Back to Journals » Journal of Hepatocellular Carcinoma » Volume 9
Postoperative Adjuvant Transarterial Chemoembolization Plus Tyrosine Kinase Inhibitor for Hepatocellular Carcinoma: a Multicentre Retrospective Study
Authors Lin K ![]() , Wei F
, Wei F ![]() , Huang Q
, Huang Q ![]() , Lai Z, Zhang J, Chen Q, Jiang Y, Kong J, Tang S, Lin J, Chen Y, Chen J, Zeng Y
, Lai Z, Zhang J, Chen Q, Jiang Y, Kong J, Tang S, Lin J, Chen Y, Chen J, Zeng Y
Received 4 December 2021
Accepted for publication 16 February 2022
Published 8 March 2022 Volume 2022:9 Pages 127—140
DOI https://doi.org/10.2147/JHC.S352480
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Imam Waked
Kongying Lin,1,* Fuqun Wei,1,2,* Qizhen Huang,3,* Zisen Lai,1,* Jinyu Zhang,1 Qingjing Chen,1 Yabin Jiang,1 Jie Kong,1,4 Shichuan Tang,1 Jianhuai Lin,5 Yufeng Chen,6 Jinhong Chen,7 Yongyi Zeng1,8
1Department of Hepatopancreatobiliary Surgery, Mengchao Hepatobiliary Hospital of Fujian Medical University, Fuzhou, 350025, People’s Republic of China; 2Department of Interventional Radiology, First Affiliated Hospital of Fujian Medical University, Fuzhou, 350025, People’s Republic of China; 3Department of Radiation Oncology, Mengchao Hepatobiliary Hospital of Fujian Medical University, Fuzhou, 350025, People’s Republic of China; 4Department of Hepatobiliary, Heze Municipal Hospital, Heze, Shandong, 274000, People’s Republic of China; 5Biobank in Mengchao Hepatobiliary Hospital of Fujian Medical University, Fuzhou, 350025, People’s Republic of China; 6Department of Hepatopancreatobiliary Surgery, Zhangzhou Affiliated Hospital of Fujian Medical University, Zhangzhou, 363000, People’s Republic of China; 7Department of General Surgery, Huashan Hospital, Cancer Metastasis Institute, Fudan University, Shanghai, 200000, People’s Republic of China; 8Department of Hepatopancreatobiliary Surgery, First Affiliated Hospital of Fujian Medical University, Fuzhou, 350025, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yongyi Zeng, Department of Hepatopancreatobiliary Surgery, Mengchao Hepatobiliary Hospital of Fujian Medical University, Xihong Road 312, Fuzhou, 350025, People’s Republic of China, Tel/Fax +86 591 8370 5927, Email [email protected]
Purpose: This study aimed to assess the efficacy and safety of adjuvant transarterial chemoembolization (TACE) plus tyrosine kinase inhibitor (TKI) treatment in patients with hepatocellular carcinoma (HCC) with a high risk of early recurrence after curative resection.
Patients and Methods: Patients from multiple centres were divided into postoperative adjuvant TACE with (n=57) or without (n=142) TKI administration groups. The disease-free survival (DFS) curve was depicted by the Kaplan–Meier method, and the difference between the two groups was tested using the log rank test. Univariate and multivariate Cox analyses were performed to identify independent risk factors for DFS. Additionally, three propensity score analyses were performed to minimise the potential confounding factors to facilitate a more reliable conclusion. Adverse events (AEs) were assessed according to the Common Terminology Criteria for Adverse Events, version 4.0.
Results: The 1-and 2-year DFS rates of the TACE plus TKI treatment group were 45.5% and 34.9%, respectively, which were significantly better than those of the TACE alone group (26.8% and 18.3%, respectively). Multivariate analysis identified adjuvant TACE plus TKI treatment as an independent prognostic factor for DFS (hazard ratio: 0.611, 95% confidence interval: 0.408– 0.915, P=0.017). Further analysis based on the various propensity score methods yielded similar results. Subgroup analysis showed that patients with tumour diameter ≥ 5 cm, tumour number < 3, absence of hepatic vein tumour thrombus and bile duct tumour thrombus, ruptured tumours, and stage IIIB could benefit more from TACE plus TKI treatment (all P< 0.05). Some patients (33.33%) experienced grade ≥ 3 AEs in the TACE plus TKI group.
Conclusion: TACE plus TKI treatment can reduce the incidence of early recurrence with tolerable adverse events in HCC patients at high risk of recurrence after hepatectomy and may be an appropriate option in postoperative anti-recurrence treatment.
Keywords: hepatocellular carcinoma, resection, TACE, TKI, early-recurrence
Introduction
Hepatocellular carcinoma (HCC) is the most common subtype of liver cancer and the fourth leading cause of cancer-related deaths worldwide, with approximately 841,000 new cases and 782,000 deaths annually.1 Liver transplantation, ablation, and hepatectomy are the main curative treatment options for patients with HCC. Due to the lack of donors, the high cost of liver transplantation and the relatively strict indications of ablation, hepatectomy remains the most performed curative treatment for HCC.2,3 However, the high incidence of postoperative relapse limits the efficacy of hepatectomy and jeopardises patients’ long-term outcomes. Even after radical resection, the rates of recurrence remain as high as 50% at 3 years and 70% at 5 years.4,5
Postoperative recurrence of HCC is mainly divided into early recurrence and late recurrence using a cut-off of 2 years, and the pathogenesis and corresponding prevention measures are quite different between the two types of recurrence.6,7 Recently, it has been confirmed that antiviral therapy is the standard treatment for the prevention of late recurrence; however, the optimal prevention measures for early recurrence remain inconclusive.8–10
The efficacy of adjuvant transarterial chemoembolization (TACE) in patients at high risk of recurrence after hepatectomy has been confirmed by a series of randomised controlled studies (RCTs) and systematic reviews and has been widely carried out in many Chinese medical centres under the recommendation of guidelines for the diagnosis and treatment of primary liver cancer in China; however, some patients still experience tumour recurrence after adjuvant TACE.9,11–13 Tyrosine kinase inhibitors (TKIs) are the cornerstone of systemic treatment of HCC, and with the rapid development of systemic treatment of HCC, several oral TKI agents, such as sorafenib, lenvatinib, and apatinib, have been approved for the treatment of HCC and have achieved good efficacy.14–16 The efficacy of TKI agents to prevent recurrence in specific populations has also been reported.17,18 However, whether TACE plus TKI agents can reduce the early recurrence of HCC and whether it has an effect on the early recurrence pattern have not been reported. Therefore, this study aimed to investigate the efficacy and safety of TACE plus TKI treatment in patients at high risk of recurrence after hepatectomy for HCC.
Materials and Methods
Patient Selection
This retrospective study was conducted in accordance with the ethical guidelines of the 1975 Declaration of Helsinki and was approved by the institutional ethics committee of the Mengchao Hepatobiliary Hospital of Fujian Medical University. The data of patients who were at high risk of early relapse after curative resection of HCC between February 2014 and January 2021 were collected from three Chinese hepatobiliary medical centres, including Mengchao Hepatobiliary Hospital of Fujian Medical University, Zhangzhou Affiliated Hospital of Fujian Medical University, and Huashan Hospital of Fudan University.
The inclusion criteria were as follows: 1) histologically confirmed HCC; 2) receipt of R0 resection, referring to the complete removal of all visible tumour nodules during surgery and a microscopically negative surgical margin; 3) receipt of adjuvant TACE with or without TKI administration to prevent recurrence; 4) high risk of early relapse after resection defined as any of the following (a) a tumour diameter >5 cm plus microvascular invasion (MVI) (b) the number of tumour nodules ≥3; (c) portal vein tumour thrombus (PVTT); (d) hepatic vein tumour thrombus (HVTT); (e) bile duct tumour thrombus (BDTT); (f) ruptured HCC. The exclusion criteria were as follows: 1) recurrent HCC; 2) palliative tumour resection; 3) recurrence within the first month after surgery; 4) medical history of other malignancies; 5) receipt of other anti-recurrence treatments after surgery; 6) incomplete clinical or follow-up data.
Preoperative Assessment, Hepatectomy, and Follow Up
The diagnosis of HCC conformed to the practice guidelines recommended by the American Association for the Study of Liver Disease.19 Each patient underwent a comprehensive preoperative assessment, including haematological tests, chest computed tomography (CT), electrocardiogram, abdominal contrast-enhanced CT or magnetic resonance imaging, and cardiopulmonary function examination. For patients diagnosed with large HCCs, three-dimensional imaging measurements were routinely used to assess remnant liver volume. Only patients with sufficient remnant liver volume to achieve R0 resection were considered candidates for surgery. The decision to perform hepatectomy was made by consensus after a multidisciplinary team discussion. The performance of anatomical or partial hepatectomy depends on the liver function status of the patients and the number, location, and extension of tumour nodules. In general, anatomical hepatectomy is the preferred procedure for tumour nodules situated in a segment, sector, and hemiliver, and partial hepatectomy was performed for patients with dissatisfactory liver function or with peripherally located tumours. For patients with macrovascular invasion or bile duct tumour thrombus, thrombectomy or en bloc resection was performed depending on the location of the tumour thrombus.
After discharge, patients received routine outpatient follow up every 2 months for 2 years after the operation, then every 3–6 months thereafter. The contents of the follow-up protocol encompassed tumour marker tests, liver and kidney function tests, chest and abdominal imaging examinations, and positron emission tomography-CT examination was performed to identify extrahepatic metastatic lesions. If recurrence was diagnosed, re-resection, ablation, TACE, radiotherapy, and systemic treatment were performed as appropriate.
The primary endpoint of this study was 2 years of disease-free survival (DFS), defined as the period from operation to recurrence, death, or loss of follow up within 2 years after surgery, whichever occurred first. The second endpoint was early recurrence patterns and treatment-related adverse events of adjuvant TKI treatment.
Clinicopathological Variables and Definitions
MVI refers to the presence of cancer cells in the portal vein, hepatic vein, or a large capsular vessel of the surrounding hepatic tissue lined by the endothelium, visible only on microscopy. According to the guidelines for pathologic diagnosis of HCC in China, all tumour samples were collected using the seven-point baseline protocol, and MVI was classified as M0, M1, and M2 based on the severity of MVI.20 M0 was defined as no MVI; M1 was defined as low risk of MVI, which refers to less than 5 invaded vessels and a distance of less than 1 cm between MVI and the primary tumour nodule; M2 was defined as high risk of MVI, which refers to more than 5 invaded vessels or a distance of more than 1 cm between MVI and the primary tumour nodule. Tumour diameter was defined as the largest tumour lesion size. Tumour cell differentiation assessment was based on the Edmondson–Steiner classification for multiple tumour nodules; the worst histologic grade of tumour differentiation was accepted. The extent of hepatectomy was divided into major and minor hepatectomy, which refers to the resection of three or more Couinaud’s segments, and minor hepatectomy was defined as the resection extent of fewer than three segments.
Adjuvant TACE and TKI
Adjuvant TACE therapy was administered within 1–2 months after recovery of postoperative liver function, and the second or more cycles of TACE was decided based on the comprehensive evaluation of the patient’s condition by the respective competent physicians, which to a certain extent depends on the experience of each medical center.11 TACE procedures were previously reported.21 The Seldinger method was used to insert the arterial angiographic catheter through the femoral artery to the proper hepatic artery, and TACE was performed on the whole remnant liver. Liver angiography and/or CT angiography were performed to detect residual tumour staining. After intrahepatic recurrent lesions exclusion, the chemotherapeutic drugs lipiodol (5–10 mL), cisplatin (10–30 mg), doxorubicin hydrochloride (10 mg), and pharmorubicin (20–40 mg) were injected via the catheter. The dosage of doxorubicin and lipiodol was determined as per the body surface area and underlying liver function status of the patients. The chemotherapeutic agents used varied from centre to centre, depending on their experience.
TKI agents were administered after either hepatectomy or adjuvant TACE once the patient’s liver function recovered. The indications for TKI agents and the specific type of TKI agent were determined by the patients’ wishes and consultation with their attending physicians. The TKI agents used in the study included sorafenib, lenvatinib, and apatinib. Sorafenib was initially administered at an oral dose of 400 mg twice daily. Apatinib was initially administered at an oral dose of 500 mg once daily. The initial dosage of lenvatinib depended on patients’ weight as follows: 12 mg once daily for patients weighing over 60 kg and 8 mg once daily for patients weighing less than 60 kg. Dosage adjustment and interruption were determined by the physician based on the grade of drug-related adverse effects (AEs) experienced by the patients. The grade of AEs was based on the National Cancer Institute Common Terminology Criteria for Adverse Events, version 4.0. The TKI agent was discontinued when the patient experienced an unacceptable AE or tumour recurrence.
Statistical Analysis
Continuous data, summarised as the mean (standard deviation), were compared using Student’s t-test or the Mann–Whitney U-test. Categorical data were expressed as a number (percentage, %) and compared using the chi-square test or Fisher’s exact test. DFS curves were presented using the Kaplan–Meier method, and the difference in DFS between groups was tested using the Log rank test. Univariate and multivariate Cox proportional hazard regression analyses were performed to identify independent risk factors for DFS. Variables with P<0.2 in univariate analysis were then evaluated by multivariate analysis.
Three propensity score methods, including inverse probability weighting (IPW), propensity score matching (PSM), and an additional adjustment of the propensity score, were performed in this study to offset the potential selection bias caused by the retrospective, non-RCT study design.22–24 Individualised propensity scores were estimated by multivariate logistic regression analysis that included the imbalanced clinicopathological variables (age, total bilirubin, intraoperative transfusion, rupture, and PVTT). For inverse probability weighting analysis, the predictive probability of the propensity score model was used to calculate the inverse probability weighting weight and construct a weighted cohort in which the confounding factors were balanced between treatment groups.23 A 1:1 PSM analysis was conducted using the nearest neighbour method with a calliper width equal to 0.1 of the standard deviation of the logit of the propensity score to create a PSM cohort. Further, we also performed multivariate Cox proportional hazards analysis with adjustment for propensity score in the primary cohort.22
All statistical analyses were two-sided, and P<0.05 was regarded as statistically significant. SPSS version 20 (SPSS, Inc., Chicago, IL, USA) and R version 4.1.1 (R Project, Vienna, Austria) were used to perform statistical analysis.
Results
Baseline Characteristics
According to the inclusion and exclusion criteria of this study, 199 patients with a high risk of recurrence after hepatectomy for HCC were included, including 142 patients in the TACE group and 57 patients in the TACE plus TKI group (Figure S1). As shown in Table 1, in the overall cohort, the mean age of patients was 51.8 ± 12.1 years. Most of the patients were male (86.4%) and had hepatitis B infection (92.0%), and the proportion of liver cirrhosis reached 69.8%. Regarding tumour characteristics, most of the patients showed aggressive tumour characteristics, with the mean tumour diameter reaching 8.59 ± 3.75 cm and the proportion of ≥3 tumour nodules reaching 16.6%. MVI was present in 97.5% of patients, and the proportions of M1 and M2 were 35.7% and 61.8%, respectively. Most patients had PVTT (52.3%), and the proportion of BDTT was 11.6%. Regarding the American Joint Committee on Cancer (AJCC) 8th staging system, most patients (47.7%) were stage IIIB, while the proportions of stage II and IIIA were 39.7% and 12.6%, respectively.
 |  |  |
Table 1 Baseline Clinical Characteristics of the Two Treatment Groups |
There were no significant differences in other variables between the two groups except for age, total bilirubin level, intraoperative blood transfusion, tumour rupture, and PVTT proportions. Compared with the TACE alone group, the patients in the TACE plus TKI group were younger, had a higher total bilirubin level, a lower incidence of PVTT, and a higher proportion of ruptured tumour nodules. We constructed a matched cohort of 96 patients through PSM analysis, and the baseline clinicopathological features of the two groups were balanced. Similarly, in the weighted cohort constructed by IPW analysis, the baseline characteristics of the two groups were balanced (Table 1).
DFS and Recurrence Patterns
The median follow-up period for the entire cohort was 23.7 months (range: 3.0–82.2 months), including 23.8 months (range: 8.2–55.2 months) for the TACE plus TKI group and 23.5 months (range: 3.0–82.2 months) for the TACE group. All the events in this cohort were recurrences (152 DFS events in 199 patients), and thus, time to progression was equivalent to time to recurrence. As shown in Figure 1A, in the primary cohort, Kaplan–Meier analysis showed that the TACE plus TKI group had higher 1-and 2-year DFS rates than the TACE group (45.5% and 34.9% vs 26.8% and 18.3%, respectively, P=0.008). In the PSM cohort, the DFS of the TACE plus TKI group was also better than that of the TACE group (P=0.01, Figure 1B), and the 1-and 2-year DFS rates were 43.7% and 20.9% in the TACE plus TKI group and 20.8% and 12.2% in the TACE group, respectively. In the IPW-weighted cohort, the Kaplan–Meier analysis showed the same result, with better DFS rates in the TACE plus TKI group than in the TACE group (P=0.01, Figure 1C). Further exploratory analysis in the primary cohort revealed that compared with the TACE group, all three TKI groups showed better DFS rates, and the DFS of the lenvatinib and sorafenib groups was slightly better than that of the apatinib group (Figure S2).
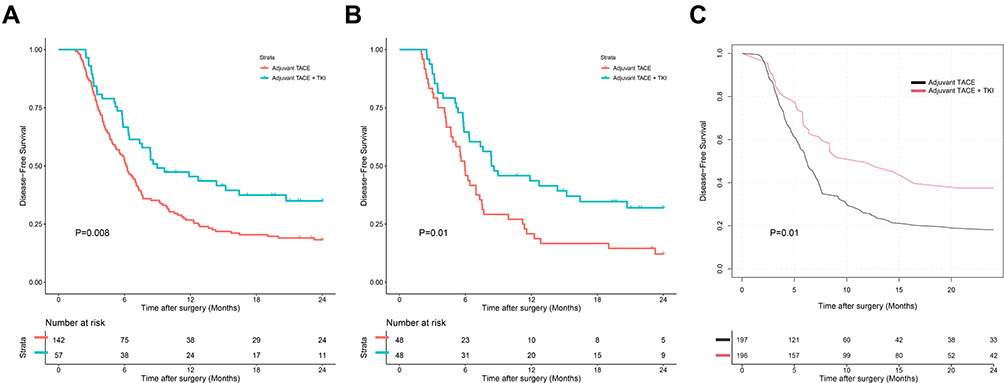 |
Figure 1 Disease-free survival of the adjuvant TACE group and adjuvant TACE combined with TKI group. (A) Primary cohort; (B) PSM cohort; (C) IPW cohort. Abbreviations: TACE, transcatheter arterial chemoembolization; TKI, tyrosine kinase inhibitor; PSM, propensity score matching; IPW, inverse probability weight. |
During the 2-year follow-up period after hepatectomy, tumour recurrence occurred in 36 (63.2%) patients in the TACE plus TKI group and 116 (81.7%) patients in the TACE group. In terms of recurrence patterns, there was no significant difference between the two groups in terms of tumour location, tumour number, and presence of macrovascular tumour thrombus of recurrent tumour lesions (both P>0.05). However, there was a difference in the treatment modalities after recurrence between the two groups (P=0.024), with a higher proportion of patients in the TACE group receiving radical treatment than in the TACE plus TKI group (33.6% vs 25.0%) (Table 2).
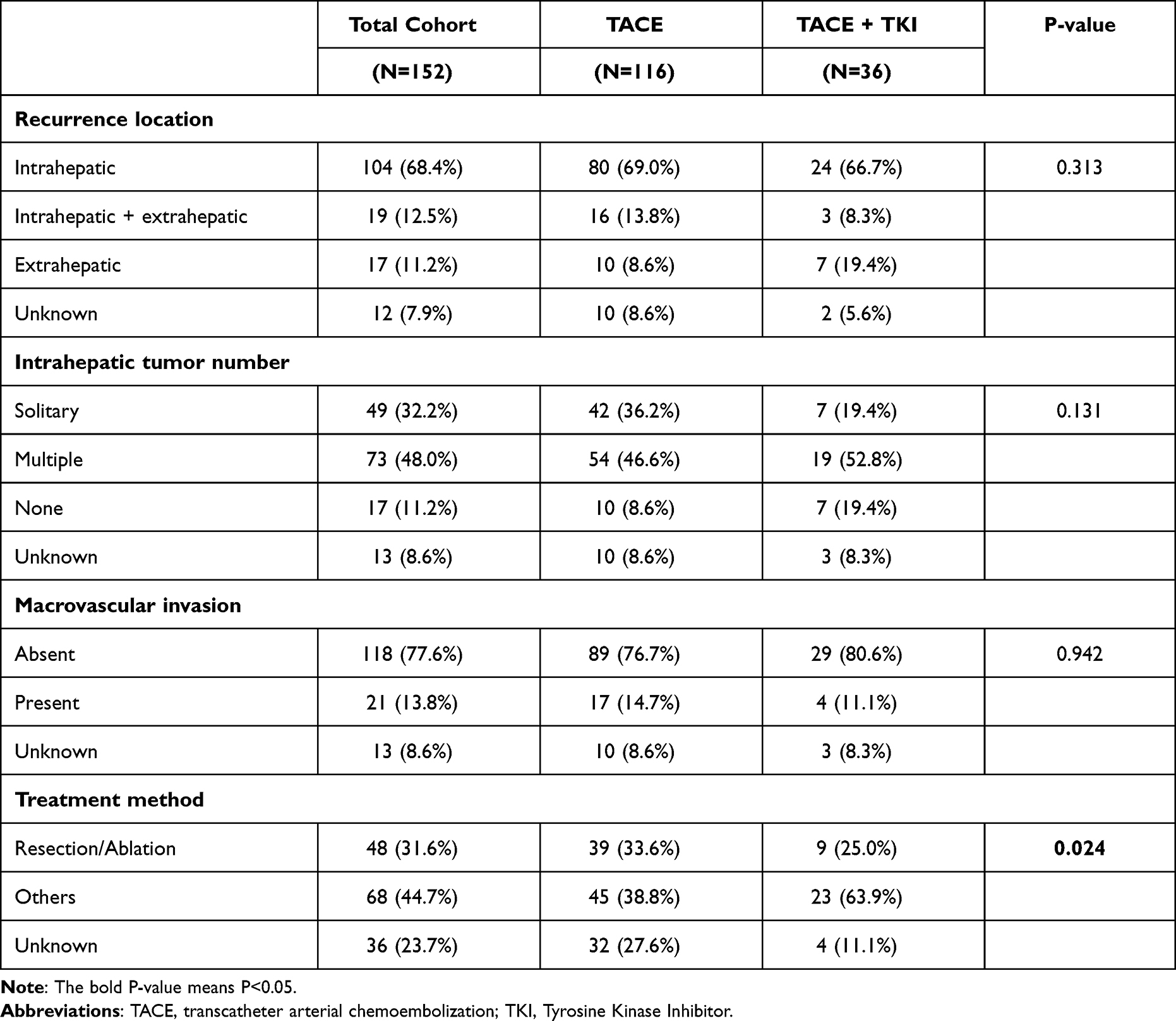 |
Table 2 Recurrence Patterns |
Risk Factors for Poor DFS
Univariate and multivariate Cox regression analyses were performed to identify independent risk factors for DFS. In the primary cohort, univariate analysis showed that 9 of the 25 included clinicopathological variables were potentially relevant (P<0.2) (Table S1). Further multivariate analysis showed that treatment modality was an independent prognostic factor for DFS; the TACE plus TKI group had a better DFS than the TACE group (hazard ratio [HR]: 0.611, 95% confidence interval [CI]: 0.408–0.915, P=0.017). Other independent prognostic factors included PVTT (HR: 1.509, 95% CI: 1.067–2.134, P=0.020), tumour diameter (HR: 1.057, 95% CI: 1.012–1.103, P=0.012), and major hepatectomy (HR: 1.615, 95% CI: 1.004–2.597, P=0.048) (Tables 3 and S1) whereas, in the propensity score analysis, the corresponding multivariate analysis yielded similar results and showed that TACE plus TKI was associated with better DFS (Tables 3, S2–S4).
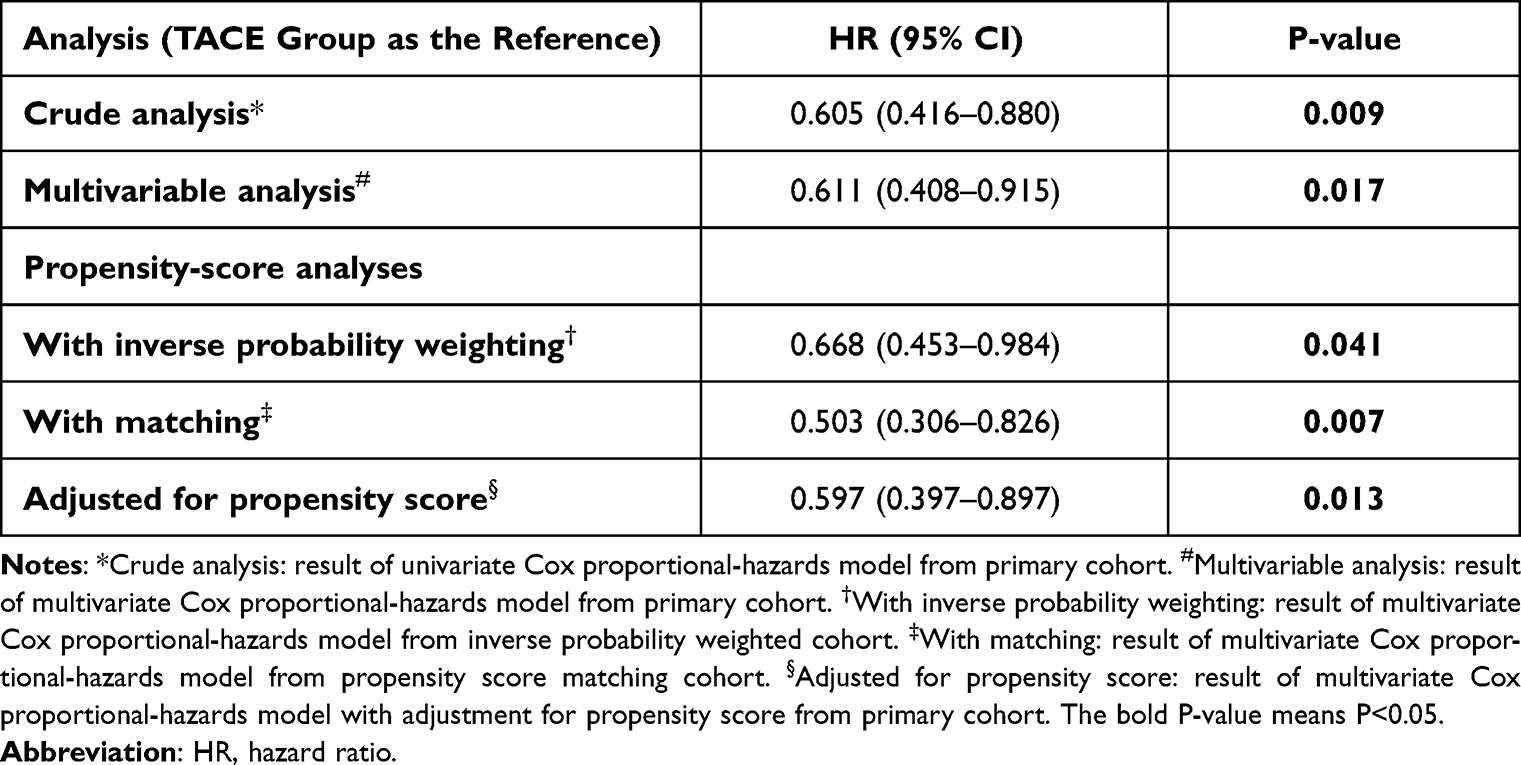 |
Table 3 Associations Between Disease-Free Survival and the Treatment Modalities in the Crude Analysis, Multivariable Analysis, and Propensity-Score Analyses |
Subgroup Analysis
Further subgroup analysis stratified by risk factors and AJCC8th staging system showed relatively consistent results in most subgroups except for HVTT-positive groups and demonstrated that patients could benefit more from TACE plus TKI treatment if they had tumour diameter ≥5 cm, tumour number <3, no HVTT, no BDTT, ruptured tumour, and stage IIIB (both P<0.05, Figure 2). A further detailed Kaplan–Meier analysis based on the corresponding risk factors is shown in Figure S3.
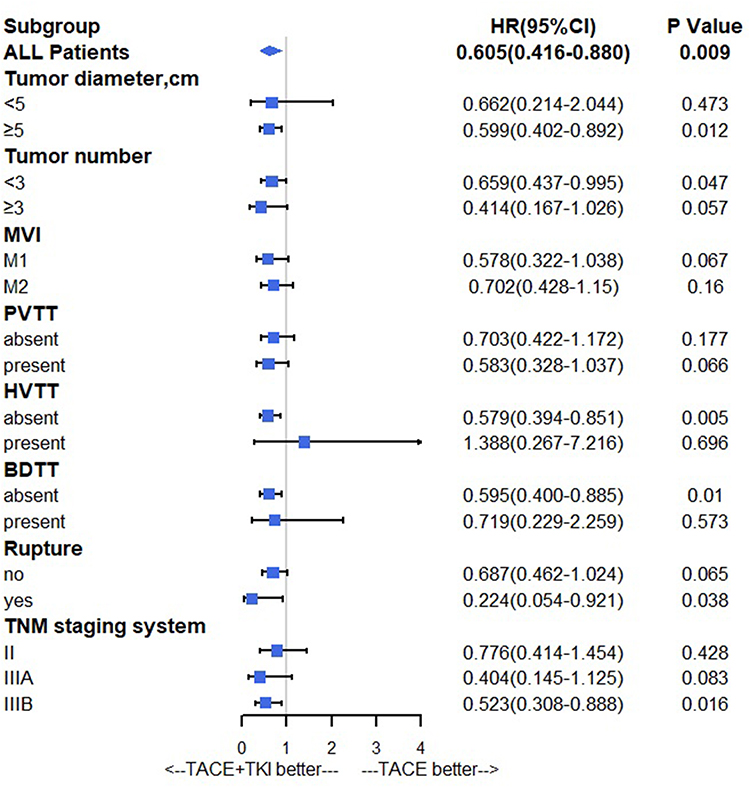 |
Figure 2 Forests plot of subgroup analysis of disease-free survival. Abbreviations: MVI, microvascular invasion; PVTT, portal vein tumour thrombus; HVTT, hepatic vein tumour thrombus; BDTT, bile duct tumour thrombus; AJCC, American Joint Committee on Cancer; TACE, transcatheter arterial chemoembolization; TKI, tyrosine kinase inhibitor. |
Adverse Events
Regarding the safety of adjuvant TKI agents, a total of 53 (93.0%) patients suffered from AEs of any grade during the treatment period; grade 3 or 4 AEs were recorded in 19 (33.3%) patients, and no fatal AEs were recorded (Table 4). The most common grade 3 or 4 AEs were neutropenia (5, 8.8%), hand-foot skin reaction (3, 5.3%), diarrhoea (3, 5.3%), thrombocytopenia (3, 5.3%), and proteinuria (3, 5.3%).
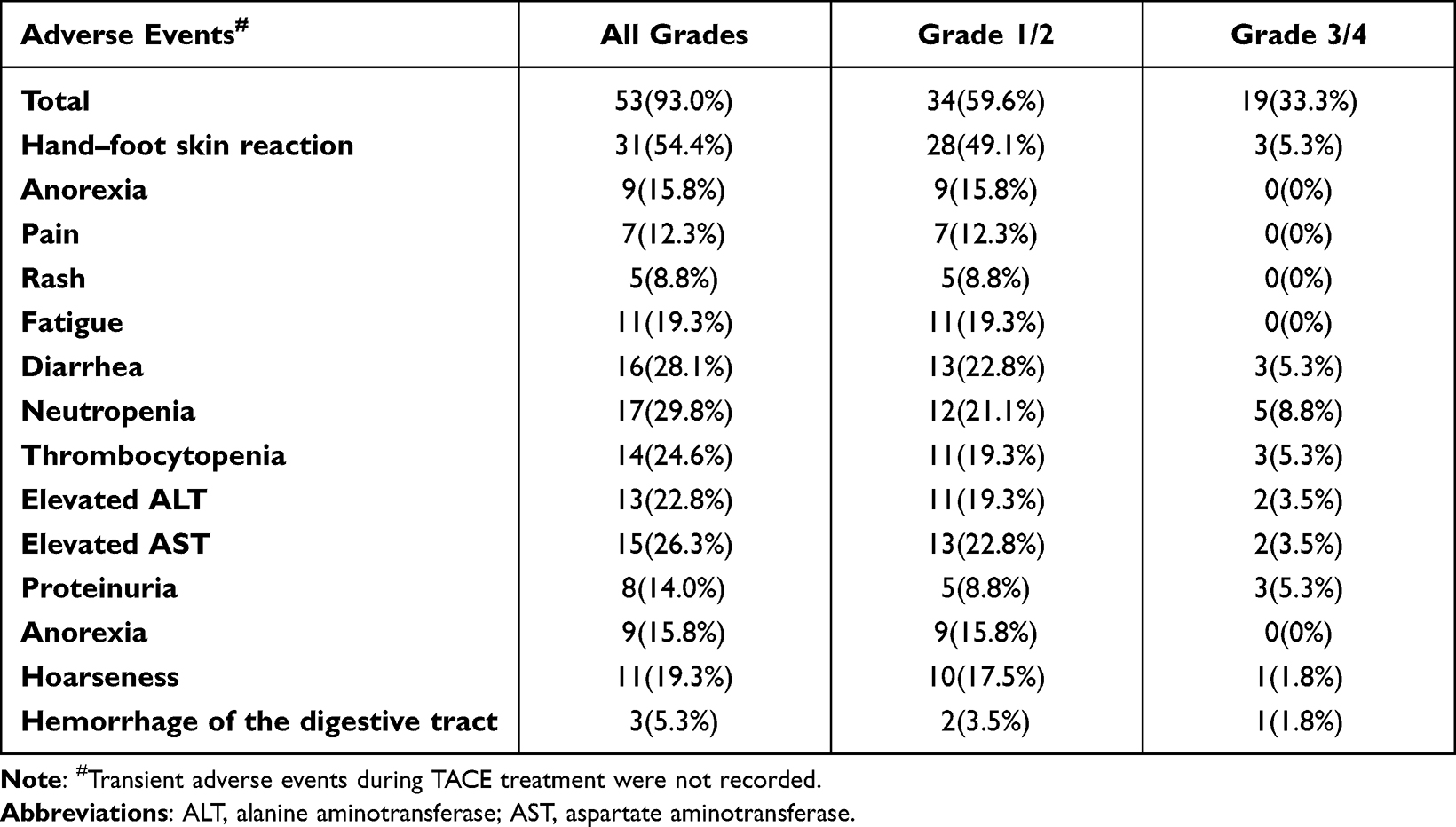 |
Table 4 Adverse Events of TKI Group |
Discussion
In this study, we demonstrated that TACE plus a TKI agent could significantly reduce the incidence of early recurrence in patients at a higher risk of recurrence after curative resection than TACE alone; further subgroup analysis also identified patients who may benefit from this adjuvant modality. This study’s results may be valuable in guiding postoperative anti-recurrence treatment planning and are clinically valuable to inform further studies on the prevention of recurrence of HCC.
The prevention of postoperative recurrence is an important part of the diagnosis and treatment of HCC and remains an unsolved clinical issue at present.4,25 The following are the two patterns of postoperative recurrence of HCC: early recurrence and late recurrence, both with different underlying mechanisms. Early recurrence mainly originates from residual microscopic metastases in the remnant liver after surgery, which mainly depends on the primary tumour burden, such as the tumour diameter, number of tumour nodules, and vascular invasion.26,27 In contrast, the mechanism of late recurrence is mainly the de novo development of new tumour lesions, which depends on the underlying liver disease aetiology, such as hepatitis virus infection and cirrhosis.6 Strategies for preventing recurrence of HCC mainly depend on the types of recurrence; thus, it is unwise to classify early recurrence and late recurrence as one group for research and analysis purposes. This retrospective multicentre study focused on the efficacy and safety of TACE plus TKI treatment in preventing early recurrence and utilised multiple propensity score analysis methods to minimise the potential bias caused by the retrospective study design as much as possible. To the best of our knowledge, this is the first study to report the efficacy of TACE plus various TKI agents’ treatment to prevent the early recurrence of HCC.
The efficacy of adjuvant TACE in preventing recurrence has been recognized by several RCTs and systematic reviews.9,11,12 An RCT performed by Wei et al reported the benefit of adjuvant TACE in patients with solitary tumours ≥5 cm plus MVI after hepatectomy.11 Another RCT conducted by Wang et al showed that adjuvant TACE significantly reduced tumour recurrence in Hepatitis B virus (HBV)-related HCC with intermediate-risk (a solitary tumour >5 cm without MVI) or high-risk (two or three tumour lesions, or a solitary tumour plus MVI) of recurrence after radical resection. Moreover, for patients with PVTT, HVTT, or BDTT, the efficacy of TACE has been reported in previous studies.21,28,29 However, the role of TKI agents in preventing recurrence remains controversial. Compared with lenvatinib and apatinib, sorafenib is the first oral TKI agent approved for the treatment of unresectable HCC, and the related published studies on recurrence prevention of TKI agents mainly focused on sorafenib. The STORM trial, the first and currently the only international multicentre RCT designed to evaluate the efficacy of sorafenib in preventing HCC recurrence, failed to reach its primary endpoints in patients with an intermediate or high risk of recurrence.30 However, the efficacy of sorafenib in preventing recurrence has been reported in several studies recently. Zhang et al reported that sorafenib significantly reduced the recurrence rate and improved the overall survival of MVI-positive HCC.17 Xia et al also reported the potential benefits and safety of adjuvant sorafenib in patients with advanced HCC after curative resection.31 Furthermore, a recent meta-analysis, which included 2655 patients from 13 studies, demonstrated that adjuvant sorafenib therapy after hepatectomy could reduce recurrence rates without intolerable side effects.18 The inconsistencies in the results may be attributed to the different clinicopathological characteristics of the patients included in these studies. Further molecular marker analysis in the STROM trial also indicated that approximately 30% of patients with a specific gene signature might benefit from adjuvant sorafenib therapy.32 Therefore, considering the inherently high heterogeneity of HCC, future studies should explore the potential benefits of sorafenib adjuvant therapy.33 Lenvatinib and apatinib are novel TKI agents approved for the treatment of advanced HCC, and only a few studies have reported their efficacy in preventing recurrence after surgery. A single-centre, open-label Phase II trial reported the positive effect of apatinib on recurrence-free survival of patients with PVTT;34 a prospective multicentre study with the aim of evaluating the adjuvant effect of lenvatinib in combination with TACE is also ongoing and has also shown promising efficacy according to its interim results.35
Despite the results of this study demonstrating the superiority of adjuvant TACE plus TKI over TACE alone, there are still some issues that deserve further attention. First, 53 (93.0%) patients in this study exhibited AEs of any grade during treatment, including 19 patients with grade 3 or 4 AEs. Considering the potential adverse reactions of TACE+TKI administration, it is particularly important to select specific benefit patients. Subgroup analyses in the present study suggested that patients with some pathological characteristics may benefit from the combination therapy. However, building a well-powered predictive model, such as a clinical-radiomic model, may be a better solution. A clinical-radiomic model constructed by Chen et al to predict objective response to first circle TACE in HCC patients achieved about 90% accuracy, which is of potential significance for clinical decision-making.36 Second, in terms of treatment modalities after recurrence, the results showed that the proportion of radical treatment after recurrence in the TACE alone group was slightly higher than that in the TACE plus TKI group (33.6% vs 25.0%). In our opinion, this may be attributed to the difference in recurrence patterns between the two treatment modalities, which was mainly reflected in the slightly higher proportion of extrahepatic metastasis and multiple tumours in the TACE plus TKI group than in the TACE alone group (27.7% vs 22.4%, 52.8% vs 46.6%). However, it cannot be ruled out that the specific mechanism underlying this difference may also be related to the drug resistance of TKI agents, and this merits further investigation. Immunotherapy represents a major breakthrough in oncology and has demonstrated promising efficacy in the treatment of HCC,37,38 and this therapy may benefit this group of patients in the future.
This study had some limitations worth noting. First, the present study was limited by its retrospective nature and limited sample size. Thus, inherent selection bias is inevitable, thereby highlighting the need for further verification by prospective multicentre trials with a larger patient population. To our best knowledge, a prospective, multicentre study (LANCE trial) aimed at evaluating the efficacy of lenvatinib plus TACE to prevent postoperative HCC recurrence is currently ongoing, and we look forward to their final results. Second, most patients included in the present study had HBV infection. The efficacy of oral TKI agents may be related to the viral background; for instance, sorafenib may have a better effect in patients with Hepatitis C virus-associated HCC, while lenvatinib may have a better effect in patients with HBV-associated HCC.15,39 Furthermore, this study only included patients who underwent hepatectomy, and further studies, including patients receiving other treatments, are required.
Conclusion
In conclusion, this study showed that TACE plus TKI agents can reduce the early recurrence incidence with tolerable adverse events in patients at a high risk of recurrence after curative resection and may represent a novel and appropriate option in postoperative anti-recurrence treatment planning.
Abbreviations
HBsAg, Hepatitis B virus surface antigen; ALT, alanine aminotransferase; AST, aspartate aminotransferase; GGT, gamma-glutamyl transpeptidase; AFP, alpha fetoprotein; MVI, microvascular invasion; PVTT, portal vein tumour thrombus; HVTT, hepatic vein tumour thrombus; BDTT, bile duct tumour thrombus; AJCC, American Joint Committee on Cancer; TACE, transcatheter arterial chemoembolization; TKI, Tyrosine Kinase Inhibitor; PSM, propensity score matching; IPW, inverse probability weights.
Ethics Approval and Consent to Participate
Considering that patient medical data was analysed retrospectively, all informed consents were waived by the ethics committee. Of note, no patients-identifiable information was utilised.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
This study was supported by Key Clinical Specialty Discipline Construction Program of Fuzhou, Fujian, P.R.C (Grant number: 201912002), Science and Technology project of Fuzhou (Grant number: 2019-S-88), Natural Science Foundation of Fujian Province, China (Grant number: 2021J01029), Chinese Foundation for Hepatitis Prevention and Control, TianQing Liver Disease Research Fund Subject (Grant number: TQGB20210098) and FuJian provincial medical center of Hepatobiliary.
Disclosure
The authors declare no conflicts of interest for this work.
References
1. Demir T, Lee SS, Kaseb AO. Systemic therapy of liver cancer. Adv Cancer Res. 2021;149:257–294.
2. Liu H, Wang ZG, Fu SY, et al. Randomized clinical trial of chemoembolization plus radiofrequency ablation versus partial hepatectomy for hepatocellular carcinoma within the Milan criteria. Br J Surg. 2016;103(4):348–356. doi:10.1002/bjs.10061
3. Yin L, Li H, Li AJ, et al. Partial hepatectomy vs. transcatheter arterial chemoembolization for resectable multiple hepatocellular carcinoma beyond Milan criteria: a RCT. J Hepatol. 2014;61(1):82–88. doi:10.1016/j.jhep.2014.03.012
4. Minami Y, Kudo M. Adjuvant therapy after radical surgery for hepatocellular carcinoma: still an unmet need. Hepatobiliary Surg Nutr. 2019;8(4):414–416. doi:10.21037/hbsn.2019.04.05
5. Bruix J, Gores GJ, Mazzaferro V. Hepatocellular carcinoma: clinical frontiers and perspectives. Gut. 2014;63(5):844–855. doi:10.1136/gutjnl-2013-306627
6. Xu XF, Xing H, Han J, et al. Risk factors, patterns, and outcomes of late recurrence after liver resection for hepatocellular carcinoma: a multicenter study from China. JAMA Surg. 2019;154(3):209–217. doi:10.1001/jamasurg.2018.4334
7. Imamura H, Matsuyama Y, Tanaka E, et al. Risk factors contributing to early and late phase intrahepatic recurrence of hepatocellular carcinoma after hepatectomy. J Hepatol. 2003;38(2):200–207. doi:10.1016/S0168-8278(02)00360-4
8. Lo CM, Liu CL, Chan SC, et al. A randomized, controlled trial of postoperative adjuvant interferon therapy after resection of hepatocellular carcinoma. Ann Surg. 2007;245(6):831–842. doi:10.1097/01.sla.0000245829.00977.45
9. Wang Z, Ren Z, Chen Y, et al. Adjuvant transarterial chemoembolization for HBV-related hepatocellular carcinoma after resection: a randomized controlled study. Clin Cancer Res. 2018;24(9):2074–2081. doi:10.1158/1078-0432.CCR-17-2899
10. Li J, Xing J, Yang Y, et al. Adjuvant 131I-metuximab for hepatocellular carcinoma after liver resection: a randomised, controlled, multicentre, open-label, Phase 2 trial. Lancet Gastroenterol Hepatol. 2020;5(6):548–560. doi:10.1016/S2468-1253(19)30422-4
11. Wei W, Jian PE, Li SH, et al. Adjuvant transcatheter arterial chemoembolization after curative resection for hepatocellular carcinoma patients with solitary tumor and microvascular invasion: a randomized clinical trial of efficacy and safety. Cancer Commun. 2018;38(1):61. doi:10.1186/s40880-018-0331-y
12. Huo YR, Chan MV, Chan C. Resection plus post-operative adjuvant transcatheter arterial chemoembolization (TACE) compared with resection alone for hepatocellular carcinoma: a systematic review and meta-analysis. Cardiovasc Intervent Radiol. 2020;43(4):572–586. doi:10.1007/s00270-019-02392-6
13. Zhou J, Sun H, Wang Z, et al. Guidelines for the Diagnosis and Treatment of Hepatocellular Carcinoma (2019 Edition). Liver Cancer. 2020;9(6):682-720. doi:10.1159/000509424
14. Cheng AL, Kang YK, Chen Z, et al. Efficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: a Phase III randomised, double-blind, placebo-controlled trial. Lancet Oncol. 2009;10(1):25–34. doi:10.1016/S1470-2045(08)70285-7
15. Kudo M, Finn RS, Qin S, et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: a randomised Phase 3 non-inferiority trial. Lancet. 2018;391(10126):1163–1173. doi:10.1016/S0140-6736(18)30207-1
16. Zhang Y, Huang G, Miao H, et al. Apatinib treatment may improve survival outcomes of patients with hepatitis B virus-related sorafenib-resistant hepatocellular carcinoma. Ther Adv Med Oncol. 2020;12:1758835920937422. doi:10.1177/1758835920937422
17. Zhang XP, Chai ZT, Gao YZ, et al. Postoperative adjuvant sorafenib improves survival outcomes in hepatocellular carcinoma patients with microvascular invasion after R0 liver resection: a propensity score matching analysis. HPB. 2019;21(12):1687–1696. doi:10.1016/j.hpb.2019.04.014
18. Huang S, Li D, Zhuang L, Sun L, Wu J. A meta-analysis of the efficacy and safety of adjuvant sorafenib for hepatocellular carcinoma after resection. World J Surg Oncol. 2021;19(1):168. doi:10.1186/s12957-021-02280-9
19. Bruix J, Sherman M. Management of hepatocellular carcinoma. Hepatology. 2005;42(5):1208–1236. doi:10.1002/hep.20933
20. Cong WM, Bu H, Chen J, et al. Practice guidelines for the pathological diagnosis of primary liver cancer: 2015 update. World J Gastroenterol. 2016;22(42):9279–9287. doi:10.3748/wjg.v22.i42.9279
21. Huang Q, Lin K, Wang L, et al. Postoperative adjuvant transarterial chemoembolization improves short-term prognosis of hepatocellular carcinoma with bile duct tumor thrombus: a propensity-score matching study. Cancer Manag Res. 2020;12:9183–9195. doi:10.2147/CMAR.S270467
22. Geleris J, Sun Y, Platt J, et al. Observational study of hydroxychloroquine in hospitalized patients with Covid-19. N Engl J Med. 2020;382(25):2411–2418. doi:10.1056/NEJMoa2012410
23. Famularo S, Di Sandro S, Giani A, et al. Treatment of hepatocellular carcinoma beyond the Milan criteria. A weighted comparative study of surgical resection versus chemoembolization. HPB. 2020;22(9):1349–1358. doi:10.1016/j.hpb.2019.12.011
24. Yang Y, Lin K, Liu L, et al. Impact of preoperative TACE on incidences of microvascular invasion and long-term post-hepatectomy survival in hepatocellular carcinoma patients: a propensity score matching analysis. Cancer Med. 2021;10(6):2100–2111. doi:10.1002/cam4.3814
25. Zhu XD, Li KS, Sun HC. Adjuvant therapies after curative treatments for hepatocellular carcinoma: current status and prospects. Genes Dis. 2020;7(3):359–369. doi:10.1016/j.gendis.2020.02.002
26. Chan A, Zhong J, Berhane S, et al. Development of pre and post-operative models to predict early recurrence of hepatocellular carcinoma after surgical resection. J Hepatol. 2018;69(6):1284–1293. doi:10.1016/j.jhep.2018.08.027
27. Lin K, Huang Q, Wang L, et al. Pre- and postoperative models for prediction of recurrence in non-B, non-C hepatocellular carcinoma. Front Oncol. 2021;11:612588. doi:10.3389/fonc.2021.612588
28. Zhang XP, Liu YC, Chen ZH, et al. Postoperative adjuvant transarterial chemoembolization improves outcomes of hepatocellular carcinoma associated with hepatic vein invasion: a propensity score matching analysis. Ann Surg Oncol. 2019;26(5):1465–1473. doi:10.1245/s10434-019-07223-z
29. Liu F, Guo X, Dong W, et al. Postoperative adjuvant TACE-associated nomogram for predicting the prognosis of resectable hepatocellular carcinoma with portal vein tumor thrombus after liver resection. Int J Biol Sci. 2020;16(16):3210–3220. doi:10.7150/ijbs.46896
30. Bruix J, Takayama T, Mazzaferro V, et al. Adjuvant sorafenib for hepatocellular carcinoma after resection or ablation (STORM): a phase 3, randomised, double-blind, placebo-controlled trial. Lancet Oncol. 2015;16(13):1344–1354. doi:10.1016/S1470-2045(15)00198-9
31. Xia F, Wu LL, Lau WY, et al. Adjuvant sorafenib after heptectomy for Barcelona clinic liver cancer-stage C hepatocellular carcinoma patients. World J Gastroenterol. 2016;22(23):5384–5392. doi:10.3748/wjg.v22.i23.5384
32. Pinyol R, Montal R, Bassaganyas L, et al. Molecular predictors of prevention of recurrence in HCC with sorafenib as adjuvant treatment and prognostic factors in the phase 3 STORM trial. Gut. 2019;68(6):1065–1075. doi:10.1136/gutjnl-2018-316408
33. Dong W, Yan K, Yu H, et al. Prognostic nomogram for sorafenib benefit in hepatitis B virus-related hepatocellular carcinoma after partial hepatectomy. Front Oncol. 2020;10:605057. doi:10.3389/fonc.2020.605057
34. Sun HC, Zhu XD, Zhou J, et al. Adjuvant apatinib treatment after resection of hepatocellular carcinoma with portal vein tumor thrombosis: a phase II trial. Ann Transl Med. 2020;8(20):1301. doi:10.21037/atm-20-6181
35. Chen J, Lu L, Wen T, et al. Adjuvant lenvatinib in combination with TACE for hepatocellular carcinoma patients with high risk of postoperative relapse (LANCE): interim results from a muticenter prospective cohort study; 2020:4580.
36. Chen M, Cao J, Hu J, et al. Clinical-radiomic analysis for pretreatment prediction of objective response to first transarterial chemoembolization in hepatocellular carcinoma. Liver Cancer. 2021;10(1):38–51. doi:10.1159/000512028
37. Finn RS, Qin S, Ikeda M, et al. Atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma. N Engl J Med. 2020;382(20):1894–1905. doi:10.1056/NEJMoa1915745
38. Qin S, Ren Z, Meng Z, et al. Camrelizumab in patients with previously treated advanced hepatocellular carcinoma: a multicentre, open-label, parallel-group, randomised, phase 2 trial. Lancet Oncol. 2020;21(4):571–580. doi:10.1016/S1470-2045(20)30011-5
39. Jackson R, Psarelli EE, Berhane S, Khan H, Johnson P. Impact of viral status on survival in patients receiving sorafenib for advanced hepatocellular cancer: a meta-analysis of randomized phase III trials. J Clin Oncol. 2017;35(6):622–628. doi:10.1200/JCO.2016.69.5197
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.