Back to Journals » ImmunoTargets and Therapy » Volume 15
Postural Orthostatic Tachycardia Syndrome, Myalgic Encephalomyelitis/Chronic Fatigue Syndrome and Long COVID as Neuroimmune Disorders
Authors Blitshteyn S ![]() , Doherty TA, Steinman L
, Doherty TA, Steinman L
Received 13 November 2025
Accepted for publication 23 January 2026
Published 2 February 2026 Volume 2026:15 581262
DOI https://doi.org/10.2147/ITT.S581262
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Michael Shurin
Svetlana Blitshteyn,1 Taylor A Doherty,2,3 Lawrence Steinman4,5
1Department of Neurology, Jacobs School of Medicine and Biomedical Sciences, University at Buffalo, Buffalo, NY, USA; 2Division of Allergy & Immunology, UC San Diego, La Jolla, CA, USA; 3Veterans Affairs San Diego Health Care System, La Jolla, CA, USA; 4Department of Neurology and Neurological Sciences, Stanford University, Stanford, CA, USA; 5Department of Pediatrics, Stanford University, Stanford, CA, USA
Correspondence: Svetlana Blitshteyn, Clinical Associate Professor of Neurology, University at Buffalo Jacobs School of Medicine and Biomedical Sciences, Buffalo, NY, USA, Email [email protected]
Abstract: Postural orthostatic tachycardia syndrome (POTS), myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) and Long COVID are heterogeneous disorders with overlapping complex, multi-factorial and multi-systemic pathophysiology. POTS and ME/CFS are the most common phenotypes of Long COVID that can lead to significant disability and functional impairment. The exact pathophysiologic mechanisms of these disorders alone or in combination are still being investigated, but important mechanistic factors have been identified, such as autonomic dysfunction, immune dysregulation, autoimmunity, mitochondrial dysfunction, cerebral hypoperfusion, and neuroinflammation. To this end, we believe that these conditions should be viewed as neuroimmune disorders and should be included in the field of neuroimmunology, with its educational curriculum, training, and clinical care pathways. Including these disorders as part of neuroimmunology subspecialty is the key to advancing the science and clinical care of this underserved patient population with these complex and disabling conditions.
Keywords: postural orthostatic tachycardia syndrome, myalgic encephalomyelitis/chronic fatigue syndrome, long COVID, neuroimmunology, dysautonomia
Postural orthostatic tachycardia syndrome (POTS) and dysautonomia in general, myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) and Long COVID are currently viewed as heterogeneous disorders with overlapping complex, multi-factorial and multi-systemic pathophysiology.1–3 POTS/dysautonomia and ME/CFS are common sequelae of SARS-CoV-2 infection and the most common phenotypes of Long COVID.1–3 The exact pathophysiologic mechanisms of these disorders alone or in combination are still under investigation, but several themes emerged as frontrunners: immune dysfunction, autoimmunity, autonomic dysfunction, cerebral hypoperfusion and neuroinflammation.1–3 In this narrative review, we discuss established and proposed pathophysiologic mechanisms of POTS, ME/CFS and Long COVID, given the existing and emerging scientific evidence. Despite the multi-factorial pathology, we believe that these syndromes should be viewed as neuroimmune disorders and should fall under the umbrella of neuroimmunology, along with multiple sclerosis, neuromyelitis optica spectrum disorders, neurologic Sjogren’s disease and others.
Autonomic Nervous System
Consisting of sympathetic, parasympathetic and enteric divisions, the autonomic nervous system (ANS) is involved in vital physiologic functions, including cardiovascular control of heart rate and blood pressure, gastric motility and secretion, bladder function, respiration, temperature control and perfusion of organs and tissues. The ANS is responsible for the “flight or fight” response to both external and internal stimuli, and the goal is to maintain homeostasis.4 The ANS and the immune system are connected, with the ANS playing a significant role in the process of inflammation via the vagus nerve, which carries the parasympathetic nervous system output. The vagus nerve is the critical component of the inflammatory reflex, which controls innate immune responses and inflammation during pathogen invasion and tissue injury.5 To this end, it has been postulated that sympathetic overactivity may be associated with a pro-inflammatory state, while increased parasympathetic activity has anti-inflammatory properties.5,6
Postural tachycardia and orthostatic intolerance are key features of POTS, but dysautonomia more broadly may include other symptoms and manifestations, such as chronic dizziness, lightheadedness, palpitations, presyncope, syncope, exercise intolerance, heat intolerance, cognitive dysfunction, fatigue and a decline in functioning. Gastrointestinal, respiratory, and genitourinary symptoms are also common and, in some patients, may be prominent and disabling.1,7
Postural Orthostatic Tachycardia Syndrome
POTS, one of the most common autonomic disorders, is a frequent sequela of SARS-CoV-2 as part of Long COVID and is a common comorbidity of ME/CFS.8,9 POTS diagnostic criteria include the following: 1) an excessive and sustained increase in heart rate (HR) of more than 30 beats per minute (bpm) within 10 minutes of standing or during a head-up tilt table test [or in individuals aged 12 to 19 years, an increase of > 40 bpm] 2) absence of orthostatic hypotension (sustained drop in systolic blood pressure of at least 20 mmHg) 3) presence of symptoms of orthostatic intolerance that are worse with standing and typically improve with lying down, such as palpitations, lightheadedness, and exercise intolerance, 4) symptom duration should be at least 3 months.10,11 Other conditions mimicking POTS, such as anemia, anorexia nervosa, anxiety, fever, infection, dehydration, pain, hyperthyroidism, pheochromocytoma, deconditioning, or use of drugs such as anticholinergics and sympathomimetics, need to be ruled out although many of these conditions can be present alongside with POTS.10,11
Myalgic Encephalomyelitis/Chronic Fatigue Syndrome
ME/CFS can be diagnosed via a number of diagnostic criteria, and orthostatic intolerance is one of the minor diagnostic criteria of ME/CFS according to the CDC.12 Both POTS and autonomic dysfunction without tachycardia (termed “dysautonomia”) are major pathophysiologic mechanisms of ME/CFS and Long COVID.12 There is emerging evidence that abnormalities in the neuroimmune pathways and neuroinflammation may be among the mechanisms of ME/CFS.13 Numerous neuroimaging studies highlighted important brain regions with hypoactivity, including insula, thalamus, and limbic cortex and suggested that cortical-limbic disconnection, impacting metabolites and brain waves, contributes to ME/CFS symptoms.14 Extensive phenotyping and studies on serum and cerebrospinal fluid markers demonstrated distinct abnormalities in patients with ME/CFS compared to healthy controls suggesting immunologic and autoimmune pathophysiologies.15,16
Long COVID
Long COVID is defined as “an infection-associated chronic condition that occurs after SARS-CoV-2 infection and is present for at least 3 months as a continuous, relapsing and remitting, or progressive disease state that affects one or more organ systems”.17 Both ME/CFS and POTS are major phenotypes associated with Long COVID, and autonomic dysfunction is present in nearly 70% of patients with Long COVID, making it a major pathophysiologic mechanism.18,19 Other major pathophysiologic mechanisms of Long COVID include autoimmune, inflammatory and immune dysregulations, which are similar to the pathophysiology of POTS. Elevated serum autoimmune and inflammatory markers have been found in patents with POTS and in patients with Long COVID.20,21 Neuroimaging studies suggest that neuroinflammation at the brainstem, specifically at the dorsolateral inferior medulla, may be a possible central nervous system localization for both POTS and Long COVID, which is where the vagal nuclei and vestibular pathways are located.22 While clinical presentation of patients with these disorders are complex and diverse, consensus guidance statements on assessment and treatment of post-COVID autonomic dysfunction have been developed. Diagnostic evaluation and therapeutic options for patients with post-COVID dysautonomia closely parallel those that are available for patients with POTS and other common autonomic disorders.23
The Immune System in POTS, ME/CFS and Long COVID
The innate immune system acts as the body’s first line of defense against infections and stressors, operating in a preprogrammed manner. Its key role in the pathophysiology of central and peripheral neurologic manifestations involves recruiting immune cells through cytokine production, activating the complement system, and initiating adaptive immune responses via antigen presentation.24
Studies have implicated abnormalities in dysregulated immunity in ME/CFS patients, including increased naïve B-cell numbers with switched memory B-cells in the blood, along with peripheral T-cell exhaustion, activation in the cerebrospinal fluid and decreased cytolytic expression.16 The immunologic abnormalities in ME/CFS are numerous and beyond the scope of this review, but include increase in CD21+, CD19+, and CD5+ B cells, and antigen-driven clonal B cell expansion; an increase in activated CD8+ T cells, a reduction in CD11b levels; decreased CD8 suppressor cell population; reduced NK cell functioning and many others.25 NK cells are innate IFN-γ-producing cells that, in conjunction with CD8 T cells, are critical for controlling viral infections. Similar to ME/CFS, the immune system in Long COVID has been found to have significant alterations, including chronic activation of a subset of CD8+ T cells, exhausted T cells, hyperactivated mast cells and elevated interleukin (IL)-1beta, IL-6, and tumor necrosis factor (TNF), as well as elevated intermediate (CD14+, CD16+) and non-classical monocyte (CD14Lo, CD16+) with SARS-CoV-2 S1 protein.3,26,27 Unlike the studies on ME/CFS and Long COVID, the assessment of immunologic profile in patients with POTS and dysautonomia has been extremely limited, aside from the autoimmune etiology. One study demonstrated elevations of IL1β, IL21, TNFα, INFγ, and CD30 in patients with POTS, and another study showed an association with human leukocyte antigen DQB1*06:09 in Korean population with POTS.28,29
T-cell exhaustion represents an aspect of immunologic dysregulation that can result from prolonged responses to chronic infections or inflammatory conditions, such as certain viral infections or autoimmune diseases.30 In this state, T-cells lose their full ability to eliminate pathogens or dysfunctional cells, leading to a suppressed immune response. Studies exploring immunologic profile and potential presence of T-cell exhaustion are urgently needed to identify an immunologic phenotype of POTS and other forms of dysautonomia that may be especially responsive to immunotherapies.
Autoimmunity
Traditionally, POTS has been classified as neuropathic, hypovolemic and hyperadrenergic although clinically, these subtypes may be indistinguishable from one another due to their overlapping and compensatory pathophysiologies.31 Despite the notion that POTS has heterogeneous and diverse pathophysiology, autoimmunity has emerged as one of its major mechanisms in the past decade. One study of 100 patients with POTS found a higher prevalence of various non-specific autoimmune markers, including antinuclear antibodies, and comorbid autoimmune disorders than in the general population.20 Subsequently, multiple studies identified a variety of antibodies important to the autonomic nervous system and vascular control, including ganglionic N-type and P/Q type acetylcholine receptor antibodies, alpha 1, beta 1 and beta 2 adrenergic antibodies, muscarinic M2 and M4 antibodies, angiotensin II type 1 receptor antibodies and opioid-like 1 receptor antibodies in patients with POTS and other forms of dysautonomia.32–36 Interestingly, many of these antibodies have been also found in overlapping or comorbid conditions with POTS, such as ME/CFS, small fiber neuropathy, complex regional pain syndromes and cardiovascular disorders.
Similar to POTS, autoimmunity is considered to be one of the major mechanisms of Long COVID, with an associated increased risk, overall incidence and range of autoimmune conditions after SARS-CoV-2 infection.21,37 Autoantibodies to inflammatory cytokines such as IgG to IL-2, D8B, thyroglobulin, and IFNδ and others have been identified in patients with Long COVID, and these autoantibodies have been associated with anti-SARS CoV2 IgG antibodies.21,26,37 Similar to patients with POTS, G protein-coupled receptor antibodies, including against alpha- and beta-adrenergic antibodies and muscarinic antibodies, as well as autoantibodies to antinuclear and extractable nuclear antigens, were also found in patients with Long COVID.38 The pro-inflammatory mediators, non-specific antibodies and antibodies relevant to the function of the autonomic nervous system are thought to be important in Long COVID and in post-COVID autonomic disorders, more specifically.26,37,39
Similarly to POTS and Long COVID, evidence of autoimmunity has been found in some patients with ME/CFS. A positive ANA has been identified in 68% of ME/CFS patients with the majority directed against nuclear envelope,40 while dsDNA antibodies were found in 12% of patients.41 Anti-ganglioside antibodies, anti-phospholipid antibodies and antibodies against cardiolipin were described in a large subset of patients with ME/CFS42 Additionally, G-coupled protein receptor antibodies, which include anti-muscarinic and anti-adrenergic receptor antibodies, that have been found in patients with POTS and Long COVID, have been also identified in patients with ME/CFS, suggesting that receptors mediating autonomic nervous system transmission are highly relevant and might be a unifying mechanism in all three disorders.36,38,42
Mitochondrial Dysfunction
Mitochondrial dysfunction has been recognized as a pathophysiologic substrate in ME/CFS and its comorbidities and as a mediator in inflammation and autoimmunity.43,44 While many potential abnormalities in mitochondrial genes, protein structure and function and the influence of external factors on mitochondrial function, such as infection or toxic clearance, are being investigated, its role in the pathogenesis of fatigue has been established.43 Chronic fatigue is one of the defining features and most disabling symptoms of ME/CFS, POTS, Long COVID and is associated with many other systemic disorders. Patients with ME/CFS, POTS and Long COVID experience chronic fatigue, both physical and mental, which is likely the most disabling and most limiting feature of these conditions, resulting in significant functional impairment and reduced quality of life.45 Importantly, most patients with POTS have chronic fatigue with at least 20% satisfying the diagnostic criteria of ME/CFS.45 Immune dysfunction, including cellular exhaustion and persistent inflammation, has been linked to mitochondrial function.43 Thus, it is possible that POTS is associated with mitochondrial and immune dysfunction, which then impacts the function of every cell, alters homeostasis and affects energy production and consumption at the cellular level.
Recently, a study of twenty POTS patients following time-restricting eating for six months demonstrated improvements in upright heart rate, energy, and mitochondrial/metabolic function.46 Additionally, several case reports on mitochondrial disorders in patients with POTS have been published,47,48 but further studies on mitochondrial structure and function in POTS and other forms of dysautonomia are needed to determine whether mitochondrial dysfunction is present in most patients with POTS and chronic fatigue and how it ties into autonomic dysfunction and immune dysregulation.
Cerebral Hypoperfusion
Cerebral hypoperfusion emerged as one of the major mechanisms of POTS, dysautonomia, myalgic encephalomyelitis/chronic fatigue syndrome and probably Long COVID.49,50 Cerebral and brainstem hypoperfusion together with neuroinflammation, specifically at the dorsolateral medulla, may be the CNS mechanisms in POTS and Long COVID and need to be investigated further.22,51,52 Why brainstem hypoperfusion occurs is unclear: multiple hypotheses exist, including a possibility that small penetrating arteries coming off the vertebrobasilar arterial system and supplying the brainstem may be damaged from endothelial dysfunction, hypercoagulable state and possible microclots, all of which have been suggested as playing a role in the pathogenesis of POTS and Long COVID.53 Other possible mechanisms may include alterations in the glymphatic system, which can lead to inadequate venous drainage of the medulla, venous congestion and toxin accumulation, all of which can result in neuroinflammation. Finally, abnormalities in the connective tissue itself, which could be caused by neuroinflammatory and immune-mediated pathways that include hyperactivated mast cells, may damage the venous and arteriolar walls and the blood-brain barrier. In turn, the altered blood-brain barrier can result in abnormal permeability and vascular contractility, thereby causing decreased perfusion of the brainstem.22,53
Neuroinflammation
Emerging evidence suggests that neuroinflammation plays an important role in the pathophysiology of Long COVID. The neuroinflammation has been identified at specific regions of the brain and brainstem that are critical to the autonomic nervous system control of the organs and vital physiologic processes, including respiration, heart rate, blood flow, digestive system, bladder function and probably immunologic response.52,54,55 Additionally, neuroinflammation might affect other brain regions, such as the insular cortex, basal ganglia and hypothalamus.3 Using advanced neuroimaging techniques and 7T MRI, structural abnormalities at the dorsolateral medulla were observed in patients with Long COVID.52 The multisystemic and diverse symptoms experienced by patients with Long COVID correlate with the structural abnormalities of the brainstem seen on 7T MRI,52 which could also be the localization for POTS and autonomic dysfunction more broadly, unrelated to SARS-CoV-2 infection.22 Importantly, systemic abnormalities consisting of central hypovolemia, hyperadrenergic response and downstream autonomic neuropathy resulting from central autonomic network dysregulation may correlate to the hypovolemic, hyperadrenergic and neuropathic POTS phenotypes and may localize to the dorsolateral medulla and hypothalamus via nucleus tractus solitarius, dorsal motor nucleus of the vagus and dorsal longitudinal fasciculus traversing near the floor of the fourth ventricle.22,52
To delineate the structural and function abnormalities in the central nervous system further, future studies should utilize advanced neuroimaging techniques and animal models with immunohistochemical brainstem tissue assessments. These studies would need to focus on the underlying mechanisms and precise localization of neuroinflammation that are likely to affect patients with Long COVID, POTS and other autonomic disorders that involve cerebral hypoperfusion. Studies demonstrate that chronic cerebral hypoperfusion can induce excessive inflammatory response that precedes neuronal dysfunction and that TRPM2 channel aggravates neuroinflammation via activation of microglia in a state of chronic cerebral hypoperfusion.56 TRMP2 channels are involved in the production of proinflammatory cytokines in macrophages and inflammation-related disorders as well as neuropathic pain.56 Clearly, the relationship between cerebral hypoperfusion and neuroinflammation as it relates to Long COVID, POTS and ME/CFS needs to be explored, and it might be modulated by the microglia and other factors that regulate perfusion, neurotransmitter concentration, metabolism and connectivity between the brain regions.
The Brain and the Immune System
The association between the brain and the immune system has been an emerging and exciting area of research, which may uncover how the brain modulates and regulates the immune system and, alternatively, how systemic immunologic response to an infection, allergen, major trauma or another trigger translates into a variety of neurologic and psychiatric manifestations.57,58 Jin et al showed that a peripheral immune insult strongly activates the body–brain axis to regulate immune responses, which is accomplished via pro-inflammatory and anti-inflammatory cytokines in communication with vagal neurons.57 Additionally, the gut-brain axis via the vagus nerve and the connection to spleen, lymph nodes and other organs activates T and B cells, macrophages, dendritic cells, plasma cells, production of antibodies, and release of pro-inflammatory cytokines.57,58 Trabanelli et al showed that anticipation of approaching infection via virtual reality activates infection-sensing brain regions and the hypothalamus and connect these effects to the hypothalamic–pituitary–adrenal axis, suggesting an integrated neuro–immune reaction in humans toward infection threats, not solely following physical contact, but through the perception of a threat.59
Besides the vagal nuclei and the hypothalamic-pituitary-adrenal axis, neurons in the insular cortex have been shown to activate during peripheral inflammation. These insular cortex neurons project to autonomic nervous system control sites: reactivation of these neurons can retrieve specific immune responses demonstrating immunological memory to neuronal representations of inflammatory information.60 Finally, the importance of meningeal lymphoid tissue, glymphatic system, cytokines produced by T cells and their impact on behavior, cognition, learning and memory have been acknowledged.61
Furthermore, microglia, the resident immune cells of the central nervous system, participate in the complex communication with other brain cells under steady-state conditions as well as with infiltrating peripheral immune cells during perturbations. Microglia are critical for maintaining the homeostasis and to overcome pathology leading to neuroinflammation.62 Importantly, microglial activation was found to be associated with the development of neurocognitive symptoms in Long COVID via specialized PET scan that used a protein ligand expressed by activated microglia as part of the neuroinflammatory response of the brain.63 Increased microglial activation was found specifically in the ventral striatal and dorsal putamen of patients with Long COVID and may identify possible CNS correlates of neurocognitive symptoms after COVID-19 infection. Microglia hyperactivation has been also considered in the CNS pathophysiology of ME/CFS;64,65 however, detailed studies on microglial activation in ME/CFS, POTS and dysautonomia more broadly are lacking. Specialized PET scans able to quantify microglial activation and immunohistochemistry of brain biopsy in the existing animal models for ME/CFS and POTS are needed to determine if microglial activation is present in these disorders.66,67
Neuroimmunology and POTS, ME/CFS and Long COVID
For many decades patients with POTS, ME/CFS and, more recently, with Long COVID, were largely neglected or misdiagnosed with a host of psychiatric disorders, including somatization, generalized anxiety disorder, depression, conversion or functional neurologic disorder, panic disorder and others. The assumption was that an infection or another acute event took place, then led to deconditioning, debility, faulty coping mechanisms and psychological disturbance with persistent sick behavior, which implied that the acute event resolved, the expected physiologic recovery occurred, but the patient’s psyche or mind continued to perpetuate the sick behavior, avoidant patterns and minimal effort preference. Physicians were erroneously taught that since all routine diagnostic tests returned as “normal,” then there should be no biological basis for the patient to remain sick. This false narrative neglected chronic inflammation, immune dysregulation, viral persistence, autonomic dysfunction, mast cell hyperactivation and other pathophysiologic mechanisms underlying post-acute infectious syndromes.3,12 Furthermore, education and training on autonomic disorders are lacking, which similarly leads to a lack of recognition and diagnostic accuracy in patients with dysautonomia and misdiagnosis with psychiatric or psychologically-based disorders. Diagnosing dysautonomia requires specialized training as patients typically present with complex neurologic, cardiovascular, rheumatologic, allergic and psychiatric symptoms. Nevertheless, as in most medical conditions, diagnosis relies on clinical skills, which includes obtaining a detailed history, performing a 10-minute stand test instead of a vital sign check while sitting only, and conducting a thorough neurologic and medical physical examination.1 Additional diagnostic tests include a tilt table test in conjunction with complete autonomic function testing if available, a skin punch biopsy to test for comorbid small fiber neuropathy, a serum panel with autoimmune and inflammatory markers, a cytokine panel if available, and other neurologic and immunologic tests as dictated by personalized case history.1,23
Similarly to POTS, patients with ME/CFS experience significant difficulty in obtaining medical care given the stigma, inadequate education and misdiagnosis with psychiatric conditions68 while patients with Long COVID appear to follow the same difficult and inadequate diagnostic and therapeutic journey. Long COVID is a major public health issue with long-lasting adverse health effects and impact on the individual and public health risks.69 Neurologic, autonomic and cognitive sequelae of SARS-CoV-2 infection represents a major healthcare burden and a threat to brain health, which would necessitate well-trained physicians and neurologists capable of diagnosing and treating Long COVID, POTS and ME/CFS.67,68 Many known and unknown adverse effects of SARS-CoV-2, including repeated infections on the developing brain of children and adolescents, the carcinogenic effects of the virus and its deleterious effects on aging and neurodegeneration, suggest that neurologists would be undoubtedly involved in the healthcare of these patients.69
The historical development of multiple sclerosis pathophysiology, biomarkers, diagnostic criteria and therapeutic options – and the treatment of patients, a majority of whom are also women as is the case with POTS, ME/CFS and Long COVID – closely parallels the patterns of POTS, ME/CFS and Long COVID.70,71 Although our understanding of these disorders is still evolving, along with the knowledge of how the brain is involved in the regulation of the immune system, we must designate POTS, other forms of dysautonomia, ME/CFS and Long COVID as an important category of neuroimmunology (Figure 1). Furthermore, we must develop educational materials, consensus guidance statements and clinical care pathways for neurologists and neuroimmunologists to gain knowledge and skills necessary for delivery of effective patient-centered care.23 For this to happen, the first step would be to abandon an outdated notion that these patients have psychiatric or psychological disturbances (or functional neurologic disorder, previously known as hysteria)70,71 – a critical change that transformed a disorder known in the past as hysterical paralysis to multiple sclerosis - a neuroimmune disease.
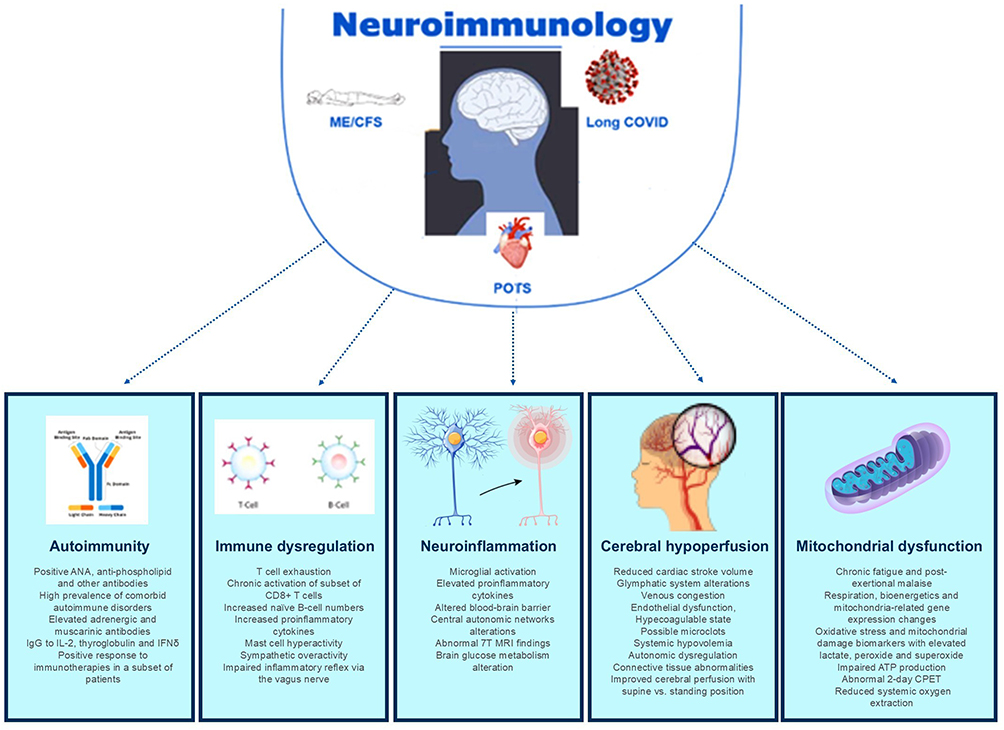 |
Figure 1 POTS, ME/CFS and Long COVID as Neuroimmune Disorders with shared pathophysiologic mechanisms. Abbreviations: POTS, postural orthostatic tachycardia syndrome; ME/CFS, myalgic encephalomyelitis/chronic fatigue syndrome; ANA, anti-nuclear antibodies; IgG, immunoglobulin G; 7T MRI, 7 Tesla magnetic resonance imaging. |
Future Direction
Neuroimmunology is a neurologic subspecialty that traditionally encompasses multiple sclerosis and other demyelinating disorders as well as neuroimmune manifestations of systemic autoimmune disorders. The field has been undergoing rapid transformation and paradigm shifts with neuroimmune aspects being identified in many neurologic and psychiatric disorders that have been traditionally viewed as not associated with neuroimmunology.72 The SARS-CoV-2 pandemic and Long COVID, with its prominent neurologic, immunologic and autonomic manifestations, further highlighted the importance of studying the brain-immune system interplay and the need to merge immunology and neuroscience research with clinical neurology going forward.
Although our knowledge of the neuroimmune mechanisms of POTS, ME/CFS and Long COVID is still expanding, along with our understanding of how the brain is involved in the modulation and regulation of the immune system, there is clinical and scientific evidence to suggest that POTS, ME/CFS and Long COVID fall into a broad category of neuroimmune disorders (Figure 1) and that immunotherapies may present an effective therapeutic option.73 Other complex disorders with significant neuropsychiatric manifestations that may fit into this category are pediatric acute-onset neuropsychiatric syndrome (PANS) and pediatric autoimmune neuropsychiatric disorder associated with streptococcal infections (PANDAS), neuropsychiatric manifestations of acute and chronic infections in adults and neuropsychiatric manifestations of systemic autoimmune, immunologic and allergic disorders, including mast cell activation syndrome.74
Neurologists, neuroimmunologists and autonomic specialists are uniquely positioned to understand and lead the scientific effort and clinical care of complex disorders involving the brain, the peripheral nervous system, the autonomic nervous system and the immune system. Expanding the scale and scope of neuroimmunology as a field would be critical from the diagnostic, therapeutic, scientific and public health perspectives. Validated and clinically available diagnostic tests, including 7T MRI, functional MRI, specialized PET scans, MR spectroscopy, autonomic function testing, skin biopsy, transcranial dopplers, wearable technology and devices that can accurately assess cerebral perfusion, as well as serum cytokine, antibody and inflammatory markers panels, would need to become available as routine diagnostic tests. There is unprecedent opportunity and an urgent call for action to improve the care of many millions of patients with complex disorders involving the brain and the immune system and to promote brain health by developing neurotherapeutics consisting of new and repurposed immunomodulating, anti-inflammatory, and, potentially, antimicrobial therapies.
Conclusion
In summary, POTS, ME/CFS and Long COVID demonstrate overlapping pathophysiologies rooted in immune-mediated and neuroinflammatory pathways involving the interplay between the brain and the immune system with mechanistic factors, such as T cell exhaustion, autoimmunity, proinflammatory cytokines, autonomic dysfunction, mitochondrial dysfunction, cerebral hypoperfusion, microglial activation and probably many other factors that remain to be identified. As neurology, neuroscience and neuroimmunology are advancing and evolving, so is our understanding of complex disorders involving the brain, the immune system and the autonomic nervous system. Once considered obscure and elusive, POTS, ME/CFS and Long COVID emerged as neuroimmune disorders, each with its own diagnostic criteria, but all three with overlapping pathophysiologies and therapeutic considerations. Classifying these disorders as neuroimmune and including them in neuroimmunology education and training is imperative to advancing the science and clinical care of millions of patients living with these complex and disabling conditions.
Disclosure
SB serves on the Executive Committee for CSL Behring. SB is a paid speaker on Long COVID for the CDC ECHO program. SB serves as a non-paid member of the NIH-RECOVER-TLC Neurological Agents Working Group. TAD is supported by NIH AI171795 and Veterans Affairs BLR&D BX005073. LS received compensation from TG Therapeutics, Inc. The authors report no other conflicts of interest in this work.
References
1. Blitshteyn S. Dysautonomia: a common comorbidity of systemic disease. Immunol Res. 2025;73(1):105. doi:10.1007/s12026-025-09661-2
2. Komaroff AL, Lipkin WI. ME/CFS and Long COVID share similar symptoms and biological abnormalities: road map to the literature. Front Med Lausanne. 2023;10:1187163. doi:10.3389/fmed.2023.1187163
3. Moen JK, Baker CA, Iwasaki A. Neuroimmune pathophysiology of long COVID. Psychiatry Clin Neurosci. 2025;79(9):514–10. doi:10.1111/pcn.13855.
4. Benarroch EE. Physiology and Pathophysiology of the Autonomic Nervous System. Continuum. 2020;26(1):12–24. doi:10.1212/CON.0000000000000817
5. Pavlov VA, Tracey KJ. The vagus nerve and the inflammatory reflex--linking immunity and metabolism. Nat Rev Endocrinol. 2012;8(12):743–754. doi:10.1038/nrendo.2012.189
6. Pongratz G, Straub RH. The sympathetic nervous response in inflammation. Arthritis Res Ther. 2014;16(6):504. doi:10.1186/s13075-014-0504-2
7. Thieben MJ, Sandroni P, Sletten DM, et al. Postural orthostatic tachycardia syndrome: the Mayo Clinic experience. Mayo Clin Proc. 2007;82(3):308–313. doi:10.4065/82.3.308
8. Blitshteyn S, Whitelaw S. Postural orthostatic tachycardia syndrome (POTS) and other autonomic disorders after COVID-19 infection: a case series of 20 patients. Immunol Res. 2021;69(2):205–211. doi:10.1007/s12026-021-09185-5
9. Jason LA, McGarrigle WJ, Vermeulen RCW. The Head-Up Tilt Table Test as a Measure of Autonomic Functioning among Patients with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. J Personalized Med. 2024;14(3):238. doi:10.3390/jpm14030238
10. Sheldon RS, Grubb II BP, Olshansky B, et al. Heart Rhythm Society expert consensus statement on the diagnosis and treatment of postural tachycardia syndrome, inappropriate sinus tachycardia, and vasovagal syncope. Heart Rhythm. 2015;12(6):e41–63. doi:10.1016/j.hrthm.2015.03.029
11. Freeman R, Wieling W, Axelrod FB, et al. Consensus statement on the definition of orthostatic hypotension, neurally mediated syncope and the postural tachycardia syndrome. Clin Auton Res. 2011;21(2):69–72. doi:10.1007/s10286-011-0119-5
12. United States National Academy of Medicine. Beyond Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: redefining an Illness. In: The National Academies Collection: Reports Funded by National Institutes of Health. Washington, DC, USA: NAM; 2015.
13. Tate W, Walker M, Sweetman E, et al. Molecular Mechanisms of Neuroinflammation in ME/CFS and Long COVID to Sustain Disease and Promote Relapses. Front Neurol. 2022;13:877772. doi:10.3389/fneur.2022.877772
14. Lee JS, Sato W, Son CG. Brain-regional characteristics and neuroinflammation in ME/CFS patients from neuroimaging: a systematic review and meta-analysis. Autoimmun Rev. 2024;23(2):103484. doi:10.1016/j.autrev.2023.103484
15. Bastos VC, Greene KA, Tabachnikova A, et al. Cerebrospinal fluid immune phenotyping reveals distinct immunotypes of myalgic encephalomyelitis/chronic fatigue syndrome. J Immunol. 2025;214(7):1539–1551. doi:10.1093/jimmun/vkaf087
16. Walitt B, Singh K, LaMunion SR, et al. Center for Human Immunology, Autoimmunity, and Inflammation (CHI) Consortium Deep phenotyping of post-infectious myalgic encephalomyelitis/chronic fatigue syndrome. Nat Commun. 2024;15:907. doi:10.1038/s41467-024-45107-3
17. National Academies of Sciences, Engineering, and Medicine. A Long COVID Definition: A Chronic, Systemic Disease State with Profound Consequences. Washington, DC: The National Academies Press; 2024. doi:10.17226/27768
18. Bonilla H, Quach TC, Tiwari A, et al. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome is common in post-acute sequelae of SARS-CoV-2 infection (PASC): results from a post-COVID-19 multidisciplinary clinic. Front Neurol. 2023;14:1090747. doi:10.3389/fneur.2023
19. Larsen NW, Stiles LE, Shaik R, et al. Characterization of autonomic symptom burden in long COVID: a global survey of 2,314 adults. Front Neurol. 2022;13:1012668. doi:10.3389/fneur.2022.1012668
20. Blitshteyn S. Autoimmune markers and autoimmune disorders in patients with postural tachycardia syndrome (POTS). Lupus. 2015;24(13):1364–1369. doi:10.1177/0961203315587566
21. Sharma C, Bayry J. High risk of autoimmune diseases after COVID-19. Nat Rev Rheumatol. 2023;19(7):399–400. doi:10.1038/s41584-023-00964-y
22. Blitshteyn S. Neuroinflammation at the Dorsolateral Inferior Medulla: a Possible Central Nervous System Localization for POTS and Long COVID. Biomedicines. 2025;13(1):166. doi:10.3390/biomedicines13010166
23. Blitshteyn S, Whiteson JH, Abramoff B, et al. Multi-disciplinary collaborative consensus guidance statement on the assessment and treatment of autonomic dysfunction in patients with post-acute sequelae of SARS-CoV −2 infection (PASC). PMRJ. 2022;14(10):1270–1291. doi:10.1002/pmrj.12894
24. Miller AH. Depression and immunity: a role for T cells? Brain Behav Immun. 2010;24(1):1–8. doi:10.1016/j.bbi.2009.09.009
25. Arron HE, Marsh BD, Kell DB, Khan MA, Jaeger BR, Pretorius E. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: the biology of a neglected disease. Front Immunol. 2024;15:1386607. doi:10.3389/fimmu.2024.1386607
26. Peluso MJ, Deeks SG. Mechanisms of long COVID and the path toward therapeutics. Cell. 2024;187(20):5500–5529. doi:10.1016/j.cell.2024.07.054
27. Patterson BK, Francisco EB, Yogendra R, et al. Persistence of SARS CoV-2 S1 Protein in CD16+ Monocytes in Post-Acute Sequelae of COVID-19 (PASC) up to 15 Months Post-Infection. Front Immunol. 2022;12:746021. doi:10.3389/fimmu.2021.746021
28. Gunning III WT, Stepkowski SM, Kramer PM, Karabin BL, Grubb BP. Inflammatory Biomarkers in Postural Orthostatic Tachycardia Syndrome with Elevated G-Protein-Coupled Receptor Autoantibodies. J Clin Med. 2021;10(4):623. doi:10.3390/jcm10040623
29. Shin YW, Moon J, Kim T-J, et al. Human leukocyte antigen associations in postural tachycardia syndrome. Ann Clin Transl Neurol. 2019;6(5):962–967. doi:10.1002/acn3.766
30. Franco F, Jaccard A, Romero P, et al. Metabolic and epigenetic regulation of T-cell exhaustion. Nat Metab. 2020;2(10):1001–1012. doi:10.1038/s42255-020-00280-9
31. Low PA, Sandroni P, Joyner M, et al. Postural tachycardia syndrome (POTS). J Cardiovasc Electrophysiol. 2009;20(3):352–358. doi:10.1111/j.1540-8167.2008.01407.x
32. Kharraziha I, Axelsson J, Ricci F, et al. Serum Activity Against G Protein-Coupled Receptors and Severity of Orthostatic Symptoms in Postural Orthostatic Tachycardia. Syndrome J Am Heart Assoc. 2020;9(15):e015989. doi:10.1161/JAHA.120.015989
33. Gunning III WT, Kvale H, Kramer PM, et al. Postural Orthostatic Tachycardia Syndrome Is Associated With Elevated G-Protein Coupled Receptor Autoantibodies. J Am Heart Assoc. 2019;8(18):e013602. doi:10.1161/JAHA.119.013602
34. Watari M, Nakane S, Mukaino A, et al. Autoimmune postural orthostatic tachycardia syndrome. Ann Clin Transl Neurol. 2018;5(4):486–492. doi:10.1002/acn3.524
35. Yu X. Angiotensin II Type 1 Receptor Autoantibodies in Postural Tachycardia. Syndrome J Am Heart Assoc. 2018;7(8):2.
36. Li H, Yu X, Liles C, et al. Autoimmune basis for postural tachycardia. Journal of the American Heart Association. 2014;3(1):e000755. doi:10.1161/JAHA.113.000755
37. Rojas M, Rodríguez Y, Acosta-Ampudia Y, et al. Autoimmunity is a hallmark of post-COVID. J Transl Med. 2022;20(1):129. doi:10.1186/s12967-022-03328-4
38. Wallukat G, Hohberger B, Wenzel K, et al. Functional autoantibodies against G-protein coupled receptors in patients with persistent Long-COVID-19 symptoms. J Transl Autoimmun. 2021;4:100100. doi:10.1016/j.jtauto.2021.100100
39. El-Rhermoul FZ, Fedorowski A, Eardley P, et al. Autoimmunity in Long Covid and POTS. Oxf Open Immunol. 2023;4(1):iqad002. doi:10.1093/oxfimm/iqad002
40. Konstantinov K, von Mikecz A, Buchwald D, Jones J, Gerace L, Tan EM. Autoantibodies to nuclear envelope antigens in chronic fatigue syndrome. J Clin Invest. 1996;98(1996):1888–1896. doi:10.1172/JCI118990
41. Op De Beéck K, Vermeersch P, Verschueren P, et al. Antinuclear antibody detection by automated multiplex immunoassay in untreated patients at the time of diagnosis. Autoimmun Rev. 2012;12(2):137–143. doi:10.1016/j.autrev.2012.02.013
42. Sotzny F, Blanco J, Capelli E, et al. European Network on ME/CFS (EUROMENE). Myalgic Encephalomyelitis/Chronic Fatigue Syndrome - Evidence for an autoimmune disease. Autoimmun Rev. 2018;17(6):601–609. doi:10.1016/j.autrev.2018.01.009
43. Wood E, Hall KH, Tate W. Role of mitochondria, oxidative stress and the response to antioxidants in myalgic encephalomyelitis/chronic fatigue syndrome: a possible approach to SARS-CoV-2 ‘long-haulers’? Chronic Dis Transl Med. 2021;7(1):14–26. doi:10.1016/j.cdtm.2020.11.002
44. Staal J, Blanco LP, Perl A. Editorial: mitochondrial dysfunction in inflammation and autoimmunity. Front Immunol. 2023;14:1304315. doi:10.3389/fimmu.2023.1304315
45. Shaw BH, Stiles LE, Bourne K, et al. The face of postural tachycardia syndrome - insights from a large cross-sectional online community-based survey. J Intern Med. 2019;286(4):438–448. doi:10.1111/joim.12895
46. Dzotsi M, Strohm A, Varshney S, et al. Time-restricted eating improves quality of life, heart rate, and mitochondrial function in patients with postural orthostatic tachycardia syndrome. An open-label pilot study. Sci Rep. 2025;15(1):34345. doi:10.1038/s41598-025-16836-2
47. Blitshteyn S. When POTS is the tip of the iceberg: rare cases of dysautonomia as a possible manifestation of another disorder. Lupus. 2021;30(5):697–701. doi:10.1177/0961203320988585
48. Kanjwal K, Karabin B, Kanjwal Y, Saeed B, Grubb BP. Autonomic dysfunction presenting as orthostatic intolerance in patients suffering from mitochondrial cytopathy. Clin Cardiol. 2010;33(10):626–629. doi:10.1002/clc.20805
49. Blitshteyn S. Is postural orthostatic tachycardia syndrome (POTS) a central nervous system disorder? J Neurol. 2022;269(2):725–732. doi:10.1007/s00415-021-10502-z
50. Khan MS, Miller AJ, Ejaz A, et al. Cerebral Blood Flow in Orthostatic Intolerance. J Am Heart Assoc. 2025;14(3):e036752. doi:10.1161/JAHA.124.036752
51. Wagoner AL, Olson JD, Westwood BM, et al. Children with orthostatic intolerance exhibit elevated markers of inflammation in the dorsal medulla. Am J Physiol Heart Circ Physiol. 2019;317(2):H323–H329. doi:10.1152/ajpheart.00680.2018
52. Rua C, Raman B, Rodgers CT, et al. Quantitative susceptibility mapping at 7 T in COVID-19: brainstem effects and outcome associations. Brain. 2024;147(12):4121–4130. doi:10.1093/brain/awae215
53. Turner S, Khan MA, Putrino D, Woodcock A, Kell DB, Pretorius E. Long COVID: pathophysiological factors and abnormalities of coagulation. Trends Endocrinol Metab. 2023;34(6):321–344. doi:10.1016/j.tem.2023.03.002
54. VanElzakker MB, Bues HF, Brusaferri L, et al. Neuroinflammation in post-acute sequelae of COVID-19 (PASC) as assessed by [11C]PBR28 PET correlates with vascular disease measures. Brain Behav Immun. 2024;119:713–723. doi:10.1016/j.bbi.2024.04.015
55. Greene C, Connolly R, Brennan D. et al. Blood–brain barrier disruption and sustained systemic inflammation in individuals with long COVID-associated cognitive impairment. Nat Neurosci. 2024;27(3):421–432. doi:10.1038/s41593-024-01576-9
56. Miyanohara J, Kakae M, Nagayasu K, et al. TRPM2 Channel Aggravates CNS Inflammation and Cognitive Impairment via Activation of Microglia in Chronic Cerebral Hypoperfusion. J Neurosci. 2018;38(14):3520–3533. doi:10.1523/JNEUROSCI.2451-17.2018
57. Jin H, Li M, Jeong E, et al. A body–brain circuit that regulates body inflammatory responses. Nature. 2024;630(8017):695–703. doi:10.1038/s41586-024-07469-y
58. Leunig A, Gianeselli M, Russo SJ, et al. Connection and communication between the nervous and immune systems. Nat Rev Immunol. 2025;25(12):912–933. doi:10.1038/s41577-025-01199-6
59. Trabanelli S, Akselrod M, Fellrath J, et al. Neural anticipation of virtual infection triggers an immune response. Nat Neurosci. 2025;28(9):1968–1977. doi:10.1038/s41593-025-02008-y
60. Koren T, Yifa R, Amer M, et al. Insular cortex neurons encode and retrieve specific immune responses. Cell. 2021;184(24):5902–5915. doi:10.1016/j.cell.2021.10.013
61. Kim MW, Kipnis J. Glymphatics and meningeal lymphatics unlock the brain-immune code. Immunity. 2025;58(5):1040–1051. doi:10.1016/j.immuni.2025.03.006
62. Borst K, Dumas AA, Prinz M. Microglia: immune and non-immune functions. Immunity. 2021;54(10):2194–2208. doi:10.1016/j.immuni.2021.09.014
63. Braga J, Lepra M, Kish SJ, et al. Neuroinflammation after COVID-19 with persistent depressive and cognitive symptoms. JAMA Psychiatry. 2023;80(8):787. doi:10.1001/jamapsychiatry.2023.1321
64. Tate W, Walker M, Sweetman E, et al. Molecular Mechanisms of Neuroinflammation in ME/CFS and Long COVID to Sustain Disease and Promote Relapses. Front Neurol. 2022;13:877772. doi:10.3389/fneur.2022.877772
65. Renz-Polster H, Tremblay ME, Bienzle D, Fischer JE. The Pathobiology of Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: the Case for Neuroglial Failure. Front Cell Neurosci. 2022;16:888232. doi:10.3389/fncel.2022.888232
66. Ohba T, Domoto S, Tanaka M, et al. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome Induced by Repeated Forced Swimming in Mice. Biol Pharm Bull. 2019;42(7):1140–1145. doi:10.1248/bpb.b19-00009
67. Li H, Zhang G, Zhou L, et al. Adrenergic autoantibody‐induced postural tachycardia syndrome in rabbits. J Am Heart Assoc. 2019;8(19):e013006. doi:10.1161/JAHA.119.013006
68. Smyth NJ, Blitshteyn S. Language Matters: what Not to Say to Patients with Long COVID, Myalgic Encephalomyelitis/Chronic Fatigue Syndrome, and Other Complex Chronic Disorders. Int J Environ Res Public Health. 2025;22(2):275. doi:10.3390/ijerph22020275
69. Ewing AG, Joffe D, Blitshteyn S, et al. Long COVID clinical evaluation, research and impact on society: a global expert consensus. Ann Clin Microbiol Antimicrob. 2025;24(1):27. doi:10.1186/s12941-025-00793-9
70. Davenport TE, Blitshteyn S, Clague-Baker N, et al. Long COVID Is Not a Functional Neurologic Disorder. J Pers Med. 2024;14(8):799. doi:10.3390/jpm14080799
71. Blitshteyn S, Treisman GJ, Ruhoy IS, et al. Postural orthostatic tachycardia syndrome and other common autonomic disorders are not functional neurologic disorders. Front Neurol. 2024;15:1490744. doi:10.3389/fneur.2024.1490744
72. Nutma E, Willison H, Martino G, Amor S. Neuroimmunology - the past, present and future. Clin Exp Immunol. 2019;197(3):278–293. doi:10.1111/cei.13279
73. Blitshteyn S, Funez-dePagnio G, Szombathy A, Hutchinson M. Immunotherapies for postural orthostatic tachycardia syndrome, other common autonomic disorders and Long COVID: current state and future direction. Front Cell Infect Microbiol. 2025;15. doi:10.3389/fcimb.2025.1647203.
74. Weinstock LB, Afrin LB, Reiersen AM, et al. Prevalence and treatment response of neuropsychiatric disorders in mast cell activation syndrome. Brain Behav Immun Health. 2025;48:101048. doi:10.1016/j.bbih.2025.101048
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.