")
Back to Journals » Infection and Drug Resistance » Volume 16
Population Pharmacokinetics of Isavuconazole in Adult: A Systematic Review
Authors Chen N, Wang X, Li Y, Yang P, Huang M, Lu X
Received 9 August 2023
Accepted for publication 29 November 2023
Published 8 December 2023 Volume 2023:16 Pages 7559—7568
DOI https://doi.org/10.2147/IDR.S434622
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Na Chen,1,2 Xiaojuan Wang,1,2 Yinyan Li,1,2 Ping Yang,1,2 Mingzhu Huang,1,2 Xiaoyang Lu1,2
1Department of Pharmaceutical, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang Province, People’s Republic of China; 2Zhejiang Provincial Key Laboratory for Drug Evaluation and Clinical Research, Hangzhou, Zhejiang Province, People’s Republic of China
Correspondence: Xiaoyang Lu; Mingzhu Huang, Email [email protected]; [email protected]
Abstract: Isavuconazole (ISA) is a second generation broad-spectrum triazole antifungal drug derived from voriconazole structure, and its oral capsules is currently the only oral preparation approved for invasive mucormycosis. In recent years, population pharmacokinetic studies of ISA have been reported continuously. This paper aims to summarize the characteristics of population pharmacokinetic models of ISA in adults, and provide theoretical basis for individualized administration of ISA. We systematically searched PubMed, Embase, CNKI, Wanfang, VIP and other databases to collect population pharmacokinetic models published from the establishment of the database to March 2023. A total of 6 studies were included in this review, including healthy men and women, invasive fungal infections with malignant tumors or neutropenia, solid organ transplantation. The dose of ISA was 40– 400mg for single-dose. The multiple-dose of ISA was 200mg every 8 hours for the first 48 hours and then 200mg once daily. All studies used a two-compartment model, first-order elimination. For oral formulations, except for one study that used first-order absorption, the others used Weibull absorption. Body mass index (BMI) was the most common covariable, followed by total body weight, lean body mass, race, sex, population type (healthy volunteers/patients), and creatinine clearance. These studies included several covariates, and the clearance rate (CL) was similar among populations. In the future, external validation and population pharmacokinetic studies in special populations such as patients with severe liver disease and ECMO support are needed.
Keywords: isavuconazonium sulfate, isavuconazole, population pharmacokinetics, covariates
Introduction
Isavuconazonium sulfate is the water-soluble prodrug of the novel, broad-spectrum, triazole antifungal agent isavuconazole (ISA). ISA is a second-generation broad-spectrum triazole antifungal drug derived from voriconazole structure, and has a wide range of activities against yeast, filamentous fungi and dimorphic fungi.1 ISA is available in two formulations: oral capsule and intravenous injection. ISA was approved by the US FDA in 2015 and granted orphan drug status. It was approved for invasive aspergillosis and invasive mucormycosis in adults in China in 2021. Especially in the treatment of mucormycosis, compared with polyenes, ISA is better tolerated and has fewer side effects, and sequential treatment with oral capsule formulations reduces the occupation of medical resources and the burden on patients.2
So far, there have been several studies on the pharmacokinetic characteristics and influencing factors of ISA. The high bioavailability of isavuconazonium sulfate capsules, close to 98%, so the dosing regimen for the oral and intravenous formulations is the same. Unlike other triazoles, the absorption of ISA is almost unaffected by food intake, gastric acid inhibitor drugs or even mucositis.3,4 The injection or oral formulation of ISA exhibits dose-dependent pharmacokinetics, with small pharmacokinetic difference in pharmacokinetics in healthy volunteers. The time to peak concentration after oral administration was 1.5–2.0 h, half-life was 56–104 h, the total clearance was 1.9–4.1 L/h, and distribution volume was 155–404 L.5–7 With the extension of treatment time, the accumulation of ISA in the body is obvious: the area under the curve (AUC) on the last day after 14–21 days of continuous administration is 3.80–5.20 times that of the first day.6 The protein binding rate of ISA is between 98–99%, mainly metabolized by CYP3A4/5 in the liver, and the minor pathway is through UGT glucuronidation, ultimately excreted in feces and urine.7 The inducers of CYP3A4/5 such as rifampicin or inhibitors such as ketoconazole can lead to a significant decrease or increase in the plasma concentration of ISA. generally, ISA do not require therapeutic drug monitoring (TDM), but TDM is recommended for patients with hepatic insufficiency, obesity, or fungal strains with high MIC values.8
Some population pharmacokinetic models of ISA have been developed. This review aims to provide a theoretical basis for improving the pharmacokinetics/pharmacodynamics (PK/PD) control rate and clinical cure rate of ISA by summarizing and summarizing the PK characteristics of these models.
Methods
Retrieval Strategy
PubMed, Embase, CNKI, Wanfang and VIP databases were searched for the literature on the population pharmacokinetics of isaconazole published since the establishment of the database.
“Search terms:” (isavuconazonium OR isavuconazole OR BAL8557 OR BAL4815) AND (“populationpharmacokinetic” OR “pharmacometrics” OR “pharmacokinetic model” OR “population model” OR “popPK” OR “popPK” OR “PPK” OR “nonlinear mixed effect model” OR “NONMEM” OR “NLME” OR “mixed effect” OR “WinNonmix” OR “Monolix”). Additional publications were identified by reviewing the reference lists of the articles identified in the search.
Exclusion Criteria
Population pharmacokinetics in children ≤14 years old; Duplicate publications; Literature with incomplete model type or parameters.
Data Extraction and Quality Assessment
Two reviewers independently screened titles and abstracts of the retrieved records for potentially eligible studies. Data extraction adhered to the Checklist for Critical Appraisal and Data Extraction for Systematic Reviews of Prediction Modeling Studies (CHARMS) and the Prediction model Risk of Bias Assessment Tool (PROBAST).9 The PROBAST was also used to assess the risk of bias for each study based on 20 signaling questions covering 4 domains (participants, predictors, outcome, and analysis). Assessment of the risk of bias was undertaken independently by two reviewers, and disagreements were resolved by consensus.
Results
Literature Search
Sixteen relevant articles were initially retrieved, and 6 duplicate articles were deleted. After screening the titles and abstracts, 7 literatures published between 2016 and 2023 were finally included. The screening flow chart is shown in Figure 1. The characteristics of the included articles, including publication years, sample size, patient characteristics, and dosing regimens, are shown in Table 1. The number of individuals included in the study ranged from 24 to 232 (median 116), with a total of 981 individuals aged 17 to 87 years. The subjects involved healthy volunteers, patients with underlying diseases including hematological diseases, malignancies and solid organ transplantation. The infected fungi included Aspergillus, Mucor, Cryptococcus, and Candida. The race of the subjects involved Caucasians, blacks, and Asians.
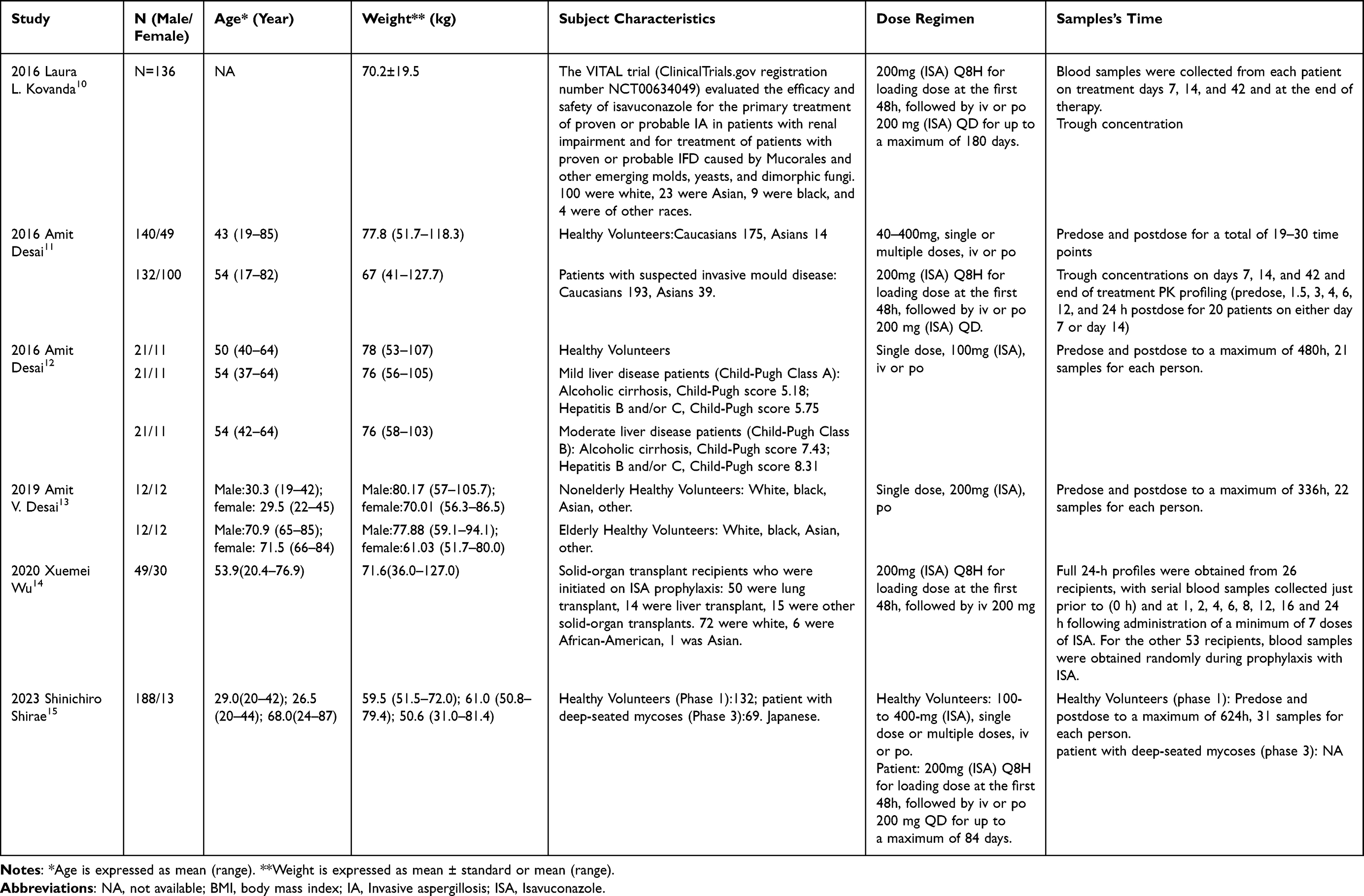 |
Table 1 Demographics of the Published Population Pharmacokinetic Studies |
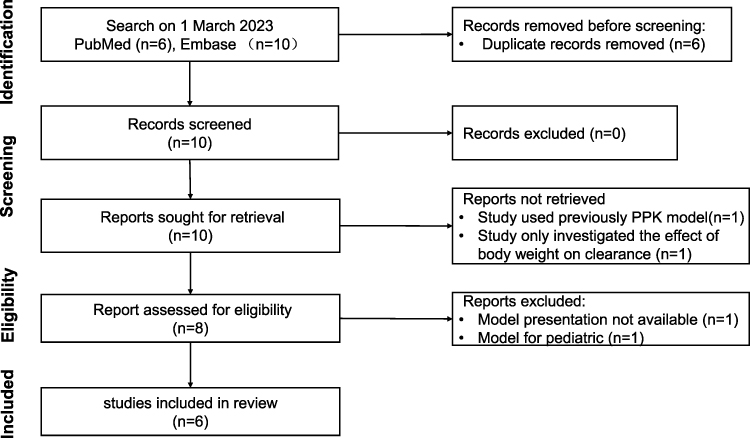 |
Figure 1 The selection process of the studies included in the systematic review. |
Model Building and Evaluation
Table 2 summarizes information on model building and evaluation. The samples used for modeling were all plasma samples, and the concentration of ISA was detected by LC-MS. In terms of dosing regimens, volunteers received a single dose from 40 to 400mg, and patients were treated with 200mg three times a day for the first 48 hours, followed by 200mg once a day. The fitting software involved NONMEM and Pmetrics. The number of samples used for modeling ranged from 458 to 6363 (median was 1449), with an average of 14.9 samples per patient. Except for one study that use Pmetrics, all studies were modeled using NONMEM software. According to visual comparisons, nonparametric bootstrap analysis, normalized prediction distribution errors (NPDE) or bootstrap models are evaluated internally for deviation, reliability, and accuracy, with no models tested externally. Almost all models show satisfactory predictive performance and robustness in internal validation. According to PROBAST, all of the studies were rated as having high overall risk of bias. Although all domains of the studies were rated as low risk of bias, none of them have been developed external validation, so consider downgrading to high risk of bias. Except for one study, all other studies were based on model-simulated dosing regimens or PK/PD target values.
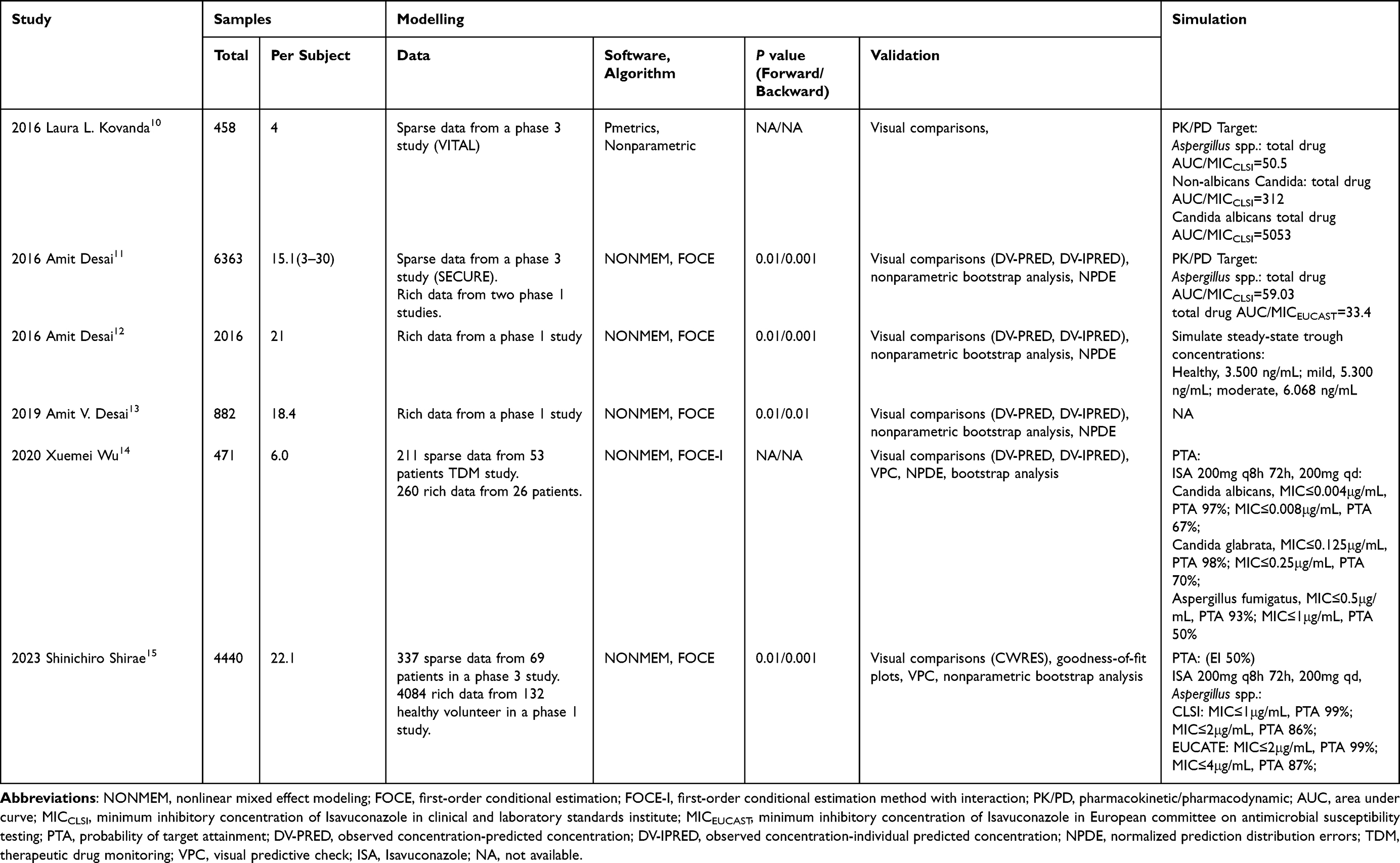 |
Table 2 Model Characteristics of Published Population Pharmacokinetic Studies of Isavuconazonium |
Model Structure
Table 3 summarizes the characteristics of the final model, such as the type of structural model used, pharmacokinetic parameters, model variability, and excluded and retained covariates. All studies used a two-compartment model, first-order elimination. For oral formulations, except for one study that used first-order absorption, all other studies used Weibull absorption. The median of total clearance (CL) and corresponding interindividual variation (IIV) were 1.99 L/h (1.33–4.28 L/h) and 46.1% (31.6–63.0%), respectively. The median volume of central compartment distribution, peripheral compartment distribution and distribution clearance were 50.3 L (9.2–361.2 L), 341 L (122–468 L) and 33.7 L/h (19.2–63.6 L/h), respectively.
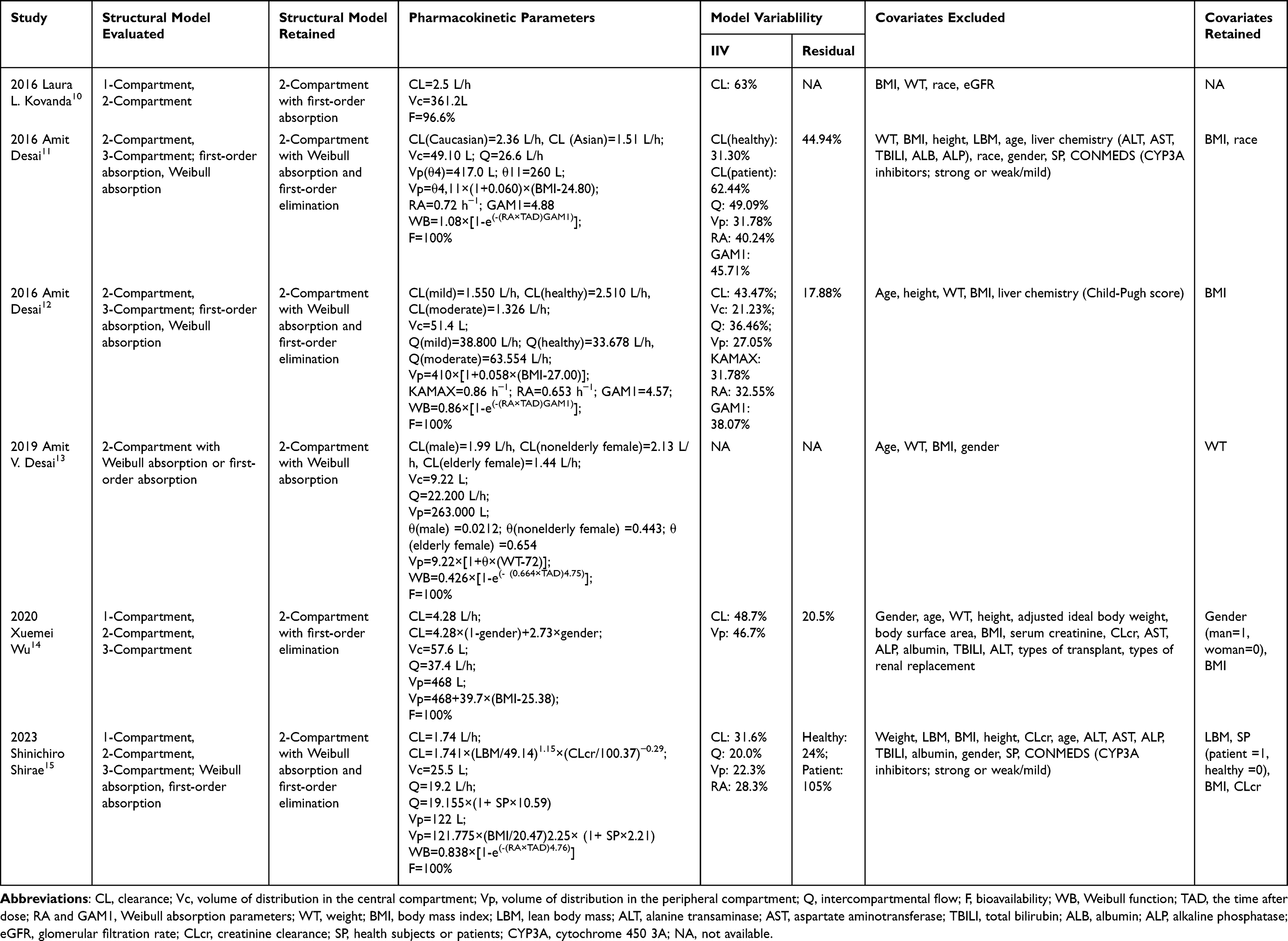 |
Table 3 Results from Published Population Pharmacokinetic Models of Isavuconazonium |
Covariates
In the process of modeling, many factors were investigated, such as healthy volunteers or patients, race, age, sex, height, total body weight (WT), body mass index (BMI), lean body mass, hepatic impairment, creatinine clearance, CYP3A4 inhibitor, and type of transplantation. Four studies included BMI as a covariate, which was positively correlated with peripheral ventricular distribution volume. One study included WT as a covariate, which was positively correlated with the volume of peripheral compartment distribution. One study included race as a covariate, which was associated with total clearance (CL); One study included sex as a covariate, which was associated with CL; In the Japanese study, lean body mass, population type (healthy volunteers/patients), and creatinine clearance were all included as covariates.
PK/PD Target Values and Probability of Target Attainment (PTA)
The model-based PK/PD target values, as well as the probability of target attainment are shown in Table 2. In the calculation of PK/PD index, AUC/MIC was used, where the total drug concentration was used for the calculation of AUC. The AUC/MIC of Aspergillus was 50.5–59.03 based on clinical and laboratory standards institute (CLSI) breakpoints, which was higher than 33.4 based on European committee on antimicrobial susceptibility testing (EUCAST) breakpoints. When the probability of achieving the target was calculated, it was based on the treatment regimen of ISA 200mg q8h for 48 h, followed by 200mg qd maintenance.
Discussion
Parameter estimation methods for population pharmacokinetic modeling mainly include parametric method, non-parametric method and Bayesian method. In the published studies, except for one study that used non-parametric method, the other five studies all used first-order conditional estimation (FOCE) or first order conditional estimation with inter- and intra-subject variability interaction (FOCE-I) in the parameter method. Study using non-parametric method was sparsely sampled, while the studies using parametric methods were densely sampled.
All studies considered the two-compartment model with first-order elimination as the most suitable pharmacokinetic model for ISA. Amit Desai11 and Shinichiro Shirae15 collected the data of Phase I and Phase III clinical trials to fit the pharmacokinetic curves of single-dose and multi-dose administration with one-compartment, two-compartment and three-compartment models, and found that the two-compartment model was more predictive.
For the absorption of itraconazole oral formulations, except for Laura L. Kovanda’s study10 that used first-order absorption, the other studies all used Weibull absorption, which may be related to the sparse sampling used in this study. Absorption phase has been adequately described by the Weibull function in densely sampled studies. The lag time of oral absorption and bioavailability (F) were estimated in the study by Laura L. Kovanda, whereas F=100% was used in the remaining studies.
Although there are differences among the PPK structural models included, the difference in CL estimated by the six studies is not significant (Figure 2), which may be due to the similar population types included in the studies. The total number of people included in all studies was 732, and the number of healthy volunteers (n=352, 48.1%) was relatively high. All the intensive sampling samples were from healthy volunteers, and the patient samples were sparsely sampled. None of the studies included ECMO-supported patients, and the number of CRRT-supported patients included was extremely limited. Secondly, the samples and measurement methods were unified among the studies. Plasma samples were collected and detected by LC-MS.
 |
Figure 2 ISA clearance and between-subject variability of the included studies. |
There may be a certain relationship between race and the PK parameters of ISA. In Amit Desai’s study,11 the CL value of Asians (1.51 L/h) was about 36% lower than that of Caucasians (2.36 L/h), and the CL value of the Japanese population (1.74 L/h) was similar to that of the Asian population in this study. No relationship between race and CL was found in the study by Laura L. Kovanda,10 which may be related to the small number of Asians included in the study. The reasons for racial differences in drug PK may be related to weight-related factors such as BMI and lean body mass, as well as the differences in metabolic phenotypes of cytochrome P450 enzymes, P-glycoprotein and other transport surface types between races, as well as many unknown factors.16 The lower CL of ISA in Asians may be partly due to lower lean body mass.
There was also some relationship between weight-related parameters such as WT, BMI or lean body mass (LBM) and PK parameters of ISA. Theoretically, about 75% of the overweight caused by obesity comes from fat, and as a highly lipophilic drug, ISA is more easily transferred from blood to tissues. Secondly, obesity can also lead to physiological changes such as liver size, biliary excretion capacity, and glomerular filtration rate. Six studies included weight-related parameters to compare the pharmacokinetics of ISA, and in the end, three studies listed BMI as a covariate, one study listed WT as a covariate, and one study listed both BMI and LBM as covariates. In these five studies, weight-related parameters were positively correlated with volume of distribution in the peripheral compartment (Vp). In the study of Amit Desai,11 the distribution of BMI of individuals ranged from 13.89 kg/m2 to 41.18 kg/m2, and Vp of obese patients with BMI > 30 kg/m2 was significantly greater than that of non-obese patients. Similarly, in the study of Xuemei Wu,14 it was found that Vp increased by 39.7L for every one-unit increase in BMI. Although the Vp of obese patients was significantly higher than that of non-obese patients, it did not seem to change the apparent distribution volume of ISA.
The individual healthy volunteer/patient status also has some relationship with the PK parameters of ISA. In the disease state, the serum albumin, liver function, and even the level of the third gap in patients differ from healthy volunteers, resulting in different PK parameters. As a drug with high plasma protein binding rate, ISA may increase the apparent distribution volume and clearance rate of the drug when patients have hypoalbuminemia.17 ISA is mainly metabolized through CYP3A4/5, which leads to slower clearance of the drug when liver dysfunction occurs.18 ISA was widely distributed into tissues, and increases in the third space, continuous renal replacement (CRRT), or (ECMO) circulatory loops, may affect the apparent volume of distribution. In studies by Laura L10 and Amit Desai,11 clearance and AUC of ISA were not different compared to healthy volunteers in invasive fungal infections (IFD) patients with malignancy or neutropenia. The disease status of patients increases the peripheral apparent distribution volume (Vp) of ISA, which means that more drugs are distributed to various tissues in the body, but does not affect the clinical dosing regimen and outcome. In various diseases, the severity of hepatic impairment is significantly correlated with CL, which decreases from 2.51 L/h in healthy people to 1.55 L/h in mild hepatic impairment and 1.32L/h in hepatic impairment.12 No studies have been published in patients with severe hepatic impairment (Child-Pugh C). In addition, in the patient population, the CL of solid organ transplant patients14 (4.28 L/h) was significantly higher than that of other studies (CL, 1.33–2.51 L/h), which may be the result of the combined effect of hypoproteinemia, enlarged third gap, and glucocorticoids. PK studies in a limited subjects continuous renal replacement therapy (CRRT) patients showed19 that the steady-state CL was 4.85±3.79 L/h and the steady-state volume of distribution was 288.78±182.11 L. A case report of pulmonary invasive fungi infection with ECMO support,20 ECMO probably changed the PK of ISA, resulting in a low trough concentration of ISA at the maintenance dose, which may require double the conventional dose to achieve clinical efficacy, which may be related to the increase of the circulatory circuit of ECMO and the chelation of ISA with the circuit.
In addition, ISA acts as a substrate of CYP3A4/5, and inhibitors or inducers of CYP3A4/5 may also have an effect on ISA PK parameters in terms of drug-drug interactions. In the PPK studies of Amit Desai11 and Shinichiro Shirae,15 the effect of inhibitors of CYP3A4/5 on the PK of ISA was investigated, and none of them were finally included as covariates. In the study of Shinichiro Shirae15, all the inhibitors of CYP3A4/5 were moderate or weak, and no strong inhibitors of CYP3A4/5 were included. When ISA was combined with rifampicin, the peak concentration (CMAX) of ISA decreased from 2.4 mg/L to 0.6 mg/L, and AUC decreased from 233.1 h·mg/L to 5.8 h·mg/L. When combined with ketoconazole, a strong inhibitor of CYP3A4/5, the peak concentration of ISA was similar between the two groups, and AUC increased from 84.8 h·mg/L to 466.4 h·mg/L.21 When ISA is combined with ritonavir, which is also a strong inhibitor of CYP3A4/5, AUC only increases by about 1-fold, which was much less than the increase observed with ketoconazole.22 In future studies, more PK data on drug interactions will be needed when including CYP3A4/5 inducers or strong inhibitors as covariates.
In this review, we comprehensively summarize the published PPK model of ISA. In these models, Body mass index (BMI) was main factor affecting the pharmacokinetics of ISA. Other influencing factors included liver function, gender and creatinine clearance. In clinical practice, the potential impact of the patients such as body weight, liver function, renal function and combination medications on drug exposure deserves to be considered. It is necessary to implement dose adjustments or formulation changes in conjunction with routine TDM to obtain desired concentrations and efficacy as well as to reduce fungal resistance. In contrast to internal validation, external evaluation of a model is considered the most rigorous validation method in model testing. However, the currently published PPK model of ISA has not been externally evaluated. Therefore, in the subsequent work, in addition to comparing the predictive performance of the published models, population pharmacokinetic studies will be needed for certain special populations such as patients with severe hepatic damage or those supported by ECMO.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The Nature Science Foundation of Zhejiang province (LYY21H300004); Zhejiang Pharmaceutical Society drug clinical comprehensive evaluation of special scientific research funding project (2022ZYYL02).
Disclosure
Na Chen, Xiaojuan Wang, Yinyan Li, Ping Yang, Mingzhu Huang, Xiaoyang Lu have no conflicts of interest to declare that are relevant to the contents of this review.
References
1. Ellsworth M, Ostrosky-Zeichner L. Isavuconazole: mechanism of action, clinical efficacy, and resistance. J Fungi. 2020;6(4):324–334. doi:10.3390/jof6040324
2. Marty FM, Ostrosky-Zeichner L, Cornely OA, et al. Isavuconazole treatment for mucormycosis: a single-arm open-label trial and case-control analysis. Lancet Infect Dis. 2016;16(7):828–837. doi:10.1016/S1473-3099(16)00071-2
3. Schmitt-Hoffmann A, Desai A, Kowalski D, et al. Isavuconazole absorption following oral administration in healthy subjects is comparable to intravenous dosing, and is not affected by food, or drugs that alter stomach pH. Int J Clin Pharmacol Ther. 2016;54(8):572–580. doi:10.5414/CP202434
4. Kovanda LL, Marth FM, Maertens J, et al. Impact of mucositis on absorption and systemic drug exposure of isavuconazole. Antimicrob Agents Chemother. 2017;61(6):e00101–e00117. doi:10.1128/AAC.00101-17
5. Schmitt-Hoffmann A, Roos B, Heep M, et al. Single-ascending-dose pharmacokinetics and safety of the novel broad-spectrum antifungal triazole BAL4815 after intravenous infusions (50, 100, and 200 milligrams) and oral administrations (100, 200, and 400 milligrams) of its prodrug, BAL8557, in healthy volunteers. Antimicrob Agents Chemother. 2006;50(1):279–285. doi:10.1128/AAC.50.1.279-285.2006
6. Schmitt-Hoffmann A, Roos B, Marres J, et al. Multiple-dose pharmacokinetics and safety of the new antifungal triazole BAL4815 after intravenous infusion and oral administration of its prodrug, BAL8557, in healthy volunteers. Antimicrob Agents Chemother. 2006;50(1):286–293. doi:10.1128/AAC.50.1.286-293.2006
7. Townsend R, Kato K, Hale C, et al. Two phase 1, open-label, mass balance studies to determine the pharmacokinetics of 14C-labeled isavuconazonium sulfate in healthy male volunteers. Clin Pharmacol Drug Dev. 2018;7(2):207–216. doi:10.1002/cpdd.376
8. Kably B, Launay M, Derobertmasure A, et al. Antifungal drugs TDM: trends and update. Ther Drug Monit. 2022;44(1):166–197. doi:10.1097/FTD.0000000000000952
9. Wolff RF, Moons KGM, Riley RD, et al. PROBAST: a tool to assess the risk of bias and applicability of prediction model studies. Ann Inter Med. 2019;170(1):51–58. doi:10.7326/M18-1376
10. Kovanda LL, Desai AV, Lu Q, et al. Isavuconazole population pharmacokinetic analysis using nonparametric estimation in patients with invasive fungal disease (results from the VITAL study). Antimicrob Agents Chemother. 2016;60(8):4568. doi:10.1128/AAC.00514-16
11. Desai A, Kovanda L, Kowalski D, et al. Population pharmacokinetics of isavuconazole from Phase 1 and Phase 3 (SECURE) trials in adults and target attainment in patients with invasive infections due to Aspergillus and other filamentous fungi. Antimicrob Agents Chemother. 2016;60(9):5483–5491. doi:10.1128/AAC.02819-15
12. Desai A, Schmitt-Hoffmann A, Mujais S, et al. Population pharmacokinetics of isavuconazole in subjects with mild or moderate hepatic impairment. Antimicrob Agents Chemother. 2016;60(5):3025–3031. doi:10.1128/AAC.02942-15
13. Desai AV, Han D, Kowalski DL, et al. No dose adjustment for isavuconazole based on age or sex. Antimicrob Agents Chemother. 2019;63(6):e02629–18. doi:10.1128/AAC.02629-18
14. Wu X, Venkataramanan R, Rivosecchi RM, et al. Population pharmacokinetics of intravenous isavuconazole in solid-organ transplant recipients. Antimicrob Agents Chemother. 2020;64(2):e01728–e01819. doi:10.1128/AAC.01728-19
15. Shirae S, Tsuruya Y, Kozaki T, et al. Population pharmacokinetics, exposure-safety, and probability of target attainment analyses for isavuconazole in Japanese patients with deep-seated mycoses. J Clin Pharmacol. 2023;63(6):704–714. doi:10.1002/jcph.2212
16. Ramamoorthy A, Pacanowski MA, Bull J, et al. Racial/ethnic differences in drug disposition and response: review of recently approved drugs. Clin Pharmacol Ther. 2015;97(3):263–273. doi:10.1002/cpt.61
17. Ulldemolins M, Roberts JA, Rello J, et al. The effects of hypoalbuminaemia on optimizing antibacterial dosing in critically ill patients. Clin Pharmacokinet. 2011;50(2):99–110. doi:10.2165/11539220-000000000-00000
18. Schmitt-Hoffmann A, Roos B, Spickerman J, et al. Effect of mild and moderate liver disease on the pharmacokinetics of isavuconazole after intravenous and oral administration of a single dose of the prodrug BAL8557. Antimicrob Agents Chemother. 2009;53(11):4885–4890. doi:10.1128/AAC.00319-09
19. Biagi M, Butler D, Tan X, et al. Pharmacokinetics and dialytic clearance of isavuconazole during in vitro and in vivo continuous renal replacement therapy. Antimicrob Agents Chemother. 2019;63(12):e01085–19. doi:10.1128/AAC.01085-19
20. Zhao Y, Seelhammer TG, Barreto E, et al. Altered pharmacokinetics and dosing of liposomal amphotericin B and isavuconazole during extracorporeal membrane oxygenation. Pharmacotherapy. 2020;40(1):89–95. doi:10.1002/phar.2348
21. Townsend R, Dietz A, Hale C, et al. Pharmacokinetic evaluation of CYP3A4-mediated drug-drug interactions of isavuconazole with rifampin, ketoconazole, midazolam, and ethinyl estradiol/norethindrone in healthy adults. Clin Pharmacol Drug Dev. 2017;6(1):44–53. doi:10.1002/cpdd.285
22. Yamazaki T, Desai A, Han D, et al. Pharmacokinetic interaction between isavuconazole and a fixed-dose combination of lopinavir 400 mg/ritonavir 100 mg in healthy subjects. Clin Pharmacol Drug Dev. 2017;6(1):93–101. doi. doi:10.1002/cpdd.282
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.