Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 12
Practice of Early Childhood Developmental Milestone Assessment and Its Determinants Among Health Professionals Working at Public Hospitals in Addis Ababa, Ethiopia: A Cross-Sectional Study
Authors Tesfay H ![]() , Sebsibe G
, Sebsibe G ![]() , Tesfaye T
, Tesfaye T ![]()
Received 25 March 2021
Accepted for publication 3 August 2021
Published 27 November 2021 Volume 2021:12 Pages 521—532
DOI https://doi.org/10.2147/PHMT.S300397
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Roosy Aulakh
Haileslassie Tesfay,1 Girum Sebsibe,2 Tewodros Tesfaye2
1College of Medicine and Health Sciences, Debre Birhan University, Debre Birhan, Ethiopia; 2Department of Nursing, School of Nursing and Midwifery, Addis Ababa University, Addis Ababa, Ethiopia
Correspondence: Tewodros Tesfaye
Department of Nursing, School of Nursing and Midwifery, Addis Ababa University, PO Box 4412, Addis Ababa, Ethiopia
Tel +251 913 69 80 81
Email [email protected]
Background: Early childhood developmental assessment refers to the continual process of observing, gathering, recording, and interpreting information to make developmental and instructional decisions and measure young children’s performance over time. Significant changes in the physical and neuropsychomotor developmental milestones take place in the first 2 years of life. Children younger than 3 years of age (36 months) who are at risk of having developmental delays may be eligible for early intervention treatment services. The study aimed to assess practice in early childhood developmental assessment and its determinants among health professionals working in public hospitals in Addis Ababa, Ethiopia.
Methods: This facility-based descriptive cross-sectional study was conducted from September to April 2018, with a total sample size of 268 health professionals from six public hospitals in Addis Ababa, Ethiopia. The data were entered into EpiData software version 4.2, and analyzed by SPSS version 23 software for bivariate and multivariable logistic regression analysis. Significant associations were taken as p< 0.05 and the strength of associations was expressed using odds ratios.
Results: The practice of early childhood developmental milestone assessment was found to be 27.8%. Being a general practitioner (AOR=23.826, 95% CI: 6.77– 83.9, p=0.000) or health officer (AOR=11.02, 95% CI: 2.1– 58.812, p=0.005), and work experience greater than 11 years (AOR=20.897, 95% CI: 1.5– 291.49, p=0.024) were significantly associated with good practice of early childhood developmental milestone assessment.
Conclusion: Practice of early childhood developmental milestone assessment remains poor. Training and sharing experiences among different professions, and assigning professionals with the highest levels of work experience in the service could improve the practice levels.
Keywords: early childhood, developmental milestone assessment, practice
Introduction
Early childhood developmental assessment refers to the continual process of observing, gathering, recording, and interpreting information to make developmental and instructional decisions and measure young children’s performance over time.1 Significant changes in physical and neuropsychomotor development take place in the first 2 years of life.2 Children younger than 3 years of age (36 months) who are at risk of having developmental delays may be eligible for early intervention treatment services.3 According to the WHO classification, early childhood refers to birth to 5 years.4
When a child is not developing and/or achieving skills according to the expected time frame, he or she should be suspected of having developmental delay.8 Currently, many countries use child development surveillance to monitor developmental status.9 Despite the technical advances in assessing this major parameter, little is known about the practice of early childhood developmental milestone assessment.
In developing nations, 200 million children (~39%) under age 5 are not reaching their developmental potential because of easily preventable factors.10 Low- and middle-income (LMIC) countries face new challenges in promoting child development.11 Studies from the US Centers for Disease Control and Prevention (CDC) show that the prevalence of developmental disabilities in the USA from 1997 to 2008 was 13.7%.12 This huge gap in child developmental problems between developed and developing countries is due to the lack of a system for the promotion and monitoring, prevention, early identification, and early intervention strategies in early childhood development.11
A detailed initial developmental assessment leads to the diagnosis of 20% of cases of developmental delay (DD). In the USA, many children with developmental disabilities were identified after age 10, when significant delays may have already occurred and opportunities for treatment may have been missed.12 This shows that the practice of early childhood developmental assessment and intervention is still low, even in developed countries.
In high-income countries, the early identification of a young child who has developmental delays or deficits is recognized as an essential part of good healthcare for children in regular pediatric practice.14 It is an integral function of the primary care medical home and an appropriate responsibility of all pediatric health care professionals. Any concerns arising during monitoring and surveillance should be promptly addressed with standardized developmental screening tests.15
Despite many recommendations and the proven effectiveness of early childhood developmental assessment, the practice remains low, even in developed countries. In a study in Brazil, the percentage of respondents completing child development surveillance was 1.1%.16 The level of consistent, universal use of these tools was only 2.6%.17
A review on global perspectives in early diagnosis and intervention describes that physicians’ attitudes, awareness, insufficient training, doubt about the value of early detection, uncertainty about how or where to refer, time limitations of the clinic visit, inadequate reimbursement, cost factors, and concern about unnecessarily alerting a family are some of the factors that influence the acceptance and practice of detection of, and interventions for, children with developmental problems.22 Good developmental screening instruments can correctly identify more than 75% of children with problems.24 Anticipatory guidance based on the surveillance assessment data helps parents to anticipate the next developmental stage and stimulate developmentally appropriate behaviors.
Barriers to the practice of using standard tools include a lack of time (93%), lack of training in the use of appropriate screening tools (88%), lack of mental health providers (79%), and lack of adequate personnel (77%).17 A study in Philadelphia identified a lack of agreement in parents’ assessments of child development, clinicians’ preference to rely on their clinical acumen; and limited time, insurance reimbursements, and training on screening as barriers to the service.25
Even though the practice of early childhood developmental assessment in Ethiopia is not yet documented, the prevalence of global developmental delay constitutes a significant public health problem. Previous studies have emphasized the importance of child developmental assessment for the early identification, treatment, and referral of developmental problems. Worldwide, the practice of early identification of child developmental problems is low, as seen in the literature. Therefore, this study aimed to assess the practice of health professionals’ early childhood developmental milestone assessment in the study area.
Methodology
Ethical Considerations
Ethical clearance was obtained from Addis Ababa University School of Nursing and Midwifery ethical review committee and then a letter of permission was obtained from the school. Letters of cooperation were written to Addis Ababa Health Bureau, Ethiopian Ministry of Health, and each hospital administrative department. Then, study participants were asked about their willingness to participate in the study, both verbally and through a written consent form on the cover page of the questionnaire. All the reasons why the participants were chosen and why the research was being conducted were explained to the study participants. Confidentiality was maintained by avoiding writing any personal identification on the questionnaire and the participants were informed that they had the right not to participate in the study. Study participants were aware that they would neither gain, nor benefit, nor be harmed by the outcome and process of this study.
Study Design and Period
A facility-based descriptive cross-sectional study design was employed to collect data from September 2017 to April 2018.
Sample Size Determination
The sample size was determined using the single-population proportion formula:
Assumptions: n=required sample size, Zα/2=critical value for the normal distribution at 95% confidence level (1.96), p=50% prevalence (P) of practice of child development assessment among health professionals, and d=0.05 (margin of error). The formula used for the sample size calculation led to a number of 384. However, as the study population was <10,000, the correction formula (Nf=n/(1+n/N)) was used, where Nf=final sample size, n=calculated sample size (ie, 384), and N=total study population (ie, 660). With a 10% non-response rate, the final estimated sample size was found to be Nf=267.
Sampling Procedure
Study populations were selected from six randomly selected public hospitals in Addis Ababa with a pediatric care unit using a simple random selection technique. The sampling units were selected from each hospital by allocating the total sample proportionately. Then, the study units were determined by a systematic random sampling technique after obtaining the sampling frame from the institutional lists. Separate K-intervals were calculated to select sampling units from each selected hospital. During proportional allocation, decimal numbers were approximated and only one subject was added to the actual sample size, which became 268.
Operational Definition
Practice
The overall practice was categorized into poor and good practice based on the calculated mean value. Those who scored above the mean were considered as having good practice and those who scored below the mean were considered as having poor practice. In this study, knowledge and attitude were independent variables and were categorized into average and above and below average, based on the calculated mean score of the variables, to determine their association.
Data Collection Tool and Procedure
Structured questionnaires were adapted from previous studies.4,25–27 The self-administered questionnaires and observational checklists were composed of questions on the practice of health professionals in child developmental assessment and questions addressing the socio-demographic, professional, and institutional variables. Six health professionals with a BSc degree and two supervisors with an MSc who were working in childcare services at other hospitals outside the study units were recruited and trained for data collection and supervision. The self-administered questionnaire and observational checklist were applied, which took a total of 15 minutes. Selected health professionals were observed during procedural assessment and then provided with the self-administered questionnaire. The data collection process was closely supervised. Data were collected in each hospital during working time. When the study participants were absent or on other rounds, the data collector rechecked at least three times at the appropriate time.
Study Variables
Health professionals’ practice on early childhood developmental milestone assessment was the outcome (dependent) variable. Independent variables included socio-demographic variables (sex, age, marital status, profession, service year, working unit, educational level), professional characteristics (training, awareness, attitude, knowledge), and facility and service variables (workload, time, duration of the work, referral choices, availability of assessment tools, source of information, supervision, screening service).
Data Quality Assurance
A questionnaire was adapted and modified for data collection. Eight experts (three from educational settings and five from clinical settings with a pediatrics specialty) evaluated the questionnaire for validity and consistency by filling in Likert scale measurements. The questionnaire was modified based on the comments given, and the content validity index (CVI) was calculated for each question; those with a CVI less than 0.7 were rejected. The total CVI was 0.955. Then, a pretest was carried out in 5% of the population in another hospital outside the study population to measure the consistency and clarity of the questionnaire. Based on the pretest results, the questionnaires were modified to ensure clarity. Training for data collectors and supervisors was given. Data collection was strictly supervised. Respondents were blinded during observation. Data cleaning was carried out immediately after the questionnaires were collected and any with less than 80% complete information were rejected. Data were cleaned and checked for completeness before data entry. Additional data cleaning and recoding were conducted using SPSS. The reliability of the data was checked by calculating the Cronbach’s alpha, which was 0.78. Multicollinearity among independent variables was assessed. The work experience and age of the health professionals had no multicollinearity effect on practice, with a variance inflation factor (VIF) of 1.163 and a tolerance of 0.860. Outliers were shown on a Q-Q plot test to select the appropriate measure of central tendency. The Hosmer and Lemeshow fitness test was used to ensure the model fitness on multivariable analysis of the binary logistic regression, and this was insignificant at a value of 0.716.
Data Analysis and Interpretation
Data were coded and entered into EpiData software, version 4.2, and then exported to and analyzed using SPSS version 23 software for descriptive statistics and bivariate and multivariate logistic regression (LR) analysis. Significant variables detected at the bivariate level were subsequently entered into a multivariate logistic regression model to control for possible confounding variables and to examine associations. Significant associations were taken as p<0.05. The strength of associations was expressed using odds ratios (ORs). Data were processed using simple descriptive statistics, ie, mean and standard deviation (SD) and frequencies with percentage distribution. Determinant variables were summarized in logistic regression tables.
Results
Socio-Demographic Characteristics of Respondents
For the 268 study subjects, the total response rate was 96.64% (N=259). The respondents were between the ages of 20 and 50 years, with a mean±SD age of 30.4±5.8 (range 20–48) years; 42.9% of the respondents’ ages ranged between 26 and 30 years (n=110) and 20.1% between 20 and 25 years (n=52). About half, 133 (51.4%), of the respondents were male and 142/259 (54.8%) were single in their marital status. Of the respondents, 176 were nurses (54.2%) (Table 1).
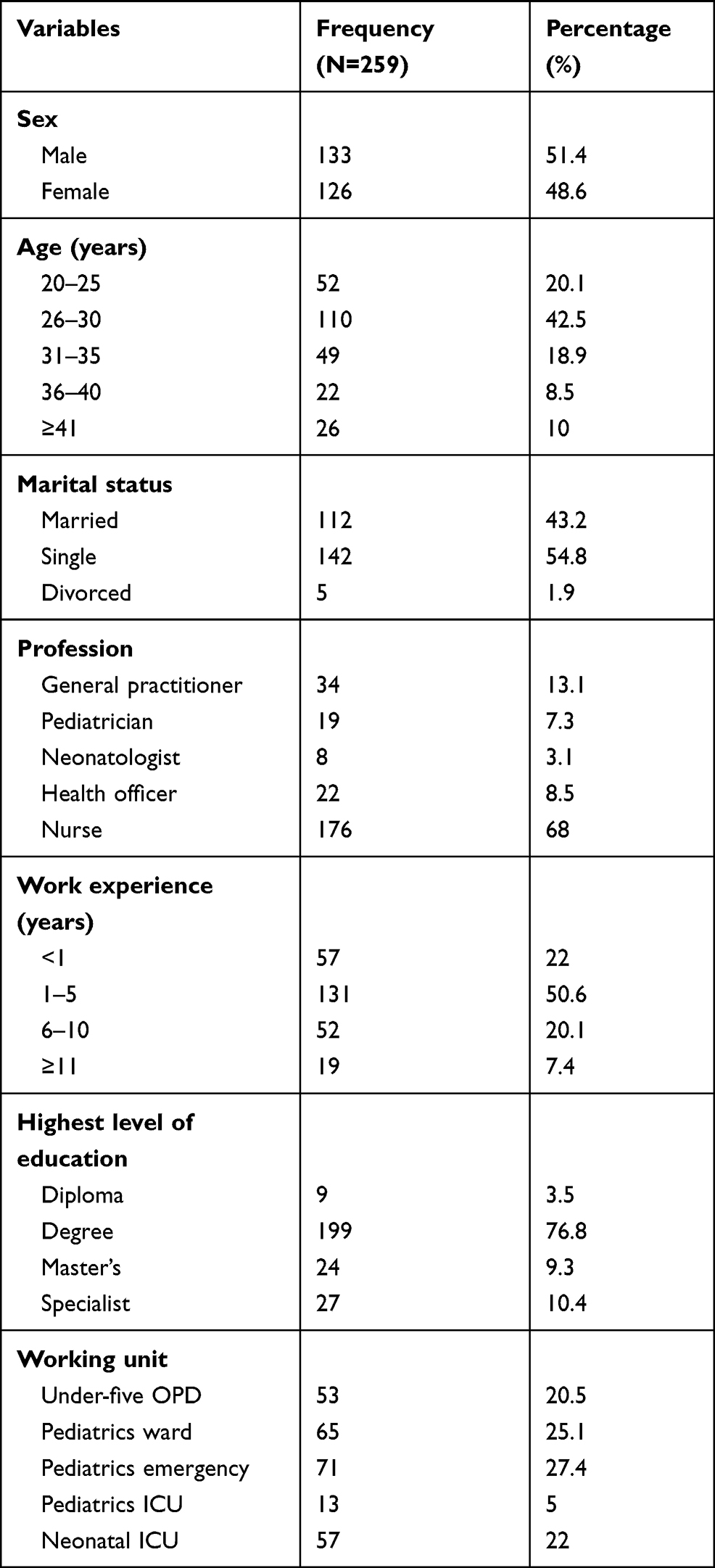 |
Table 1 Socio-Demographic Characteristics of Health Professionals Working in Public Hospitals, Addis Ababa, Ethiopia, 2018 (N=259) |
Professional and Institutional Variables in Child Developmental Milestone Assessment
From N=259 respondents, the majority of health professionals, 84.9% (n=220), reported that they assess children for developmental disorders in their childcare practice set-up. The majority of them, 58.6% (n=129), reported that they apply child developmental assessment at all well and sick children’s visits. The majority of health professionals, 88%, had received information on child developmental assessment during their college education; only 22.8% (n=59) had received additional training on child developmental assessment and 44.1% (n=26) of them had been trained by university educators as a project. The majority of health professionals, 62.2% (n=161), make appointments for children for developmental screening and 30.9% (n=50) reported making appointments for developmental screening only when a previous developmental assessment demonstrates a risk. Only 36.7% (n=95) of respondents reported that they use a standardized developmental screening tool to assess the developmental status of the child, and 56.25% of them used an ages and stages questionnaire tool for developmental assessment (Figures 1 and 2).
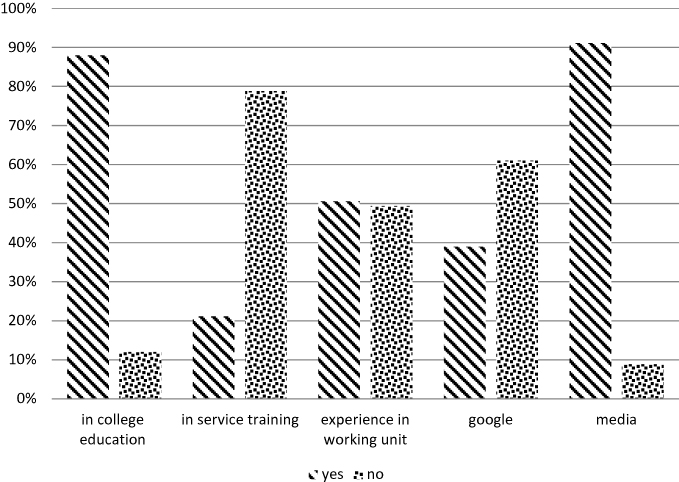 |
Figure 1 Source of information on child developmental milestone assessment (N=259). |
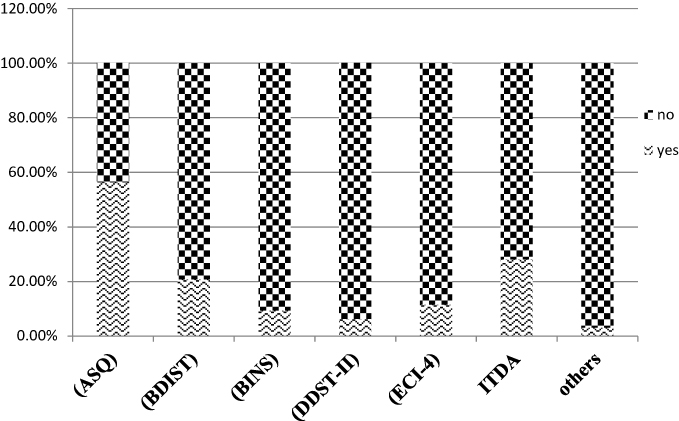 |
Figure 2 Developmental assessment tools used by health professionals working at public hospitals in Addis Ababa, Ethiopia, 2018. |
Health Professionals’ Awareness of Child Developmental Screening and Surveillance Service
The majority of health professionals, 78.4% (n=203), reported that they had information on the child developmental screening and surveillance service, but 81.8% (n=166) of them correctly defined the type of service as regular age-appropriate developmental assessment by health professionals. Thirty five percent (n=91) of health professionals reported that they were aware of the child developmental screening and surveillance service in Ethiopia. Based on profession, 75% of nurses and all neonatologists and pediatricians correctly defined developmental screening and surveillance service as regular age-appropriate developmental assessment by health professionals.
Knowledge of Health Professionals on Child Developmental Assessment
The highest knowledge score was seen in the physical development domain; 58% (n=150) had good knowledge on physical development, with a mean value of 2.64 and above, SD= ±1.08 (range 0–4). The lowest knowledge score was found for cognitive development, with only 21.2% (n=55) scoring average and above, with a mean±SD value of 1±0.704 (range 0–3). In the social developmental milestone domain, 48.3% (n=125) scored above the mean value of 1.67±1.123 (range 0–5). Regarding the emotional and language developmental domains, 42.5% (n=110) and 45.9% (n=119) scored average and above, with the same mean values of 1.47±0.967 and 1.47±0.733 (ranges 0–5 and 0–3), respectively. Overall, 39.4% (n=102) of health professionals had good knowledge of child developmental milestone assessment, with a mean±SD value of 2.15±1.214 (range 0–5) (Table 2).
 |
Table 2 Knowledge of Health Professionals on Early Childhood Developmental Milestone Assessment |
Practice of Health Professionals on Child Developmental Milestone Assessment
From N=259 participants, only 28.6% (n=73) reported that they assess the child for developmental milestone status. Of those who perform the assessment, 82.2% (n=60) ask about child developmental risk factors. Feeding and nutritional patterns, gynecological–obstetric risk factors, and family history of mental illness are the most frequently assessed developmental risk factors, with frequencies of 88.3%, 75%, and 70%, respectively. Only 13.7% (n=10) of the health professionals who assess the child developmental status use standardized developmental screening tool as a guide for reference. Seven (70%) of those who use the assessment tool had downloaded it to their mobile phone. There was no standardized child developmental assessment tool kept as hard copy for office reference.
Therefore, from N=259 participants, 27.8% (n=72) of the health professionals had good practice of early childhood developmental assessment, with a mean±SD value of 1.46±2.4 (range 0–8) (Figure 3).
 |
Figure 3 Practice of health professionals on early childhood developmental assessment. |
Determinants of Early Childhood Developmental Assessment Practice
Bivariate and multivariable logistic regression was performed to determine the association of different determinant variables with health professionals practice of early child developmental milestone assessment. All variables that had an association with the outcome variables in bivariate logistic regression analyses at 0.25 level were included in the multiple logistic regression models. After controlling for the effects of potentially confounding variables using multiple logistic regression, only two variables (profession and work experience) remained significantly associated with health professionals’ practice of early childhood developmental milestone assessment at p<0.05. Of the professionals, general practitioners were more than 23 times more likely to practice early childhood developmental milestone assessment than nurses (AOR=23.826, 95% CI: 6.77–83.9, p=0.000). In addition, health officers were more than 11 times more likely to perform the practice than nurses (AOR=11.02, 95% CI: 2.1–58.812, p=0.005. Health professionals with work experience greater than 11 years were more than 20 times more likely to practice early childhood developmental assessment than those who had less than 1 year’s work experience (AOR=20.897, 95% CI: 1.5–291.49, p=0.024) (Table 3).
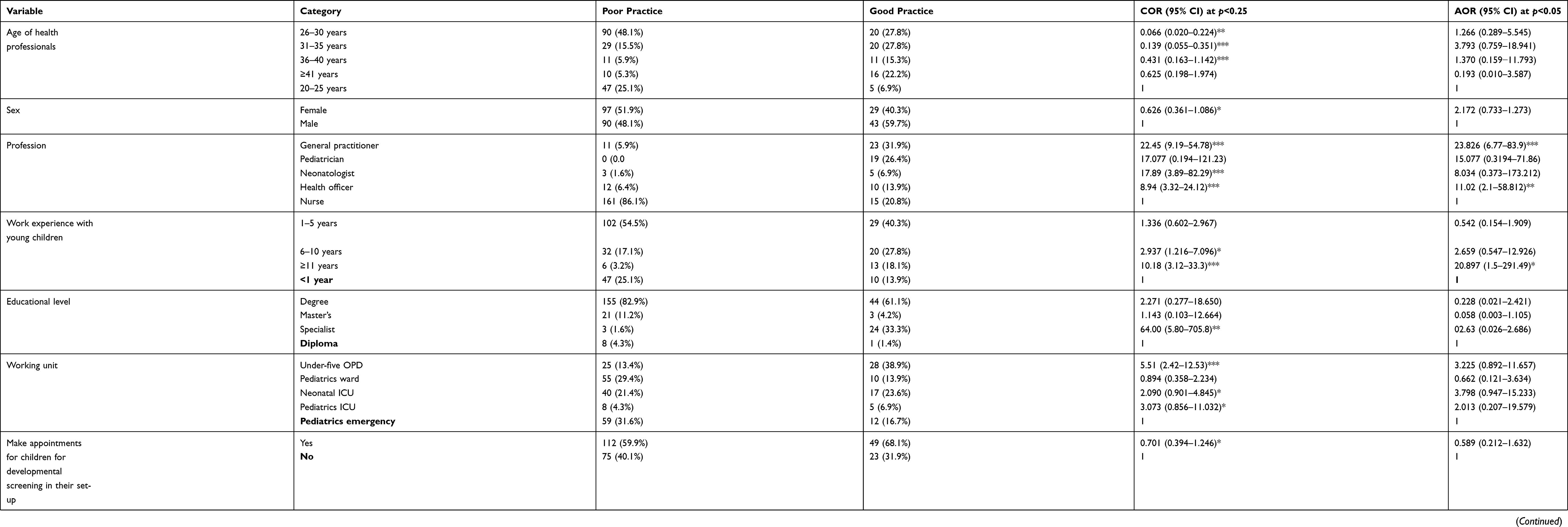 |
Table 3 Determinants on Practice of Health Professionals in Child Developmental Milestone Assessment Working in Public Hospitals, Addis Ababa, Ethiopia, 2018 (N=259) |
Discussion
In this study, from a total of 259 participants, only 28.6% reported that they assess the child for developmental milestone status. Only 3.68% of the health professionals use a standardized developmental screening tool as a guide for reference. Of the participants, 18.5% classify the child for developmental delay and 18.1% use a clinical diagnosis classification system. Only 0.77% use the Integrated Management of Childhood Illness (IMCI) context classification system for child developmental delay. A study on the attitudes, practices, and barriers in primary care practitioners in screening emotional–behavioral problems in children showed that traditional techniques and clinical observation are the most commonly used, with over 90% of respondents endorsing non-standardized interviewing (review of systems). Consistent, universal use of standardized assessment tools was endorsed by only 2.6% of respondents.17 Therefore, our research finding is similar to the previous research finding, which showed that the use of standardized child developmental milestone assessment tools was low and health professionals rely more on clinical observation than on systematized instruments. Research has shown that a good developmental screening instrument can correctly identify more than 75% of children with problems,24 but despite this, the level of practice of using this important tool was low. Our study even found that there is no standardized child developmental assessment tool kept as hard copy for office reference. Seven health professionals who practice the child developmental milestone assessment use a reference tool on their mobile.
In this study, only 27.8% of health professionals reported that they perform child developmental screening at regular intervals (9, 18, 24, 30, and 36 months). The American Academy of Pediatrics (AAP) 2007 recommends surveillance at every visit for well and sick child visits and standardized screening at 9 months, 18 months, 24 and/or 30 months, and pre-kindergarten. The application of this basic childcare recommendation was low in our study. Although research findings indicate that the majority of countries accept the importance of using surveillance tools, the practice of using the tools regularly is low.4 This finding is consistent with our research finding.
Overall, 27.8% of health professionals in the present study have good practice of early childhood developmental assessment. A study on family health strategies in João Pessoa, Brazil, found that 75.4% did not have the child developmental assessment supplementary guide.16 This finding is consistent with our research finding, which could be due to the reason that in both studies there was a lack of referral forms and a lack of developmental milestone assessment tools. Although it has been shown that anticipatory guidance based on the surveillance assessment data helps parents to anticipate the next developmental stage and stimulate developmentally appropriate behaviors, this study shows low practice of counseling based on the findings of child developmental assessment.15
This study found that 27.79% of health professionals ask the family for their opinion on their child’s development and 23.5% provide guidance to the family on how to stimulate child development. Only 3.86% of health professionals use a standardized developmental assessment tool to evaluate the child’s development. An intervention study conducted with nurses in Latin America on child development surveillance showed that 73% of nurses asked the opinion of mothers about their children’s development and 91% of nurses provided guidance to mothers on how to stimulate child development. Only 42% of nurses used a systematized instrument to evaluate child developmental status.4 The difference in the frequency between these studies may result from differences in professional characteristics and service provision setting, in that the study in Latin America included only nurse professionals who worked in primary health care, whereas this study involved various professionals who worked at public hospitals.
Although there were no other findings reporting the degree of association of determinant variables, in this study, being a general practitioner as a profession and having at least 11 years’ experience were significantly associated with health professionals’ practice in early childhood developmental milestone assessment. General practitioners were more than 23 times more likely to practice early childhood developmental milestone assessment than nurses. In addition, health officers were more than 11 times more likely to perform the practice than nurses. General practitioners and health officers mostly provide their services in an outpatients setting, where relatively healthy children are seen, which is an appropriate place to provide basic childcare services. In addition to this, there is a difference between these professions regarding the care and treatment of children in these hospitals.
This study also shows that health professionals with work experience of more than 11 years were more than 20 times more likely to practice early childhood developmental assessment than those who had less than 1 year’s work experience. This may be due to their experience, which gave them skills in providing health services.
Conclusion
The findings of this research show that the practice of early childhood developmental milestone assessment was poor. Profession and years of experience are variables that are significantly associated with health professionals’ practice in early childhood developmental milestone assessment. Training and retraining of all health professionals, and the sharing of experience among professionals with the highest levels of work experience could improve the practice level. Health professionals should be encouraged to place emphasis on child developmental milestone assessment practice, because this assessment service is the only indicator that can be used to determine and intervene in any developmental problems early in life, before significant morbidities occur. In addition, health professionals with more experience in the service should transfer their practice skills to others. As this research has been conducted in the health facilities, further research is indicated within the community (preferably in schools), using validated instruments.28–30
Ethical Approval
Ethical clearance was obtained from Addis Ababa University School of Nursing and Midwifery ethical review committee. Informed consent was taken from each participant. This study was conducted in accordance with the Declaration of Helsinki.
Acknowledgments
Our special thanks goes to Addis Ababa University, College of Health Science, School of Nursing and Midwifery, for the provision of technical and financial support. We would also like to thank the academic and clinical experts for their important comments and suggestions on the validation of the research questionnaire. Our genuine gratitude also goes to the respective hospital staff and administrators for their cooperation in providing necessary information and support. Our deepest gratitude goes to data collectors, supervisors, and study participants for their willingness and cooperation in completing this study by devoting their time. Our heartfelt gratitude also goes to Mr Yohanes Gebregzabiher (PhD fellow) and Mr Tefera Mulugeta for their constructive comments during the data analysis section of the thesis development. All authors have a patent for this original research. As stated in the Ethical Approval section, the findings of this study were presented and submitted to Addis Ababa University, College of Health Sciences as a postgraduate thesis, and the whole thesis file is available online in Addis Ababa University (AAU) institutional repository (URL: http://etd.aau.edu.et/handle/123456789/14289).
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
Addis Ababa University.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Moodie S, Daneri P, Goldhagen S, Halle T, Green K, LaMonte L. Early Childhood Developmental Screening: A Compendium of Measures for Children Ages Birth to Five. OPRE Report 2014-2011. US Department of Health and Human Services; 2014.
2. Olusanya BO. Priorities for early childhood development in low-income countries. J Develop Behav Ped. 2011;32(6):476–481. doi:10.1097/DBP.0b013e318221b8c5
3. Radecki L, Sand-Loud N, O’Connor KG, Sharp S, Olson LM. Trends in the use of standardized tools for developmental screening in early childhood: 2002–2009. Pediatrics. 2011;128(1):14–19. doi:10.1542/peds.2010-2180
4. Reichert A, Collet N, Eickmann SH, Lima M. Child development surveillance: intervention study with nurses of the Family Health Strategy. Revistalatino Americana de Enfermagem. 2015;23(5):954–962. doi:10.1590/0104-1169.0272.2636
5. Pem D. Factors affecting early childhood growth and development: golden 1000 days”. Adv Practice Nurs. 2015;1:101.
6. Oberklaid F, Wake M, Harris C, Hesketh K, Wright M. Child Health Screening and Surveillance: A Critical Review of the Evidence. Canberra: National Health and Medical Research Council; 2002. Available from: http://wwwnhmrcgovau/guidelines/publications/ch42.
7. Browning T-M. The Common Assessment Framework for Supporting Families: An Educational Perspective. University of Birmingham; 2014.
8. Accardo PJ, Whitman BY, Behr SK. Dictionary of Developmental Disabilities Terminology. Paul H Brookes Publishing Company; 2002.
9. Blair M, Hall D. From health surveillance to health promotion: the changing focus in preventive children’s services. Arch Dis Child. 2006;91(9):730–735. doi:10.1136/adc.2004.065003
10. Grantham-McGregor S, Cheung YB, Cueto S, Glewwe P, Richter L, Strupp B; International Child Development Steering Group. Developmental potential in the first 5 years for children in developing countries. The Lancet. 2007;369(9555):60–70. doi:10.1016/S0140-6736(07)60032-4
11. World Health Organization. Developmental Difficulties in Early Childhood: Prevention Early Identification Assessment and Intervention in Low-And Middle-Income Countries: A Review. World Health Organization; 2012.
12. Boyle CA, Boulet S, Schieve LA, et al. Trends in the prevalence of developmental disabilities in US children, 1997–2008. Pediatrics. 2011;127(6):1034–1042. doi:10.1542/peds.2010-2989
13. Ayele M. Developmental Delays Among Infants and Young Children in Addis Ababa: Screening, Risk Factors and Intervention. 2014.
14. Oberklaid F, Efron D. Developmental delay: identification and management. Aust Fam Physician. 2005;34(9):
15. Council on Children With Disabilities; Section on Developmental Behavioral Pediatrics; Bright Futures Steering Committee; Medical Home Initiatives for Children With Special Needs Project Advisory Committee. Identifying infants and young children with developmental disorders in the medical home: an algorithm for developmental surveillance and screening. Pediatrics. 2006;118(1):405–420. doi:10.1542/peds.2006-1231
16. Monteiro AI, Macedo I, Santos A, Araújo W. Nursing and the collective action: accompanying child growth and development. Northeast Net Nurs J. 2011;12:1.
17. Murray KE, Barnes AJ, Ireland M, Kohen DP. Emotional-Behavioral Screening by Primary Care Practitioners: Attitudes, Practices, and Barriers.
18. Engle PL, Fernald LC, Alderman H, et al. Strategies for reducing inequalities and improving developmental outcomes for young children in low-income and middle-income countries. The Lancet. 2011;378(9799):1339–1353. doi:10.1016/S0140-6736(11)60889-1
19. Poon JK, Larosa AC, Pai GS. Developmental delay: timely identification and assessment. Indian Pediatr. 2010;47(5):415–422. doi:10.1007/s13312-010-0077-3
20. Haymond M, Kappelgaard A-M, Czernichow P, Biller BM, Takano K, Kiess W. Early recognition of growth abnormalities permitting early intervention. Acta Paediatrica. 2013;102(8):787–796. doi:10.1111/apa.12266
21. Mukherjee SB, Aneja S, Krishnamurthy V, Srinivasan R. Incorporating developmental screening and surveillance of young children in office practice. Indian Pediatr. 2014;51(8):627–635. doi:10.1007/s13312-014-0465-1
22. Scherzer AL, Chhagan M, Kauchali S, Susser E. Global perspective on early diagnosis and intervention for children with developmental delays and disabilities. Dev Med Child Neurol. 2012;54(12):1079–1084. doi:10.1111/j.1469-8749.2012.04348.x
23. Caminha M, Silva S, Lima M, Azevedo PTÁCC, Figueira M, Batista Filho M. Surveillance of child development: an analysis of Brazil’s situation. Rev Paul Pediatr. 2017;35:102–109.
24. Sheldrick RC, Merchant S, Perrin EC. Identification of developmental-behavioral problems in primary care: a systematic review. Pediatrics. 2011;128(2):356–363. doi:10.1542/peds.2010-3261
25. Pediatrics A. Council on children with disabilities, section on developmental behavioral pediatrics, bright futures steering committee, medical home initiatives for children with special needs project advisory committee. Identifying infants and young children with developmental disorders in the medical home: an algorithm for developmental surveillance and screening. Pediatrics. 2006;118(1):405–420.
25. Morelli DL, Pati S, Butler A, et al. Challenges to implementation of developmental screening in urban primary care: a mixed methods study. BMC Pediatr. 2014;14(1):16. doi:10.1186/1471-2431-14-16
26. Iyanuoluwa O-BA, Esther A-O-O, Adeleye AA. Primary health care workers’ role in monitoring children’s growth and development in Nigeria, West Africa. Glob J Health Sci. 2011;3(1):30. doi:10.5539/gjhs.v3n1p30
27. Smith S, Reji E. Doctors’ attitudes to and knowledge and usage of growth charts. South African Family Pract. 2015;57(3):219–222. doi:10.1080/20786190.2014.976978
28. Honrubia-Montesinos C, Gil-Madrona P, Losada-Puente L. Motor development among spanish preschool children. Children. 2021;8:41. doi:10.3390/children8010041
29. Romero Martínez SJ, Ordóñez Camacho XG, Gil Madrona P. Development of the checklist of psychomotor activities for 5- to 6-year-old children. Percept Mot Skills. 2018;125(6):1070–1092. doi:10.1177/0031512518804359
30. Gil Madrona P, Romero Martínez SJ, Sáez-Gallego NM, Ordóñez Camacho XG. Psychomotor Limitations of overweight and obese five-year-old children: influence of body mass indices on motor, perceptual, and social-emotional skills. Int J Environ Res Public Health. 2019;16:427. doi:10.3390/ijerph16030427
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.