Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 15
Poor Self-Care Practices and Being Urban Resident Strongly Predict Chronic Complications Among Patients with Type 2 Diabetes in Eastern Ethiopia: A Hospital-Based Cross-Sectional Study
Authors Letta S ![]() , Aga F
, Aga F ![]() , Yadeta TA, Geda B
, Yadeta TA, Geda B ![]() , Dessie Y
, Dessie Y
Received 22 April 2022
Accepted for publication 12 July 2022
Published 20 July 2022 Volume 2022:15 Pages 2095—2106
DOI https://doi.org/10.2147/DMSO.S368165
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ming-Hui Zou
Shiferaw Letta,1 Fekadu Aga,2 Tesfaye Assebe Yadeta,1 Biftu Geda,3 Yadeta Dessie4
1School of Nursing and Midwifery, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia; 2School of Nursing and Midwifery, College of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia; 3Department of Nursing, College of Health Sciences, Madda Walabu University, Shashamene Campus, Shashamene, Ethiopia; 4School of Public Health, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia
Correspondence: Shiferaw Letta, School of Nursing and Midwifery, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia, Tel +251911771934, Email [email protected]
Background: Diabetes, together with its complications, has a considerable negative influence on people’s quality of life and healthcare delivery and raises diabetic mortality. However, there is limited information about the diabetes-associated chronic complications in the study setting. Therefore, this study aimed to determine the burden and factors related to the chronic complications among patients with type 2 diabetes (T2D) in Eastern Ethiopia.
Methods: A hospital-based cross-sectional study was conducted among 879 patients with T2D at two public hospitals in Harar. The data were collected through interviews using a structured questionnaire. Data related to the diagnosis of chronic complications and biochemical tests were extracted from medical records. The outcome variable was the number of chronic complications that happened to the patients. A generalized Poisson regression model with robust variance estimation was used to investigate the association of independent variables with chronic complications. An adjusted prevalence ratio with a 95% CI was reported to show an association using a p-value ≤ 0.05.
Results: One or more chronic complications were presented in 43% of T2D (95% CI: 39.65, 46.19). Macrovascular and microvascular complications were found in 27.6% and 23.5% of patients, respectively. Urban residence (APR = 2.64; 95% CI: 1.54, 4.54), low wealth status (APR = 1.80; 95% CI: 1.17, 2.76), diabetes duration ≥ 5 years (APR = 1.46; 95% CI: 1.05, 2.01), hypertriglyceridemia (APR = 1.48; 95% CI: 1.07, 2.09) and poor self-care practices (APR = 1.62; 95% CI: 1.18, 2.23) were factors significantly associated with the chronic complications.
Conclusion: The burden of chronic complications was high, with nearly half of T2D patients experiencing one or more chronic complications. Almost one in ten patients suffered from multiple chronic complications. The complications were mainly influenced by being urban resident, low wealth status, and poor self-care practices. Therefore, health care providers need to educate patients and promote self-care practices and healthy lifestyles to achieve treatment goals and lower the risk of chronic complications.
Keywords: chronic complications, type 2 diabetes, Harar, Eastern Ethiopia
Introduction
Type 2 diabetes (T2D) is the most common type of diabetes that highly affects low-and middle-income countries (LMICs).1 According to the International Diabetes Federation (IDF), an estimated 537 million adults aged 20–79 are living with diabetes while about 240 million have undiagnosed diabetes worldwide.2
Even though self-care practice is a key component of diabetes management to prevent patients’ morbidity and premature death,3 it is affected by patients, health care providers, and system-related barriers.4 Moreover, prolonged hyperglycemia increased the risk of chronic complications.5,6 These complications are broadly branded into vascular, and non-vascular complications.1 The microvascular complications include neuropathy, nephropathy, retinopathy, and sexual dysfunction.7 Macrovascular complications occur due to damage to the large vessel, resulting in a stroke, coronary artery diseases, heart failure, and peripheral artery diseases including foot ulcers, gangrene, and lower limb amputations.8 Most vascular complications are worsened by uncontrolled blood pressure and hyperglycemia with limited access to appropriate diabetes care.9 Gastroparesis, skin changes, hearing loss, and infections are non-vascular complications and a significant proportion of patients also had multiple chronic complications.10–12
Globally, about 6.7 million adults die because of diabetes-related complications.2 Cardiovascular disease is a major cause of premature morbidity and mortality.7,13,14 Diabetes also increases the risk of tuberculosis, pneumonia, sepsis, dental diseases, and birth complications.15,17 Most of these complications likely occur during a productive time of life that results in extensive economic sequelae.7,18 Diabetes also affects people’s quality of life19 and drains healthcare systems.18 Specifically, vascular complications, hyperlipidemia, obesity, and erectile dysfunction are rampant in Sub-Saharan Africa including Ethiopia.16,20–22
The Ethiopian Federal Ministry of Health has made several steps to mitigate its impacts, through developing a national strategic plan for prevention and control,23 conducting a countrywide survey to identify common risk factors for non-communicable diseases (NCDs),24 and advocating for small-scale studies that would generate local evidence.12,21,25 Following that, studies conducted in different parts of the country showed a considerable burden of chronic complications, ranging from 24.5% to 42.5% among adult patients with diabetes.10,11,26 Other studies also found that sociodemographic, clinical, and behavioral factors influence diabetes complications.10,11,27–31
Some of the studies done so far in Ethiopia largely focused on microvascular complications32–35 while one study assessed only hypertensive heart diseases, heart failure, and stroke from numerous macrovascular complications.36 To the best of our literature review, both macrovascular and non-vascular complications remained less explored. There was also a scarcity of information about factors relevant to chronic complications in the study area. Therefore, this study aimed to determine the burden, and factors related to chronic complications among patients with T2D on follow-up in Harar, Eastern Ethiopia. The findings of this study are thought to have significant implications for health planners, and implementers to draw tailored strategies that prevent, and mitigate the impact of diabetes-associated chronic complications.
Materials and Methods
Study Setting and Design
A cross-sectional study was conducted among patients with T2D at two public health hospitals in Harar over four months until March 30, 2021. Harar city is in eastern Ethiopia, which is 526 kilometers away from Addis Ababa. Hiwot Fana Specialized Comprehensive Hospital and Jugal General Hospital are public hospitals that offer health services in each department for the entire community of Eastern Ethiopia and neighboring regions and zones. In addition to other services, there are established chronic follow-up clinics that provide services such as regular blood glucose tests, medication refills, and complication screening for 1985 diabetes patients (1333 T2D were attending their care at Jugal General hospital, whereas 652 were attending their care at Hiwot Fana Specialized Comprehensive Hospital). Nurses are among the frontline team of allied disciplines involved in delivering care for patients with diabetes.
Population, Sample Size, and Sampling Strategy
The sample was recruited from adult T2D patients (age ≥18 years) who had at least three follow-up appointments at Hiwot Fana Specialized Comprehensive Hospital and Jugal General Hospital for pharmacological therapy and blood glucose monitoring. However, two patients with T2D with severe illness and hearing impairment were excluded from the study as they might not accurately respond to our questions and could not give valid consent. The required sample size was estimated by Epi Info version 7 using single and double population proportion formula, where Zα/2=1.96; d=0.05; P= 61%,21 and the sample size was 402 with a 10% non-response rate. Then the sample was also estimated for the subsequent objective using a 95% confidence level, 80% power, 1.59 odds ratio, one-to-one ratio, 34.6% (unexposed), and 45.7% (exposed). The calculated sample size was 712, which was higher than the initial, but less than other objectives of our project. As a result, the largest sample size was taken for this study; that was 891. Then, based on the caseloads of each hospital, a proportional allocation was done. Accordingly, 598 T2D patients were selected from 1333 patients on follow-up at Jugal General Hospital, whereas 293 were selected from 652 T2D patients on follow-up at Hiwot Fana Specialized Comprehensive Hospital. Finally, utilizing a systematic random sampling technique, study participants were randomly selected every two cases after the first case was nominated by the lottery method.
Measurements, and Data Collection Methods
We employed three data collection strategies. Firstly, participants’ demographic information, clinical characteristics (diabetes duration, family history of diabetes, current regimen, and comorbidity),37,38 and self-care practice (physical activities, dietary plan, medication adherence, blood glucose monitoring, foot care, smoking behaviors, and alcohol use) were collected by interviewing eligible participants using pre-tested, semi-structured questionnaires developed after reviewing various literature.39 A wealth score was computed using principal component analysis (PCA) from 23 variables including household assets, farmland, and animals.40
Secondly, blood pressure (BP) measurements were carried out using a digital automated BP monitor (Model UA-767F/UA-767FAC, manufactured by A and D Company, Limited, Japan) while patients were sitting after resting for at least 15 minutes. The measurement was performed on a left arm with the elbow supported and the palm facing upward. BP measurements were taken three times in a 3-minute interval, and the mean of the second and third readings was recorded.41 BP measurement ≥140/90 mmHg indicates raised BP or hypertension.42
Anthropometric data such as height, body weight, hip circumference, and waist circumference were collected using standard procedures and calibrated instruments at the end of the interview. The height was measured using a stadiometer with the patient barefoot, hair gear removed, and the patient’s face away from the wall, looking straight ahead with their heels together and the back as straight as possible. The head, shoulders, buttocks, and heels were kept in contact with the vertical surface, and the height measurement was recorded to the nearest 0.1cm. Similarly, the body weight was measured with the patient barefooted and wearing light clothes using a Seca 803 digital body weight scale made in Japan and measuring to the nearest 0.1 kg. BMI was calculated as a patient’s weight in kilograms; divided by height in meters squared (kg/m2) after data collection. BMI was categorized into four: underweight (BMI <18.5 kg/m2), normal (BMI=18.5–24.9 kg/m2), overweight (BMI=25.0–29.9 kg/m2), and obese (BMI ≥30 kg/m2).41
Waist circumference (WC) was measured in centimeters using a fixed tension tape at the midpoint of the line between the lower margin of the last palpable (12th) rib and the top of the iliac crest (hip bone) over the light clothing without compressing the skin. The measurement was taken at the end of an expiration with the arms relaxed at the sides, and the measurement was recorded to the nearest 0.1 cm. The WC measurements were classified based on cutoffs recommended by the WHO into three health risk categories: low risk (men, WC =93.9 cm or less; women, WC =79.9 cm or less); increased risk (men, WC =94.0–101.9 cm; women, WC =80.0–87.9 cm); and high risk (men, WC =102.0 cm or more; women, WC =88.0 cm or more). Hip circumference (HC) was taken around the maximum circumference of the buttocks while the patients were standing with their feet together with weight evenly distributed over both feet and holding their arms relaxed at the sides. The hip circumference was measured using an inelastic measuring tape and recorded to the nearest 0.1 cm. Then waist-hip ratio (WHR) is calculated by dividing WC by HC in centimeters. The cutoff point used for WHR was ≤0.9 for males and ≤0.85 for females.41
Thirdly, biochemical data (fasting blood glucose, lipid profile), current regimen, diabetes-associated complications, and other co-morbidity were collected from the respective patients’ medical records using the checklist. Three most recent fasting blood glucose measurements were collected to determine glycemic levels, which were classified into two categories: optimal glycemic control (average fasting blood glucose of 80–130 mg/dL), and suboptimal glycemic control (average FPG of <70 mg/dL and >130 mg/dL).43
A chronic complication was the outcome variable of the study, and related data were collected through medical record review. All kinds of chronic complications diagnosed and recorded on the patient’s chart by a physician were collected to pre-designed checklists. The presence of at least one vascular or non-vascular complication was considered to have a chronic complication. In addition, the data on chronic complications were computed and count data were generated for further analysis. Microvascular complications include neuropathy, nephropathy, sexual dysfunction, and retinopathy. Hypertension, angina, myocardial infarction, stroke, transient ischemic attack, heart failure, foot ulcers, skin, and feet/leg problems are macrovascular complications whereas non-vascular complications include gastroparesis, hearing loss, skin problems, infections other than skin, tooth, and gum problems.10,44,45 The absence of any of these chronic complications was taken as no complication.
Statistical Analysis
The data were entered into Epidata software version 3.1. The statistical analysis was done using Stata version 14.0. Descriptive statistics were used to summarize the overall data. The data about chronic complications were computed to generate numbers of chronic complications (count data) ranging from zero to four. A Poisson regression model was fitted to identify the independent predictors of chronic complications in patients with T2D. Poisson regression model assumes that the mean and variance are the same. However, the data showed under dispersion, meaning the variance is smaller than the mean. Therefore, generalized Poisson (GP) is recommended for under-dispersed count data.46,47 Adjusted Prevalence Ratio (APR) with a 95% confidence interval was used to report association. A statistical significance was declared at a p-value ≤0.05. Hosmer and Lemeshow goodness-fit-tests indicated model fitness (P-value=0.6588). The mean-variance inflation factor was 1.17 which did not demonstrate the existence of collinearity/multicollinearity among independent variables.
Results
Socio-Demographic Characteristics
Most of the study participants, 493 (56.1%) were females. The mean age was 52.7±13.3 years. Four hundred forty-seven (50.9%) were older than 55 years while 352 (40.0%) had not received formal education. More than four-in-five of the participants, 714 (81.2%) were married, and a little above three in four, or 684 (77.8%) were urban residents. Five hundred seventy-seven (65.6%) had health insurance for their medical expense (Table 1).
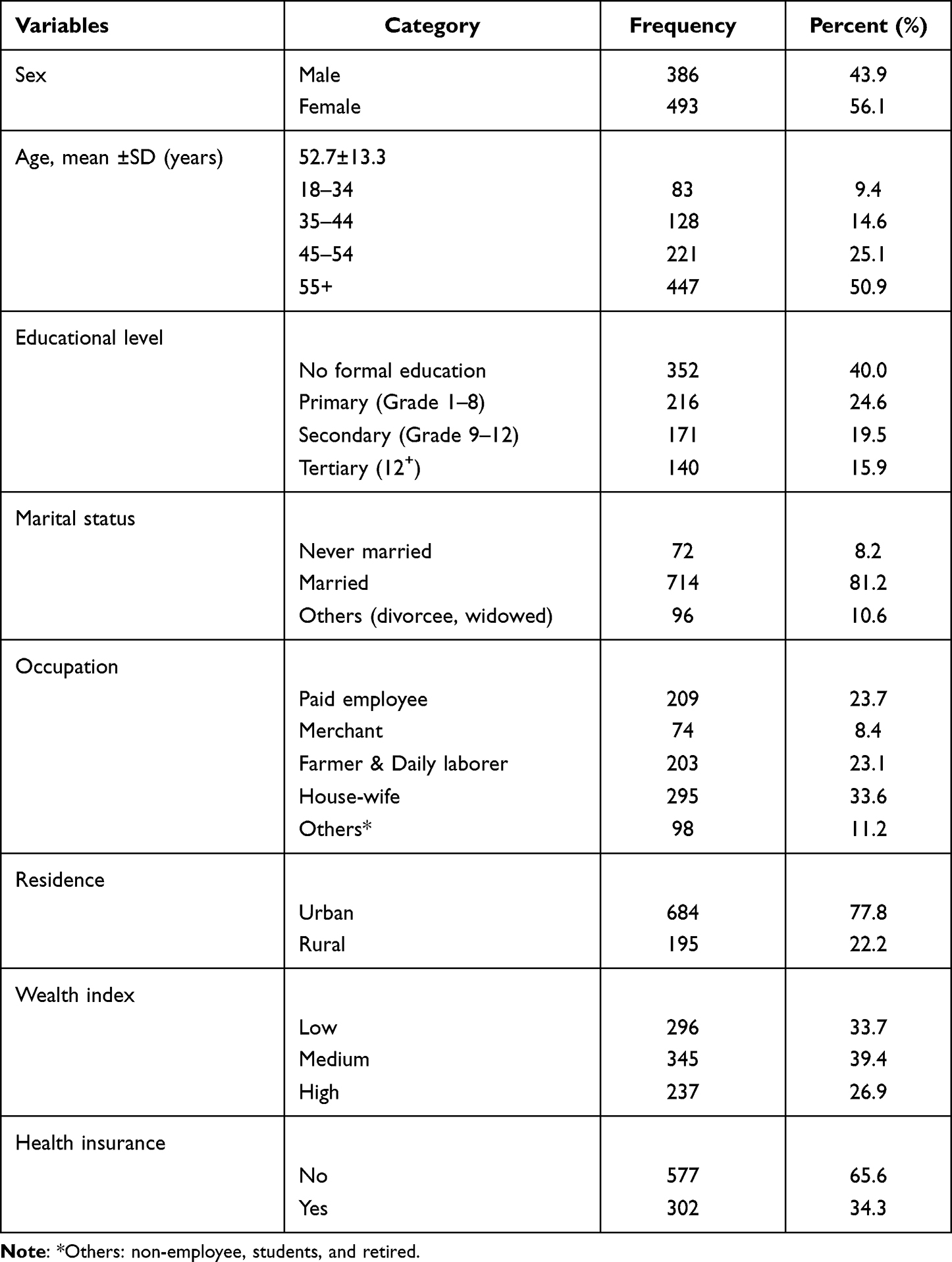 |
Table 1 Demographic Characteristics of Patients with Patients with T2D in Eastern Ethiopia, 2020/21 (n=879) |
Clinical Related Characteristics
Of all patients with T2D, six hundred-eighty (77.4%) had a diabetes duration of fewer than five years. Almost three-in-four, (74.1%) of patients with T2D had co-morbid conditions. Seven hundred thirty-nine, (84.1%) had no hypertension co-morbidity. About three-in-four (74%) of them had a suboptimal level of glycemic control. Three hundred-eighty (43.2%) patients with T2D were on combination therapy of oral glycemic agents. More than half, (55.5%) were overweight and obese, and 30.3% of them had high total cholesterol levels (≥240mg/dL). In the same manner, about one-third (35.8%) of Patients with T2D had high to very high triglyceride levels (≥200mg/dL). Five hundred-eight (57.8%) had moderate social support (Table 2).
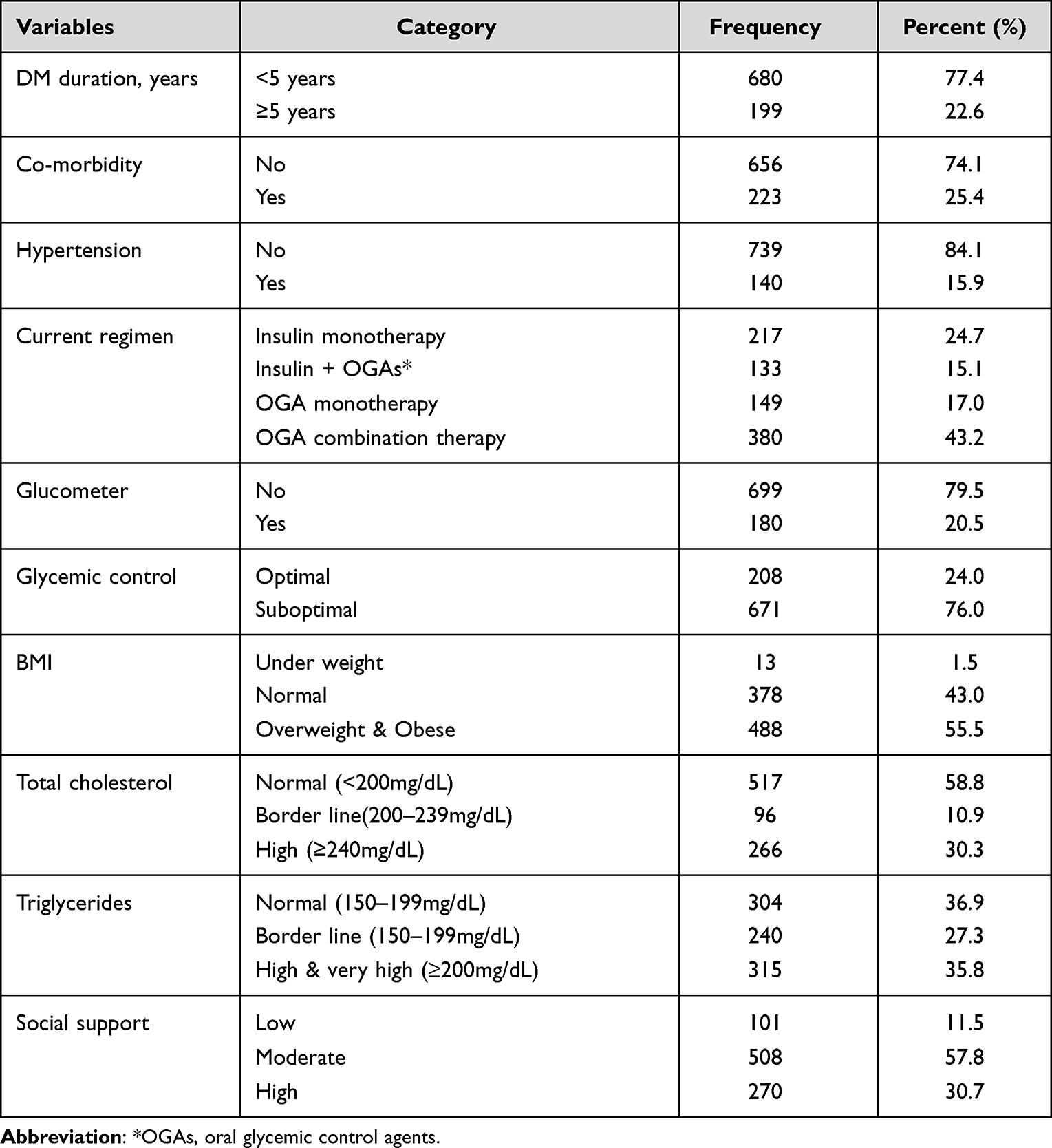 |
Table 2 Clinical Related Characteristics of Patients with T2D in Eastern Ethiopia, 2020/21 (n=879) |
Burden and Patterns of Chronic Complications
Chronic complications were found in 43% of patients with T2D (95% CI:39.65, 46.19), while 12.4% of them had more than one chronic complication (Figure 1).
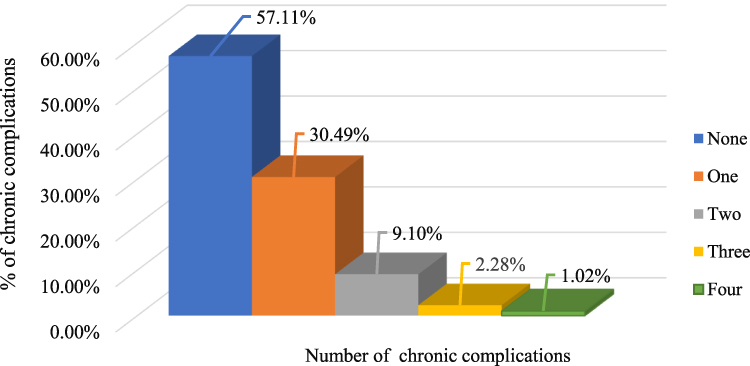 |
Figure 1 The numbers of chronic complications among patients with T2D in Eastern Ethiopia, 2020/21 (n=879). |
Among all patients with T2D, 243 (27.6%), 206 (23.5%), and 76 (8%) of them had macrovascular, microvascular, and non-vascular complications respectively. Hypertension was identified in 15.9% of T2D patients, and peripheral neuropathy was found in 6.8%. Non-vascular complications were less common, accounting for only 4.5% of all cases (Table 3).
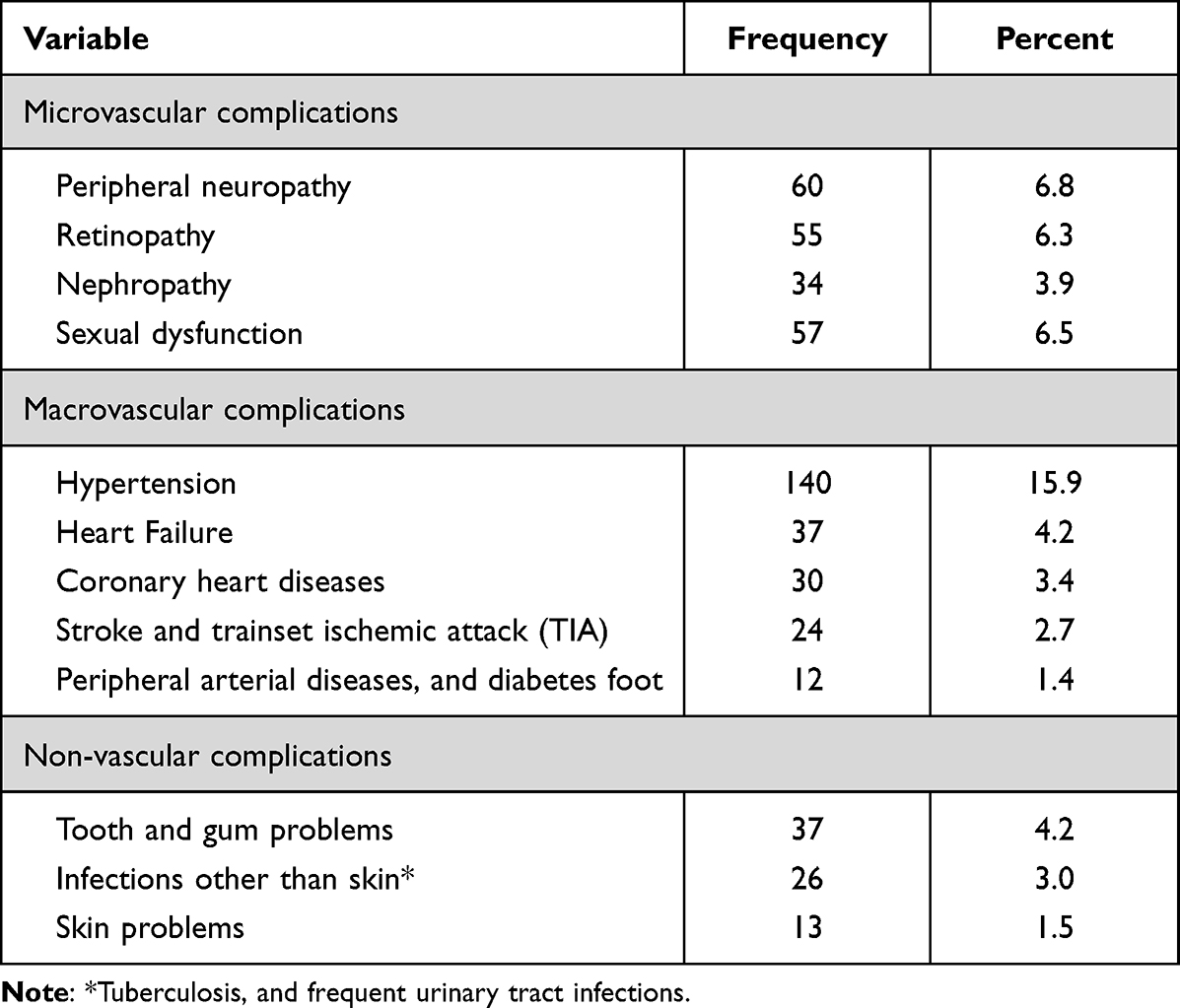 |
Table 3 The Distributions of Chronic Complications Among Patients with T2D in Eastern Ethiopia, 2020/21 (n=879) |
Factors Associated with Chronic Complications Among Patients with T2D
Bivariate Poisson regression analysis identified that being female, urban resident, having no formal education, low wealth status, disease duration ≥5 years, low social support, use of single oral glycemic agent (OGA), hypertriglyceridemia (>200mg/dL), and poor self-care practices were significantly associated with chronic complications in patients with T2D.
After adjusting for confounding variables, the prevalence of chronic complications was 1.8% higher (APR= 1.80; 95% CI:1.17, 2.76) among low wealth status patients with T2D compared to the high wealth quintile patients. Similarly, the prevalence of chronic complications was 2.64% higher (APR=2.64; 95% CI:1.54, 4.54) among urban dwellers compared to their counterparts who dwelled in rural. Those who experienced diabetes for five or more years were 1.5 times more likely to develop the number of chronic complications than those with diabetes duration <5 years (APR=1.46;95% CI:1.05, 2.01). The prevalence of chronic complications was 1.5% higher (APR=1.48;95% CI:1.06, 2.08) among T2D patients with hypertriglyceridemia (>200mg/dL) compared to patients who had a normal range of triglycerides level (150–199 mg/dL). Patients with poor self-care practices were 1.6 times (APR=1.62;95% CI: 1.18, 2.23) more likely to develop chronic complications than those with good self-care practices (Table 4).
 |
Table 4 Factors Associated with Chronic Complications Among Patients with T2D in Eastern Ethiopia, 2020/21 (n=879) |
Discussion
The study found that nearly one in every two patients with T2D experienced one or more chronic complications. A slightly more than one in ten had multiple chronic complications. Each of the vascular complications, macrovascular and microvascular accounted for one-fourth of the cases. This implies that the burden of chronic complications among the cohort of patients with T2D was considerably high, endangering their lives in various ways. Primarily chronic complications significantly increase the need for medical care, which places an undue strain on families7 and degrades patients’ productivity, quality of life, and life expectancy.48,49 Aside from that, complications further raise the expense of care, and risks of admission, and result in premature death.50
This finding was comparable with the previous studies conducted in Mettu, and Addis Ababa, Ethiopia where 38.5% and 42.5% of patients had chronic complications.11,26 The similarity could be attributed to the presence of a significant proportion of patients with similar co-morbid conditions and suboptimal glycemic control across the studies, typically associated with chronic complications in T2D patients.25,51,52 However, the result of this study was lower than other studies conducted in northern Ethiopia, and Nairobi, Kenya.12,34,53,54 This could be because more than three-quarters of the patients in the current study had shorter diabetes durations, which may minimize the likelihood of chronic complications, and other potential risk factors such as alcohol and smoking were not present. Multiple co-morbidity was also less rampant even if diabetes care quality and efforts towards early detection were inadequate.55
Hypertension and peripheral neuropathy were found to be the most common macrovascular and microvascular complications among patients with T2D, respectively. Urban residence, low wealth status, diabetes duration ≥5 years, hypertriglyceridemia (>200mg/dL), and poor diabetes self-care practices were associated with the number of chronic complications.
The current study’s finding demonstrated that low wealth status was found to be associated with chronic complications, which was consistent with a Japanese study that revealed patients with a middle and low income had microvascular complications.56 A systematic review and a study conducted in China also reported the correlation between a low level of income and vascular, and non-vascular complications in patients with T2D.27,57 In contrast, longitudinal research in the East of Scotland found no link between socioeconomic status and retinopathy.58 The measurement of economic status and study design might mediate this difference.
Urban residence was a strong predictor of chronic complications. This finding was supported by a previous study conducted in Ethiopia that showed a significant association between urban residence and chronic complications,11 whereas studies conducted in Bangladesh and China also reported increased metabolic risk factors with urban residency.31,59 The similarity might be because people who live in an urban setting have a sedentary life, unhealthy eating practice, less physical activity, and a high rate of obesity which amplify the risk of chronic complications.59,60 In the current study, there was a higher proportion of overweight, obesity, physical inactivity, and suboptimal glycemic control. However, the role of length of residence/urban exposure in increasing the risk of complications among patients with T2D needs further study.
Diabetes duration ≥ 5 years showed an association with chronic complications in this study which was in line with previous studies.61,62 It was congruent with the finding of the local studies in Debre Tabor, Nekemte Ethiopia, and Sri Lanka where longer duration of diabetes was a predictor of vascular complications.10,60,63 This might be because as a disease duration increases, there is increased exposure of blood vessels to hyperglycemia and a cluster of other risk factors which can lead to vascular complications.64
Hypertriglyceridemia (>200mg/dL) was associated with chronic complications, which was consistent with the findings of several large studies that found hypertriglyceridemia increased the risk of chronic complications (CVDs).65 Another study conducted in India reported that triglycerides were significantly associated with neuropathy and retinopathy.66 This could be due to the inability of large triglyceride-rich chylomicrons to enter the arterial wall which causes endothelial dysfunction, subclinical atherosclerosis, and increase the risk of CVDs.67 On the other hand, lower triglyceride levels were associated with better endothelial function.68
Poor diabetes self-care practices appeared to be another strong predictor of chronic complications. Evidence showed that all dimensions of proper self-care practice were positively associated with optimal glycemic control, lowering the risk of complications and improving the patients’ quality of life.69 Recent studies showed that better diabetes self-care practices improve glycemic control which in turn reduces the incidence of microvascular complications.70–74 On the other hand, a study revealed that patients with poor diabetes self-care practices had higher rates of microvascular complications such as nephropathy and neuropathy.75
Strength and Limitations of the Study
This study has several strengths. It examined the burden and predictors of chronic complications, reflecting the true problem of patients with T2D in the study area. We also used an adequate sample size with robust statistical analysis. However, the study was not without limitations. Causal inferences and temporality could not be established because of the cross-sectional nature of the study. The study employed a review of medical records to determine the burden of chronic complications rather than making a direct diagnosis. Therefore, the inadequacy of records might constrain the study.
Conclusion
Nearly one in every two patients with T2D had one or more chronic complications, influenced by urban residence, low wealth status, longer diabetes duration, hypertriglyceridemia, and poor diabetes self-care practices. The findings suggested the necessity of health policies that reduce socioeconomic disparities to lower the incidence of chronic diabetes complications. It is also crucial to devise an intervention that targets both general risk factors and the social determinants of health. Health care providers should also offer ongoing health information on potential risk factors related to chronic complications for diabetic patients. Moreover, promoting diabetes self-care behaviors demands systematic and integrated approaches.
Ethical Approval
The study protocol was approved by the Institutional Health Research and Ethical Review Committee of the College of Health and Medical Sciences, Haramaya University with Ref. No: IRERC/217/2020). The study participants were recruited voluntarily after receiving sufficient information about the study. All those volunteer participants signed written informed consent. The interview and anthropometric measurements were taken in a separate room to maintain the participants’ privacy. Personal identifiers were never used, and all information was kept confidential. We also checked that this study complies with the Helsinki Declaration.76
Acknowledgments
We thank the study participants, data collectors, supervisors, RHB, hospital administrators, and Haramaya University.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The research’s field activities were funded by Haramaya University. The grant code was HURG-2020-02-02-09. The funder had no role in the design, data collection, analysis, interpretation, writing, or publication of the manuscript.
Disclosure
The authors declare that they have no conflicts of interest.
References
1. World Health Organization. Classification of diabetes mellitus; 2019.
2. IDF. IDF diabetes atlas 10th edition; 2021.
3. Stephani V, Opoku D, Beran D. Self-management of diabetes in Sub-Saharan Africa: a systematic review. BMC Public Health. 2018;18:1148. doi:10.1186/s12889-018-6050-0
4. Letta S, Aga F, Yadeta TA, et al. Barriers to diabetes patients’ self-care practices in Eastern Ethiopia: a qualitative study from the health care providers perspective. Diabetes Metab Syndr Obes Targets Ther. 2021;14:4335–4349. doi:10.2147/DMSO.S335731
5. Giri B, Dey S, Das T, et al. Chronic hyperglycemia mediated physiological alteration and metabolic distortion leads to organ dysfunction, infection, cancer progression and other pathophysiological consequences: an update on glucose toxicity. Biomed Pharmacother. 2018;107:306–328. doi:10.1016/j.biopha.2018.07.157
6. Marcovecchio ML. Complications of Acute and Chronic Hyperglycemia. Rev Diabetes. 2017. doi:10.17925/USE.2017.13.01.17
7. IDF. Diabetes atlas 9th edition; 2019.
8. ADA. Standards of medical care in diabetes. J Clin Appl Res Educ. 2017;40:S4.
9. Godman B, Basu D, Pillay Y, et al. Review of ongoing activities and challenges to improve the care of patients with type 2 diabetes across Africa and the implications for the future. Front Pharmacol. 2020;11:108. doi:10.3389/fphar.2020.00108
10. Korsa AT, Genemo ES, Bayisa HG, et al. Diabetes mellitus complications and associated factors among adult diabetic patients in selected hospitals of West Ethiopia. Open Cardiovasc Med J. 2019;13(1):41–48. doi:10.2174/1874192401913010041
11. Sheleme T, Mamo G, Melaku T, et al. Prevalence, patterns and predictors of chronic complications of diabetes mellitus at a large referral hospital in Ethiopia: a prospective observational study. Diabetes Metab Syndr Obes. 2020;13:4909–4918. doi:10.2147/DMSO.S281992
12. Abejew AA, Belay AZ, Kerie MW. Diabetic complications among adult diabetic patients of a Tertiary Hospital in Northeast Ethiopia. Adv Public Health. 2015;2015:1–7. doi:10.1155/2015/290920
13. Pastakia SD, Nuche-Berenguer B, Pekny CR, et al. Retrospective assessment of the quality of diabetes care in a rural diabetes clinic in Western Kenya. BMC Endocr Disord. 2018;18:97. doi:10.1186/s12902-018-0324-5
14. Papatheodorou K, Banach M, Bekiari E, et al. Complications of Diabetes 2017. J Diabetes Res. 2018;2018:3086167. doi:10.1155/2018/3086167
15. Papatheodorou K, Banach M, Bekiari E, et al. Complications of Diabetes. Hindawi J Diabetes Res. 2017. doi:10.1155/2018/3086167
16. Bishua KG, Jenkins C, Yebyod HG, et al. Diabetes in Ethiopia: a systematic review of prevalence, risk factors, complications, and cost. Obes Med. 2019;15:100132.
17. Atun R, Davies JI, Gale EAM, et al. Diabetes in sub-Saharan Africa: from clinical care to health policy. Lancet Diabetes Endocrinol. 2017;5:622–667. doi:10.1016/s2213-8587(17)30181-x
18. Pastakia SD, Pekny CR, Manyara SM, et al. Diabetes in sub-Saharan Africa – from policy to practice to progress: targeting the existing gaps for future care for diabetes. Diabetes Metab Syndr Obes. 2017;10:247–263. doi:10.2147/DMSO.S126314
19. Jing X, Chen J, Dong Y, et al. Related factors of quality of life of type 2 diabetes patients: a systematic review and meta-analysis. Health Qual Life Outcomes. 2018;16. doi:10.1186/s12955-018-1021-9
20. Trikkalinou A, Papazafiropoulou AK, Melidonis A. Type 2 diabetes and quality of life. World J Diabetes. 2017;8:120–129. doi:10.4239/wjd.v8.i4.120
21. Gebre BB, Assefa ZM. The magnitude and associated factors of diabetic complication among diabetic patients attending Gurage zone hospitals, South West Ethiopia. BMC Res Notes. 2019;12:780. doi:10.1186/s13104-019-4808-9
22. Abebe N, Kebede T, Addise D. Diabetes in Ethiopia 2000–2016 –prevalence and related acute and chronic complications; a systematic review. Afr J Diabetes Med. 2017;25:7–12.
23. FMOH. National strategic action plan (NSAP) for prevention & control; 2014.
24. EPHI, FMoH, and WHO. Steps survey on risk factors for non-communicable diseases and prevalence of selected NCDs, Ethiopia summary report; 2016.
25. Fasil A, Biadgo B, Abebe M. Glycemic control and diabetes complications among diabetes mellitus patients attending at University of Gondar Hospital, Northwest Ethiopia. Diabetes Metab Syndr Obes. 2019;12:75–83. doi:10.2147/DMSO.S185614
26. Negash Z, Yismaw M. Management practice and contributing risk factors for chronic complications among type 2 diabetes mellitus adult patients in follow-up at a tertiary care teaching hospital. Diabetes Metab Syndr Obes. 2020;13:3969–3976. doi:10.2147/DMSO.S275677
27. Tao X, Li J, Zhu X, et al. Association between socioeconomic status and metabolic control and diabetes complications: a cross-sectional nationwide study in Chinese adults with type 2 diabetes mellitus. Cardiovasc Diabetol. 2016;15:61. doi:10.1186/s12933-016-0376-7
28. Bonora E, Trombetta M, Dauriz M, et al. Chronic complications in patients with newly diagnosed type 2 diabetes: prevalence and related metabolic and clinical features: the Verona Newly Diagnosed Type 2 Diabetes Study (VNDS) 9. BMJ Open Diabetes Res Care. 2020;8(1):e001549. doi:10.1136/bmjdrc-2020-001549
29. Bui HDT, Jing X, Lu R, et al. Prevalence of and factors related to microvascular complications in patients with type 2 diabetes mellitus in Tianjin, China: a cross-sectional study. Ann Transl Med. 2019;7:325. doi:10.21037/atm.2019.06.08
30. Iradukunda A, Kembabazi S, Ssewante N, et al. Diabetic complications and associated factors: a 5-year Facility-Based Retrospective Study at a Tertiary Hospital in Rwanda. Diabetes Metab Syndr Obes. 2021;14:4801–4810. doi:10.2147/DMSO.S343974
31. Afroz A, Zhang W, Wei Loh AJ, et al. Macro- and micro-vascular complications and their determinants among people with type 2 diabetes in Bangladesh. Diabetes Metab Syndr. 2019;13(5):2939–2946. doi:10.1016/j.dsx.2019.07.046
32. Asefa A, Nigussie T, Henok A, et al. Prevalence of sexual dysfunction and related factors among diabetes mellitus patients in Southwest Ethiopia. BMC Endocr Disord. 2019;19(1):141. doi:10.1186/s12902-019-0473-1
33. Azeze TK, Sisay MM, Zeleke EG. Incidence of diabetes retinopathy and determinants of time to diabetes retinopathy among diabetes patients at Tikur Anbessa Hospital, Ethiopia: a retrospective follow up study. BMC Res Notes. 2018;11:542. doi:10.1186/s13104-018-3660-7
34. Reba Lebeta K. Prevalence of diabetic complications and its associated factors among diabetes mellitus patients attending diabetes mellitus clinics; institution based cross-sectional study. Am J Health Res. 2017;5:38. doi:10.11648/j.ajhr.20170502.13
35. Tadesse DB, Gebrewahd GT, Hailay A, et al. Diabetic Peripheral Neuropathy in Ethiopia: a Systematic Review and Meta-Analysis. J Diabetes Res. 2021;2021:5304124. doi:10.1155/2021/5304124
36. Regassa LD, Tola A, Ayele Y. Prevalence of cardiovascular disease and associated factors among type 2 diabetes patients in Selected Hospitals of Harari Region, Eastern Ethiopia. Front Public Health. 2020;8:532719. doi:10.3389/fpubh.2020.532719
37. Abate TW, Tareke M, Tirfie M. Self-care practices and associated factors among diabetes patients attending the outpatient department in Bahir Dar, Northwest Ethiopia. BMC Res Notes. 2018;11. doi:10.1186/s13104-018-3874-8
38. Ayele BH, Mengesha MM, Tesfa T. Predictors of self-care activities of outpatient diabetic residents in Harar and Dire Dawa: a hospital-based cross-sectional study. SAGE Open Med. 2019;7:2050312119865646. doi:10.1177/2050312119865646
39. Toobert DJ, Hampson SE, Glasgow RE. The summary of diabetes self-care activities measure: results from 7 studies and a revised scale. Diabetes Care. 2000;23:943–950. doi:10.2337/diacare.23.7.943
40. EDHS. Ethiopian demographic and health survey; 2016.
41. World Health Oorganization. The WHO STEPwise approach to noncommunicable disease risk factor surveillance manual; 2020.
42. Unger T, Borghi C, Charchar F, et al. International Society of Hypertension: global hypertension practice guidelines. Hypertension. 2020;75(6):1334–1357.
43. ADA. Standards of medical care in diabetes. Diabetes Care. 44;2021. doi:10.2337/dc21-S002
44. Ahmed SI. Diabetes an Old Disease, A New Insight. Springer Science & Business Media; 2013.
45. Liu Z, Fu C, Wang W, et al. Prevalence of chronic complications of type 2 diabetes mellitus in outpatients - a cross-sectional hospital based survey in urban China. Health Qual Life Outcomes. 2010;8(1):62. doi:10.1186/1477-7525-8-62
46. Allo CBG, Otok BW. Estimation parameter of generalized poisson regression model using generalized method of moments and its application. IOP Conf Series. 2019;546. doi:10.1088/1757-899X/546/5/052050
47. Harris T, Yang Z, Hardin JW. Modeling underdispersed count data with generalized Poisson regression. Stata J. 2012;12:736–747. doi:10.1177/1536867X1201200412
48. Afroz A, Hird TR, Zomer E, et al. The impact of diabetes on the productivity and economy of Bangladesh. BMJ Global Health. 2020;5(6):e002420. doi:10.1136/bmjgh-2020-002420
49. Tönnies T, Hoyer A, Brinks R. Productivity-adjusted life years lost due to type 2 diabetes in Germany in 2020 and 2040. Diabetologia. 2021;64(6):1288–1297. doi:10.1007/s00125-021-05409-3
50. IDF. IDF clinical practice recommendations for managing type 2 diabetes in primary care. Diabetes Res Clin Pract. 2017;132:169–170.
51. Abdissa D, Hirpa D. Poor glycemic control and its associated factors among diabetes patients attending public hospitals in West Shewa Zone, Oromia, Ethiopia: an Institutional based cross-sectional study. Metab Open. 2022;13:100154. doi:10.1016/j.metop.2021.100154
52. Oluma A, Abadiga M, Mosisa G, et al. Magnitude and predictors of poor glycemic control among patients with diabetes attending public hospitals of Western Ethiopia. PLoS One. 2021;16(2):e0247634. doi:10.1371/journal.pone.0247634
53. Evans U, Joseph M, Daniel N. Factors associated with complications among type 2 diabetes patients visiting regional referral hospital in Nairobi, Kenya. Pharmaceutical J Kenya. 2020;24:1–11.
54. Astatkie BG, Ayele WM, Dawed YA. Chronic diabetic complications and associated factors among people with type-2 diabetes mellitus in Debretabor Hospital, Northwest Ethiopia, 2018. J Diabetes Metab. 2020;11:845. doi:10.35248/2155-6156.20.11.845
55. Gudina EK, Amade ST, Tesfamichael FA, et al. Assessment of quality of care given to diabetic patients at Jimma University Specialized Hospital diabetes follow-up clinic, Jimma, Ethiopia. BMC Endocr Disord. 2011;11(1):19. doi:10.1186/1472-6823-11-19
56. Funakoshi M, Azami Y, Matsumoto H, et al. Socioeconomic status and type 2 diabetes complications among young adult patients in Japan. PLoS One. 2017;12(4):e0176087. doi:10.1371/journal.pone.0176087
57. Tatulashvilia S, Fagherazzib G, Dowb C, et al. Socioeconomic inequalities and type 2 diabetes complications: a systematic review. Diabetes Metab. 2020;46(2):89–99. doi:10.1016/j.diabet.2019.11.001
58. Low L, Law JP, Hodson J, et al. Impact of socioeconomic deprivation on the development of diabetic retinopathy: a population-based, cross-sectional and longitudinal study over 12 years. BMJ. 2015;351. doi:10.1136/bmjopen-2014-007290
59. Du G-I, Su Y-X, Yao H, et al. Metabolic risk factors of type 2 diabetes mellitus and correlated glycemic control/ complications: a cross-sectional study between Rural and Urban Uygur Residents in Xinjiang Uygur Autonomous Region. PLoS One. 2016;11(9):e0162611. doi:10.1371/journal.pone.0162611
60. Arambewela MH, Somasundaram NP, Jayasekara H, et al. Prevalence of chronic complications, their risk factors, and the cardiovascular risk factors among patients with type 2 diabetes attending the diabetic clinic at a Tertiary Care Hospital in Sri Lanka. J Diabetes Res. 2018;2018:4504287. doi:10.1155/2018/4504287
61. Islam SM, Alam DS, Wahiduzzaman M, et al. Clinical characteristics and complications of patients with type 2 diabetes attending an urban hospital in Bangladesh. Diabetes Metab Syndr. 2015;9:7–13. doi:10.1016/j.dsx.2014.09.014
62. Ramanathan AS. Correlation of duration, hypertension and glycemic control with microvascular complications of diabetes mellitus at a tertiary care hospital. Integr Mol Med. 2017;4. doi:10.15761/imm.1000272
63. Astatkie BG, Ayele WM, Dawed YA. Chronic diabetic complications and associated factors among people with type-2 diabetes mellitus in Debretabor Hospital, Northwest Ethiopia. J Diabetes Metab. 2018;10. doi:10.35248/2155-6156.20.11.845
64. Paneni F, Beckman JA, Creager MA, et al. Diabetes and vascular disease: pathophysiology, clinical consequences, and medical therapy: part I. Eur Heart J. 2013;34(31):2436–2443. doi:10.1093/eurheartj/eht149
65. Reiner Ž. Hypertriglyceridaemia and risk of coronary artery disease. Nat Rev Cardiol. 2017;14(7):401–411. doi:10.1038/nrcardio.2017.31
66. Bansal D, Gudala K, Esam HP, et al. Microvascular complications and their associated risk factors in newly diagnosed type 2 diabetes mellitus patients. Int J Chronic Dis. 2014;2014. doi:10.1155/2014/201423
67. Kajikawa M, Maruhashi T, Matsumoto T, et al. Relationship between serum triglyceride levels and endothelial function in a large community-based study. Atherosclerosis. 2016;249:70–75. doi:10.1016/j.atherosclerosis.2016.03.035
68. Takaeko Y, Maruhashi T, Kajikawa M, et al. Lower triglyceride levels are associated with better endothelial function. J Clin Lipidol. 2021;15(1):1–12. doi:10.1016/j.jacl.2021.01.003
69. Shrivastava SR, Shrivastava PS, Ramasamy J. Role of self-care in management of diabetes mellitus. J Diabetes Metab Disord. 2013;12. doi:10.1186/2251-6581-12-14
70. Nathan DM, Group DER. The diabetes control and complications trial/epidemiology of diabetes interventions and complications study at 30 years: overview. Diabetes Care. 2014;37:9–16. doi:10.2337/dc13-2112
71. Fullerton B, Jeitler K, Seitz M, et al. Intensive glucose control versus conventional glucose control for type 1 diabetes mellitus. Cochrane Database Syst Rev. 2014:CD009122. doi:10.1002/14651858.CD009122.pub2
72. Zhao FF, Suhonen R, Katajisto J, et al. Association between diabetes-related self-care activities and positive health: a cross-sectional study. BMJ Open. 2019;9:e023878. doi:10.1136/BMJopen-2018-023878
73. Bukhsh A, Khan TM, Sarfraz Nawaz M, et al. Association of diabetes knowledge with glycemic control and self-care practices among Pakistani people with type 2 diabetes mellitus. Diabetes Metab Syndr Obes. 2019;12:1409–1417. doi:10.2147/DMSO.S209711
74. Almomani MH, Al-Tawalbeh S. Glycemic control and its relationship with diabetes self-care behaviors among patients with type 2 diabetes in Northern Jordan: a cross-sectional study. Patient Prefer Adherence. 2022;16:449–465. doi:10.2147/PPA.S343214
75. Mehravar F, Mansournia MA, Mansournia N, et al. Associations between diabetes self-management and microvascular complications in patients with type 2 diabetes. Epidemiol Health. 2015;38. doi:10.4178/epih/e2016004
76. Warraich HJ; World Medical Association. World medical association declaration of Helsinki ethical principles for medical research involving human subjects. JAMA. 2013;310:373. doi:10.1001/jama.2013.66054
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Red Blood Cell Parameters and Their Correlation with Glycemic Control Among Type 2 Diabetic Adult Patients in Eastern Ethiopia: A Comparative Cross-Sectional Study
Arkew M, Asmerom H, Tesfa T, Tsegaye S, Gemechu K, Bete T, Haile K
Diabetes, Metabolic Syndrome and Obesity 2022, 15:3499-3507
Published Date: 9 November 2022
Real-World Effectiveness and Safety of Hydrogen Inhalation in Chinese Patients with Type 2 Diabetes: A Single-Arm, Retrospective Study
Ji H, Zhao Z, Liu Z, Sun R, Li Y, Ding X, Ni T
Diabetes, Metabolic Syndrome and Obesity 2023, 16:2039-2050
Published Date: 5 July 2023
Determinants of Glycemic Control in Thai Adults with Insulin-Treated Type 2 Diabetes Mellitus: A Cross-Sectional Study
Riangkam C, Sanguanthammarong S, Lertwattanarak R
Patient Preference and Adherence 2025, 19:1909-1922
Published Date: 5 July 2025