Back to Journals » Journal of Pain Research » Volume 15
Post-Stroke Complex Regional Pain Syndrome and Upper Limb Inactivity in Hemiplegic Patients: A Cross-Sectional Study
Authors Katsura Y, Ohga S ![]() , Shimo K
, Shimo K ![]() , Hattori T
, Hattori T ![]() , Yamada T, Matsubara T
, Yamada T, Matsubara T
Received 24 June 2022
Accepted for publication 14 September 2022
Published 18 October 2022 Volume 2022:15 Pages 3255—3262
DOI https://doi.org/10.2147/JPR.S379840
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jonathan Greenberg
Yuichi Katsura,1,2 Satoshi Ohga,3 Kazuhiro Shimo,3 Takafumi Hattori,2 Tsukasa Yamada,1,2 Takako Matsubara2,3
1Department of Rehabilitation, Kishiwada Rehabilitation Hospital, Kishiwada-shi, Osaka, 596-0827, Japan; 2Faculty of Rehabilitation, Kobe Gakuin University Graduate School, Kobe, Hyogo, 651-2180, Japan; 3Faculty of Rehabilitation, Kobe Gakuin University, Kobe, Hyogo, 651-2180, Japan
Correspondence: Yuichi Katsura, Department of Rehabilitation, Kishiwada Rehabilitation Hospital, 8-10, Kanmatsu-chou, Kishiwada-shi, Osaka, 596-0827, Japan, Tel +81-72-426-7777, Fax +81-72-426-7771, Email [email protected]
Purpose: The purpose of this study was to investigate the prevalence of post-stroke complex regional pain syndrome (CRPS) and to examine the characteristics of inactivity status of the upper limb in post-stroke CRPS patients. In addition, as a sub-analysis, the association between the upper limb inactivity status and pain intensity was investigated in post-stroke CRPS patients.
Patients and Methods: This cross-sectional study included 102 patients with first-ever stroke between April 2019 and February 2020. Each patient was allocated into one of two groups based on the presence or absence of CRPS. Demographic data (age, sex, stroke etiology, lesion side, and number of days since stroke onset) were collected. The following evaluations were performed in all patients: Fugl–Meyer Assessment (FMA), Action Research Arm Test (ARAT), and Motor Activity Log (MAL). The numerical rating scale (NRS) to determine pain intensity was assessed only in patients with post-stroke CRPS.
Results: Nineteen and 83 patients were assigned to the post-stroke CRPS and control group, respectively. The prevalence of post-stroke CRPS was 18.6% (19/102). FMA, ARAT, and MAL scores were significantly lower in patients with post-stroke CRPS than those without it. FMA and ARAT scores were significantly correlated with NRS scores, but MAL was almost zero-scored in patients with post-stroke CRPS.
Conclusion: The study results indicated that activity status of the affected upper limb was severely deteriorated, and more inactivity of the upper limb was associated with higher pain intensity in patients with post-stroke CRPS. Thus, our results suggest that post-stroke CRPS may be influenced by the degree of upper limb inactivity after stroke.
Keywords: complex regional pain syndrome, post-stroke shoulder-hand syndrome, stroke, Fugl–Meyer Assessment, Action Research Arm Test, Motor Activity Log
Introduction
Complex regional pain syndrome (CRPS), formerly referred to as reflex sympathetic dystrophy and causalgia, is a neuropathic pain disorder caused by painful trauma, nerve lesions, immobilization of the extremities, stroke, spinal cord injury, or myocardial infarction.1,2 CRPS is characterized by pain combined with abnormal sensory, autonomic, nutritional, and motor function, and is classified based on the absence (type I) or presence (type II) of peripheral nerve injury.3 Previous studies have reported immobilization, psychological, and genetic factors as risk factors for developing CRPS.4 Furthermore, prior studies have reported that immobilization, even in healthy limbs, induces changes in limb temperature, mechanosensitivity, and thermosensitivity that are characteristic of CRPS.5,6 Therefore, immobilization induces peripheral and central sensitization, resulting in CRPS.
CRPS that occurs after stroke has been known as shoulder-hand syndrome. The prevalence of post-stroke CRPS ranges from 12.5% to 50%.7–9 Post-stroke CRPS has been classified as type I due to the lack of obvious peripheral nerve injury.10 The main symptoms of post-stroke CRPS include pain, hyperalgesia, allodynia, edema, swelling, limited range of motion of the shoulder, wrist, and hand joints, and feverish sensation and redness of the wrists and hands.10 Previous studies reported that risk factors associated with post-stroke CRPS included length of hospital stay, shoulder subluxation, soft tissue lesions of the shoulder, adhesive arthritis, spasticity, severe hand paralysis, entrapment neuropathy, brachial plexus injury, lower respiratory tract infection, urinary infection, depression, protein-energy malnutrition, and coronary artery disease.11–13 Moreover, a recent meta-analysis reported that characteristics of post-stroke CRPS patients included female sex, left hemiplegia, shoulder subluxation, spasticity, severe hand paralysis, and impaired activities of daily living (ADL).14 In addition to those factors, since the affected upper limb is inevitably inactive after stroke due to motor paralysis, the immobilization/disuse condition may be a risk factor for post-stroke CRPS. However, no studies have examined whether immobilization/disuse due to motor paralysis is also a risk factor for the developing CRPS in patients after stroke.
Recently, a combination of outcome measures has been recommended to assess activity status of the upper limb in patients after stroke, owing to the wide variation in severity of symptoms and motor paralysis.15 The Fugl–Meyer Assessment (FMA) and Action Research Arm Test (ARAT) have been used internationally as outcome measures for activity status of the upper limb in stroke rehabilitation.15 These outcome measures consist of performance assessment batteries. The Motor Activity Log (MAL) is the only assessment that evaluates the usage frequency of the affected upper limb during ADL. To determine whether disuse due to upper limb motor paralysis after stroke is associated with the development of post-stroke CRPS and the severity of pain, an internationally recognized outcome measure reflecting the degree of inactivity should be used. Clarifying this issue will lead to a better understanding of the pathophysiology of post-stroke CRPS, enabling the prevention and early treatment of stroke patients at high risk of developing CRPS.
The purpose of this study was to investigate the prevalence of post-stroke CRPS and to examine the characteristics of inactivity status of the upper limb in post-stroke CRPS patients using motor function (ARAT) and usage frequency in daily life (MAL) in addition to the severity of motor paralysis (FMA). In addition, the correlation between the inactivity status of the upper limb and pain intensity was investigated in post-stroke CRPS patients.
Materials and Methods
Participants
The study included 210 patients with a first-ever stroke and allocated into the post-stroke CRPS and control group according to the presence or absence of CRPS. Patients were enrolled between April 2019 and February 2020 at Kishiwada Rehabilitation Hospital in Osaka, Japan. The physician diagnosed stroke via neurological examination, brain computed tomography, or magnetic resonance imaging at the initial medical examination. The inclusion criterion was a first-ever confirmed supratentorial stroke. The exclusion criteria comprised the following: a diagnosis of other central nervous system disorders, such as traumatic brain injury, hypoxic brain injury, or brain neoplasm; a history of neurodegenerative disorders; bilateral hemispheric or infratentorial lesions; bodily or visuospatial hemineglect and apraxia; and a history of injury, major trauma, or surgery in the upper limb on the paralyzed side. Post-stroke CRPS was defined using the Budapest research diagnostic criteria for CRPS (the “Budapest Criteria”), as adopted by the International Association for the Study of Pain.16 The control group was defined as stroke patients who were pain-free and did not match the diagnostic criteria. The study protocol was approved by the respective research ethics committees at Kobe Gakuin University (approval number: 20-29) and Kishiwada Rehabilitation Hospital (approval number: 2021-002), and was conducted in accordance with the 1964 Helsinki Declaration and its later amendments. All patients provided verbal and written informed consent.
Demographic and Clinical Data
Demographic data (age, sex, etiology of stroke, side of the lesion, and number of days since stroke onset) and three outcome measures for upper limb motor function (FMA, ARAT, and MAL) were assessed in all patients. The numerical rating scale (NRS) to determine pain intensity was assessed only in patients with post-stroke CRPS. NRS is a tool for obtaining the patient’s subjective response to pain on a scale from 0 (no pain at all) to 10 (unbearable pain).
Inactivity Status Measures
The 33-item FMA (3-point ordinal scale; score range, 0–66 points) was used to assess the severity of upper limb paralysis.17 The FMA is the most widely used assessment of upper limb motor impairment in stroke rehabilitation research. A higher FMA score indicates a lower level of impairment in the paralyzed upper limb. The FMA has shown excellent intra-rater [intraclass correlation coefficient (ICC) = 0.994–0.999] and inter-rater (ICC = 0.991–0.999) reliability when used to assess people with stroke.17
The 19-item ARAT (4-level ordinal scale; score range, 0–57 points) was used to assess motor function in the paralyzed upper limb. The ARAT is a performance test that is representative of the major activities of the upper extremities in ADL.18 A higher ARAT score indicates a lower level of impairment in the paralyzed upper limb. The ARAT has shown excellent intra-rater (r = 0.996–0.997) and inter-rater (r = 0.989) reliability in assessing people with stroke.19
The MAL was used to assess the frequency of use of the paralyzed arm and hand in daily life; it is a structured interview that elicits information about 14 ADL.20 Patients were asked to assess how well (quality of movement scale: QOM) and how much (amount of use scale: AOU) they used their affected upper limb to perform each ADL. A higher MAL score indicates more frequent use of the paralyzed arm and hand. Both the MAL-QOM and MAL-AOU have demonstrated good test-retest reliability (QOM: ICC = 0.82; AOU: ICC = 0.79) and excellent internal consistency (QOM: Cronbach's α = 0.87; AOU: Cronbach's α > 0.82) in assessing people with stroke.20
Statistical Analysis
Data are presented as mean ± standard deviation. Since the data were not normally distributed, we used the less sensitive (but more robust) nonparametric tests for all statistical analyses. Demographic data and inactivity status measures of the upper limb were compared between the post-stroke CRPS and control groups using the Mann–Whitney U-test and Fisher’s exact test, respectively, to investigate the upper limb inactivity status in post-stroke CRPS patients. The correlation between NRS scores and state of upper limb inactivity outcomes in the post-stroke CRPS group was evaluated using the Spearman’s rank test. The level of statistical significance was set at p<0.05 for all analyses.
Results
Post-Stroke CRPS and Control Group Allocation
During the study period, a total of 210 stroke patients were admitted to our hospital, and 108 patients were excluded. The reasons for exclusion were cognitive dysfunction (N=40), bodily or visuospatial hemineglect and apraxia (N=27), traumatic brain injury (N=25), and bilateral hemispheres or infratentorial lesion (N=16). Finally, 102 patients were included in this study; 19 and 83 patients were assigned to the post-stroke CRPS and control group, respectively (Figure 1). The prevalence of post-stroke CRPS was 18.6%.
 |
Figure 1 Flow chart of participants through the study. After the classification process, a total of 102 patients were finally included in the study, of which 19 and 83 patients were assigned to the post-stroke CRPS and control group, respectively. Abbreviation: CRPS, complex regional pain syndrome. |
Demographic Data
Demographic data are presented in Table 1. No significant differences between the groups were found for the following variables: age (70.3±10.4 years in the control group; 73.9±7.7 years in the post-stroke CRPS group; p = 0.187), sex (male: 38 [45.7%], female: 45 [54.3%] in the control group; male: 6 [31.5%], female: 13 [68.5%] in the post-stroke CRPS group; p = 0.311), etiology of stroke (infarction: 36 [43.4%], hemorrhage: 47 [56.6%] in the control group; infarction: 7 [36.8%], hemorrhage: 12 [63.2%] in the post-stroke CRPS group; p = 0.797), side of lesion (right: 42 [51.0%], left: 41 [49.0%] in the control group; right: 6 [31.5%], left: 13 [68.5%] in the post-stroke CRPS group; p = 0.202), and number of days since stroke onset (96.9±29.5 days in the control group; 99.6±33.4 days in the post-stroke CRPS group; p = 0.840).
 |
Table 1 Demographic Data of Each Group |
Inactivity Status of Upper Limb
The status of inactivity of the upper limb in both groups is shown in Figure 2. The mean FMA score in the post-stroke CRPS group was lower than that in the control group (10.1±7.0 in the post-stroke CRPS group; 34.4±26.1 in the control group; p<0.001). The mean ARAT score in the post-stroke CRPS group was lower than that in the control group (3.8±4.5 in the post-stroke CRPS group; 24.8±25.6 in the control group; p<0.001). The mean MAL score at AOU in the post-stroke CRPS group was lower than that in the control group (0.12±0.28 in the post-stroke CRPS group; 2.56±2.0 in the control group; p<0.001). The mean MAL score at QOM in the post-stroke CRPS group was lower than that in the control group (0.06±0.22 in the post-stroke CRPS group; 2.36±2.0 in the control group; p<0.001).
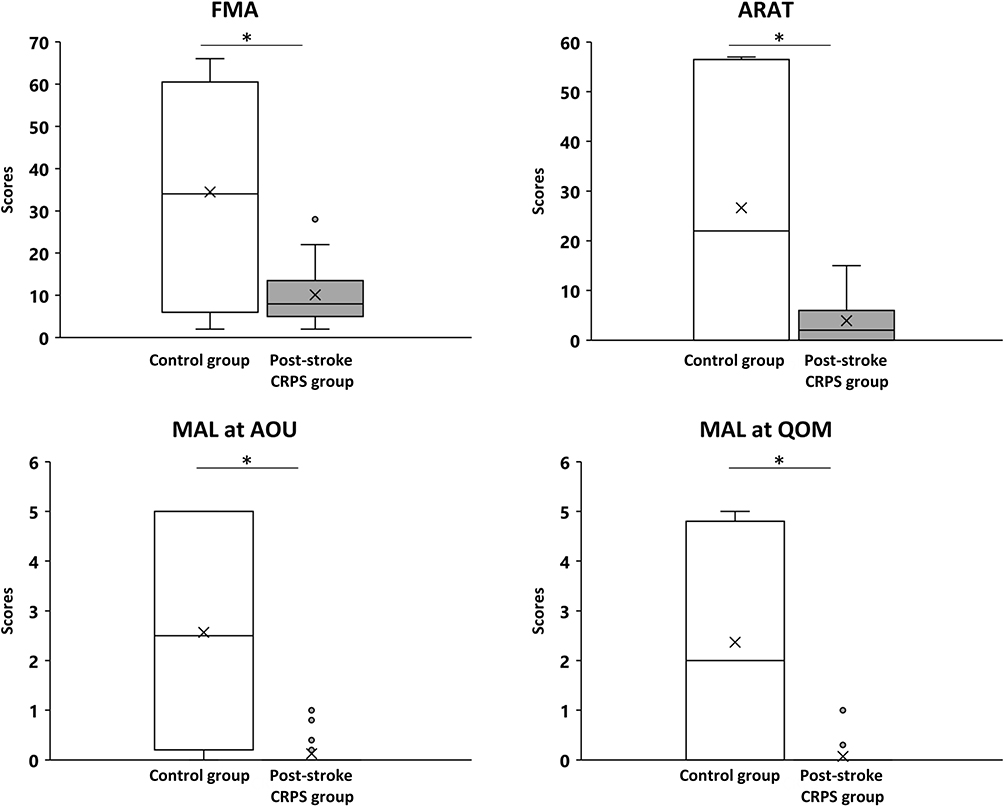 |
Figure 2 Inactivity status of the upper limb in both groups. Control group (N=83), Post-stroke CRPS group (N=19). *Significance at p<0.001. Abbreviations: FMA, Fugl–Meyer Assessment; ARAT, Action Research Arm Test; MAL at AOU, Motor Activity Log at Amount of Use; MAL at QOM, Motor Activity Log at Quality of Movement. |
Correlations
The relationship between the NRS scores, the degree of pain, and each inactivity status in the post-stroke CRPS group is shown in Figure 3. NRS scores were significantly correlated with the FMA (rs = −0.743; p<0.01) and ARAT (rs = −0.558; p<0.01) scores. There was no correlation between the NRS and MAL (AOU [p = 0.073]; QOM [p = 0.502]) scores.
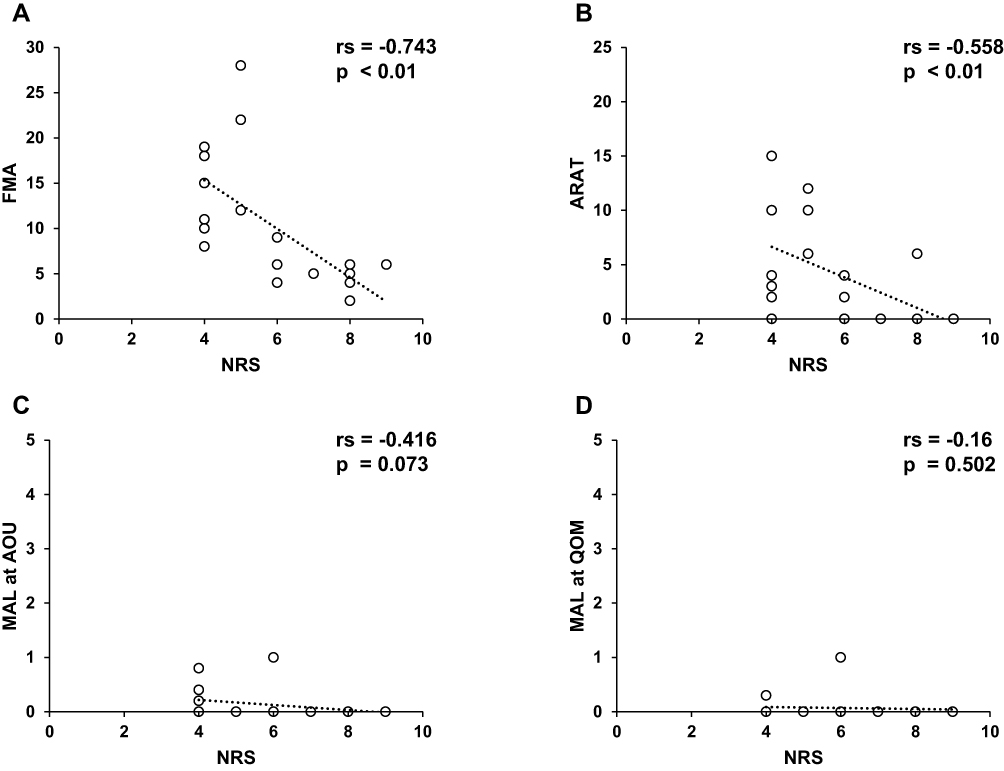 |
Figure 3 The correlation analysis and scatter plot of NRS and FMA, ARAT, and MAL at AOU and QOM. Post-stroke CRPS group (N = 19). (A) The correlation analysis and scatter plot of NRS and FMA, (B) ARAT, (C) MAL at AOU, and (D) MAL at QOM. Abbreviations: NRS, Numerical Rating Scale; FMA, Fugl–Meyer Assessment; ARAT, Action Research Arm Test; MAL at AOU, Motor Activity Log at Amount of Use; MAL at QOM, Motor Activity Log at Quality of Movement. |
Discussion
This study was the first to investigate the relationship between post-stroke CRPS and inactivity of the affected upper limb after stroke using comprehensive outcome measures, including the FMA, ARAT, and MAL. The prevalence of post-stroke CRPS in our hospital was 18.6%, and mean FMA, ARAT, and MAL scores were significantly lower in the post-stroke CRPS group than in the control group, indicating immobilization/disuse. In addition, both FMA and ARAT scores were significantly correlated with pain intensity in the post-stroke CRPS group. Since most of the post-stroke CRPS patients had no frequency of upper extremity use (MAL score of 0), there might be no significant correlation between the MAL score and pain intensity due to the floor effect. Thus, our results suggest that the post-stroke CRPS may be influenced by the degree of upper limb inactivity after stroke.
The prevalence of post-stroke CRPS in our study was 18.6% (19 out of 102 patients), similar to the previous study results.7 Since there were no significant differences in demographic data (age, sex, etiology of stroke, side of the lesion, and the number of days since stroke onset) between the post-stroke CRPS and control groups, other factors may have been involved in the development of post-stroke CRPS. While immobilization is known to be a risk factor for CRPS, it is currently unknown whether immobilization/disuse due to upper limb paralysis in post-stroke patients contributes to the development of post-stroke CRPS. Therefore, in this study, we comprehensively assessed inactivity status of the upper limb in patients with post-stroke CRPS by evaluating motor paralysis severity, motor function, and the usage frequency of the affected upper limb in daily life via the FMA, ARAT, and MAL, respectively. The FMA defines the boundary between severe and moderate disability as 19±2 points and between moderate and mild disability as 47±2 points.21 In this study, upper limb motor function in post-stroke CRPS patients was characterized by severe disability; thus, this supports the results of a previous study.13 MAL scores at AOU of <2.5 points are defined as disuse.22 Our results indicated that the paralyzed upper limb of post-stroke CRPS patients was used less frequently in daily life. In this study, even though the paralyzed upper limb was not immobilized with a cast or sling, our findings suggest that inactivity status of the paralyzed upper limb may influence post-stroke CRPS.
In this study, the upper limb motor dysfunction assessed by FMA and ARAT and pain intensity were significantly correlated, but MAL was almost zero-scored in patients with post-stroke CRPS. In other words, our results suggest that a greater degree of inactivity in the upper limb is associated with higher pain intensity. Previous studies in animals and patients with low back pain have shown that longer immobilization periods lead to greater pain intensity.23,24 Our results indicate that a greater degree of inactivity is associated with higher pain intensity; thus, inactivity of the paralyzed upper limb may contribute to the pain severity of post-stroke CRPS.
Animal studies have shown that immobilization causes changes in peripheral nerve fiber density, inflammatory mediator production, and neuropeptide signaling. These changes induce sustained nociceptive stimulation, resulting in central changes in the spinal cord.23,25,26 These mechanisms result in hyperalgesia (exaggerated responses to nociceptive stimuli) and allodynia (activation of nociceptive pathways by normally nonpainful stimuli such as light touch or cold). Thus, the aforementioned peripheral and central changes associated with immobilization may also be related to the disuse of paralyzed upper limbs in stroke patients and the subsequent onset and pain severity of post-stroke CRPS. The present results are the first to show that post-stroke CRPS patients have upper limb inactivity and that it may be also associated with pain severity.
This study has two limitations. First, it was a single-center, cross-sectional study design. Second, the sample size of post-stroke CRPS group is small. Therefore, further multicenter longitudinal study is needed to determine whether the upper limb inactivity status is associated with pain severity in the development of post-stroke CRPS.
Conclusion
This study showed that activity status of the affected upper limb was severely decreased in post-stroke CRPS patients. Furthermore, a greater degree of inactivity was associated with higher pain intensity, suggesting that upper limb inactivity might influence post-stroke CRPS.
Acknowledgments
We would like to thank Editage for English language editing.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wasner G, Backonja MM, Baron R. Traumatic neuralgias: complex regional pain syndromes (reflex sympathetic dystrophy and causalgia): clinical characteristics, pathophysiological mechanisms and therapy. Neurol Clin. 1998;16(4):851–868. doi:10.1016/s0733-8619(05)70101-8
2. Wasner G, Schattschneider J, Heckmann K, Maier C, Baron R. Vascular abnormalities in reflex sympathetic dystrophy (CRPS I): mechanisms and diagnostic value. Brain. 2001;124(3):587–599. doi:10.1093/brain/124.3.587
3. Merskey H, Bogduk N. Classification of Chronic Pain: Descriptions of Chronic Pain Syndromes and Definitions of Pain Terms.
4. Marinus J, Moseley GL, Birklein F, et al. Clinical features and pathophysiology of complex regional pain syndrome. Lancet Neurol. 2011;10(7):637–648. doi:10.1016/S1474-4422(11)70106-5
5. Guo TZ, Offley SC, Boyd EA, Jacobs CR, Kingery WS. Substance P signaling contributes to the vascular and nociceptive abnormalities observed in a tibial fracture rat model of complex regional pain syndrome type I. Pain. 2004;108(1–2):95–107. doi:10.1016/j.pain.2003.12.010
6. Terkelsen AJ, Bach FW, Jensen TS. Experimental forearm immobilization in humans induces cold and mechanical hyperalgesia. Anesthesiology. 2008;109(2):297–307. doi:10.1097/ALN.0b013e31817f4c9d
7. Van Ouwenaller C, Laplace PM, Chantraine A. Painful shoulder in hemiplegia. Arch Phys Med Rehabil. 1986;67(1):23–26.
8. Kocabas H, Levendoglu F, Ozerbil OM, Yuruten B. Complex regional pain syndrome in stroke patients. Int J Rehabil Res. 2007;30(1):33–38. doi:10.1097/MRR.0b013e3280146f57
9. Gokkaya NK, Aras M, Yesiltepe E, Koseoglu F. Reflex sympathetic dystrophy in hemiplegia. Int J Rehabil Res. 2006;29(4):275–279. doi:10.1097/MRR.0b013e328010b961
10. Chae J. Poststroke complex regional pain syndrome. Top Stroke Rehabil. 2010;17(3):151–162. doi:10.1310/tsr1703-151
11. Altas EU, Onat ŞŞ, Konak HE, Polat CS. Post-stroke complex regional pain syndrome and related factors: experiences from a tertiary rehabilitation center. J Stroke Cerebrovasc Dis. 2020;29(9):104995. doi:10.1016/j.jstrokecerebrovasdis.2020
12. Kim JY, Yoon SY, Kim J, Jeong YH, Kim YW. Neural substrates for poststroke complex regional pain syndrome type I: a retrospective case-control study using voxel-based lesion symptom mapping analysis. Pain. 2020;161(6):1311–1320. doi:10.1097/j.pain.0000000000001816
13. Lee JI, Kwon SW, Lee A, Tae WS, Pyun SB. Neuroanatomical correlates of poststroke complex regional pain syndrome: a voxel-based lesion symptom-mapping study. Sci Rep. 2021;11(1):13093. doi:10.1038/s41598-021-92564-7
14. Su YC, Guo YH, Hsieh PC, Lin YC. A meta-analysis and meta-regression of frequency and risk factors for poststroke complex regional pain syndrome. Medicina. 2021;57(11):1232. doi:10.3390/medicina57111232
15. Santisteban L, Térémetz M, Bleton JP, Baron JC, Maier MA, Lindberg PG. Upper limb outcome measures used in stroke rehabilitation studies: a systematic literature review. PLoS One. 2016;11(5):e0154792. doi:10.1371/journal.pone.0154792
16. Harden NR, Bruehl S, Perez RS, et al. Validation of proposed diagnostic criteria (the ‘Budapest Criteria’) for Complex Regional Pain Syndrome. Pain. 2010;150(2):268–274. doi:10.1016/j.pain.2010.04.030
17. Amano S, Umeji A, Uchita A, et al. Clinimetric properties of the Fugl-Meyer assessment with adapted guidelines for the assessment of arm function in hemiparetic patients after stroke. Top Stroke Rehabil. 2018;25(7):500–508. doi:10.1080/10749357.2018.1484987
18. Amano S, Umeji A, Uchita A, et al. Clinimetric properties of the action research arm test for the assessment of arm activity in hemiparetic patients after stroke. Top Stroke Rehabil. 2020;27(2):127–136. doi:10.1080/10749357.2019.1667656
19. Van der Lee JH, De Groot V, Beckerman H, Wagenaar RC, Lankhorst GJ, Bouter LM. The intra-and interrater reliability of the action research arm test: a practical test of upper extremity function in patients with stroke. Arch Phys Med Rehabil. 2001;82:14–19. doi:10.1053/apmr.2001.18668
20. Uswatte G, Taub E, Morris D, Vignolo M, McCulloch K. Reliability and validity of the upper-extremity Motor Activity Log-14 for measuring real-world arm use. Stroke. 2005;36(11):2493–2496. doi:10.1161/01.STR.0000185928.90848.2e
21. Woodbury ML, Velozo CA, Richards LG, Duncan PW. Rasch analysis staging methodology to classify upper extremity movement impairment after stroke. Arch Phys Med Rehabil. 2013;94(8):1527–1533. doi:10.1016/j.apmr.2013.03.007
22. Molle Da Costa RD, Luvizutto GJ, Martins LG, et al. Clinical factors associated with the development of nonuse learned after stroke: a prospective study. Top Stroke Rehabil. 2019;26(7):511–517. doi:10.1080/10749357.2019.1631605
23. Hamaue Y, Nakano J, Sekino Y, et al. Immobilization-induced hypersensitivity associated with spinal cord sensitization during cast immobilization and after cast removal in rats. J Physiol Sci. 2013;63(6):401–408. doi:10.1007/s12576-013-0277-4
24. Verbunt JA, Sieben J, Vlaeyen JW, Portegijs P, André Knottnerus J. A new episode of low back pain: who relies on bed rest? Eur J Pain. 2008;12(4):508–516. doi:10.1016/j.ejpain.2007.08.001
25. Sekino Y, Nakano J, Hamaue Y, et al. Sensory hyperinnervation and increase in NGF, TRPV1 and P2X3 expression in the epidermis following cast immobilization in rats. Eur J Pain. 2014;18(5):639–648. doi:10.1002/j.1532-2149.2013.00412.x
26. Wei T, Guo TZ, Li WW, Kingery WS, Clark JD. Acute versus chronic phase mechanisms in a rat model of CRPS. J Neuroinflammation. 2016;13:14. doi:10.1186/s12974-015-0472-8
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.