Back to Journals » International Journal of General Medicine » Volume 14
Population-based Study Comparing Predictors of Ischemic Stroke Recurrence After Index Ischemic Stroke in Non-elderly Adults with or without Diabetes
Authors Elhefnawy ME ![]() , Sheikh Ghadzi SM, Tangiisuran B, Zainal H, Looi I, Ibrahim KA
, Sheikh Ghadzi SM, Tangiisuran B, Zainal H, Looi I, Ibrahim KA ![]() , Sidek NN, Loo KW, Lee KY
, Sidek NN, Loo KW, Lee KY ![]() , Abdul Aziz Z, Harun SN
, Abdul Aziz Z, Harun SN ![]()
Received 25 January 2021
Accepted for publication 8 March 2021
Published 7 April 2021 Volume 2021:14 Pages 1205—1212
DOI https://doi.org/10.2147/IJGM.S303641
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Marwa Elsaeed Elhefnawy,1 Siti Maisharah Sheikh Ghadzi,1 Balamurugan Tangiisuran,1 Hadzliana Zainal,1 Irene Looi,2 Khairul Azmi Ibrahim,3 Norsima Nazifah Sidek,3 Keat Wei Loo,4 Keng Yee Lee,5 Zariah Abdul Aziz,3 Sabariah Noor Harun1
1School of Pharmaceutical Sciences, Universiti Sains Malaysia, Penang, 11800, Malaysia; 2Clinical Research Centre, Seberang Jaya Hospital, Penang, Malaysia; 3Clinical Research Centre, Hospital Sultanah Nur Zahirah, Terengganu, Malaysia; 4Department of Biological Science, Faculty of Science, Universiti Tunku Abdul Rahman (UTAR) Kampar Campus, Perak, Malaysia; 5National Clinical Research Centre, Kuala Lumpur, Malaysia
Correspondence: Sabariah Noor Harun
Discipline of Clinical Pharmacy, School of Pharmaceutical Sciences, Universiti Sains Malaysia, Penang, 11800, Malaysia
Tel +604-6532487
Email [email protected]
Background and Purpose: Factors associated with ischemic stroke (IS) recurrence and the contribution of pharmacological treatment as secondary preventions among nondiabetics especially in the non-elderly population are unclear and not widely investigated. This was a population-based study that aimed to identify recurrent IS predictors and to determine the possible impact of secondary preventive medications on the IS recurrence in non-elderly adults with or without diabetes.
Methods: Data of 3386 patients < 60 years old who had a history of index IS were extracted from the Malaysian National Neurology Registry (NNEUR) from 2009 to 2016. Recurrent IS was defined as any IS event recorded after the index IS in the NNEUR database. Multivariate logistic regression analysis was performed by using SPSS version 22.
Results: Ischemic heart disease (IHD) was the significant predictor of IS recurrence in non-elderly adults both with or without diabetes (adjusted odds ratio (AOR) of 3.210; 95%CI: 1.909– 5.398 and 2.989; 95%CI: 1.515– 5.894) respectively). Receiving antiplatelet as secondary stroke prevention (AOR: 0.194; 95%CI: 0.046– 0.817) and continuation of antidiabetic medication after the index IS event (AOR: 0.510; 95%CI: 0.298– 0.872) reduced the odds of IS recurrence only in non-elderly diabetic adults. Among non-elderly adults without diabetes, hyperlipidemia and every increased in 1 mmHg of systolic blood pressure significantly increased the odds of IS recurrence following the indexing event (AOR: 1.796; 95%CI: 1.058– 3.051 and 1.009; 95%CI: 1.002– 1.016 respectively).
Conclusion: IHD was found as the main predictor of IS recurrence regardless of diabetes status in non-elderly adults after the index IS event. Receiving antidiabetic and antiplatelet medications upon discharge after index IS were significant predictors of recurrent IS in non-elderly diabetic adults. A proper randomized clinical trial may be required to determine the impact of secondary preventive medication on IS recurrence, especially in non-elderly adults.
Keywords: ischemic stroke, recurrence, prevention, diabetic, nondiabetic, non-elderly
Introduction
Stroke is the second leading cause of mortality and morbidity worldwide.1–4 Having diabetes mellitus (DM) increases the risk of ischemic stroke (IS) two-to-five-fold.5,6 Because of the strong association between DM and other stroke risk factors,7 diabetic patients with stroke are also known to have poor prognosis, higher mortality rate,8 and high risk of recurrent stroke compared to those without DM.9 In Malaysia, 27.4% to 55.2% population with IS have DM,10 and this indicates almost 50% of the stroke population are nondiabetics. Moreover, almost 33% of the IS population had recurrent stroke.10 DM is a well known risk factor of recurrent IS, however is there any difference in terms of recurrent IS between those with or without DM? What would be the risk factor of recurrent IS in those who do not have DM? Any difference in risk factors of recurrent stroke in adults with or without DM need to be investigated to tailor better preventive strategies and early management especially at the stage of screening for DM.
In a group of adult patients with IS, 10–15% of all strokes were experienced by so-called “young stroke” adults.11 Nevertheless, heterogeneity in “young stroke” definition lead to a wide range of stroke incidence in this patient population.11 Emerging data has elevated public health concerns about the increasing prevalence of vascular risk factors in young adults, and their potential role in increasing the risk of IS, and stroke recurrence.12 Although the global risk of mortality is low, stroke in young adults has severe implications. Only about 50% of patients are fully recovered and return to work after the first-ever ischemic stroke, and the risk of recurrent stroke is greater for the survivors of acute IS.13–15 Loss of working years and long-term dependency on social care may affect the socioeconomic outcome of non-elderly adults with stroke.16 Thus, stroke prevention and improvement of outcomes are particularly crucial in this group.
Age limits defining “young stroke“ adults differ across studies in which age ranges of 18 to upper age limit of 55 years were the most used.17–19 Nevertheless, in Malaysia older persons are defined as those who are 60 years and over.20 Therefore, this current study involved the adult population aged 18 to <60 years old and term “non-elderly” adults is used throughout the manuscript. This aim of this study was to identify predictors of recurrent IS in non-elderly adults with or without DM. The possible benefits of secondary prevention medications on the recurrent IS between diabetics and nondiabetic non-elderly adults were also investigated in this study.
Method
Study Population and Design
Data of all Malaysian patients with history of index IS who were 18 to <60 years old from August 2009 to December 2016, were extracted from the National Neurology Registry (NNEUR) of Malaysia. The details on the National Stroke Registry of Malaysia were published previously.21 The stroke was diagnosed according to the World Health Organization’s criteria.22 All diagnoses were confirmed using brain computed tomography or magnetic resonance imaging. The patient’s neurological function deficit was evaluated using the National Institute of Health Stroke Scale (NIHSS), and the Modified Rankin Scale (MRS) upon admission. DM was either defined as patient’s self-reported, physician diagnosis, or based on the use of hypoglycemic medications prior to the index ischemic stroke, during hospitalization secondary to stroke or at discharge. Index stroke was defined as first stroke registered into the NNEUR for the particular patient from 2009 to 2016. Recurrent IS was defined as any IS event recorded by the involving hospital after the index IS for a particular patient in the NNEUR database. Data of non-Malaysian, patients registered as having epilepsy or seizure and data that have missing information on citizenship status were excluded from this study.
Ethics Approval
Ethical approval for this study was obtained from the Medical Research and Ethics Committee (MREC), Ministry of Health, Malaysia (Research ID: NMRR-08-1631-3189).
Stroke Registry in Malaysia
The NNEUR in Malaysia was initiated and established in 2009. The NNEUR has recorded data from multi-ethnic involving stroke cases from 13 states in the country. The aim of the NNEUR is to provide comprehensive epidemiological data on the country’s stroke statistics, trend, and management, representing an ongoing multicenter, hospital-based registry. The registry development is funded by the Ministry of Health, Malaysia (MOH). The comprehensive explanation on the NNEUR has been previously described.23
Investigated Variables
In this study, investigated variables include demographic data such as gender and ethnicity. Malaysians comprise of ethnic groups such as Malay, Chinese and Indians, and others. Most of the other ethnics such as Ibans, Kadazan/Dusun are from East Malaysia. Educational status, either a formal or an informal education (those who received a formal type of education as in graduate schools and collages), was also investigated. Data during the index IS event were included as variables. These data were vital signs at emergency department, clinical presentation apparent at the start of the index IS (eg headache, speech disturbance, hemiparesis) and NIHSS as the physical examination tool. Data on the risk factors of stroke that patients have as well as medications taken prior to index IS event such as angiotensin converting enzyme inhibitors (ACEIs), antihyperlipidemic drugs either indicated for primary stroke prevention or for other indications were also included. In addition, medications prescribed upon discharge from hospitalization secondary to index IS event either indicated for secondary stroke prevention or for other indications were included as variables. Other laboratory clinical data such as total cholesterol level, blood glucose level (random) taken throughout the hospitalization secondary to stroke event were also included as variables.
Analysis
The data were stratified into population with DM or without DM. Statistical analyses were performed using SPSS version 22.0 (IBM Corporation, Armonk, NY, USA). The categorical variables were presented in percentages, while the values for continuous variables were expressed as mean ± standard deviation. A comparison between groups were analysed using chi-squared and Fisher’s exact tests for categorical variables, while an independent sample t-test was used for continuous data. The significant variables obtained from the univariate analysis were then included into the multivariate logistic regression and association between exposure and outcomes was reported as an OR with a 95%CI. In order to minimize bias from missing data, the pattern of missing values of independent variables was analyzed. Multiple imputations were used to handle variables with missing values above 5%. Missing values in body mass index (BMI), prior medications, and total cholesterol level during the index IS event were imputed from multiple imputation methods. Five imputations were used, and Rubin’s rules were implemented to combine the results. A P-value of <0.05 was considered significant in both univariate and multivariate analyses.
Results
Descriptive Results
A total of 3386 of non-elderly adults with or without DM have been extracted and included in this study. The median time from index stroke to recurrent stroke was 4.2 months. As shown in Table 1, the majority of the patients in both groups were female. Of the 1576 non-elderly adults with DM, 96 (6.1%) had recurrent IS whereas among the 1820 nondiabetics, 69 (3.8%) had recurrent IS after the index IS event. Nondiabetics (N=902, 53%) were more obese than their diabetic peers (N=651, 41.3%). In both groups, the majority of data in the database were contributed from hospitals in East Malaysia, hence the higher number of other ethnicities in the results. The percentages of smokers in both diabetic and nondiabetic groups were 53.6% and 49.2% respectively. One thousand two hundred and ninety-nine (82.4%) diabetics and 959 (53%) nondiabetics had concurrent hypertension upon the index IS presentation. The number of subjects with hyperlipidemia in the diabetic group was 528 (33.5%), while in the nondiabetic group it was 374 (20.7%). The number of patients who had ischemic heart disease (IHD) was higher in the diabetic group (186, 11.8%) than the nondiabetic group (133, 7.3%). Non-elderly adults with DM group had more death stroke outcomes (7.2%) compared to the nondiabetic group (5.3%) (Table 1)
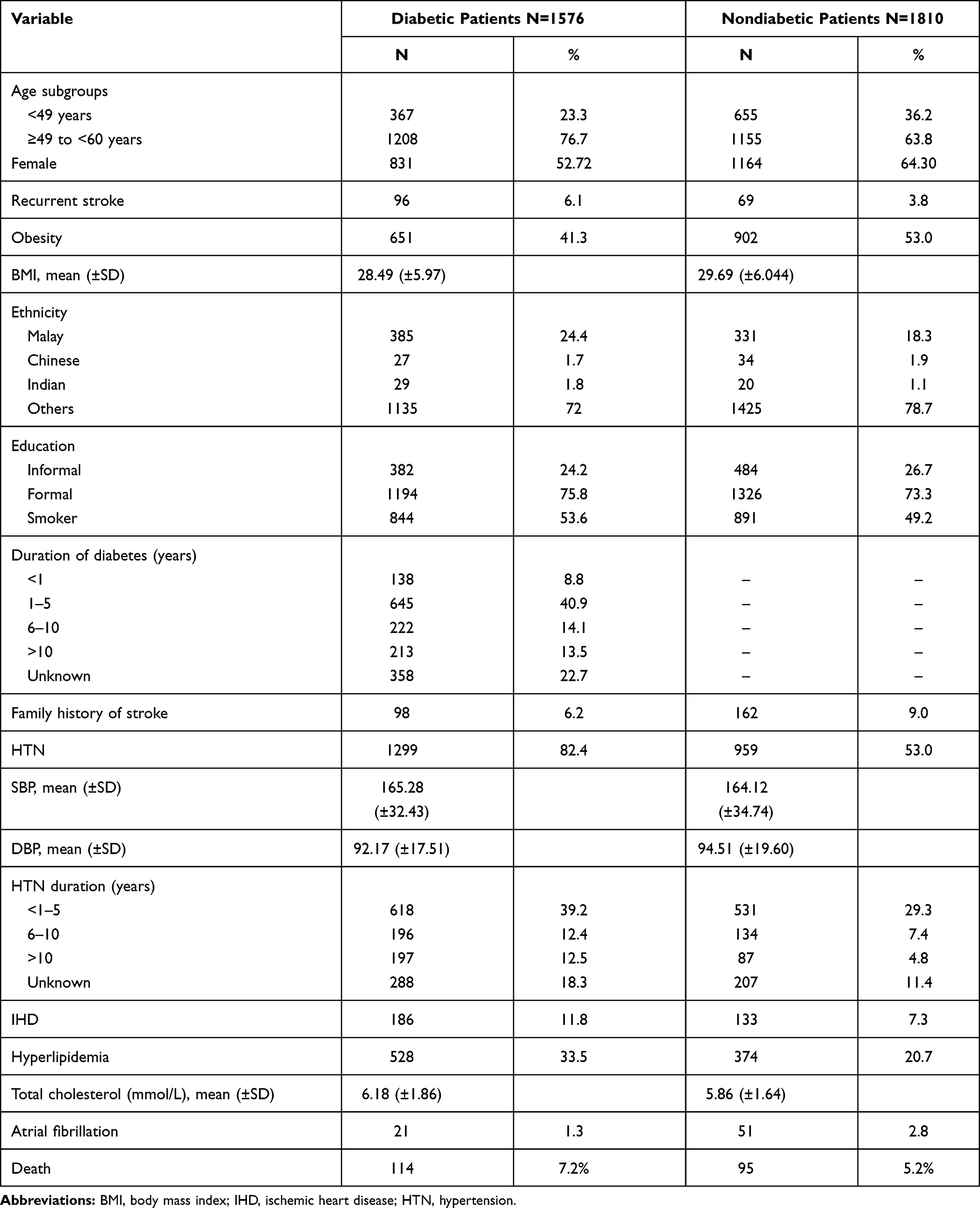 |
Table 1 Characteristics of Diabetics and Nondiabetics Non-elderly Adults (Aged <60 Years) with History of Index Ischemic Stroke Attack that were Included in the Study (N=3386) |
Comparison of Recurrent Ischemic Stroke Predictors in Diabetic and Nondiabetic Non-elderly Adults
Significant predictors of IS recurrence after the index IS event both for diabetic and nondiabetic non-elderly adults are showed in Table 2. IHD increased the odds of having recurrent IS in both groups significantly with adjusted odds ratio (AOR) of 3.21 (95%CI: 1.91–5.40) and 2.99 (95%CI: 1.52–5.90), respectively. The increase of 1 mmHg in SBP upon admission for index IS event was found to increase the odds of IS recurrence in the nondiabetic group significantly (AOR: 1.01; 95%CI: 1.01–1.02). Hyperlipidemia significantly increased the odds of having IS recurrence in nondiabetics but not in their diabetic peers. Patients who were given antiplatelet drugs upon hospital discharge after the index IS event reduced the odds of having recurrent IS in the diabetic group significantly (AOR: 0.19; 95%CI: 0.05–0.82) but had no significant influence on the nondiabetic group. Continuation of antidiabetic medications (ADMs) after the index IS event was shown to significantly reduce the odds of having IS recurrence in the diabetic group (AOR: 0.51; 95%CI: 0.30–0.87). Clinical manifestation apparent at the point of index IS such as speech disturbance and hemiparesis were found significant in the univariate model but were removed in the final multivariate model both in the diabetic and nondiabetic groups (Table 2).
 |
Table 2 Univariate and Multivariable Logistic Regression Analysis of Variables Associated with Recurrent Ischemic Stroke in Diabetic and Nondiabetic Non-elderly Adults (Aged <60 Years) After Index Ischemic Stroke Attack (N=3386) |
Discussion
This study identified predictors of IS recurrence after index IS event in non-elderly Malaysian with and without DM. Non-elderly Malaysian adults were reported to have higher rate of stroke incidence than the elderly group.24 Regardless of DM status, IHD was found to be an independent predictor of recurrent IS in the current study whereby patients with history of IHD have three times the risk of IS recurrence. This finding is consistent with data reported previously21,25–29 which illustrates that IHD should be considered as the main indicator of recurrent IS regardless of age and DM status. IS shares a similar pathophysiology with IHD, mainly because atherosclerosis is manifested in both conditions.28 Patients who are affected by atherosclerosis become at risk for acute coronary syndrome and acute stroke. In both cases, a sudden change of circulation arises, and as a result the blood supply was decreased to part of the brain or heart.28
In this study, antiplatelet medication prescribed upon discharge from hospital secondary to index IS event significantly reduced the probability of recurrent IS by 80% in the non-elderly with DM. This finding supports the recommendation of antiplatelet medication as a mainstay preventive therapy for recurrent stroke, especially in patients with a modifiable risk factor such as DM.30 Interestingly, but not surprisingly, antiplatelet therapy received upon discharge from hospital secondary to index IS was not a statistically significant factor influencing the odds of recurrent IS in the non-elderly without DM. Similarly, in the subanalysis done (Supplementary Document), receiving antiplatelet medication only upon discharge from the hospital secondary to index IS, was not significantly associated with recurrent IS in the same population. However, with a small number of patients with recurrent IS in this current analysis, caution must be applied, as the findings may go against the well-known recommendation of antiplatelet as secondary prevention of IS. Moreover, in the current analysis, the indication of antiplatelet medication prescribed upon discharge from the hospital could be indicated either for a secondary prevention of recurrent IS or for other reasons.
Optimizing the management of hyperlipidemia may play a vital role in reducing recurrent IS in the non-elderly without DM as hyperlipidemia significantly increased the probability of recurrent IS in this population by 79.6%. This finding may indirectly support the previous hypotheses in which stroke experienced by diabetic may differ from nondiabetics. This could be explained by the angiopathy resulting from DM and atherosclerotic plaque.31
The reported effect of BP during the acute stroke presentation varies between previous studies. High BP at the presentation of acute stroke is associated with poor functional outcomes,32 and poses a higher risk of recurrent stroke.33,34 This effect appears to be independent of prognostic factors such as age, stroke severity, level of consciousness, and atrial fibrillation.30 While in another study, high BP on arrival at the emergency room is associated with improved functional outcomes in elderly patients with stroke (mean >78 years).35 Nevertheless, the current study supports the previous findings that high BP at the presentation of acute IS or on arrival at the emergency room, increased the risk of recurrent IS. Moreover, this study showed that every 1 mmHg increase in SBP at presentation of acute IS significantly increased the probability of recurrent IS by 0.9% in non-elderly without DM but not in their peers with DM. The inconsistency of the reported effect of BP on the stroke outcome may be due to difference in stroke outcomes being investigated and the duration of outcomes from the acute stroke event. In most of the previous studies, the post-acute stroke functional outcome was measured at least after 12 months of the acute event while for mortality or recurrent stroke, the outcomes were investigated at least after two years or longer after the acute event. This suggests that the effect of higher BP on admission may have a beneficial short-term effect, but a deleterious long-term effect. This phenomenon has also been suggested in a previous study.35 Elevated BP during acute IS might be either advantageous by improving cerebral perfusion to the ischemic tissue or harmful by exacerbating cerebral edema and hemorrhagic transformation of the ischemic tissue.32,33,36.
Limitations
This study was a retrospective study based on the available data from the National Stroke Registry of Malaysia. Therefore, the first stroke captured from the NNEUR from 2009 to 2016 was assumed to be the first ever stroke experienced by the patient. Any data on the prior TIA or stroke prior to the NNEUR establishment was not available and not taken into account in the current study. Furthermore, medications prescribed upon discharge from hospital secondary to index IS event either served as the indicator for secondary stroke prevention or for other indications were included in this study. Thus, the factors that may influence these medication effects such as adherence are unknown. Data on stoke etiology, diet and lifestyle, and recreational drug use, were not available, which could be influential factors of stroke. Data on medication adherence was available, however the usage of the data in the current analysis was limited with high missing value in which handling with data imputation may not be feasible. Besides, missing data on estrogenic intake constrained us from identifying it as a predictor of recurrent IS in non-elderly women. In addition, an external validation cohort is required to verify these results. Nevertheless, this study was a population-based study and large samples representing various ethnic groups across the country, as well as data from real clinical practice, have been used. Moreover, most of the previous studies compare the risk factors of poor functional outcome secondary to stroke between diabetics and nondiabetics but in terms of recurrent stroke; it is very limited especially in the non-elderly population. Thus, the current study may shed some light on the predictors of recurrent IS between non-elderly with andor without DM. Furthermore, this study highlights the possible role of secondary prevention of IS recurrence in the non-elderly population.
Conclusions
IHD was found as the main predictor of IS recurrence regardless of DM status in non-elderly adults after the index IS event. Received antiplatelet medication and ADMs upon discharge after index IS significantly reduced the odds of IS recurrence in non-elderly adults with DM while 1 mmHg elevation in SBP at presentation of acute IS and hyperlipidemia significantly increase the odds of IS recurrent in their peers without DM. A proper randomized clinical trial may be required to determine the impact of secondary preventive medication on the IS recurrence especially in non-elderly adults.
Acknowledgment
The authors would like to acknowledge the Director General of Health Malaysia for his permission to publish this work. This study has been supported by the Short-Term Grants from Universiti Sains Malaysia (304/PFARMASI/6315188).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zheng S, Yao B. Impact of risk factors for recurrence after the first ischemic stroke in adults: a systematic review and meta-analysis. J Clin Neurosci. 2019;60:24–30. doi:10.1016/j.jocn.2018.10.026
2. Oza R, Rundell K, Garcellano M. Recurrent ischemic stroke: strategies for prevention. Am Fam Physician. 2017;96(7):436–440.
3. Putaala J, Liebkind R, Gordin D, et al. Diabetes mellitus and ischemic stroke in the young: clinical features and long-term prognosis. Neurology. 2011;76(21):1831–1837. doi:10.1212/WNL.0b013e31821cccc2
4. Jin P, Matos Diaz I, Stein L, Thaler A, Tuhrim S, Dhamoon MS. Intermediate risk of cardiac events and recurrent stroke after stroke admission in young adults. Int J Stroke. 2018;13(6):576–584. doi:10.1177/1747493017733929
5. Jamrozik K, Broadhurst RJ, Forbes S, Hankey GJ, Anderson CS. Predictors of death and vascular events in the elderly: the Perth Community Stroke Study. Stroke. 2000;31(4):863–868. doi:10.1161/01.STR.31.4.863
6. Davis TM, Millns H, Stratton IM, Holman RR, Turner RC. Risk factors for stroke in type 2 diabetes mellitus: United Kingdom Prospective Diabetes Study (UKPDS) 29. Arch Intern Med. 1999;159(10):1097–1103. doi:10.1001/archinte.159.10.1097
7. Tun NN, Arunagirinathan G, Munshi SK, Pappachan JM. Diabetes mellitus and stroke: a clinical update. World J Diabetes. 2017;8(6):235. doi:10.4239/wjd.v8.i6.235
8. Sander D, Sander K, Poppert H. Stroke in type 2 diabetes. Br J Diabetes Vasc Dis. 2008;8(5):222–229. doi:10.1177/1474651408096677
9. Anwar MMU, Jahan SMS, Afrin S, Hossain MZ. Diabetic and non-diabetic subjects with ischemic stroke: risk factors, stroke topography and hospital outcome. J Med. 2017;18(2):75–79. doi:10.3329/jom.v18i2.33684
10. Kooi CW, Peng HC, Aziz ZA, Looi I. A review of stroke research in Malaysia from 2000–2014. Med J Malaysia. 2016;71:58–69.
11. Sarecka-Hujar B, Kopyta I. Risk factors for recurrent arterial ischemic stroke in children and young adults. Brain Sci. 2020;10(1):24. doi:10.3390/brainsci10010024
12. Singhal AB, Biller J, Elkind MS, et al. Recognition and management of stroke in young adults and adolescents. Neurology. 2013;81(12):1089–1097. doi:10.1212/WNL.0b013e3182a4a451
13. Varona JF. Long-term prognosis of ischemic stroke in young adults. Stroke Res Treat. 2011;2011:1–5. doi:10.4061/2011/879817
14. Donnan GA, Fisher M, Macleod M, Davis SM. Stroke. Lancet. 2008;371(9624):1612–1623. doi:10.1016/S0140-6736(08)60694-7
15. Davis SM, Donnan GA. Secondary prevention after ischemic stroke or transient ischemic attack. N Engl J Med. 2012;366(20):1914–1922. doi:10.1056/NEJMcp1107281
16. Kappelle LJ, Adams HP
17. Stack CA, Cole JW. A diagnostic approach to stroke in young adults. Curr Treat Options Cardiovasc Med. 2017;19(11):84. doi:10.1007/s11936-017-0587-6
18. von Sarnowski B, Putaala J, Grittner U, et al. Lifestyle risk factors for ischemic stroke and transient ischemic attack in young adults in the Stroke in Young Fabry Patients study. Stroke. 2013;44(1):119–125. doi:10.1161/STROKEAHA.112.665190
19. Putaala J, Metso AJ, Metso TM, et al. Analysis of 1008 consecutive patients aged 15 to 49 with first-ever ischemic stroke: the Helsinki young stroke registry. Stroke. 2009;40(4):1195–1203. doi:10.1161/STROKEAHA.108.529883
20. Malaysia, C.R., Country Reports Malaysia; 2012. http://www.mhlw.go.jp/bunya/kokusaigyomu/asean/2013/dl/Malaysia_CountryReport.pdf.
21. Aziz S, Sheikh Ghadzi SM, Abidin NE, et al. Gender differences and risk factors of recurrent stroke in Type 2 diabetic malaysian population with history of stroke: the Observation from Malaysian National Neurology Registry. J Diabetes Res. 2019;2019:1–10. doi:10.1155/2019/1794267
22. Truelsen T, Heuschmann P, Bonita R, et al. Standard method for developing stroke registers in low-income and middle-income countries: experiences from a feasibility study of a stepwise approach to stroke surveillance (STEPS Stroke). Lancet Neurol. 2007;6(2):134–139. doi:10.1016/S1474-4422(06)70686-X
23. Aziz ZA, Lee YY, Sidek NN, et al. Gender disparities and thrombolysis use among patient with first-ever ischemic stroke in Malaysia. Neurol Res. 2016;38(5):406–413. doi:10.1080/01616412.2016.1178948
24. Chen Y-M, Lin Y-J, Po HL. Comparison of the risk factor profile, stroke subtypes, and outcomes between stroke patients aged 65 years or younger and elderly stroke patients: a hospital-based study. Int J Gerontol. 2013;7(4):205–208. doi:10.1016/j.ijge.2012.11.011
25. Gongora-Rivera F, Labreuche J, Jaramillo A, Steg PG, Hauw -J-J, Amarenco P. Autopsy prevalence of coronary atherosclerosis in patients with fatal stroke. Stroke. 2007;38(4):1203–1210. doi:10.1161/01.STR.0000260091.13729.96
26. Touzé E, Varenne O, Calvet D, Mas J-L. Coronary risk stratification in patients with ischemic stroke or transient ischemic stroke attack. Int J Stroke. 2007;2(3):177–183. doi:10.1111/j.1747-4949.2007.00136.x
27. De Silva DA, Woon FP, Moe KT, Chen C, Chang HM, Wong MC. Concomitant coronary artery disease among Asian ischaemic stroke patients. Ann Acad Med Singapore. 2008;37(7):573–575.
28. Palomeras Soler E, Casado Ruiz V. Epidemiology and risk factors of cerebral ischemia and ischemic heart diseases: similarities and differences. Curr Cardiol Rev. 2010;6(3):138–149. doi:10.2174/157340310791658785
29. Fu G-R, Yuan W-Q, Du W-L, et al. Risk factors associated with recurrent strokes in young and elderly patients: a hospital-based study. Int J Gerontol. 2015;9(2):63–66. doi:10.1016/j.ijge.2015.02.004
30. Leonardi-Bee J, Bath PM, Phillips SJ, Sandercock PA. Blood pressure and clinical outcomes in the International Stroke Trial. Stroke. 2002;33(5):1315–1320. doi:10.1161/01.STR.0000014509.11540.66
31. Chen W, Pan Y, Jing J, et al. Recurrent stroke in minor ischemic stroke or transient ischemic attack with metabolic syndrome and/or diabetes mellitus. J Am Heart Assoc. 2017;6(6):e005446. doi:10.1161/JAHA.116.005446
32. Willmot M, Leonardi-Bee J, Bath PM. High blood pressure in acute stroke and subsequent outcome: a systematic review. Hypertension. 2004;43(1):18–24. doi:10.1161/01.HYP.0000105052.65787.35
33. Jauch EC, Saver JL, Adams HP
34. Li C, Zhang Y, Xu T, et al. Systolic blood pressure trajectories in the acute phase and clinical outcomes in 2-year follow-up among patients with ischemic stroke. Am J Hypertens. 2019;32(3):317–325. doi:10.1093/ajh/hpy174
35. Bager JE, Hjalmarsson C, Manhem K, Andersson B. Acute blood pressure levels and long‐term outcome in ischemic stroke. Brain Behav. 2018;8(6):e00992. doi:10.1002/brb3.992
36. Fagan SC, Bowes MP, Lyden PD, Zivin JA. Acute hypertension promotes hemorrhagic transformation in a rabbit embolic stroke model: effect of labetalol. Exp Neurol. 1998;150(1):153–158. doi:10.1006/exnr.1997.6756
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.