Back to Journals » Clinical Ophthalmology » Volume 20
Potential Refractive Error Due to Axial Displacement of Intraocular Lenses with Clinically Relevant Compression Diameters
Authors Maxwell A, Marotta JS, McGough M, Almir N, Valenzuela S, LaFleur A ![]() , Ong MD, Das KK, Wensrich D
, Ong MD, Das KK, Wensrich D
Received 2 April 2026
Accepted for publication 26 June 2026
Published 8 July 2026 Volume 2026:20 613894
DOI https://doi.org/10.2147/OPTH.S613894
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Bharat Gurnani
Andrew Maxwell,1,* James S Marotta,2,* Maddi McGough,2,* Neaz Almir,2,* Sandy Valenzuela,2,* Alesha LaFleur,2,* Marcia D Ong,2,* Kamal K Das,2,* Doug Wensrich2,*
1InSight Vision Center, California Eye Institute, Fresno, CA, USA; 2Research & Development, Alcon Research, LLC., Fort Worth, TX, USA
*These authors contributed equally to this work
Correspondence: James S Marotta, Email [email protected]
Purpose: To compare the mechanical stability and associated potential refractive error (RE) of 9 different intraocular lens (IOL) models using compression diameters that are aligned with published clinical mean capsular bag diameters (CBD).
Setting: Research Laboratory.
Design: Prospective, non-randomized, in vitro bench testing using physiological conditions.
Methods: Single-piece acrylic IOLs (3– 5 per model) were tested for axial displacement, optic decentration, optic tilt, and haptic compression force at both 9-mm and 10-mm compression diameters under simulated physiological conditions. Potential RE was calculated based on the mean axial displacement observed and using a schematic eye model.
Results: The three different Clareon optical models had statistically equivalent results, confirming that mechanical stability performance is not affected by the optical design. At 9-mm compression, the measured axial displacement values of the Clareon models were significantly lower than the 6 other models assessed (P < 0.05). At both diameters, the haptic compression force for Clareon was statistically lower than 5 of the other models (P < 0.05). Between the two compression diameters, there were substantial increases in axial displacement and haptic compression force for some of the IOL models. There were no statistical differences among the IOL models studied with respect to either optic decentration or optic tilt.
Conclusion: Clareon IOL models had lower levels of axial displacement, compression force and potential RE. Refractive errors may occur with those IOL models that show significant axial displacement with compression, especially in short eyes.
Keywords: refractive error, refractive outcome, axial stability, capsular diameter, axial length, laboratory bench testing
Introduction
During cataract surgery, the natural crystalline lens is removed and replaced with an intraocular lens (IOL). Each IOL has a central optical portion which provides the visual performance and mechanical support elements (also known as haptics) which provide the proper positioning and stability of the lens within the capsular bag. IOL designs may include either 2 or 4 haptics of various shapes/geometries such as open-loop, closed-loop, or plate. Haptic designs for different IOL models may also vary in thickness, width, and volume. In addition, the haptic position relative to the optic may either be planar, step-vaulted or angulated with the posterior optic edge.1 The mechanical stability of the IOL within the capsular bag can have an impact on the final effective lens position (ELP) or anterior chamber depth (ACD) of the IOL, which can determine the refractive correction. Numerous clinical studies have examined the influence of post-operative IOL movement on the refractive correction provided to the patient.2–8 IOL mechanical stability is a function of the interaction between the capsular bag with the lens haptics, resulting in potential axial displacement, rotation, decentration, and/or tilt of the lens.9–15 The International Organization for Standardization (ISO 11979–3:2012) requires that the mechanical stability (axial displacement, tilt, and decentration) of posterior chamber IOLs be evaluated prior to commercialization.16 This ISO standard requires 10-mm diameter testing; however, IOLs may be exposed to even smaller compression diameters during use.
Capsular bag diameter (CBD) varies widely among cataract patients, with a reported range of 8.5 mm to 14.0 mm at the time of surgery, with the mean published value being 10.4 mm.4,17–19 In general, the CBD is correlated with the eye axial length with long (myopic) eyes having larger diameters than short (hyperopic) eyes.4,18 In addition, as part of the early healing process after cataract surgery, the capsular bag shrink-wraps around the IOL, becoming 10% to 15% smaller in diameter.17,18,20 Clinical studies have reported 3-month postoperative mean CBD values of 9.07 ± 0.78 mm and 9.43 ± 0.39 mm after cataract surgery.17,20 Changes in the ELP (or the axial position of an IOL) during the first months of healing have been associated with post-operative refractive shifts. Wirtitsch et al in 2004 examined the postoperative changes in ACD between single-piece and multipiece IOLs, comparing those ACD shifts with changes in postoperative refractive outcomes.2 The following year, the same university was among the first to clinically correlate patient CBD with a refractive shift due to changes in ACD during the first month after surgery.4 The authors concluded that “Myopic eyes with large capsular bags showed less IOL shift in the early postoperative period than hyperopic eyes with smaller capsular bags.” More recently, surgeons in Japan (Hayashi et al and Goto et al) measured the change in Manifest Refractive Spherical Equivalent (MRSE) values during the first few months after surgery for various single-piece IOL models, and concluded that post-operative refractive stability was IOL model-dependent.5,8 It is therefore important to understand the mechanical performance of IOLs at different diameters of compression that may be encountered during their clinical application; 10-mm to represent the mean CBD at the time of surgery and 9-mm to represent the CBD which may occur months after surgery as the capsule shrink-wraps around the IOL.
Our laboratory has previously published an in vitro study comparing the mechanical stability of five different IOL models over a range of compression diameters (9.0 to 11.0 mm) and used the axial displacement measurements observed to calculate the potential dioptric power shift (D) for each lens model.1 That study found that some IOL models have significant axial displacement at diameters lower than 10-mm, representing a large potential refractive power shift with compression (especially in short eyes). The current study expands that evidence by evaluating the axial stability of additional IOL models at both 9-mm and 10-mm. As done previously, the axial displacement measurements were mathematically converted into a potential refractive error (RE) for each IOL model. The discussion section of this paper will also compare our laboratory calculated potential RE values (non-clinical) with published clinically measured refractive outcomes for those models which have published data. Other mechanical properties such as haptic compression force, optic decentration, and optic tilt were also assessed using these two compression diameters. Combined, the lenses from our previous study and this report comprise IOL models from the top 8 manufacturers and represent ~73% of global sales (based on a recent Market Scope Report).21 Some of these IOL models lack published data on their mechanical stability and/or refractive outcomes which presents a knowledge gap. Thus, understanding the mechanical stability differences across these IOL models should be relevant to cataract surgeons who might be deciding between different models.
Materials and Methods
Nine different IOL models were assessed in this study (see Table 1). Three to five samples per model were tested in Balanced Salt Solution (BSS®) at 35°C ± 2°C using previously published1 standardized methods for axial displacement, optic decentration, and optic tilt and consistent with the International Standard (ISO 11979–3, section 4.9).16 Cylindrical wells (a compression cell) with an inner diameter of either 9-mm and 10-mm (±0.04 mm) were used for all measurements. The diameter of each compression cell was verified prior to use using an optical comparator at 20X magnification equipped with a digital readout. Each IOL was carefully positioned in the compression cell, with the posterior side facing upward. The IOL was centered manually via visual inspection within the compression cell prior to measurement. Groups were measured sequentially. All measurements were conducted in a masked manner with the IOL description and expected results, thereby minimizing potential measurement bias. The initial haptic compression force was also measured. All IOLs were hydrated in BSS at 35°C for a minimum of 24 hours prior to conducting the mechanical testing. All tests were performed under identical conditions. Representative axial displacement side view images were captured using a Nikon digital camera at 20X magnification. Positive displacement values represent axial movement in the posterior direction and negative values represent movement in the anterior direction.
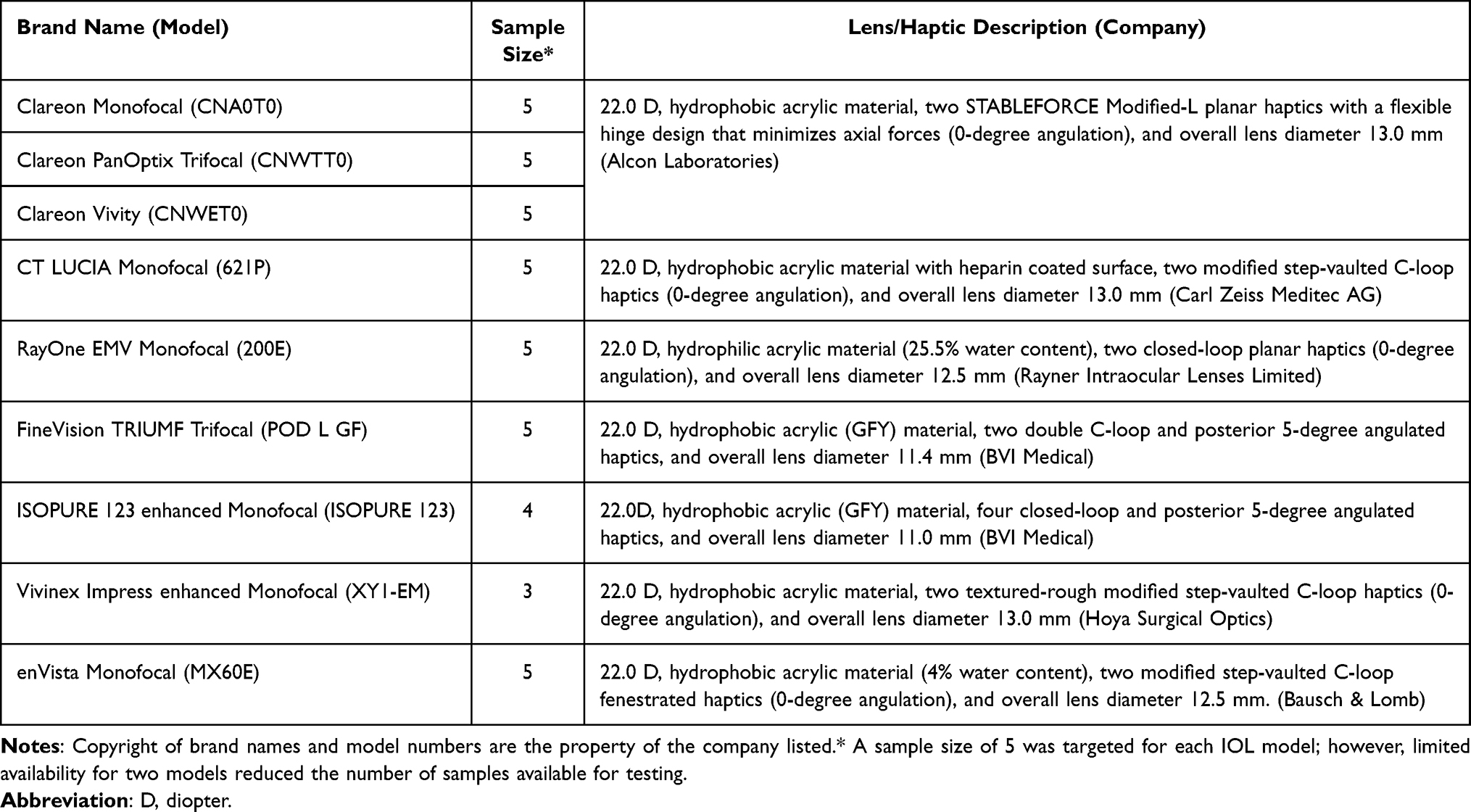 |
Table 1 Intraocular Lenses Tested |
Schematic Raytrace Based Model Eye to Calculate the Power Shift
A ray-trace-based model eye was created using Ansys Zemax OpticStudio software (Ansys, Inc) program with established clinical parameters, based on a mean corneal power of 43.877 D from previous Alcon clinical studies. The thickness of the cornea is 0.55 mm. The eye model uses a corneal refractive index of 1.376. The refractive index of aqueous and vitreous is taken as 1.336 at 550 nm. A spectacle lens was placed at a vergence distance of 12 mm from the anterior cornea. The object distance was set to 6 meters (20 ft). The model also incorporates a mean spherical aberration of 0.28 µm. Next, a 22.0 diopter (D) biconvex IOL was placed to produce an image on the retina. The through-focus Modulation Transfer Function (MTF) at 50 lp/mm and the MTF as a function of spatial frequency were obtained to optimize that the IOL formed the diffraction limited image at the retina or achieved emmetropia for a potential patient. Once the optimized image was obtained, the axial length and other eye parameters were kept unchanged with an IOL that moves axially. For any axial movement, the image would be defocused on the retina. Therefore, the posterior surface of the IOL was adjusted so that the retinal image becomes emmetropic. However, this will result in a different power than the original 22.0 D lens because of the axial displacement. The adjusted IOL power was used in the SRK/T-based formula for an average model eye to determine the potential refractive error (RE) for each lens model. Note that for higher power IOLs (like those used in shorter eyes), the same observed axial displacement would generally produce even larger RE values. Note that the potential RE values calculated in this research represent a laboratory estimate, as actual clinical refractive outcomes may be different.
Statistical Analysis and Superiority Test
Descriptive statistics of the mean ± standard deviation (SD) were calculated for each IOL group for axial displacement, optic decentration, optic tilt, and compression force at both compression diameters. One Way Analysis of Variance (ANOVA), followed by either Games-Howell (for unequal variance) test or Dunnett’s method (for equal variance) for multiple comparison procedures using MiniTab 17 Statistical Software (Minitab, Inc.) was conducted to compare the different IOL models. Variance assumptions were evaluated within the ANOVA procedure in Minitab (first Anova followed by test for equal variances). Datasets that satisfied the equal variance assumption were identified as “passed with equal variance” in the ANOVA output and analyzed using Dunnett’s method, while datasets that did not meet this assumption were labeled as “test with unequal variance” and analyzed using the Games–Howell test. Models with similar optic types were also compared. The significance level (α) was set at 0.05.
Results
Axial Displacement and Potential RE
The mean axial displacement and calculated potential RE for each model at both compression diameters are summarized in Table 2. The results at the top of Table 2 are those generated through this research, for reference we have also included the historical data from our previous publication.1 The three Clareon optical models (Monofocal, Trifocal and extended depth of focus; EDOF) had statistically equivalent axial displacement values (P > 0.05), substantiating that mechanical stability performance is not dependent on the optical design for lenses that use the same mechanical design. Detailed results of the statistical analysis are provided in Supplemental Tables 1–3. At 10-mm compression diameter, the Clareon axial displacement was statistically lower than CT LUCIA 621P, ISOPURE 123, and enVista MX60E (P < 0.05) but was not statistically different than RayOne EMV and Vivinex Impress. At the 9-mm compression diameter, Clareon axial displacement was statistically lower than CT LUCIA 621P, enVista MX60E, RayOne EMV, ISOPURE 123 and Vivinex Impress (P < 0.05). Comparing the 2 trifocal IOLs, Clareon PanOptix had significantly less axial displacement than the FineVision Trifocal at both diameters (P < 0.05). The RayOne EMV model had a substantial increase in axial displacement from 0.01 mm with 10-mm compression to 2.06 mm at 9-mm compression (absolute change +2.05 mm, ~206 fold). The three next largest increases were enVista MX60E, CT LUCIA 621P and FineVision, which had absolute changes of +1.16 mm, +0.97 mm, and +0.58 mm, respectively. The calculated potential RE for each model based on their axial displacement at both 9-mm and 10-mm compression are graphically shown in Figure 1. For both compression diameters, the calculated RE for the three Clareon models was less than 0.2 D (range of 0.02 to 0.17 D). At 10-mm compression, the calculated RE exceeded 1.6 D for four IOL models (range of 1.63 to 2.79 D). At 9-mm compression, the calculated RE exceeded 4 D for five models: CT LUCIA 621P, RayOne EMV, FineVision Trifocal, ISOPURE 123, and enVista MX60E. These RE values represent the power change that would be expected for a 22.0 D lens based on the axial movement observed. Because the calculated RE values depend on IOL power, short eyes which require higher power lenses may have a greater RE value. These findings suggest a potential mechanism for model specific refractive shifts that might occur in small capsular bags and during the early healing period after cataract surgery. These potential RE values are calculated from the axial movement observed in a laboratory setting, and actual clinical refractive outcomes may be different.
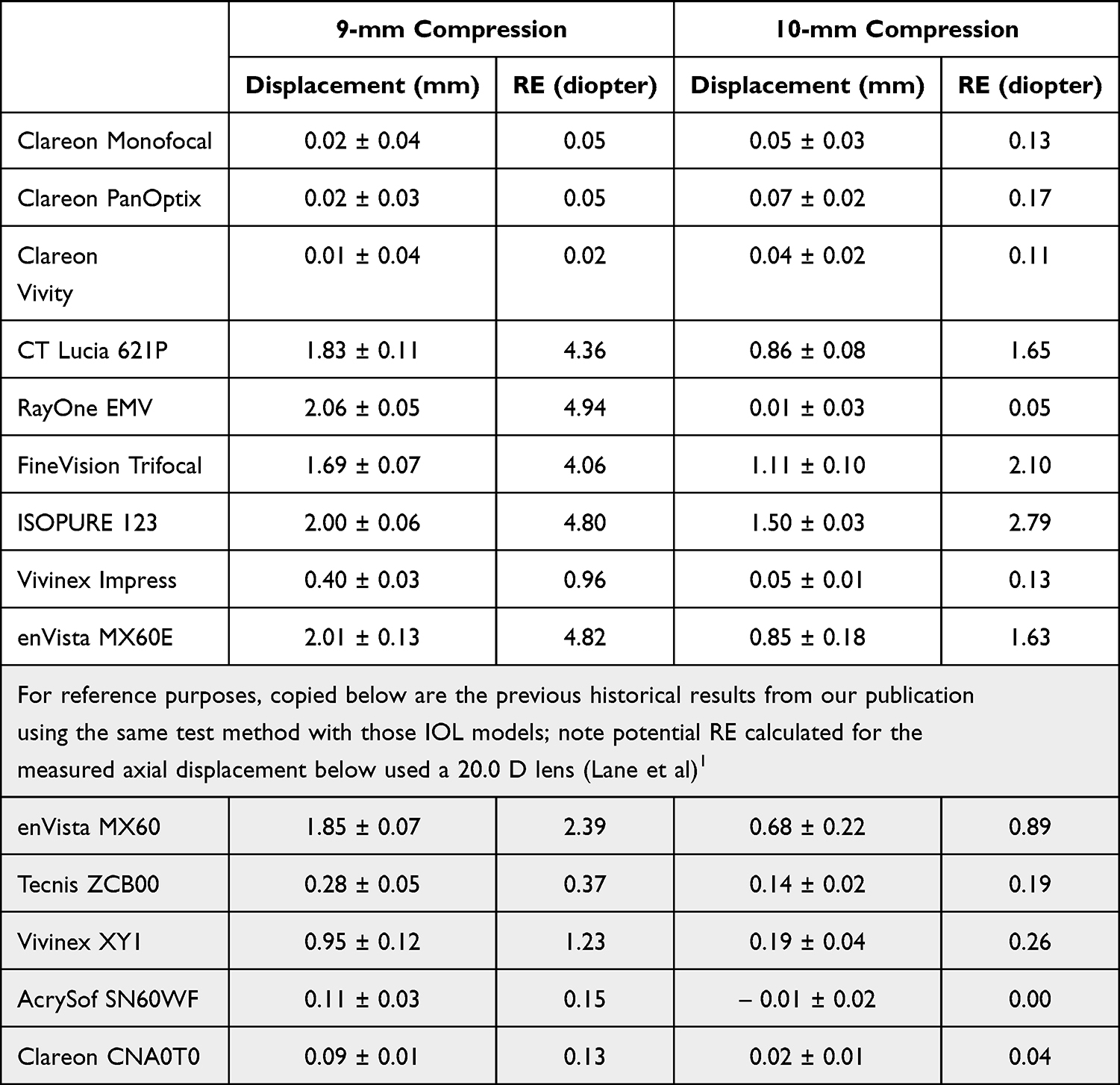 |
Table 2 Axial Displacement (Mm; Mean ± Standard Deviation) Observed and Potential Refractive Error (RE) at 9-mm and 10-mm Compression Diameter (Calculation Used a 22.0 D Lens) |
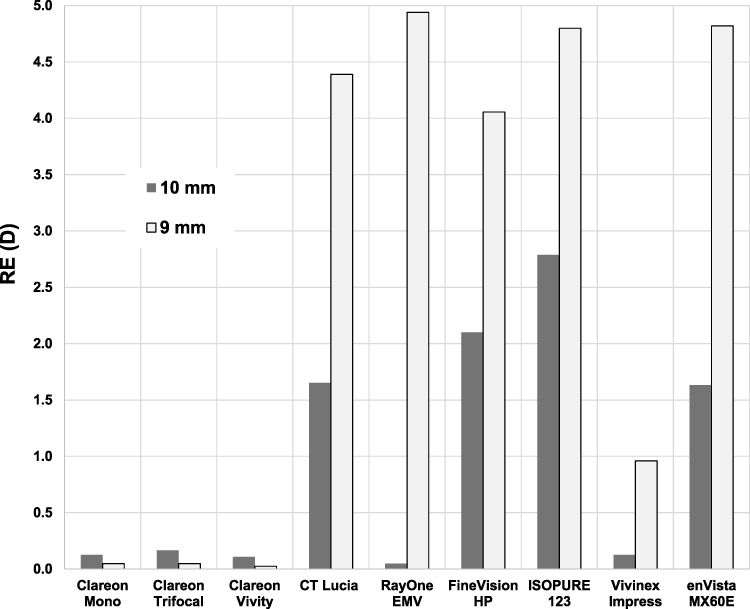 |
Figure 1 Potential Refractive Error (RE) calculated from axial displacement that was observed with 9-mm and 10-mm compression diameters. |
Haptic Compression Force
The initial haptic compression force in millinewtons (mN) results at both 9-mm and 10-mm compression diameters are summarized for each test group in Table 3. As expected, the haptic compression force increased with decreasing diameter for all IOL models. At both the 10-mm and 9-mm compression diameters the measured compression force values for the three Clareon models were statistically lower (P < 0.05) than CT LUCIA 621P, enVista MX60E, FineVision Trifocal, ISOPURE 123 and RayOne EMV. At 9-mm compression, those lenses had 3x to 30x the compression forces as compared to the Clareon models. Two IOLs showed substantial increases in haptic compression force between the two compression diameters; Vivinex Impress and RayOne EMV had force increases of 117% (0.24 mN to 0.52 mN) and 340% (2.0 mN to 8.9 mN), respectively. High compression force values may result in capsular stress or striae, especially in short eyes that tend to have smaller CBDs.
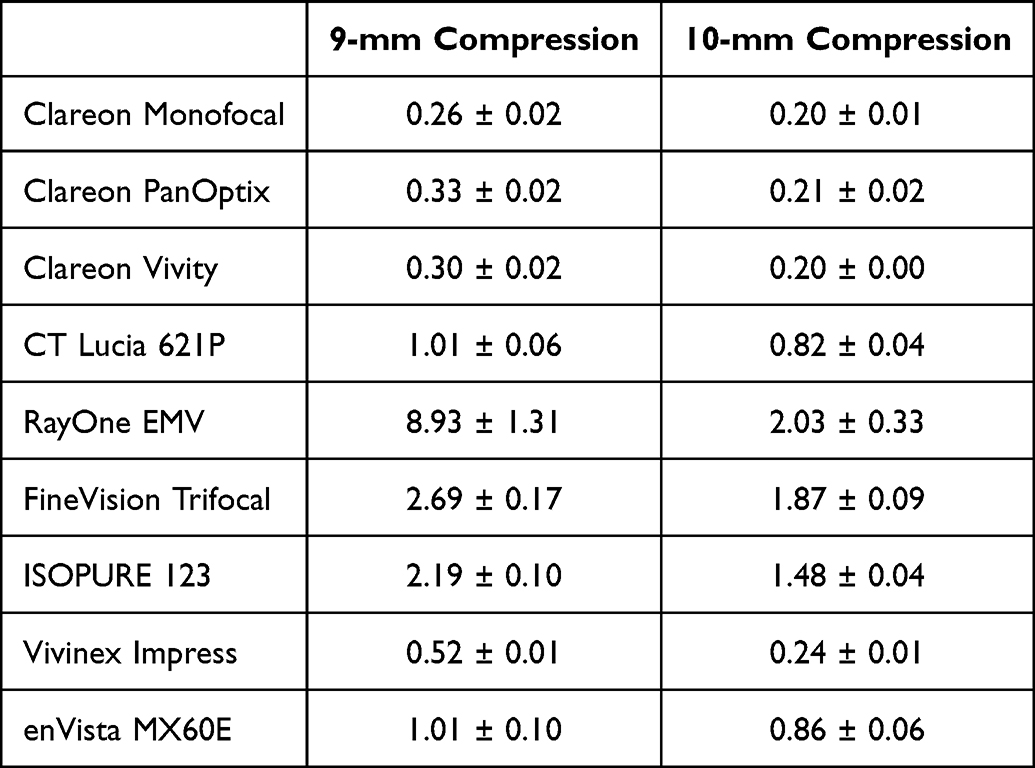 |
Table 3 Haptic Compression Force in Millinewtons (Mean ± Standard Deviation) at Two Compression Diameters (Initial Measurement, at Time = 0) |
Optic Decentration and Optic Tilt
There were no statistical differences (P > 0.05) among all IOL models with respect to optic decentration and optic tilt at either the 9-mm or 10-mm compression diameters (individual model results not presented). Mean optic decentration across all IOL models was extremely small and ranged between 0.02 ± 0.01 to 0.06 ± 0.03 mm at 10-mm compression. At 9-mm compression the decentration range was between 0.02 ± 0.01 to 0.17 ± 0.09 mm. Mean optic tilt across all the models ranged between 0.5 ± 0.03 to 1.3 ± 0.05 degrees at 10-mm compression and 0.8 ± 0.07 to 1.6 ± 1.4 degrees for 9-mm compression.
Discussion
The reaction of an IOL to the compressive forces exerted by the capsular bag can be like those of a building column when excessive weight is present on the roof. Under the normal weight (load), the column remains straight, but excessive weight beyond what the column can support will cause it to deform (bow-out or buckle). In the case of an IOL, inner radial compression forces are exerted by the capsular bag against the lens haptics; in response, the IOL haptics exert opposing outer radial forces against the bag to maintain optic stability. Smaller CBDs will exert higher compression forces than larger CBDs. When the force from the capsular bag exceeds the amount that the haptics can withstand (beyond the haptic critical load), the lens haptics buckle within the bag, causing the optic body to move in the axial direction (resulting in a refractive shift). The compression force from the capsular bag will increase during the healing period when the capsular bag further shrinks around the IOL. Therefore, a given IOL model may experience a range of different forces during the early healing period. The variability of these forces among the cataract patient population may result in unpredictable amounts of axial displacement for some IOL models (based on their haptic design), ultimately changing the lens position and refractive outcome. Engineers designing IOL haptics need to account for the compressive stress that capsular bags might exert during their clinical use (across the population of both long and short eyes).
IOL mechanical stability is a platform performance property based on the design of the haptic and the haptic material irrespective of what optic type might also be present on the lens. At both compression diameters, the three Clareon optical models (Monofocal, Trifocal and EDOF) each had similar axial displacement, decentration and tilt values (because these models have the same haptic design and lens material). Clareon haptics were designed to produce similar mechanical properties to the previous AcrySof® STABLEFORCE® haptics, which have been proven to provide a biomechanical advantage over other lens haptic designs both in bench testing and in clinical studies.1,2,22,23 The equivalence of mechanical performance between Clareon and AcrySof was originally confirmed in our previous laboratory publication.1 Ullrich et al performed a prospective randomized clinical study which measured the (6 month postoperative) ACD of Clareon monofocal versus AcrySof IQ monofocal IOLs and found no significant differences in ACD or refractive outcomes, clinically confirming the mechanical equivalence between AcrySof and Clareon.24 Tutchenko et al have reported significantly larger changes in clinical ACD values (measured between 4 week and 8 weeks after surgery) for Tecnis IOLs when compared to AcrySof IOLs, which may suggest a higher risk of refractive error with Tecnis IOL models.25
Since CBD is correlated with the axial length, one might expect that hyperopic patients (short axial length eyes) who have relatively smaller CBDs would experience a high refractive error when implanted with those IOL models that show large axial displacement at 9-mm compression. Cooke et al conducted a retrospective analysis of a large deidentified database from 71,183 cataract surgeries to examine the refractive prediction errors across multiple IOL models.26 For the Tecnis lenses (6 different models from 19,516 surgeries) there was a myopic refractive error that started with the 23.5 D lens group which became larger with higher power IOLs (error started at - 0.3 D increasing to - 1.5 D). For the enVista model (MX60E from 7,066 surgeries) there was a hyperopic refractive shift also starting with the 23.5 D lenses becoming larger with higher powers (error started 0.1 D increasing to 0.8 D). For the AcrySof and Clareon lenses (6 different models from 38,990 surgeries) there was a relatively smaller myopic error which started at 31.0 D (error started at −0.2 D and increased to −0.4 D). Bosc et al studied the refractive outcomes for the FineVision Trifocal IOL in eyes with different axial lengths.27 At 3-month follow-up, a smaller percentage of short eyes were within ± 0.50 D spherical equivalent as compared to medium or long eyes (70.59% vs. 84.34% vs. 100%). These real-world clinical refractive outcomes further support our laboratory testing which suggest that these IOL platforms have a higher risk of refractive error in short eyes (hyperopic patients who tend to have smaller CBDs) as compared to the AcrySof and Clareon platforms.
Our previous study measured the enVista model MX60 single-piece hydrophobic acrylic IOL originally approved in 2012.28 In 2017, Bausch & Lomb made a change to the enVista IOL material formulation to improve the unfolding time and introduced that new lens as enVista model MX60E.29,30 Subsequently, in this work, we included testing of the new enVista model MX60E. Despite the change in material formula to improve unfolding time, both models have extremely high axial displacement values at 9-mm suggesting that the haptic design of this lens might have a larger impact on the overall mechanical stability.
One limitation of this study is that it uses in vitro laboratory testing with BSS at a physiological temperature to simulate the in vivo clinical conditions. The compression wells are an open model of diameter and lack the surrounding anatomic tissues that might constrain lens movement. Therefore, the laboratory displacement values from these experiments are a worst-case measurement of how much the lens could move under compression. Despite this limitation, our previous and current results which showed large axial displacement with both Tecnis and enVista IOLs do align with clinical observations of refractive shifts seen by Cooke et al,26 Tutchenko et al,25 Hayashi et al,3 and Goto et al.8 Although published clinical studies show magnitudes of refractive error less (Cooke et al reported a clinical maximum of 1.6 D)26 than what is predicted by our laboratory results (maximum 4 D). Further clinical study of the changes in MRSE (a measure of potential RE) during the first 3 months after surgery would help to correlate the in vitro measured axial stability and the refractive stability of the other IOLs studied in our work, especially during that critical healing period when the capsular bag shrinks around the IOL. Another limitation is the small sample size tested, but as shown in Table 2 the within-group variability (represented as the standard deviation) was relatively low. As a reminder, our results represent potential RE values from in vitro measurements in our laboratory. Thus, it is recommended that surgeons compare their clinical refractive outcomes with IOLs both below and above 23 diopters for the model that they are using. The results from the Cooke et al26 clinical publication suggest this power as a critical inflection point for observing refractive error.
Conclusion
Shifts in refractive outcomes may be the result of IOL axial movement (which changes the effective lens position) during the early healing period when the capsular bag shrinks around the lens and is dependent on the haptic design and haptic material for each lens model. In our in vitro laboratory model, all three Clareon IOL models were among the lowest levels of axial displacement and haptic compression force at clinically relevant diameters of 10-mm and 9-mm compression. Consequently, the Clareon IOLs showed the lowest amounts of potential RE when compared to the other studied IOLs. Given these findings, Clareon should have more consistent axial stability at CBDs that are closely aligned with the full range of those reported to occur in the population of cataract surgery patients, which might play a role in more predictable refractive outcomes. In clinical practice, smaller capsular bags (those less than 10 mm in diameter) are more often encountered in shorter axial length eyes, thus these patients may experience more significant refractive shifts due to IOL position changes. We recommend that surgeons consider using IOL models with more stable axial displacement when treating hyperopic patients with short axial lengths (refractive error in these patients may not a “surprise” rather it may be a direct result of the mechanical design of the lens haptics). Additional clinical studies of the refractive error when IOLs are implanted into small capsular bags (IOLs 23 D and above) are warranted to better understand the potential impact on patient outcomes, perhaps using a large patient registry that includes information on the lens model, lens power and post-operative refraction.
Abbreviations
ACD, anterior chamber depth; ANOVA, One Way Analysis of Variance; BSS, Balanced Saline Solution; CBD, capsular bag diameter; D, diopter; EDOF, extended depth of focus; ELP, effective lens position; IOL, intraocular lens; ISO, International Standard Organization, lp/mm, line pair per millimeter spatial frequency; mN, millinewton of force; MRSE, Manifest Refractive Spherical Equivalent; MTF, Modulation Transfer Function; RE, refractive error.
Acknowledgments
The authors thank Nanhong Lou and Maria Jockovich, Alcon Research LLC, who conducted internal independent reviews of this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that was in the conception, study design, execution, acquisition of data, or analysis and interpretation or in all these areas. All authors took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
The study was supported by Alcon Research, LLC, Fort Worth, Texas, USA.
Disclosure
Maxwell is a consultant for Alcon Research, LLC and has no financial interest related to this study. Other authors are employees of Alcon Research, LLC. The authors report no other conflicts of interest in this work.
References
1. Lane S, Collins S, Das KK, et al. Evaluation of intraocular lens mechanical stability. J Cataract Refract Surg. 2019;45:501–10. doi:10.1016/j.jcrs.2018.10.043
2. Wirtitsch MG, Findl O, Menapace R, et al. Effect of haptic design on change in axial lens position after cataract surgery. J Cataract Refract Surg. 2004;30(1):45–51. doi:10.1016/S0886-3350(03)00459-0
3. Hayashi K, Hayashi H. Comparison of the stability of 1-piece and 3-piece acrylic intraocular lenses in the lens capsule. J Cataract Refract Surg. 2005;31:337–342. doi:10.1016/j.jcrs.2004.06.042
4. Koeppl C, Findl O, Kriechbaum K, Sacu S, Drexler W. Change in IOL position and capsular bag size with an angulated intraocular lens early after cataract surgery. J Cataract Refract Surg. 2005;31:348–353. doi:10.1016/j.jcrs.2004.04.063
5. Hayashi K, Yoshida M, Hayashi S, Yoshimura K. Short-term changes in prediction error after cataract surgery in eyes receiving 1 of 3 types of single-piece acrylic intraocular lenses. Am J Ophthalmol. 2020;219:12–20. doi:10.1016/j.ajo.2020.05.031
6. Fukumitsu H, Camps VJ, Miraflores S, Piñero DP. Could anatomical changes occurring with cataract surgery have a clinically significant effect on effective intraocular lens position? Int Ophthalmol. 2021;41(5):1895–1907. doi:10.1007/s10792-021-01751-y
7. Teshigawara T, Meguro A, Mizuki N. Relationship between postoperative intraocular lens shift and postoperative refraction change in cataract surgery using three different types of intraocular lenses. Ophthalmol Ther. 2021;10(4):989–1002. doi:10.1007/s40123-021-00390-x
8. Goto S, Maeda N, Ohnuma K, Noda T. Comparison of two one-piece acrylic foldable intraocular lenses: short-term change in axial movement after cataract surgery and its effect on refraction. PLoS One. 2022;17(8):e0273431. doi:10.1371/journal.pone.0273431
9. Apple DJ, Escobar-Gomez M, Zaugg B, Kleinmann G, Borkenstein AF. Modern cataract surgery: unfinished business and unanswered questions. Surv Ophthalmol. 2011;56(6 Suppl):S3–53. doi:10.1016/j.survophthal.2011.10.001
10. Bozukova D, Pagnoulle C, Jérôme C. Biomechanical and optical properties of 2 new hydrophobic platforms for intraocular lenses. J Cataract Refract Surg. 2013;39(9):1404–1414. doi:10.1016/j.jcrs.2013.01.050
11. Cabeza-Gil I, Pérez-Gracia J, Remón L, Calvo B. Effect of haptic geometry in C-loop intraocular lenses on optical quality. J Mech Behav Biomed Mater. 2021;114:104165. doi:10.1016/j.jmbbm.2020.104165
12. Werner L. Intraocular lenses: overview of designs, materials, and pathophysiologic features. Ophthalmology. 2021;128(11):e74–e93. doi:10.1016/j.ophtha.2020.06.055
13. Borkenstein AF, Borkenstein EM. Geometry of acrylic, hydrophobic IOLs and changes in haptic-capsular bag relationship according to compression and different well diameters: a bench study using computed tomography. Ophthalmol Ther. 2022;11(2):711–727. doi:10.1007/s40123-022-00469-z
14. Cabeza-Gil I, Frechilla J, Calvo B. Evaluation of the mechanical stability of intraocular lenses using digital image correlation. Sci Rep. 2023;13(1):9437. doi:10.1038/s41598-023-36694-0
15. Borkenstein AF, Borkenstein EM. Geometry of modern presbyopia-correcting intraocular lenses and changes in haptic-capsular bag behavior according to compression and different well diameters: a bench study using computed tomography. Ophthalmol Ther. 2024;13(12):3059–3077. doi:10.1007/s40123-024-01046-2
16. International Organization for Standardization. Ophthalmic implants – intraocular lenses – part 3: mechanical properties and test methods (ISO Standard No. 11979-3:2012); December 01, 2012. 2012.
17. Tehrani M, Dick HB, Krummenauer F, Pfirrmann G, Boyle T, Stoffelns BM. Capsule measuring ring to predict capsular bag diameter and follow its course after foldable intraocular lens implantation. J Cataract Refract Surg. 2003;29(11):2127–2134. doi:10.1016/S0886-3350(03)00352-3
18. Kim JH, Lee D, Cha YD, Oh SH, Mah KC, Lee MS. The analysis of predicted capsular bag diameter using modified model of capsule measuring ring in Asians. Clin Exp Ophthalmol. 2008;36(3):238–244. doi:10.1111/j.1442-9071.2008.01726.x
19. Modesti M, Pasqualitto G, Appolloni R, Pecorella I, Sourdille P. Preoperative and postoperative size and movements of the lens capsular bag: ultrasound biomicroscopy analysis. J Cataract Refract Surg. 2011;37(10):1775–1784. doi:10.1016/j.jcrs.2011.04.035
20. Dick HB, Conrad-Hengerer I, Schultz T. Intraindividual capsular bag shrinkage comparing standard and laser-assisted cataract surgery. J Refract Surg. 2014;30:228–233. doi:10.3928/1081597X-20140320-01
21. Market Scope. IOL market report. 2025. Available from: https://www.market-scope.com/.
22. Lane SS, Burgi P, Milios GS, Orchowski MW, Vaughan M, Schwarte E. Comparison of the biomechanical behavior of foldable intraocular lenses. J Cataract Refract Surg. 2004;30:2397–2402. doi:10.1016/j.jcrs.2004.03.041
23. Behrouz MJ, Kheirkhah A, Hashemian H, Nazari R. Anterior segment parameters: comparison of 1-piece and 3-piece acrylic foldable intraocular lenses. J Cataract Refract Surg. 2010;36(10):1650–1655. doi:10.1016/j.jcrs.2010.05.013
24. Ullrich M, Ruiss M, Hienert J, et al. Anterior chamber depth variability between two hydrophobic acrylic single-piece intraocular lenses: a randomized trial. J Cataract Refract Surg. 2021;47(11):1460–1465. doi:10.1097/j.jcrs.0000000000000668
25. Tutchenko L, Patel S, Skovron M, Voytsekhivskyy OV, Gilevska F. Fluctuations of anterior chamber depth and astigmatism in pseudophakic eyes. Clin Ophthalmol. 2024;18:3739–3752. doi:10.2147/OPTH.S492253
26. Cooke DL, Seward MS, Cooke TL. Improving refractive predictability with high-powered intraocular lenses: refractive implications of various optic designs. J Cataract Refract Surg. 2025;51(7):600–606. doi:10.1097/j.jcrs.0000000000001660
27. Bosc C, Joubert R, Le Maléfan E, Boury P, Bernier M, Barrucand A. Visual and refractive outcomes of a hydrophobic trifocal diffractive intraocular lens in eyes with different axial lengths. Clin Ophthalmol. 2025;19:4765–4774. doi:10.2147/OPTH.S562243
28. Packer M, Fry L, Lavery KT, et al. Safety and effectiveness of a glistening-free single-piece hydrophobic acrylic intraocular lens (enVista). Clin Ophthalmol. 2013;7:1905–1912. doi:10.2147/OPTH.S50499
29. Gebhart F. New IOL design gives premium results from non-premium lens. Ophthalmology Times. 2018. Available from: https://www.ophthalmologytimes.com/view/new-iol-design-gives-premium-results-non-premium-lens.
30. ENVISTA IOL Model MX60E Approval, P910056 / S024. From the FDA premarket approval (PMA) database. 2017. Available from: https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfpma/pma.cfm?id=P910056S024.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Dry Eye Disease as a Cause of Refractive Errors After Cataract Surgery – A Systematic Review
Biela K, Winiarczyk M, Borowicz D, Mackiewicz J
Clinical Ophthalmology 2023, 17:1629-1638
Published Date: 6 June 2023