Back to Journals » Degenerative Neurological and Neuromuscular Disease » Volume 13
Practical Guidance on the Use of Cladribine Tablets in the Management or Relapsing Multiple Sclerosis: Expert Opinion from Qatar
Authors Deleu D, Garcia Canibano B, Elalamy O, Sayed Abdelmoneim M ![]() , Boshra A
, Boshra A
Received 1 August 2023
Accepted for publication 2 November 2023
Published 13 December 2023 Volume 2023:13 Pages 81—88
DOI https://doi.org/10.2147/DNND.S433459
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Thomas Müller
Dirk Deleu,1,* Beatriz Garcia Canibano,1,* Osama Elalamy,1,* Mohamed Sayed Abdelmoneim,1,* Amir Boshra2,*
1Department of Neurology (Neurosciences Institute), Hamad Medical Corporation, Doha, Qatar; 2Merck Serono Middle East FZ-Ltd., Dubai, UAE, an affiliate of Merck KGaA, Dubai, United Arab Emirates
*These authors contributed equally to this work
Correspondence: Dirk Deleu, Department of Neurology (Neuroscience Institute), Hamad Medical Corporation, PO Box 3050, Doha, Qatar, Email [email protected]
Abstract: The increasing availability of high-efficacy disease-modifying therapies (DMT) for the management of relapsing multiple sclerosis (RMS) has increased the potential for individualised patient management but has added complexity to the design of treatment regimens. The long-term application of immune reconstitution therapy (IRT) is supported by an increasing database of real world studies that have added important information on the long-term safety and efficacy of this approach. Cladribine tablets (CladT) is an IRT given as two annual short courses of treatment, following which a majority of patients then demonstrate no significant MS disease activity over a period of years. Whether, and how, to treat patients beyond the first two years of treatment remains a matter for debate, as clinical evidence accumulates. We, a group of neurologists who manage people with RMS in Qatar, provide our expert consensus recommendations on the application and long-term management of CladT therapy based on our experience with treatment in the last 5 years. These include pragmatic recommendations for people with MS disease activity in years 3 and 4 (ie up to four years following first dose of CladT), and for people with or without MS disease activity in subsequent years. We believe our recommendations will help to ensure the optimal application of CladT-based IRT, with the potential benefit for the patient of achieving prolonged periods free of both MS disease symptoms and the burden of regular applications of immunosuppressive DMT.
Keywords: multiple sclerosis, disease-modifying therapy, cladribine tablets, Qatar
Introduction
The management of relapsing multiple sclerosis (RMS) has been transformed in recent years by the introduction of a number of new, high-efficacy disease-modifying treatments (DMTs).1 Some of these are given continuously to suppress aspects of immune function (including natalizumab, ocrelizumab, and S1P inhibitors).2 Alternatively, immune reconstitution therapies (IRTs, currently represented by cladribine tablets [CladT] and alemtuzumab) are given as two short pulsed courses of treatment one year apart.2,3 There is no requirement for regular treatment between these courses, nor for further treatment for years afterwards in patients without further MS relapse activity.2,3
Each of the high-efficacy DMTs have distinct efficacy, tolerability, safety and administration profiles. This has increased choice of high-efficacy DMTs has expanded the prospects for personalised care, but also introduced complexity into the design of a regimen for an individual patient with RMS.4,5 Moreover, the evidence base supporting the use of the newer agents is expanding rapidly, especially with regard to real world experience.6,7 The authors, a group of neurologists who care routinely for patients with RMS in Qatar, provided expert recommendations on the management of RMS in Qatar in 2020.8 The purpose of this article is to provide an update with recommendations specifically on the therapeutic use of CladT in people with RMS, focussed mainly on identifying the most appropriate group of patients to be considered for this treatment.
Characteristics of Multiple Sclerosis in Qatar
All patients with RMS are assessed initially at the Hamad General Hospital, the main tertiary centre for MS care in Qatar. Survey data have demonstrated a medium-to-high prevalence of MS in Qatar, with an over representation of females that is typical of most countries (Box 1).9 The average level of disability was relatively low at diagnosis of MS, with a median Kurtzke Expanded Disability Status Scale (EDSS) value of 2, indicating minimal impairment of a single functional system.10 Other data showed that the radiologic presentation tended to be more severe than in neighbouring countries, however. The prevalence of MS has increased by 45% in Qatari residents between 2010 and 2017.
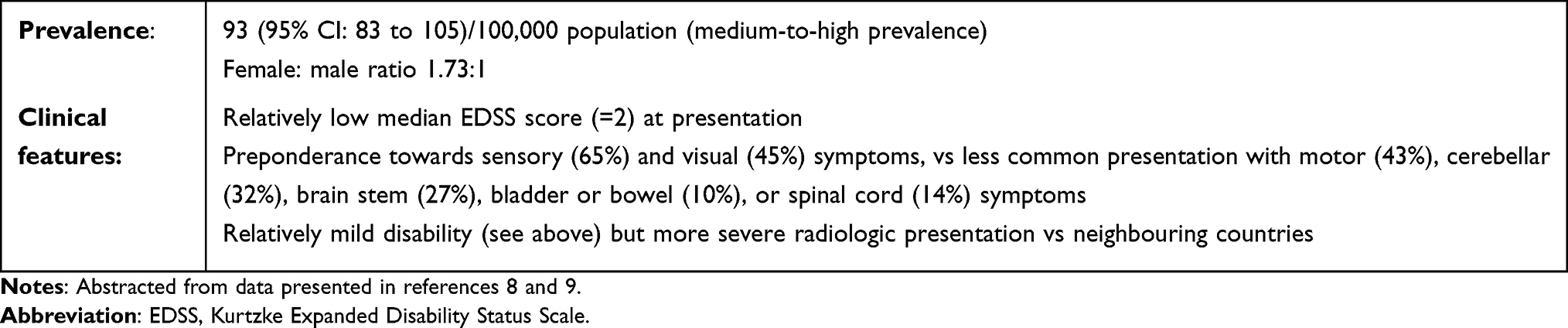 |
Box 1 Multiple Sclerosis in Qatar |
Clinical Experience with Cladribine Tablets in Qatar
Real World Data
No randomised trial has compared CladT with placebo and/or another DMT in a specifically Qatari population. However, data on the effects of this agent in our population are available from retrospective real-world evidence presented recently at the 2022 meeting of The European Committee For Treatment And Research In Multiple Sclerosis.11 Forty-nine people with MS (94% had a diagnosis of RMS) received CladT, of whom 32 received both courses of CladT and were followed up for a mean of 32 months. Treatment with CladT (compared with baseline, ie before treatment) was associated with higher proportions of subjects who were relapse-free (81% vs 25%) or free of gadolinium-enhancing MRI lesions (75% vs 38%). The annual relapse rate (ARR) was reduced from 0.97 at baseline to 0.08 after treatment. Radiologic evidence of MS disease activity was observed in 8 subjects during the first year of treatment, but in only a single subject after the second course. Almost all (31/32, 97%) were free of confirmed 3-month EDSS progression at study end.
The most common all-cause adverse event (AE) in the safety population (all 49 subjects who received CladT) was Covid-19 infection (24%); all cases were mild and none required hospital care. Five subjects (1.5%) developed Grade 3 lymphocytopenia (there was no Grade 4 lymphocytopenia). Other AEs were upper respiratory tract infections (n = 3, 6%) and a single case (2%) of each of oral candidiasis, herpes zoster, and urinary tract infection. Thirty-one patients (63%) did not report any AE.
Safety of Cladribine Tablets in Qatar Vs Elsewhere
The purpose of this section is to compare our clinical experience with CladT in Qatar with experience elsewhere. However, we will not describe the efficacy and tolerability/safety profiles of CladT in detail in this article, as these have been reviewed comprehensively already in the clinical literature.12–14 Briefly, the principal side-effect associated with CladT is transient lymphocytopenia. Levels of B lymphocytes (CD19+) are reduced markedly and reach a nadir by about 6 months after each treatment course and recover slowly thereafter. T-cells (CD4+ or CD8+) are affected less than B lymphocytes, and average T-cell counts do not fall below the normal range; recovery of T-cells proceeds more slowly.
The pivotal evaluation of CladT in people with RMS occurred in the 2-year CLARITY study and its 2-year extension phase.15,16 Grade 3 lymphocytopenia (absolute lymphocyte count [ALC] 200–500 mm−3) was a relatively common finding in that study (24.9% of patients, and 0.7% developed Grade 4 lymphocytopenia [<200 mm−3]). The much lower incidence of Grade 3 (and absence of Grade 4) lymphocytopenia in our study is probably due to a change in the posology of CladT following the CLARITY study. A rigid schedule of administration of CladT was employed in CLARITY, such that lymphocytes had not recovered in some patients by the time of the year 2 treatment course. The labelling for CladT was changed, based on that experience, so that a further 6 months can be allowed for lymphocytes to recover before giving the second course.17 This is the practice that we follow in Qatar, and the updated approach appears to be effective in reducing the risk of higher-grade lymphocytopenia.12
The other relatively common safety/tolerability issue with CladT is the emergence of opportunistic infections.12 The sporadic appearance of herpes zoster and oral candidiasis is typical of this, and can be minimised by appropriate screening for latent infections and vaccinating where required.2 Overall, no new or noteworthy safety concerns emerged from our real-world study, compared with published evidence.
Head-to-head clinical trials comparing high-efficacy DMTs are lacking, although most meta-analysis have suggested that the efficacy of Clad T is broadly comparable with that of other high-efficacy DMTs in terms of suppressing relapses, limiting disability progression or promoting the state of “no evidence of disease activity”.13,18–22 Moreover, CladT seems to be more effective in reducing relapse rates patients with higher vs lower disease activity.18,23 Figure 1 shows our expert opinion on the safety and efficacy of CladT and other DMTs used in the management of RMS.
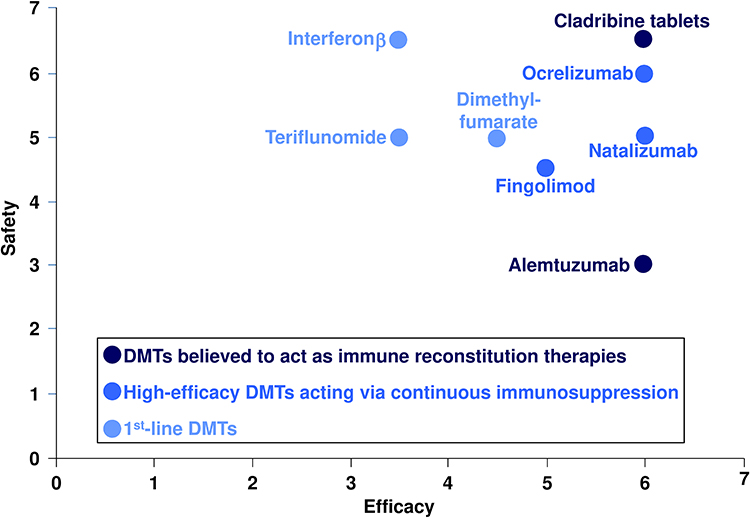 |
Figure 1 Consensus ratings of the efficacy and safety of disease-modifying therapies (DMTs) used in the management of relapsing multiple sclerosis. Expert neurologists (the authors) rated safety and efficacy on a Likert scale of 1 (least favourable) to 7 (most favourable). Average ratings are shown here. |
Recommendations on the Role of Cladribine Tablets in the Management of RMS in Qatar
Table 1 summarises our recommendations for the management of MS, and these are also discussed briefly below.
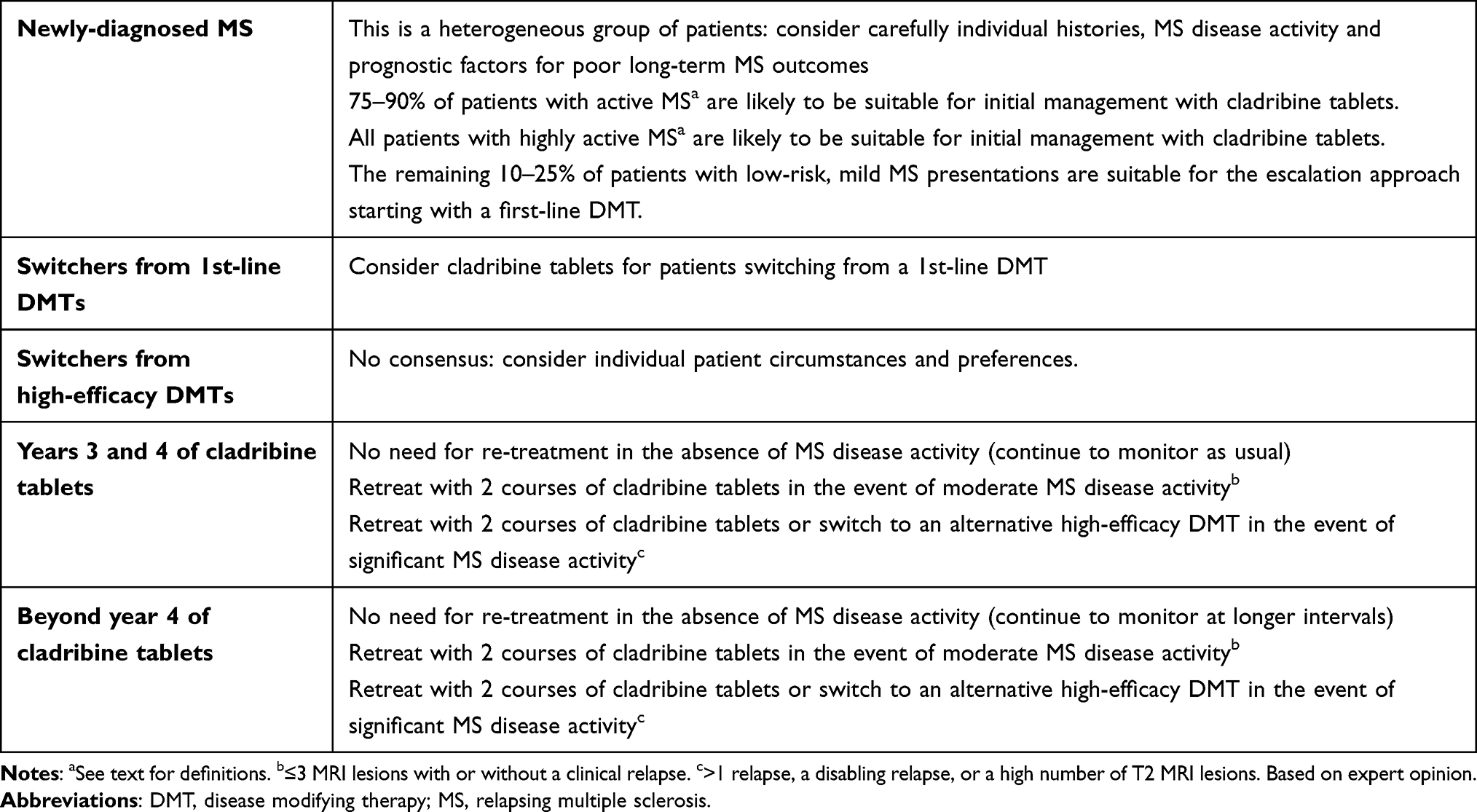 |
Table 1 Summary of Recommendations |
Newly-Diagnosed Patients with Relapsing Multiple Sclerosis
The term, “newly-diagnosed” with RMS, should be used with caution when considering a new therapeutic regimen: this population is likely to contain people with mild MS disease activity for some time before a formal diagnosis, and also people who have presented for diagnosis with significant MS disease activity. Accordingly, a personalised approach is indispensable here, considering the patient’s history and whether there are risk factors for MS disease progression, such as older age, spinal, infratentorial or cortical lesions, oligoclonal bands, frequent early relapses, early progression of disability, and lesions affecting motor function, among others.24–28
We suggest that the level of MS disease activity is more useful for identifying patients who need earlier intervention with a high-efficacy DMT such as CladT. US29 and European17 labelling for CladT and other high-efficacy DMTs employs terms such as “active” and “highly active” MS. These are not defined, however, and a recent consensus statement from the Gulf that included senior neurologists from Qatar among its authorship discusses this issue and provides recommendations.30 Briefly, according to this classification, patients with “active MS” are those with one relapse in the last year, or two relapses in the last 2 years, but do not have poor prognostic indicators; those with “highly active” MS are those with at least two relapses in the previous year and more than nine T2 lesions, or more than one gadolinium-enhancing lesion without an impact on EDSS. A further category of “rapidly evolving severe RMS” have had at least two disabling relapses, with residual disability, or with MRI lesions in strategic prognostic areas (spinal cord, cerebellum, brain stem), or poor prognostic factors. Here, for conciseness, we consider the category of “highly active MS” to encompass the latter two groups.
The use of high-efficacy DMTs from diagnosis of MS (the “induction therapy” approach) remains controversial, despite accumulating evidence of superior long-term outcomes compared with the initial use of first-line DMTs (interferons, teriflunomide, dimethyl fumarate, glatiramer acetate where available) followed by escalation to high-efficacy DMTs when this approach proves insufficiently effective.1,31–36 We support the early intensive therapy approach: in our experience, prescription of CladT as the initial DMT after diagnosis of MS is suitable for 75–90% of patients with active MS and all patients with highly active MS.
It should be noted that patient preferences play an important role in the decision to start with treatment a high efficacy DMT. For example, people with MS tend to fear disability above all and are often likely to trade off perceived risks of a high-efficacy DMT for the prospect of improved long-term outcomes.37,38
Treatment Switches
The results of scoring of perceptions of attributes of the therapeutic profile of CladT are shown in Table 2. There was strong support for early use of CladT in DMT-naïve patients, where suitable, as described above. Support was especially strong for use of this agent in patients with breakthrough MS disease activity on 1st-line DMTs. There was no consensus on the use of CladT for patients requiring a switch from other high-efficacy DMTs, consistent with observations that the efficacy of CladT and other high-efficacy DMTs is comparable.20,39 Patient preferences will be again important here, as some patients may prefer the potential of the IRT approach to deliver years free of active treatment for responders to therapy (see below).2
 |
Table 2 Factors Influencing the Suitability of Cladribine Tablets for Different Subgroups of Patients with Relapsing MS |
There was also strong agreement that CladT effectively suppresses clinical and radiologic MRI activity, with a good tolerability profile.12
Long-Term Use of Cladribine Tablets
The CLARITY study and its extension demonstrated that two annual courses of CladT provided durable efficacy throughout the following two years. However, there is no definitive evidence base at this time to guide the management of patients with breakthrough MS disease activity during years 3 or 4 of CladT therapy, or for management beyond 4 years.
It is important that all patients are monitored carefully after treatment with CladT as part of their usual care, including annual MRI scans and periodic measurement of the EDSS, according to local practice. We see no need to re-treat a patient without evidence of MS disease activity during years 3 and 4, as per the label. There was strong support for re-treatment with CladT during this period in response to moderate MS disease activity (eg ≤3 MRI lesions with or without a clinical relapse). This is broadly consistent with expert consensus recommendations from southeast Europe which called for retreatment with CladT in years 3, 4 and beyond in the case of “minimal” MS disease activity, defined as 1–2 new lesions without clinical relapse, or “moderate” MS disease activity, defined as a single relapse with 3–4 MRI new lesions.40 An international expert panel did not achieve a consensus of treatment of a patient with new MS disease activity in years 3 and 4, but supported an individualized choice between retreatment with CLadT or a switch to another high-efficacy DMT beyond year 4.41 It is less clear how to proceed in the face of more serious MS disease activity (eg >1 relapse, a disabling relapse, or a high number of T2 MRI lesions), and clinical judgement is required.40–42 For example, recent expert opinion from Germany on the management of CladT-treated patients beyond year 4 considered that either retreatment with CladT or a switch to another high-efficacy DMT is indicated in the presence of recurrence of MS disease activity, with the decision based on consideration of the time since the last treatment with CladT, the severity of the relapse(s), trends in the level of MS disease activity over time, and the frequency, nature and location within the CNS of new MRI activity.42 Taken together, these clinical findings can be used to assess whether the patient may benefit from retreatment with CladT or is a non-responder to this treatment.
Recommendations for managing patients treated with CladT beyond year 4 were similar. Patients without MS disease activity at this time can be followed up at longer monitoring intervals (eg 6-monthly clinic visits with 2-yearly MRI scans).
Conclusions
The potential benefits of successful prescription of an IRT are substantial in that responders to treatment do not require active treatment following the completion of the second annual course of treatment. Thus, patients who presented with high MS disease activity may be free of the twin burdens of MS-related symptoms and of the need for regular intakes of immunosuppressive DMTs for a period of years.43–49 Most high-efficacy DMTs are contraindicated in pregnancy, so that such a situation can be of particular benefit for patients who wish to pursue a pregnancy (as long as the 6-month washout period following the last dose of CladT is respected, as per the product label).2,17,50–52, Patients who adhere poorly to a regular regimen, a common issue in the management of RMS, may also benefit from the IRT approach.2,17,50,51,53 Finally, the monitoring burden associated with CladT is relatively light, compared with other (especially infusional) DMTs, which suggests greater convenience and a lower impact on clinic time and patients’ usual activities, compared with some other high-efficacy DMTs.2
The recommendations summarized above are intended to support the practising physician in the application of CladT-based therapy, especially beyond the first 2 years of treatment, at which time the product label provides little or no support. Further revisions to these recommendations will be needed in future as the evidence base for the long-term use of CladT grows. Our recommendations and others40–42 emphasize the need for clinical judgment when faced with a patient with recurrent MS disease activity more than 2 years after the first course of CladT. The accrual of longer-term data on the therapeutic profile of CladT over time will help to answer important clinical questions, including which demographic and/or phenotypic subgroups of patients respond best to retreatment with CLadT beyond years 3 and 4, and what level of clinical or radiologic MS disease activity recurrence supports or precludes successful retreatment.
Acknowledgments
Dr Mike Gwilt (GT Communications) provided editorial assistance, funded by Merck Serono Middle East FZ-Ltd, Dubai, UAE, an affiliate of Merck KGaA.
Funding
The consensus meeting that gave rise to this article was funded by Merck Serono Middle East FZ-Ltd, Dubai, UAE, an affiliate of Merck KGaA (CrossRef Funder ID: 10.13039/100009945). This company did not influence the treatment recommendations made here, which are the views of the authors. Merck Serono Middle East FZ-Ltd, Dubai, UAE, an affiliate of Merck KGaA, also funded editorial assistance (see above). No other funding applied.
Disclosure
DD has served on Advisory Boards of Merck, Novartis, Biologix, Roche and Sanofi and is a member of MENACTRIMS. BC has received travel, speaker and consultant honoraria from Merck, Novartis, Biologix, Roche and Sanofi. OE received an honorarium from Merck. MSA reported no duality of interest additional to participation in the consensus meeting funded by Merck Serono Middle East FZ-Ltd, Dubai, UAE, an affiliate of Merck KGaA described in the “Funding” section. AB is an employee of Merck Serono Middle East FZ-Ltd, Dubai, UAE, an affiliate of Merck KGaA. The authors report no other conflicts of interest in this work.
References
1. Freeman L, Longbrake EE, Coyle PK, Hendin B, Vollmer T. High-efficacy therapies for treatment-naïve individuals with relapsing-remitting multiple sclerosis. CNS Drugs. 2022;36(12):1285–1299. doi:10.1007/s40263-022-00965-7
2. AlSharoqi IA, Aljumah M, Bohlega S, et al. Immune reconstitution therapy or continuous immunosuppression for the management of active relapsing-remitting multiple sclerosis patients? A narrative review. Neurol Ther. 2020;9(1):55–66. doi:10.1007/s40120-020-00187-3
3. Sorensen PS, Sellebjerg F. Pulsed immune reconstitution therapy in multiple sclerosis. Ther Adv Neurol Disord. 2019;12:1756286419836913. doi:10.1177/1756286419836913
4. Giovannoni G. Personalized medicine in multiple sclerosis. Neurodegener Dis Manag. 2017;7(6s):13–17. doi:10.2217/nmt-2017-0035
5. Yamout B, Sahraian M, Bohlega S, et al. Consensus recommendations for the diagnosis and treatment of multiple sclerosis: 2019 revisions to the MENACTRIMS guidelines. Mult Scler Relat Disord. 2020;37:101459. doi:10.1016/j.msard.2019.101459
6. Caffrey M Bringing real-world data to multiple sclerosis treatment decisions. Conference report. Am J Manag Care September; 2019. Available from: https://www.ajmc.com/view/bringing-realworld-data-to-multiple-sclerosis-treatment-decisions.
7. Fox RJ, Mehta R, Pham T, Park J, Wilson K, Bonafede M. Real-world disease-modifying therapy pathways from administrative claims data in patients with multiple sclerosis. BMC Neurol. 2022;22(1):211. doi:10.1186/s12883-022-02738-7
8. Deleu D, Canibaño B, Mesraoua B, et al. Management of relapsing-remitting multiple sclerosis in Qatar: an expert consensus. Curr Med Res Opin. 2020;36(2):251–260. doi:10.1080/03007995.2019.1669378
9. Ibrahim F, Canibano B, Deleu D. Increasing prevalence of multiple sclerosis in Qatar: 27-year data. Mult Scler J. 2020;26(S3):1.
10. Kishner S, Weilenman ZN. Kurtzke expanded disability status scale. Medscape drugs and diseases; 2023. Available from: https://emedicine.medscape.com/article/2172461.
11. Garcia-Cañibano B, Zamrath Zahir F, Safan A, Ibrahim F, Deleu D. Two years efficacy and safety results from real world experience for cladribine tablets in management of relapsing multiple sclerosis in Qatar. Mult Scler J. 2022;28(Issue 3_Suppl):391.
12. Clavelou P, Giovanni Castelnovo G, Valérie Pourcher V, et al. Expert narrative review of the safety of cladribine tablets for the management of relapsing multiple sclerosis. Neurol Ther. 2023;12(5):1457–1476. doi:10.1007/s40120-023-00496-3)
13. Nabizadeh F, Mohamadi M, Rahmani S, et al. Safety and efficacy of cladribine in multiple sclerosis: a systematic review and meta-analysis. Neurol Sci. 2023;2023:1–13.
14. Leist T, Cook S, Comi G, et al. Long-term safety data from the cladribine tablets clinical development program in multiple sclerosis. Mult Scler Relat Disord. 2020;46:102572. doi:10.1016/j.msard.2020.102572
15. Giovannoni G, Comi G, Cook S, et al. A placebo-controlled trial of oral cladribine for relapsing multiple sclerosis. N Engl J Med. 2010;362(5):416–426. doi:10.1056/NEJMoa0902533
16. Giovannoni G, Soelberg Sorensen P, Cook S, et al. Safety and efficacy of cladribine tablets in patients with relapsing-remitting multiple sclerosis: results from the randomized extension trial of the CLARITY study. Mult Scler. 2018;24(12):1594–1604. doi:10.1177/1352458517727603
17. European Medicines Agency. Mavenclad, INN-cladribine. Available from: https://www.ema.europa.eu/en/documents/product-information/mavenclad-epar-product-information_en.pdf.
18. Signori A, Saccà F, Lanzillo R, et al. Cladribine vs other drugs in MS: merging randomized trial with real-life data. Neurol Neuroimmunol Neuroinflamm. 2020;7(6):e878. doi:10.1212/NXI.0000000000000878
19. Bartosik-Psujek H, Kaczyński Ł, Górecka M, et al. Cladribine tablets versus other disease-modifying oral drugs in achieving no evidence of disease activity (NEDA) in multiple sclerosis-A systematic review and network meta-analysis. Mult Scler Relat Disord. 2021;49:102769. doi:10.1016/j.msard.2021.102769
20. Siddiqui MK, Khurana IS, Budhia S, Hettle R, Harty G, Wong SL. Systematic literature review and network meta-analysis of cladribine tablets versus alternative disease-modifying treatments for relapsing-remitting multiple sclerosis. Curr Med Res Opin. 2018;34(8):1361–1371. doi:10.1080/03007995.2017.1407303
21. Piasecka-Stryczyńska K, Kaczyński Ł, Rolka M, et al. Systematic review and network meta-analysis (NMA) for cladribine tablets in achieving sustained disability improvement (SDI) in multiple sclerosis. Neurol Neurochir Pol. 2022;56(6):480–489. doi:10.5603/PJNNS.a2022.0068
22. Śladowska K, Kawalec P, Holko P, Osiecka O. Comparative safety of high-efficacy disease-modifying therapies in relapsing-remitting multiple sclerosis: a systematic review and network meta-analysis. Neurol Sci. 2022;43(9):5479–5500. doi:10.1007/s10072-022-06197-3
23. Giovannoni G, Soelberg Sorensen P, Cook S, et al. Efficacy of Cladribine Tablets in high disease activity subgroups of patients with relapsing multiple sclerosis: a post hoc analysis of the CLARITY study. Mult Scler. 2019;25(6):819–827. doi:10.1177/1352458518771875
24. Scalfari A, Romualdi C, Nicholas RS, et al. The cortical damage, early relapses, and onset of the progressive phase in multiple sclerosis. Neurology. 2018;90(24):e2107–e2118. doi:10.1212/WNL.0000000000005685
25. Engel S, Zipp F. Preventing disease progression in multiple sclerosis-insights from large real-world cohorts. Genome Med. 2022;14(1):41. doi:10.1186/s13073-022-01044-8
26. Fambiatos A, Jokubaitis V, Horakova D, et al. Risk of secondary progressive multiple sclerosis: a longitudinal study. Mult Scler. 2020;26(1):79–90. doi:10.1177/1352458519868990
27. Espiritu A, Oh J Prognostic factors in multiple sclerosis. Prediction of highly active disease and rapid disability accumulation is crucial to optimizing clinical outcomes over time. Practical Neurol 2022;February:44–48. Available from: https://practicalneurology.com/articles/2022-feb/prognostic-factors-in-multiple-sclerosis.
28. Lebrun-Frénay C, Rollot F, Mondot L, et al. Risk factors and time to clinical symptoms of multiple sclerosis among patients with radiologically isolated syndrome. JAMA Netw Open. 2021; 4:e2128271.
29. Food and Drug Administration. Mavenclad - Accessdata.fda.gov. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/022561s000lbl.pdf.
30. Alroughani R, Inshasi J, Al-Asmi A, et al. Expert consensus from the Arabian Gulf on selecting disease-modifying treatment for people with multiple sclerosis according to disease activity. Postgrad Med. 2020;132(4):368–376. doi:10.1080/00325481.2020.1734394
31. Filippi M, Amato MP, Centonze D, et al. Early use of high-efficacy disease‑modifying therapies makes the difference in people with multiple sclerosis: an expert opinion. J Neurol. 2022;269(10):5382–5394. doi:10.1007/s00415-022-11193-w
32. Casanova B, Quintanilla-Bordás C, Gascón F. Escalation vs. Early intense therapy in multiple sclerosis. J Pers Med. 2022;12(1):119. doi:10.3390/jpm12010119
33. Stankiewicz JM, Weiner HL. An argument for broad use of high efficacy treatments in early multiple sclerosis. Neurol Neuroimmunol Neuroinflamm. 2019;7(1):e636. doi:10.1212/NXI.0000000000000636
34. Prosperini L, Mancinelli CR, Solaro CM, et al. Induction versus escalation in multiple sclerosis: a 10-year real world study. Neurotherapeutics. 2020;17(3):994–1004. doi:10.1007/s13311-020-00847-0
35. Iaffaldano P, Lucisano G, Caputo F, et al. Long-term disability trajectories in relapsing multiple sclerosis patients treated with early intensive or escalation treatment strategies. Ther Adv Neurol Disord. 2021;14:17562864211019574. doi:10.1177/17562864211019574
36. Spelman T, Magyari M, Piehl F, et al. Treatment escalation vs immediate initiation of highly effective treatment for patients with relapsing-remitting multiple sclerosis: data from 2 different national strategies. JAMA Neurol. 2021;78(10):1197–1204. doi:10.1001/jamaneurol.2021.2738
37. Wilson LS, Loucks A, Gipson G, et al. Patient preferences for attributes of multiple sclerosis disease-modifying therapies: development and results of a ratings-based conjoint analysis. Int J MS Care. 2015;17(2):74–82. doi:10.7224/1537-2073.2013-053
38. Garcia-Dominguez JM, Muñoz D, Comellas M, Gonzalbo I, Lizán L, Polanco Sánchez C. Patient preferences for treatment of multiple sclerosis with disease-modifying therapies: a discrete choice experiment. Patient Prefer Adherence. 2016;10:1945–1956. doi:10.2147/PPA.S114619
39. Berardi A, Siddiqui MK, Treharne C, Harty G, Wong SL. Estimating the comparative efficacy of cladribine tablets versus alternative disease modifying treatments in active relapsing-remitting multiple sclerosis: adjusting for patient characteristics using meta-regression and matching-adjusted indirect treatment comparison approaches. Curr Med Res Opin. 2019;35(8):1371–1378. doi:10.1080/03007995.2019.1585779
40. Habek M, Drulovic J, Brecl Jakob G, et al. Treatment with cladribine tablets beyond year 4: a position statement by southeast European multiple sclerosis centers. Neurol Ther. 2023;12(1):25–37. doi:10.1007/s40120-022-00422-z
41. Sørensen PS, Centonze D, Giovannoni G, et al. Expert opinion on the use of cladribine tablets in clinical practice. Ther Adv Neurol Disord. 2020;13:1756286420935019. doi:10.1177/1756286420935019
42. Meuth SG, Bayas A, Kallmann B, et al. Long-term management of multiple sclerosis patients treated with cladribine tablets beyond year 4. Expert Opin Pharmacother. 2022;23(13):1503–1510. doi:10.1080/14656566.2022.2106783
43. Bose G, Rush C, Atkins HL, Freedman MS. A real-world single-centre analysis of alemtuzumab and cladribine for multiple sclerosis. Mult Scler Relat Disord. 2021;52:102945. doi:10.1016/j.msard.2021.102945
44. Rauma I, Viitala M, Kuusisto H, et al. Finnish multiple sclerosis patients treated with cladribine tablets: a nationwide registry study. Mult Scler Relat Disord. 2022;61:103755. doi:10.1016/j.msard.2022.103755
45. Patti F, Visconti A, Capacchione A, Roy S, Trojano M, Study Group CLARINET-MS. Long-term effectiveness in patients previously treated with cladribine tablets: a real-world analysis of the Italian multiple sclerosis registry (CLARINET-MS). Ther Adv Neurol Disord. 2020;13:1756286420922685. doi:10.1177/1756286420922685
46. Frau J, Coghe G, Lorefice L, Fenu G, Musu L, Cocco E. Efficacy and safety of alemtuzumab in a real-life cohort of patients with multiple sclerosis. J Neurol. 2019;266(6):1405–1411. doi:10.1007/s00415-019-09272-6
47. Coles AJ, Arnold DL, Bass AD, et al. Efficacy and safety of alemtuzumab over 6 years: final results of the 4-year CARE-MS extension trial. Ther Adv Neurol Disord. 2021;14:1756286420982134. doi:10.1177/1756286420982134
48. Steingo B, Al Malik Y, Bass AD, et al. Long-term efficacy and safety of alemtuzumab in patients with RRMS: 12-year follow-up of CAMMS223. J Neurol. 2020;267(11):3343–3353. doi:10.1007/s00415-020-09983-1
49. Russo CV, Saccà F, Frau J, et al. A real-world study of alemtuzumab in a cohort of Italian patients. Eur J Neurol. 2022;29(1):257–266. doi:10.1111/ene.15121
50. Alroughani R, Inshasi J, Al-Asmi A, et al. Disease-modifying drugs and family planning in people with multiple sclerosis: a consensus narrative review from the gulf region. Neurol Ther. 2020;9(12):265–280. doi:10.1007/s40120-020-00201-8
51. De Sèze J, Suchet L, Mekies C, et al. The place of immune reconstitution therapy in the management of relapsing multiple sclerosis in France: an Expert Consensus. Neurol Ther. 2023;12(2):351–369. doi:10.1007/s40120-022-00430-z
52. Dobson R, Dassan P, Roberts M, et al. UK consensus on pregnancy in multiple sclerosis: ‘Association of British Neurologists’ guidelines. Pract Neurol. 2019;19(2):106–114. doi:10.1136/practneurol-2018-002060
53. Mardan J, Hussain MA, Allan M, Grech LB. Objective medication adherence and persistence in people with multiple sclerosis: a systematic review, meta-analysis, and meta-regression. J Manag Care Spec Pharm. 2021;27(9):1273–1295. doi:10.18553/jmcp.2021.27.9.1273
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Factors Associated with Therapeutic Adherence in Multiple Sclerosis in Spain
Soria C, Prieto L, Lázaro E, Ubeda A
Patient Preference and Adherence 2023, 17:679-688
Published Date: 14 March 2023
Harmonized Data Quality Indicators Maintain Data Quality in Long-Term Safety Studies Using Multiple Sclerosis Registries/Data Sources: Experience from the CLARION Study
Hillert J, Butzkueven H, Magyari M, Wergeland S, Moore N, Soilu-Hänninen M, Ziemssen T, Kuhle J, Pontieri L, Forsberg L, Aarseth JH, Zhu C, Sicignano N, Mushnikov V, Bezemer I, Sabidó M
Clinical Epidemiology 2024, 16:717-732
Published Date: 17 October 2024
Patient Experiences with the Impacts of Multiple Sclerosis & Disease-Modifying Therapies
Talente B, Finseth LT, Blake N, Costello K, Schmidt H, Vandigo J, Oehrlein EM
ClinicoEconomics and Outcomes Research 2025, 17:199-215
Published Date: 15 March 2025