")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
Potential for Use of Portable Ultrasound Devices in Rural and Remote Settings in Australia and Other Developed Countries: A Systematic Review
Authors Shaddock L, Smith T
Received 19 January 2022
Accepted for publication 17 March 2022
Published 29 March 2022 Volume 2022:15 Pages 605—625
DOI https://doi.org/10.2147/JMDH.S359084
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Liam Shaddock,1 Tony Smith2
1Medical Radiation Science, School of Health Sciences, The University of Newcastle, Newcastle, New South Wales, Australia; 2The University of Newcastle Department of Rural Health & School of Health Sciences, The University of Newcastle, Newcastle, New South Wales, Australia
Correspondence: Tony Smith, The University of Newcastle Department of Rural Health, C/- 69A High Street, Taree, Newcastle, NSW, Australia, Tel +61 466 440 037, Email [email protected]
Introduction: Point of care ultrasound (POCUS) has become more common for rapid evaluation. Applications are limited by lack of training of users, difficulty maintaining ultrasound competencies, access to equipment for optimal imaging, and limitations in quality control. Such barriers exist in low-resource, underserved health care settings.
Objective: The aim was to explore the use of POCUS in under-resourced health care settings, such as rural and remote locations in Australia and other countries. Key variables include health outcomes, quality of care, service availability, examinations types performed, equipment used, who performs the examinations, and the ultrasound training received.
Methods: Literature was identified via CINAHL, Cochrane, Embase, Medline, PubMed, SCOPUS, and Web of Science, plus grey literature. Recommended guidelines were followed, and only research-based articles were included, with searches limited to English language and 2010–present.
Results: After screening, 23 articles were reviewed. No studies had low risk of bias and, overall, the quality was poor and only two studies used random sampling. The majority were from developing countries, with only one performed in Australia. Echocardiographic screening in schools was common. Others included emergency department (ED) patients, abdominal aorta screening, obstetric scans, and intensive care unit (ICU) management. Operators included ED doctors, medical students, nurses, community healthcare workers and general practitioners, who received limited training in protocol-driven scanning, often monitored by experts. In comparison to clinical assessment, standard ultrasound or other imaging, accuracy was of the order of 70– 95%, depending on the condition, with high efficacy in improving patient care.
Conclusion: Lack of studies of POCUS in Australia and other developed countries suggests a need for further research. Current evidence supports use of limited ultrasound using portable machines in locations with limited access to diagnostic ultrasound performed by sonographers, which has the potential to improve health outcomes in under-resourced communities in Australia and elsewhere.
Keywords: point-of-care, POCUS, sonography, mobile, handheld, rural health
Introduction and Background
Ultrasound is a valuable imaging modality that has been used increasingly for a variety of diagnostic procedures in medicine since becoming more common place in the 1960s.1 While most commonly used for obstetric scans in the early days, its uses now extend beyond obstetrics into many facets of medicine. Through recent technological improvements, ultrasound machines have also become more portable, user friendly and affordable, including hand-held devices.2 Ultrasound examinations are usually performed by sonographers, health professionals with extensive training, or by radiologists and other specialist medical practitioners, somewhat limiting access and availability of the modality. As the technology has changed, however, access to ultrasound has broadened to include other practitioners with appropriate training and equipment.3,4 The advances have allowed ultrasound machines to be used by a range of health professionals at a patient’s bedside for a variety of examination types, increasing the diagnostic utility of ultrasound at the point-of-care.
As a consequence of the technological evolution, point of care ultrasound (POCUS) has become increasingly common, particularly in emergency medicine and in locations remote from mainstream, usual care.4 Scanning protocols suited to such applications and relevant training programs have been developed. Many undergraduate and postgraduate medical education programs now integrate some basic ultrasound training into the curriculum.5 Nevertheless, the application of POCUS is limited by several factors, including: lack of training of users in the scans they need to perform; shortage of time for practitioners to maintain their US competencies; access to the equipment, particularly the standard of ultrasound machines necessary for acquiring best possible images;6 and limited availability of maintenance, repair and quality control of the ultrasound devices and images. Barriers such as these are prevalent in low-resource or underserved health care settings, such as in rural and remote locations.7
The World Health Organisation (WHO) defines underserved areas as ‘geographical areas where populations have limited access to qualified health-care providers and quality health-care services’.8 Under that definition, the WHO includes
remote and rural areas, small or remote islands, urban slums, conflict and post-conflict zones, refugee camps, minority and indigenous communities, and any place that has been severely affected by a major natural or man-made disaster8.
As of 2020, approximately 44% of the world fits this description, making this a relevant issue across the world,9 including within developed countries. Much of rural and remote Australia, for example, fits the definition of being underserved, particularly by virtue of limited staffing, especially specialist medical and allied health service providers, lack of available facilities, equipment and health care resources, and relatively poor patient outcomes compared with urban populations.10,11
As in other countries, in Australia, rural or remote areas are classified as according to the government’s classification systems,12 which are used this to prioritise and incentivise staffing, including allocation of funding for education and training.13 Such incentives, however, do not generally extend to support for medical imaging practitioners.14 This can lead to limitations on the range of services and resources available for the variety of patient presentations that a rural health service faces. One measure to address these limitations involves the local health professionals, other than medical imaging practitioners, acquiring a broader skillset and extending their role beyond traditional professional boundaries. This usually requires a time and monetary commitment to undertake further training, on top of the cost of acquiring the necessary medical imaging equipment. There is a risk that, in order to bridge the affordability-gap, concessions may be made in training, as well as in equipment type, capability and quality, potentially leading to sub-optimal patient outcomes.
Previous Reviews
There have been other literature reviews performed evaluating various specific aspects of ultrasound use in resource-limited settings. Obstetric examinations were the focus of some recent reviews, which concluded that ultrasound has the potential to improve aspects of foetal, perinatal and maternal health.15,16 While the potential was recognised, appropriate support and monitoring were recommended to ensure positive outcomes. In both reviews, limited training of providers and inappropriate use of ultrasound were raised as significant concerns related to the use of ultrasound to determine foetal sex, inadequate image quality and consequent misdiagnosis. Those concerns are increased with the growing availability of low-cost portable ultrasound devices, particular when used by practitioners with limited knowledge and experience.
Two other reviews focused on the potential impact on ultrasound use of tele-communication technology.17,18 While the studies included were potentially biased due to self-reporting, both studies concluded that tele-ultrasound has a potential future role in imaging. Neither of those reviews had a specific focus on resource-limited settings, though both acknowledged the potential benefits in remote locations as transmission and reception limitations are overcome and the image quality of portable ultrasound devices improves. A further review explored the impact of tele-ultrasound in rural settings,19 though not specifically POCUS. Again, the quality of the evidence was lacking but the authors concluded that the image quality was satisfactory for diagnosis and patient management.
In further reviews, the search and exclusion criteria used led to a very specific field of interest and limited retrieval of relevant literature. Telford et al20 explored articles comparing standard echocardiography machines with handheld equipment, finding high levels of accuracy for handheld ultrasound in detecting definite rheumatic heart disease, though poor accuracy for detection of borderline disease. That review included metropolitan and rural areas, with more focus on proof of concept for handheld devices, rather than the potential benefit of portable devices in low-resource settings. Similarly, Marangou et al21 explored the use of echocardiography in Indigenous and underprivileged populations, highlighting the need for more accessible ultrasound technology for screening and diagnosis of disease in those populations. Both reviews focused on particular conditions and examination types, rather than the variety of uses of ultrasound.
Becker et al22 performed a systematic review in 2016 with a focus on portable ultrasound in low-and middle-income countries, as defined by the WHO, which included Argentina, Bangladesh, Nepal, South Africa, and Thailand. They found that ultrasound is used for a variety of patient presentations and conditions in low-resource areas, including screening for heart disease, various emergency and trauma presentations, and both within and outside the hospital setting. That review also reflected on the types of ultrasound machines being used. It was concluded that further higher quality research is needed to better inform the general use recommendations, as well as the scope and impact of handheld, portable ultrasound devices. That study, as well as others that delved into ultrasound use in underserved areas,23,24 provides relevant background relating to the use of ultrasound in resource-limited settings. However, those studies do not necessarily translate into the Australian rural and remote health care environment, which is the context of interest to the authors of this systematic review.
Aim of This Review
Building on the previous research above, this systematic review aims to explore the use of POCUS in relatively under-resourced health care settings, with particular reference to rural and remote contexts in developed countries, such as Australia. A range of study types will be included in the review, so comparison may be made with mainstream, conventional ultrasound service provision, including in metropolitan locations, or pre-existing services, which may include having no prior ultrasound services available. Principal outcome variables may include health outcomes, quality of care, and service access and availability, provided relevant data is reported. Other descriptive variables that will be collated include: the types of ultrasound examinations performed; the types of equipment used; who was performing the examinations; and, if not performed by a sonographer with formal tertiary education, the type of training received for their ultrasound imaging role.
Methods
This systematic review was registered with PROSPERO Centre for Systematic Reviews and Dissemination (ID: 273142; 09/09/21). The method used was based on the Cochrane Guidelines for Systematic Reviews25 and reporting is in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA; 2020 Statement).26 Following development of the above study aim in PICO (Population, Intervention, Comparison and Outcomes)27 format and identification of relevant search terms, a consultation was held with a University Research Liaison Librarian to design a search strategy. Key search terms, with relevant truncations were linked using Boolean operators, as below:
(Ultraso*.mp. OR (exp ultrasound/) OR sonogr*.mp.) AND (rural.mp. OR resource.mp.) AND (access*.mp. OR avail*.mp.) AND (portable mp OR handheld.mp. OR pocket.mp. OR mobile.mp. OR (point-of-care.mp. OR (“point of care ultrasound”/)))
In order to minimise the risk of publication bias and the capture as many relevant studies as possible, searches were performed on seven electronic databases (CINAHL, Cochrane, Embase, Medline, PubMed, SCOPUS, and Web of Science). These were accessed via the University of Newcastle’s library between December 2020 and October 2021 by first author (LS), the last search having been performed on 16th of October 2021.
Variations of words or database syntax were occasionally required for an individual database, but the results reflected the search as intended. To address the use of “‘rural’ OR ‘resource’”, the authors discussed various terms and decided on these key words to best represent resource-limited environments. While this expanded search results to a variety of articles mentioning resources, it was deemed appropriate to ensure no articles were missed that addressed resource limitations in different words. As mentioned in the introduction, advances of ultrasound technology have provided more mobile, accessible, and affordable ultrasound units, particularly in the last decade or so. Becker et al found that most relevant articles for their review were published after 2010,22 so that time period was the focus of this review. An example of the search strategy is shown in Table 1, including the number of records identified with each search string. Data base search results were supplemented by a hand-searching references lists of peer-reviewed journal articles, especially other relevant reviews of literature. Grey literature was sourced and subject to the same limitations as database searching.
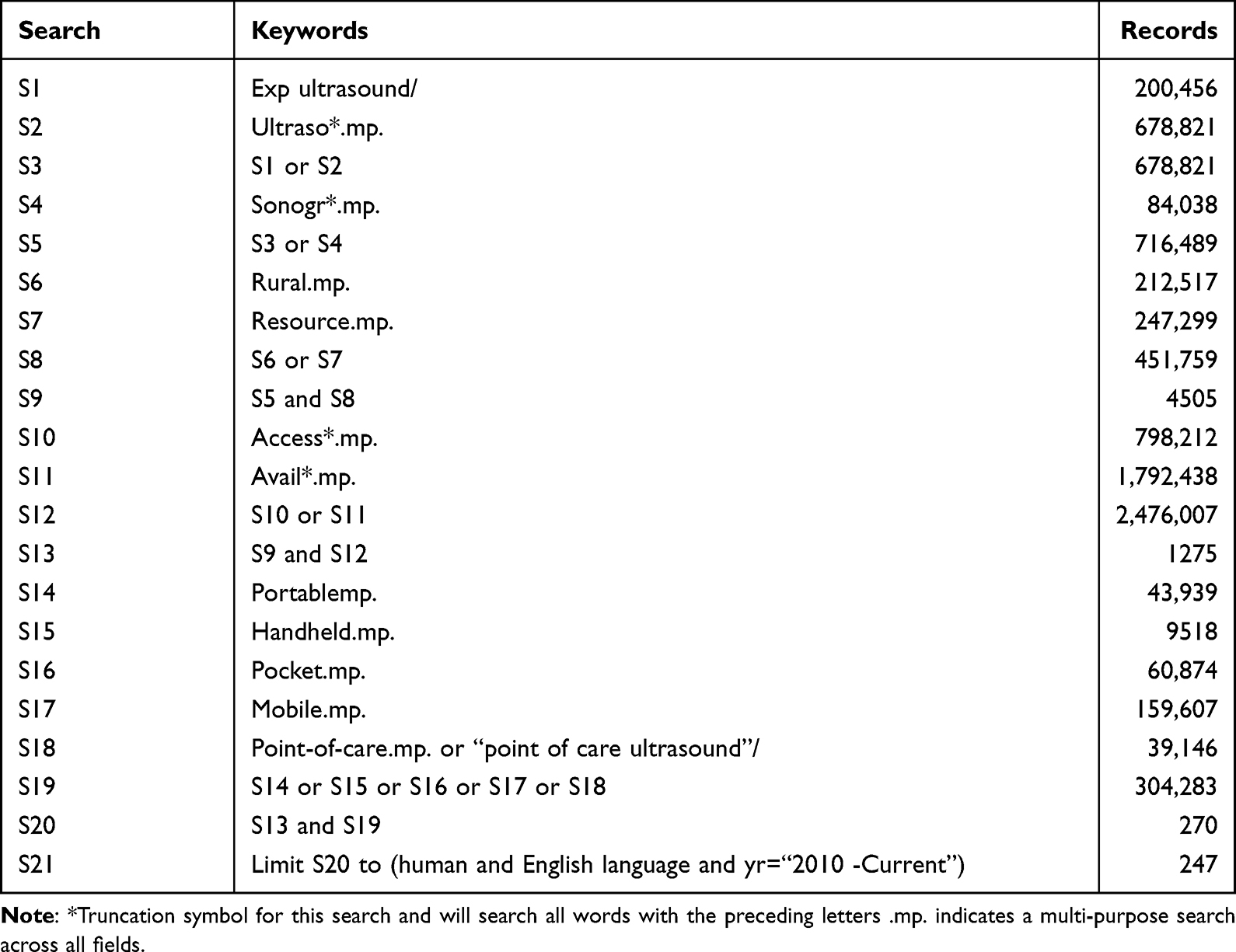 |
Table 1 Embase via Ovid Search (Last Performed October 2021) |
Records from all databases, including electronic copies of abstract and full-text articles, were compiled using Endnote 20 software (Clarivate, Philadelphia: https://endnote.com/contact/) and then exported to Covidence (Veritas Health Innovation, Melbourne: https://www.covidence.org/). After removal of duplicates, title and abstract screening was carried out by both authors (LS and TS), with conflicts resolved by consensus. Inclusion and exclusion criteria were as shown in Table 2. Types of articles excluded were non-research-based reviews, case reports, editorials and discussion papers. Remaining eligible records then underwent full-text screening in Covidence, again by both authors and with conflict resolution, as necessary. Subsequently, all retained articles were subject to quality assessment using standardised risk of bias criteria based on the Cochrane RoB2 tool.28 Data extraction and synthesis used a template constructed in Covidence to record first author, year of publication, country of study, study type, study aims, population description, sample size study methods, type of ultrasound equipment used, provider training, and the results of the study.
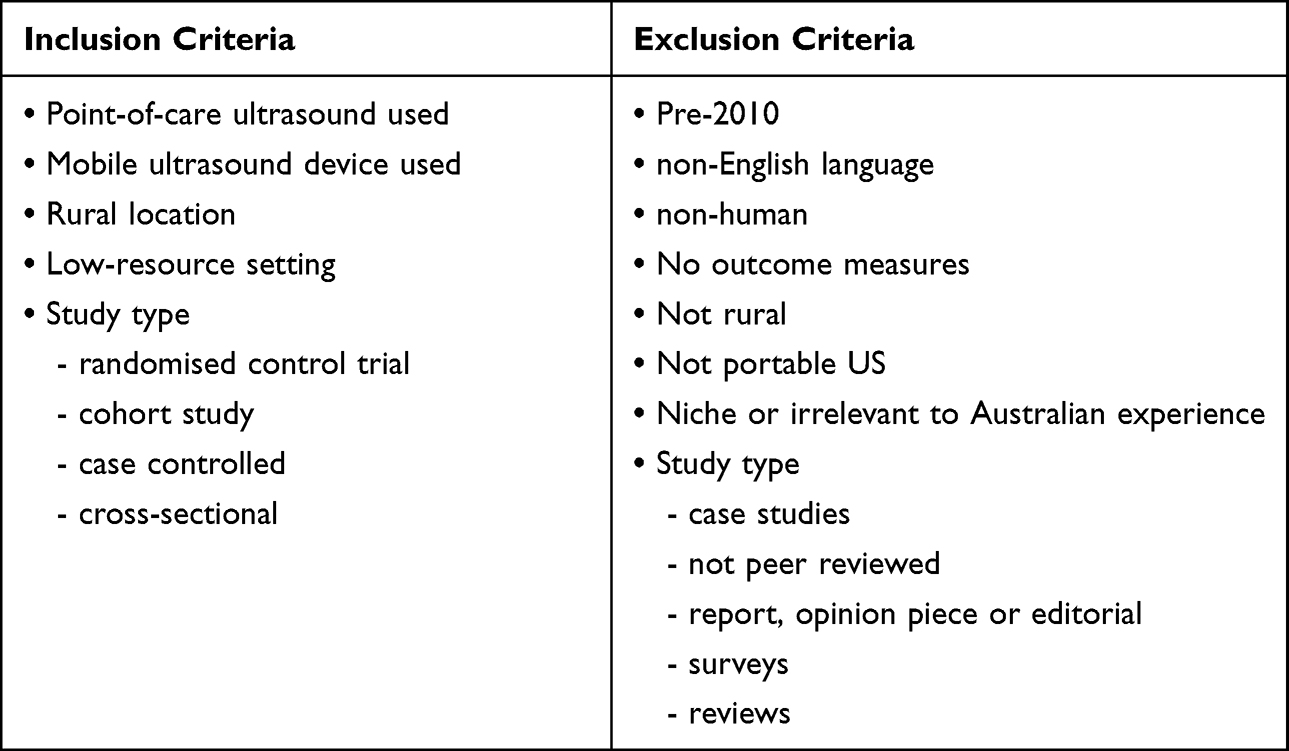 |
Table 2 Inclusion and Exclusion Criteria Used in This Systematic Review |
Results
Figure 1 shows the PRISMA flowchart of the articles screened, with the initial searches of the various databases yielding 806 articles. After screening was completed, 23 articles remained eligible and were included for quality assessment and data extraction. The results of quality assessment are shown in Table 3. None of the studies had a low risk of bias in all seven assessment criteria of the RoB2 tool and, overall, the quality of studies was poor, with a high risk of bias being common. One study, by Ketelaars et al,29 was considered to have a high risk of bias in all categories. For two other studies, no criteria were considered to meet the expectations for low risk, although there was uncertainty for some criteria. Seven of the studies appeared to have low risk of bias in a majority of the criteria but none had low risk in all categories.
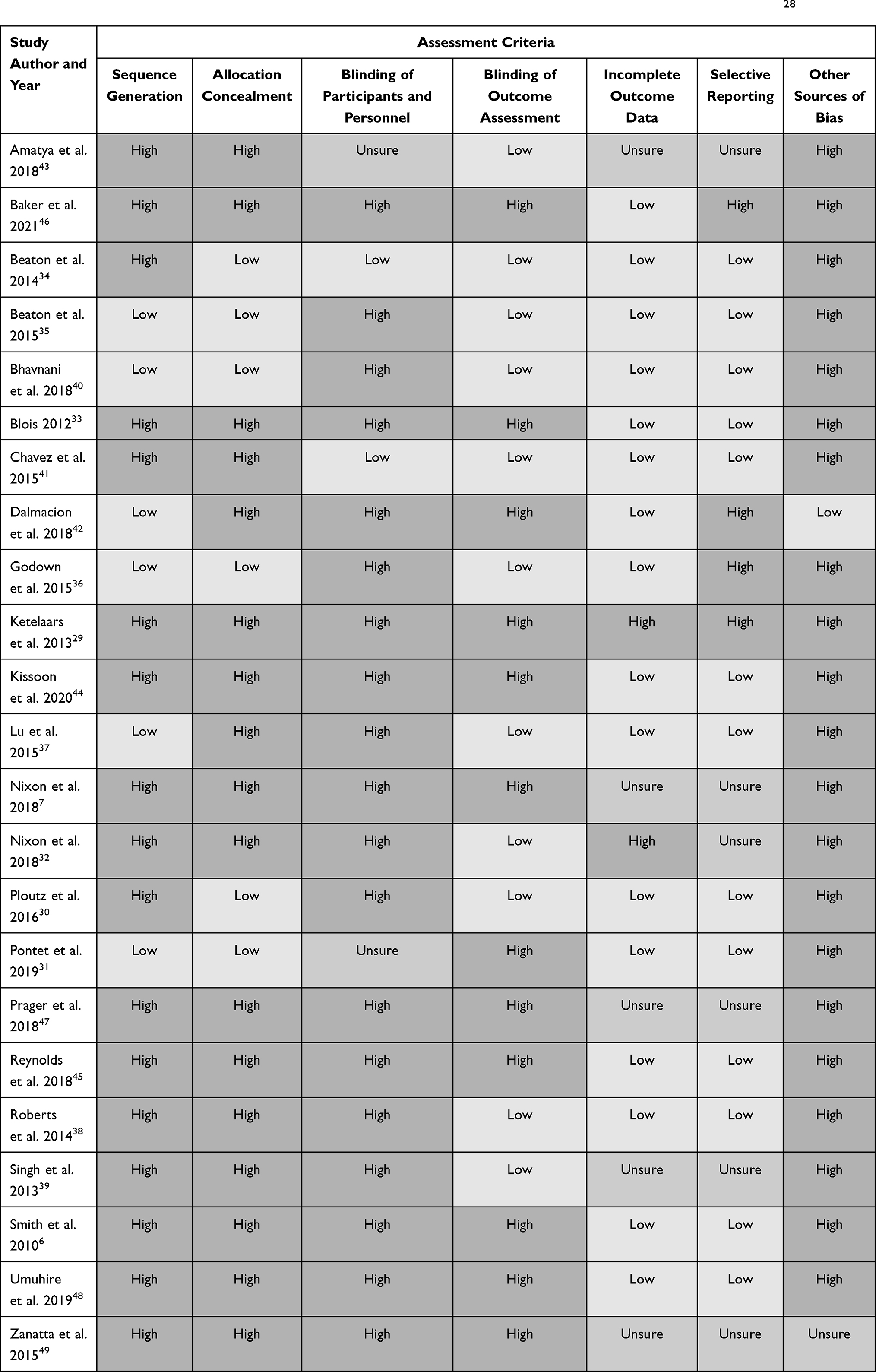 |
Table 3 Risk of Bias Quality Assessment of Studies Included in This View, According to the Cochrane RoB2 Criteria.28 |
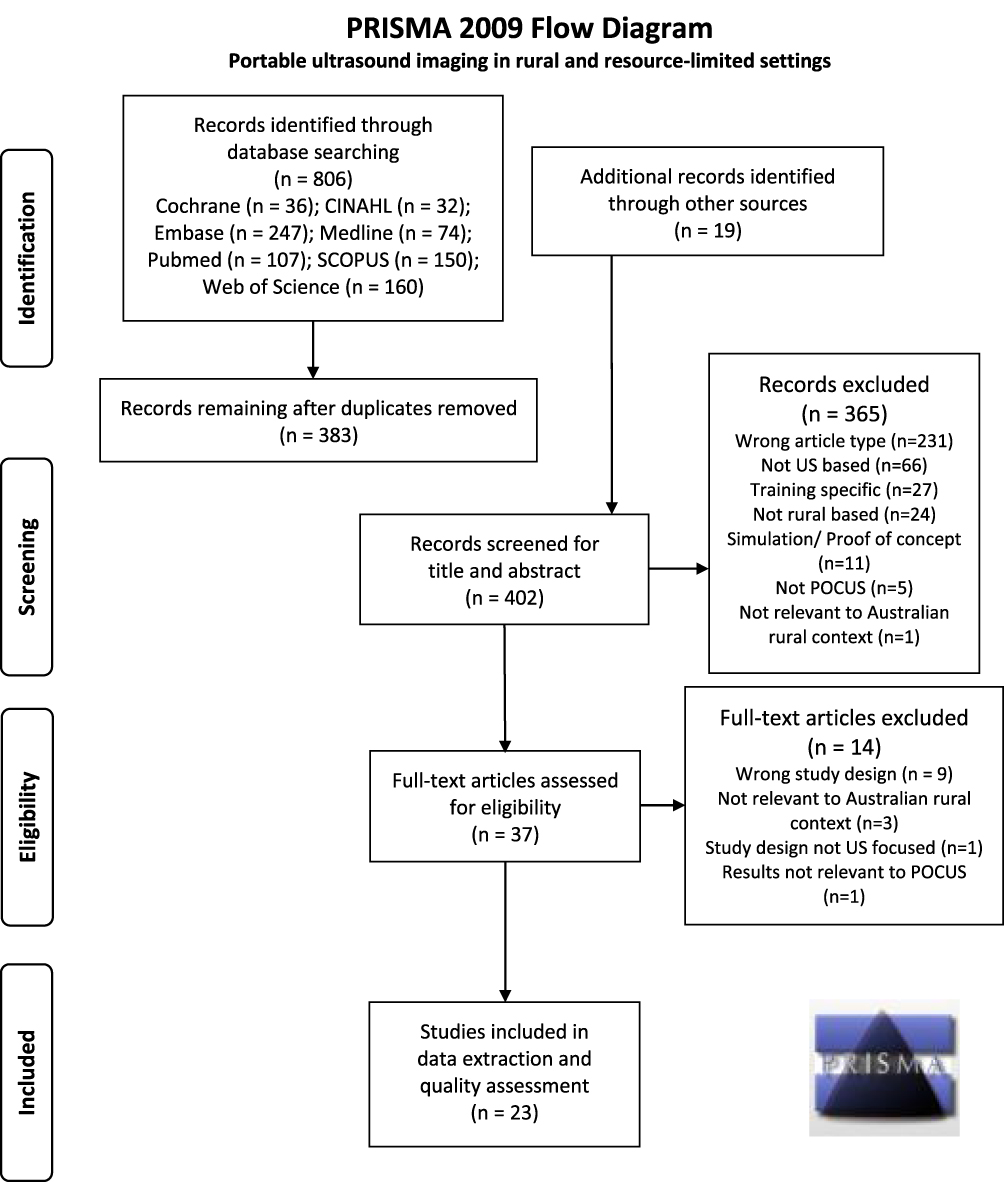 |
Figure 1 PRISMA flow diagram showing the process used and records included and excluded at the various stages of this systematic review. Notes: Adapted from Page MJ, McKenzie JE, Bossuyt PM et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372: n71. Creative Commons license and disclaimer available from: http://creativecommons.org/licenses/by/4.0/legalcode26. |
The results of the data extraction are shown in Table 4, with details expanded upon below. Given the focus on resource-limited regions, the majority of the studies were performed in developing countries. Only one study had been performed in Australia. Most were cross-sectional and descriptive cohort studies, of which four were retrospective and the rest prospective. There was one prospective comparative study, by Ploutz et al,30 but only two studies employed some form of random sampling, while only one, by Pontet et al,31 had a control group comparator. In total, there were 18,893 patients or study subjects, taking into account that Nixon et al reported two studies with different outcomes measures on the same study cohort.7,32 In total, about 4000 of the study subjects (21%) were school children, most being in screening studies for cardiac abnormalities.
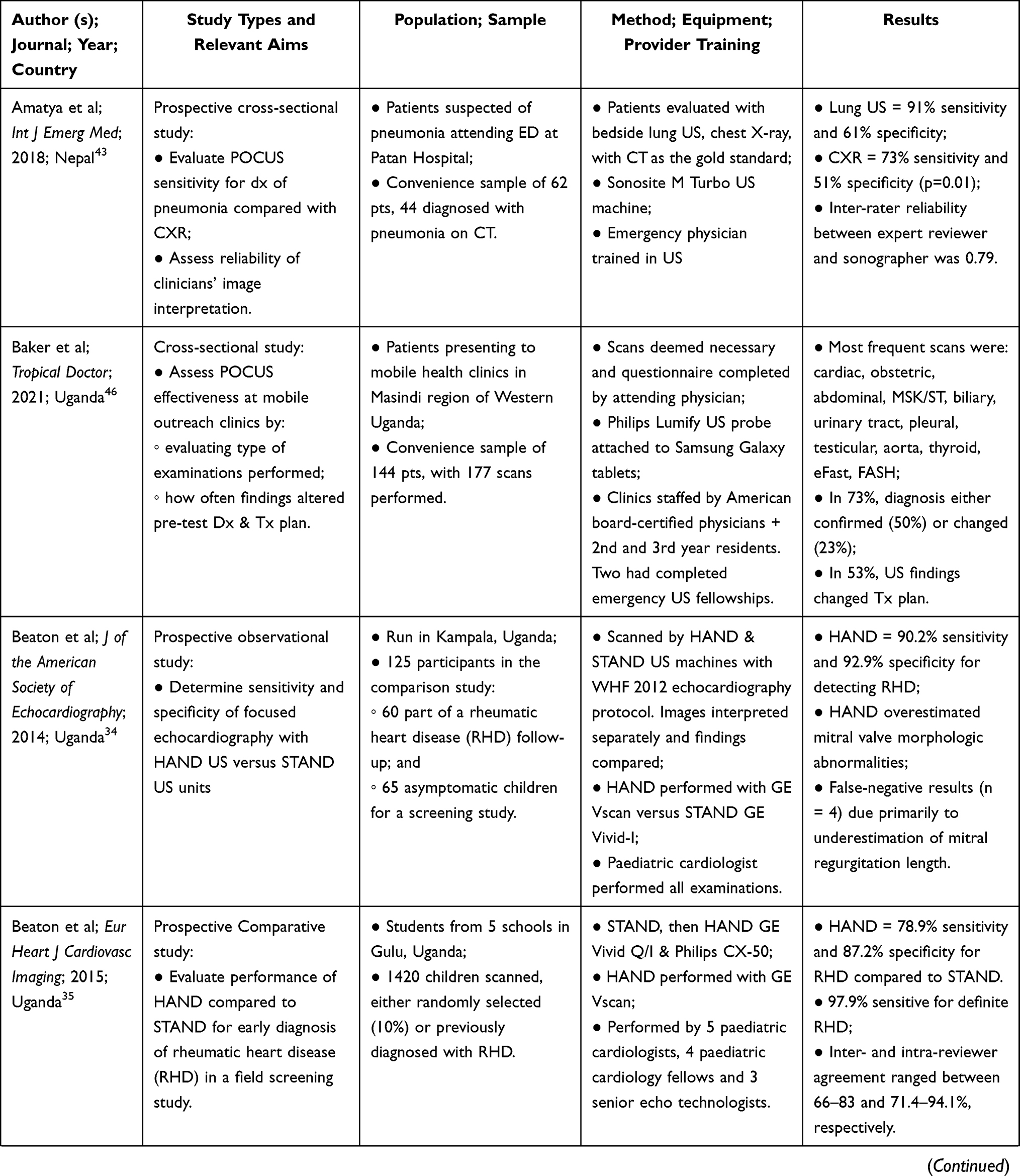 | 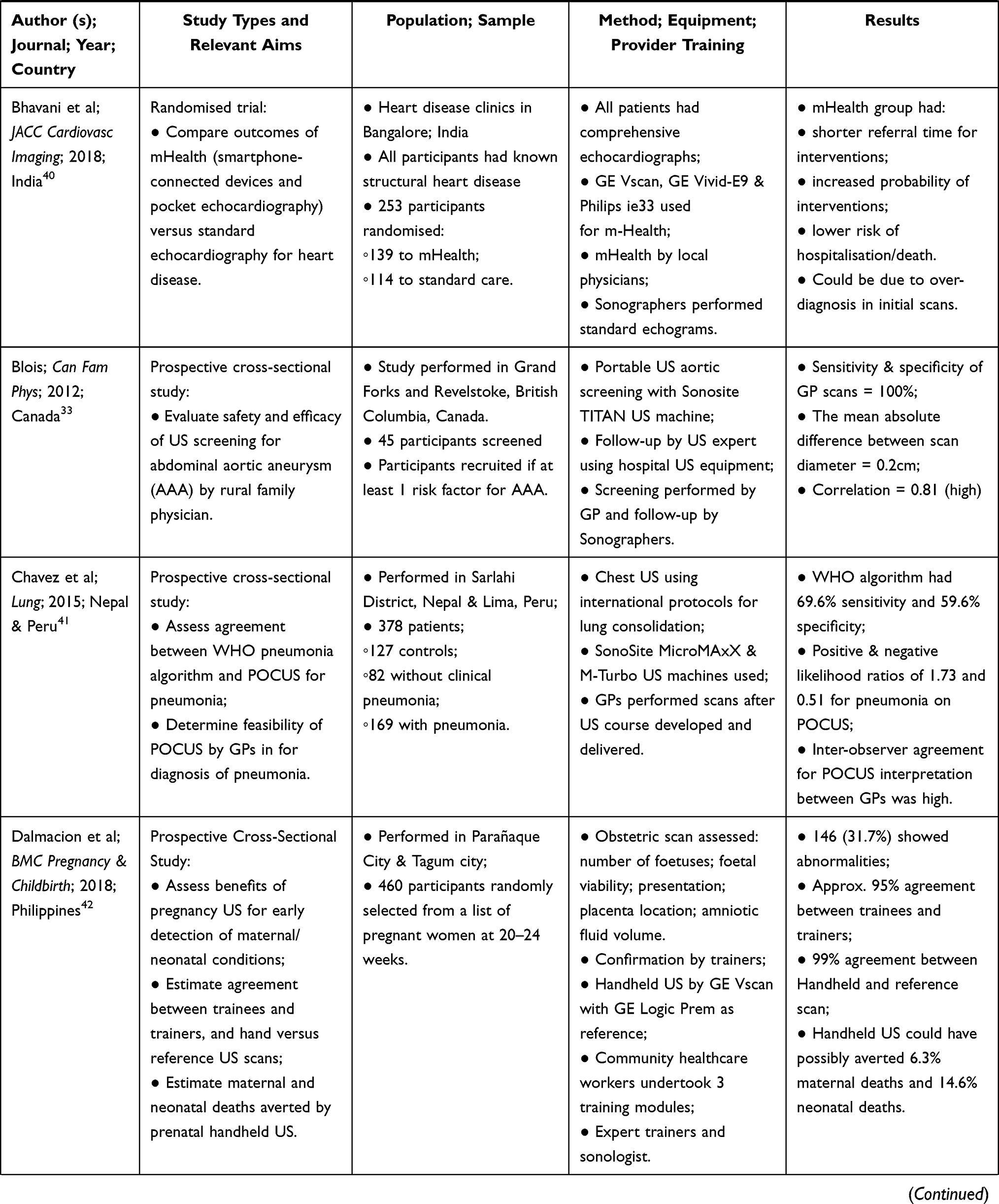 |  | 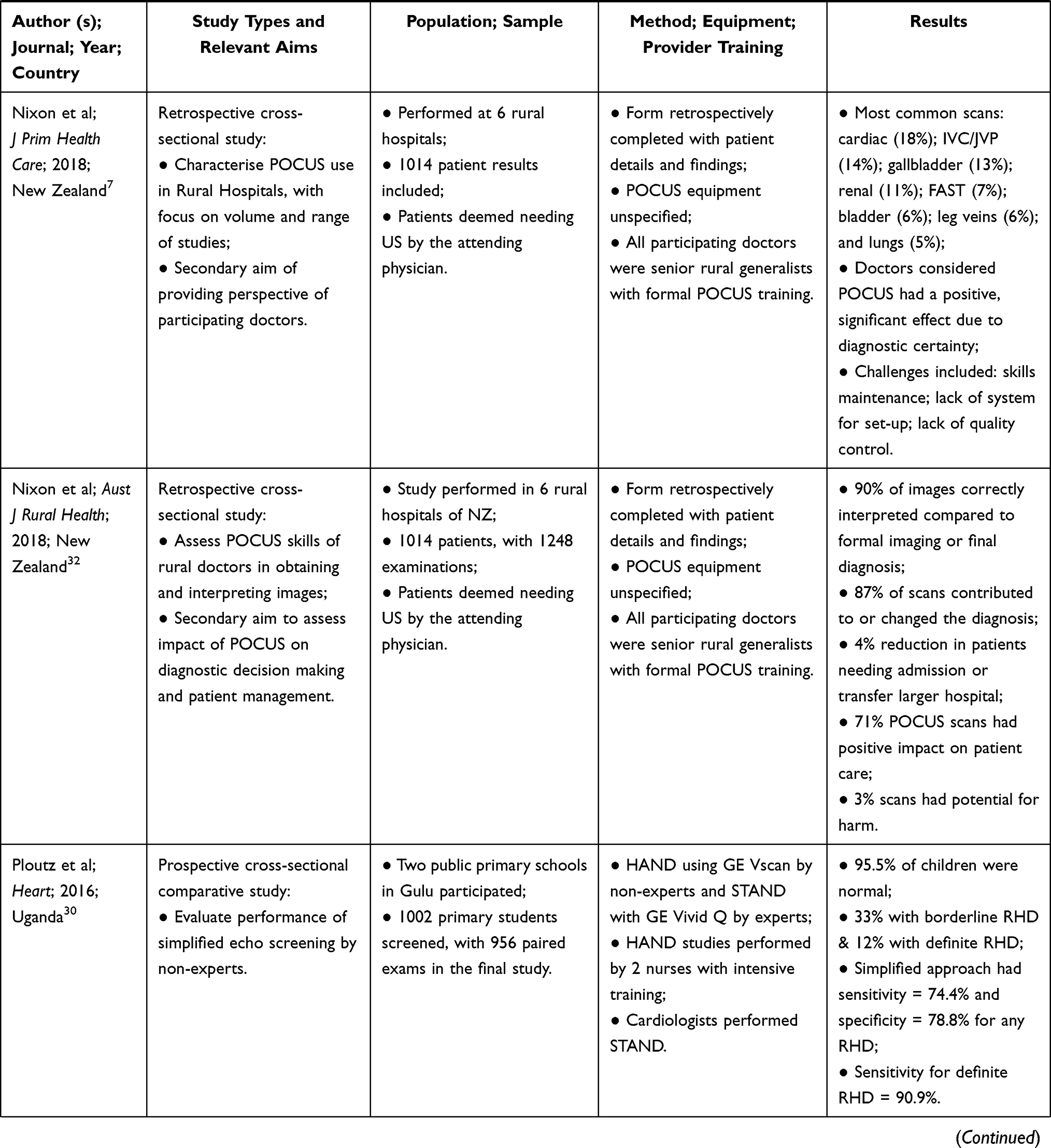 | 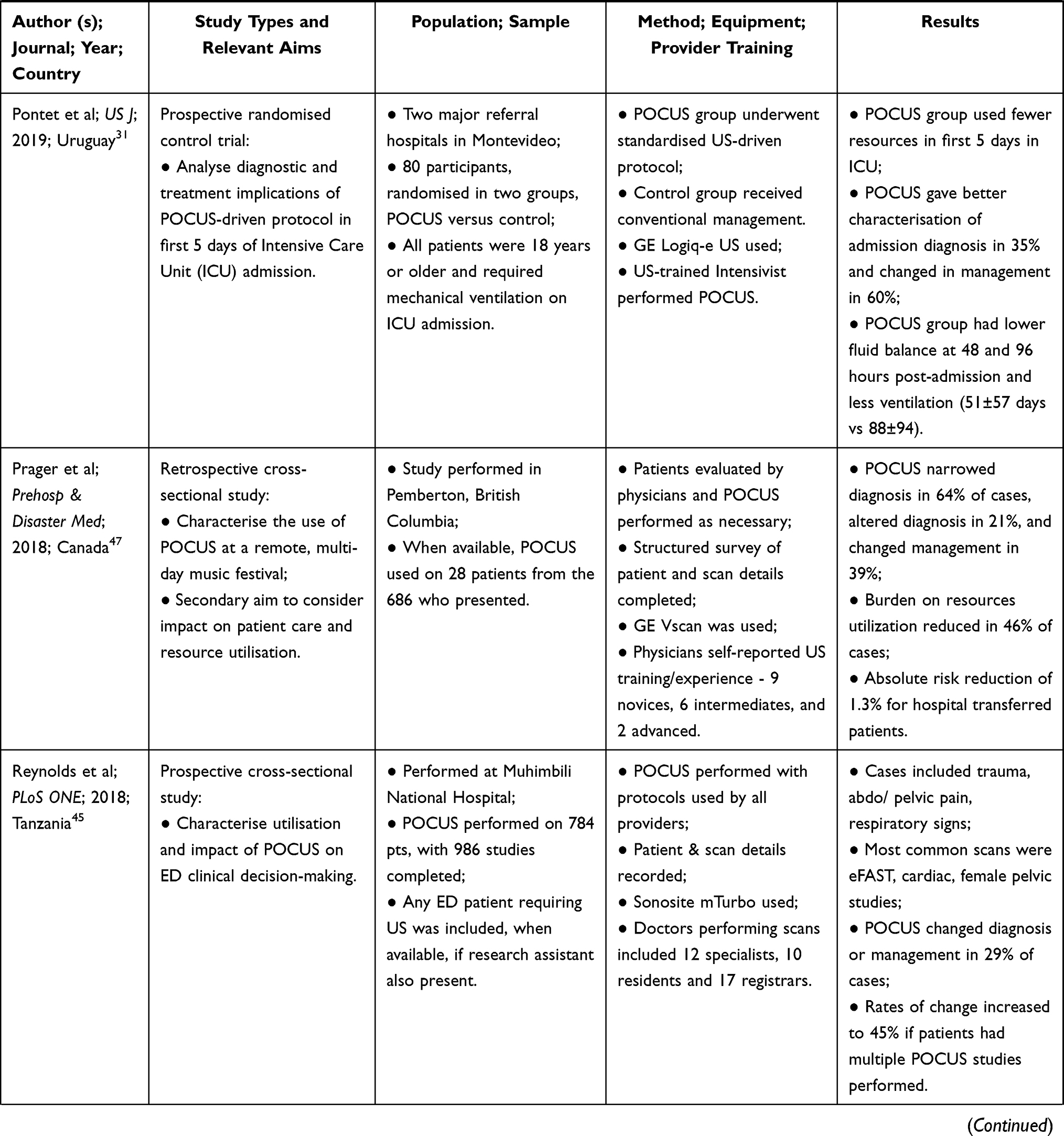 | 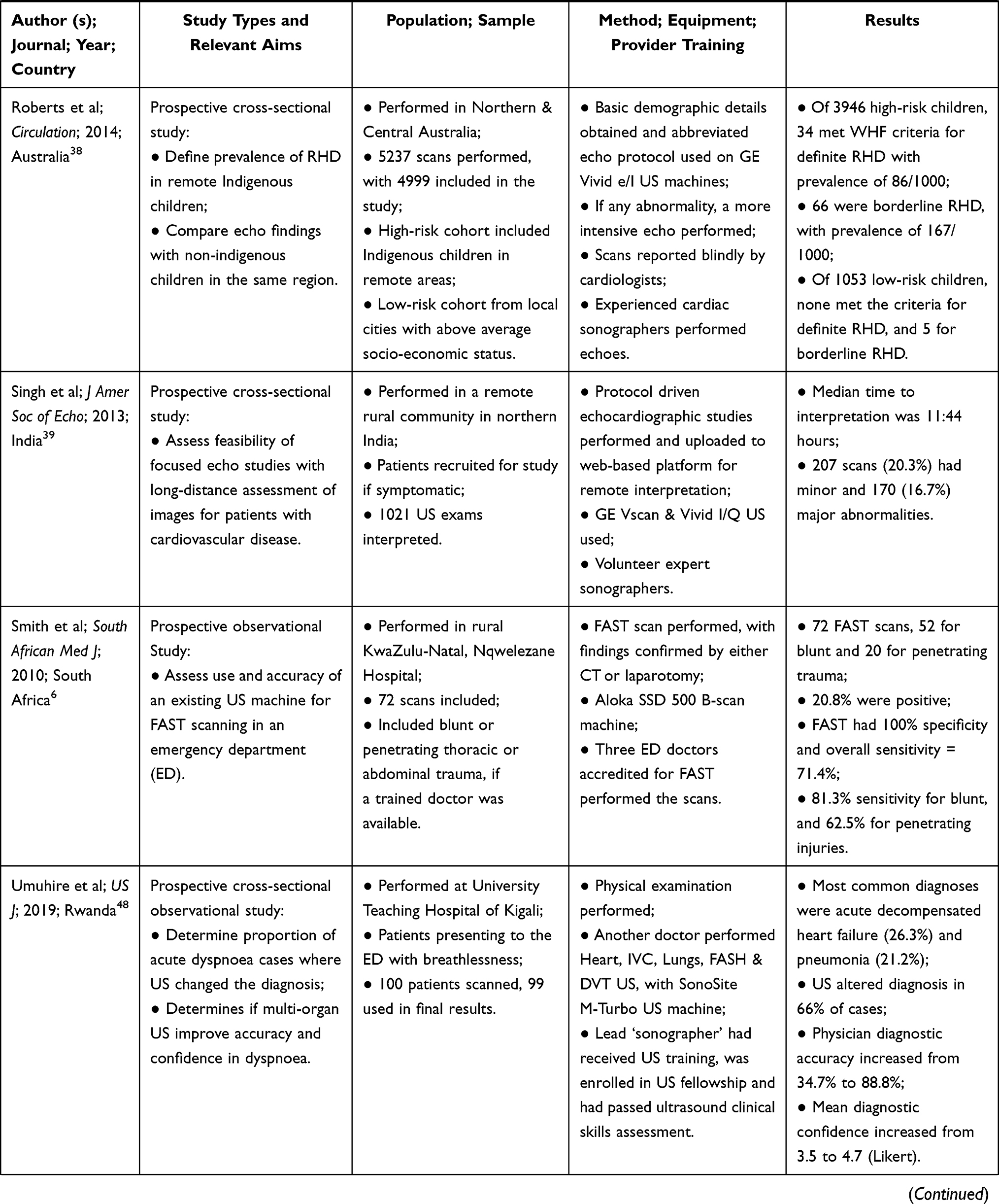 | 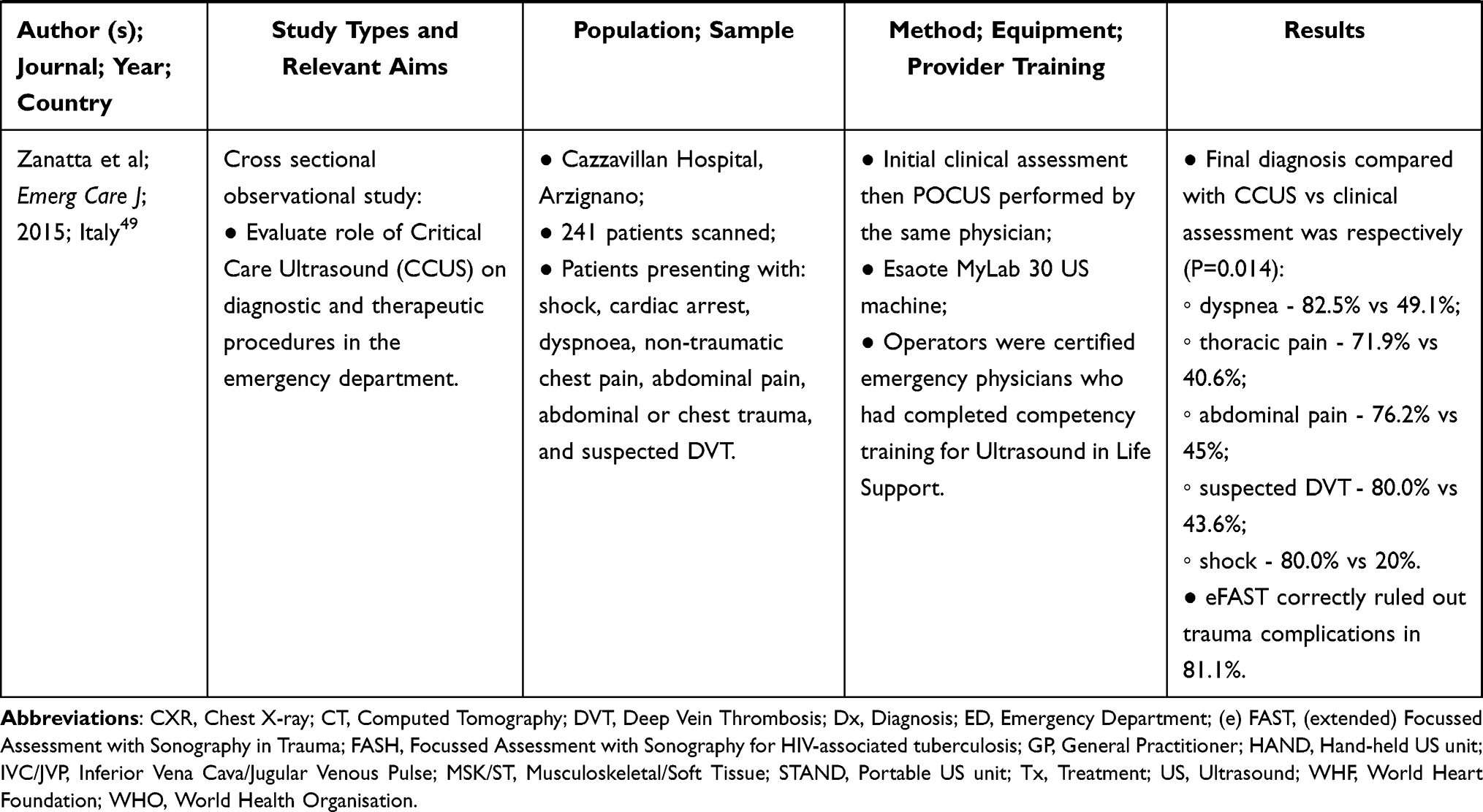 |
Table 4 Summary of the Characteristics of the Studies Included in This Systematic Review Following Data Extraction |
Setting and Context
As mentioned above, most studies were performed in developing countries that face challenges related to limited healthcare resource access and availability, including limited access to medical imaging services. As shown in Table 4, eight of those studies were performed in Africa, six in Uganda alone, while others were based in Nepal, India, The Philippines and South America. Another eight studies were performed in rural and remote regions of countries with a westernised health care system, in Canada, Europe, Australia and New Zealand.
Although cardiac screening in schools was reported in several studies, most studies took place in hospitals, usually in the emergency department (ED), or in other health care settings, such as General Practice (GP) clinics. One study looked at the use of POCUS in a helicopter retrieval service, finding that its use changed treatment plans in 21% of patients.29 The ED studies commonly investigated the diagnostic accuracy of the ultrasound examinations compared with other diagnostic tests, as well as effects on patient management and disposition for definitive care. The one prospective randomised control trial investigated the use of ultrasound in the Intensive Care Unit (ICU) of two major referral hospitals and found lower overall utilisation of resources for the POCUS cohort compared to the control group.31 In that study, while mortality rates were the same in both cohorts, there was a decreased ICU length of stay in the POCUS group.
In 52% (12/23) of the studies, ultrasound equipment was provided specifically for the purpose of the study, reflecting a lack of access under normal circumstances. This is assumed to have been the case for the screening studies, particularly for those performed in schools. In six studies, previous ownership of equipment was either stated or implied, although in other studies no mention was made of how the ultrasound equipment was acquired.
Examination Types
There was a broad range of ultrasound examination types performed across the different studies. Most studies used POCUS for ED patients (10/23) or for echocardiography (8/23), while other examinations types included lung ultrasound (2/23), abdominal aorta screening (1/23), obstetric scans (1/23), and ICU diagnosis and management (1/23). Many of the studies involved multiple examination types, with a summary shown in the bar chart in Figure 2, cardiac scanning being the most common, documented in 15 different studies.
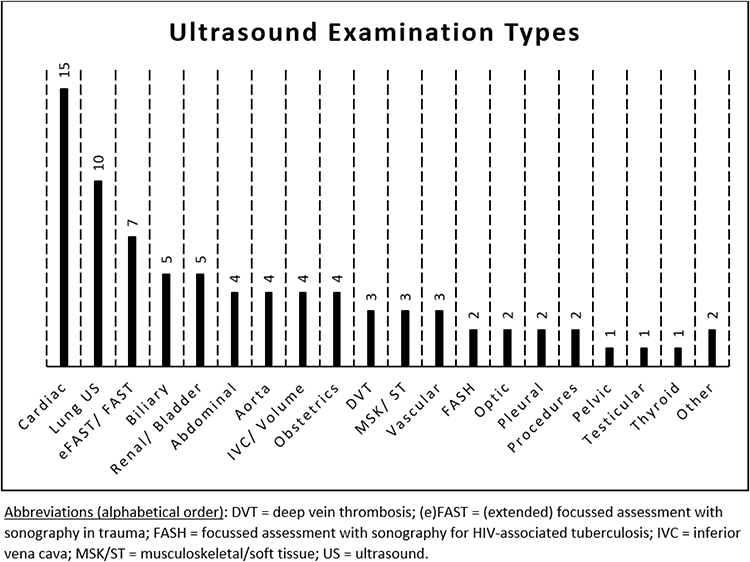 |
Figure 2 Barchart showing the range of ultrasound examination types and the number of articles in this systematic review that included each type of examination. |
Diagnostic accuracy and utility were generally high. All screening studies were able to successfully confirm or exclude the conditions of interest compared to a gold standard. For example, Blois performed aortic screening at a GP clinic, comparing the findings with those for an examination performed by a trained sonographer and found 100% sensitivity and specificity.33 Other screening studies were echocardiographs that compared findings for different patient presentations, scanning protocols, operators, or equipment and comparisons.30,34–40 Patients who screen positively for the abnormality in question underwent appropriate diagnostic follow-up and treatment.
Practitioners and Training
There was a broad range of POCUS imaging providers, with various prior qualifications and experience, including 10 studies involving ED doctors with varying levels of experience. Other studies included medical students, nursing staff, community healthcare workers and general practitioners (GPs). The screening studies were performed or closely monitored by experts, who were sonographers, specialist echocardiographers, paediatric cardiologists, cardiology specialist trainees or experienced ICU specialists.
Training of ultrasound providers for specifically for POCUS was described in four of the articles, which included: nurses with limited ultrasound experience trained in a echocardiography protocol;30 GPs undertaking standardised training course for detection of pneumonia;41 community health care workers receiving device-specific training in obstetric scanning;42 and, local physicians training in the use of a pocket ultrasound device for echocardiography using a previously published protocol.40 Training courses used either classroom or computer-based learning modules, taught by specialists, with a practical component completed under supervision. Studies reported high rates of success. For example, the study by Dalmacion et al42 compared the finding of obstetric scans performed by community health workers using handheld portable ultrasound equipment with examinations performed by experts, finding 99% agreement. Significantly, the authors of that study concluded that POCUS had the potential to avoid an estimated 6.3% of maternal and 14.6% of neonatal deaths.42
Outcomes Measures
The results of each study in terms of various outcome measures are shown in the far-right column of Table 4. In several descriptive studies, the outcome was reported simply in terms of the types of examinations performed. Other studies reported the sensitivity and specificity of POCUS compared to other diagnostic examinations, such as auscultation,36 CT,43,44 specialist consultation and surgery.45 Several studies reported comparisons between different types of ultrasound equipment, such as hand-held (HAND) compared to standard mobile units (STAND) or between portable units and conventional ultrasound performed by sonographers or other experts.
Overall, there were conclusive benefits from the use of POCUS in a variety of clinical contexts. In the ED, it has been found that focussed assessment with sonography in trauma (FAST) had 81% sensitivity for detection of free intra-abdominal fluid in blunt trauma and 63% sensitivity in penetrating injuries, while the specificity was 100%.6 Also in the ED setting, Amatya et al43 concluded that lung ultrasound had a better sensitivity and specificity than plain chest radiographs, while in the studies by Chavez et al41 lung ultrasound performed by GPs using a standardised protocol had 70% sensitivity and 60% specificity.
Changes to patient management pathways was also used as an outcome measure in some studies,29,44–49 as confirmation or a change in diagnosis has potential to alter treatment and disposition of patients. Again, the findings of the individual studies are given in Table 4; however, it was found that POCUS contributed to diagnosis and management in as much as 87%32 or changed the final disposition of patients in up to 65% of cases.44
Various methods were used to assess the quality and accuracy of examinations and in most studies (17/23) images were assessed by experts. In other studies, such as that by Pontet et al.31 POCUS was performed to monitor ventilated patients in ICU, with scans performed by an intensive care physician, so diagnosis and image quality were less relevant, with the emphasis instead on changes in patient condition in comparison to initial imaging on admission to ICU. The expertise in several studies involved follow-up scans performed by sonographers using more sophisticated ultrasound equipment, which common in the screening studies, and interpretation of images by expert trainers, clinical specialists or sonologists. Nixon et al32 used experts to evaluate diagnostic image quality and according to those experts the rural generalist doctors who performed the POCUS examinations correctly interpreted 90% of the images compared with formal imaging or the final diagnosis.
Discussion
The aim of this review was to investigate the use of portable ultrasound imaging devices in under-resourced healthcare contexts, particular where comparisons may be drawn to rural and remote healthcare settings in Australia, the country of origin of the review. The study was motivated by, firstly, a perception that the use of ultrasound performed by non-sonographers has proliferated in recent times and, secondly, that ultrasound has potential to appreciably increase diagnostic capabilities in locations where service access and availability is limited and, thus, improve patient outcomes. In fact, only one of the studies included in this review was performed in Australia,38 although others were performed in other developed countries. Most of the studies were performed in under-resourced settings in developing countries. The challenges facing low-resource settings in healthcare transcend country borders, however, with accessibility and resource constraints being a general limitation to health outcomes for populations in poorly resourced regions of the world.50 The lack of evidence for the use of POCUS in rural and remote Australia may be reflective of a lack of research in this field, rather than a lack of the use of ultrasound in diagnosis. It is, therefore, suggested that future research should explore questions related to the use the POCUS in rural and remote areas of Australia and other developed countries, in order to fill the apparent gap in the literature.
As in Figure 2, a wide variety of ultrasound examination types are performed using POCUS in the settings included in this review, often using prescribed protocols and targeting particular conditions. Cardiac examinations were the most common, particular echocardiographic screening studies, although cardiac scans were also performed emergency departments for various patient presentations. Screening studies were mainly performed in developing countries, with examinations performed by non-expert operators, and were aimed at early detection of cardiac abnormalities in school children, generally using a focused scanning protocol to detect morphological and physiological changes related to rheumatic heart disease.51 One of the echocardiographic screening studies was performed in Australia, confirming health disparities between the at risk young Indigenous population and a non-Indigenous urban population.38 Another screening study performed in a developed country involved scans performed in a GP clinic in rural Canada by appropriately trained health professionals and intended to confirm or exclude abdominal aortic aneurysms in an older adult population.33 These screening studies and the use of limited, focused scanning protocols demonstrated the potential use of POCUS as a tool for early detection of disease, thus avoiding late-stage diagnosis, a recognised problem in rural areas where access is limited, though principally in relation to cancer diagnosis rather than other conditions.52
Other than cardiac examinations, lung ultrasound and FAST or eFAST scans were also common in emergency departments, in particular for confirming or excluding the presence of lung consolidation and intrathoracic or intra-abdominal fluid collections, particularly in trauma management.53 The evidence supports the use of POCUS in emergency departments to increase confidence in the diagnosis, expedite treatment, to better target patient disposition for definitive care, and for better allocation of resources. Similarly, in other critical care settings, such as in the ICU, the use of ultrasound as a monitoring tool can improve patient outcomes and overall resource allocation.31 Though performed in metropolitan ICUs, other studies support the finding that POCUS has important applications in monitoring, diagnosis and procedural guidance in critical care.54
Ultrasound technology is evolving rapidly, including increasingly sophisticated telemedicine applications17,18,55 and the use of artificial intelligence (AI) and automated machine learning.56 These new applications include real-time, remote image guidance and volume sweep imaging (VSI),19,57,58 with standardisation of scanning protocols and measurements.59,60 Such technological advances, together with wider availability of low cost, hand-held ultrasound equipment, promise to increase the access to ultrasound for a variety of non-expert users.61,62 The advances may be of benefit in low-resource, rural and remote health care settings,19 provided high quality of examinations and standards of care are assured.
While in some of the studies included in this review expert sonographers performed the examinations, in many of the studies the operators performing the scans were non-sonographers who had undergone training in a particular examination type and were following a given protocol. In several cases, those operators were working beyond their traditional health professional scope of practice, which may be a way to bridge the gap in low resource settings, where ultrasound services provided by a sonographer may be unavailable. This raises issues about the perceived need to clearly defined practice roles and boundaries, as acknowledged in the cases of other extended scope of practice roles.63 Patient safety is of paramount importance and, while ultrasound is a safe imaging modality with no known adverse effects, unless high exposure levels occur,64 diagnostic accuracy is still an important consideration.
Studies included in this review used various means to ensure the quality of the examinations was adequate for diagnosis, such as training regimens, adherence to protocols, or having guidance by expert trainers or other senior health professionals. Nevertheless, a variety of problems can occur if regular equipment maintenance and quality control testing is not carried out, which can compromise diagnostic accuracy.7 In some studies, particularly screening studies, a second examination was performed by an experienced sonographer on a standard ultrasound device to confirm the diagnosis and ensure optimum quality images were produced. Previously published review articles have found that legal actions related to the use of POCUS had only been brought against emergency physicians where they had failed to perform an ultrasound examination that was within scope in a timely manner.65,66 No legal actions related to malpractice or misdiagnosis when using POCUS were found in this review.
This review has found that portable ultrasound has a wide range of uses in rural and remote, low-resource settings. In the studies reviewed, POCUS was performed a range of health care settings, including emergency departments, GP clinics, schools, a helicopters retrieval service, and in the medical station at a music festival, demonstrating the versatility and flexibility of the equipment used. Patient outcomes across the studies were generally improved, with clinical information gained through early diagnosis of conditions in emergency care or screening studies. It is concluded that, in locations where there is limited access to diagnostic ultrasound examinations performed by sonographers or medical specialists, the use of limited ultrasound examinations performed by non-sonographers on small portable machines, including hand-held devices, has potential to improve diagnostic accuracy and patient care, as well as the overall health outcomes of under-resourced communities, including in rural and remote areas of Australia and other developed countries.
While non-sonographer ultrasound performed on small portable units is prevalent in many high-resource, urban healthcare settings, anecdotally, its use in low-resource settings in Australia is less common. Its increased use may be a step toward better healthcare equity of access between urban and rural populations. This may be increasingly the case as the technology continues to advance; however, this progress must be accompanied by some caveats in order to ensure that rural communities are not exposed to poor practice. Primarily, it is recommended that limited ultrasound practice is specific to certain examination types that are relevant to community needs, and that the education and training programs are of high quality. Practice should be regularly monitored, with practitioners required to undertake recurrent assessment of their competency to perform ultrasound, as well as regular quality control monitoring of equipment and image quality. If such measures are in place, POCUS may become a key component of diagnosis in rural healthcare.
Strengths and Limitations of This Review
Though this review has shed light on the widespread use of POCUS in under-resourced health care settings and the wide range of examination types performed, a large number of the studies lacked consistency and reliability in terms of the outcome variables evaluated. While comprehensive, the lack of consistency in study type did not lend itself to a more detailed meta-analysis. Overall, the quality of the studies extracted was low, as indicated in the risk of bias table. There were only two studies fitting the inclusion criteria that involved some form of randomisation. Self-reporting of outcome measures was common and there was minimal blinding of participants, as blinding is not possible when the physicians assessing patients clinically were themselves performing the ultrasound examinations. On the issue of self-reporting the authors of one of the studies commented that their research would ‘be expected to underestimate the actual impact of POCUS’, as the providers were likely to be influenced by “pre-ultrasound diagnostic impression consistent with ultrasound findings”.45 In another study, the authors acknowledged that because the physicians knew that research was underway, they may have been inclined to respond favourable about the diagnostic value of the ultrasound examinations.47
A key strength of this review, however, is the depth of the searches, with articles extracted across seven databases, as well as being sourced through bibliographical and grey literature searches. This provides certainty about the scope of the search strategy and is beyond the search parameters used in other literature reviews found on related topics. It should also be noted, however, that only studies reported in English language were included in the review so some relevant studies published in other languages may have overlooked.
Conclusions
Very little research was found about the use of POCUS that was directly relevant to the Australian rural and remote healthcare experience, necessitating extrapolation of the findings of studies performed in other countries and locations where the health system is under-resourced. The variety of papers found from across the world indicates the vast array of settings in which portable ultrasound is used, and the reported improvements to patient management and health outcomes as a result of the implementation of POCUS. Although there are various studies demonstrating the accessibility, utility and importance of POCUS in low-resource settings, there is a need for more high-quality research to investigate both the benefits and risks of this valuable diagnostic tool. In rural and remote locations in Australia, as well as in other countries where distance from mainstream health services is a serious problem, technological developments have potential to lessen the negative impact of some healthcare access and availability issues. It is highly probable that technology will evolve even further and that small portable and hand-held ultrasound units will be available for use by an increasingly wide variety of users. Practitioners may be encouraged to adopt innovative technological solutions; however, implementation should be informed by sound research evidence.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kane D, Grassi W, Sturrock R, Balint PV. A brief history of musculoskeletal ultrasound: ‘From bats and ships to babies and hips’. Rheumatology. 2004;43(7):931–933. doi:10.1093/rheumatology/keh004
2. Wright J, Noriega O, Ho H. The application of hand-held ultrasound scanner in teaching of telemedicine and rural medicine. Donald School J Ultrasound Obstet Gynecol. 2014;8(1):87–91. doi:10.5005/jp-journals-10009-1340
3. Wise J. Everyone’s a radiologist now. BMJ. 2008;336(7652):1041–1043. doi:10.1136/bmj.39560.444468.AD
4. Moore CL, Copel JA. Point-of-care ultrasonography. N Engl J Med. 2011;364(8):749–757. doi:10.1056/NEJMra0909487
5. Smallwood N, Dachsel M. Point-of-care ultrasound (POCUS): unnecessary gadgetry or evidence-based medicine? Clin Med. 2018;18(3):219–224. doi:10.7861/clinmedicine.18-3-219
6. Smith ZA, Postma N, Wood D. FAST scanning in the developing world emergency department. S Afr Med J. 2010;100(2):
7. Nixon G, Blattner K, Muirhead J, Finnie W, Lawrenson R, Kerse N. Scope of point-of-care ultrasound practice in rural New Zealand. J Prim Health Care. 2018;10(3):224–236. doi:10.1071/HC18031
8. World Health Organisation (WHO). Increasing Access to Health Workers in Remote and Rural Areas Through Improved Retention: Global Policy Recommendations. Geneva: WHO; 2010.
9. World Bank Group. Rural population (% of total population). World Bank; 2020. Available from: https://data.worldbank.org/indicator/SP.RUR.TOTL.ZS?end=2020&start=2020&view=bar.
10. Australian Institute of Health and Welfare (AIHW). Rural & remote health. AIHW, Australian Government; 2019. Available from: https://www.aihw.gov.au/reports/rural-remote-australians/rural-remote-health.
11. Australian Institute of Health and Welfare (AIHW). Allied health workforce 2012. AIHW, Australian Government; 2013. Available from: https://www.aihw.gov.au/reports/workforce/allied-health-workforce-2012/summary.
12. Beks H, Walsh S, Alston L, et al. Approaches used to describe, measure and analyze place of practice in dentistry, medical, nursing and allied health rural graduate workforce research in Australia: a systematic scoping review. Int J Environ. 2022;19(3):1438.
13. Australian Government Department of Health. Stronger rural health strategy. department of health; 2019. Available from: https://www.health.gov.au/health-topics/rural-health-workforce/stronger-rural-health-strategy?utm_source=health.gov.au&utm_medium=callout-auto-custom&utm_campaign=digital_transformation.
14. National Rural Health Alliance (NRHA). Medical practitioners in rural, regional & remote Australia. NRHA; 2019. Available from: https://www.ruralhealth.org.au/.
15. Luntsi G, Ugwu AC, Nkubli FB, Emmanuel R, Ochie K, Nwobi CI. Achieving universal access to obstetric ultrasound in resource constrained settings: a narrative review. Radiography. 2020;27(2):709–715. doi:10.1016/j.radi.2020.10.010
16. Kim ET, Singh K, Moran A, Armbruster D, Kozuki N. Obstetric ultrasound use in low and middle income countries: a narrative review. Reprod Health. 2018;15(1):15. doi:10.1186/s12978-018-0460-4
17. Marsh-Feiley G, Eadie L, Wilson P. Telesonography in emergency medicine: a systematic review. PLoS One. 2018;13(5):5. doi:10.1371/journal.pone.0194840
18. Salerno A, Tupchong K, Verceles AC, McCurdy MT. Point-of-care teleultrasound: a systematic review. Telemed J E Health. 2020;26(11):1314–1321. doi:10.1089/tmj.2019.0177
19. Britton N, Miller MA, Safadi S, Siegel A, Levine AR, McCurdy MT. Tele-ultrasound in resource-limited settings: a systematic review. Front Public Health. 2019;7:244. doi:10.3389/fpubh.2019.00244
20. Telford LH, Abdullahi LH, Ochodo EA, Zuhlke LJ, Engel ME. Standard echocardiography versus handheld echocardiography for the detection of subclinical rheumatic heart disease: a systematic review and meta-analysis of diagnostic accuracy. BMJ Open. 2020;10(10):10. doi:10.1136/bmjopen-2020-038449
21. Marangou J, Beaton A, Aliku TO, Nunes MCP, Kangaharan N, Remenyi B. Echocardiography in indigenous populations and resource poor settings. Heart Lung Circ. 2019;28(9):1427–1435. doi:10.1016/j.hlc.2019.05.176
22. Becker DM, Tafoya CA, Becker SL, Kruger GH, Tafoya MJ, Becker TK. The use of portable ultrasound devices in low- and middle-income countries: a systematic review of the literature. Trop Med Int Health. 2016;21(3):294–311. doi:10.1111/tmi.12657
23. Sippel S, Muruganandan K, Levine A, Shah S. Review article: use of ultrasound in the developing world. Int J Emerg Med. 2011;4(1):72. doi:10.1186/1865-1380-4-72
24. Groen RS, Leow JJ, Sadasivam V, Kushner AL. Review: indications for ultrasound use in low- and middle-income countries. Trop Med Int Health. 2011;16(12):1525–1535. doi:10.1111/j.1365-3156.2011.02868.x
25. Higgins JPT, Thomas J, Chandler J, et al. Cochrane handbook for systematic reviews of interventions version 6.2. Cochrane; 2021. Available from: www.training.cochrane.org/handbook.
26. Page MJ, McKenzie JE, Bossuyt PM, et al. 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:71. PMID: 33782057; PMCID: PMC8005924. doi:10.1136/bmj.n71
27. Pollock A, Berge E. How to do a systematic review. Int J Stroke. 2018;13(2):138–156. doi:10.1177/1747493017743796
28. Sterne JAC, Savović J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898. PMID: 31462531. doi:10.1136/bmj.l4898
29. Ketelaars R, Hoogerwerf N, Scheffer GJ. Prehospital chest ultrasound by a Dutch helicopter emergency medical service. J Emerg Med. 2013;44(4):811–817. doi:10.1016/j.jemermed.2012.07.085
30. Ploutz M, Lu JC, Scheel J, et al. Handheld echocardiographic screening for rheumatic heart disease by non-experts. Heart. 2016;102(1):35–39. doi:10.1136/heartjnl-2015-308236
31. Pontet J, Yic C, Díaz-Gómez JL, et al. Impact of an ultrasound-driven diagnostic protocol at early intensive-care stay: a randomized-controlled trial. Ultrasound J. 2019;11(1):24. PMID: 31595353; PMCID: PMC6783485. doi:10.1186/s13089-019-0139-2
32. Nixon G, Blattner K, Koroheke-Rogers M, et al. Point-of-care ultrasound in rural New Zealand: safety, quality and impact on patient management. Aust J Rural Health. 2018;26(5):342–349. PMID: 30303278. doi:10.1111/ajr.12472
33. Blois B. Office-based ultrasound screening for abdominal aortic aneurysm. Can Fam Physician. 2012;58(3):e172–e178.
34. Beaton A, Aliku T, Okello E, et al. The utility of handheld echocardiography for early diagnosis of rheumatic heart disease. J Am Soc Echocardiogr. 2014;27(1):42–49. PMID: 24183541. doi:10.1016/j.echo.2013.09.013
35. Beaton A, Lu JC, Aliku T, et al. The utility of handheld echocardiography for early rheumatic heart disease diagnosis: a field study. Eur Heart J Cardiovasc Imaging. 2015;16(5):475–482. PMID: 25564396; PMCID: PMC4542771. doi:10.1093/ehjci/jeu296
36. Godown J, Lu JC, Beaton A, et al. Handheld echocardiography versus auscultation for detection of rheumatic heart disease. Pediatrics. 2015;135(4):e939–44. PMID: 25780068. doi:10.1542/peds.2014-2774
37. Lu JC, Sable C, Ensing GJ, et al. Simplified rheumatic heart disease screening criteria for handheld echocardiography. J Am Soc Echocardiogr. 2015;28(4):463–469. doi:10.1016/j.echo.2015.01.001
38. Roberts K, Maguire G, Brown A, et al. Echocardiographic screening for rheumatic heart disease in high and low risk Australian children. Circulation. 2014;129(19):1953–1961. doi:10.1161/CIRCULATIONAHA.113.003495
39. Singh S, Bansal M, Maheshwari P, et al. American society of echocardiography: remote echocardiography with web-based assessments for referrals at a distance (ASE-REWARD) Study. J Am Soc Echocardiogr. 2013;26(3):221–233. doi:10.1016/j.echo.2012.12.012
40. Bhavnani SP, Sola S, Adams D, Venkateshvaran A, Dash PK, Sengupta PP. A randomized trial of pocket-echocardiography integrated mobile health device assessments in modern structural heart disease clinics. JACC Cardiovasc Imaging. 2018;11(4):546–557. doi:10.1016/j.jcmg.2017.06.019
41. Chavez MA, Naithani N, Gilman RH, et al. Agreement between the world health organization algorithm and lung consolidation identified using point-of-care ultrasound for the diagnosis of childhood pneumonia by general practitioners. Lung. 2015;193(4):531–538. PMID: 25921013. doi:10.1007/s00408-015-9730-x
42. Dalmacion GV, Reyles RT, Habana AE, et al. Handheld ultrasound to avert maternal and neonatal deaths in 2 regions of the Philippines: an iBuntis® intervention study. BMC Pregnancy Childbirth. 2018;18(1):32. PMID: 29347926; PMCID: PMC5774122. doi:10.1186/s12884-018-1658-8
43. Amatya Y, Rupp J, Russell FM, Saunders J, Bales B, House DR. Diagnostic use of lung ultrasound compared to chest radiograph for suspected pneumonia in a resource-limited setting. Int J Emerg Med. 2018;11(1):1. doi:10.1186/s12245-018-0170-2
44. Kissoon DV, Jagjit SD, Bales BD, Luke-Blyden Z, Boyd JS, Rupp JD. Observational descriptive study of ultrasound use and its impact on clinical decisions in the accident and emergency department at Georgetown public hospital corporation. PLoS One. 2020;15(5):e0233379. doi:10.1371/journal.pone.0233379
45. Reynolds TA, Amato S, Kulola I, Chen C-J-J, Mfinanga J, Sawe HR. Impact of point-of-care ultrasound on clinical decision-making at an urban emergency department in Tanzania. PLoS One. 2018;13(4):e0194774. doi:10.1371/journal.pone.0194774
46. Baker DE, Nolting L, Brown HA. Impact of point-of-care ultrasound on the diagnosis and treatment of patients in rural Uganda. Trop Dr. 2021;2021:49475520986425.
47. Prager R, Sedgwick C, Lund A, et al. Prospective evaluation of point-of-care ultrasound at a remote, multi-day music festival. Prehosp Disaster Med. 2018;33(5):484–489. doi:10.1017/S1049023X18000821
48. Umuhire OF, Henry MB, Levine AC, Cattermole GN, Henwood P. Impact of ultrasound on management for dyspnea presentations in a Rwandan emergency department. Ultrasound J. 2019;11(1):18. doi:10.1186/s13089-019-0133-8
49. Zanatta M, Benato P, De Battisti S, Pirozzi C, Cianci V. Point-of-care critical ultrasound in a rural emergency department. Emerg Care J. 2015;11(2):26–31. doi:10.4081/ecj.2015.5017
50. Strasser R. Rural health around the world: challenges and solutions. Fam Pract. 2003;20(4):457–463. PMID: 12876121. doi:10.1093/fampra/cmg422
51. Mirabel M, Bacquelin R, Tafflet M, et al. Screening for rheumatic heart disease: evaluation of a focused cardiac ultrasound approach. Circ Cardiovasc Imaging. 2015;8(1):e002324. doi:10.1161/CIRCIMAGING.114.002324
52. Zhou K, Pickering TA, Gainey CS, et al. Presentation, management, and outcomes across the rural-urban continuum for hepatocellular carcinoma. JNCI Cancer Spectr. 2021;5(1):pkaa100. doi:10.1093/jncics/pkaa100
53. Netherton S, Milenkovic V, Taylor M, Davis PJ. Diagnostic accuracy of eFAST in the trauma patient: a systematic review and meta-analysis. CJEM. 2019;21(6):727–738. PMID: 31317856. doi:10.1017/cem.2019.381
54. Zieleskiewicz L, Muller L, Lakhal K, et al. CAR’Echo and AzuRea Collaborative Networks. Point-of-care ultrasound in intensive care units: assessment of 1073 procedures in a multicentric, prospective, observational study. Intensive Care Med. 2015;41(9):1638–1647. PMID: 26160727. doi:10.1007/s00134-015-3952-5
55. Dougherty A, Kasten M, DeSarno M, et al. Validation of a telemedicine quality assurance method for point-of-care obstetric ultrasound used in low-resource settings. J Ultrasound Med. 2021;40(3):529–540. PMID: 32770709. doi:10.1002/jum.15429
56. Seetharam K, Kagiyama N, Sengupta PP. Application of mobile health, telemedicine and artificial intelligence to echocardiography. Echo Res Pract. 2019;6(2):R41–R52. doi:10.1530/ERP-18-0081
57. Ferrer J, Chaumont T, Trujillo L, et al. New tele-diagnostic model using volume sweep imaging for rural areas. Annu Int Conf IEEE Eng Med Biol Soc. 2017;2017:2622–2625. PMID: 29060437. doi:10.1109/EMBC.2017.8037395
58. Marini TJ, Oppenheimer DC, Baran TM, et al. New ultrasound telediagnostic system for low-resource areas: pilot results from Peru. J Ultrasound Med. 2021;40(3):583–595. PMID: 32798267. doi:10.1002/jum.15420
59. Saavedra AC, Arroyo J, Tamayo L, Egoavil M, Ramos B, Castaneda B. Automatic ultrasound assessment of placenta previa during the third trimester for rural areas. IEEE Int Ultrason Symp. 2020;1–4. doi:10.1109/IUS46767.2020.9251764
60. van den Heuvel TLA, Petros H, Santini S, de Korte CL, van Ginneken B. Automated fetal head detection and circumference estimation from free-hand ultrasound sweeps using deep learning in resource-limited countries. Ultrasound Med Biol. 2019;45(3):773–785. doi:10.1016/j.ultrasmedbio.2018.09.015
61. Burleson SL, Swanson JF, Shufflebarger EF, et al. Evaluation of a novel handheld point-of-care ultrasound device in an African emergency department. Ultrasound J. 2020;12(1):53. PMID: 33284368; PMCID: PMC7721766. doi:10.1186/s13089-020-00200-8
62. Baribeau Y, Sharkey A, Chaudhary O, et al. Handheld point-of-care ultrasound probes: the new generation of POCUS. J Cardiothorac Vasc Anesth. 2020;34(11):3139–3145. PMID: 32736998; PMCID: PMC7340048. doi:10.1053/j.jvca.2020.07.004
63. Smith T, McNeil K, Mitchell R, Boyle B, Ries N. A study of macro-, meso- and micro-barriers and enablers affecting extended scopes of practice: the case of rural nurse practitioners in Australia. BMC Nurs. 2019;18(1):14. doi:10.1186/s12912-019-0337-z
64. Izadifar Z, Babyn P, Chapman D. Mechanical and biological effects of ultrasound: a review of present knowledge. Ultrasound Med Biol. 2017;43(6):1085–1104. doi:10.1016/j.ultrasmedbio.2017.01.023
65. Blaivas M, Pawl R. Analysis of lawsuits filed against emergency physicians for point-of-care emergency ultrasound examination performance and interpretation over a 20-year period. Am J Emerg Med. 2012;30(2):338–341. doi:10.1016/j.ajem.2010.12.016
66. Stolz L, O’Brien KM, Miller ML, Winters-Brown ND, Blaivas M, Adhikari S. A review of lawsuits related to point-of-care emergency ultrasound applications. West J Emerg Med. 2015;16(1):1–4. doi:10.5811/westjem.2014.11.23592
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.