")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 15
Posttraumatic Stress Disorder and Associated Factors Among Drivers Surviving Road Traffic Crashes in Southwest Ethiopia
Authors Alenko A , Berhanu H , Tareke AA , Reta W , Bariso M , Mulat E , Kenenisa C , Debebe W, Tolesa K, Girma S
Received 9 October 2019
Accepted for publication 5 December 2019
Published 24 December 2019 Volume 2019:15 Pages 3501—3509
DOI https://doi.org/10.2147/NDT.S233976
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Arefayne Alenko,1 Hiwot Berhanu,2 Amare Abera Tareke,2 Wondu Reta,2 Moyeta Bariso,2 Elias Mulat,2 Chala Kenenisa,2 Wondwossen Debebe,2 Kumale Tolesa,3 Shimelis Girma1
1Department of Psychiatry, Faculty of Medical Science, Institute of Health, Jimma University, Jimma, Ethiopia; 2Department of Biomedical Sciences, Faculty of Medical Science, Institute of Health,, Jimma University, Jimma, Ethiopia; 3Department of Ophthalmology, Faculty of Medical Science, Institute of Health , Jimma University, Jimma, Ethiopia
Correspondence: Arefayne Alenko
Jimma University, Institute of Health, Department of Psychiatry, Faculty of Medical Science, Institute of Health, Jimma University, Jimma, Ethiopia Tel +251 96 767 0149
Email [email protected]
Background: Road traffic crashes (RTCs) can cause serious and long-lasting consequences for drivers, both in terms of physical and mental health outcomes. Posttraumatic stress disorder (PTSD) is the most frequent mental disorder occurring after traumatic exposure. Ethiopian drivers experience RTCs more frequently than other sub-Saharan countries. Despite this prevailing phenomenon, limited attention has been given to PTSD among drivers.
Objective: To determine the prevalence of PTSD and associated factors among drivers surviving RTCs in southwest Ethiopia.
Methods: A cross-sectional quantitative study was conducted among 402 male drivers who had survived RTCs. The study was conducted in Jimma zone, southwest Ethiopia from March to June, 2019. All drivers who had survived RTCs in the last year were included in the study. The Trauma Screening Questionnaire was used to determine the prevalence of PTSD. Data were entered in EpiData 3.1 and exported to SPSS 24 for analysis.
Results: The response rate of the study was 398(99%). Fifty of 398 (12.6%, 95% CI 9.5%–16.1%) met PTSD criteria based on the questionnaire. A history of near-miss RTCs (AOR 3.49, 95% CI 1.89–6.43), depression (AOR 3.32, 95% CI 1.36–5.12), and severe-risk cannabis use (AOR 2.51, 95% CI 1.96–7.52) were significantly associated with PTSD.
Conclusion and recommendation: The prevalence of PTSD among drivers surviving RTCs was high compared to the general population. A record of near-miss RTCs, depression, and severe-risk cannabis use shown significant associations with PTSD. Strategies and guidelines must be developed to screen and treat PTSD among drivers surviving RTCs. Drivers with experience of near-miss RTCs, depression, and severe-risk cannabis use should be given priority when screening for PTSD.
Keywords: stress disorders, posttraumatic, traffic crash, prevalence, drivers, Ethiopia
Introduction
A road traffic crash (RTC) is a crash originating from, terminating with, or involving a vehicle partially or fully on a public road that results in property damage, morbidity, and mortality.1 RTCs nowadays are becoming a global public health concern, especially in low- and middle-income countries. According to a World Health Organization (WHO) report in 2015, Ethiopia is one of the 50 countries with the deadliest roads in the world.2 According to the report, RTCs kill more people in African countries and most other sub-Saharan countries than malaria does. RTC fatalities are predicted to be the second-leading cause of disability-adjusted life-years lost (>85% of all fatalities and 90% of disability-adjusted life-years) in developing countries, most of which are African, by the year 2020.3,4 More than 90% of road traffic deaths occur in low- and middle-income countries. RTCs are the leading cause of death for those aged 5–29 years, and 73% of all road traffic deaths occur among young males aged <25 years, who are almost three times as likely to be killed.5
According to a study in northern Ethiopia, from 2007 to 2011 there are 9,255 RTCs registered in the region. A total of 2,761 people died due to the accidents, while 9,062 were severely and mildly injured.6 A study conducted in Burayu, central Ethiopia from July 2010 to June 2015 showed that 533 RTCs resulted in the death of 117 (25%) and injured 345 (75%).7 In 2019, RTCs were the second–most common form of accidents and injuries, accounting for 22.8% of incidents. RTCs contributed to 43.8% of all fatalities, secondary to falling accidents and fighting injuries. Among RTC causalities, 21.9% were drivers.8 As such, drivers are highly affected by RTCs compared to the general population.
RTCs can have serious and long-lasting consequences for survivors, including drivers, both in terms of physical and mental health outcomes.4,9 RTCs have the capacity to provoke anxiety and fear in response to the experience or witness of trauma and finally result in full blown posttraumatic stress disorder (PTSD).10 According to the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders, diagnosis of PTSD is primarily based on recurrent and distressing memories and dreams, persistent avoidance of stimuli associated with the traumatic event, marked sleep difficulty, and hypervigilance. Although PTSD can begin immediately after a traumatic event, it is not diagnosed unless the symptoms last for at least 1 month after trauma and cause either significant distress or functional disability. PTSD occurs in people of any age, sex, and nationality who have been exposed to life-threatening or horrifying events.11 The lifetime prevalence of PTSD in the general population ranges from 1.3% in Japan12 to 2.3% in South Africa.13
PTSD can occur due to deep unconscious intrapsychic conflict resulting from exposure to an overwhelmingly stressful event, such as RTCs.11 Epidemiological studies have found that most RTCs survivor, including drivers, develop PTSD.14–18 The prevalence of PTSD among a group of Iranian commercial motor vehicle drivers was 19.2%.14 The 1-year prevalence of PTSD among South Korean subway drivers was 5.6%.15 A meta-analysis showed that the pooled prevalence of PTSD among RTC survivors was 22.25%. In that study, PTSD prevalence varied from 6.3% to 58.3%.17 The prevalence of PTSD was found to be 22.8% among survivors of RTCs in public hospitals in Addis Ababa, Ethiopia.18 Prevalence rates of PTSD following RTCs vary from 5.6% to 45%.14–18
Not all individuals exposed to RTCs develop PTSD,11 and injury severity is not associated with PTSD.19 Rather, there are risk factors that are associated with the development of PTSD. These are female sex, having poor social support, time since accident (1–3 months), and depression.18 Higher age and job experience and history or familial history of psychiatric disorders are also predictors of developing PTSD. The disease is more prevalent among those with a beginner's driving license.14 Drivers experiencing a sudden stop due to an emergency bell and with a history of a near accident have increased risk of PTSD.15
Untreated PTSD can cause long-term morbidity, functional impairments, and decreased quality of life in terms of health, productivity, and social interaction.11–13 The disorder is associated with such comorbidities as depression and substance abuse, and results in significant economic burden.11,12 Despite this burden, there has been limited research on the prevalence of PTSD and associated factors among drivers who have survived RTCs in sub-Saharan countries. Therefore, this study intended to fill this gap by assessing the prevalence and associated factors of PTSD among drivers who had survived RTCs. This would also help to integrate the mental health status of drivers in the Employers’ Liability Act for make early diagnosis and timely treatment of PTSD.
Methods
Study Design and Period
A cross-sectional quantitative study was conducted in Jimma zone, southwest Ethiopia from March to June 2019.
Study Area and Setting
This study was conducted in Jimma zone, which is located 352 km southwest of Addis Ababa, the capital of Ethiopia. According to a 2007 Ethiopian central statistics report, the population of Jimma was 2,486,155, of whom 1,250,527 were men and 1,235,628 women.20 otal Registered and licensed drivers of public transport under Jimma Zone Transport Authority numbered 6,046: bus and minibus drivers 4,446, three- wheel vehicle (bajaj) drivers 1,352, and taxi drivers 248.
Study Population
Drivers working in public transport in Jimma from July 2018 to May 2019 numbered 6,046. Of these, 402 had experienced an RTC and survived it in that period (Jimma Zone Transport Authority). All these 402 were included in the study (Figure 1). Drivers who had at least 1 year's experience driving and had had mild, moderate, or severe RTCs at least 1 month prior to the study registered on road traffic police reports were included. Drivers who were imprisoned or had left Jimma were excluded.
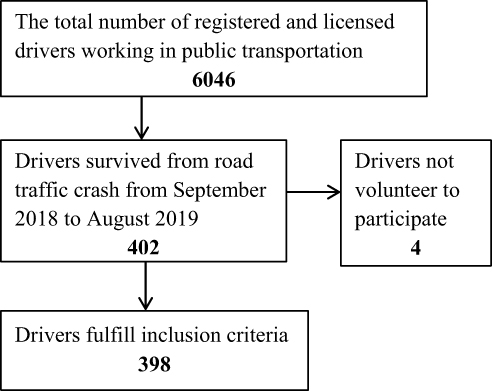 |
Figure 1 Flowchart of selection process of drivers surviving road traffic crashes in southwest Ethiopia, 2019 (n=398). |
Variables
The outcome variable was PTSD. Independent variables were age, marital status, education, driving experience, income, work schedule, hospitalization after accident, death witnessed, time since accident, history of actual RTCs, history of near-miss RTCs, depression, history of mental illness, family history of mental illness, chronic physical illness, alcohol-use risk, khat-use risk, tobacco-use risk, and cannabis-use risk.
Data-Collection Instrument
Data were collected using structured self-administered questionnaires. A questionnaire was prepared in English, translated to the local language Oromo, and back-translated to check whether it had been translated correctly and was understandable to the data collectors. Sociodemographic questionnaires were used to assess drivers’ background information. The Trauma Screening Questionnaire (TSQ) was used to determine the presence of PTSD. The TSQ is a ten-item symptom screen that was designed for use with survivors of all types of traumatic stress, including RTCs, and is based on items from the PTSD Symptom Scale — Self Report, and has five “reexperiencing” items and five “arousal” items. PTSD is “positive” when at least six items are endorsed.21 The TSQ is an effective means to screen PTSD, with sensitivity of 0.85 and specificity 0.89.22 Interrater reliability (κ) of the TSQ in this study was 0.73. Substance-use risk was assessed using the WHO Alcohol, Smoking, and Substance Involvement Screening Test version 3.1.23 The test's risk score ranges 0–31 for tobacco and 0–39 for alcohol and khat (amphetamine-like substance). Total score ranges are for alcohol are 0–10 (low risk), 11–26 (moderate), and ≥27 high risk). Total risk scores for khat, tobacco, and cannabis are similar: low 0–3, moderate 4–26, and high ≥27.24 The Self-Reporting Questionnaire 20 was used to assess depression among drivers. This was developed by the WHO primarily to screen common mental disorders in developing countries,25 has sensitivity of 73%, specificity 82%, and interrater reliability (κ) 0.79,26 and a total score ≥8 is considered to represent depression.25 A near-miss RTC is defined as an event/crash that does not result in physical injury or property damage. Drivers having such an event in the past were considered to have a history of near-miss RTCs. A questionnaire was developed to assess accident-related and clinical factors among drivers. Drivers were approached for data collection at their stations based on information given by the transport office of Jimma zone, town, and district and drivers' associations.
Data Analysis
Data were entered and cleaned using EpiData 3.1 and exported to SPSS 24 for analysis. Descriptive statistics are used to summarize the data and graphs, and statistical summary measures are used for presentation. After getting an overview of the data, simple binary logistic regression was fitted for each explanatory variable, and those variables with p<0.25 were fitted in multiple logistic regressions to get AORs with 95% CIs to identify factors associatedwith (PTSD. p<0.05 was considered statistically significant.
Ethical Considerations
Ethical clearance was obtained from the Jimma University Ethical Review Board. Formal letters were obtained from Jimma Zone Transport Authority and the respective district offices. Written consent was obtained from each participant before data collection. Study participants were informed about the research and their right to cease their involvement at any time. All information was kept confidential.
Results
Sociodemographic and Economic Characteristics
The response rate was 99% (n=398). The mean age of respondents was 32.11±9.133 (20–60 years). Among the respondents, 119 (30%) were in aged 20–30 years. More than half the respondents were married (214, 53.8%) and had completed primary education (218,54.8%). The majority of drivers (238, 59.8%) had a monthly income of ETB2,000–3,000 and driving experience of 1–5 years (238, 59.8%). Most drivers worked day shifts (262, 65.8, Table 1).
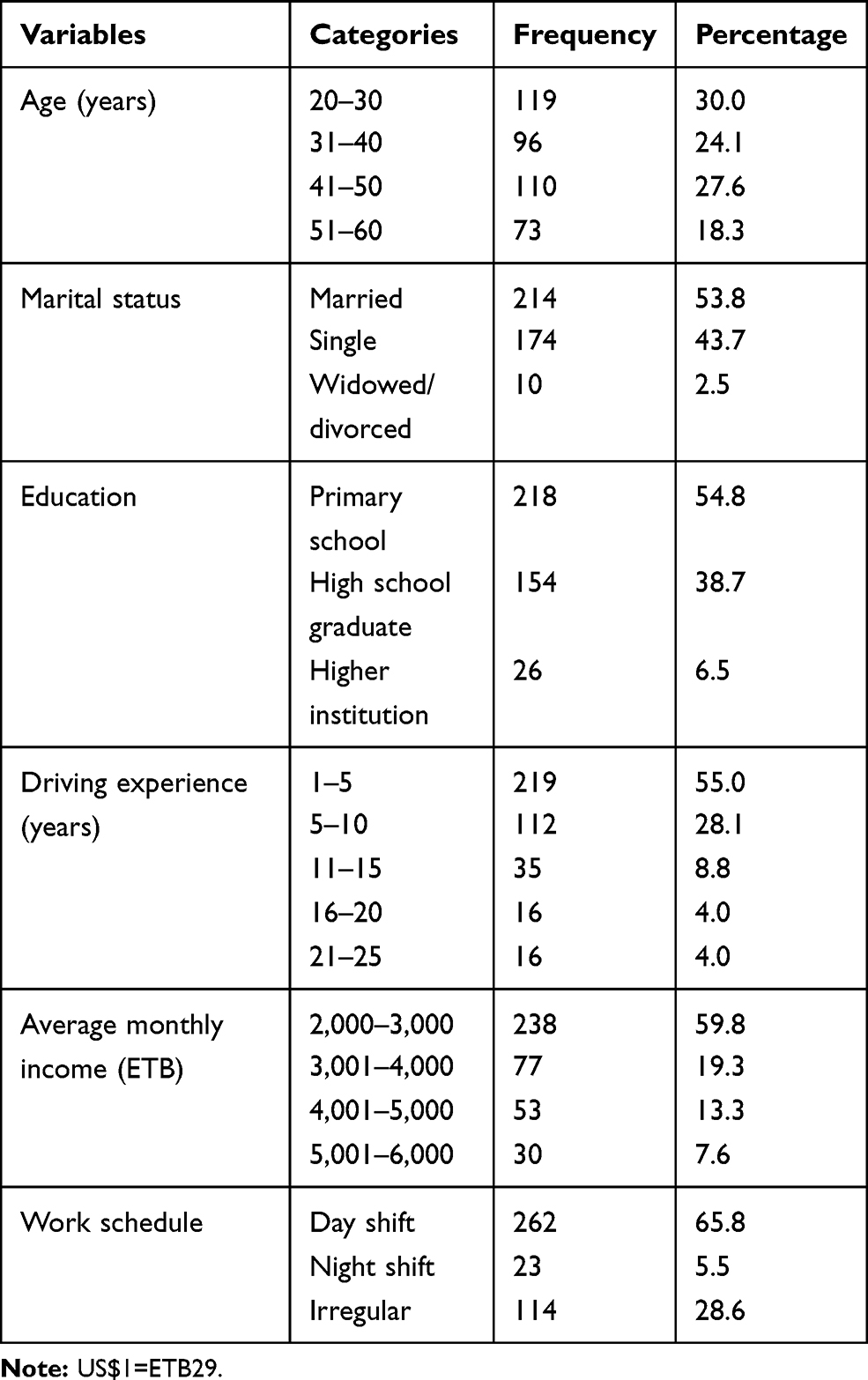 |
Table 1 Sociodemographic and Economic Characteristics of Drivers Surviving Road Traffic Crashes in Southwest Ethiopia, 2019 (n=398) |
Accident-Related and Clinical Factors
Regarding accident-related characteristics, the majority of drivers (267, 68.6%) had been hospitalized after an accident, a third (124, 31.1%) had witnessed the death of someone during accident/crash, 87 (21.8%) had had actual RTCs, and 121 (31.1%) had had near-miss RTCs. In addition, 255 (65.6%) were interviewed 1–3 months after experiencing an RTC. From the total study participants, 104 (26.1%) had depression, 32 (8.2%) had a history of mental illness, 21 (5.4%) had a family history of mental illness, and 43 (11.0%) had a history of chronic physical illness (Table 2).
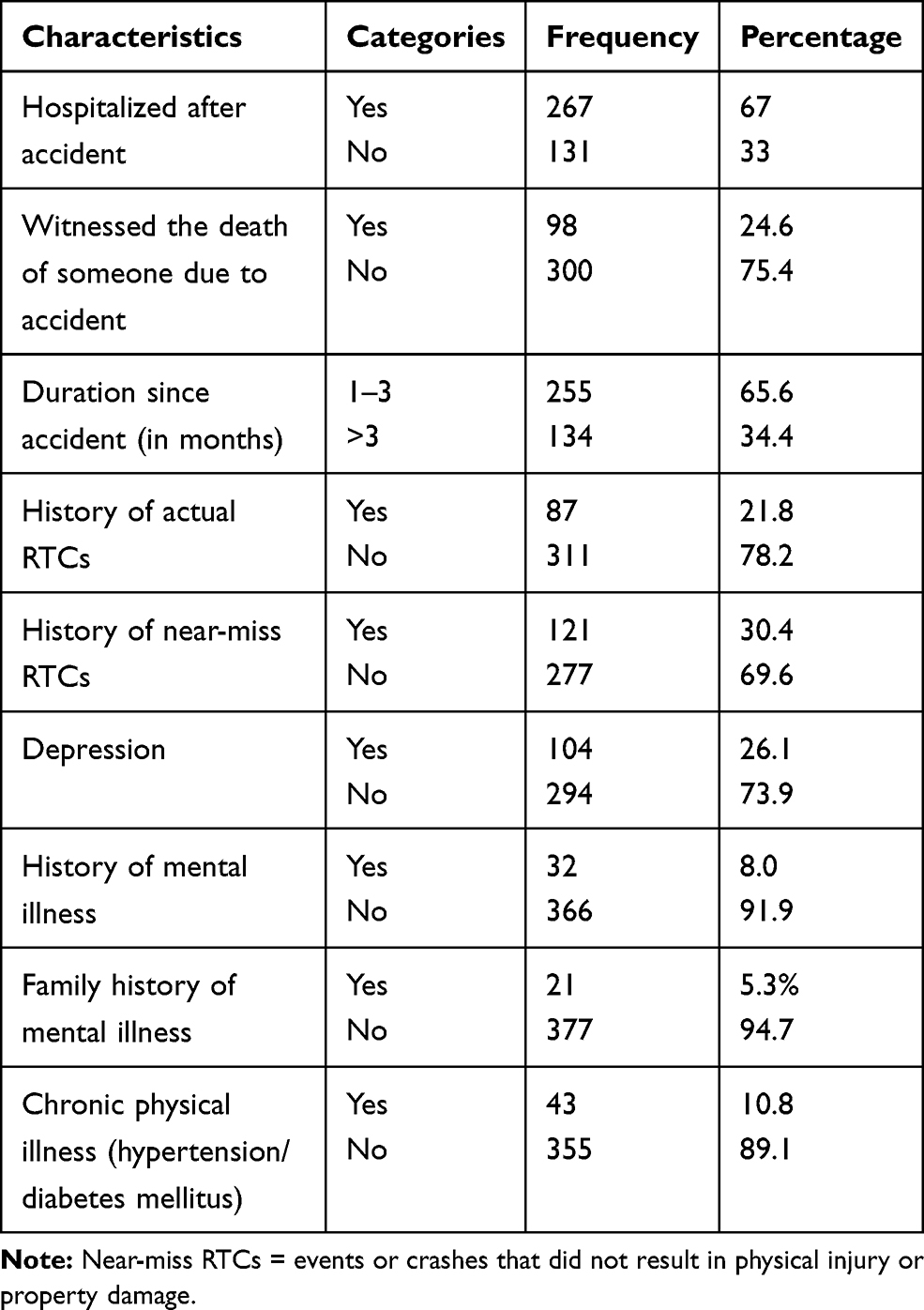 |
Table 2 Accident-related and Clinical Factors Among Drivers Surviving Road Traffic Crashes (RTCs) in Southwest Ethiopia, 2019 (n=398) |
Substance-Use Risk
Regarding alcohol-use risk, 124 (31.2%) had moderate risk and 94 (23.6%) severe risk. A third (131, 32.9%) and half (191, 48.0%) of respondents had severe- and moderate-risk khat use, respectively. In sum, 115 (28.9%) and 97 (24.4%) study participants had moderate- and severe-risk tobacco use, respectively. Regarding cannabis use, 68 (17.1%) had moderate- and 31 (7.8%) severe-risk cannabis use. (Table 3)
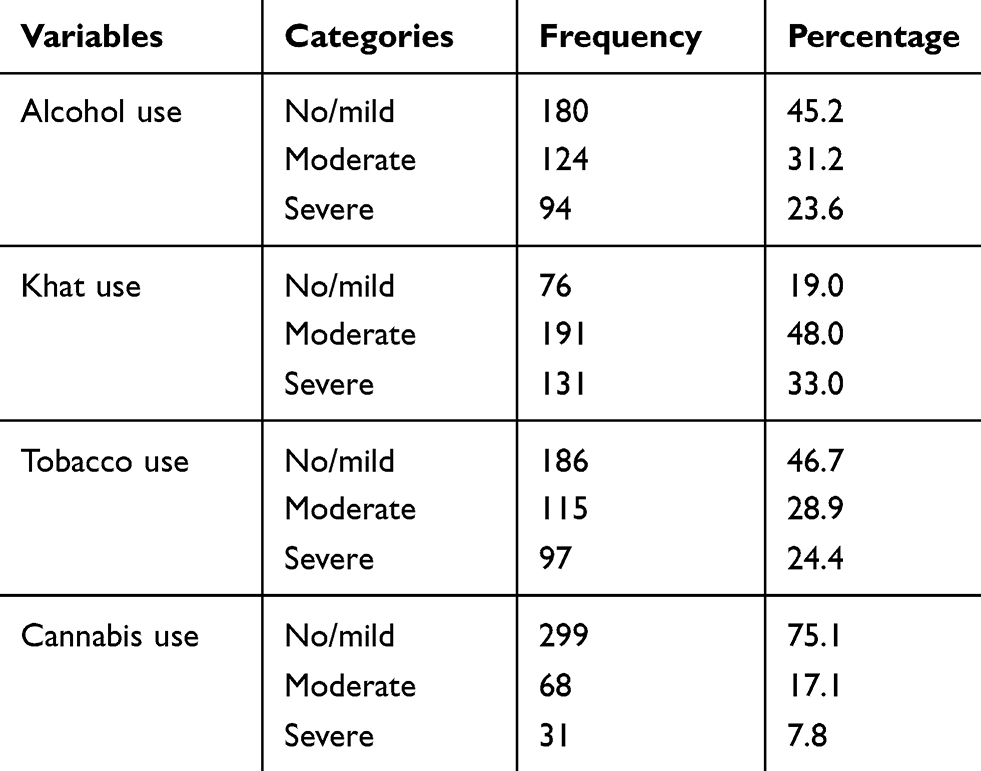 |
Table 3 Substance-use Risk Among Drivers Surviving Road Traffic Crash in Southwest Ethiopia, 2019 (n=398) |
Prevalence of Posttraumatic Stress Disorder
Based on the TSQ, the prevalence of PTSD was found to be 50 (12.6%, 95% CI 9.5%–16.1%) among drivers who had survived an RTC. Among PTSD symptoms, heightened awareness of potential dangers or hypervigilance (24.9%) and difficulty falling asleep (17.6%) were highly prevalent (Figure 2).
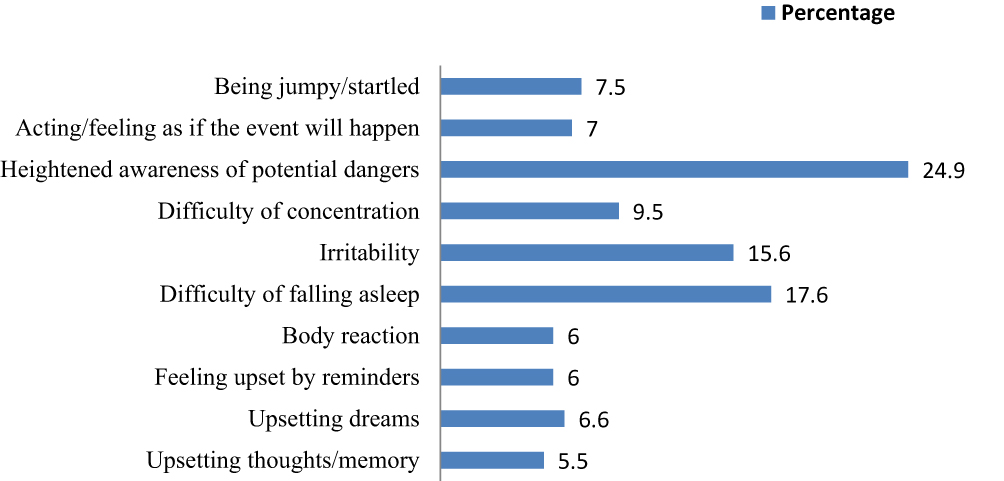 |
Figure 2 Prevalence of posttraumatic stress–disorder symptoms using Trauma Screening Questionnaire among drivers surviving road traffic crash in southwest Ethiopia, 2019 (n=398). |
Factors Associated With Posttraumatic Stress Disorder
Multivariate logistic regression revealed that a history of near-miss RTCs, depression, and severe-risk cannabis use had significant associations with PTSD. Drivers who had a record of near-miss RTCs were more likely to develop PTSD than who with no record of RTCs (AOR 3.49, 95% CI 1.89–6.43), odds of developing PTSD among those with depression were 3.3 times higher than those without depression (AOR 3.32, 95% CI 1.36–5.12), and drivers who had severe-risk cannabis use were 2.5 times as likely to develop PTSD than their counterparts (AOR 2.51, 95% CI 1.96–7.52, Table 4).
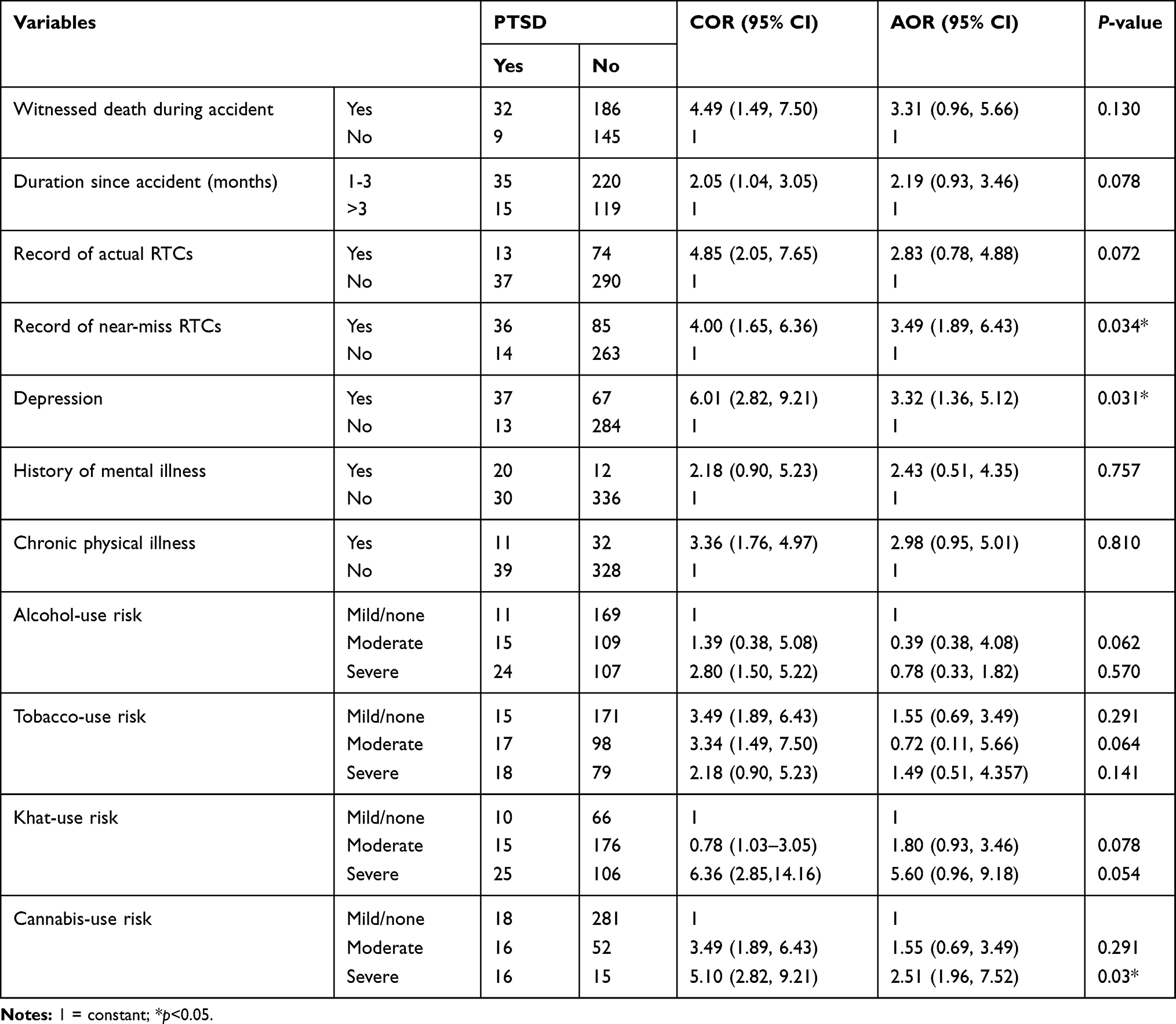 |
Table 4 Bivariate and Multivariate Analysis of Factors Associated with Posttraumatic Stress Disorder (PTSD) Among Drivers Surviving Road Traffic Crashes (RTCs) in Southwest Ethiopia, 2019 (n=398) |
Discussion
Prevalence of Posttraumatic Stress Disorder
In this study, the prevalence of PTSD among drivers surviving RTCs and its possible associations with different variables was assessed. The findings from the current study revealed a significant proportion of drivers who surviving RTCs had PTSD. The prevalence of PTSD was found to be 12.6% (95% CI 9.5%–16.1%) among drivers surviving RTCs. The findings of this study are in line with one done in Canada among bus drivers (14.3%),27 and also agree with a studies conducted among RTC survivors attending orthopedic and trauma clinics in Kenya (13.3%)28 and Cape Town (12.2%).29 However, the proportion in this study was lower than others among a group of Iranian commercial motor-vehicle drivers (19.2%),14 survivors of RTCs in public hospitals in Addis Ababa (22.8%),18 and Nigerians (26.7%).30 The magnitude of PTSD among drivers surviving RTCs varies widely as a result of the country of study, sample-size differences, the time point of PTSD screening and diagnosis, and tools used to assess PTSD, evidenced by the variation in PTSD prevalence in a meta-analysis.17 Contrarily, the finding of this study was higher than the 1-year prevalence of PTSD among South Korean subway drivers (5.6%).15 A possible explanation for the observed differences could be the difference in tools used. The South Korean study used the Korean version of the Composite International Diagnostic Interview to screen PTSD, but the current study used the TSQ Also, the South Korean study conducted among all subway drivers, whereas the current study included only drivers who had survived RTCs.
Factors Associated with Posttraumatic Stress Disorder
This study revealed that factors associated with PTSD among drivers surviving RTCs were a record of near-miss RTCs, depression, and severe-risk cannabis use. The odds of developing PTSD among drivers who had a record of near-miss RTCs was three and a half times (AOR 3.49, 95% CI 1.89–6.43) that of drivers with no records of near-miss RTCs. A near-miss RTC is when drivers are involved in an accident where they think they will die or be badly hurt, but are not.31 This can cause emotional harm and create disturbing reactions. Near-miss RTCs create persistent thoughts about the incident. When drivers face a moment of danger, the instinctive mechanisms of the brain and body create a state of high alert that prepares for survival. Drivers with near-miss RTCs also have heightened senses, which make them act instinctively (without thinking or reasoning) and react and make decisions much more quickly than usual, as there is no time for emotion or to make sense of the event. Due to this, drivers with near-miss RTCs are highly exposed to severe accidents and end up with PTSD.31 The other possible mechanism is that even though the threatened event or anticipated outcome of death or injury does not occur, the danger is replaced by unfamiliar and demanding experiences requiring mental health intervention. When this need for intervention is unmet, confusion reigns, leaving drivers stuck in that terrible moment deep down and putting them at risk of developing PTSD. This is supported by the study conducted among subway drivers in South Korea, in which having a history of a near-miss accident increased the risk of PTSD.15
In addition, depression was significantly associated with the presence of PTSD in this study. The odds of developing PTSD among drivers with depression were 3.3 times (AOR 3.32, 95% CI 1.36–5.12) higher than those without depression. This could be due to the fact that having another psychiatric diagnosis increases the risk of developing PTSD and poor long-term health outcomes, including impaired physical functioning and lower self-reported quality of life, may contribute. Preexisting untreated depression can put individuals at risk of PTSD when exposed to traumatic life events, such as RTCs.11 Comorbidity rates are high among individuals with PTSD, with about two-thirds having at least two other psychiatric disorders, such as major depressive disorder.32 The current finding was supported by studies conducted in Addis Ababa,18 Cape Town,29 and Nigeria.30
Furthermore, severe-risk cannabis use was found to be significantly associated with PTSD. The odds of developing PTSD among drivers with severe-risk cannabis use were 2.5 times (AOR 2.51, 95% CI 1.96, 7.52) those with mild- and moderate-risk cannabis use. A possible reason is that individuals with PTSD use cannabis as self-medication. For example, it has been found that veterans with PTSD who also use cannabis say that cannabis is used specifically to reduce their PTSD symptoms, particularly intrusive thoughts and memories, sleep problems, and hyperarousal.33 In addition, studies have also found that PTSD symptoms are associated with cannabis use to cope with unpleasant emotions, such as anxiety and sadness.34
Strengths and Limitations
The study has a couple of strengths. First, it included all drivers from a well-defined catchment area. Second, we used the standardized instrument for measuring PTSD. A limitation of the study is that since the study assessed only drivers with RTCs, the results are difficult to generalize to drivers without RTCs. Other different traumas that could have occurred in drivers’ lifetimes were not taken into account. Another limitation is that due to the cross-sectional nature of the study, associations between different factors and PTSD do not imply cause and effect.
Conclusion
In the current study, the prevalence of PTSD among drivers surviving RTCs was high compared to the general population. A record of near-miss RTCs, depression, and severe-risk cannabis use showed significant associations with PTSD. Road and transport authorities should develop strategies and guidelines to screen and treat PTSD among drivers who have survived RTCs, in order to improve the quality of life of drivers and to ensure passengers’ safety in case they return to driving. Further research using diagnostic tools should be conducted to strengthen the current findings.
Data-Sharing Statement
The data sets used and analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
The authors acknowledge Jimma University Institute of Health for funding the study. The Jimma Zone Transport Office, study participants, and data collectors are also highly acknowledged.
Author Contributions
All authors contributed to data analysis and drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Ethics Approval and Consent to Participate
Ethical approval was obtained from the Institutional Review Board of Jimma University Institute of Health. Drivers who agreed to participate gave written consent. Confidentiality was maintained by omitting identifiers from study tools, and privacy was ensured during interviews. Participants were informed that involvement in this study had no financial or political benefit, and would not affect their career (driving). All participants were given an information sheet, and were included in the study only after providing informed consent.
Disclosure
The authors declare that they have no competing interests.
References
1. WHO. Global Status Report on Road Safety: Time for Action. Geneva: World Health Organization; 2009.
2. The Economist. Road deaths in Africa Worse than malaria. October 24 2015.
3. Nantulya VM, Reich MR. The neglected epidemic: road traffic injuries in developing countries. Br Med J. 2002;7346:1139. doi:10.1136/bmj.324.7346.1139
4. Hassen A, Godesso A, Abebe L, Girma E. Risky driving behaviors for road traffic accident among drivers in Mekele city, Northern Ethiopia. BMC Res Notes. 2011;4(1):535. doi:10.1186/1756-0500-4-535
5. World Health Organization. Road traffic injuries. December 7 2018.
6. Mekonnen FH, Teshager S. Road traffic accident: the neglected health problem in Amhara National Regional State, Ethiopia. Ethiop J Health Dev. 2014;28(1):3–10.
7. Weldemarium TD. Prevalence of fatality and associated factors of road traffic accidents among victims reported to Burayu town police stations, between 2010 and 2015, Ethiopia. J Transp Health. 2018. doi:10.1016/j.jth.2018.06.007
8. Abegaz T, Gebremedhin S, Useche SA. Magnitude of road traffic accident related injuries and fatalities in Ethiopia. PLoS One. 2019;14(1):e0202240. doi:10.1371/journal.pone.0202240
9. Gopinath B, Jagnoor J, Harris IA, et al. Comparison of health outcomes between hospitalised and nonhospitalised persons with minor injuries sustained in a road traffic crash in Australia: a prospective cohort study. BMJ Open. 2015;5(9):e009303. doi:10.1136/bmjopen-2015-009303
10. Seid M, Azazh A, Enquselassie F, Yisma E. Injury characteristics and outcome of road traffic accident among victims at Adult Emergency Department of Tikur Anbessa Specialized Hospital, Addis Ababa, Ethiopia: a prospective hospital based study. BMC Emerg Med. 2015;15(1):10. doi:10.1186/s12873-015-0035-4
11. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders-Fifth Edition. Washington (DC): American Psychiatric Association; 2013.
12. Kawakami N, Tsuchiya M, Umeda M, et al. Trauma and posttraumatic stress disorder in Japan: results from the World Mental Health Japan Survey. J Psychiatr Res. 2014;53:157–165. doi:10.1016/j.jpsychires.2014.01.015
13. Atwoli L, Stein DJ, Williams DR, et al. Trauma and posttraumatic stress disorder in South Africa: analysis from the South African Stress and Health Study. BMC Psychiatry. 2013;13:182. doi:10.1186/1471-244X-13-182
14. Saberi HR, Abbasian H, Motalebi Kashani M, Naseri Esfahani AH. Post-traumatic stress disorder: a neglected health concern among commercial motor vehicle drivers. Int J Occup Environ Med. 2013;4:185–194.
15. Kim S-E, Kim H-R, Park J-I. The association between psychiatric disorders and work-related problems among subway drivers in Korea. Ann Occup Environ Med. 2014;26:39. doi:10.1186/s40557-014-0039-7
16. Craig A, Tran Y, Guest R, et al. Psychological impact of injuries sustained in motor vehicle crashes: systematic review and meta- analysis. BMJ Open. 2016;6:e011993. doi:10.1136/bmjopen-2016-011993
17. Lin W, Gong L, Xia W, et al. Prevalence of posttraumatic stress disorder among road traffic accident survivors. Systematic review and meta- analysis. Medicine. 2018;97:3. doi:10.1097/MD.0000000000009693
18. Yohannes K, Gebeyehu A, Adera T. Prevalence and correlates of post-traumatic stress disorder among survivors of road traffic accidents in Ethiopia. Int J Ment Health Syst. 2018;12:50. doi:10.1186/s13033-018-0229-8
19. Herrera-Escobar P, Al Rafai SS, Seshadri AJ, et al. A multicenter study of post-traumatic stress disorder after injury: mechanism matters more than injury severity. Surgery. 2018;164:1246–1250. doi:10.1016/j.surg.2018.07.017
20. Federal Democratic Republic of Ethiopia. Population Census Commission. Summary and Statistical Report of the 2007 Population and Housing Census Results. Addis Ababa; 2008.
21. Brewin C, Rose S, Andrews B, et al. Brief screening instrument for post-traumatic stress disorder. Br J Psychiatry. 2002;181:158–162. doi:10.1192/bjp.181.2.158
22. Walters J, Bisson JI, Shepherd JP, et al. Predicting post-traumatic stress disorder: validation of the Trauma Screening Questionnaire in victims of assault. Psychol Med. 2007;37:143–150. doi:10.1017/S0033291706008658
23. Humeniuk R, Henry-Edwards S, Ali R, Poznyak V, Monteiro MGV. The Alcohol, Smoking and Substance Involvement Screening Test (ASSIST) Manual for Use in Primary Care. World Health Organization; 2010.
24. Newcombe D, Tanielu-stowers H, Mcdermott R, Stephen J, Nosa V. The validation of the Alcohol, Smoking and Substance Involvement Screening Test (ASSIST) amongst Pacific people in New Zealand. N Z J Psychol. 2016;45(1).
25. Beusenberg M, Orley JH, World Health Organization. Division of Mental Health. A User's guide to the self-reporting questionnaire (SRQ / compiled by M. Beusenberg and J. Orley). World Health Organization, 1994. Available from: https://apps.who.int/iris/handle/10665/61113. Accessed December 16, 2019.
26. Taun T, Harpham T, Huong NT. Validity and reliability of the self-reporting questionnaire 20 items in Vietnam. Hong Kong J Psychiatry. 2004;14(3):15–18.
27. Zhou B, Boyer R, Guay S. Dangerson the road: a longitudinal examination of passenger-initiated violence against bus drivers. Stress Health. 2018;34:253–265. doi:10.1002/smi.2779
28. Ongecha-Owuor F, Kathuku D, Othieno CJ, et al. Post traumatic stress disorder among motor vehicle accident survivors attending the orthopaedic and trauma clinic at Kenyatta National Hospital, Nairobi. East Afr Med J. 2004;81(7):362–366. doi:10.4314/eamj.v81i7.9192
29. Dickov A, Martinović-Mitrović S, Vučković N, et al. Psychiatric consequences of stress after a vehicle accident. Psychiatr Danub. 2009;21(4):483–489.
30. Iteke O, Bakare MO, Agomoh AO, et al. Road traffic accidents and posttraumatic stress disorder in an orthopedic setting in South-Eastern Nigeria: a controlled study. Scand J Trauma Resusc Emerg Med. 2011;19:39. doi:10.1186/1757-7241-19-39
31. Near-miss experiences and traumatic events, Better Health. Department of Health and Human Services - Emergency Management. Available from: www.betterhealth.vic.gov.au.
32. Kaplan & Sadock’s Synopsis of Psychiatry: Behavioral Sciences/Clinical Psychiatry.
33. Wilkinson ST, Stefanovics E, Rosenheck RA. Marijuana use is associated with worse outcomes in symptom severity and violent behavior in patients with posttraumatic stress disorder. J Clin Psychiatry. 2015;76:1–478. doi:10.4088/JCP.14m09475
34. Bettenhauser K, Pilz J, Vollmer LE. Use and effects of cannabinoids in military veterans with posttraumatic stress disorder. Am J Health Syst Pharm. 2015;72:1279–1284. doi:10.2146/ajhp140523
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.