute carrier family 22-member 1 (SLC22A1) gene. On the other hand, OCT2, encoded by SLC22A2, is primarily responsible for metformin’s tubular secretion.149,150
Genetic variants in these transporter molecules, as well as in multidrug and toxin extrusion (MATE) transporters responsible for metformin excretion through bile and urine, have been associated with both metformin efficacy and intolerance.151 For example, certain genetic variants in the SLC22A1 gene (OCT1), such as SNP rs622342 AA and rs594709, have been linked to increased response to metformin among South Indian and Chinese patients with T2DM, respectively.1,2 In another study of Chinese patients with T2DM, the SLC22A2 808G>T (rs316019) variant was associated with a greater reduction in HbA1c levels, along with reduced renal clearance of metformin.152 Likewise, several variants within the SLC22A2 gene (OCT2), namely rs201919874 and rs316019, were identified as being linked to decreased renal clearance of metformin and a consequent improvement in HbA1c levels.3,4 However, the latter association was observed in certain populations but not in others.5,153 Conversely, the variant rs10755577 did not exhibit any significant impact on glycemic control.6 Furthermore, carriers of the SLC47A1 rs2289669 variant in Chinese patients demonstrated an increased response to metformin.7 Conversely, the SLC47A2 (solute carrier family 47 member 2, encoding MATE2) variant rs12943590 was associated with a poor treatment response to metformin in a US population.8 However, the predictive insights have been modest.145,154
Sulfonylurea and Thiazolidinedione
With the spread of new drug therapies, the use of both Sulfonylurea and Thiazolidinedione is decreasing because of an increased risk of side effects as well as little effect on cardiovascular outcomes.143 Observational data from the UK Clinical Practice Research Datalink (CPRD), which enrolled approximately 22,000 patients starting sulfonylurea or thiazolidinedione therapy, reported that males without obesity benefit most from sulfonylurea treatment on glucose-lowering response rather than thiazolidinedione. Conversely, women with obesity showed a greater response to thiazolidinedione than sulfonylurea treatment.155 Notably, pioglitazone has proven to be effective in patients with non-alcoholic steatohepatitis (NASH) and T2DM, in reducing hepatic steatosis, inflammation, aspartate aminotransferase and alanine aminotransferase serum levels, and in improving liver fibrosis.156 However, further studies are needed to better assess this relationship and to include this treatment option in non-alcoholic fatty liver disease (NAFLD) treatment guidelines.
Information on sulfonylureas comes from decades of research and clinical experience. The best study example testing treatment response to genetic variation is the GoDARTS study, which reported reduced glycemic control achieved through sulfonylurea treatment in carriers of the TCF7L2 T2DM risk allele.11 In addition, various pharmacogenetic determinants have been investigated, encompassing genetic variations in genes associated with sulfonylurea metabolism, sulfonylurea receptors, insulin action, and β-cell function. These genes include CYP2C9, ABCC8, KCNJ11, IRS1, CDKAL1, CDKN2A, CDKN2B, KCNQ1, and NOS1AP.145,157 Among these, the sulfonylurea receptor-1 (SUR1) coding variant ABCC8 S1369A has been associated in functional studies with an enhanced treatment response to a particular subclass of sulfonylureas (gliclazide, an A-site sulfonylurea).9,158 Moreover, the metabolism of sulfonylureas is primarily mediated by cytochrome P450 2C9 (CYP2C9), and variants of this enzyme (rs1057910, rs1799853) result in reduced clearance of sulfonylureas and increased sensitivity to sulfonylureas therapy.10 Consequently, individuals carrying these CYP2C9 variants are recommended to take lower doses to minimize the risk of hypoglycemia.151 In addition, carriers of TCF7L2 gene variants, particularly the T/T genotype at rs12255372, which is well-known for its association with type 2 diabetes, have been found to exhibit reduced responsiveness to sulfonylureas.11 Besides pharmacogenetic responses, these varied genotype–treatment interactions may also reflect the extent of b-cell dysfunction influenced by these genetic variants, ultimately impacting the individual’s response to sulfonylureas therapy.
In contrast, thiazolidinediones’ understanding of the genetic determinants underlying beneficial or adverse therapeutic responses has been less investigated. In carriers of rs4149056 variants within SLCO1B1, which encodes the organic anion transporting polypeptide 1B1 (OATP1B1), the use of rosiglitazone enhanced glycemic response, and in carriers of variations within CYP2C8, encoding cytochrome P450 2C8 metabolizing enzyme (rs10509681), rosiglitazone was associated with reduced glycemic response and reduced weight gain. Moreover, these results did not appear to be applicable to pioglitazone therapy.12 Limited data from a small Asian sample size have highlighted that genetic variation in PPARγ rs1801282 and protein tyrosine phosphatase receptor type D (PTPRD) gene polymorphism rs17584499 are associated with increased responsivity to thiazolidinediones. However, this result was not confirmed by a previous study. Therefore, its clinical relevance remains uncertain.13,145
Acarbose
Acarbose is an α-glucosidase inhibitor with limited use in Western countries; however, it is widely used in some parts of Asia, particularly in China. Major benefits of acarbose treatment have been reported in the management of postprandial hyperglycemia as it delays carbohydrate digestion from the brush border of the small intestine. An old meta-analysis of seven randomized, double-blind, placebo-controlled acarbose studies (MeRIA7) found an association between the reduced incidence of cardiovascular events in T2DM and acarbose treatment (HR 0.65, 95% CI 0.48–0.88).159 However, none of the included trials were explicitly conducted to test this hypothesis, and the number of myocardial infarction was extremely low in both arms (19 in placebo vs 9 in acarbose treatment).160 The Acarbose Cardiovascular Evaluation (ACE) large-scale cardiovascular outcome trial reported that acarbose failed to reduce the risk of Major Adverse Cardiovascular Events but reduced the risk of new-onset diabetes by 18% for a median of 5.0 years follow-up.161
The STOP-NIDDM trial found associations between genetic variations in PPARα, HNF4A, LIPC, PPARG2, PPARGC1A, and acarbose treatment response in prediabetic patients.162 However, these associations are modest and have not been tested in patients with overt diabetes.
Dipeptidyl Peptidase 4 Inhibitors and Glucagon-Like Peptide-1 Receptor Agonist
A prospective predicting response to incretin-based agents (PRIBA) study reported that in patients with higher levels of insulin resistance (fasting C-peptide, HOMA2 insulin resistance, and triglycerides), treatment with Dipeptidyl Peptidase-4 Inhibitors (DPP-4is) is associated with a reduced glycaemic response.163 The same study highlighted an increased treatment response in patients with obesity and high triglyceride levels, compared to non-obese, low triglyceride subgroup, at 6-months evaluation (25.3 mmol/mol [20.5%] and 211.3 mmol/mol [21.0%], respectively). However, no evidence has been reported on the association between markers of insulin resistance and treatment response in patients initiating GLP-1RA.163 Similar findings were reported in non-insulin-treated diabetic patients from the UK National Health Service starting with GLP-1RA treatment. However, in the same study, a reduced glycemic response to GLP-1RAs was associated with a longer duration of diabetes, lower C-peptide levels, and positive glutamic acid decarboxylase (GAD) or Islet Antigen 2 (IA-2) autoantibodies.164 A recent systematic review showed that a higher baseline HbA1c level was associated with a greater treatment response to both DPP-4i and GLP-1RA therapies.165 In addition, DPP-4i treatment response seems to be increased in Asian ethnicity.166 There have been limited pharmacogenetic investigations concerning DPP-4i treatment efficacy to date. In one association study, researchers observed a correlation between rs7202877, located near CTRB1/2 (chymotrypsinogen B1/2), and a reduced HbA1c response to dipeptidyl peptidase-4 inhibitors.14 In addition, in an association study, researchers reported that the diabetes risk-related variant TCF7L2 rs7903146 was associated with a smaller reduction in HbA1c after linagliptin treatment in homozygous T-allele carriers, representing 10% of the patients.15 However, the role of other potential predictors remains unclear and requires further investigation. In a recent meta-analysis of 764 trials enrolling more than 400,000 diabetic patients, GLP-1RA have been proven to reduce the overall risk of all-cause cardiovascular mortality (OR 0.88, 95% CI 0.80–0.96), non-fatal myocardial infarction (OR 0.92, 95% CI 0.85–0.99), non-fatal stroke (OR 0.84, 95% CI 0.76–0.93), and kidney failure (OR 0.91, 95% CI 0.69–1.20), with an increasing benefit according to the risk profile. Moreover, GLP-1RA treatment may also lower body weight, with a mean difference of −1.45 kg (95% CI −1.72 to −1.18), which may be beneficial in obese patients.167
Genetic variants of the glucagon-like peptide 1 (GLP-1) receptor gene have been implicated in a reduced glycemic lowering response to DPP-4i treatment. Moreover, other gene variants (KCNQ1, KCNJ11, CTRB1/2, PRKD1, CDKAL1, IL6 promoter region, TCF7L2, DPP4, and PNPLA3) have been suggested to induce similar or minimal responses to DPP-4i treatment, although replication studies are lacking.168 Several studies investigating GLP1R variant allele carriers found a greater weight reduction benefit with GLP-1RA treatment.16,169 Other variants related to GLP-1RA response were cannabinoid receptor 1 (CNR1), TCF7L2, and SORCS1. The CNR1 A polymorphism (rs1049353) improved insulin resistance after liraglutide treatment owing to weight loss and glycaemic control improvement, whereas non-carriers of the A allele showed an improvement in cholesterol levels after weight loss.170 Carrier of TCF7L2 rs7903146 T allele showed a significant reduction in postprandial plasma insulin peak levels compared to non-carriers after exenatide treatment.17 Finally, it was highlighted that newly diagnosed type 2 diabetic patients carrying the SORCS1 gene rs1416406 with the GG genotype might benefit the most from early exenatide treatment.18
Sodium-Glucose Cotransporter 2 Inhibitors
Trial data analysis has shown an incremental reduction in HbA1c with increasing baseline HbA1c with SGLT2i treatment compared to DPP-4i or sulfonylureas.171,172 In a retrospective study enrolling more than 10,000 patients initiating Sodium-glucose co-transporter-2 inhibitors (SGLT2is), a greater response to SGLT2is treatment was reported in subjects with a higher estimated glomerular filtration rate (eGFR) and alanine transaminase.173 Several studies have reported a different response to SGLT2i treatment according to baseline renal function, with increasing efficacy with higher eGFR levels (90 vs 60–90 mL/min/1.73 m2).174–177 A recent prospective meta-analysis reported that SGLT2Is effectively improve liver function parameters in patients with diabetes and ameliorate alanine transaminase levels and liver steatosis in a prospective study.178,179 In a recent large-scale metanalysis, SGLT2i have been proven to reduce the overall risk of all-cause cardiovascular mortality (OR 0.85, 95% CI 0.79–0.92), non-fatal myocardial infarction (OR 0.87, 95% CI 0.79–0.97), admission for heart failure (OR 0.70, 95% CI 0.63–0.77), and kidney failure (OR 0.71, 95% CI 0.57–0.89), with an increasing benefit based on the risk profile. Moreover, SGLT2is treatment might also impact on body weight lowering, with a mean difference of 1.92 kg (95% CI −2.23 to −1.62).167
SGLT2 is encoded by the SLC5A2 gene, which is located on chromosome 16. It has been suggested that four intronic nucleotide polymorphisms within SLC5A2 could affect the SGLT2is response to treatment. However, a cross-sectional study enrolling 2600 diabetic patients showed that the SLC5A2 common genetic variants (rs9934336, rs9924771, rs3813008, and rs3116150) did not affect diabetes-related metabolic traits nor had a clinically relevant impact on SGLT2 treatment response.19
SGLT2 inhibitors are primarily eliminated through O-glucuronidation, a process facilitated by uridine diphosphate glucuronosyl-transferases (UGTs). A study involving 134 participants, comprising both healthy individuals and those with T2DM, revealed that individuals carrying the reduced-function variants UGT1A9*3 and UGT2B4*2 exhibited higher plasma concentrations of canagliflozin when compared to individuals with the wild-type alleles.180 However, a large population study including 9061 pharmacokinetic samples from 1616 volunteers (both healthy volunteers and type 2 diabetic patients) failed to prove that polymorphisms of genes encoding uridine 5’-diphospho-glucuronosyltransferase affected canagliflozin pharmacokinetics.20 Further studies are needed to assess the role of genetic variant’s role in SGLT2is treatment response.
Classification of Diabetes According to Multiple Subtypes
Evidence regarding the treatment response continues to increase over time, also for what concerns other diseases and systems.181–183 However, how this can be easily translated into current clinical practice remains debated. Currently, researchers are looking for methods to detect subtypes of diabetes in several phenotypes, which could help predict drug therapy responses. In 2018, Ahlqvist et al aimed to identify discrete subtypes of diabetes that could provide a powerful tool for personalized treatment regimen.184 By performing a cluster analysis of 8980 newly diagnosed diabetic patients from the Swedish All New Diabetics in Scania cohort, Ahlqvist et al identified five different diabetes subtypes. This distinction was made based on the following clinical variables: age at diagnosis, autoantibodies, BMI, HbA1c level, and estimates of β-cell function and insulin resistance. This clustering was further supported by similar results obtained in newly diagnosed patients and in longer-term diabetes by the C-peptide levels, which were relatively constant over time, and the clustering of established genetic associations differed between these subtypes. Moreover, the risk of complications differs across the subtypes. In particular, researchers reported that diabetic retinopathy was detected earlier in subjects presenting with relative insulin deficiency, whereas the risk of diabetic kidney disease increased in insulin-resistant patients.184 Several other researchers have attempted to validate and/or add new diabetes subtypes to improve targeted prevention and treatment, thus enabling a more accurate model for precision medicine applicability in diabetes and its complications.185–189 However, further studies are needed to assess the treatment response to different drug classes among the subtypes of diabetes, as well as to refine and improve this classification.
Limitations
Currently, there is an increase in medical demand owing to a growing life expectancy, which is accompanied by an increased number of comorbidities. The potential for treating a patient with a disease at best represents the optimal target. By estimating the different treatment responses to a specific treatment, we can implement clinical outcomes and reduce the onset of micro- and macrovascular complications. However, to do so, a better understanding of the underlying disease mechanisms, as well as of the pharmacogenetics is mandatory.26 Moreover, numerous challenges still exist in the future of precision medicine, including cost, ethics, Big Data security, and trained researchers being able to deal with these data and create new algorithms.190 However, one of the main questions is whether we truly need this complexity in diabetes management. In fact, several reports and studies have reported that making small improvements in any healthcare setting care delivery would have a bigger impact on our patient’s wellness than precision medicine.191 In fact, it has been reported in the STENO-2 trial that small changes in the intensity of multifactorial interventions were associated with a 50% reduction in the incidence of cardiovascular events, which was recently confirmed in the NID-2 study.192–195 This highlights the need to implement effective approaches beyond the development of new strategies. Another main issue is represented by increased health-care costs, which, of course, will lead to inequalities as, at least at the beginning, will be available within high-income countries and rich individuals.
Our study presents several limitations. We did not address some important aspects of precision medicine, described elsewhere by other authors. First of all, it lacks a section describing adverse drug reactions that can be evaluated through a pre-emptive genotyping strategy. Some authors have recently observed the importance of this approach in reducing the incidence of adverse drug reactions.196 Secondly, an evaluation of the pathways involved through the cardiovascular response to intensive glycaemic control obtained from specific drugs (eg GLP-1 agonists and fibrates) has not been described.197–199
Conclusions
In summary, our perspective underscores the evolving potential of precision medicine in revolutionizing the landscape of diabetes management. While the existing evidence does not robustly support its widespread use based on genetic variants, algorithms, and drug responses, the future holds immense promise. To fully harness this potential, it is imperative to enhance the availability of novel clinical markers. Lowering the cost of genetic variant analysis can enable specialists to categorize patients effectively, predicting prognosis and treatment responses with higher precision. Additionally, the integration of genetic markers and clinical data from electronic records into advanced algorithms stands as a beacon of progress. These innovative algorithms can pave the way for tailored clinical approaches in treating patients with T2DM. Moreover, the application of data-driven machine learning and artificial intelligence offers exciting possibilities. These approaches can decipher complex genetic and clinical data, leading to the creation of new predictive models. This, in turn, facilitates a more comprehensive and customized therapeutic approach for patients with T2DM. In light of these advancements, it is crucial to focus on refining precision medicine applications. Conducting rigorous and insightful future trials will be instrumental. These trials should explore the full spectrum of possibilities that precision medicine offers. Through ongoing research and continuous improvement, we can unlock the true potential of precision medicine, ensuring its transformative impact on diabetes care and paving the way for a future where personalized and effective treatments are the norm.
Abbreviations
DPP-4is, Dipeptidyl Peptidase-4 Inhibitors; DMCs, differentially methylated CpGs; DMRs, differentially methylated regions; ESC, European Society of Cardiology; GLP-1RA, Glucagon-Like Peptide-1 Receptor Agonist; HR, hazard ratio; KCNIP, 1 Kv channel-interacting protein 1; RR, risk ratio; socioeconomic status; SGLT2i, Sodium-Glucose cotransporter 2 inhibitors; T2DM, type 2 diabetes mellitus; T1DM, type 1 diabetes; UCP2, uncoupling protein 2; SES.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Umamaheswaran G, Praveen RG, Damodaran SE, Das AK, Adithan C. Influence of SLC22A1 rs622342 genetic polymorphism on metformin response in South Indian type 2 diabetes mellitus patients. Clin Exp Med. 2015;15(4):511–517. doi:10.1007/s10238-014-0322-5
2. Xiao D, Guo Y, Li X, et al. The Impacts of SLC22A1 rs594709 and SLC47A1 rs2289669 Polymorphisms on Metformin Therapeutic Efficacy in Chinese Type 2 Diabetes Patients. Int J Endocrinol. 2016;2016:4350712. doi:10.1155/2016/4350712
3. Moeez S, Khalid Z, Jalil F, et al. Effects of SLC22A2 (rs201919874) and SLC47A2 (rs138244461) genetic variants on metformin pharmacokinetics in Pakistani T2DM patients. J Pak Med Assoc. 2019;69:155–163.
4. Song IS, Shin HJ, Shim EJ, et al. Genetic variants of the organic cation transporter 2 influence the disposition of metformin. Clin Pharmacol Ther. 2008;84(5):559–562. doi:10.1038/clpt.2008.61
5. Resendiz-Abarca CA, Flores-Alfaro E, Suarez-Sanchez F, et al. Altered glycemic control associated with polymorphisms in the SLC22A1 (OCT1) gene in a Mexican population with type 2 diabetes mellitus treated with metformin: a cohort study. J Clin Pharmacol. 2019;59:1384–1390. doi:10.1002/jcph.1425
6. Phani NM, Vohra M, Kakar A, et al. Implication of critical pharmacokinetic gene variants on therapeutic response to metformin in type 2 diabetes. Pharmacogenomics. 2018;19:905–911. doi:10.2217/pgs-2018-0041
7. He R, Zhang D, Lu W, et al. SLC47A1 gene rs2289669 G>A variants enhance the glucose-lowering effect of metformin via delaying its excretion in Chinese type 2 diabetes patients. Diabetes Res Clin Pract. 2015;109(1):57–63. doi:10.1016/j.diabres.2015.05.003
8. Choi JH, Yee SW, Ramirez AH, et al. A common 5’-UTR variant in MATE2-K is associated with poor response to metformin. Clin Pharmacol Ther. 2011;90(5):674–684. doi:10.1038/clpt.2011.165
9. Fatehi M, Raja M, Carter C, Soliman D, Holt A, Light PE. The ATP-sensitive K(+) channel ABCC8 S1369A type 2 diabetes risk variant increases MgATPase activity. Diabetes. 2012;61(1):241–249. PMID: 22187380; PMCID: PMC3237651. doi:10.2337/db11-0371
10. Hansen T, Ambye L, Grarup N, et al. Genetic variability of the SUR1 promoter in relation to beta-cell function and Type II diabetes mellitus. Diabetologia. 2001;44:1330–1334. doi:10.1007/s001250100651
11. Pearson ER, Donnelly LA, Kimber C, et al. Variation in TCF7L2 influences therapeutic response to sulfonylureas: a GoDARTs study. Diabetes. 2007;56:2178–2182. doi:10.2337/db07-0440
12. Dawed AY, Donnelly L, Tavendale R, et al.CYP2C8 and SLCO1B1 Variants and Therapeutic Response to Thiazolidinediones in Patients With Type 2 Diabetes. Diabetes Care. 2016;39(11):1902–1908. PMID: 27271184. doi:10.2337/dc15-2464
13. Pei Q, Huang Q, Yang GP, et al. PPAR-γ2 and PTPRD gene polymorphisms influence type 2 diabetes patients’ response to pioglitazone in China. Acta Pharmacol Sin. 2013;34(2):255–261. doi:10.1038/aps.2012.144
14. Hart LM, Fritsche A, Nijpels G, et al.The CTRB1/2 locus affects diabetes susceptibility and treatment via the incretin pathway. Diabetes. 2013;62(9):3275–3281. PMID: 23674605; PMCID: PMC3749354. doi:10.2337/db13-0227
15. Zimdahl H, Ittrich C, Graefe-Mody U, et al. Influence of TCF7L2 gene variants on the therapeutic response to the dipeptidylpeptidase-4 inhibitor linagliptin. Diabetologia. 2014;57(9):1869–1875. PMID: 24906949; PMCID: PMC4119242. doi:10.1007/s00125-014-3276-y
16. de Luis DA, Diaz Soto G, Izaola O, et al. Evaluation of weight loss and metabolic changes in diabetic patients treated with liraglutide, effect of RS 6923761 gene variant of glucagon-like peptide 1 receptor. J Diabetes Complicat. 2015;29(4):595–598. doi:10.1016/j.jdiacomp.2015.02.010
17. Ferreira MC, da Silva MER, Fukui RT, et al. Effect of TCF7L2 polymorphism on pancreatic hormones after exenatide in type 2 diabetes. Diabetol Metab Syndr. 2019;11:10. PMID: 30700996; PMCID: PMC6347826. doi:10.1186/s13098-019-0401-6
18. hou LM, Xu W, Yan XM, Li MXY, Liang H, Weng JP. Association between SORCS1 rs1416406 and therapeutic effect of exenatide. Zhonghua Yi Xue Za Zhi. 2017;97(18):1415–1419. doi:10.3760/cma.j.issn.0376-2491.2017.18.0131
19. Zimdahl H, Haupt A, Brendel M, et al. Influence of common polymorphisms in the SLC5A2 gene on metabolic traits in subjects at increased risk of diabetes and on response to empagliflozin treatment in patients with diabetes. Pharmacogenet Genomics. 2017;27(4):135–142. PMID: 28134748. doi:10.1097/FPC.0000000000000268
20. Hoeben E, De Winter W, Neyens M, et al. Population Pharmacokinetic Modeling of Canagliflozin in Healthy Volunteers and Patients with Type 2 Diabetes Mellitus. Clin Pharmacokinet. 2016;55(2):209–223. PMID: 26293616. doi:10.1007/s40262-015-0307-x
21. Bonnefond A, Unnikrishnan R, Doria A, et al. Monogenic diabetes. Nat Rev Dis Primers. 2023;9(1):12. doi:10.1038/s41572-023-00421-w
22. Shepherd M, Shields B, Hammersley S, et al. Systematic population screening, using biomarkers and genetic testing, identifies 2·5% of the UK pediatric diabetes population with monogenic diabetes. Diabetes Care. 2016;39:1879–1888. doi:10.2337/dc16-0645
23. Pearson ER, Flechtner I, Njølstad PR, et al.; Neonatal Diabetes International Collaborative Group. Switching from insulin to oral sulfonylureas in patients with diabetes due to Kir6.2 mutations. N Engl J Med. 2006; 355(5):467–477. doi:10.1056/NEJMoa061759
24. Gloyn AL, Pearson ER, Antcliff JF, et al. Activating mutations in the gene encoding the ATP-sensitive potassium-channel subunit Kir6.2 and permanent neonatal diabetes. N Engl J Med. 2004;350(18):1838–1849. doi:10.1056/NEJMoa032922
25. Rafiq M, Flanagan SE, Patch AM, et al. Effective treatment with oral sulfonylureas in patients with diabetes due to sulfonylurea receptor 1 (SUR1) mutations. Diabetes Care. 2008;31(2):204–209. doi:10.2337/dc07-1785
26. Dennis JM. Precision Medicine in Type 2 Diabetes: using Individualized Prediction Models to Optimize Selection of Treatment. Diabetes. 2020;69(10):2075–2085. PMID: 32843566; PMCID: PMC7506836. doi:10.2337/dbi20-0002
27. Gloyn AL, Drucker DJ. Precision medicine in the management of type 2 diabetes. Lancet Diabetes Endocrinol. 2018;6(11):891–900. PMID: 29699867. doi:10.1016/S2213-8587(18)30052-4
28. Morris AP, Voight BF, Teslovich TM, et al. Large-scale association analysis provides insights into the genetic architecture and pathophysiology of type 2 diabetes. Nat Genet. 2012;44(9):981–990. doi:10.1038/ng.2383
29. Sladek R, Rocheleau G, Rung J, et al. A genome-wide association study identifies novel risk loci for type 2 diabetes. Nature. 2007;445(7130):881–885. doi:10.1038/nature05616
30. Saxena R, Voight BF, et al.; Diabetes Genetics Initiative of Broad Institute of Harvard and MIT, Lund University, and Novartis Institutes of BioMedical Research. Genome-wide association analysis identifies loci for type 2 diabetes and triglyceride levels. Science. 2007;316(5829):1331–1336. doi:10.1126/science.1142358
31. Scott LJ, Mohlke KL, Bonnycastle LL, et al. A genome-wide association study of type 2 diabetes in Finns detects multiple susceptibility variants. Science. 2007;316(5829):1341–1345. doi:10.1126/science.1142382
32. Steinthorsdottir V, Thorleifsson G, Reynisdottir I, et al. A variant in CDKAL1 influences insulin response and risk of type 2 diabetes. Nat Genet. 2007;39(6):770–775. doi:10.1038/ng2043
33. Zeggini E, Weedon MN, Lindgren CM, et al. Replication of genome-wide association signals in UK samples reveals risk loci for type 2 diabetes. Science. 2007;316(5829):1336–1341. doi:10.1126/science.1142364
34. Chen J, Spracklen CN, Marenne G, et al. The trans-ancestral genomic architecture of glycemic traits. Nat Genet. 2021;53(6):840–860. doi:10.1038/s41588-021-00852-9
35. Scott RA, Scott LJ, Mägi R, et al. An Expanded Genome-Wide Association Study of Type 2 Diabetes in Europeans. Diabetes. 2017;66(11):2888–2902. doi:10.2337/db16-1253
36. Laakso M, Fernandes Silva L. Genetics of Type 2 Diabetes: past, Present, and Future. Nutrients. 2022;14(15):3201. doi:10.3390/nu14153201
37. Baca P, Barajas-Olmos F, Mirzaeicheshmeh E, et al. DNA methylation and gene expression analysis in adipose tissue to identify new loci associated with T2D development in obesity. Nutr Diabetes. 2022;12(1):50. PMID: 36535927; PMCID: PMC9763387. doi:10.1038/s41387-022-00228-w
38. Domingo-Relloso A, Gribble MO, Riffo-Campos AL, et al. Epigenetics of type 2 diabetes and diabetes-related outcomes in the Strong Heart Study. Clin Epigenetics. 2022;14(1):177. PMID: 36529747; PMCID: PMC9759920. doi:10.1186/s13148-022-01392-7
39. Eftekharian MM, Sayad A, Omrani MD, et al. Single nucleotide polymorphisms in the FOXP3 gene are associated with increased risk of relapsing-remitting multiple sclerosis. Hum Antibodies. 2016;24(3–4):85–90. doi:10.3233/HAB-160299
40. Khalifa O, Pers YM, Ferreira R, et al. X-Linked miRNAs Associated with Gender Differences in Rheumatoid Arthritis. Int J Mol Sci. 2016;17(11):1852. doi:10.3390/ijms17111852
41. Wang X, Liu Z, Zhang S, et al. Forkhead box P3 gene polymorphisms predispose to type 2 diabetes and diabetic nephropathy in the Han Chinese populations: a genetic-association and gender-based evaluation study. Hereditas. 2023;160(1):1–2. doi:10.1186/s41065-023-00264-1
42. Liu J, Li L, Li WJ, et al. The role of uncoupling proteins in diabetes mellitus. J Diabetes Res. 2013;2013:1–7.
43. Udler MS, Kim J, von Grotthuss M, et al. Type 2 diabetes genetic loci informed by multi-trait associations point to disease mechanisms and subtypes: a soft clustering analysis. PLoS Med. 2018;15(9):e1002654. doi:10.1371/journal.pmed.1002654
44. Brand MD, Parker N, Afourtit C, et al. Mitochondrial uncoupling protein 2 in pancreatic beta-cells. Diabetes Obes Metab. 2010;12:134–140. doi:10.1111/j.1463-1326.2010.01264.x
45. Brand MD, Esteves TC. Physiological functions of the mitochondrial uncoupling proteins UCP2 and UCP3. Cell Metab. 2005;2:85–93. doi:10.1016/j.cmet.2005.06.002
46. Sasahara M, Nishi M, Kawashima H, et al. Uncoupling protein 2 promoter polymorphism −866G/A affects its expression in beta-cells and modulates clinical profiles of Japanese type 2 diabetes patients. Diabetes. 2004;53(2):482–485. doi:10.2337/diabetes.53.2.482
47. Gluckman PD, Hanson MA, Buklijas T, Low FM, Beedle AS. Epigenetic mechanisms that underpin metabolic and cardiovascular diseases. Nat Rev Endocrinol. 2009;5(7):401–408. doi:10.1038/nrendo.2009.102
48. Wang S, Se YM, Liu ZQ, et al. Effect of genetic polymorphism of UCP2- 866 G/A on repaglinide response in Chinese patients with type 2 diabetes. Pharmazie. 2012;67(1):74–79.
49. Din I, Majid S, Rashid F, et al. Mitochondrial uncoupling protein 2 (UCP2) gene polymorphism - 866 G/A in the promoter region is associated with type 2 diabetes mellitus among Kashmiri population of Northern India. Mol Biol Rep. 2023;50(1):475–483. doi:10.1007/s11033-022-08055-z
50. Chen YT, Lin WD, Liao WL, Tsai YC, Liao JW, Tsai FJ. NT5C2 methylation regulatory interplay between DNMT1 and insulin receptor in type 2 diabetes [published correction appears in Sci Rep. 2021 Mar 22;11(1):6961]. Sci Rep. 2020;10(1):16087. doi:10.1038/s41598-020-71336-9
51. Lawlor N, George J, Bolisetty M, et al. Single-cell transcriptomes identify human islet cell signatures and reveal cell-type-specific expression changes in type 2 diabetes. Genome Res. 2017;27(2):208–222. doi:10.1101/gr.212720.116
52. Liu J, Liu S, Yu Z, et al. Uncovering the gene regulatory network of type 2 diabetes through multi-omic data integration. J Transl Med. 2022;20(1):604. doi:10.1186/s12967-022-03826-5
53. Clish CB. Metabolomics: an emerging but powerful tool for precision medicine. Cold Spring Harb Mol Case Stud. 2015;1(1):
54. Wang TJ, Larson MG, Vasan RS, et al. Metabolite profiles and the risk of developing diabetes. Nat Med. 2011;17(4):448–453. PMID: 21423183; PMCID: PMC3126616. doi:10.1038/nm.2307
55. Wang TJ, Ngo D, Psychogios N, et al. 2-Aminoadipic acid is a biomarker for diabetes risk. J Clin Invest. 2013;123(10):4309–4317. doi:10.1172/JCI64801
56. Meng J, Huang F, Shi J, et al. Integrated biomarker profiling of the metabolome associated with type 2 diabetes mellitus among Tibetan in China. Diabetol Metab Syndr. 2023;15(1):146. doi:10.1186/s13098-023-01124-8
57. Ben Othman M, Sakamoto K. Effect of inactivated Bifidobacterium longum intake on obese diabetes model mice (TSOD). Food Res Int. 2020;129:108792. PMID: 32036897. doi:10.1016/j.foodres.2019.108792
58. Kwek E, Yan C, Ding H, et al. Effects of hawthorn seed oil on plasma cholesterol and gut microbiota. Nutr Metab (Lond). 2022;19(1):55. PMID: 35962418; PMCID: PMC9373405. doi:10.1186/s12986-022-00690-4
59. Wang H, Shen Q, Fu Y, et al. Effects on Diabetic Mice of Consuming Lipid Extracted from Foxtail Millet (Setaria italica): gut Microbiota Analysis and Serum Metabolomics. J Agric Food Chem. 2023;71(26):10075–10086. doi:10.1021/acs.jafc.3c02179
60. Jin Z, Hu W, Yang Y. Serum metabolomic analysis revealed potential metabolite biomarkers for diabetes mellitus with coronary heart disease. Anal Methods. 2023;15(28):3432–3438. PMID: 37434552. doi:10.1039/d3ay00778b
61. Shi C, Wan Y, He A, et al. Urinary metabolites associate with the presence of diabetic kidney disease in type 2 diabetes and mediate the effect of inflammation on kidney complication. Acta Diabetol. 2023;60(9):1199–1207. PMID: 37184672; PMCID: PMC10359369. doi:10.1007/s00592-023-02094-z
62. Fang J, Wang H, Niu T, et al. Integration of Vitreous Lipidomics and Metabolomics for Comprehensive Understanding of the Pathogenesis of Proliferative Diabetic Retinopathy. J Proteome Res. 2023;22(7):2293–2306. PMID: 37329324. doi:10.1021/acs.jproteome.3c00007
63. Gary-Webb TL, Suglia SF, Tehranifar P. Social epidemiology of diabetes and associated conditions. Curr Diab Rep. 2013;13(6):850–859. doi:10.1007/s11892-013-0427-3
64. Agardh E, Allebeck P, Hallqvist J, et al. Type 2 diabetes incidence and socio-economic position: a systematic review and meta-analysis. Int J Epidemiol. 2011;40(3):804–818. doi:10.1093/ije/dyr029
65. NDC Risk Factor Collaboration. Worldwide trends in diabetes since 1980: a pooled analysis of 751 population-based studies with 4.4 million participants. Lancet. 2016;387:1513–1530. doi:10.1016/S0140-6736(16)00618-8
66. Chatterjee S, Khunti K, Davies MJ. Type 2 diabetes. Lancet. 2017;389(10085):2239–2251. doi:10.1016/S0140-6736(17)30058-2
67. Ng M, Fleming T, Robinson M, et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2014;384:766–781. doi:10.1016/S0140-6736(14)60460-8
68. Ma RC, Chan JC. Type 2 diabetes in East Asians: similarities and differences with populations in Europe and the United States. Ann N Y Acad Sci. 2013;1281::64–91. doi:10.1111/nyas.12098
69. Unnikrishnan R, Anjana RM, Mohan V. Diabetes in South Asians: is the phenotype different? Diabetes. 2014;63:53–55. doi:10.2337/db13-1592
70. Ding C, Chan Z, Magkos F. Lean, but not healthy: the ‘metabolically obese, normal-weight’ phenotype. Curr Opin Clin Nutr Metab Care. 2016;19:408–417. doi:10.1097/MCO.0000000000000317
71. Wang DD, Hu FB. Precision nutrition for prevention and management of type 2 diabetes. Lancet Diabetes Endocrinol. 2018;6(5):416–426. doi:10.1016/S2213-8587(18)30037-8
72. Visseren FLJ, Mach F, Smulders YM, et al. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice. Eur J Prev Cardiol. 2022;29(1):5–115. doi:10.1093/eurjpc/zwab154
73. Willett W, Rockström J, Loken B, et al. Food in the Anthropocene: the EAT-Lancet Commission on healthy diets from sustainable food systems [published correction appears in Lancet. 2019 Feb 9;393(10171):530] [published correction appears in Lancet. 2019 Jun 29;393(10191):2590] [published correction appears in Lancet. 2020 Feb 1;395(10221):338] [published correction appears in Lancet. 2020 Oct 3;396(10256):e56]. Lancet. 2019;393(10170):447–492. doi:10.1016/S0140-6736(18)31788-4
74. Ma Y, He FJ, Yin Y, et al. Gradual reduction of sugar in soft drinks without substitution as a strategy to reduce overweight, obesity, and type 2 diabetes: a modelling study. Lancet Diabetes Endocrinol. 2016;4(2):105–114. doi:10.1016/S2213-8587(15)00477-5
75. Kolb H, Martin S. Environmental/lifestyle factors in the pathogenesis and prevention of type 2 diabetes. BMC Med. 2017;15(1):131. doi:10.1186/s12916-017-0901-x
76. Dendup T, Feng X, Clingan S, Astell-Burt T. Environmental Risk Factors for Developing Type 2 Diabetes Mellitus: a Systematic Review. Int. J Environ Res Public Health. 2018;15(1):78. doi:10.3390/ijerph15010078
77. Jannasch F, Kröger J, Schulze MB. Dietary Patterns and Type 2 Diabetes: a Systematic Literature Review and Meta-Analysis of Prospective Studies. J Nutr. 2017;147(6):1174–1182. doi:10.3945/jn.116.242552
78. Yanai H, Hamasaki H, Katsuyama H, Adachi H, Moriyama S, Sako A. Effects of intake of fish or fish oils on the development of diabetes. J Clin Med Res. 2015;7(1):8–12. PMID: 25368695; PMCID: PMC4217746. doi:10.14740/jocmr1964w
79. Shin JY, Xun P, Nakamura Y, He K. Egg consumption in relation to risk of cardiovascular disease and diabetes: a systematic review and meta-analysis. Am. J Clin Nutr. 2013;98(1):146–159. doi:10.3945/ajcn.112.051318
80. Satija A, Bhupathiraju SN, Rimm EB, et al. Plant-Based Dietary Patterns and Incidence of Type 2 Diabetes in US Men and Women: results from Three Prospective Cohort Studies. PLoS Med. 2016;13(6):e1002039. doi:10.1371/journal.pmed.1002039
81. Gardner CD, Landry MJ, Perelman D, et al. Effect of a ketogenic diet versus Mediterranean diet on glycated hemoglobin in individuals with prediabetes and type 2 diabetes mellitus: the interventional Keto-Med randomized crossover trial [published correction appears in Am J Clin Nutr. 2022 Dec 19; 116(6):1904]. Am J Clin Nutr. 2022;116(3):640–652. doi:10.1093/ajcn/nqac154
82. Vitale M, Masulli M, Calabrese I, et al. Impact of a Mediterranean Dietary Pattern and Its Components on Cardiovascular Risk Factors, Glucose Control, and Body Weight in People with Type 2 Diabetes: a Real-Life Study. Nutrients. 2018;10(8):1067. doi:10.3390/nu10081067
83. Alonso-Domínguez R, García-Ortiz L, Patino-Alonso MC, Sánchez-Aguadero N, Gómez-Marcos MA, Recio-Rodríguez JI. Effectiveness of A Multifactorial Intervention in Increasing Adherence to the Mediterranean Diet among Patients with Diabetes Mellitus Type 2: a Controlled and Randomized Study (EMID Study). Nutrients. 2019;11(1):162. doi:10.3390/nu11010162
84. Wilder RMA. The effects of ketonemia on the course of epilepsy. Mayo Clin Bull. 1921;2:307.
85. Wilson J, Lowery R. The Ketogenic Bible. Las Vegas, NV, USA: Victory Belt Publishing Inc.; 2017. ISBN 13:978-1-628601-04-6.
86. Rafiullah M, Musambil M, David SK. Effect of a very low-carbohydrate ketogenic diet vs recommended diets in patients with type 2 diabetes: a meta-analysis. Nutr Rev. 2022;80:488–502. doi:10.1093/nutrit/nuab040
87. Li S, Lin G, Chen J, et al. The effect of periodic ketogenic diet on newly diagnosed overweight or obese patients with type 2 diabetes. BMC Endocr Disord. 2022;22:34. CrossRef. doi:10.1186/s12902-022-00947-2
88. Gardner CD, Landry MJ, Perelman D, et al. Effect of a ketogenic diet versus Mediterranean diet on glycated hemoglobin in individuals with prediabetes and type 2 diabetes mellitus: the interventional Keto-Med randomized crossover trial. Am J Clin Nutr. 2022;116:640–652. Erratum in Am. J. Clin. Nutr. 2022 Nov. 09. [CrossRef]. doi:10.1093/ajcn/nqac154
89. Saslow LR, Kim S, Daubenmier JJ, et al. A randomized pilot trial of a moderate carbohydrate diet compared to a very low carbohydrate diet in overweight or obese individuals with type 2 diabetes mellitus or prediabetes. PLoS One. 2014;9:e91027. doi:10.1371/journal.pone.0091027
90. Saslow LR, Daubenmier JJ, Moskowitz JT, et al. Twelve-month outcomes of a randomized trial of a moderate-carbohydrate versus very low-carbohydrate diet in overweight adults with type 2 diabetes mellitus or prediabetes. Nutr Diabetes. 2017;7:304. doi:10.1038/s41387-017-0006-9
91. Landry MJ, Crimarco A, Perelman D, et al. Adherence to Ketogenic and Mediterranean Study Diets in a Crossover Trial: the Keto-Med Randomized Trial. Nutrients.2021;13:967. doi:10.3390/nu13030967
92. Dyńka D, Kowalcze K, Ambrozkiewicz F, Paziewska A. Effect of the Ketogenic Diet on the Prophylaxis and Treatment of Diabetes Mellitus: a Review of the Meta-Analyses and Clinical Trials. Nutrients. 2023;15(3):500. PMID: 36771207; PMCID: PMC9919384. doi:10.3390/nu15030500
93. Sharma SK, Mudgal SK, Kalra S, Gaur R, Thakur K, Agarwal R. Effect of Intermittent Fasting on Glycaemic Control in Patients With Type 2 Diabetes Mellitus: a Systematic Review and Meta-analysis of Randomized Controlled Trials. REV Endocrinol. 2023;19(1):25–32. PMID: 37313231; PMCID: PMC10258621. doi:10.17925/EE.2023.19.1.25
94. Yang X, Zhou J, Shao H, et al. Effect of an Intermittent Calorie-restricted Diet on Type 2 Diabetes Remission: a Randomized Controlled Trial. J Clin Endocrinol Metab. 2023;108(6):1415–1424. PMID: 36515429. doi:10.1210/clinem/dgac661
95. Cienfuegos S, Gabel K, Kalam F, et al. Effects of 4- and 6-h time-restricted feeding on weight and cardiometabolic health: a randomized controlled trial in adults with obesity. Cell Metab. 2020;32:366–78.e3. doi:10.1016/j.cmet.2020.06.018
96. Carter S, Clifton PM, Keogh JB. Effect of intermittent compared with continuous energy restricted diet on glycemic control in patients with type 2 diabetes: a randomized noninferiority trial. JAMA Netw Open. 2018;1:e180756.
97. Carter S, Clifton PM, Keogh JB. The effects of intermittent compared to continuous energy restriction on glycaemic control in type 2 diabetes; a pragmatic pilot trial. Diabetes Res Clin Pract. 2016;122:106–112. doi:10.1016/j.diabres.2016.10.010
98. Khalfallah M, Elnagar B, Soliman SS, Eissa A, Allaithy A. The Value of Intermittent Fasting and Low Carbohydrate Diet in Prediabetic Patients for the Prevention of Cardiovascular Diseases. Arq Bras Cardiol. 2023. 120(4):e20220606. English, Portuguese. PMID: 37042857. doi:10.36660/abc.20220606
99. Ibrahim M, Barker MM, Ahmad E, et al. Optimizing Ramadan fasting: a randomised controlled trial for people with type 2 diabetes during Ramadan applying the principles of the ADA/EASD consensus. Diabetes Metab Res Rev. 2023;39(3):e3604. PMID: 36547366. doi:10.1002/dmrr.3604
100. Elmajnoun HK, Faris ME, Abdelrahim DN, Haris PI, Abu-Median AB. Effects of Ramadan Fasting on Glycaemic Control Among Patients with Type 2 Diabetes: systematic Review and Meta-analysis of Observational Studies. Diabetes Ther. 2023;14(3):479–496. PMID: 36725794; PMCID: PMC9981835. doi:10.1007/s13300-022-01363-4
101. Franzago M, Santurbano D, Vitacolonna E, Stuppia L. Genes and Diet in the Prevention of Chronic Diseases in Future Generations. Int. J Mol Sci. 2020;21(7):2633. doi:10.3390/ijms21072633
102. Ortega-Azorín C, Sorlí JV, Asensio EM, et al. Associations of the FTO rs9939609 and the MC4R rs17782313 polymorphisms with type 2 diabetes are modulated by diet, being higher when adherence to the Mediterranean diet pattern is low. Cardiovasc Diabetol. 2012;11(137). doi:10.1186/1475-2840-11-137
103. Fisher E, Boeing H, Fritsche A, Doering F, Joost HG, Schulze MB. Whole-grain consumption and transcription factor-7-like 2 (TCF7L2) rs7903146: gene-diet interaction in modulating type 2 diabetes risk. Br. J Nutr. 2009;101(4):478–481. doi:10.1017/S0007114508020369
104. Bordoni L, Gabbianelli R. Primers on nutrigenetics and nutri(epi)genomics: origins and development of precision nutrition. Biochimie. 2019;160:156–171. doi:10.1016/j.biochi.2019.03.006
105. Kanaley JA, Colberg SR, Corcoran MH, et al. Exercise/Physical Activity in Individuals with Type 2 Diabetes: a Consensus Statement from the American College of Sports Medicine. Med Sci Sports Exerc. 2022;54(2):353–368. PMID: 35029593; PMCID: PMC8802999. doi:10.1249/MSS.0000000000002800
106. Seyedizadeh SH, Cheragh-Birjandi S, Hamedi Nia MR. The Effects of Combined Exercise Training (Resistance-Aerobic) on Serum Kinesin and Physical Function in Type 2 Diabetes Patients with Diabetic Peripheral Neuropathy (Randomized Controlled Trials). J Diabetes Res. 2020;2020(6978128):1–7. doi:10.1155/2020/6978128
107. Kriska AM, Rockette-Wagner B, Edelstein SL, et al.; DPP Research Group. The Impact of Physical Activity on the Prevention of Type 2 Diabetes: evidence and Lessons Learned From the Diabetes Prevention Program, a Long-Standing Clinical Trial Incorporating Subjective and Objective Activity Measures. Diabetes Care. 2021;44(1):43–49. PMID: 33444158; PMCID: PMC7783946. doi:10.2337/dc20-1129
108. Balducci S, Haxhi J, Sacchetti M, et al. Italian Diabetes and Exercise Study 2 (IDES_2) Investigators. Relationships of Changes in Physical Activity and Sedentary Behavior With Changes in Physical Fitness and Cardiometabolic Risk Profile in Individuals With Type 2 Diabetes: the Italian Diabetes and Exercise Study 2 (IDES_2). Diabetes Care. 2022;45(1):213–221. PMID: 34728529. doi:10.2337/dc21-1505
109. Sattelmair J, Pertman J, Ding EL, et al. Dose response between physical activity and risk of coronary heart disease: a meta-analysis. Circulation. 2011;124(7):789–795. PMID: 21810663; PMCID: PMC3158733. doi:10.1161/CIRCULATIONAHA.110.010710
110. Barakat R, Refoyo I, Coteron J, et al. Exercise during pregnancy has a preventative effect on excessive maternal weight gain and gestational diabetes. A randomized controlled trial. Braz J Phys Ther. 2019;23(2):148–155. PMID: 30470666; PMCID: PMC6428908. doi:10.1016/j.bjpt.2018.11.005
111. Kluding PM, Pasnoor M, Singh R, et al. The effect of exercise on neuropathic symptoms, nerve function, and cutaneous innervation in people with diabetic peripheral neuropathy. J Diabetes Complications. 2012;26(5):424–429. PMID: 22717465; PMCID: PMC3436981. doi:10.1016/j.jdiacomp.2012.05.007
112. Nataraj M, Maiya AG, Nagaraju SP, Shastry BA, Shivashankara KN. Effect of exercise on renal function in diabetic nephropathy-A systematic review and meta-analysis. J Taibah Univ Med Sci. 2022;18(3):526–537. PMID: 36818178; PMCID: PMC9906014. doi:10.1016/j.jtumed.2022.11.002
113. Soleimani A, Soltani P, Karimi H, et al. The effect of moderate-intensity aerobic exercise on non-proliferative diabetic retinopathy in type II diabetes mellitus patients: a clinical trial. Microvasc Res. 2023;149:104556. PMID: 37269942. doi:10.1016/j.mvr.2023.104556
114. Merino J, Guasch-Ferré M, Li J, et al. Polygenic scores, diet quality, and type 2 diabetes risk: an observational study among 35,759 adults from 3 US cohorts. PLoS Med. 2022;19(4):e1003972. doi:10.1371/journal.pmed.1003972
115. Trief PM, Kalichman S, Uschner D, et al. Association of psychosocial factors with medication adherence in emerging adults with youth-onset type 2 diabetes: the iCount study. Pediatr Diabetes. 2022;23(8):1695–1706. doi:10.1111/pedi.13431
116. Roy T, Lloyd CE. Epidemiology of depression and diabetes: a systematic review. J Affect Disord. 2012;142 Suppl:S8–S21. doi:10.1016/S0165-0327(12)70004-6
117. Trief PM, Uschner D, Kalichman S, et al. Psychosocial factors predict medication adherence in young adults with youth-onset type 2 diabetes: longitudinal results from the TODAY2 I Count study. Diabet Med. 2023;40:e15062. PMID: 36751994. doi:10.1111/dme.15062
118. Castañeda SF, Gallo LC, Garcia ML, et al. Effectiveness of an integrated primary care intervention in improving psychosocial outcomes among Latino adults with diabetes: the LUNA-D study. Transl Behav Med. 2022;12(8):825–833. doi:10.1093/tbm/ibac042
119. Marmot M, Allen JJ. Social determinants of health equity. Am J Public Health. 2014;104:Suppl 4(Suppl 4):S517–9. PMID: 25100411; PMCID: PMC4151898. doi:10.2105/AJPH.2014.302200
120. Mezuk B, Eaton WW, Albrecht S, et al. Depression and type 2 diabetes over the lifespan: a meta-analysis. Diabetes Care. 2008;31(12):2383–2390. doi:10.2337/dc08-0985
121. Lin EH, Von Korff M, Alonso J, et al. Mental disorders among persons with diabetes--results from the World Mental Health Surveys. J Psychosom Res. 2008;65(6):571–580. doi:10.1016/j.jpsychores.2008.06.007
122. Gudala K, Bansal D, Schifano F, et al. Diabetes mellitus and risk of dementia: a meta-analysis of prospective observational studies. J Diabetes Investig. 2013;4(6):640–650. doi:10.1111/jdi.12087
123. Cukierman T, Gerstein HC, Williamson JD. Cognitive decline and dementia in diabetes--systematic overview of prospective observational studies. Diabetologia. 2005;48(12):2460–2469. GBD 2019 Diseases and Injuries Collaborators. doi:10.1007/s00125-005-0023-4
124. Vos T, Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1204–1222. doi:10.1016/S0140-6736(20)30925-9
125. Mallorquí-Bagué N, Lozano-Madrid M, Toledo E, et al. Type 2 diabetes and cognitive impairment in an older population with overweight or obesity and metabolic syndrome: baseline cross-sectional analysis of the PREDIMED-plus study. Sci Rep. 2018;8(1):16128. doi:10.1038/s41598-018-33843-8
126. Pelle MC, Zaffina I, Giofrè F, Pujia R, Arturi F. Potential Role of Glucagon-like Peptide-1 Receptor Agonists in the Treatment of Cognitive Decline and Dementia in Diabetes Mellitus. Int. J Mol Sci. 2023;24(14):11301. doi:10.3390/ijms241411301
127. Salvatore T, Pafundi PC, Morgillo F, et al. Metformin: an old drug against old age and associated morbidities. Diabetes Res Clin Pract. 2020;160:108025. doi:10.1016/j.diabres.2020.108025
128. Cukierman-Yaffe T, Gerstein HC, Colhoun HM, et al. Effect of dulaglutide on cognitive impairment in type 2 diabetes: an exploratory analysis of the REWIND trial [published correction appears in Lancet Neurol. 2020 Oct;19(10):e9]. Lancet Neurol. 2020;19(7):582–590. doi:10.1016/S1474-4422(20)30173-3
129. Lee CH, Jeon SJ, Cho KS, et al. Activation of Glucagon-Like Peptide-1 Receptor Promotes Neuroprotection in Experimental Autoimmune Encephalomyelitis by Reducing Neuroinflammatory Responses. Mol Neurobiol. 2018;55(4):3007–3020. doi:10.1007/s12035-017-0550-2
130. Kremers SHM, Wild SH, Elders PJM, et al. The role of mental disorders in precision medicine for diabetes: a narrative review. Diabetologia. 2022;65(11):1895–1906. doi:10.1007/s00125-022-05738-x
131. Galiero R, Pafundi PC, Nevola R, et al. The Importance of Telemedicine during COVID-19 Pandemic: a Focus on Diabetic Retinopathy. J Diabetes Res. 2020;2020:1–8. doi:10.1155/2020/9036847
132. Sasso FC, Pafundi PC, Gelso A, et al.; NO BLIND Study Group. Telemedicine for screening diabetic retinopathy: the NO BLIND Italian multicenter study. Diabetes Metab Res Rev. 2019;35(3):e3113. PMID: 30548967. doi:10.1002/dmrr.3113
133. Gómez AM, Henao D, Parra D, et al. Early and sustained increase in time in range 1 year after initiation of hybrid close loop therapy via telemedicine in type 1 diabetes patients. Acta Diabetol. 2023;60(7):943–949. PMID: 37010594; PMCID: PMC10068726. doi:10.1007/s00592-023-02051-w
134. Díaz-Soto G, Ibáñez MS, Del Amo Simón S, et al. Metabolic control and satisfaction in a diabetes education programme in flash glucose monitoring through telemedicine in type 1 diabetes. Endocrinol Diabetes Nutr. 2023;70(6):408–414. PMID: 36456461. doi:10.1016/j.endien.2022.01.009
135. Longwitz A, Palokas M. Diabetes self-management education for adults with type 2 diabetes via telehealth in conjunction with remote patient monitoring: a best practice implementation project. JBI Evid Implement. 2023;21(2):156–166. PMID: 36458653. doi:10.1097/XEB.0000000000000360
136. Zamanillo-Campos R, Fiol-deRoque MA, Serrano-Ripoll MJ, Mira-Martínez S, Ricci-Cabello I. Development and evaluation of DiabeText, a personalized mHealth intervention to support medication adherence and lifestyle change behaviour in patients with type 2 diabetes in Spain: a mixed-methods Phase II pragmatic randomized controlled clinical trial. Int J Med Inform. 2023;176:105103. PMID: 37267809. doi:10.1016/j.ijmedinf.2023.105103
137. van Bastelaar KM, Pouwer F, Cuijpers P, Riper H, Snoek FJ. Web-based depression treatment for type 1 and type 2 diabetic patients: a randomized, controlled trial. Diabetes Care. 2011;34(2):320–325. doi:10.2337/dc10-1248
138. Hill-Briggs F, Adler NE, Berkowitz SA, et al. Social Determinants of Health and Diabetes: a Scientific Review. Diabetes Care. 2020;44(1):258–279. doi:10.2337/dci20-0053
139. Lenzi FR, Filardi T. Social determinants of vulnerabilities in type 2 diabetes: a call to action. J Endocrinol Invest. 2023;46(4):841–844. PMID: 36318450. doi:10.1007/s40618-022-01952-x
140. Bijlsma-Rutte A, Rutters F, Elders PJM, et al. Socio-economic status and HbA1c in type 2 diabetes: a systematic review and meta-analysis. Diabetes Metab Res Rev. 2018;34(6):e3008. PMID: 29633475. doi:10.1002/dmrr.3008
141. Xu X, Yang W, Deng Y, et al. Association of socioeconomic status with glycated haemoglobin level and risk factors for diabetic retinopathy: a cross-sectional study in Sichuan, western China. BMJ Open. 2023;13(2):e067475. PMID: 36797020; PMCID: PMC9936295. doi:10.1136/bmjopen-2022-067475
142. Egnew TR. Suffering, meaning, and healing: challenges of contemporary medicine. Ann Fam Med. 2009;7(2):170–175. PMID: 19273873; PMCID: PMC2653974. doi:10.1370/afm.943
143. ElSayed NA, Aleppo G, Aroda VR, et al. Pharmacologic Approaches to Glycemic Treatment: standards of Care in Diabetes-2023. Diabetes Care. 2023;46(Suppl 1):S140–S157. PMID: 36507650; PMCID: PMC9810476. doi:10.2337/dc23-S009
144. Choi JG, Winn AN, Skandari MR, et al. First-Line Therapy for Type 2 Diabetes With Sodium-Glucose Cotransporter-2 Inhibitors and Glucagon-Like Peptide-1 Receptor Agonists: a Cost-Effectiveness Study. Ann Intern Med. 2022;175(10):1392–1400. PMID: 36191315; PMCID: PMC10155215. doi:10.7326/M21-2941
145. Zhou K, Pedersen HK, Dawed AY, Pearson ER. Pharmacogenomics in diabetes mellitus: insights into drug action and drug discovery. Nat Rev Endocrinol. 2016;12(6):337–346. doi:10.1038/nrendo.2016.51
146. Tsapas A, Karagiannis T, Kakotrichi P, et al. Comparative efficacy of glucose-lowering medications on body weight and blood pressure in patients with type 2 diabetes: a systematic review and network meta-analysis. Diabetes Obes Metab. 2021;23(9):2116–2124. doi:10.1111/dom.14451
147. Caturano A, Galiero R, Pafundi PC. Metformin for Type 2 Diabetes. JAMA. 2019;322(13):1312. PMID: 31573630. doi:10.1001/jama.2019.11489
148. Zhou K, Donnelly L, Yang J, et al.; Wellcome Trust Case Control Consortium 2; Spencer CC, Groop L, Morris AD, Colhoun HM, Sham PC, McCarthy MI, Palmer CN, Pearson ER. Heritability of variation in glycaemic response to metformin: a genome-wide complex trait analysis. Lancet Diabetes Endocrinol. 2014;2(6):481–487. doi:10.1016/S2213-8587(14)70050-6
149. Wang DS, Jonker JW, Kato Y, Kusuhara H, Schinkel AH, Sugiyama Y. Involvement of organic cation transporter 1 in hepatic and intestinal distribution of metformin. J Pharmacol Exp Ther. 2002;302(2):510–515. doi:10.1124/jpet.102.034140
150. Kimura N, Masuda S, Tanihara Y, et al. Metformin is a superior substrate for renal organic cation transporter OCT2 rather than hepatic OCT1. Drug Metab Pharmacokinet. 2005;20(5):379–386. doi:10.2133/dmpk.20.379
151. Singh S, Usman K, Banerjee M. Pharmacogenetic studies update in type 2 diabetes mellitus. World J Diabetes. 2016;7(15):5. doi:10.4239/wjd.v7.i15.302
152. Hou W, Zhang D, Lu W, et al. Polymorphism of organic cation transporter 2 improves glucose-lowering effect of metformin via influencing its pharmacokinetics in Chinese type 2 diabetic patients. Mol Diagn Ther. 2015;19(1):25–33. doi:10.1007/s40291-014-0126-z
153. Tkáč I, Klimčáková L, Javorský M, et al. Pharmacogenomic association between a variant in SLC47A1 gene and therapeutic response to metformin in type 2 diabetes. Diabetes Obes Metab. 2013;15:189–191. doi:10.1111/j.1463-1326.2012.01691.x
154. Florez JC. Pharmacogenetics in type 2 diabetes: precision medicine or discovery tool? Diabetologia. 2017;60(5):800–807. PMID: 28283684. doi:10.1007/s00125-017-4227-1
155. Dennis JM, Henley WE, Weedon MN, et al. MASTERMIND Consortium. Sex and BMI Alter the Benefits and Risks of Sulfonylureas and Thiazolidinediones in Type 2 Diabetes: a Framework for Evaluating Stratification Using Routine Clinical and Individual Trial Data. Diabetes Care. 2018;41(9):1844–1853. PMID: 30072404; PMCID: PMC6591127. doi:10.2337/dc18-0344
156. Vetrano E, Rinaldi L, Mormone A, et al. Non-alcoholic Fatty Liver Disease (NAFLD), Type 2 Diabetes, and Non-viral Hepatocarcinoma: pathophysiological Mechanisms and New Therapeutic Strategies. Biomedicines. 2023;11(2):468. PMID: 36831004; PMCID: PMC9953066. doi:10.3390/biomedicines11020468
157. Lyssenko V, Bianchi C, Del Prato S. Personalized therapy by phenotype and genotype. Diabetes Care. 2016;39(suppl 2):s127–36. doi:10.2337/dcS15-3002
158. Hamming KS, Soliman D, Matemisz LC, et al. Coexpression of the type 2 diabetes susceptibility gene variants KCNJ11 E23K and ABCC8 S1369A alter the ATP and sulfonylurea sensitivities of the ATP-sensitive K(+) channel. Diabetes. 2009;58(10):2419–2424. PMID: 19587354; PMCID: PMC2750221. doi:10.2337/db09-0143
159. Hanefeld M, Cagatay M, Petrowitsch T, et al. Acarbose reduces the risk for myocardial infarction in Type 2 diabetic patients: meta-analysis of seven long-term studies. Eur Heart J. 2004;25(1):10–16. doi:10.1016/S0195-668X(03)00468-8
160. Wei Y, Xu W. Effect of acarbose on cardiovascular events and new-onset diabetes in patients with coronary heart disease and impaired glucose tolerance. Future Cardiol. 2019;15(2):127–133. PMID: 30793928. doi:10.2217/fca-2018-0062
161. Holman RR, Coleman RL, Chan JCN, et al. Effects of acarbose on cardiovascular and diabetes outcomes in patients with coronary heart disease and impaired glucose tolerance (ACE): a randomised, double-blind, placebo-controlled trial. Lancet Diabetes Endocrinol. 2017;5(11):877–886. doi:10.1016/S2213-8587(17)30309-1
162. Maruthur NM, Gribble MO, Bennett WL, et al. The pharmacogenetics of type 2 diabetes: a systematic review. Diabetes Care. 2014;37:876–886. doi:10.2337/dc13-1276
163. Dennis JM, Shields BM, Hill AV, et al. MASTERMIND Consortium. Precision Medicine in Type 2 Diabetes: clinical Markers of Insulin Resistance Are Associated With Altered Short- and Long-term Glycemic Response to DPP-4 Inhibitor Therapy. Diabetes Care. 2018;41(4):705–712. PMID: 29386249; PMCID: PMC6591121. doi:10.2337/dc17-1827
164. Jones AG, McDonald TJ, Shields BM, et al. Markers of β-Cell Failure Predict Poor Glycemic Response to GLP-1 Receptor Agonist Therapy in Type 2 Diabetes. Diabetes Care. 2016;39(2):250–257. PMID: 26242184; PMCID: PMC4894547. doi:10.2337/dc15-0258
165. Bihan H, Ng WL, Magliano DJ, Shaw JE. Predictors of efficacy of GLP-1 agonists and DPP-4 inhibitors: a systematic review. Diabetes Res Clin Pract. 2016;121:27–34. PMID: 27622682. doi:10.1016/j.diabres.2016.08.011
166. Davis TME, Mulder H, Lokhnygina Y, et al. Effect of race on the glycaemic response to sitagliptin: insights from the Trial Evaluating Cardiovascular Outcomes with Sitagliptin (TECOS). Diabetes Obes Metab. 2018;20(6):1427–1434. PMID: 29405540. doi:10.1111/dom.13242
167. Palmer SC, Tendal B, Mustafa RA, et al. Sodium-glucose cotransporter protein-2 (SGLT-2) inhibitors and glucagon-like peptide-1 (GLP-1) receptor agonists for type 2 diabetes: systematic review and network meta-analysis of randomised controlled trials. BMJ. 2021;372:
168. Rathmann W, Bongaerts B. Pharmacogenetics of novel glucose-lowering drugs. Diabetologia. 2021;64(6):1201–1212. PMID: 33594477; PMCID: PMC8099830. doi:10.1007/s00125-021-05402-w
169. Yu M, Wang K, Liu H, et al. GLP1R variant is associated with response to exenatide in overweight Chinese Type 2 diabetes patients. Pharmacogenomics. 2019;20(4):273–277. doi:10.2217/pgs-2018-0159
170. de Luis DA, Ovalle HF, Soto GD, et al. Role of genetic variation in the cannabinoid receptor gene (CNR1) (G1359A polymorphism) on weight loss and cardiovascular risk factors after liraglutide treatment in obese patients with diabetes mellitus type 2. J Investig Med. 2014;62(2):324–327. PMID: 24322329. doi:10.2310/JIM.0000000000000032
171. DeFronzo RA, Ferrannini E, Schernthaner G, et al. Slope of change in HbA1c from baseline with empagliflozin compared with sitagliptin or glimepiride in patients with type 2 diabetes. Endocrinol Diabetes Metab. 2018;1(2):e00016. PMID: 30815552; PMCID: PMC6354821. doi:10.1002/edm2.16
172. Rosenstock J, Hansen L, Zee P, et al. Dual add-on therapy in type 2 diabetes poorly controlled with metformin monotherapy: a randomized double-blind trial of saxagliptin plus dapagliflozin addition versus single addition of saxagliptin or dapagliflozin to metformin. Diabetes Care. 2015;38(3):376–383. PMID: 25352655. doi:10.2337/dc14-1142
173. Dennis JM, Young KG, McGovern AP, et al. Development of a treatment selection algorithm for SGLT2 and DPP-4 inhibitor therapies in people with type 2 diabetes: a retrospective cohort study. Lancet Digit Health. 2022;4(12):e873–e883. PMID: 36427949. doi:10.1016/S2589-7500(22)00174-1
174. Macha S, Mattheus M, Halabi A, et al. Pharmacokinetics, pharmacodynamics and safety of empagliflozin, a sodium glucose cotransporter 2 (SGLT2) inhibitor, in subjects with renal impairment. Diabetes Obes Metab. 2014;16(3):215–222. PMID: 23859488. doi:10.1111/dom.12182
175. Cherney DZI, Cooper ME, Tikkanen I, et al. Pooled analysis of Phase III trials indicate contrasting influences of renal function on blood pressure, body weight, and HbA1c reductions with empagliflozin. Kidney Int. 2018;93(1):231–244. PMID: 28860019. doi:10.1016/j.kint.2017.06.017
176. Shields BM, Dennis JM, Angwin CD, et al. TriMaster Study group. Patient stratification for determining optimal second-line and third-line therapy for type 2 diabetes: the TriMaster study. Nat Med. 2023;29(2):376–383. PMID: 36477733; PMCID: PMC7614216. doi:10.1038/s41591-022-02120-7
177. Salvatore T, Galiero R, Caturano A, et al. An Overview of the Cardiorenal Protective Mechanisms of SGLT2 Inhibitors. Int J Mol Sci. 2022;23(7):3651. PMID: 35409011; PMCID: PMC8998569. doi:10.3390/ijms23073651
178. Coelho FDS, Borges-Canha M, von Hafe M, et al. Effects of sodium-glucose co-transporter 2 inhibitors on liver parameters and steatosis: a meta-analysis of randomized clinical trials. Diabetes Metab Res Rev. 2021;37(6):e3413. PMID: 33010191. doi:10.1002/dmrr.3413
179. Caturano A, Galiero R, Loffredo G, et al. Effects of a Combination of Empagliflozin Plus Metformin vs. Metformin Monotherapy on NAFLD Progression in Type 2 Diabetes: the IMAGIN Pilot Study. Biomedicines. 2023;11(2):322. PMID: 36830859; PMCID: PMC9952909. doi:10.3390/biomedicines11020322
180. Francke S, Mamidi RN, Solanki B, et al. In vitro metabolism of canagliflozin in human liver, kidney, intestine microsomes, and recombinant uridine diphosphate glucuronosyltransferases (UGT) and the effect of genetic variability of UGT enzymes on the pharmacokinetics of canagliflozin in humans. J Clin Pharmacol. 2015;55(9):1061–1072. doi:10.1002/jcph.506
181. Gentile S, Turco S, Guarino G, et al. Comparative efficacy study of atorvastatin vs simvastatin, pravastatin, lovastatin and placebo in type 2 diabetic patients with hypercholesterolaemia. Diabetes Obes Metab. 2000;2(6):355–362. doi:10.1046/j.1463-1326.2000.00106.x
182. Rinaldi L, Nevola R, Franci G, et al. Risk of Hepatocellular Carcinoma after HCV Clearance by Direct-Acting Antivirals Treatment Predictive Factors and Role of Epigenetics. Cancers. 2020;12(6):1351. doi:10.3390/cancers12061351
183. Cozzolino D, Sessa G, Salvatore T, et al. The involvement of the opioid system in human obesity: a study in normal weight relatives of obese people. J Clin Endocrinol Metab. 1996;81(2):713–718. doi:10.1210/jcem.81.2.8636293
184. Ahlqvist E, Storm P, Käräjämäki A, et al. Novel subgroups of adult-onset diabetes and their association with outcomes: a data-driven cluster analysis of six variables. Lancet Diabetes Endocrinol. 2018;6(5):361–369. PMID: 29503172. doi:10.1016/S2213-8587(18)30051-2
185. Zaharia OP, Strassburger K, Strom A, et al.; German Diabetes Study Group. Risk of diabetes-associated diseases in subgroups of patients with recent-onset diabetes: a 5-year follow-up study. Lancet Diabetes Endocrinol. 2019;7(9):684–694. PMID: 31345776. doi:10.1016/S2213-8587(19)30187-1
186. Xiong XF, Yang Y, Wei L, et al. Identification of two novel subgroups in patients with diabetes mellitus and their association with clinical outcomes: a two-step cluster analysis. J Diabetes Investig. 2021;12(8):1346–1358. PMID: 33411406; PMCID: PMC8354513. doi:10.1111/jdi.13494
187. Pafundi PC, Garofalo C, Galiero R, et al. Role of Albuminuria in Detecting Cardio-Renal Risk and Outcome in Diabetic Subjects. Diagnostics (Basel). 2021;11(2):290. PMID: 33673215; PMCID: PMC7918197. doi:10.3390/diagnostics11020290
188. Salvatore T, Galiero R, Caturano A, et al. Dysregulated Epicardial Adipose Tissue as a Risk Factor and Potential Therapeutic Target of Heart Failure with Preserved Ejection Fraction in Diabetes. Biomolecules. 2022;12(2):176. PMID: 35204677; PMCID: PMC8961672. doi:10.3390/biom12020176
189. Preechasuk L, Khaedon N, Lapinee V, et al. Cluster analysis of Thai patients with newly diagnosed type 2 diabetes mellitus to predict disease progression and treatment outcomes: a prospective cohort study. BMJ Open Diabetes Res Care. 2022;10(6):e003145. PMID: 36581330; PMCID: PMC9806077. doi:10.1136/bmjdrc-2022-003145
190. Naithani N, Atal AT, Tvsvgk T, Vasudevan B, Misra P, Sinha S. Precision medicine: uses and challenges. Med J Armed Forces India. 2021;77(3)::258–265. PMID: 34305277; PMCID: PMC8282516. doi:10.1016/j.mjafi.2021.06.020
191. Griffin S. Diabetes precision medicine: plenty of potential, pitfalls and perils but not yet ready for prime time. Diabetologia. 2022;65(11):1913–1921. PMID: 35999379; PMCID: PMC9522689. doi:10.1007/s00125-022-05782-7
192. Gaede P, Lund-Andersen H, Parving HH, Pedersen O. Effect of a multifactorial intervention on mortality in type 2 diabetes. N Engl J Med. 2008;358(6):580–591. PMID: 18256393. doi:10.1056/NEJMoa0706245
193. Gaede P, Vedel P, Larsen N, et al. Multifactorial intervention and cardiovascular disease in patients with type 2 diabetes. N Engl J Med. 2003;348(5):383–393. PMID: 12556541. doi:10.1056/NEJMoa021778
194. Sasso FC, Pafundi PC, Simeon V, et al.; NID-2 Study Group Investigators. Efficacy and durability of multifactorial intervention on mortality and MACEs: a randomized clinical trial in type-2 diabetic kidney disease. Cardiovasc Diabetol. 2021;20(1):145. PMID: 34271948; PMCID: PMC8285851. doi:10.1186/s12933-021-01343-1
195. Sasso FC, Simeon V, Galiero R, et al. NID-2 study group Investigators. The number of risk factors not at target is associated with cardiovascular risk in a type 2 diabetic population with albuminuria in primary cardiovascular prevention. Post-hoc analysis of the NID-2 trial. Cardiovasc Diabetol. 2022;21(1):235. PMID: 36344978; PMCID: PMC9641842. doi:10.1186/s12933-022-01674-7
196. Swen JJ, van der Wouden CH, Manson LE, et al.; Ubiquitous Pharmacogenomics Consortium. A 12-gene pharmacogenetic panel to prevent adverse drug reactions: an open-label, multicentre, controlled, cluster-randomised crossover implementation study. Lancet. 2023;401(10374):347–356. PMID: 36739136. doi:10.1016/S0140-6736(22)01841-4
197. Shah HS, Morieri ML, Marcovina SM, et al. Modulation of GLP-1 Levels by a Genetic Variant That Regulates the Cardiovascular Effects of Intensive Glycemic Control in ACCORD. Diabetes Care. 2018;41(2):348–355. PMID: 29183908; PMCID: PMC5780047. doi:10.2337/dc17-1638
198. Morieri ML, Shah HS, Sjaarda J, et al. PPARA Polymorphism Influences the Cardiovascular Benefit of Fenofibrate in Type 2 Diabetes: findings From ACCORD-Lipid. Diabetes. 2020;69(4):771–783. PMID: 31974142; PMCID: PMC7085251. doi:10.2337/db19-0973
199. Siminerio L, Krall J, Johnson P, et al. Examining a Diabetes Self-Management Education and Support Telemedicine Model With High-Risk Patients in a Rural Community. J Diabetes Sci Technol. 2023;20:19322968231180884. PMID: 37338130. doi:10.1177/19322968231180884
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development and Validation of a Model That Predicts the Risk of Diabetic Nephropathy in Type 2 Diabetes Mellitus Patients: A Cross-Sectional Study
Yang J, Jiang S
International Journal of General Medicine 2022, 15:5089-5101
Published Date: 20 May 2022
Awareness and Predictors of the Use of Bioinformatics in Genome Research in Saudi Arabia
Alomair L, Abolfotouh MA
International Journal of General Medicine 2023, 16:3413-3425
Published Date: 11 August 2023
Evaluation of Vitamin B12 Deficiency Among Patients with Type 2 Diabetes Mellitus on Metformin at Hoima Regional Referral Hospital, Uganda
Ali HO, Agwu E, Ali MA, Jama YM, Ahmed AH, Yusuf MAM, Araye AA, Osobow IM, Sandeyl AA, Ahmed ZA, Onyanga N, Nor FI, Mohamed AH, Karshe AH, Hirsi AM, Mohamed AA, Jayte M
Diabetes, Metabolic Syndrome and Obesity 2026, 19:562440
Published Date: 21 January 2026