Back to Journals » Clinical Ophthalmology » Volume 20
Posture-Induced Intraocular Pressure Changes at Different Times of Day in Primary Open-Angle Glaucoma: Associated Factors and Exploratory Analyses of Antiglaucoma Medication Regimens
Authors Mino T, Udagawa S ![]() , Yamashita Y, Kobayashi A
, Yamashita Y, Kobayashi A ![]() , Higashide T
, Higashide T
Received 18 February 2026
Accepted for publication 29 May 2026
Published 23 June 2026 Volume 2026:20 600670
DOI https://doi.org/10.2147/OPTH.S600670
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 7
Editor who approved publication: Dr Sotiria Palioura
Tsuyoshi Mino, Sachiko Udagawa, Yoko Yamashita, Akira Kobayashi, Tomomi Higashide
Department of Ophthalmology, Kanazawa University Graduate School of Medical Sciences, Kanazawa, Ishikawa, Japan
Correspondence: Tomomi Higashide, Department of Ophthalmology, Kanazawa University Graduate School of Medical Sciences, 13-1 Takara-machi, Kanazawa, Ishikawa, 920-8641, Japan, Tel +81-76-265-2403, Fax +81-76-222-9660, Email [email protected]
Purpose: To compare posture-induced intraocular pressure (IOP) differences at two measurement times in eyes with primary open-angle glaucoma (POAG) and to identify associated factors.
Methods: In this retrospective observational study, 108 eyes of 61 POAG participants receiving antiglaucoma medications were included. Sitting and supine IOP were measured at 9 a.m. and 9 p.m. using the iCare IC200 rebound tonometer. Ocular parameters, including subfoveal choroidal thickness, corneal hysteresis, and systemic parameters, including body mass index and blood pressure, were assessed. Mixed-effects models were used to analyze factors related to posture-induced IOP differences (supine minus sitting IOP).
Results: Posture-induced IOP differences were significantly greater at 9 a.m. (3.5 ± 2.0 mmHg) than at 9 p.m. (2.7 ± 1.7 mmHg; P < 0.001). At 9 a.m. higher sitting IOP (P = 0.010) and greater subfoveal choroidal thickness (P = 0.003) were associated with larger IOP differences. At 9 p.m. lower body mass index (P = 0.005), higher blood pressure (P = 0.004), greater supine blood pressure elevation (P = 0.036), and higher corneal hysteresis (P = 0.017) were associated with larger IOP differences. The presence of any individual antiglaucoma medication class within the topical regimen was not significantly associated with posture-induced IOP differences. However, in exploratory analyses, combination therapy with an α 2-adrenergic agonist and a Rho kinase inhibitor was associated with smaller IOP differences, particularly at 9 a.m. (P = 0.031).
Conclusion: Posture-induced IOP elevation was greater in the morning in POAG eyes. Multiple ocular and systemic factors, including blood pressure–related parameters, contributed to these differences, which varied by measurement time. Analyses of antiglaucoma medication regimens were exploratory, and findings should be interpreted with caution.
Keywords: primary open-angle glaucoma, intraocular pressure, posture, diurnal variation, antiglaucoma medications
Introduction
Intraocular pressure (IOP) varies with body position, and a previous study reported that IOP is higher in the supine position than in the sitting position.1 In eyes with primary open-angle glaucoma (POAG), posture-induced IOP changes are greater than those observed in eyes without glaucoma.2 In normal-tension glaucoma (NTG), the magnitude of IOP elevation in the supine position may also be associated with visual field progression.3 Thus, posture-related IOP fluctuations represent one of the factors that should be considered in the clinical management of glaucoma. Similar IOP elevations have also been documented during postural changes in other contexts, such as head-down yoga exercises, further highlighting the clinical relevance of body-position-related IOP changes.4 Posture-induced IOP elevation has been reported to range from approximately 2 to 6 mmHg in glaucoma patients, with greater elevations observed in NTG compared with high-tension glaucoma or healthy controls.3,5
Several factors influencing posture-induced IOP differences have been reported, including the time of IOP measurement,6 the sitting IOP level,7 the presence of obstructive sleep apnea,8 and a history of glaucoma surgery such as Ahmed glaucoma valve implantation.9 To our knowledge, the possible influence of ocular parameters such as corneal hysteresis and choroidal thickness on posture-related IOP differences has not been systematically investigated in POAG patients. In contrast, the use of individual antiglaucoma medication classes such as latanoprost, timolol, and brinzolamide does not appear to have a significant impact on posture-related IOP differences.10 Our study included POAG patients across the full IOP spectrum, encompassing both high-tension and normal-tension subtypes, although pretreatment IOP was not systematically recorded and most participants had treated IOP levels consistent with NTG. However, it remains unclear which factors are associated with posture-induced IOP differences at different measurement times, and whether other medication classes or combination therapy affects these differences. A clinically relevant question is also whether antiglaucoma medications can sufficiently attenuate the posture-induced IOP rise that occurs during sleep.
In the present study, posture-induced IOP differences were assessed at two time points — 9 a.m. and 9 p.m. — corresponding to the standard clinical schedule used during inpatient diurnal IOP monitoring at our institution. These time points represent two physiologically distinct periods: the morning, when participants are transitioning from nocturnal recumbency to daytime activity, and the evening, when participants are preparing to return to the supine sleeping position. Comparing posture-induced IOP responses between these two time points in a treated POAG population represents a novel aspect of the present study.
To date, no previous study has systematically compared posture-induced IOP differences at different times of day across multiple medication classes and combination regimens in a clinical POAG population, nor identified the factors associated with these differences at each time point. The purpose of the present study was therefore to compare posture-induced IOP differences between sitting and supine positions at 9 a.m. and 9 p.m. in eyes with POAG and to identify clinical factors, including antiglaucoma medication regimens, associated with these differences at each time point.
Methods
Study Design and Participants
This was a retrospective observational study. The study protocol was approved by the Medical Ethics Committee of Kanazawa University Hospital (Approval No. 2013–041) and was conducted in accordance with the tenets of the Declaration of Helsinki. Written informed consent was obtained from all participants prior to enrollment.
Patients with POAG who underwent diurnal IOP fluctuation testing at our hospital between October 2022 and March 2025 were included. POAG was defined as the presence of glaucomatous optic disc appearance with corresponding visual field defects and normal open anterior chamber angles on gonioscopy, regardless of baseline IOP level. Exclusion criteria included: (1) secondary causes of IOP elevation such as pseudoexfoliation or uveitis; (2) history of glaucoma surgery, including laser trabeculoplasty; (3) history of any other intraocular surgery; and (4) presence of ocular diseases such as clinically significant cataract, diabetic retinopathy, age-related macular degeneration, epiretinal membrane, optic nerve, or retinal abnormality that could affect visual fields or measurements of IOP or choroidal thickness. Of the 184 eyes from 96 patients initially screened, 76 eyes from 35 patients were excluded based on these criteria; in some participants, one eye met exclusion criteria while the fellow eye did not. The remaining 108 eyes from 61 participants were included in the final analysis.
IOP and Blood Pressure Measurements
During hospitalization for diurnal IOP monitoring, IOP and blood pressure measurements were performed at two time points: 9 a.m. and 9 p.m. At each time point, measurements were obtained in both the sitting and supine positions following a standardized protocol.
For sitting measurements, patients were asked to sit quietly for 5 minutes, after which systemic blood pressure was measured using an automated sphygmomanometer, preferentially on the right arm. In participants for whom right-arm measurement was contraindicated (eg, history of breast cancer surgery), the left arm was used; the same arm was consistently used for all measurements throughout the study. Following an additional 5 minutes of rest, IOP was measured using the iCare IC200 rebound tonometer (iCare Finland Oy, Finland). For supine measurements, patients were then positioned supine and allowed to rest for 5 minutes before blood pressure measurement, followed by an additional 5 minutes of rest (10 minutes total from the onset of the supine position) before IOP measurement. At each time point, IOP was measured first in the supine position using the iCare IC200, followed by IOP measurement in the sitting position using the iCare IC200, then corneal hysteresis measurement using the Ocular Response Analyzer (ORA) in the sitting position, and finally Goldmann applanation tonometry (GAT) in the sitting position, as GAT cannot be performed in the supine position. This sequence was standardized across all participants and time points. Three consecutive IOP readings were obtained at each measurement, and the mean value was used for analysis. IOP measurements were performed by trained orthoptists and ophthalmologist as part of the standardized clinical protocol. Within each session, measurements were performed by a single examiner for each participant. Examiners were not formally masked to prior IOP readings, as this was a retrospective clinical study.
Mean arterial pressure (MAP) was calculated as: MAP = diastolic pressure + (systolic pressure − diastolic pressure) / 3.
Ocular and Systemic Parameters
Comprehensive ophthalmic examinations were performed, including best-corrected visual acuity (BCVA), slit-lamp biomicroscopy, gonioscopy, dilated fundus examination, and visual field testing using the Humphrey Field Analyzer (Carl Zeiss Meditec, Dublin, CA, USA) with the Swedish Interactive Threshold Algorithm standard 24–2 program. The mean deviation (MD) value was recorded.
GAT was performed at 9 a.m. and 9 p.m. during hospitalization as part of standardized diurnal IOP assessment. Central corneal thickness (CCT) was measured using anterior segment optical coherence tomography (AS-OCT) (CASIA2; TOMEY, Japan). Corneal hysteresis (CH) was measured using the Ocular Response Analyzer (Reichert Inc., USA) once during the morning session (at 9 a.m.). Axial length and anterior chamber volume were measured using optical biometry using OA-2000 (TOMEY, Japan).
Subfoveal choroidal thickness was measured using enhanced depth imaging optical coherence tomography (RS-3000 Advance; NIDEK Co., Ltd., Gamagori, Japan). Horizontal and vertical scans centered on the fovea were obtained, and choroidal thickness was manually measured as the perpendicular distance from the outer border of the retinal pigment epithelium to the inner surface of the sclera. The mean of the horizontal and vertical measurements was used for analysis. Subfoveal choroidal thickness was measured once during the afternoon of the outpatient visit conducted in the week prior to hospitalization (typically between 15:00 and 16:30), as part of the same visit at which visual field testing was performed. Circumpapillary retinal nerve fiber layer thickness (cpRNFLT) was automatically measured using a circular scan centered on the optic nerve head.
Body mass index (BMI) was calculated as weight (kg) divided by height squared (m2). Systemic comorbidities and medication use were documented from medical records.
Antiglaucoma Medication Assessment
All antiglaucoma medications were documented at the time of IOP measurement. Medications were classified into six classes: prostaglandin F2α (FP) agonists (latanoprost, travoprost, tafluprost), prostaglandin E2 (EP2) agonists (omidenepag isopropyl), β-adrenergic blockers, carbonic anhydrase inhibitors, α2-adrenergic agonists (brimonidine), and Rho kinase (ROCK) inhibitors (ripasudil). The number of glaucoma medications was calculated as the total number of medication classes used. For analyses of individual drug classes, each medication class was treated as a binary variable (yes/no) based on its inclusion in the patient’s current topical regimen, regardless of concomitant use of other agents. Two-drug combination analyses were performed for all medication classes except EP2 agonists, which were evaluated only as an individual drug class because the number of eyes receiving EP2 agonists in combination therapy was insufficient for stable subgroup analysis. Regarding dosing frequency, prostaglandin F2α agonists and EP2 agonists are typically administered once daily in the evening, whereas β-adrenergic blockers, carbonic anhydrase inhibitors, α2-adrenergic agonists, and ROCK inhibitors are typically administered twice daily. However, the specific timing of the last instillation relative to IOP measurements was not strictly standardized in this retrospective study. Instead, the instillation time was recorded.
Statistical Analysis
Posture-induced IOP difference was defined as the IOP in the supine position minus the IOP in the sitting position at each time point. The primary outcome was the posture-induced IOP difference, and the secondary outcomes were the factors associated with this difference at 9 a.m. and 9 p.m.
Because both eyes of some patients were included, mixed-effects linear regression models were used to account for inter-eye correlation, with patient as a random effect. The association between posture-induced IOP difference and measurement time (9 a.m. vs 9 p.m.) was evaluated using a mixed-effects model with measurement time as a fixed effect.
Multivariate mixed-effects models were constructed separately for 9 a.m. and 9 p.m. to identify factors associated with posture-induced IOP differences. In multivariate analyses, sitting IOP measured by GAT was used as the predictor variable rather than iCare IC200 values, because GAT is considered the gold standard for IOP measurement and provides more reliable assessment of baseline IOP status. Furthermore, inclusion of iCare IC200 sitting IOP values could potentially result in mathematical coupling, as sitting IOP constitutes a component of the posture-induced IOP difference. Covariates included as potential confounder were sitting IOP (GAT), number of antiglaucoma medication classes, age, BMI, sitting heart rate, sitting MAP, increase in MAP from sitting to supine position, change in heart rate from sitting to supine position, CCT, CH, anterior chamber volume, axial length, and subfoveal choroidal thickness.
The effect of antiglaucoma medications on posture-induced IOP difference was analyzed using mixed-effects models adjusted for sitting IOP (GAT), measurement time, number of medication classes, BMI, sitting MAP, increase in MAP from sitting to supine, CH, and subfoveal choroidal thickness. Both individual drug classes (presence vs. absence within the topical regimen) and two-drug combinations were evaluated. For medication combinations showing significant associations, additional time-stratified analyses (9 a.m. and 9 p.m. separately) were performed using simplified mixed-effects models adjusted for key covariates (sitting IOP [GAT], number of medication classes, and subfoveal choroidal thickness) to avoid model overfitting in the setting of reduced sample sizes. All analyses of individual drug classes and two-drug combinations were exploratory, and no adjustment for multiple comparisons was applied; results should be interpreted accordingly.
To assess multicollinearity among covariates, pairwise correlation coefficients and variance inflation factors (VIF) were calculated prior to multivariate modeling. The absolute values of all pairwise correlation coefficients were below 0.6 (maximum |r| = 0.584, between axial length and anterior chamber volume), and all VIF values were below 3.0 (range 1.35–2.70; mean VIF = 1.78), indicating no substantial multicollinearity among the independent variables. These results are presented in Supplementary Table S2. Two pre-specified sensitivity analyses were performed. First, to address the potential confounding effect of antiglaucoma medication instillation timing, participants for whom instillation times were uncertain and cases in which eye drops were administered after the respective IOP measurement time point (after 9 a.m. for the morning session or after 9 p.m. for the evening session) were excluded, and the main analyses were repeated. Second, to examine the influence of the severity of functional or structural damage on posture-induced IOP differences measured at 9 a.m. and 9 p.m., two additional multivariate mixed-effects models were constructed by separately incorporating the visual field MD and the cpRNFLT as additional covariates, each in independent models.
All statistical analyses were performed using Stata software (version 18.0; StataCorp LLC, College Station, TX, USA). Two-sided P values and 95% confidence intervals were obtained from the model output, and P < 0.05 was considered statistically significant.
Results
Patient Demographics and Clinical Characteristics
A total of 184 eyes from 96 patients were initially screened. Of these, 76 eyes from 35 patients were excluded based on the pre-specified exclusion criteria (secondary causes of IOP elevation, history of glaucoma surgery, history of other intraocular surgery, and presence of ocular diseases affecting visual fields or measurements); in some participants, one eye met exclusion criteria while the fellow eye did not. The remaining 108 eyes from 61 participants were included in the final analysis. The demographic and clinical characteristics of the study population are summarized in Table 1. The mean age was 57.2 ± 10.3 years (range, 34–88 years), and 28 participants (47 eyes) were male. The mean visual field MD value was −11.6 ± 8.16 dB (range, −30.86 to +1.3 dB), indicating a wide range of glaucoma severity. Mean cpRNFLT was 57.4 ± 13.5 μm (range, 25–93 μm). Participants were receiving a mean of 3.44 ± 1.23 antiglaucoma medication classes (range, 1–5).
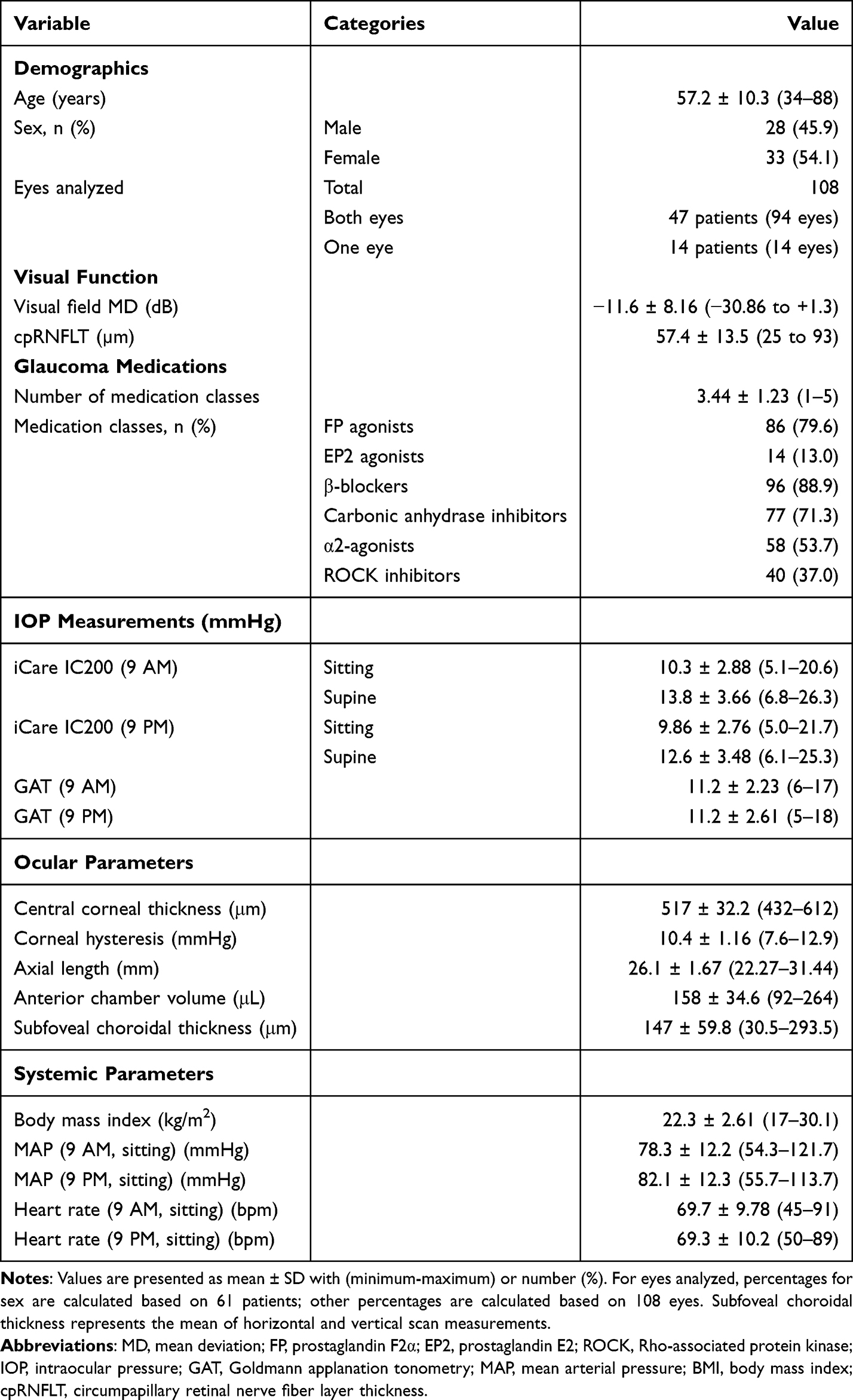 |
Table 1 Demographic and Clinical Characteristics of Study Participants |
Mean sitting IOP measured by iCare IC200 was 10.3 ± 2.88 mmHg at 9 a.m. and 9.86 ± 2.76 mmHg at 9 p.m. Mean supine IOP was 13.8 ± 3.66 mmHg at 9 a.m. and 12.6 ± 3.48 mmHg at 9 p.m. Mean sitting IOP measured by GAT during hospitalization was 11.2 ± 2.23 mmHg at 9 a.m. and 11.2 ± 2.61 mmHg at 9 p.m.
Mean CCT was 517 ± 32.2 μm, mean CH was 10.4 ± 1.16 mmHg, mean axial length was 26.1 ± 1.67 mm, and mean anterior chamber volume was 158 ± 34.6 μL. Mean subfoveal choroidal thickness was 147 ± 59.8 μm. Mean BMI was 22.3 ± 2.61 kg/m2.
Comparison of Posture-Induced IOP Differences Between Measurement Times
The mean posture-induced IOP difference (supine minus sitting IOP) was significantly greater at 9 a.m. than at 9 p.m. (Figure 1). Specifically, the mean posture-induced IOP difference was 3.5 ± 2.0 mmHg (range, −0.5 to +9.0 mmHg) at 9 a.m. and 2.7 ± 1.7 mmHg (range, −2.9 to +8.1 mmHg) at 9 p.m. (P < 0.001, mixed-effects model).
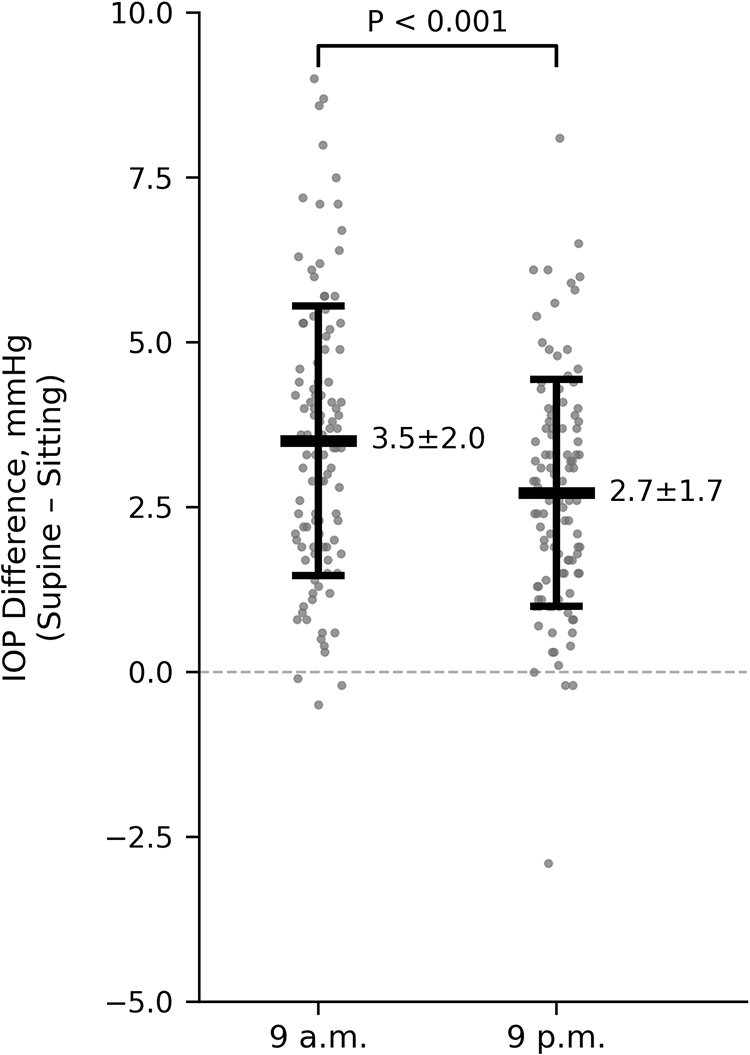 |
Figure 1 Comparison of posture-induced intraocular pressure (IOP) differences between measurement times. Posture-induced IOP differences (supine minus sitting IOP) measured at 9 a.m. and 9 p.m. in eyes with primary open-angle glaucoma. Individual data points are shown with horizontal jitter to reduce overplotting. Horizontal bars indicate the mean, and error bars represent ±1 standard deviation. The mean posture-induced IOP difference was 3.5 ± 2.0 mmHg (range, −0.5 to +9.0 mmHg) at 9 a.m. and 2.7 ± 1.7 mmHg (range, −2.9 to +8.1 mmHg) at 9 p.m. Posture-induced IOP differences were significantly greater at 9 a.m. than at 9 p.m. (mean difference = 0.8 mmHg; 95% CI: 0.4–1.2 mmHg; P < 0.001, mixed-effects linear regression with participant as a random intercept). |
Factors Associated with Posture-Induced IOP Differences at 9 A.m.
Results of the multivariate mixed-effects model for factors associated with posture-induced IOP differences at 9 a.m. are presented in Table 2. Greater subfoveal choroidal thickness (coefficient = 0.01, SE = 0.004, P = 0.003) and higher sitting IOP (coefficient = 0.26, SE = 0.10, P = 0.010) were significantly associated with larger posture-induced IOP differences, corresponding to approximately a 1.0-mmHg increase in posture-induced IOP difference per 100-μm increase in subfoveal choroidal thickness. Other variables were not significantly associated with posture-induced IOP differences at 9 a.m.
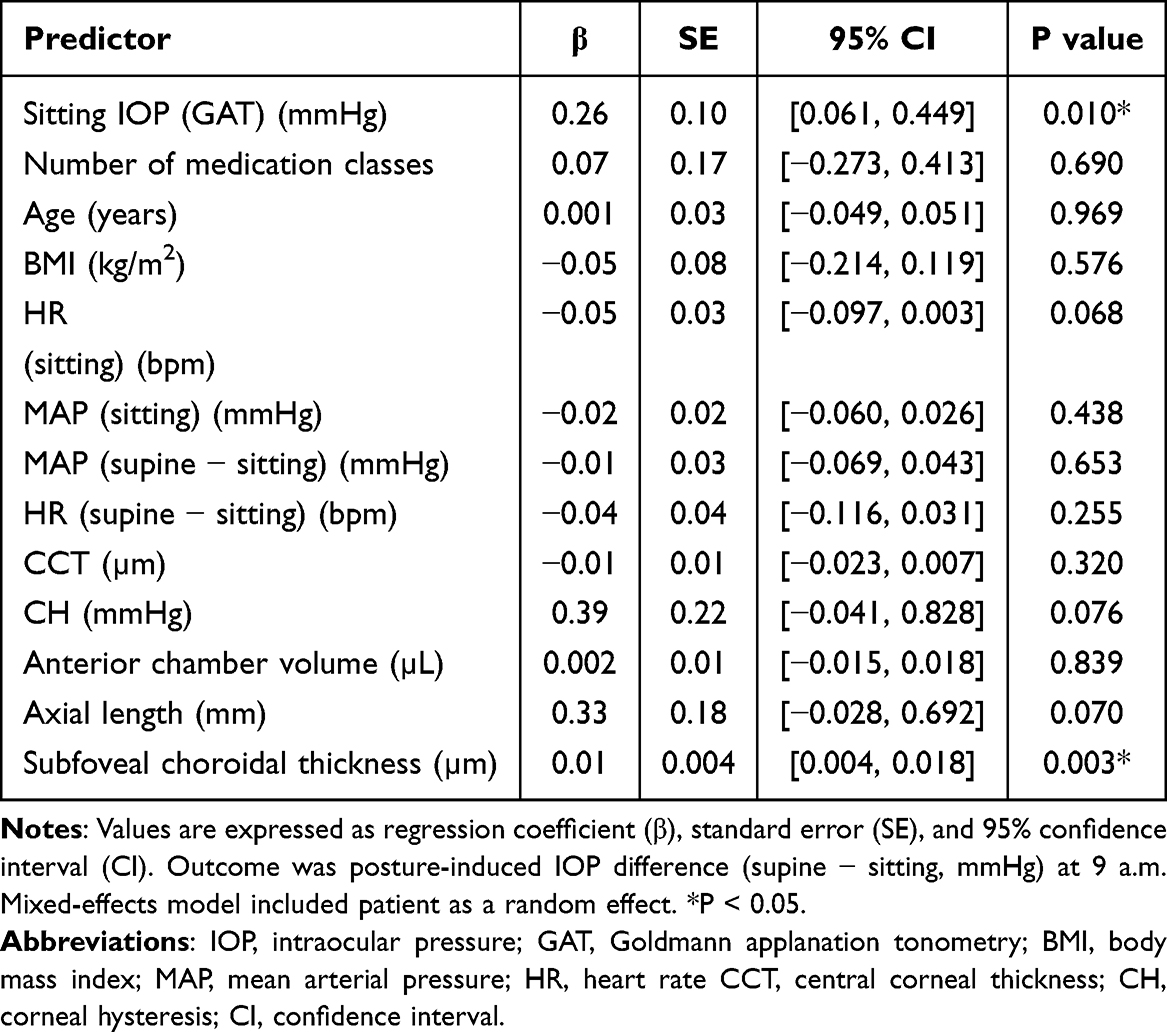 |
Table 2 Multivariate Mixed-Effects Linear Regression for Posture-Induced IOP Differences at 9 a.m. |
Factors Associated with Posture-Induced IOP Differences at 9 P.m.
Results of the multivariate mixed-effects model for factors associated with posture-induced IOP differences at 9 p.m. are presented in Table 3. Lower BMI (coefficient = −0.17, SE = 0.06, P = 0.005), higher sitting MAP (coefficient = 0.05, SE = 0.02, P = 0.004), greater increase in MAP from sitting to supine (coefficient = 0.05, SE = 0.03, P = 0.036), and higher CH (coefficient = 0.40, SE = 0.17, P = 0.017) were significantly associated with larger posture-induced IOP differences. Subfoveal choroidal thickness, which was significant at 9 a.m., was not significantly associated at 9 p.m. (coefficient = 0.003, SE = 0.003, P = 0.317).
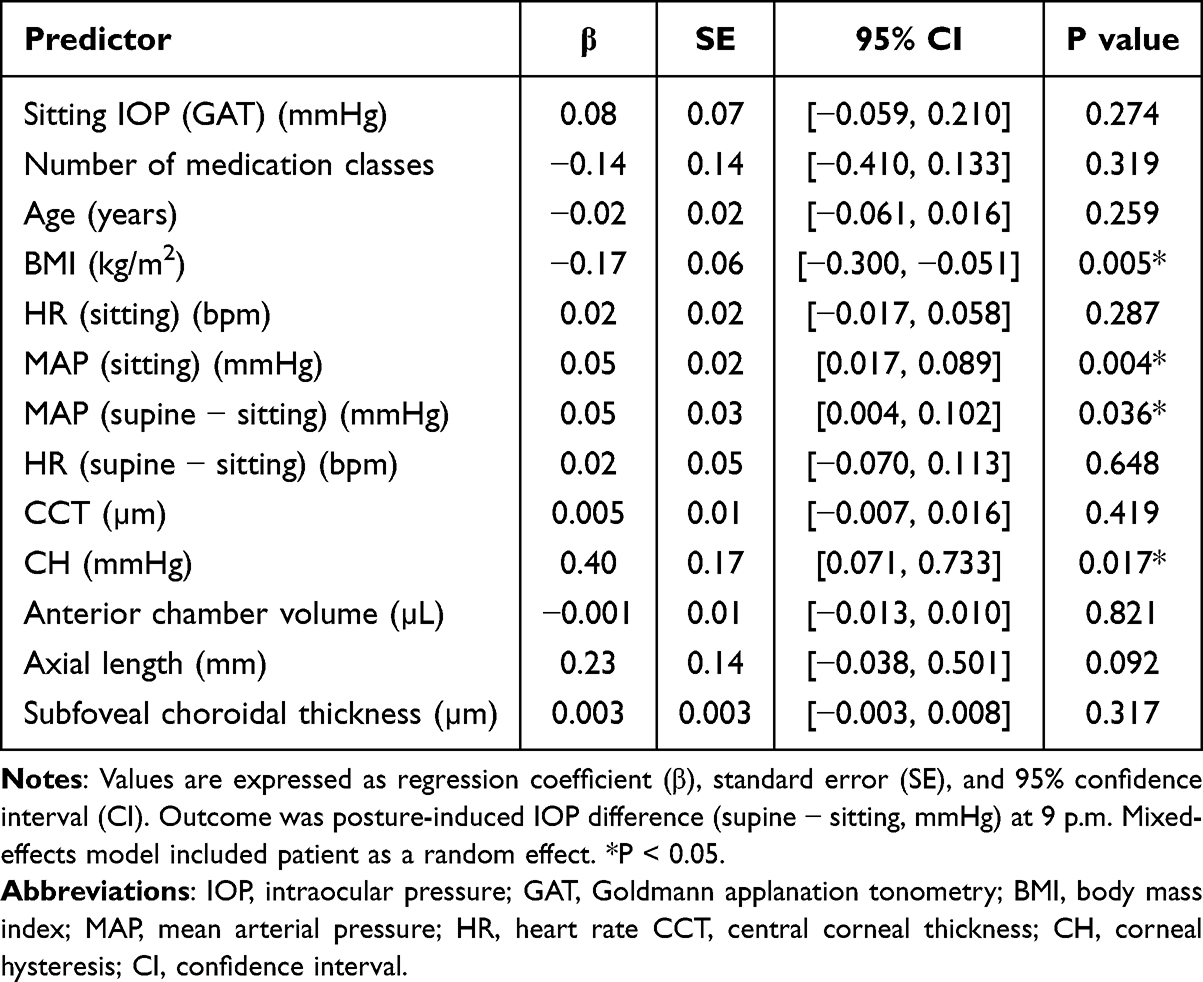 |
Table 3 Multivariate Mixed-Effects Linear Regression for Posture-Induced IOP Differences at 9 p.m. |
Effects of Antiglaucoma Medications on Posture-Induced IOP Differences
Results for individual drug classes and two-drug combinations (defined by the presence of each class/combination within the topical regimen, regardless of concomitant agents) are provided in Supplementary Table S1. In analyses adjusted for potential confounders, the presence of any individual medication class within the topical regimen was not significantly associated with posture-induced IOP differences.
Among two-drug combinations excluding EP2 agonists, only the combination of an α2- adrenergic agonist and a ROCK inhibitor (n = 31 eyes) was associated with significantly smaller posture-induced IOP differences compared with eyes not receiving this combination (n = 77 eyes) (β = −1.06, SE = 0.47, P = 0.023; Table 4). No other two-drug combinations showed significant associations (Supplementary Table S1).
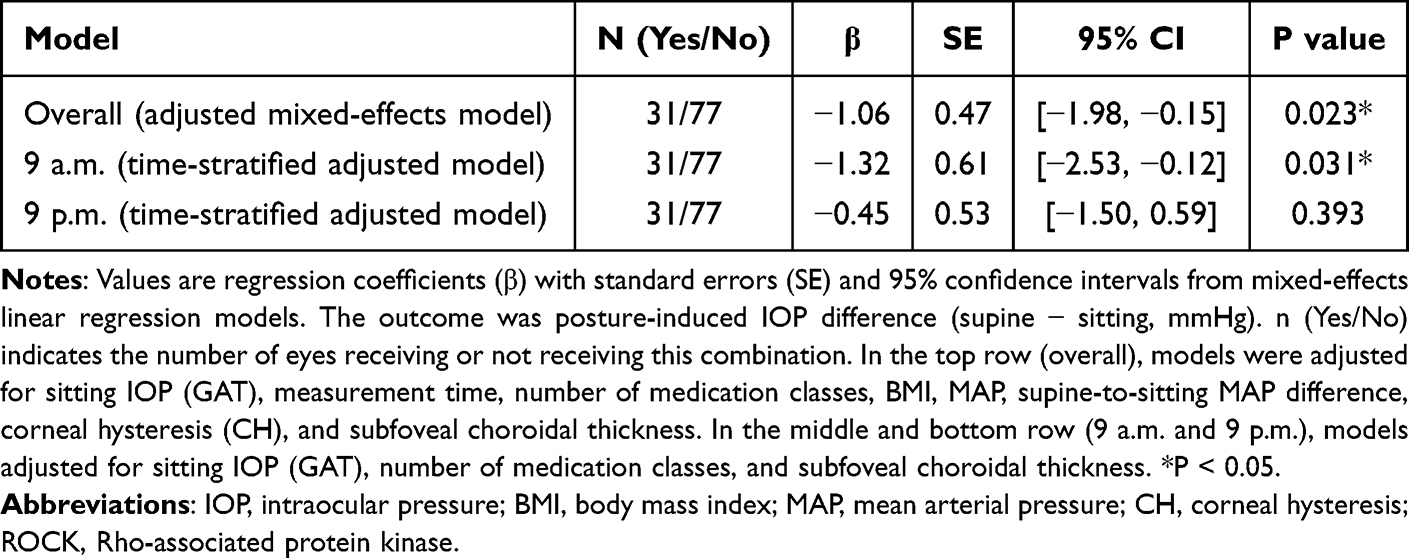 |
Table 4 Association Between Antiglaucoma Medication Regimens and Posture-Induced IOP Differences Two-Drug Combination Therapy (α2-Adrenergic Agonist + ROCK Inhibitor) |
Time-Specific Effects of α2- Adrenergic Agonist and ROCK Inhibitor Combination
Additional time-stratified analyses revealed that the effect of α2- adrenergic agonist plus ROCK inhibitor combination on posture-induced IOP differences was significant at 9 a.m. (β = −1.32, SE = 0.61, P = 0.031) but not at 9 p.m. (β = −0.45, SE = 0.53, P = 0.393), after adjusting for relevant covariates at each time point (Table 4).
Sensitivity Analyses
In the sensitivity analyses examining the influence of disease severity and structural damage, the significant associations in Table 2 and Table 3 remained unchanged in both the model additionally adjusted for visual field MD and the model additionally adjusted for cpRNFLT, indicating robustness of the main findings to glaucoma severity indicators.
In the sensitivity analysis addressing antiglaucoma medication instillation timing, participants with uncertain instillation times and those who received eye drops after the respective IOP measurement time point (after 9 a.m. or after 9 p.m.) were excluded, resulting in 108 eyes of 61 participants for the morning analysis and 104 eyes of 59 participants for the evening analysis. After these exclusions, the significant associations in Tables 2–4 — including the association of the α2-adrenergic agonist plus ROCK inhibitor combination with smaller posture-induced IOP differences — remained unchanged.
Discussion
In this study of 108 eyes from 61 participants with POAG receiving medical treatment, we found that posture-induced IOP differences were significantly greater in the morning (9 a.m.) than in the evening (9 p.m.). This time-dependent difference in posture-induced IOP elevation is illustrated in Figure 1. Furthermore, the factors associated with these IOP differences varied depending on the measurement time. At 9 a.m., higher sitting IOP and greater subfoveal choroidal thickness were associated with larger posture-induced IOP differences, whereas at 9 p.m., lower BMI, higher blood pressure, greater supine blood pressure elevation, and higher corneal hysteresis were the primary associated factors. Regarding antiglaucoma medications, the presence of any individual antiglaucoma medication class within the topical regimen did not materially affect posture-induced IOP differences, but combination therapy with an α2-adrenergic agonist and a ROCK inhibitor was associated with smaller IOP differences, particularly in the morning.
The finding that posture-induced IOP differences were greater at 9 a.m. than at 9 p.m. is consistent with previous reports showing diurnal variation in postural IOP responses.6 Gautam et al6 reported that posture-induced IOP changes were larger at 4:30 a.m. compared with 9:00 a.m. in glaucoma patients, suggesting that the magnitude of postural IOP elevation decreases throughout the day. Although we did not measure IOP during the early morning hours, our findings support the concept of time-dependent modulation of posture-induced IOP changes. These results extend previous work by Gautam et al,6 who examined posture-induced IOP at two time points in a mixed glaucoma population, by providing a more detailed analysis of the clinical and ocular factors associated with these time-dependent differences in a homogeneous treated POAG cohort.
The observation that different factors were associated with posture-induced IOP changes at 9 a.m. versus 9 p.m. warrants mechanistic consideration. At 9 a.m., subfoveal choroidal thickness was the predominant ocular factor, which may reflect diurnal variations in choroidal vascular regulation driven by circadian changes in autonomic nervous system activity and hormonal influences such as cortisol. In contrast, at 9 p.m., blood pressure–related parameters were the primary associated factors, likely reflecting the increasing role of cardiovascular dynamics as participants transition toward the nocturnal supine state. These time-dependent differences in associated factors suggest that the mechanisms underlying posture-induced IOP elevation are not static but vary throughout the day, possibly reflecting the complex interplay between ocular and systemic physiological rhythms. These interpretations remain speculative, however, and require prospective investigation with simultaneous measurement of relevant physiological parameters.
The clinical significance of posture-induced IOP elevation during different times of day warrants consideration. Participants typically spend the longest period in the supine position during nocturnal sleep, making evening measurements (9 p.m.) potentially more relevant for approximating IOP-related conditions during the habitual sleep period. Our finding that multiple blood pressure–related factors (sitting MAP, supine MAP elevation) were associated with posture-induced IOP differences at 9 p.m. suggests that cardiovascular dynamics play an important role in nocturnal IOP regulation, consistent with previous findings demonstrating an association between ambulatory blood pressure and 24-hour IOP-related profiles measured using contact lens sensors in untreated glaucoma patients.11 Previous studies have demonstrated that episcleral venous pressure increases in the supine position due to increased venous return,12,13 and this effect may be modulated by systemic blood pressure changes. Our finding that supine blood pressure–related parameters were associated with posture-induced IOP differences at 9 p.m. raises the hypothesis that participants with higher nocturnal blood pressure — as approximated by evening supine blood pressure — may experience greater IOP elevation during sleep; however, this remains speculative as true nocturnal blood pressure during sleep was not measured in this study. This finding suggests that assessment of blood pressure patterns may be clinically relevant in glaucoma management, particularly in patients with poorly controlled nocturnal IOP.
The inverse association between BMI and posture-induced IOP differences at 9 p.m. was unexpected, as previous studies have reported positive correlations between BMI and IOP.14,15 Geloneck et al14 found that higher BMI was associated with higher IOP in both sitting and supine positions, but reported no significant association between BMI and the posture-induced IOP difference specifically We hypothesize, although without direct supporting evidence from our data, that individuals with lower BMI may have different body fluid distribution patterns or vascular compliance characteristics that result in greater IOP fluctuations with postural change. This hypothesis requires testing in future dedicated studies. From a clinical standpoint, the inverse association with BMI requires further investigation before any clinical recommendations can be made.
At 9 a.m., higher sitting IOP and greater subfoveal choroidal thickness were associated with larger posture-induced IOP differences. The association with sitting IOP level is consistent with previous reports7 and likely reflects a baseline dependency of posture-induced IOP elevation, rather than an independent pathophysiological mechanism. Najmanová et al also reported that the magnitude of posture-induced IOP change was greater in eyes with higher baseline IOP, supporting this interpretation.7 The association with choroidal thickness is particularly interesting, as choroidal thickness is known to vary with posture and time of day.16,17 The choroid has been suggested to play a role in posture-induced IOP changes,18 and alterations in choroidal volume in the supine position may contribute to IOP elevation through mechanical effects on the globe or indirect influences on aqueous humor dynamics. Our finding that choroidal thickness was associated with posture-induced IOP differences only in the morning suggests that choroidal vascular regulation may vary throughout the day, possibly related to diurnal variations in autonomic nervous system activity or hormonal influences. Regarding the clinical significance of the association with choroidal thickness, the between-subject difference in choroidal thickness exceeded 200 µm in this study, as shown in Table 1. Based on the estimated regression coefficient, this range could correspond to approximately a 2-mmHg difference in posture-induced IOP differences at 9 a.m. Given that a 2-mmHg IOP difference may be clinically meaningful in glaucoma management, the effect of choroidal thickness may be clinically relevant in eyes with extremely thin or thick choroids.
Corneal hysteresis, a measure of corneal biomechanical properties, was associated with larger posture-induced IOP differences at 9 p.m. and showed a similar trend at 9 a.m. Previous studies have shown that CH is smaller in glaucoma eyes, including patients with POAG, and is associated with disease progression.19,20 The relationship between CH and posture-induced IOP differences has not been extensively studied, but our findings suggest that corneal biomechanical properties may influence the accuracy of tonometry measurements in different body positions or may reflect underlying differences in ocular tissue compliance that affect IOP regulation. The mean CH in our cohort was 10.4 ± 1.16 mmHg, which, while within the normal range reported in some studies, is consistent with values reported in other treated POAG cohorts with a wide range of disease severity. The clinical relevance of the observed association between higher CH and greater posture-induced IOP differences, independent of other variables, may be modest, given the partial Nakagawa’s R2 value of 0.03, indicating that CH accounted for approximately 3% of the variability in posture-induced IOP differences at 9 p.m. (2.7 ± 1.7 mmHg).
Regarding antiglaucoma medications, our finding that the presence of individual medication classes, including prostaglandin analogs, β-blockers, and carbonic anhydrase inhibitors, within the topical regimen did not affect posture-induced IOP differences is consistent with the previous report by Kiuchi et al10 in patients with NTG. Our study extends these findings to a treated POAG population in which most participants had IOP levels consistent with NTG (mean treated IOP 11.2 mmHg, maximum 17–18 mmHg), and additionally evaluates combination regimens — an aspect not addressed in prior studies. Furthermore, we demonstrated that the presence of α2-adrenergic agonists or ROCK inhibitors within the topical regimen was also not associated with posture-induced IOP differences. In contrast, the combination of an α2-adrenergic agonist and a ROCK inhibitor was associated with smaller posture-induced IOP differences, and this effect was significant specifically at 9 a.m. Taken together, the presence of any individual antiglaucoma medication class within the topical regimen did not materially alter posture-induced IOP differences in our cohort, whereas only the α2-adrenergic agonist plus ROCK inhibitor combination was associated with an attenuated postural IOP response in exploratory analyses. This finding highlights a potential regimen-specific effect on posture-related IOP fluctuations that may not be captured when medication classes are evaluated individually. This finding should be interpreted with considerable caution given the limited subgroup size (n = 31 eyes), the non-randomized design, and the exploratory nature of the analysis without multiple comparison adjustment. The result is best regarded as hypothesis-generating and requires confirmation in prospective, adequately powered studies.
The mechanism underlying this combination effect remains unclear. Previous studies have shown that brimonidine monotherapy reduces daytime IOP but has limited efficacy during the nocturnal period.21 Liu et al21 reported that brimonidine significantly reduced sitting and supine IOP during the day but did not lower IOP during sleep, which may explain why the α2-adrenergic agonist plus ROCK inhibitor combination was effective only in the morning measurements. ROCK inhibitors enhance conventional outflow through the trabecular meshwork22 and may counteract IOP elevations associated with increased episcleral venous pressure in the supine position. The combination of these complementary mechanisms may contribute to the observed reduction in posture-induced IOP differences. These findings should be interpreted with considerable caution. The analyses of individual drug classes and two-drug combinations were exploratory in nature, no adjustment for multiple comparisons was applied, and the timing of medication instillation relative to IOP measurements was not uniformly standardized in this retrospective study. These results should therefore be regarded as hypothesis-generating only, and prospective studies with standardized medication protocols are needed for definitive evaluation.
This study has several limitations. First, given the relatively limited sample size, and the number of covariates included in the multivariate mixed-effects models, the possibility of model overfitting cannot be entirely excluded, and the results should be interpreted with appropriate caution, despite the absence of substantial multicollinearity as confirmed by pairwise correlation analysis (all |r| < 0.6) and VIF analysis (all VIF < 3.0). In addition, the retrospective design and single-center setting may limit the generalizability of the findings. A prospective cross-sectional design would have been preferable to minimize selection bias and allow more rigorous control of measurement conditions. Second, the mean axial length in our cohort was 26.1 ± 1.67 mm, which is longer than typically reported for the general Japanese population (approximately 24.0–24.5 mm), likely reflecting the higher prevalence of myopia in our clinical glaucoma population. This characteristic may limit the generalizability of our findings to populations with different refractive profiles. Third, IOP measurements were performed only at two time points (9 a.m. and 9 p.m.)., and true nocturnal IOP during sleep was not assessed. Future studies using continuous IOP monitoring or home tonometry during habitual sleep may provide more comprehensive insight into nocturnal IOP patterns. Fourth, subfoveal choroidal thickness was measured only once during the afternoon of the outpatient visit conducted in the week prior to hospitalization (typically between 15:00 and 16:30). Corneal hysteresis was measured only once during the morning session (9 a.m.). Both parameters may exhibit diurnal variation — choroidal thickness is known to exhibit diurnal fluctuation, and corneal hysteresis may also vary throughout the day.20 Therefore, these single measurements may not accurately reflect the states of these parameters at the time of IOP measurements, and the associations we report might differ somewhat if measurements had been performed at each time point. Fifth, the specific timing of antiglaucoma medication instillation relative to IOP measurements was not strictly standardized in this retrospective study. As different medication classes have different pharmacokinetic profiles — for example, prostaglandin F2α agonists reduce both diurnal and nocturnal IOP, whereas β-blockers and carbonic anhydrase inhibitors have limited nocturnal efficacy — the variability in instillation timing may have introduced heterogeneity into the medication-related analyses and could have influenced the observed associations. This limitation should be considered when interpreting the medication-related findings. However, because this study was conducted under inpatient monitoring, instillation times were ascertained from patient activity logs and nursing records where available; morning instillation times were relatively consistent (typically around 7:00 a.m)., whereas evening instillation times were more variable and not uniformly documented. A sensitivity analysis excluding participants with uncertain instillation times and those who received eye drops after the respective IOP measurement time point confirmed that the main findings in Tables 2–4 — including the association of the α2-adrenergic agonist plus ROCK inhibitor combination with smaller posture-induced IOP differences — remained unchanged. Sixth, the heterogeneity of medication combinations limited our ability to evaluate all possible interactions. The binary (presence/absence) classification of individual drug classes is a simplification that may not fully capture the complexity of real-world polypharmacy regimens; more granular analyses based on specific complete medication regimens would have been preferable but were precluded by the limited sample size. Seventh, the significant association observed for the α2-agonist plus ROCK inhibitor combination must be interpreted cautiously, given the exploratory nature of medication analyses and the risk of type I error from multiple comparisons without adjustment. Eighth, all participants were receiving antiglaucoma medications as part of their clinical care, and the study did not include a control group of healthy subjects or treatment-naive glaucoma patients. The inclusion of such controls in future studies would allow characterization of the reference posture-induced IOP response and would strengthen interpretation of medication-related findings. Furthermore, pretreatment IOP was not systematically recorded, precluding formal classification of participants into HTG and NTG subtypes. The mean treated IOP in our cohort (11.2 mmHg, maximum 17–18 mmHg) suggests that most participants had IOP levels consistent with NTG, and our findings may therefore not be directly applicable to HTG patients. Future studies with clearly defined IOP subtypes would allow more granular analysis of posture-induced IOP changes across glaucoma subtypes. In addition, while visual field MD and cpRNFLT were included as a descriptive characteristic, neither visual field indices nor OCT-derived structural parameters were included as independent variables in the multivariate models, as our primary aim was to identify modifiable physiological and medication-related factors. Future studies with larger sample sizes should explore whether glaucoma severity and structural damage, as assessed by visual field testing and OCT, are associated with posture-induced IOP changes. In addition, examiners were not formally masked to prior IOP readings, which may have introduced measurement bias. Future prospective studies should incorporate masked examination protocols to minimize this potential source of bias. Finally, other factors that may influence posture-induced IOP changes, such as sleep position preference, severity of obstructive sleep apnea, or the use of specific cardiovascular medications, were not assessed.
In conclusion, posture-induced IOP differences in treated POAG eyes were greater in the morning than in the evening, with different factors associated at each time point. Blood pressure–related parameters were particularly important in the evening, and combination therapy with an α2-adrenergic agonist and a ROCK inhibitor was associated with smaller IOP differences in exploratory analyses. These findings suggest that comprehensive assessment of ocular and systemic factors, including cardiovascular parameters, may be relevant in the clinical management of glaucoma. Prospective cohort studies with standardized medication protocols and rigorous recording of instillation times are needed for definitive evaluation of medication effects on posture-induced IOP changes.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
All authors declare no conflicts of interest.
References
1. Anderson DR, Grant WM. The influence of position on intraocular pressure. Invest Ophthalmol. 1973;12:204–13.
2. Ireka OJ, Ogbonnaya CE, Arinze OC, et al. Comparing posture induced intraocular pressure variations in normal subjects and glaucoma patients. Int J Ophthalmol. 2021;14:402–407. doi:10.18240/ijo.2021.03.11
3. Kiuchi T, Motoyama Y, Oshika T. Relationship of progression of visual field damage to postural changes in intraocular pressure in patients with normal-tension glaucoma. Ophthalmology. 2006;113:2150–2155. doi:10.1016/j.ophtha.2006.06.014
4. Jasien JV, Jonas JB, de Moraes CG, Ritch R. Intraocular pressure rise in subjects with and without glaucoma during four common yoga positions. PLoS One. 2015;10(12):e0144505. doi:10.1371/journal.pone.0144505
5. Tsukahara S, Sasaki T. Postural change of IOP in normal persons and in patients with primary wide open-angle glaucoma and low-tension glaucoma. Br J Ophthalmol. 1984;68(6):389–392. doi:10.1136/bjo.68.6.389
6. Gautam N, Kaur S, Kaushik S, et al. Postural and diurnal fluctuations in intraocular pressure across the spectrum of glaucoma. Br J Ophthalmol. 2016;100:537–541. doi:10.1136/bjophthalmol-2015-306861
7. Najmanová E, Pluháček F, Haklová M. Intraocular pressure response affected by changing of sitting and supine positions. Acta Ophthalmol. 2020;98(3):e368–e372. doi:10.1111/aos.14267
8. Fang SY, Wan Abdul Halim WH, Mat Baki M, et al. Effect of prolonged supine position on the intraocular pressure in patients with obstructive sleep apnea syndrome. Graefes Arch Clin Exp Ophthalmol. 2018;256:783–790.
9. Belkin A, Dar N, Pillar S, et al. The effect of trabeculectomy and glaucoma drainage device implantation on postural intraocular pressure changes in glaucomatous eyes. Acta Ophthalmol. 2021;99:e1095–e1101. doi:10.1111/aos.14776
10. Kiuchi T, Motoyama Y, Oshika T. Influence of ocular hypotensive eyedrops on intraocular pressure fluctuation with postural change in eyes with normal-tension glaucoma. Am J Ophthalmol. 2007;143(4):693–695. doi:10.1016/j.ajo.2006.11.020
11. Nakazawa K, Higashide T, Tsuchiya S, Shioya S, Okayama M, Sugiyama K. Association of ambulatory blood pressure and other factors with intraocular pressure–related 24-hour contact lens sensor profile in untreated glaucoma. Transl Vis Sci Technol. 2022;11(10):18.
12. Sultan M, Blondeau P. Episcleral venous pressure in younger and older subjects in the sitting and supine positions. J Glaucoma. 2003;12:370–373. doi:10.1097/00061198-200308000-00013
13. Friberg TR, Sanborn G, Weinreb RN. Intraocular and episcleral venous pressure increase during inverted posture. Am J Ophthalmol. 1987;103:523–526. doi:10.1016/S0002-9394(14)74275-8
14. Geloneck MM, Crowell EL, Wilson EB, et al. Correlation between intraocular pressure and body mass index in the seated and supine positions. J Glaucoma. 2015;24:130–134. doi:10.1097/01.ijg.0000435775.05032.87
15. Mori K, Ando F, Nomura H, et al. Relationship between intraocular pressure and obesity in Japan. Int J Epidemiol. 2000;29:661–666. doi:10.1093/ije/29.4.661
16. Ross A, Ostrin LA. Influence of body position and time of day on ocular rhythms. Sci Rep. 2025;15(1):26556. doi:10.1038/s41598-025-10873-7
17. Tan CS, Ouyang Y, Ruiz H, et al. Diurnal variation of choroidal thickness in normal, healthy subjects measured by spectral domain optical coherence tomography. Invest Ophthalmol Vis Sci. 2012;53:261–266. doi:10.1167/iovs.11-8782
18. Prata TS, De Moraes CGV, Kanadani FN, et al. Posture-induced intraocular pressure changes: considerations regarding body position in glaucoma patients. Surv Ophthalmol. 2010;55:445–453. doi:10.1016/j.survophthal.2009.12.002
19. Medeiros FA, Meira-Freitas D, Lisboa R, et al. Corneal hysteresis as a risk factor for glaucoma progression: a prospective longitudinal study. Ophthalmology. 2013;120:1533–1540. doi:10.1016/j.ophtha.2013.01.032
20. Okayama M, Tsuchiya S, Higashide T, et al. Diurnal variation of corneal hysteresis in patients with untreated primary open-angle glaucoma and normal individuals. J Glaucoma. 2022;31(11):891–897. doi:10.1097/IJG.0000000000002112
21. Liu JH, Medeiros FA, Slight JR, et al. Diurnal and nocturnal effects of brimonidine monotherapy on intraocular pressure. Ophthalmology. 2010;117:2075–2079. doi:10.1016/j.ophtha.2010.03.026
22. Rao PV, Pattabiraman PP, Kopczynski C. Role of the Rho GTPase/Rho kinase signaling pathway in pathogenesis and treatment of glaucoma: bench to bedside research. Exp Eye Res. 2017;158:23–32. doi:10.1016/j.exer.2016.08.023
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Treatment of Open-Angle Glaucoma and Ocular Hypertension with the Fixed-Dose Combination of Preservative-Free Tafluprost/Timolol: Clinical Outcomes from Ophthalmology Clinics in Italy
Oddone F, Scorcia V, Iester M, Sisto D, De Cilla S, Bettin P, Cagini C, Figus M, Marchini G, Rossetti L, Rossi G, Salgarello T, Scuderi GL, Staurenghi G
Clinical Ophthalmology 2022, 16:1707-1719
Published Date: 1 June 2022
Assessment of the Effectiveness, Tolerability, and Safety of the Preservative-Free Fixed Combination of Timolol, Dorzolamide, and Brimonidine Compared to Separate Therapies in Patients with Glaucoma, a Randomized Controlled Trial
Belalcazar S, Tornero-Jimenez A, Mejia-Morales C, Olvera-Montaño O, Muñoz-Villegas P
Clinical Ophthalmology 2026, 20:580973
Published Date: 19 February 2026