Back to Journals » Journal of Asthma and Allergy » Volume 16
Pre-Existing Allergies Patients with Higher Viral Load and Longer Recovery Days Infected by SARS-CoV-2 Omicron BA.2 in Shanghai, China, 2022
Authors Wen R, Li J, Wang X, Xu P, Li G, Wang J, Zeng X ![]() , Liu C
, Liu C ![]()
Received 13 January 2023
Accepted for publication 12 June 2023
Published 1 September 2023 Volume 2023:16 Pages 903—913
DOI https://doi.org/10.2147/JAA.S402674
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Luis Garcia-Marcos
Ru Wen,1– 3,* Jingwen Li,4,* Xingang Wang,1,* Peng Xu,1 Guizhu Li,5 Jian Wang,1 Xianchun Zeng,2,6 Chen Liu1
1Department of Radiology, Southwest Hospital, Army Medical University (Third Military Medical University), Chongqing, 400038, People’s Republic of China; 2Department of Medical Imaging, Guizhou Provincial People Hospital, Guiyang City, Guizhou Province, 550000, People’s Republic of China; 3Medical College, Guizhou University, Guiyang City, Guizhou Province, 550000, People’s Republic of China; 4Department of Gastroenterology, Southwest Hospital, Army Medical University (Third Military Medical University), Chongqing, 400038, People’s Republic of China; 5College of Mathematics and Statistics, Chongqing University, Chongqing, 400044, People’s Republic of China; 6NHC Key Laboratory of Pulmonary Immunological Diseases (Guizhou Provincial People’s Hospital), Guiyang, Guizhou, China
*These authors contributed equally to this work
Correspondence: Chen Liu, Department of Radiology, Southwest Hospital, Army Medical University (Third Military Medical University), 30 Gao Tan Yan St, Chongqing, 400038, People’s Republic of China, Tel +8613108968808, Email [email protected] Xianchun Zeng, Department of Medical Imaging, Guizhou Provincial People Hospital, No. 83, East Zhongshan Road, Nanming District, Guiyang City, Guizhou Province, 550000, People’s Republic of China, Tel +8615286061024, Email [email protected]
Background: It is not known whether the viral load and the number of days to negative nucleic acid increased in patients with a history of allergy during the COVID-19 pandemic.
Objective: To investigate the impact of allergy labels on SARS-CoV-2 Omicron outcomes.
Methods: This retrospective cohort study included 62,293 patients with mild Omicron infection between April 9, 2022, and May 31, 2022. Using 1:2 propensity score matching, we identified 2177 COVID-19 patients with a history of allergy and 4254 COVID-19 patients with no history of allergy. The differences in viral load, days to nucleic acid turning negative, and clinical symptoms were compared between the two groups.
Results: Compared with the group with no allergies, the number of days before negative nucleic acid conversion of COVID-19 patients with allergies was significantly higher, the viral load was significantly higher, and the cumulative negative conversion rates at 5– 10 days were all lower (p < 0.01). Patients with a history of allergy to antibiotics had higher viral load and more days with negative nucleic acid levels (p < 0.001). Subgroup analysis revealed that the viral load in penicillin-allergic and cephalosporins-allergic patients was significantly compared to patients without any history of allergies (p < 0.05).
Conclusion: Patients with a history of allergy have a more significant viral load and a longer duration of nucleic acid negative conversion upon COVID-19 infection, particularly those allergic to antibiotics.
Keywords: COVID-19, omicron, allergy history, antibiotics allergy, ct value, nucleic acid turning-negative-time
Introduction
The World Health Organization has recognized the Omicron variant of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) as a variation of concern.1 The variation contains up to 36 spikes known to avoid neutralizing antibodies created by the coronavirus disease 2019 (COVID-19) vaccine, raising concerns about the virus’ potential to dodge infection or the efficacy of vaccine-induced antibodies.2 Previous research has demonstrated that the intensification of COVID-19 is closely related to changes in the immune system’s defense. The overstress response of the immune system is likely to trigger the inflammatory storm after COVID-19, resulting in further deterioration of the patient’s condition and even death.3
The association between allergic disorders and the prognosis of COVID-19 has garnered growing interest, as allergic diseases are regarded as placing an undue burden on the immune system.4,5 At present, it is controversial whether allergic diseases are related to the severe clinical results of COVID-19. According to some reports, there may not be a connection between asthma and the elevated risk of COVID-19.6,7 However, there is a correlation between allergic rhinitis and adverse COVID-19 clinical outcomes (eg, intensive care or death).8–11 There is little information on the behavior of Omicron variants in patients with allergic diseases. Due to the characteristics of mild symptoms and strong transmissibility, the Omicron variant is bound to have new immune response features, so it is worth studying the clinical changes of Omicron-infected allergic patients and their relationship. During the COVID-19 global pandemic, people with a history of allergies are relatively vulnerable and easily overlooked due to the imbalance of the immune system. For Omicron-infected patients with allergic history, it is of great importance to clarify their clinical features and the severity of the disease outcome.12 We hypothesized that the number of days of negative nucleic acid and viral load of COVID-19 patients with a history of allergy were significantly different from those without a history of allergy.
At the end of March 2022, another outbreak of Omicron appeared in Shanghai, China. In this study, mildly affected patients with a history of allergies were the main subjects admitted to The Convention Center (Shanghai) Fangcang shelter hospital. We evaluated the clinical manifestations, viral load, and the days of nucleic acid negative conversion in patients with Omicron infection, to identify the relationship between Omicron infection, allergic status, and viral load. The aim was to offer further clinical and prognostic information for COVID-19 patients with a history of allergy or anaphylaxis.
Method
Patients’ Enrollment
This retrospective study involved patients with the Omicron variant infection who had mild symptoms and were admitted to The Convention Center (Shanghai) Fangcang shelter hospital from April 29 to May 31, 2022. The hospital is Shanghai’s largest Fangcang shelter hospital for treating Omicron-infected people. It only treats patients with mild symptoms diagnosed with COVID-19. If the condition worsens, the patient will be transferred to another designated hospital for further treatment. Screening for SARS-CoV-2 nucleic acids was carried out using real-time reverse transcription polymerase chain reaction (RT-PCR) tests in all patients who had been exposed to confirmed or suspected COVID-19 cases. The RT-PCR test results were confirmed by ORF1ab and N genes according to the Guidelines for the Diagnosis and Treatment of Coronavirus Disease 2019 (Trial 9th edition).13 In our study, we only included adult patients with mild COVID-19 symptoms and a history of allergies or anaphylaxis. All individuals enrolled in this study tested positive. All patients admitted to Fangcang hospitals were discharged after two negative PCR tests. The deadline for follow-up is the closing date of the Fangcang shelter hospital.
This research was conducted in accordance with the principles outlined in the Helsinki Declaration. The Ethics Review Committee of the Southwest Hospital of the Army Medical University waived the requirement for patient consent as this study involved a retrospective analysis of de-identified data (approval number KY2022114). We place on safe guarding patient data confidentiality and all patient data are confidential.
Data Collection
The data include demographic information, clinical manifestations, past disease history, and nucleic acid testing information. These data come from epidemiological investigations and medical record systems, which are examined independently by Dr. Li and Dr. Wang’s researchers. The medical record system recorded the PCR test results and circulatory threshold (Ct) values of each SARS-CoV-2 positive sample. The nucleic acid Ct value refers to the number of cycles corresponding to the detection of fluorescent signals. A smaller Ct value means fewer cycles. That is, the presence of a virus can be detected in a short time, indicating a large number of viruses. The larger the Ct value, the more cycles, and the more challenging it is to detect the virus. We measured the Ct value of nucleic acid (ORF1ab and N genes). The average value based on all positive results represented the average viral load of the patient, and the minimum of all positive results represented the highest viral load. We calculated the nucleic acid turning-negative-time (the time from the first positive result of the SARS-CoV-2 gene test to the first negative result). Allergy was defined as a patient’s self-reported history of allergies.
The COVID-19 vaccination status includes whether or not the patient has been vaccinated, the vaccination brand (adenovirus-vectored, inactivated, recombinant protein subunit vaccines), and whether or not booster injections have been administered; the data was gathered from the patient’s self-report. The presence of allergies is determined before the event of COVID-19 diagnostic indicators, including antibiotic allergy, Chinese herbal medicine allergy, foodborne allergy, and antipyretic analgesic drug allergy.
Two Cohorts Studied
Our study included a total of two cohorts: (1) Cohort A included 2369 COVID-19 patients with an allergy history and 62,293 COVID-19 patients without an allergy history among mild-symptom patients admitted to The Convention Center (Shanghai) Fangcang shelter hospital from April 9 to May 31; Match two groups of patients in cohort A by 1:2 propensity score matching (PSM) (2177 COVID-19 patients with a history of allergy based on the medical record system and 4254 COVID-19 patients without allergies), and (2) cohort B included 1675 COVID-19 patients with a history of antibiotic allergy and 3271 COVID-19 patients without an allergy history after 1:2 tendency matching. A diagram of the two queues is shown in Figure 1.
 |
Figure 1 Flow chart of the inclusion and exclusion criteria of the study sample. |
Control Variables
PSM was used to minimize bias when comparing differences in viral load and days to negative nucleic acid in the cohort study. This has been widely used in the medical literature.14 The control variables in the study cohort matched based on demographic differences, vaccination status (vaccine availability, vaccine brand, and booster availability), and comorbidities (including hypertension, diabetes, cardiovascular disease, cerebrovascular disease, respiratory disease, renal insufficiency, other inflammation, and tumor). The study results were the days of negative conversion and the virus load of COVID-19 patients who were admitted to the Fangcang shelter hospital. The viral load was measured by the mean and minimum values of the ORF1ab and N genes with positive results in the fangcang shelter hospital; the mean value represented the average viral load, and the minimum value represented the highest viral load. We explored the viral load, negative nucleic acid, and clinical signs risk of allergic patients.
Statistical Analyses
Continuous variables were described by mean and variance (SD) values, and categorical variables were expressed in frequency and percentage (%). The t-test was used for continuous variables, and the χ2 test or Fisher exact test was used for categorical variables. We estimated the results of different study cohorts for absolute risk, odds ratios (OR), and 95% confidence interval (CI). Through logistic regression modeling, we determined a propensity score for each patient. Patients were then matched 1:2, with the caliper width set to 0.01 for the SD.15 To assess the balance, standardized mean differences were calculated before and after matching, and a value of less than 0.1 was regarded as not being significant between groups. The mean viral load, maximum viral load, and the time for nucleic acid to turn negative were compared between the two groups by the independent sample t-test. Analysis of variance was used to compare the average and maximum viral loads of different allergens and the difference in the time for nucleic acid to turn negative. With a Log rank test, the Kaplan–Meier method was used to calculate the time to the primary endpoint. Statistical analysis was performed using SPSS version 26.0 and R language version 4.2. For all analyses, p < 0.05 was the level of statistical significance.
Results
Cohort A
We identified 2369 COVID-19 patients with a history of allergies (age:47.55 (15.56), male:45.3%) and 62,293 COVID-19 patients with no history of allergies (age:44.92 (14.77), male:61.6%) in Fangcang shelter hospitals. Compared to patients with no history of allergies, those with a history of allergies have a higher incidence of hypertension, diabetes, cardiovascular diseases, cerebrovascular diseases, respiratory diseases, renal insufficiency, other inflammation, and tumors (p < 0.01). The vaccination rates of COVID-19 patients with allergic history were significantly lower than those without an allergic history (75.1 vs 77.7, p < 0.01). After 1:2 PSM, there were no significant imbalances in baseline characteristics in the PSM-matched cohort of 2177 COVID-19 patients with a history of allergies and 4254 COVID-19 patients with no history of allergies (Table 1; Supplementary Figure 1; all p > 0.05).
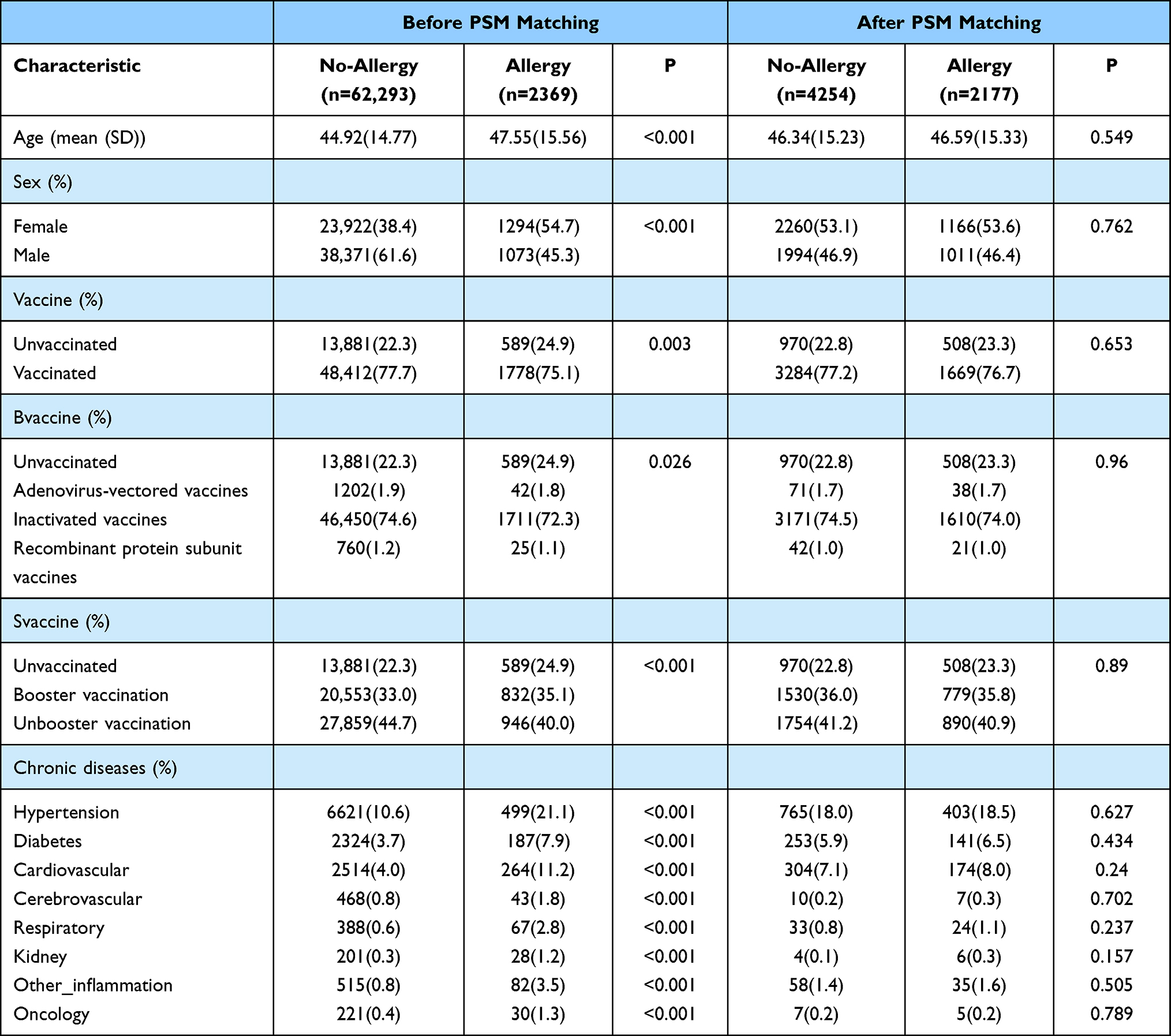 |
Table 1 Baseline Characteristics of COVID-19 Patients with and without Allergy History Before and After PSM Matching |
Relationship Between the History of Allergy and Days of Nucleic Acid Negative Conversion and Viral Load
The number of days for nucleic acid to turn negative in COVID-19 patients with previous allergic history was significantly higher than that in non-allergic patients (5.65 vs 5.17, p < 0.001). Compared with patients without allergy history, the mean Ct values of the ORF1ab gene and N gene were significantly higher than those in patients with allergy history (ORF1ab gene, 32.91 vs 32.5; N gene, 30.88 vs 30.53; p < 0.001); the minimum Ct values of the ORF1ab gene and N gene were significantly higher than those in patients with an allergy history (ORF1ab gene, 30.85 vs 29.82; N gene, 28.92 vs 27.98; p < 0.001); Table 2 lists the differences in viral load and negative nucleic acid conversion among COVID-19 patients with and without allergy labels.
 |
Table 2 Differences in Days to Negative Conversion and Viral Load Between COVID-19 Patients with and without Allergy History |
The cumulative negative conversion rates at 5, 6, 7, 8, 9, and 10 days in the allergy group were all lower than those in the non-allergy group (55.8% vs 62.6%; 67.7% vs 73.6%; 76.1% vs 82.4%; 82.5% vs 88.5%; 88.5% vs 92.4%; and 92.7% vs 95.6%; all p < 0.001) (Table 3). Log-rank analysis showed that patients with allergy history had approximately 0.867-fold (95%, CI 0.823–0.913, p < 0.001) lower conversion rates than those without allergy history (Figure 2).
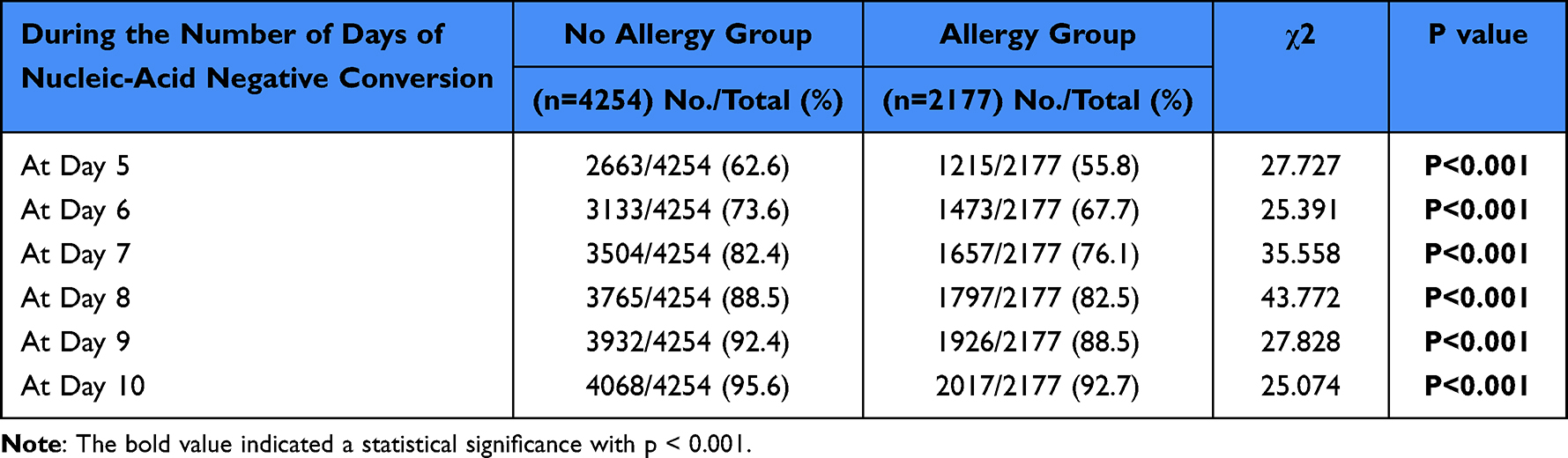 |
Table 3 Cumulative Negative Conversion Rates of SARS-CoV-2 Between COVID-19 Patients with and without Allergy History |
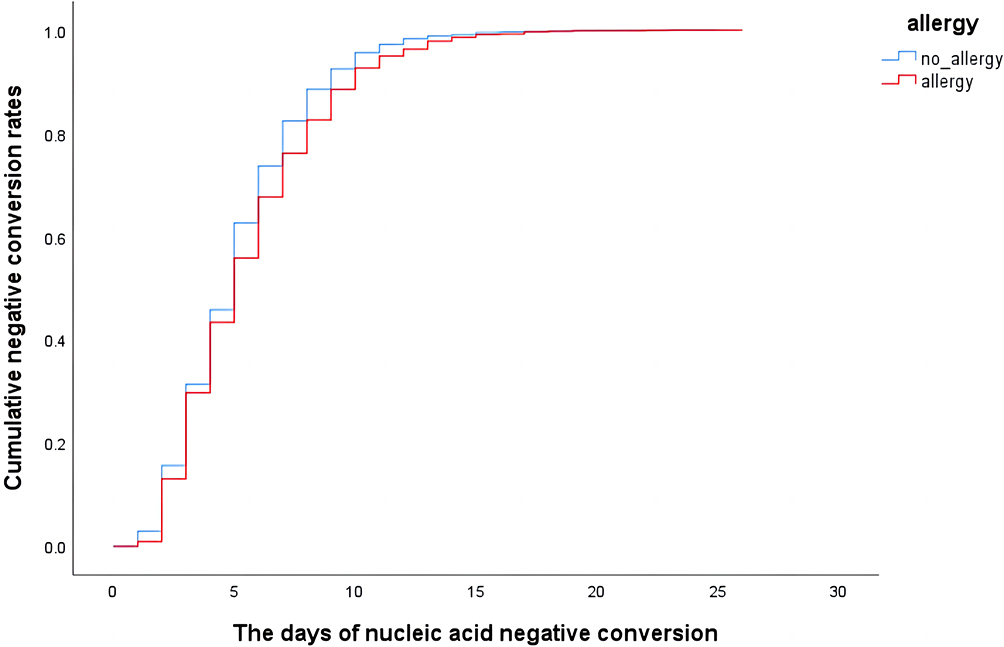 |
Figure 2 Overall survival analysis performed in the allergy group and non-allergy groups. The Kaplan–Meier method is used to analyze the time to the primary endpoint using a Log rank test. |
Differences in Days for Nucleic Acid to Turn Negative and Viral Load in Patients with Different Allergens
Further, we classify the allergens into the following categories: antibiotic allergy, Chinese herbal medicine allergy, foodborne allergy, antipyretic analgesic drug allergy, and NA (unknown allergen). As shown in Supplementary Table 1, the results of multiple comparisons and corrections showed that nucleic acid negative conversion days in patients with antibiotic allergy were significantly higher than in those with no history of allergy (5.61 vs 5.17, p < 0.001). The mean and lowest Ct values (ORF1ab and N genes) of patients with a history of allergy were significantly lower than those of COVID-19 patients without a history of allergy (p < 0.001). The minimum value of ORF1ab in COVID-19 patients with foodborne allergies was significantly lower than that in patients with no history of allergies (p < 0.01). Compared with patients without a history of allergy, there was no significant difference in viral load and nucleic acid turning negative days between patients with an allergy to traditional Chinese medicine and patients with an allergy to antipyretic and analgesic drugs (Supplementary Table 2; p > 0.05).
The Relationship Between Allergy and Clinical Signs in the Early Stage of Infection
At the initial stage of entering the Fang shelter hospital, 916 (42.1%) COVID-19 patients with a history of allergy showed positive signs, and 1345 (31.6%) patients in the non-allergic group showed positive signs (Supplementary Table 3). The proportion of cough, sputum, fatigue, fever, myalgia, sore throat, and stuffy nose symptoms in COVID-19 patients with an allergy history was higher than that in patients without an allergy history (p < 0.05).
Cohort B
Among COVID-19 patients with a history of allergies, there were 1832 patients with antibiotic allergies (age:47.64 (15.69), female:55.5%), and 62,293 patients with no history of allergies (age:44.92 (14.77), female:38.4%). After 1:2 PSM, there were 1675 COVID-19 patients with a history of antibiotic allergy and 3281 without an allergy history. There was no significant difference in the baseline characteristics of the cohort after PSM matching (Supplementary Table 4; Supplementary Figure 2; all p > 0.05).
Relationship Between Antibiotic Allergy and Viral Load and Days of Nucleic Acid Negative Conversion
The viral load and the days of nucleic acid negative conversion in patients with antibiotic allergy were significantly higher than those in non-allergic patients (p < 0.01) (Table 4). We divided antibiotics into six categories: penicillin, cephalosporins, sulfonamides, macrolides, quinolones, and NA (allergic to antibiotics, but the exact type is unknown). Compared with patients with no history of allergy, there were significant differences in days for nucleic acid to turn negative and viral load among patients with different kinds of antibiotic allergies (Supplementary Table 5). The results of multiple comparisons showed that the number of days for nucleic acid to turn negative in patients with penicillin allergy was significantly higher than that in patients with no history of penicillin allergy (5.63 vs 5.17, p < 0.01). The mean and lowest Ct values (ORF1ab and N genes) of patients with a history of penicillin allergy were significantly lower than those of COVID-19 patients without a history of allergy (p < 0.01). Patients with penicillin allergy had significantly higher viral loads than those with no history of allergy. There was no statistically significant difference in viral load or the number of days of negative nucleic acid conversion between patients with cephalosporin allergies, sulfonamides allergies, macrolides allergies, and quinolones allergies and those without allergy history (Supplementary Table 6; p > 0.05).
 |
Table 4 Differences in Days to Negative Conversion and Viral Load Between COVID-19 Patients with and without a History of Antibiotic Allergy |
The cumulative negative conversion rates at 5, 6, 7, 8, 9, and 10 days in the antibiotic allergy group were all lower than those in the non-allergy group (56.6% vs 62.6%; 67.6% vs.73.3%; 76.3% vs 82.4%; 82.8% vs 88.8%; 88.7% vs 92.7%; and 93% vs 95.8%; all p < 0.001) (Table 5). Log-rank analysis showed that patients with antibiotic allergy history had approximately 0.876-fold (95% CI 0.825–0.929, p < 0.001) lower conversion rates than those without allergy history (Figure 3).
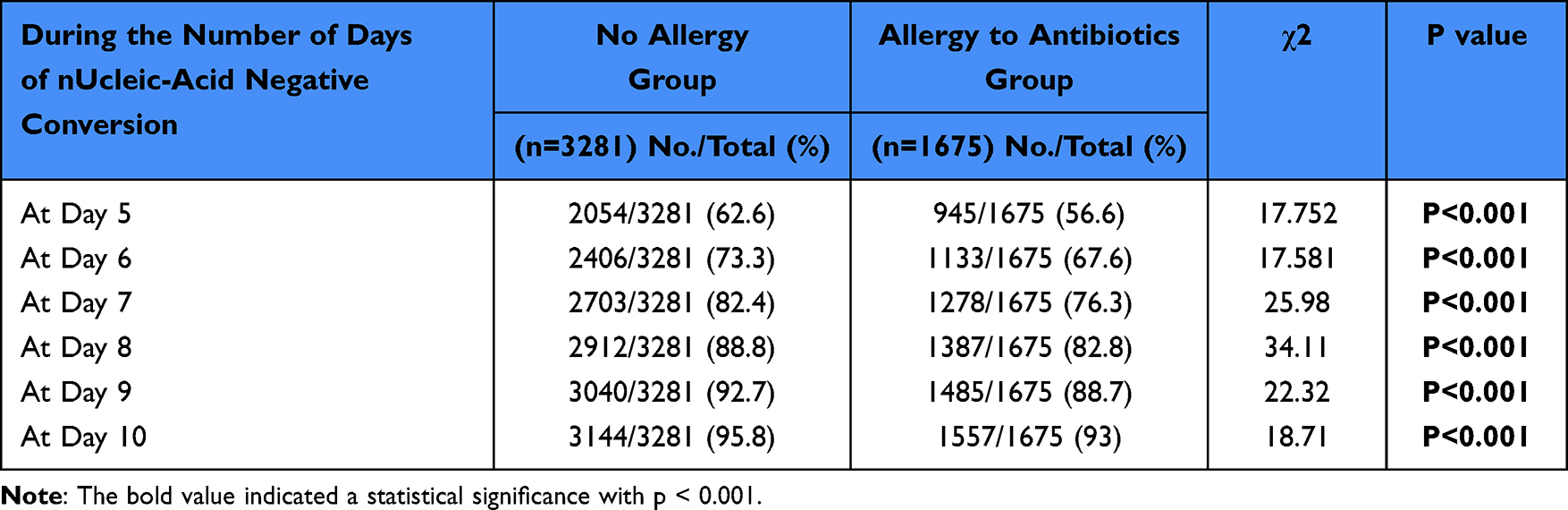 |
Table 5 Cumulative Negative Conversion Rates of SARS-CoV-2 Between COVID-19 Patients with and without a History of Antibiotic Allergy |
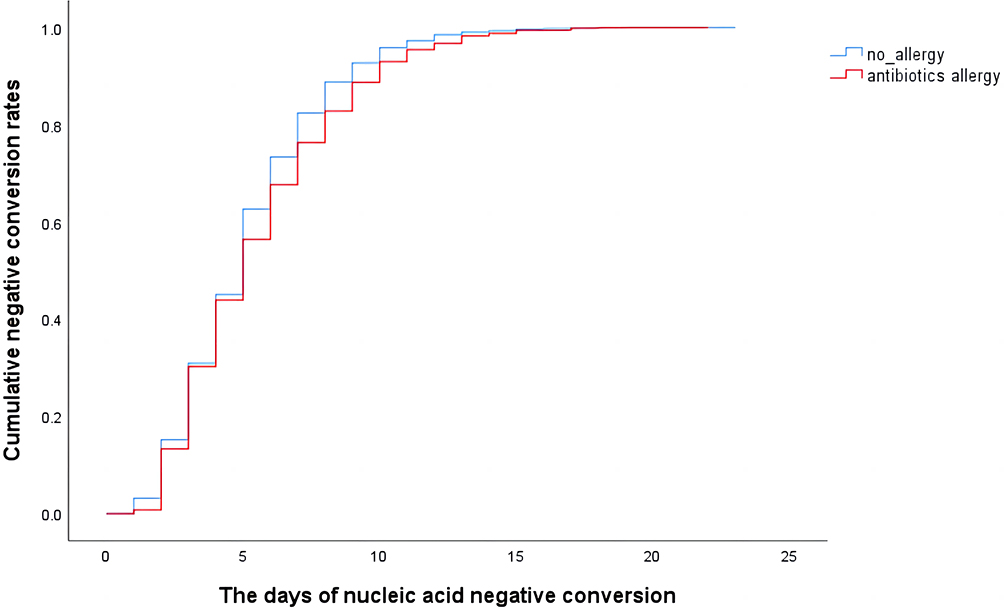 |
Figure 3 Overall survival analysis performed in the antibiotic allergy group and non-allergy group. The Kaplan–Meier method is used to analyze the time to the primary endpoint using a Log rank test. |
Relationship Between Antibiotic Allergy and Clinical Signs at the Beginning of Infection
In the early stages of infection, 709 (42.3%) patients in the antibiotic allergy group and 1053 (32.1%) patients in the non-allergy group showed positive signs (Supplementary Table 7). The proportion of cough, sputum, fatigue, fever, myalgia, sore throat, and stuffy nose symptoms in COVID-19 patients with antibiotic allergic history was higher than that in patients without allergic history (p < 0.05).
Discussion
This study investigated the association between allergic history and mild SARS-CoV-2 Omicron infection in 64,662 patients. We studied the association between clinical symptoms of COVID-19, viral load, days to negative nucleic acid, and allergic disease in 6430 Omicron-infected mild-symptom patients after 1:2 PSM matching. The history of allergy was related to the days of nucleic acid negative conversion and viral load in patients with Omicron mutant infection, and the allergic constitution was related to the prolongation of the duration for nucleic acid to turn negative. For people with a history of allergy, COVID-19 infection resulted in a higher SARS-CoV-2 viral load, more significant clinical symptoms, and longer days for nucleic acid negative conversion. This is a large retrospective cohort study designed to investigate the influence of various past allergens on the clinical outcomes of patients with mild Omicron variant infection.
The existing research on COVID-19 and allergic diseases mainly focuses on allergic asthma, allergic rhinitis, and allergic reactions to vaccines. It has been hypothesized that a pre-existing allergy may increase a person’s vulnerability to SARS-CoV-2 infection through various pathophysiological processes, which facilitates the entry of respiratory viruses into the bronchial epithelium of the upper and lower airways, resulting in a local inflammatory cascade.7,16 The vulnerability to hypersensitivity is triggered by neutrophil recruitment, T-lymphocyte translocation, and activation of resident monocytes, which results in a breakdown of the bronchial defense system, by stimulating the production of cytokines in epithelial cells such as IL-25 and IL-33.7 Eosinophilia, increased secretion of pro-inflammatory cytokines (ie, IL-4, IL-5, and IL-13), and elevated mucin synthesis are all results of TH2 activation through the SARS-CoV-2 pathway.7 These immunochemical alterations ultimately exacerbate respiratory symptoms.8 Innate interferon (IFN) secretion, including IFN-I and IFN-III, is impaired in allergic patients’ monocytes and airway epithelium, making them more vulnerable to respiratory viruses.17,18 These stimulate the expression of genes associated with antiviral activity through the well-known Janus kinase/signaling transducers and transcriptional activator pathways in bronchial epithelial and alveolar cells.19
We theorized that SARS-CoV-2 could make allergies worse, which in turn could increase the risk of viral infections and, ultimately, the devastating effects of COVID-19.20,21 Although they are both allergic diseases, it is worth noting that there is no potential association between atopic dermatitis and the clinical outcome of COVID-19.22 This means that when an infection progresses, the local immunological milieu of the respiratory system undergoes modifications. Patients with respiratory allergic diseases have a higher risk of deterioration of COVID-19 clinical outcomes, and the effects of the disease on the upper and lower respiratory tract appear to be more important than the systemic immunological effect.23 Therefore, spray-inhaled COVID-19 vaccine may be more suitable for allergic patients to protect them from infection.
We observed a significant association between food-borne allergy and penicillin allergy and lower Ct values, suggesting a potential link between immune system responses to viral infections in individuals with food-borne allergy. Notably, patients with food-borne allergy exhibit the presence of a specific immune cell type called mast cells in their blood. Currently, food allergy is known to involve IgE cross-linking, which triggers the activation of mast cells and basophils leading to the release of inflammatory mediators. Furthermore, chronic allergic inflammation resulting from eosinophil activation is believed to be associated with helper T lymphocytes 2 (TH2 cells), CD8 T cells, CD4 T cells, and basophils.24–26 However, it is worth noting that mast cells can also play a role in combating viral infections by releasing substances such as interferons, which inhibit viral replication. In the case of patients with foodborne allergies, however, it is possible that mast cells have been depleted or impaired, leading to a compromised defense against novel coronavirus infection and consequently, an increase in viral load. In response to penicillin allergy resulting in lower Ct values and longer negative nucleic acid days, As demonstrated by Lauren et al, the presence of penicillin allergy has been associated with an increased risk of adverse COVID-19 outcomes. Specifically, patients with penicillin allergy have shown a higher likelihood of experiencing infection recurrence and an extended duration of stay in the intensive care unit (ICU). These findings suggest that penicillin allergy may contribute to the worsening of COVID-19 outcomes in affected individuals.16 Although the exact molecular mechanism remains unclear, the presence of penicillin allergy poses limitations on antibiotic choices and may necessitate the use of broad-spectrum or alternative antibiotics during the course of the disease. This, in turn, can increase the likelihood of drug-related side effects. Moreover, the presence of penicillin allergy has been associated with a higher risk of adverse COVID-19 outcomes in affected patients.27 Our results show that patients with penicillin allergy have more days of negative conversion and higher viral load. Previous studies have shown that penicillin allergy labels increase the risk of deterioration of COVID-19 clinical results.16,28 Antibiotic use is widespread among COVID-19 patients; numerous studies have demonstrated that over 60% of patients (varying from 6% to 95%) utilize antibiotics.16,29 Commonly used antibiotics include moxifloxacin, azithromycin, cephalosporin, and penicillin. The influence of this extended and substitute antibiotic treatment may regulate the elevated risk of worse outcomes in patients with penicillin allergy in COVID-19.30 Due to the risk of penicillin allergy, including broader use of antibiotics, patients can experience more extended hospital stays, worse response to treatment, and increased resistance to antibiotics. Therefore, the position of the American Society of Allergy, Asthma, and Immunology supports further examination and testing of patients with documented penicillin allergy, and more than 90% of patients can clear the history of penicillin allergy after proper evaluation.31
Although the emergence of our study provides new insights into the relationship between allergic histories, days to nucleic acid turning negative, and viral load during COVID-19, this study has some limitations. First, the allergy history was obtained from the medical record system. The history of allergy and allergens were described by the patient according to the history of allergy, without allergen testing. There may be some undiscovered allergens in our inclusion of people without any allergic predisposition, which may influence the results. Second, since our data only included Omicron-infected patients, there may be a selection bias compared with the general population. Third, although we have taken into account confounding variables as much as possible, PSM is used to compensate confounding variables to make our results as reliable as possible, we most likely have not taken into account relevant confounding variables that are still unknown. Fourth, our study subjects were mainly mild patients. The relationship between allergy and disease progression has yet to be studied and validated for patients with more severe clinical conditions. In this study, although we observed a slight disparity in viral load and the number of nucleic acid negative days among patients with different allergies compared to non-allergic patients, it is crucial to interpret the findings cautiously. The underlying causes for these variances should be substantiated through prospective clinical studies and animal-based experiments to ensure the reliability of the results. Nonetheless, the outcomes of this study hold significant clinical and scientific value in guiding future basic experiments.
Conclusion
Based on these findings, allergic patients have higher viral load and more days of nucleic acid negative conversion after being infected by SARS-CoV-2 Omicron BA.2. Strategies to reduce these increased risks for allergic patients, especially those with antibiotic allergies, include early treatment to reduce immune overreaction and early vaccination, which may enhance the protective effect of allergic patients during the epidemic.
Acknowledgments
We acknowledge all the health care workers for their help.
Funding
This study has received funding from Magor science and technology projects of Chongqing city (Grant No. cstc2018jszx-cyztzxX0017),the Young and Middle-aged Medical Talents Foundation Project of Chongqing (Grant No. 414Z395), Emergency Project for Technological Breakthrough in Clinical Treatment of Hospital-acquired COVID-19 Infection in 2023 (Grant No.2023XGIIT07), National Key Research and Development Program of China (Grant No.2021YFF0704100).
Disclosure
The authors declare that there is no conflict of interest regarding the publication of this paper.
References
1. Available from: https://covid19.who.int/.
2. Hoffmann M, Kruger N, Schulz S, et al. The Omicron variant is highly resistant against antibody-mediated neutralization: implications for control of the COVID-19 pandemic. Cell. 2022;185:447–56 e11.
3. Du H, Dong X, Zhang JJ, et al. Clinical characteristics of 182 pediatric COVID-19 patients with different severities and allergic status. Allergy. 2021;76(2):510–532. doi:10.1111/all.14452
4. Baseggio Conrado A, Ierodiakonou D, Gowland MH, Boyle RJ, Turner PJ. Food anaphylaxis in the United Kingdom: analysis of national data, 1998–2018. BMJ. 2021;372:n251. doi:10.1136/bmj.n251
5. Krishnamoorthy N, Douda DN, Bruggemann TR, et al. Neutrophil cytoplasts induce TH17 differentiation and skew inflammation toward neutrophilia in severe asthma. Sci Immunol. 2018;3(26). doi:10.1126/sciimmunol.aao4747
6. Hou X, Luo W, Wu L, et al. Associations of Four sensitization patterns revealed by Latent Class Analysis with Clinical symptoms: a multi-center study of China. EClinicalMedicine. 2022;46:101349.
7. Yang JM, Koh HY, Moon SY, et al. Allergic disorders and susceptibility to and severity of COVID-19: a nationwide cohort study. J Allergy Clin Immunol. 2020;146(4):790–798. doi:10.1016/j.jaci.2020.08.008
8. Lu L, Mok BW, Chen LL, et al. Neutralization of SARS-CoV-2 Omicron variant by sera from BNT162b2 or Coronavac vaccine recipients. Clin Infect Dis. 2021;75(1):e822–e826.
9. Gilles S, Blume C, Wimmer M, et al. Pollen exposure weakens innate defense against respiratory viruses. Allergy. 2020;75(3):576–587. doi:10.1111/all.14047
10. Leino A, Lukkarinen M, Turunen R, et al. Pulmonary function and bronchial reactivity 4 years after the first virus-induced wheezing. Allergy. 2019;74:518–526.
11. Papadopoulos NG, Christodoulou I, Rohde G, et al. Viruses and bacteria in acute asthma exacerbations--a GA² LEN-DARE systematic review. Allergy. 2011;66(4):458–468. doi:10.1111/j.1398-9995.2010.02505.x
12. Dong X, Cao YY, Lu XX, et al. Eleven faces of coronavirus disease 2019. Allergy. 2020;75(7):1699–1709. doi:10.1111/all.14289
13. Guideline on diagnosis and treatment of COVID-19; 2022. Available from http://www.nhc.gov.cn/yzygj/s7653p/202203/b74ade1ba4494583805a3d2e40093d88/files/ef09aa4070244620b010951b088b8a27.
14. Austin PC. A critical appraisal of propensity-score matching in the medical literature between 1996 and 2003. Stat Med. 2008;27:2037–2049.
15. Kim SY, Yeniova AÖ. Global, regional, and national incidence and mortality of COVID-19 in 237 countries and territories, January 2022: a systematic analysis for World Health Organization COVID-19 Dashboard. Life Cycle. 2022;2. doi:10.54724/lc.2022.e10
16. Kaminsky LW, Dalessio S, Al-Shaikhly T, Al-Sadi R. Penicillin allergy label increases risk of worse clinical outcomes in COVID-19. J Allergy Clin Immunol Pract. 2021;9(10):3629–37.e2. doi:10.1016/j.jaip.2021.06.054
17. Gutierrez-Merino J, Isla B, Combes T, Martinez-Estrada F, Maluquer De Motes C. Beneficial bacteria activate type-I interferon production via the intracellular cytosolic sensors STING and MAVS. Gut Microbes. 2020;11:771–788.
18. Kimura I, Konno Y, Uriu K, et al. Sarbecovirus ORF6 proteins hamper induction of interferon signaling. Cell Rep. 2021;34(13):108916. doi:10.1016/j.celrep.2021.108916
19. Turner PJ, Gowland MH, Sharma V, et al. Increase in anaphylaxis-related hospitalizations but no increase in fatalities: an analysis of United Kingdom national anaphylaxis data, 1992–2012. J Allergy Clin Immunol. 2015;135(4):956–63 e1. doi:10.1016/j.jaci.2014.10.021
20. Moghimi SM. Allergic reactions and anaphylaxis to LNP-based COVID-19 vaccines. Mol Ther. 2021;29(3):898–900. doi:10.1016/j.ymthe.2021.01.030
21. Mullins RJ, Wainstein BK, Barnes EH, Liew WK, Campbell DE. Increases in anaphylaxis fatalities in Australia from 1997 to 2013. Clin Exp Allergy. 2016;46:1099–1110.
22. Vezir E, Hizal M, Cura Yayla B, et al. Does aeroallergen sensitivity and allergic rhinitis in children cause milder COVID-19 infection? Allergy Asthma Proc. 2021;42(6):522–529. doi:10.2500/aap.2021.42.210087
23. Singhal T. The Emergence of Omicron: challenging Times Are Here Again! Indian J Pediatr. 2022;89(5):490–496. doi:10.1007/s12098-022-04077-4
24. Yu W, Freeland DMH, Nadeau KC. Food allergy: immune mechanisms, diagnosis and immunotherapy. Nat Rev Immunol. 2016;16:751–765.
25. Valenta R, Hochwallner H, Linhart B, Pahr S. Food allergies: the basics. Gastroenterology. 2015;148:1120–31.e4.
26. Cianferoni A, Votto M, Marseglia GL. COVID-19 and allergy: how to take care of allergic patients during a pandemic? Pediatr Allergy Immunol. 2020;31(Suppl 26):96–101. doi:10.1111/pai.13367
27. Rose M, Trubiano J. Assessing low-risk penicillin allergies in critical COVID-19, a novel perspective on an emerging antibiotic allergy opportunity. J Allergy Clin Immunol Pract. 2023;11(2):636–637. doi:10.1016/j.jaip.2022.11.048
28. Pérez-Encinas M, Lorenzo-Martínez S, Losa-García JE, Walter S, Tejedor-Alonso MA. Impact of penicillin allergy label on length of stay and mortality in hospitalized patients through a clinical administrative national dataset. Int Arch Allergy Immunol. 2022;183:498–506.
29. Sacco KA, Bates A, Brigham TJ, Imam JS, Burton MC. Clinical outcomes following inpatient penicillin allergy testing: a systematic review and meta-analysis. Allergy. 2017;72(9):1288–1296. doi:10.1111/all.13168
30. Harrison SL, Fazio-Eynullayeva E, Lane DA, Underhill P, Lip GYH, Kretzschmar MEE. Comorbidities associated with mortality in 31,461 adults with COVID-19 in the United States: a federated electronic medical record analysis. PLoS Med. 2020;17(9):e1003321. doi:10.1371/journal.pmed.1003321
31. Sieswerda E, de Boer MGJ, Bonten MMJ, et al. Recommendations for antibacterial therapy in adults with COVID-19 - an evidence based guideline. Clin Microbiol Infect. 2021;27:61–66.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Old Age is an Independent Risk Factor for Pneumonia Development in Patients with SARS-CoV-2 Omicron Variant Infection and a History of Inactivated Vaccine Injection
Tong X, Huang Z, Zhang X, Si G, Lu H, Zhang W, Xue Y, Xie W
Infection and Drug Resistance 2022, 15:5567-5573
Published Date: 21 September 2022
Could the New BA.2.75 Sub-Variant Cause the Emergence of a Global Epidemic of COVID-19? A Scoping Review
Shaheen N, Mohamed A, Attalla A, Diab RA, Swed S, Nashwan AJ, Rababah AA, Hefnawy MT, Soliman Y, Abdelwahab OA, Desouki MT, Khaity A, Shaheen A, Ramadan A, Meshref M
Infection and Drug Resistance 2022, 15:6317-6330
Published Date: 31 October 2022
Clinico-Epidemiological Profile of COVID-19 Patients with Omicron Variant Admitted in a Tertiary Care Center, South India
Ethirajan T, Natarajan G, Velayudham R, Jayakumaran P, Karnan I, Rajendran K, Doraisamy S, Chenakeswarar Sridhar S, Kumaran P, Kamaraj K, Kandasamy A, Natarajan M
International Journal of General Medicine 2023, 16:185-191
Published Date: 17 January 2023
Value of Laboratory Indicators in Predicting Pneumonia in Symptomatic COVID-19 Patients Infected with the SARS-CoV-2 Omicron Variant
Zhu K, Ma S, Chen H, Xie J, Huang D, Fu C, Ma G, Huang Y
Infection and Drug Resistance 2023, 16:1159-1170
Published Date: 28 February 2023
Predictors of COVID-19 Severity in Elderly Patients Infected by Omicron in China, 18 December 2022–5 February 2023
Xing Y, Li Y, Feng L, Huo R, Ma X, Dong Y, Liu D, Niu Y, Tian X, Chen E
Infection and Drug Resistance 2023, 16:4505-4518
Published Date: 11 July 2023