")
Back to Journals » Psychology Research and Behavior Management » Volume 15
Postpartum Maternal Emotional Disorders and the Physical Health of Mother and Child
Authors Dragomir C , Popescu R , Jurca MA, Laza R, Ivan Florian R, Dragomir I, Negrea R, Craina M, Dehelean CA
Received 15 July 2022
Accepted for publication 20 September 2022
Published 7 October 2022 Volume 2022:15 Pages 2927—2940
DOI https://doi.org/10.2147/PRBM.S382073
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mei-Chun Cheung
Cristina Dragomir,1 Roxana Popescu,2,3 Monica Alisa Jurca,4 Ruxandra Laza,5 Roxana Ivan Florian,6 Ion Dragomir,7 Romeo Negrea,8 Marius Craina,9 Cristina Adriana Dehelean10,11
1Doctoral School, University of Medicine and Pharmacy “Victor Babes”, Timisoara, Romania; 2Department II – Microscopic Morphology, Discipline of Cellular and Molecular Biology, University of Medicine and Pharmacy “Victor Babes”, Timisoara, Romania; 3ANAPATMOL Research Center, University of Medicine and Pharmacy “Victor Babes”, Timisoara, Romania; 4County Emergency Clinical Hospital “Pius Brinzeu”, Timisoara, Romania; 5Department XIII, Discipline of Infectious Disease, University of Medicine and Pharmacy “Victor Babes”, Timisoara, Romania; 6Dynata Company, Timisoara, Romania; 7Individual Family Medical Office, Ostroveni, Dolj, Romania; 8Department of Mathematics, Polytechnica University of Timisoara, Timisoara, Romania; 9Department XII - Obstetrics-Gynecology, Discipline of Obstetrics-Gynecology III, University of Medicine and Pharmacy “Victor Babes”, Timisoara, Romania; 10Department of Toxicology and Drug Industry, Faculty of Pharmacy, University of Medicine and Pharmacy, Timisoara “Victor Babes”, Timișoara, Romania; 11FARMATOX Research Centre for Pharmaco-Toxicological Evaluation, University of Medicine and Pharmacy “Victor Babes”, Timisoara, Romania
Correspondence: Roxana Popescu; Cristina Dragomir, University of Medicine and Pharmacy “Victor Babes”, Eftimie Murgu Square, No. 2, Timisoara, 300041, Romania, Tel +40723649886 ; +40753036306, Email [email protected]; [email protected]
Purpose: The purpose of this study is to identify the relationships between postpartum emotional manifestations and various neonatal variables, as well as variables within this category, in the context of hospitalization together after birth.
Patients and Methods: Between 1 March 2020 and 1 September 2020, a cross-sectional research design was used including mother–child couples (112 mothers, 121 newborns - 13 twins/triplets).
Results: Using a t-test for independent samples, we observed: a) the symptoms of depression were more severe in mothers of newborns hospitalized in neonatal intensive care units (NICUs) [t(110) = 4.334)], provided oxygen therapy [t(109.99) = 3.162], born prematurely [t(110) = 3.157], or with adjustment disorders [t(109) = − 2.947] (p < 0.01); b) a similar, for anxiety as a state [t(82.38) = 5.251], t(107.29) = 4.523, t(110) = 3.416, t(109) = − 3.268, p < 0.01], and as a trait was more common [t(80.79) = 4.501, t(108.790) = 4.669, t(109) = − 3.268, p < 0.001] compared to other mothers. Using Pearson’s test (p < 0.001), several very strong correlations were observed between neonatal variables, including number (no.) of days of hospitalization with birth weight (BW) (r = − 0.802), head circumference (HC) (r = − 0.822), and gestational age (GA) (r = − 0.800) and the mother’s postpartum anxiety as a state/trait (r = 0.770). Using Poisson regression, it was observed that anxiety as a state (Λ = 0.020, z = 4.029, p < 0.001) and as a trait (Λ = 0.800, z = 6.160, p < 0.001) stimulated the intensity of symptoms of postpartum depression (optimal models).
Conclusion: Postpartum maternal psychological manifestations were associated with NICU hospitalization, pathology, and some neonatal therapies. We also noticed, that the duration of hospitalization, BW, HC, and GA, were correlated with maternal emotional disorders. Results will facilitate future optimization of birth management and postnatal care.
Keywords: anxiety as a state, anxiety as a trait, attachment, postpartum depression symptoms, newborn at risk, prematurity
Introduction
Pregnancy, birth, and the postpartum period are often pathological and can be associated with the birth of a high-risk newborn. Mothers sometimes suffer from various uncomfortable psychological manifestations such as depression and anxiety.1–3
The global postpartum depression rate is 17.22% (3.4% in the general population), with some differences in the distribution of the conditions in each country and region, depending, for example, on socioeconomic levels, race, and climate.4,5 The prevalence of postpartum depression is 18.80% in Romania (5.00% in the general population), 17.01–21.71% in different regions of the USA (5.90%), 13.53–22.32% in different regions of Asia (4.20%), and 22.99% in Egypt (3.50%).4–7 Postpartum depression manifests itself through an unjustified fear of self, child and partner, stress, somatization (headache, tinnitus, phosphenes, and abdominal pain), irritability, depersonalization, frequent crying, loss of appetite, bulimia, sleep disturbances, fatigue, indecision, selflessness or concern about one’s appearance, anhedonia, guilt, shyness, panic, and delusions.8,9 Vulnerable categories for postpartum depression include teenage mothers, surrogate mothers (women who agree to become pregnant, give birth, and have their children raised by other families/individuals as their own children), and those who give anonymous birth (or confidential birth, which is a birth where the mother gives birth to a child without disclosing or registering her identity).10,11
Another maternal psychological manifestation is postpartum anxiety, which occurs with a prevalence of 13–40% (4% in the general population).12,13 The prevalence of postpartum anxiety is 33.70% in Romania (23.80% in the general population), 25–50% in the USA (19.10%), 15.20% in Asia (25.80%), and 10% in Egypt (21.20%).14–21 Anxiety is a condition with different signs such as tremors, facial erythema and/or pallor, dyspnea, tachycardia, palpitation, sweating, and paresthesias, as well as symptoms of fear, hypoprosexia, hypervigilance, insomnia, anhedonism, and digestive disorders.22 Anxiety can be seen as both a condition (temporary characteristic) and a trait (general characteristic).23
The pioneer of attachment theory, John Bowlby, defined genetically programmed attachment as a special emotional relationship that involves an exchange of comfort, pleasure, and care between mother and child.24 The second pioneer of this theory, Mary Ainsworth, performed the so-called foreign procedure (originally the foreign experiment) and observed the child’s coping strategies for separation anxiety (internal work patterns) by activating the attachment system.25 Guided by the attachment styles of the child, attachment in intimate relationships was classified as either a secure, avoidant, or anxious attachment style.26
The family and, especially, the mother, who each have their own belief systems in the sociocultural context of Romania are sometimes on alert if the newborn has problems.27
“Newborn at risk” refers to a child exposed to maternal risk factors such as poverty, smoking, alcohol and/or drug use, malnutrition, disease, obstetric history (for example, women with a history of perinatal death, especially early neonatal death, miscarriages, and stillbirths), and being a mother under 16 or over 35 years of age.28 The fetal risk factors for newborns include prematurity, postmaturity, intrauterine growth restriction, macrosomia, presentation abnormalities, cardiac arrhythmias, oligohydramnios or polyhydramnios, and hyperreactivity. Lastly, birth-related risk factors for newborns include premature or postmature birth, fever, hypotension, precipitous or prolonged labor, and placental pathology.29 Delays in child development can prevent mothers from bonding with the baby.30,31 The admission of infants to neonatal intensive care units can sometimes cause mothers to experience feelings of psychological separation in addition to physical separation.32,33
In the present study, using a sample of mothers and a sample of newborns (mother–infant couples), our goal was to identify the relationships between postpartum emotional manifestations and various neonatal variables, as well as the relationships within the categories of variables, in the context of hospitalization together after birth.
Materials and Methods
Study Participants and Procedure
The present study was conducted according to a cross-sectional research design. The participants consisted of mother–child couples (children), accompanying mothers (n = 112), and their newborns (n = 121, including twins and triplets n = 13). Data for the newborns/infants were selected from the observation sheets during hospitalization at the County Emergency Hospital “Pius Brinzeu” Timisoara, Department of Neonatology, and the Children Emergency Hospital “Louis Turcanu” Timisoara, Department of Neonatology during the period between 1 March 2020 and 1 September 2020. In addition, the accompanying mothers completed both a mother’s file and a form for the newborn, which were specially designed for this study.
Inclusion criteria for mothers in this study were as follows: mothers hospitalized with their newborn/newborns and who fully responded to psychological tests after a patient evaluation. Exclusion criteria for mothers in this study were as follows: being a non-hospitalized mother or a mother who did not respond totally to the psychological tests. Inclusion criteria for newborns/infants were as follows: all those admitted to one of the two above-mentioned clinics during the above-specified period of admission and those who were accompanied by their mothers. Exclusion criteria were as follows: all newborns/infants not accompanied by their mothers.
The psychological instruments were completed by the mothers during hospitalization after giving informed consent. Data from the observation sheets were collected after the newborn and mother were discharged.
Instruments Used for Psychological Assessment of the Accompanying Mothers
Postpartum Depression
Edinburgh Postnatal Depression Scale (EPDS) is a screening instrument used to detect a risk of postpartum maternal depression. Answers receive 0, 1, 2, and 3 points (directly quoted items) and 3, 2, 1, and 0 points (reverse quoted items). The total score obtained at EPDS (maximum 30 points) determines the intensity of the symptoms of postpartum depression and can indicate mild/possible depression (score greater than 10), moderate to severe depression (score greater than 13), or severe depression (score greater than 15).33,34 Cronbach’s alpha is the most common measure of internal consistency (reliability) and determines how closely related a set of items are as a group. This measure was calculated with the SPPS 23 program using mothers’ answers to the items for each psychological scale.35 The Cronbach’s coefficient for EPDS has very good values in the Romanian population (α = 0.89).33 Cronbach’s coefficient α in our study was 0.85, indicating high internal consistency among the scale items.
Postpartum Anxiety
Spielberger’s Inventory of Anxiety Traits (STAI-Y) includes Anxiety scale S (form STAI Y1) for anxiety as a condition (response scale: 1—not at all, 2—less, 3—moderate, and 4—very much) and Anxiety scale T (form STAI Y2) for anxiety as a trait (response scale: 1—almost never, 2—sometimes, 3—often, and 4—almost always). Each scale has 20 items.36 Depending on the score obtained on each scale (maximum 80 points), anxiety can by mild (score 35 or greater), moderate (score 50 or greater), or severe (score 65 or greater). In our study, the Cronbach’s coefficient had the following values: α = 0.92 for STAI-Y1 and α = 0.92 for STAI-Y2. The analyses showed very good coefficients for the Romanian population for STAI-Y1 (α = 0.92–0.95) and STAI-Y2 (α = 0.85–0.90).36
Attachment in the Couple’s Relationship
Collins and Read Adult Attachment Rating Scale (AAS) evaluates the style of adult attachment within a romantic couple using 18 items, with 6 for each style of attachment. Each item is evaluated on a 5-step scale (1—totally disagree, 2—partially disagree, 3—do not know, 4—partially agree, and 5—totally agree). The arithmetic mean of the scores for each attachment style can then be calculated. In our study, the Cronbach’s coefficient was α = 0.52 for AAS secure, α = 0.57 for avoidant, and α = 0.56 for anxious (low values). The Cronbach’s coefficient for AAS was found to be very good in studies on the Romanian population, with α = 0.95 for secure attachment style, α = 0.94 for avoidance, and α = 0.94 for anxious.37,38
Neonatal Parameters Investigated
Newborns were assessed by birth weight (BW; the first weight of the newborn at birth), length (L; the measurement from the top of the head to the heal of the foot at birth), head circumference (HC; the distance around the newborn’s head at birth), gestational age (GA; describe how far along the pregnancy is), APGAR score, neonatal adjustment, number (no.) of acute episodes, no. of chronic infant diseases, oxygen therapy, hospitalization in a neonatal intensive care unit (NICU), and no. of days of hospitalization.39 The APGAR score is a method for evaluating a newborn immediately after birth (at 1, 5, and even up to 20 minutes if the newborn has values below 7) and includes five components (evaluated with 0, 1, and 2 points each): color, heart rate, reflexes, muscle tone, and respiration.40
Statistical Analysis
The SPSS 23.0 program was used for statistical analyses. Descriptive statistics were used to give information about maternal and neonatal characteristics. Independent samples t-tests were conducted to examine differences between two independent groups when the dependent variable was numerical. Pearson’s correlation analyses were used to give information about the strength and direction or association between numeric variables. Interpretation of the coefficients was performed based on Colton’s rule as follows: a) an absent or very weak correlation with r from −0.25 to −0.25; b) a reasonable correlation with r from −0.50 to −0.25 and r from 0.25 to 0.50; c) a moderately strong correlation with r from −0.75 to −0.50 and r from 0.5 to 0.75; d) a very strong correlation with r < −0.75 and r > 0.75; e) and a perfect correlation with r = −1 or r = 1. The correlations were considered significant at p < 0.05, very significant at p < 0.01, and extremely significant at p < 0.001.41,42 Subsequently, with the R system, the response variables and their determinants in this study were identified using Poisson regression and multiple regression.43
Results
The Group of Mothers
The mothers had an average age of 29.68 years (14–53 years). The family of origin was nuclear in 75%, cohabitation in 12.50% and extended to 12.50% of mothers. In the terms of mother’s psychiatric history, two woman had antepartum and postpartum major depression (with psychotic symptoms) and were not included in the study. Half of the mothers had a current pathological pregnancy, and their after birth pathology rate was 15.18% [Table 1]. The cesarean section (C-section) rate was 65.17%, and the natural birth rate was 34.83%. Most mothers (77, 68.75%) breastfed, which is beneficial for the immunity of the newborn and for the mother–child couple. Psychological tests showed mothers with different degrees of symptoms of depression, anxiety as a state, and anxiety traits. The mothers responded to the tests on the third day of life postpartum (in the case of a full-term birth) and in the first month postpartum (in the case of a preterm birth). Additionally, the dominant attachment style in the romantic relationship was secure, avoidant, or anxious [Table 1].
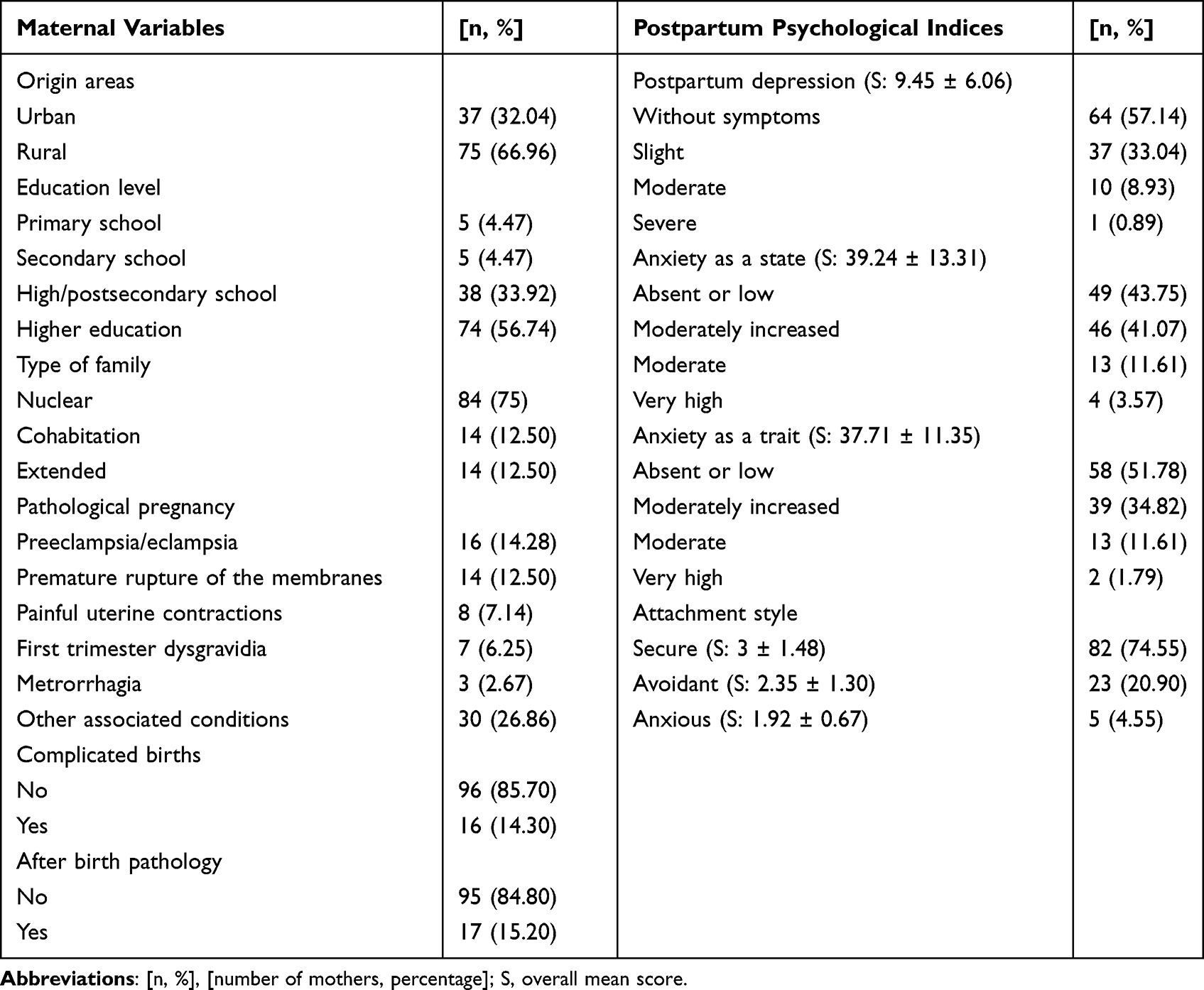 |
Table 1 Descriptive Statistics About Maternal Variables |
The Group of Newborns
The anthropometric indices of the newborns were as follows: average BW of 2575 g (650–4430 g), average L of 47 cm (29–57 cm), average HC of 32 cm (22–38 cm), and average GA of 36 weeks (26–41 weeks). There were 70 (57.85%) boys and 51 (42.15%) girls, as well as 70 (57.85%) full-term and 51 (42.15%) premature newborns. During hospitalization, newborns frequently had acute conditions. The most common episodes were neonatal jaundice in 86 (71.07%), hydroelectrolytic disorders in 51 (42.14%), and eating disorders in 50 (41.32%) [Figure 1]. Additionally, the most common chronic diseases were multifactorial anemia in 57 (47.10%), cerebral hemorrhage in 30 (24.79%), and premature retinopathy in 20 (16.52%) [Figure 2].
 |
Figure 1 Neonatal diseases: acute episodes in hospitalized infants. |
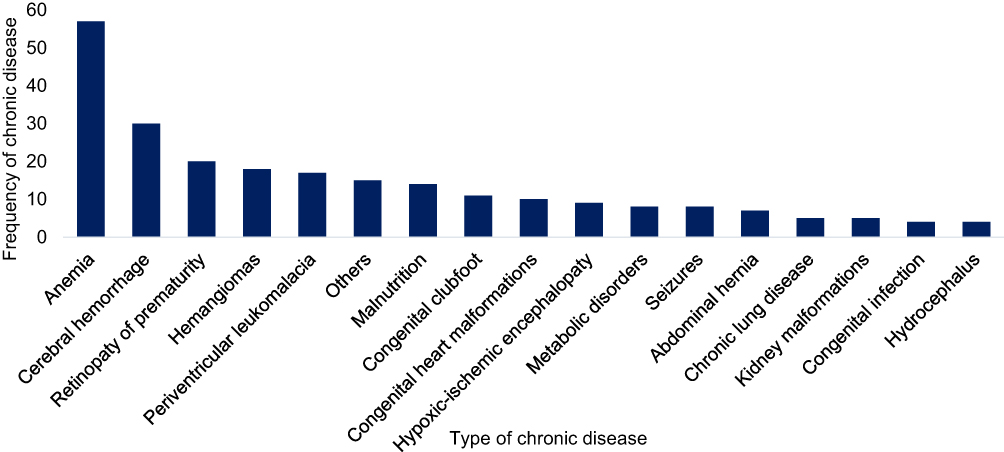 |
Figure 2 Neonatal diseases: chronic diseases in hospitalized infants. |
The duration of hospitalization of mothers and newborns (during the study) was 2–128 days, and 56 (46.28%) of the infants were hospitalized in a NICU.
Relations Between Different Variables
By applying a t test for independent samples (p < 0.05), we found significant differences in the mother’s postpartum mental health depending on the particularities of the newborns: a) The symptoms of depression were more frequent and more severe in mothers of newborns hospitalized in a NICU [t(110) = 4.334, p < 0.001)], those who required oxygen therapy [t(109.99) = 3.162, p = 0.002], those were premature [t(110) = 3.157, p = 0.002], and those with neonatal adjustment disorders [t(109) = −2.947, p = 0.004] compared to other mothers; b) anxiety as a state was more severe among mothers with newborns hospitalized in a NICU [t(82.38) = 5.251, p < 0.001], those who required oxygen therapy [t(107.29) = 4.523, p < 0.001], those who were premature [t(110) = 3.416, p = 0.001], and those with neonatal adjustment disorders [t(109) = −3.268, p = 0.002] compared to the others; and c) anxiety as a trait was more common among mothers of newborns hospitalized in a NICU [t(80.79) = 4.501, p < 0.001], those who required oxygen therapy [t(108.790) = 4.669, p < 0.001], and those with neonatal adjustment disorders [t(109) = −3.268, p < 0.001] compared to mothers that did not fall into these categories. The most severe symptoms of depression, anxiety as a state, and anxiety as a trait are highlighted in Figures 3–5.
 |
Figure 3 Postpartum maternal psychological manifestations: level (score) of intensity of postpartum depression symptoms. |
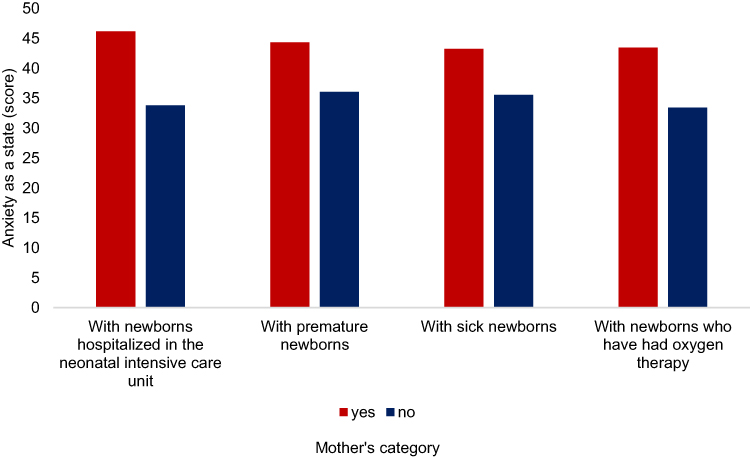 |
Figure 4 Postpartum maternal psychological manifestations: level (score) of anxiety as a state. |
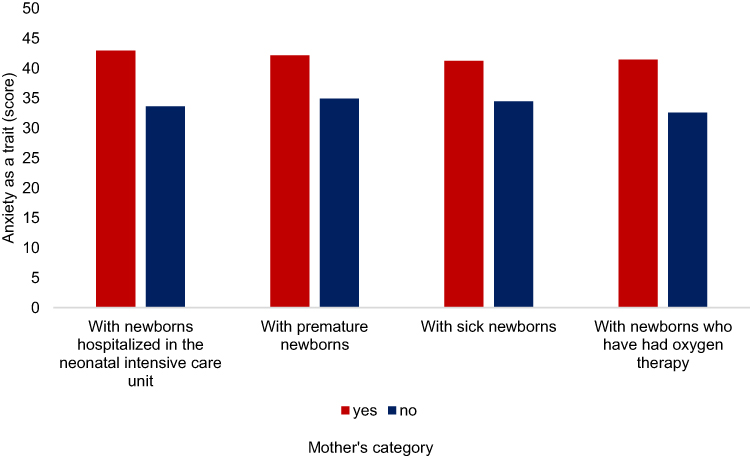 |
Figure 5 Postpartum maternal psychological manifestations: level (score) of anxiety as a trait. |
By applying a bilateral Pearson’s r test, a number of correlations were observed regarding the mother’s postpartum psycho-affective levels. We observed very strong correlations between the two forms of anxiety (r = 0.770, p < 0.001) and moderately strong correlations between postpartum depression and anxiety as a state (r = 0.720, p < 0.001), as well as anxiety as a trait (r = 0.691, p < 0.001) [Table 2]. Similarly, several very strong correlations were observed between neonatal variables (p < 0.001), including BW with HC (r = 0.924) and GA (r = 0.879); GA with HC (r = 0.865); no. of days of hospitalization with BW (r = −0.802), HC (r = −0.822); and GA (r = −0.800) [Table 3]. Reasonable correlations between the mother’s postpartum mental state and the newborn’s state of health were also identified. The intensity of postpartum maternal depression symptoms were correlated with the GA (r = −0.326, p < 0.001), APGAR score (r = −0.329, p < 0.001), no. of chronic diseases (r = 0.300, p <0.001), and no. of days of hospitalization of infants (r = 0.272, p = 0.004); anxiety as a state was correlated with GA (r = − 0.307, p < 0.001), APGAR (r = −0.359, p < 0.001), no. of chronic diseases (r = 0.333, p < 0.001); and no. of days of hospitalization of infants (r = 0.267, p = 0.005). Anxiety as a trait was correlated with APGAR (r = −0.269, p = 0.004) [Table 4].
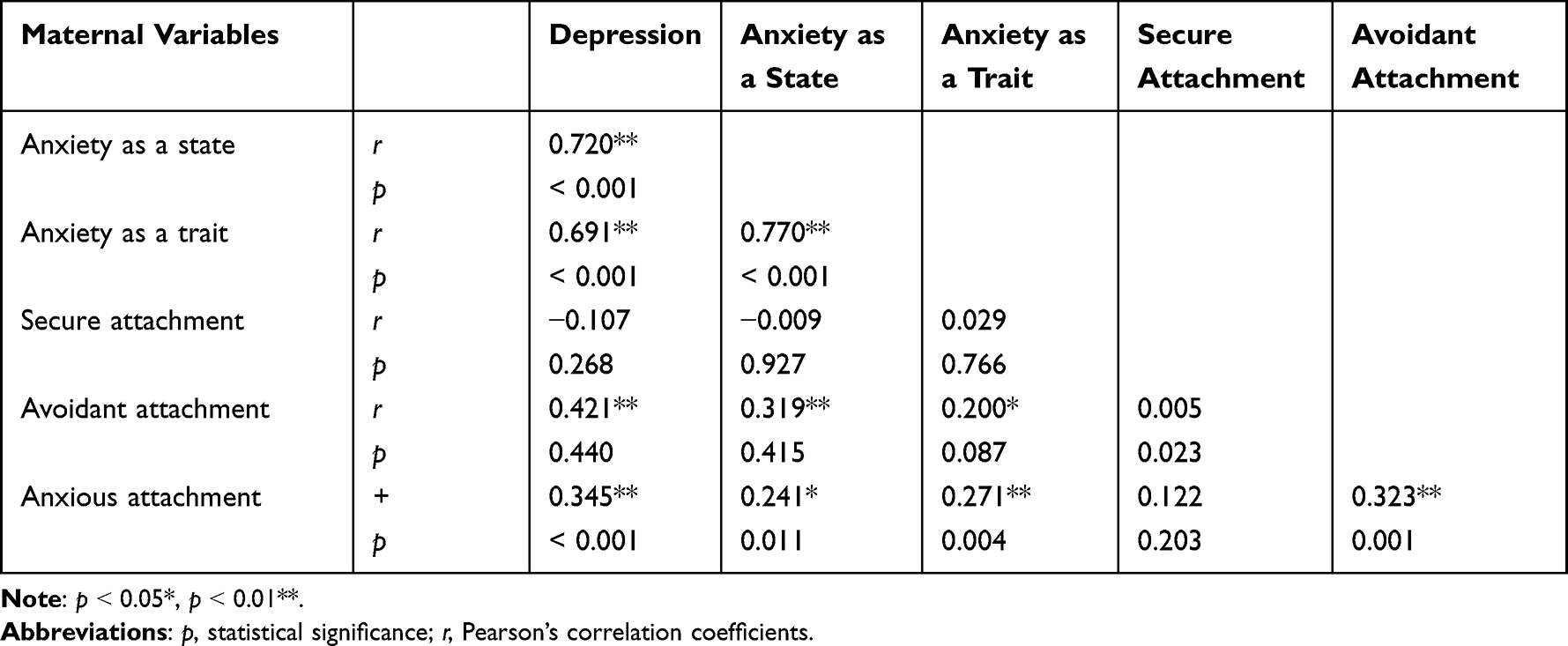 |
Table 2 Correlations Between Postpartum Maternal Psychological Indices |
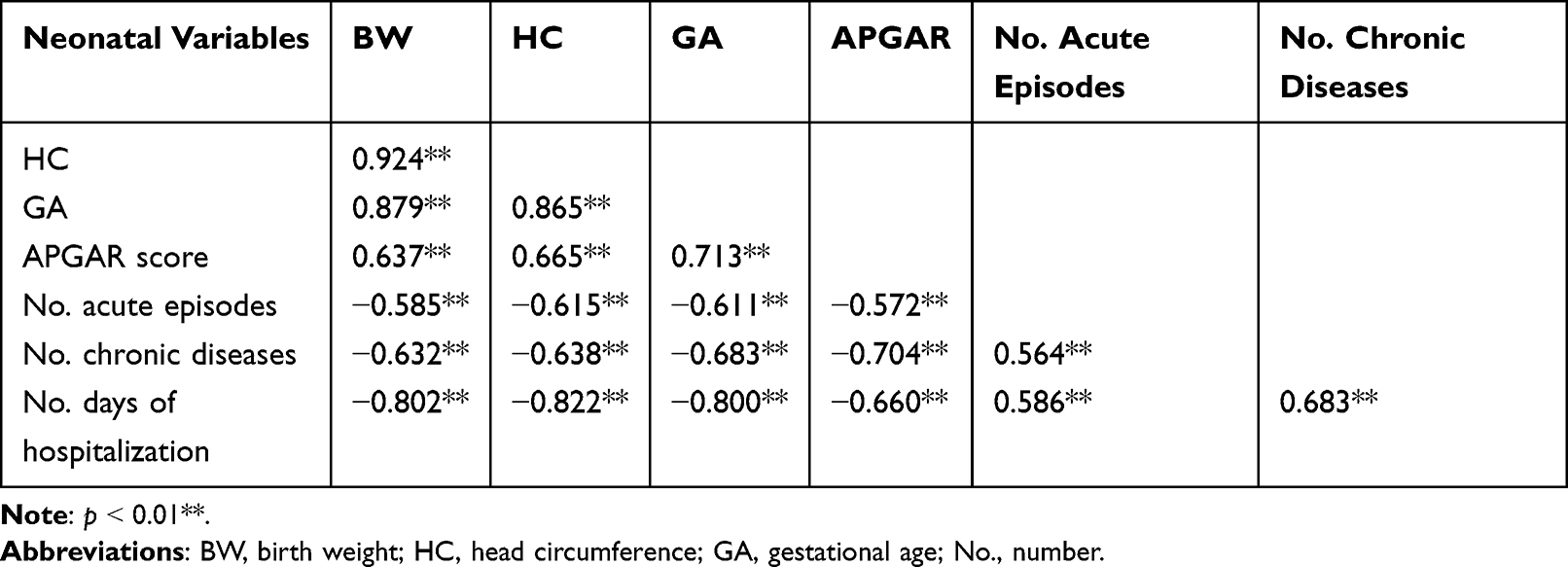 |
Table 3 Correlations Between Neonatal Indices |
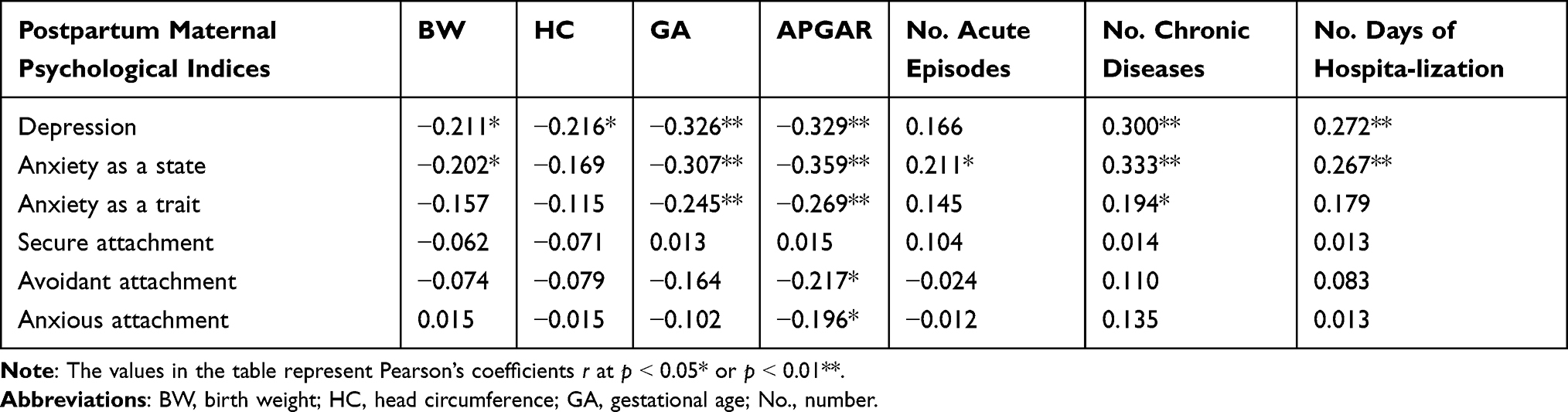 |
Table 4 Correlations Between Postpartum Maternal Psychological Indices and Neonatal Indicators |
Poisson regression was used in cases where the response variable was an a categorical variable; otherwise, we used the multiple linear regression method. Generalized Poisson regression was performed with p as the Poisson variable, and backward selection was also optimized. We observed the following: a) anxiety as a state (Λ = 0.020, z = 4.029, p < 0.001), anxiety as a trait (Λ = 0.800, z = 6.160, p < 0.001), and GA (Λ = −0.077, z = −2.935, p < 0.001) were determinants (the stimulus variables) of the intensity of symptoms of postpartum depression, and the first two Poisson regression models were optimal; and b) the APGAR score was a determinant of anxiety as a state (Λ = −0.096, z = −2.895, p = 0.003) and a trait (Λ = 0.056, z = −1.521, p = 0.128) [Table 5]. Multiple regression was also applied, indicating that avoidant attachment is a determinant of anxious attachment (R2 = 0.157, R2adj = 0.150, p << α, at α < 0.05) and that HC and no. of chronic diseases are determinants for no. of days of hospitalization of the infant–mother couple (R2 = 0.691, R2adj = 0.685, p << α, α < 0.05) [Table 6].
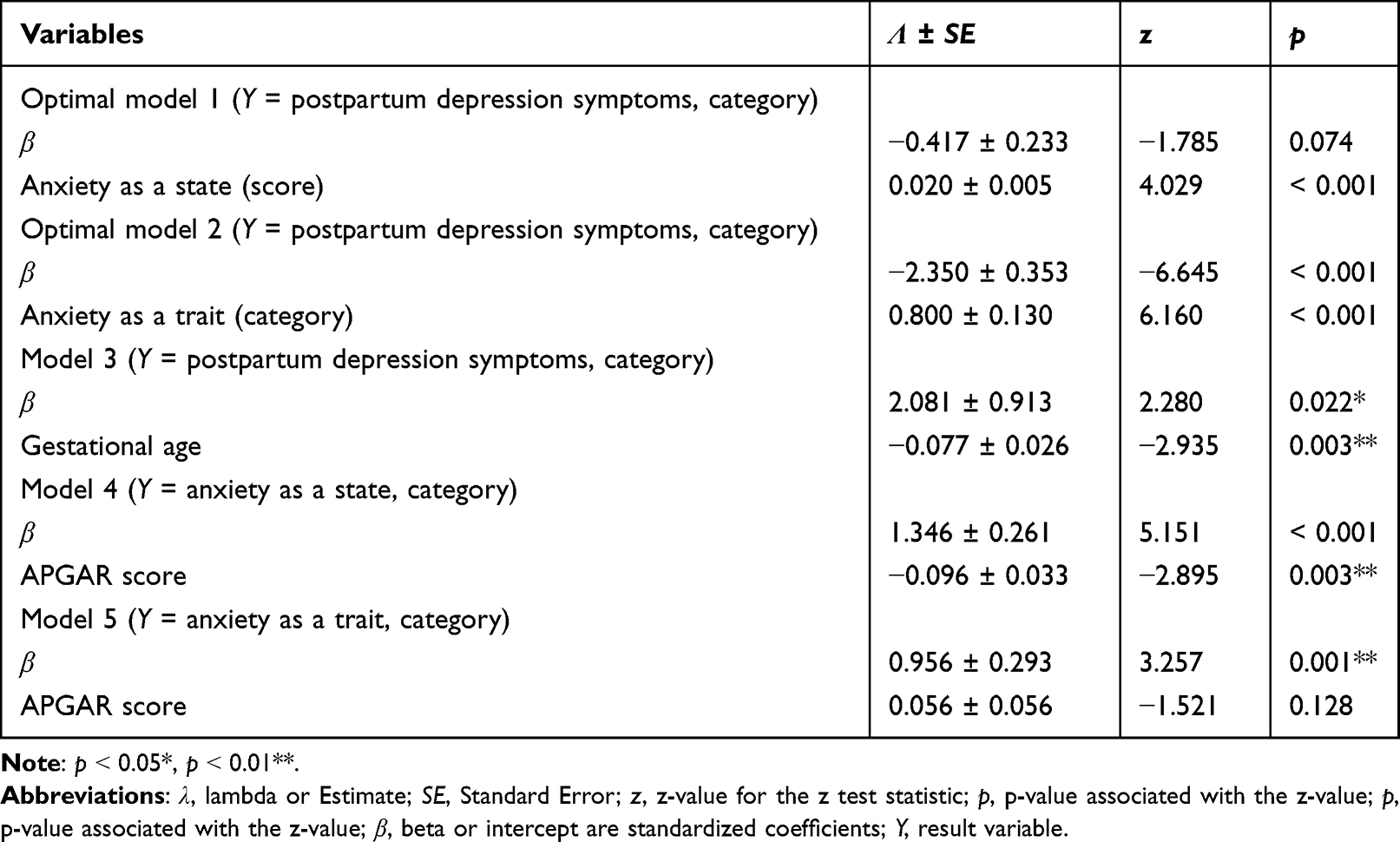 |
Table 5 Results from Poisson’s Regression |
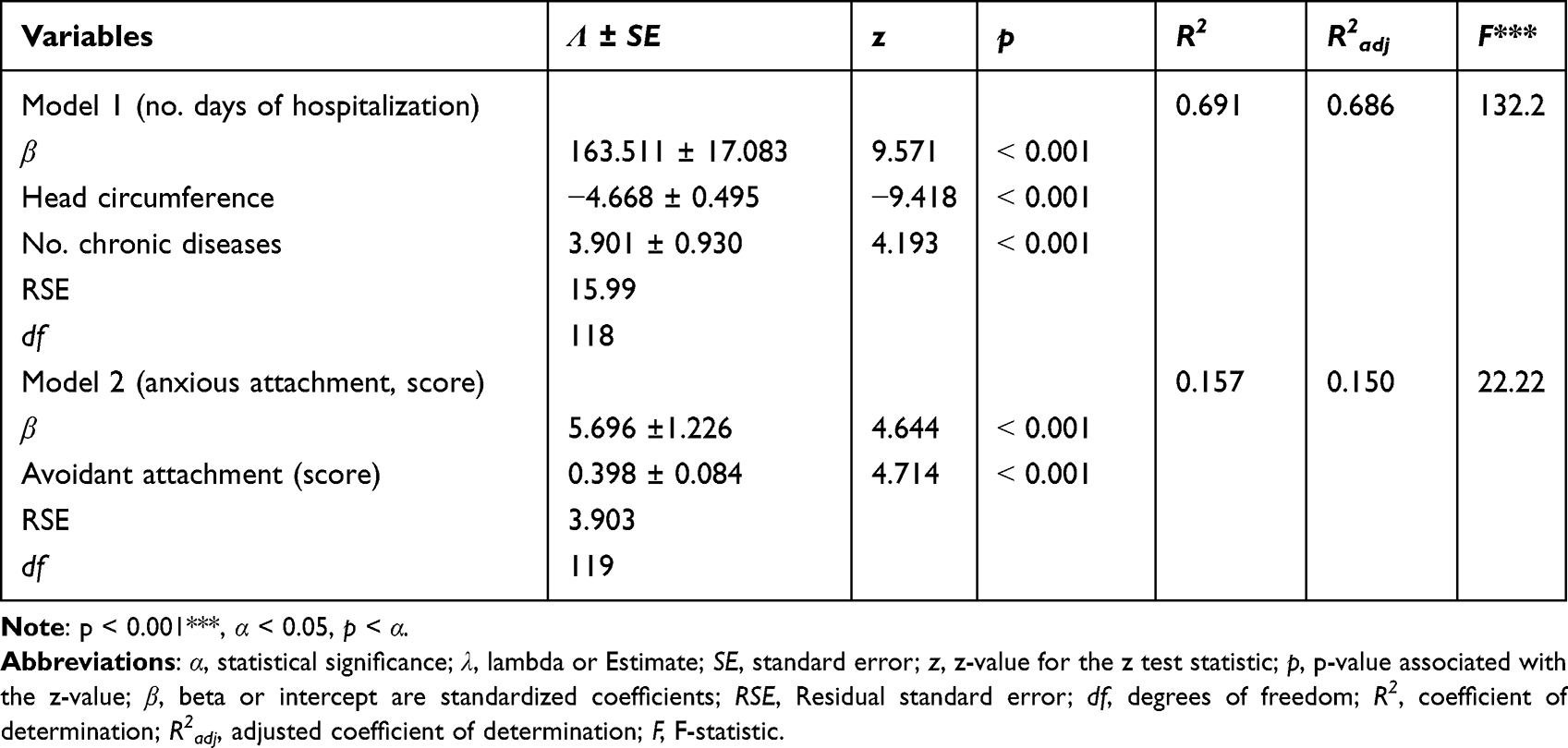 |
Table 6 Results for Multiple Linear Regressions |
Discussion
The high rate of cesarean births in our study has a worldwide correspondence of up to 21% of births and is on the rise according to World Health Organization (WHO) data.44
Pregnancy, childbirth, and the postpartum period are often pathological and lay the groundwork for various psychological manifestations, as well as pathological ones, in the aforementioned proportions. Of the 1406 participants in the study conducted at two university hospitals in the Netherlands, 8% had an EDPS score of ≥ 9 and 14.70% and a STAI score of ≥ 42.36 The authors identified the most important risk factors for postpartum depression and anxiety based on a multitude of risk factors that act prenatally during pregnancy and postpartum, including male newborns, primiparity, low maternal self-efficacy, a history of maternal depression, poor maternal health, a lack of breastfeeding within the first 3 weeks of childbirth, non-initiation of breastfeeding, life events during pregnancy, pregnancy with a pathology, complications at birth, home birth, and alcohol consumption during pregnancy.45
The most common acute neonatal episodes were neonatal jaundice, hydroelectrolytic disorders, and eating disorders. Additionally, the most common chronic diseases among infants were multifactorial anemia, cerebral hemorrhaging, and premature retinopathy. In the study group, the survival rate of newborns was 98.40%. In the literature, survival was 80% and was clearly influenced by GA (survival was 19% at a GA of 23 weeks, and 93% at 28 weeks), BW, and major morbidities such as chronic lung disease, late neonatal sepsis, premature retinopathy, cerebral hemorrhaging, and necrotizing enterocolitis.46–48
The following categories of mothers were identified to have more frequent and severe forms of depressive symptoms, including anxiety as a condition and anxiety as a trait, compared to those who did not fall into these categories: a) mothers whose newborns were hospitalized in the NICU; b) newborns who had oxygen therapy; c) premature newborns; and d) newborns with neonatal adaptation disorders. A review of 366 articles published between 1976 and 2020 in the Scopus database on stress, anxiety, and postpartum depression among mothers of premature newborns admitted to the NICU showed that the stressful environment of the NICU, appearance, and behavior created intense negative feelings for premature babies and also negatively influenced mother–child attachment.49
By applying a bilateral Pearson r test, a number of correlations were identified between the mother’s postpartum psycho-affective variables, including a) very strong correlations between anxiety as a state and a trait; b) moderately strong correlations between postpartum depression with anxiety as a state and a trait; c) reasonable correlations between anxious attachment with postpartum depression, anxiety as trait, and avoidant attachment; and d) weak correlations between secure with avoidant attachment and anxious attachment with anxiety as a state.
Avoidant and anxious attachment, anxiety as a condition and a trait, and the two types of attachment were also associated with the two variants of anxiety, with similar data found in the literature.50–52 A study conducted in Kenya indicated that of the 172 hospitalized children, 44.20% had their depression measured by EPDS (of which 77.60% were mothers of premature babies), 35.10% had anxiety (75% mothers of premature babies), and 25% had associated conditions (83.70% mothers of premature babies).51 The risk factors for this comorbidity were numerous, including a history of depression, psychological distress of the mother, prematurity, violence from the partner, and a lack of social support.53,54 The results of the study showed that avoidant attachment and anxiety were associated with a poor-quality mother–child relationship, which was mediated mainly by maternal distress.
By applying a bilateral Pearson r test, several correlations were observed between neonatal variables, including a) very strong correlation between BW with HC and GA; GA with HC; and no. of days of hospitalization with BW, HC, and GA; b) a moderately strong correlation between BW with APGAR, no. of acute episodes, and no. of chronic diseases; HC with APGAR, no. of acute episodes, and no. of chronic diseases; GA with APGAR, no. of acute episodes, and no. of chronic diseases; APGAR with no. of acute episodes, no. of chronic diseases, and no. of days of hospitalization; no. of acute episodes with no. of chronic diseases; and no. of days of hospitalization, no. of chronic diseases, and no. of days of hospitalization.
The Pearson’s correlation test identified reasonable correlations between the mother’s postpartum mental state and the newborn’s health: the postpartum maternal depression symptoms with GA, APGAR, no. of chronic diseases and no. of days of hospitalization of infants; anxiety as a state with GA, APGAR, no. of chronic diseases, and no. of days of hospitalization of infants; and anxiety as a trait with APGAR. These may be major risk factors for the neuro-psycho-motor development of infants in the study group.46,55
A review that included 81 studies and 132,917 women before becoming pregnant, during pregnancy, and at childbirth showed that the incidence of moderate and severe forms of depression and/or anxiety in 16 studies was 20–64%.50
The application of generalized Poisson regression identified that anxiety as a state, anxiety as a trait, and gestational age are stimulus variables of the symptoms of postpartum depression and that the first two Poisson models are optimal. The APGAR score was found to be a determinant of anxiety as a state and a trait.
With multiple regression, it was identified that avoidant attachment is a stimulus variable for anxious attachment and that HC and no. of chronic diseases are determinants for no. of days of hospitalization of the infant–mother couple.
The Japan Environment and Children’s Study found that postpartum depression in 83,109 mothers (using EPDS) was a predictor of a poor mother-to-child relationship for up to one year of the child’s life (using the Mother-to-Infant Bonding Scale Japanese version, MIBS-J).56 For newborns with prolonged hospitalization (for example, premature newborns), the permanent presence of the mother next to the newborn, which is difficult to achieve in both public and private systems, possibly represents a solution for postpartum depression and anxiety.57–63
Limitations of the Study
The subjectivity of the hospitalized postpartum mothers who participated in the study increased as a result of their postpartum depression and the hospital environment. The Coronavirus Disease 2019 (COVID-19) pandemic, which began during the study, required repeated testing for COVID-19, as well as strict hospitalization and isolation, which severely reduced the number of study participants and created an even more anxious environment than usual, especially for mothers accompanying children hospitalized in the NICU. Available psychological instruments also limited the study—namely, EPDS measures depressive symptoms and cannot indicate the diagnosis. Although the Cronbach’s coefficient α for attachment scales is small, its results were very good in the literature, so we decided to use it.
Study Implications
Those with previous high-risk pregnancies and current high-risk pregnancies are recommended to give birth in highly specialized centers, where the conditions of care and hospitalization for mother and child are of high quality. Pre-pregnancy and post-pregnancy or postpartum psychological disorders may require early multidisciplinary interventions (eg, from a gynecologist, anesthetist, neonatologist, psychologist, and psychiatrist) to prevent possible complications from pregnancy, childbirth, and confinement. Factors related to the behavior of the medical staff involved in supporting the mother–child couple are also important. Several activities can improve the situation of a postpartum mother, such as preventing the occurrence of postpartum maternal mental disorders and detecting postpartum depression at an early stage to determine appropriate solutions.
Conclusion
The symptoms of depression, anxiety as a state and anxiety as a trait were more frequent and severe among mothers of newborns hospitalized in the NICU, those who required oxygen therapy, premature newborns, and those with neonatal adjustment disorders compared to others. Several very strong correlations were observed between no. of days of hospitalization with BW, HC, and GA, as well as between anxiety as both a state and trait. Both forms of anxiety, as a state and a trait, and gestational age were stimulus variables for the intensity of symptoms of postpartum depression. The APGAR score was taken as a determinant of anxiety as a state and a trait, and avoidant attachment was a determinant for anxious attachment. Additionally, HC and no. of chronic diseases were determinants for no. of days of hospitalization of the infant–mother couple. Knowledge of maternal and neonatal pathology, correlations, and determinants can facilitate the optimization of birth and postnatal care management for mothers and newborns, especially in medical systems with limited material resources.
Abbreviations
BW, birth weight; C-section, Cesarean section; COVID-19, coronavirus disease 2019; GA, gestational age; HC, head circumference; L, length; nCPAP, nasal Continuous Positive Airway Pressure; m(Y), mean (result variable); NICU, neonatal intensive care unit; n, number of population; no., number; OTI/MV, orotracheal intubation and mechanical ventilation; p, statistical significance; r, Pearson’s correlation coefficient; R2, coefficient of determination; R2adj, adjusted coefficient of determination; t, statistic t test; z, z-value for the z test statistic; var(Y), variance (result variable); α, Cronbach’s Alpha coefficient; α, statistical significance; β, beta or intercept are standardized coefficients; λ, lambda or Estimate; WHO, World Health Organization.
Data Sharing Statement
The datasets generated/analyzed during the current study are available. The datasets generated/analyzed during the current study are available in the corresponding author repository.
Ethics Statements
This study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee for Scientific Research of the University of Medicine and Pharmacy “Victor Babes” from Timisoara (protocol code No. 07/28.02.2020) and the Local Commission of Ethics in Scientific Research of the County Emergency Clinical Hospital “Pius Brinzeu” from Timisoara with No. 195/15.06.2020.
Consent for Publication
Informed consent was obtained from all subjects involved in the study. Written informed consent was obtained from the patient(s) to publish this paper. For newborns, consent was obtained from mothers, and for mothers younger than the age of majority, consent was obtained from an adult.
Author Contributions
Significant contributions to this work were provided by all authors with respect to the conception, study design, execution, acquisition of data, analysis, and interpretation. All authors took part in drafting, revising, and critically reviewing the article and gave their final approval of the version submitted for publication. All authors have agreed on the journal for submission and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Fernandez DV, Canavaro MC, Moreirra H. Self-compassion and mindful parenting among postpartum mothers during the COVID-19 pandemic: the role of depressive and anxious symptoms. Curr Psychol. 2022. doi:10.1007/s12144-022-02959-6
2. Kuipers YJ, Bleijenbergh R, Van den Branden L, et al. Psychological health of pregnant and postpartum women before and during the COVID-19 pandemic. PLoS One. 2022;17(4):e0267042. doi:10.1371/journal.pone.0267042
3. Beato AF, Albuquerque S, Komurcu Akik B, Costa LP, Salvador A. Do maternal self-criticism and symptoms of postpartum depression and anxiety mediate the effect of history of depression and anxiety symptoms on mother-infant bonding? Parallel-serial mediation models. Front Psychol. 2022;13:858356. doi:10.3389/fpsyg.2022.858356
4. Wang Z, Liu J, Shuai H, et al. Mapping global prevalence of depression among postpartum women. Transl Psychiatry. 2021;11:543. doi:10.1038/s41398-021-01663-6
5. Depression Rates by Country 2022 [homepage on the internet]. Walnut: world population review; 2022. Available from: https://worldpopulationreview.com/country-rankings/depression-rates-by-country.
6. Citu C, Gorun F, Motoc A, et al. Prevalence and risk factors of postpartum depression in Romanian woman during two periods of COVID-19 pandemic. J Clin Med. 2022;11(6):1628. doi:10.3390/jcm11061628
7. Depression [homepage on the internet]. Geneva: World Health Organization; 2021. Available from: https://www.who.int/news-room/fact-sheets/detail/depression.
8. Postpartum depression [homepage on the internet]. Washington: American Psychological Association; 2022. Available from: https://www.apa.org/pi/women/resources/reports/postpartum-depression.
9. Crucianelli L, Wheatley L, Filippetti ML, Jenkinson PM, Kirk E, Fotopoulou A. The mindedness of maternal touch: an investigation of maternal mind-mindedness and mother-infant touch interactions. Dev Cogn Neurosci. 2019;35:47–56. doi:10.1016/j.dcn.2018.01.010
10. Felnhofer A, Kernreiter J, Klier C, Huscsava M, Fiale C, Zeiler M. Anonimous birth: biographical knowledge and diadic coping in adoptive mothers and fathers. Curr Psychol. 2021;38(3):811–820. doi:10.1007/s12144-021-01620-y
11. Van Gasse D, Mortelmans D. With or without you – starting single-parent families: a qualitative study on how single parents by choice reorganise their lives to facilitate single parenthood from a life course perspective. J Fam Issues. 2020;41:2223–2248. doi:10.1177/0192513X20911971
12. Field T. Postpartum anxiety prevalence, predictors and effects on child development: a review. J Psychiatry Psychiatric Disord. 2017;1:86–102. doi:10.1016/j.infbeh.2018.02.005
13. Fleming S. This is the world's biggest mental health problem-and you might not have heard of it. Geneva: Mental Health; 2019. Available from: https://www.weforum.org/agenda/2019/01/this-is-The-worlds-biggest-mental-health-problem/.
14. Enatescu I, Craina M, Gluhovsci A, et al. The role of personality dimensions and trait anxiety in increasing the likelihood of suicide ideation in woman during the perinatal period. J Psychosom Obstet Gynaecol. 2021;42(3):242–252. doi:10.1080/0167482X.2020.1734790
15. Vancea F, Apostol M-S. Changes in mental health during the COVID-19 crisis in Romania: a repeated cross-section study based on the measurement of subjective perceptions and experiences. Sci Prog. 2021;104(2):1–20. doi:10.1177/00368504211025873
16. Anxiety&Depression Association of America. Anxiety disorders – facts&Statistics. Silver spring: ADAA; 2022. Available from: https://adaa.org/understanding-anxiety/facts-statistics.
17. Wallace K, Araji S, Griffin A, et al. An overview of maternal anxiety during pregnancy and the post-partum period. J Ment Health Clin Psychol. 2020;4(4):47–56. doi:10.29245/2578-2959/2020/4.1221
18. Salari N, Hosseinian-Far A, Jalali R, et al. Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: a systematic review and meta-analysis. Global Health. 2020;16:57. doi:10.1186/s12992-020-00589-w
19. Liu Y, Guo N, Li T, Zhuang W, Jiang H. Prevalence and associated factors of postpartum anxiety and depression symptoms among woman in Shanghai, China. J Affect Disord. 2020;274:848–856. doi:10.1016/j.jad.2020.05.028
20. Wassif O, Abdo A, Elawady M, Elmaksoud AA, Eldesouky R. Assessment of postpartum depression and anxiety among females attending primary health care facilities in Qaliubeya Governorate, Egypt. J Environ Public Health. 2019;2019:1–9. doi:10.1155/2019/3691752
21. Rabei SH, El Fatah WOA. Assessing COVID19-related anxiety in an Egyptian sample and correlating it to knowledge and stigma about the virus. Middle East Curr Psychiatry. 2021;28(1). doi:10.1186/s43045-021-00094-9
22. Sadock B, Sadock V, Ruiz P. Kaplan and Sadock’s Comprehensive Textbook of Psychiatry.
23. Weber A, Harrison TM. Reducing toxic stress in the neonatal intensive care unit to improve infant outcomes. Nurs Outlook. 2019;67:169–189. doi:10.1016/j.outlook.2018.11.002
24. Thompson RA, Simpson JA, Berlin LJ. Taking perspective on attachment theory and research: nine fundamental questions. Attach Hum Dev. 2022;1–18. doi:10.1080/14616734.2022.2030132
25. Spies R, Duschinsky R. Inheriting Mary Ainsworth and the strange situation: questions of legacy, authority, and methodology for contemporary developmental attachment researchers. SAGE Open. 2021;11:215824402110475. doi:10.1177/21582440211047577
26. Fernandez AM, Dufey M. Adaptation of collins’ revised adult attachment dimensional scale to the Chilean context. Psicol Reflex Crit. 2015;28:242–252. doi:10.1590/1678-7153.201528204
27. Matei A, Dimitriu MCT, Cirstoveanu CG, Socea B, Ionescu CA. Assessment of postpartum depression in adolescents who delivered during COVID-19 social restrictions: the experience of a tertiary hospital, from Bucharest, Romania. Healthcare. 2021;9(7):807. doi:10.3390/healthcare9070807
28. Khan JY, Dookeran KA. Maternal history of neonatal death as an emerging risk factor of subsequent neonatal mortality in low- and middle-income countries. JAMA Netw Open. 2020;3:e202972. doi:10.1001/jamanetworkopen.2020.2972
29. Eichenwald E, Hansen A, Martin C, Stark A. Cloherty and Stark’s Manual of Neonatal Care.
30. Gomella TL, Cunningham D, Eyal F, Tuttle D. Gomella’s Neonatology. Management, Procedures, on-Call Problems, Diseases, and Drugs.
31. Tasker R, Acerini C, McClure R, Holloway E, Shah A, Lillitos P. Oxford Handbook of Paediatrics.
32. Siegel D, Bryson TP. The Whole-Brain Child: 12 Revolutionary Strategies to Nurture Your Child’s Developing Mind. London: Ant Hive Media; 2016.
33. Siegel D, Bryson TP. No-Drama Discipline: The Whole-Brain Way to Calm the Chaos and Nurture Your Child’s Developing Mind. London: Bartham Press; 2016.
34. Wallis A, Fernandez R, Oprescu F, Chereches R, Zlati A, Dungy C. Validation of a Romanian scale to detect antenatal depression. Open Med. 2012;7:216–223. doi:10.2478/s11536-011-0130-1
35. EPDSromanian [homepage on the internet]. Bucharest: NHS Ayrshire and Arran; 2022. Available from: https://www.nhsaaa.net/media/6400/20190117epdsromanian.pdf.
36. Cronbach’s Alpha (α) using SPSS Statistics [homepage on the internet]. Bath: AERD Statistics; 2018. Available from: https://statistics.laerd.com/spss-tutorials/cronbachs-alpha-using-spss-statistics.php.
37. Spielberger C, Pitariu H, Peleasa C. State-Trait Anxiety Inventory. Cluj-Napoca, Romania: Sinapsis; 2007.
38. Adult attachment Scale (AAS) [homepage on the internet]. US: Complete Dissertation by Statistics Solutions; 2022. Available from: https://www.statisticssolutions.com/free-resources/directory-of-survey-instruments/adult-attachment-scale-aas/.
39. The attachment project [homepage on the internet]. US: Complete Dissertation by Statistics Solutions; 2022. Available from: https://www.attachmentproject.com/blog/10-attachment-style-tests-used-in-research/.
40. Newborn measurements [homepage on the internet]. Stanford: Stanford Medicine Children’s Health; 2021. Available from: https://www.stanfordchildrens.org/en/topic/default?id=newborn-measurements-90-P02673.
41. The apgar score [homepage on the internet]. Washington: ACOG. The American College of Obstetrician and Gynecologists; 2022. Available from: https://acog.org/clinical/clinical-guidance/committee-opinion/articles/2015/10/the-apgar-score.
42. Pearsons’s correlations coefficient [homepage on the internet]. US: Complete Dissertation by Statistics Solutions; 2022. Available from: https://www.statisticssolutions.com/free-resources/directory-of-statistical-analyses/pearsons-correlation-coefficient/.
43. How to run Levene’s test in SPSS [homepage on the internet]. Netherland: SPSS Tutorials; 2022. Available from: https://www.spss-tutorials.com/levenes-test-in-spss/.
44. Poisson Regression. R data analysis examples [homepage on internet]. Los Angeles: UCLA. Advanced Research Computing. Statistical Methods and Data Analytics; 2021. Available from: https://stats.oarc.ucla.edu/r/dae/poisson-regression/.
45. Caesarean section rates continue to rise, amid growing inequalities in access [homepage on the internet]. Geneva: World Health Organization; 2021. Available from: https://www.who.int/news/item/16-06-2021-caesarean-section-rates-continue-to-rise-amid-growing-inequalities-in-access.
46. Smith-Nielsen J, Egmose I, Wendelboe KI, Steinmejer P, Lange T, Vaever MS. Can the Edinburgh postnatal depression Scale-3A be used to screen for anxiety? BMC Psychol. 2021;9:118. doi:10.1186/s40359-021-00623-5
47. Faienza MF, D’Amato E, Natale MP, et al. Metabolic bone disease of prematurity: diagnosis and management. Front Pediatr. 2019;7:143. doi:10.3389/fped.2019.00143
48. Aher SM, Ohlsson A. Late erythropoiesis-stimulating agents to prevent red blood cell transfusion in preterm or low birth weight infants. Cochrane Database Syst Rev. 2019. doi:10.1002/14651858.CD004868.pub5
49. Carlo WA, Vento M. Oxygen therapy for preterm infants. Clin Perinatol. 2019;46:xvii–xviii. doi:10.1016/j.clp.2019.06.001
50. Turcan N, Bohiltea R, Ionita-Radu F, et al. Unfavorable influence of prematurity on the neonatal prognostic of small for gestational age fetuses. Exp Ther Med. 2020;20:2415–2422. doi:10.3892/etm.2020.8744
51. Iyengar U, Jaiprakash B, Haitsuka H, Kim S. One year into the pandemic: a systematic review of perinatal mental health outcomes during COVID-19. Front Psychiatry. 2021;12:674194. doi:10.3389/fpsyt.2021.674194
52. Mutua J, Kigamwa P, Ng’ang’a P, Tele A, Kumar M. A comparative study of postpartum anxiety and depression in mothers with pre-term births in Kenya. JAD Reports. 2020;2:100043. doi:10.1016/j.jadr.2020.100043
53. Cristobal-Canadas D, Bonillo-Perales A, Casado-Belmonte M. Mapping the field in stress, anxiety, and postpartum depression in mothers of preterm infants in neonatal intensive care. Children. 2021;8:730. doi:10.3390/children8090730
54. Sperry L. Handbook of Diagnosis and Treatment of DSM-5 Personality Disorders: Assessment, Case Conceptualization, and Treatment.
55. Bergua V, Meillon C, Potvin O, et al. Short STAI-Y anxiety scales: validation and normative data for elderly subjects. Aging Ment Health. 2016;20:987–995. doi:10.1080/13607863.2015.1051511
56. Seymour-Smith M, Cruwys T, Haslam SA, Brodribb W. Loss of group memberships predicts depression in postpartum mothers. Soc Psychiatry Psychiatr Epidemiol. 2017;52:201–210. doi:10.1007/s00127-016-1315-3
57. Ishitsuka K, Nakayama SF, Kishi R, et al. Japan environment and children’s study: backgrounds, activities, and future directions in global perspectives. Environ Health Prev Med. 2017;22:61. doi:10.1186/s12199-017-0667-y
58. Fallon V, Silverio SA, Halford JCG, Bennet KM, Harrold JA. The Postpartum-specific anxiety and maternal bonding: further evidence to support the use of childbearing specific mood tools. J Reprod Infant Psychol. 2021;39:114–124. doi:10.1080/02646838.2019.1680960
59. Nordahl D, Rognmo K, Bohne A, et al. Adult attachment style and maternal-infant bonding: the indirect path of parenting stress. BMC Psychol. 2020;8:58. doi:10.1186/s40359-020-00424-2
60. Dehelean L, Papava I, Musat MI, et al. Coping strategies and stress related disorders in patients with COVID-19. Brain Sci. 2021;11:1287. doi:10.3390/brainsci11101287
61. Dragomir C, Muranyi D. (coord.) Attachment and Emotional Disorders in Mothers of Postnatal Toddlers [Bachelor’s Thesis in Psychology]. Timisoara: TIBISCUS University; 2019.
62. Dragomir C, Munteanu A. (coord.) RELATIONSHIPS Between Human Factors Associated with Birth in a State Maternity Hospital [Psychology dissertation]. Timisoara: West University; 2012.
63. Van der Zee-van den Berg A, Boere-Boonekamp M, Groothuis-Oudshoorn C, Reijneveld S. Postpartum depression and anxiety: a community-based study on risk factors before, during and after pregnancy. J Affect Disord. 2021;286:158–165. doi:10.1016/j.jad.2021.02.062
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.