Back to Journals » Nature and Science of Sleep » Volume 18

Polysomnographic Characteristics and Sleep Disorders in Pediatric Moyamoya Arteriopathy
Authors Sirianansopa K ![]() , Amin R
, Amin R ![]() , Chiang J
, Chiang J ![]()
Received 13 January 2026
Accepted for publication 28 April 2026
Published 15 May 2026 Volume 2026:18 596046
DOI https://doi.org/10.2147/NSS.S596046
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Kantisa Sirianansopa,1,2 Reshma Amin,2– 4 Jackie Chiang2,3
1Division of Pulmonary Medicine, Department of Pediatrics, Faculty of Medicine, Prince of Songkla University, Songkhla, Thailand; 2Division of Respiratory Medicine, The Hospital for Sick Children, Toronto, Ontario, Canada; 3Department of Pediatrics, University of Toronto, Toronto, Ontario, Canada; 4Child Health and Evaluative Science, SickKids Research Institute, Toronto, Ontario, Canada
Correspondence: Reshma Amin, Department of Pediatrics, University of Toronto, Toronto, Ontario, Canada, M5G 1X8, Tel +1 416-813-7654 ext. 415683, Email [email protected]
Purpose: This study aimed to describe the polysomnographic characteristics and sleep-related symptoms in pediatric patients with Moyamoya arteriopathy (MMA) referred for sleep evaluation.
Patients and Methods: We conducted a retrospective case series of pediatric patients with MMA who were referred to the sleep clinic at The Hospital for Sick Children, Toronto, Canada, and underwent level 1 polysomnography (PSG) between 2014 and 2024. Clinical, demographic, genetic, and sleep-related data, including PSG and multiple sleep latency test (MSLT) findings were reviewed.
Results: Eleven pediatric patients were included, with a median (IQR) age of 15 (13, 17) years. Sleep fragmentation was commonly observed on PSG (n=10, 90.9%), while no patients demonstrated clinically significant sleep-disordered breathing. A trend toward shorter REM latency was noted compared with age-matched normative values. Daytime fatigue was the most frequently reported symptom (n=6, 54.5%). Two patients underwent MSLT due to persistent hypersomnolence; one met diagnostic criteria for narcolepsy.
Conclusion: In this retrospective case series, sleep fragmentation and a trend toward shorter REM latency were commonly observed in pediatric patients with MMA. However, given the small sample size and absence of pre-revascularization baseline data, these findings should be interpreted with caution. These results are descriptive and hypothesis-generating, and further prospective studies are needed to better understand sleep disturbances in this population.
Keywords: moyamoya arteriopathy, sleep fragmentation, REM latency, hypersomnolence, polysomnography, pediatric
Introduction
Moyamoya arteriopathy (MMA) is a progressive cerebrovascular disorder characterized by stenosis of the intracranial carotid arteries and the development of compensatory collateral vessels in response to chronic cerebral ischemia. Although these collateral vessels initially serve a compensatory function, they are often fragile and prone to rupture, increasing the risk of hemorrhagic events.1 The prevalence of MMA is highest in Japan, with an annual incidence of approximately 0.94 cases per 100,000 individuals,2 whereas it remains rare in Western populations, with an estimated incidence of less than 0.1 cases per 100,000 persons per year.3 MMA may present as an isolated condition, referred to Moyamoya disease (MMD), or as Moyamoya syndrome (MMS), in which similar angiographic findings occur in association with underlying conditions such as sickle cell disease, Down syndrome, neurofibromatosis type 1, or autoimmune disorders.4 Clinically, MMA is associated with recurrent ischemic or hemorrhagic strokes, cognitive impairment, and other neurovascular complications. While its neurological and cognitive consequences are well established,5,6 its impact on sleep remains poorly understood.
Cerebral hypoperfusion may influence neural pathways involved in sleep regulation. Evidence from other cerebrovascular conditions suggests that impaired cerebral blood flow alters neurotransmitter systems and contributes to sleep disturbances.7 The hypothalamus plays a central role in sleep-wake regulation, and ischemic or hypoxic injury in this region may disrupt neuronal networks responsible for maintaining sleep stability.8 In particular, the orexin system, which regulates wakefulness and REM sleep transitions, has been shown to be vulnerable to ischemic injury, and dysfunction in this system has been associated with excessive daytime sleepiness and altered REM sleep architecture.9 However, the relevance of these mechanisms in pediatric MMA remains uncertain and direct evidence in this population is lacking.
Children with MMA typically present with neurological symptoms related to cerebral ischemia, including hemiparesis, paresthesia, aphasia, visual disturbances, and cognitive impairments, depending on the vascular territories involved.10 Headache is also frequently reported and is thought to result from hypoperfusion-related activation of pain-sensitive intracranial and extracranial structures.11 In addition to these neurological manifestations, sleep related symptoms including excessive daytime sleepiness, sleep paralysis, and sleep hallucinations have been described in some patients.12 Despite these observations, the relationship between MMA and sleep disturbances remains incompletely characterized.
The existing literature on sleep disturbances in pediatric MMA is limited, with few studies systematically evaluating sleep using objective measures such as polysomnography (PSG).13,14 Given this gap, the present study aimed to describe the polysomnographic characteristics and sleep-related symptoms in a retrospective case series of pediatric patients with MMA referred for sleep evaluation. We also explored associated clinical features, including daytime sleepiness and multiple sleep latency test (MSLT) findings, to provide an initial descriptive characterization of sleep disturbances in this population.
Materials and Methods
Study Design and Population
This retrospective case series reviewed pediatric patients diagnosed with MMA who were referred to the sleep clinic at The Hospital for Sick Children, Toronto, Canada, for evaluation of sleep-related symptoms and underwent level 1 PSG between 2014 and 2024. All included patients had previously undergone revascularization surgery as part of their clinical management.
Demographic and baseline clinical data were obtained from electronic medical records. Inclusion criteria were: (1) confirmed diagnosis of MMA, (2) age ≤18 years at the time of PSG, and (3) completion of PSG and, where applicable, MSLT. Patients with incomplete PSG data or significant comorbid conditions unrelated to MMA that could independently affect sleep were excluded.
Data Collection
Demographic variables included age, sex, and body mass index (BMI). Clinical data were extracted from electronic medical records and included neurological and sleep-related characteristics. Neurological variables included age at onset of neurological symptoms, type of neurological presentation (eg, stroke, headache, seizure), cerebrovascular involvement (anterior, posterior, or both circulations), RNF213 mutation status, and underlying diagnosis classified as MMD or MMS based on associated conditions.
Sleep History and Sleep-Related Symptoms
Sleep history and sleep-related symptoms were extracted from the medical records at the time of referral to the sleep clinic. These variables were based on clinician documented history and primary presenting complaints. The main presenting sleep complaints were categorized as daytime fatigue, daytime sleepiness, sleep-related obstructive symptoms (eg, snoring, gasping, or witnessed apneas), and insomnia. Sleep pattern variables included reported total sleep time, frequency of nocturnal awakenings (≥1 per night), and the presence of daytime napping. Situations associated with daytime sleepiness were recorded, including sleepiness occurring in a car, while reading, at school, or while watching television. Daytime sleepiness was further assessed using the Epworth Sleepiness Scale (ESS), a validated questionnaire for measuring subjective sleepiness,15 administered in accordance with its licensing requirements. Functional and behavioral consequences potentially related to sleep disturbances, including hyperactivity, concentration difficulties, irritability, and symptoms of anxiety or depression, were also recorded when documented.
Polysomnography (PSG)
All PSG studies were conducted in a sleep laboratory using level 1 diagnostic monitoring in accordance with American Academy of Sleep Medicine (AASM) guidelines.16 Recorded parameters included electroencephalography (EEG), electrooculography (EOG), electromyography (EMG), airflow, thoracoabdominal movements, pulse oximetry, and carbon dioxide monitoring using both end-tidal (EtCO2) and transcutaneous (TcCO2) methods. PSG studies were scored by trained sleep technologists and interpreted by board-certified sleep physicians. Sleep architecture parameters included total sleep time, sleep efficiency, sleep onset latency, and REM latency.
Sleep-disordered breathing was evaluated according to AASM criteria.17 In pediatric patients (< 13 years), obstructive sleep apnea severity was primarily classified based on the obstructive apnea-hypopnea index (OAHI) as follows: <2 events/hour (normal), 2–5 (mild), 5–10 (moderate), and >10 (severe). In older adolescents (≥ 13 years), adult AASM criteria were also considered for contextual interpretation, where an apnea-hypopnea index (AHI) <5 events/hour is generally considered within normal limits, 5–15 mild, 15–30 moderate, and >30 severe. Additional parameters included central apnea-hypopnea index (CAHI), oxygen desaturation index (ODI), oxygen saturation (SpO2), and periodic limb movement index (PLMI) were also assessed.
Arousal events were categorized as spontaneous, respiratory-related, and limb movement-related according to PSG scoring. Sleep fragmentation was defined based on the overall clinical interpretation documented in the sleep physician’s report, taking into account sleep stage transitions, wake after sleep onset (WASO), sleep efficiency, and supported by spontaneous arousal index metrics in the context of existing pediatric normative data. Given the variability in reported normal values, which range approximately from 5 ± 2 to 10.8 ± 4.2 events per hour in children,18 arousal indices were interpreted in conjunction with overall PSG findings to inform the assessment of sleep fragmentation.
Multiple Sleep Latency Testing (MSLT)
MSLT was performed following overnight PSG in patients with clinically significant daytime sleepiness, in accordance with pediatric protocols recommended by AASM.19 The test consisted of five scheduled nap opportunities at two-hour intervals. Mean sleep latency and the presence of sleep-onset rapid eye movement periods (SOREMPs) were recorded. MSLT results were interpreted according to the International Classification of Sleep Disorders, Third Edition (ICSD-3).20 Narcolepsy was defined as a mean sleep latency ≤8 minutes with the presence of ≥2 SOREMPs.
Statistical Analysis
Descriptive statistics were used to summarize demographic, clinical characteristics, PSG, and MSLT variables. Continuous variables are presented as medians with interquartile ranges (IQR) or means with standard deviations (SD), depending on normality distribution. Categorical variables are reported as frequencies and percentages. Comparisons with published aged-matched normative data (eg, REM latency) were performed descriptively. All statistical analyses were conducted using R software version 4.4.2.
Ethical Considerations
This study was approved by the institutional research ethics board at the Hospital for Sick Children (REB No. 3414–33,601). This research was performed in accordance with the ethical standards of the Declaration of Helsinki. The requirement for informed consent was waived due to the retrospective design, and all data were de-identified prior to analysis.
Results
A total of 11 pediatric patients with MMA who underwent level 1 PSG were included in this study. Eight patients (72.7%) were diagnosed with MMD, while three (27.3%) had MMS associated with sickle cell disease (n=1), neurofibromatosis type 1 (n=1), and beta-thalassemia (n=1). Approximately half of the cohort were female (n=6, 54.5%). The mean (SD) age at onset of neurological symptoms was 5.1 (3.4) years. The most common neurological presentation was transient ischemic attacks (TIA), followed by chronic headache, ischemic stroke, and seizures. Most patients demonstrated involvement of both anterior and posterior circulations, and six patients (54.5%) carried the RNF213 mutation. All patients underwent pial synangiosis as a revascularization procedure. Baseline demographic and clinical characteristics are summarized in Table 1.
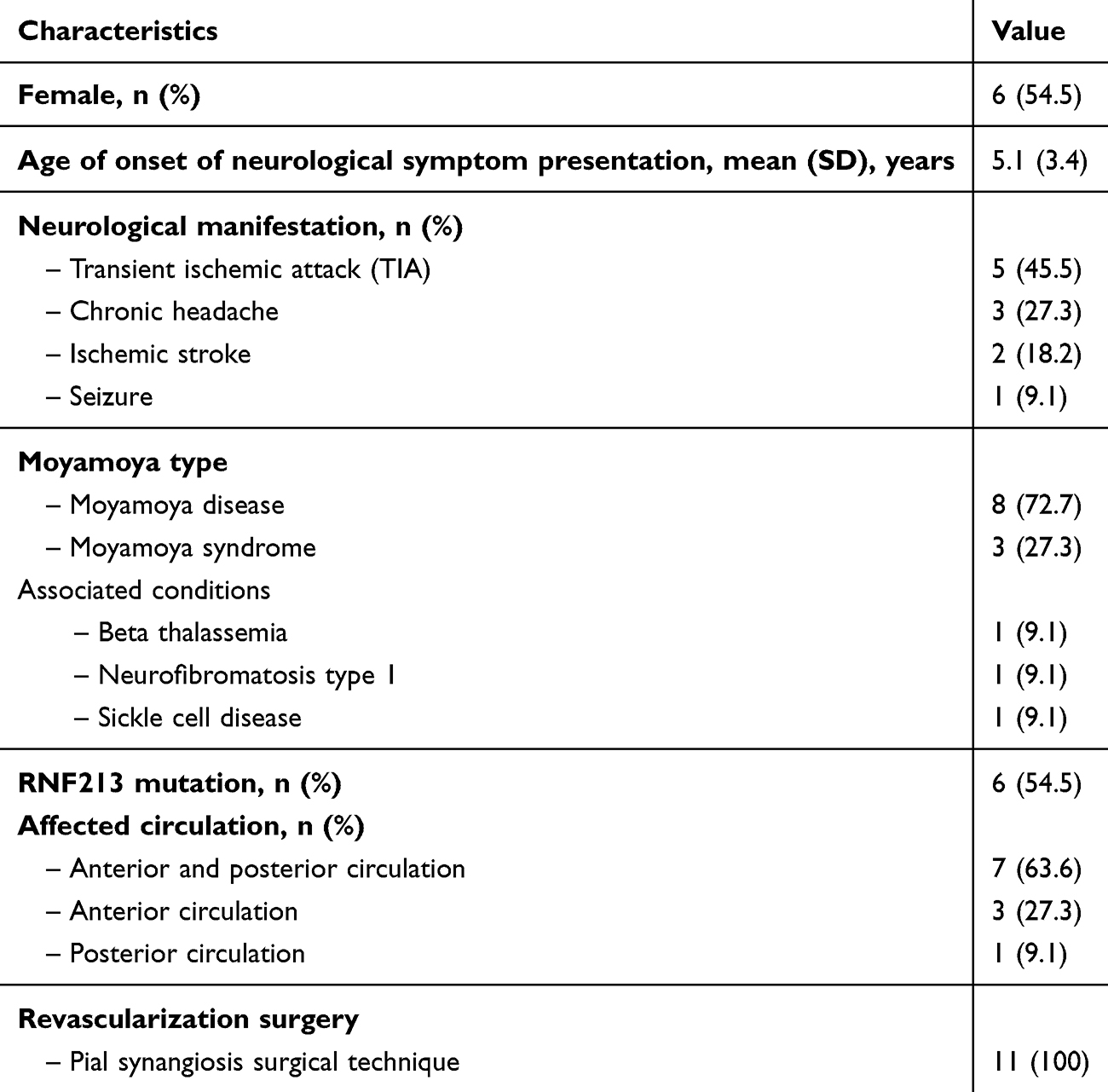 |
Table 1 Baseline Characteristics and Demographic Data of Pediatric Moyamoya Patients (n=11) |
Clinical sleep history and sleep-related symptoms are shown in Table 2. Daytime fatigue was the most frequently reported complaint, followed by daytime sleepiness and sleep-related obstructive symptoms, while insomnia was less commonly reported. More than half of patients reported at least one nocturnal awakening per night, and a subset reported daytime napping. The reported total sleep time overnight was 8.9 (1.8) hours per day. Situations most commonly associated with daytime sleepiness included falling asleep in a car, followed by reading and being at school. The median (IQR) ESS score was 6 (3, 6.5). A small proportion of patients demonstrated behavioral or cognitive consequences, including hyperactivity, concentration difficulties, and irritability.
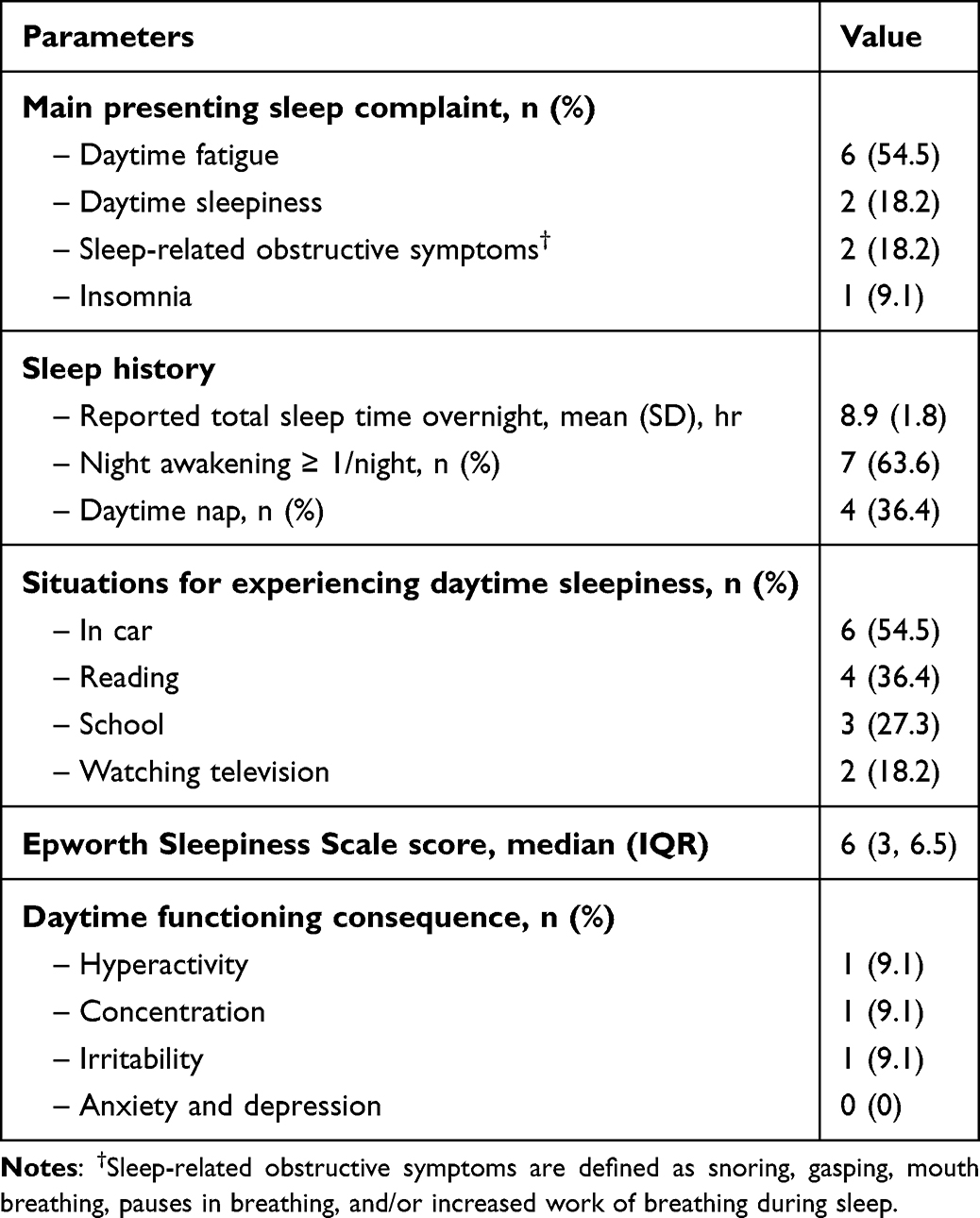 |
Table 2 Sleep History and Sleep-Related Symptoms in Pediatric Moyamoya Patients (n=11) |
The objective sleep parameters obtained from polysomnography are presented in Table 3. All patients underwent PSG following revascularization surgery. The median (IQR) age at the time of PSG assessment was 15 (13, 17) years, with a median (IQR) BMI of 20.7 (18.9, 23.3) kg/m2. Sleep fragmentation, based on sleep physician interpretation, was observed in the majority of patients (n=10, 90.9%). The median (IQR) total sleep time derived from PSG was 403 (376, 438) minutes, with a median (IQR) sleep efficiency of 87.1% (86.4, 93.8). The median (IQR) sleep onset latency was 11.5 (6.5, 23) minutes and the mean (SD) REM latency was 87 (43.5) minutes. The median (IQR) OAHI was 0.7 (0.1, 2.4) events/hr, and the CAHI was 0.3 (0.2, 0.9) events/hr. Oxygen saturation parameters were generally within expected ranges at the group level. However, isolated nocturnal desaturations (nadir SpO2 <90%) were observed in a subset of patients, including values of 87% and 88% in two cases (Supplementary Table S1). These findings were reviewed clinically and were not associated with evidence of sleep-disordered breathing based on AHI/OAHI criteria or clinical assessment. The mean (SD) spontaneous arousal index was 12 (3.5) events/hour. Individual PSG characteristics are provided in Supplementary Table S1.
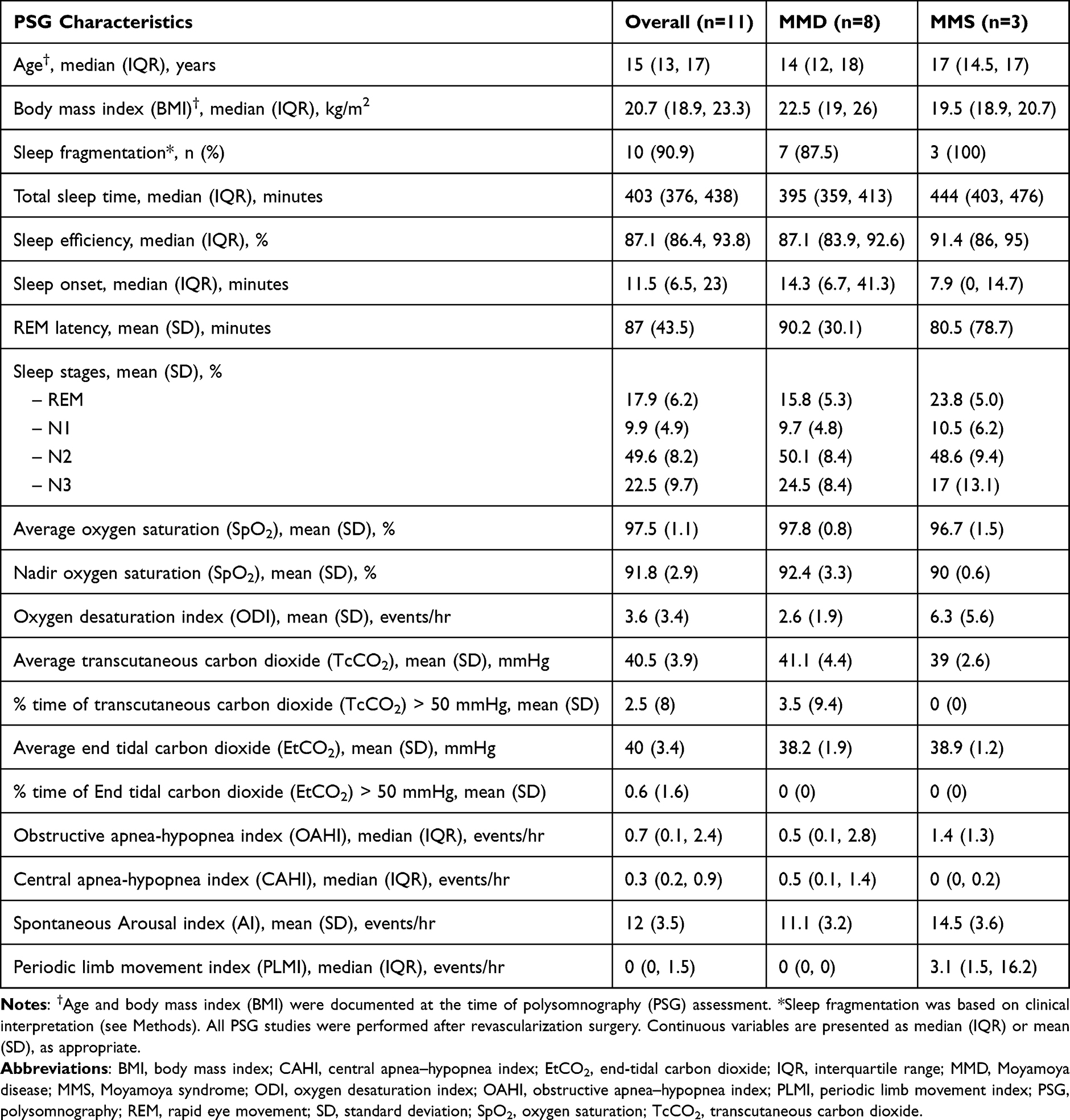 |
Table 3 Polysomnographic Characteristics of Pediatric Patients with Moyamoya Arteriopathy After Revascularization Surgery, Stratified by Moyamoya Disease and Moyamoya Syndrome |
Two patients underwent MSLT due to clinically significant daytime sleepiness (ESS >10). One patient, with underlying sickle cell disease, met diagnostic criteria for narcolepsy and had both pre- and post- revascularization PSG and MSLT data available (Table 4). The ESS score decreased from 21 to 19 following surgery. MSLT findings remained consistent with narcolepsy. The second patient, with neurofibromatosis type 1, underwent MSLT due to persistent daytime sleepiness (ESS = 12) despite the absence of sleep-disordered breathing on PSG, but did not meet diagnostic criteria for narcolepsy.
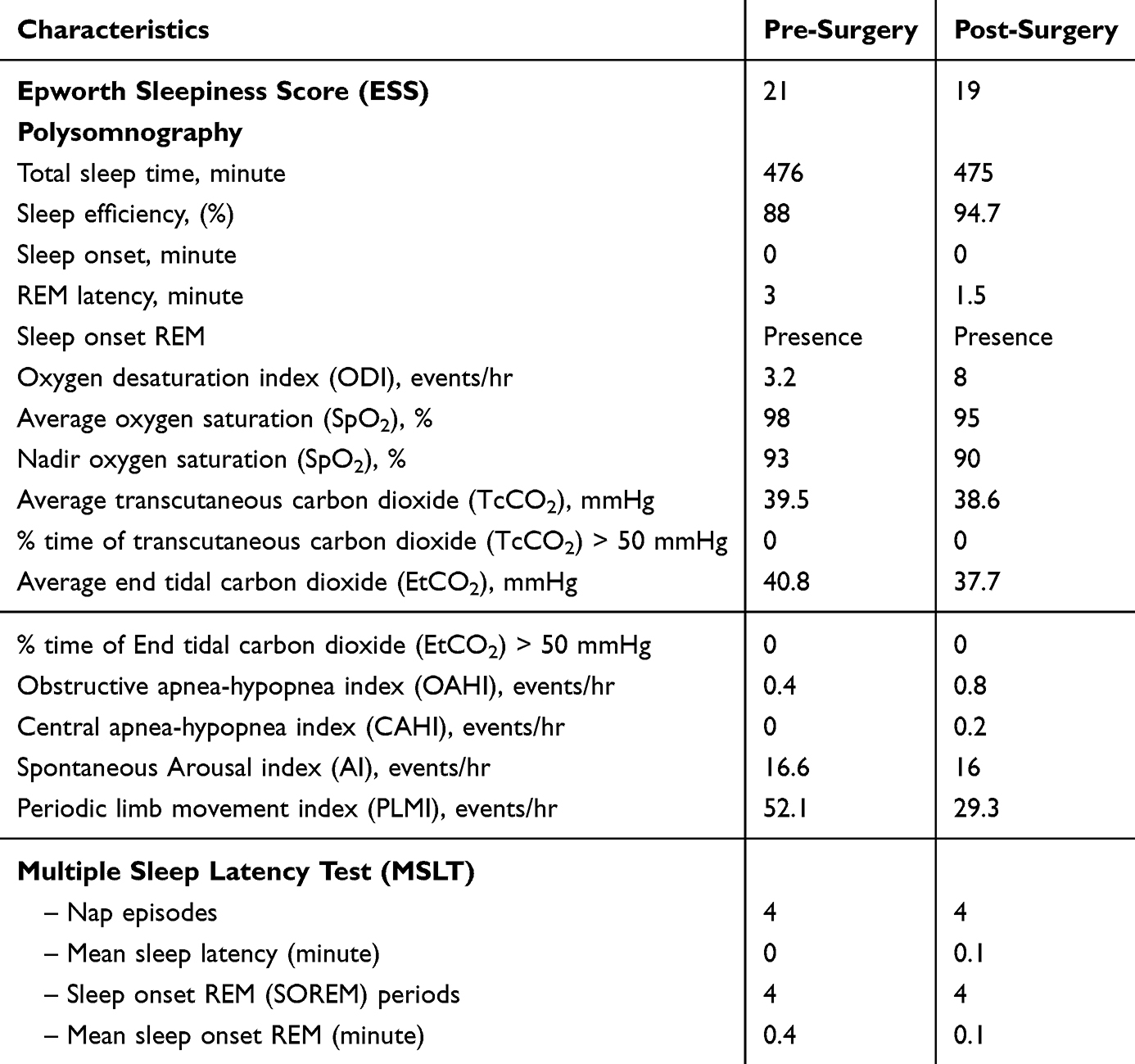 |
Table 4 Comparison of Polysomnographic and MSLT Findings Pre- and Post-Revascularization Surgery in a Patient with Moyamoya Syndrome Diagnosed with Narcolepsy |
Discussion
To our knowledge, this study provides an early descriptive characterization of polysomnographic features in pediatric patients with MMA. Given the small sample size and retrospective design, these findings should be interpreted as descriptive and hypothesis-generating. Nonetheless, the integration of clinical symptoms with PSG and MSLT data offers a comprehensive overview of sleep disturbances in this referred population. Daytime fatigue was the most frequently reported symptom, and polysomnographic findings demonstrated a high prevalence of sleep fragmentation, despite the absence of clinically significant sleep-disordered breathing. In addition, a trend toward shorter REM latency was observed compared with published normative values in pediatric populations. Together, these findings suggest potential alterations in sleep architecture in this small case series. However, the underlying mechanisms remain uncertain.
Sleep fragmentation in MMA may reflect non-respiratory mechanisms, potentially related to cerebrovascular or neurological factors. While other contributors such as sleep hygiene, medication use, or psychiatric comorbidities can influence sleep quality, these were not documented in our cohort. However, the use of single-night PSG introduces the possibility of a first-night effect, a well-documented phenomenon in pediatric sleep studies characterized by reduced sleep efficiency, prolonged sleep onset latency, and increased arousal indices during initial laboratory recordings compared with subsequent nights. This effect has been consistently reported in children undergoing PSG and may lead to overestimation of sleep fragmentation.21 In our cohort, at least one patient demonstrated PSG features suggestive of a first-night effect, including reduced sleep efficiency and prolonged sleep onset latency. Therefore, the classification of sleep fragmentation in this case, and potentially others, should be interpreted with caution. Recent literature has also reported a high prevalence of poor sleep quality and insomnia symptoms in adults with MMA, with significant associations between sleep disturbance and headache burden.22 These findings support the concept that sleep dysfunction may represent an underrecognized comorbidity in Moyamoya and may have implications for neurological outcomes and quality of life. An additional observation relates to the elevated PLMI in the patient with narcolepsy. Although PLMI was increased, these events were not associated with a corresponding increase in cortical arousals on PSG, suggesting that the limb movements were unlikely to be a major contributor to sleep fragmentation in this case. Clinical evaluation, including relevant laboratory investigations, did not identify a treatable underlying cause, and specific treatment for periodic limb movements was not indicated.23 These findings suggest that the patient’s hypersomnolence was more likely attributable to central mechanisms rather than limb movement-related sleep disruption.
The observed trend toward shortened REM sleep latency on nocturnal polysomnography is notable In healthy children and adolescents (10–18 years), REM latency typically ranges from approximately 115 to 156 minutes.24–26 In our cohort, the mean REM latency was 87 minutes, suggesting a relative reduction compared with normative data. Previous studies have demonstrated that REM latency is progressively shorter across sleep disorders associated with hypersomnolence. Mason et al reported a mean REM latency of 137 minutes in healthy adolescents, compared with 96 minutes in patients with obstructive sleep apnea and 60 minutes in patients with narcolepsy.27 Similarly, Rao et al found that shortened REM latency on nocturnal PSG was associated with narcolepsy diagnosed by MSLT.28 Although shortened REM latency has been associated with REM instability and hypersomnolence, this finding is not specific and may also be influenced by other factors, including sleep deprivation, medication effects, or physiological variability.29 In our cohort, no such confounding factors were documented. However, these possibilities cannot be entirely excluded. One potential explanation involves disruption of sleep-wake regulatory pathways, including the orexin system.30,31 Orexin-producing neurons in the hypothalamus play a role in maintaining wakefulness and regulating REM sleep transitions and are known to be vulnerable to ischemic or metabolic stress.32 It is therefore plausible that chronic or intermittent cerebral hypoperfusion in MMA could affect these pathways. However, this hypothesis remains speculative in the absence of direct measurements, such as cerebrospinal fluid orexin levels or targeted neuroimaging of hypothalamic structures. Accordingly, our findings should be interpreted as being consistent with, but not confirmatory of orexin-related mechanisms.
The impact of revascularization surgery on sleep outcomes remains uncertain. A previously published case has suggested that revascularization procedures may partially alleviate sleep-related symptoms, particularly daytime sleepiness.33 In our cohort, a similar pattern was observed in the patient with narcolepsy, who reported subjective improvement in daytime sleepiness following surgery, with a reduction in ESS score from 21 to 19. This change is consistent with the reported minimum clinically important difference (MCID) for the ESS.34 However, objective findings remained largely unchanged. Despite an improvement in sleep efficiency on PSG, mean sleep latency and the number of sleep-onset REM periods (SOREMPs) on MSLT were unchanged, supporting the persistence of narcolepsy following revascularization. This observation highlights the complexity of interpreting postoperative sleep outcomes and suggests that central sleep regulation abnormalities may persist despite surgical intervention. However, given the absence of preoperative PSG data in most patients, it is not possible to determine whether the observed sleep abnormalities are attributable to the underlying disease, the effects of surgery, or other factors.
Comorbid conditions may also contribute to the observed sleep disturbances. The two patients who underwent MSLT had MMS associated with sickle cell disease and neurofibromatosis type 1, respectively, both conditions linked to cerebrovascular abnormalities. Sickle cell disease is characterized by chronic anemia, microvascular occlusion, and recurrent ischemic events, with associated vasculopathy increasing the risk of stroke and silent cerebral infarcts that may disrupt neural pathways involved in sleep regulation.35 Similarly, neurofibromatosis type 1 is associated with intracranial vasculopathy, and mutations affecting neurofibromin expression lead to dysregulation of the RAS signaling pathway and altered neural excitability, which may contribute to hypersomnolence.36 Notably, the most pronounced abnormalities in polysomnographic parameters were observed in patients with MMS. Elevated arousal indices, higher oxygen desaturation indices, and increased PLMI values were primarily seen in patients with underlying conditions such as sickle cell disease, neurofibromatosis type 1, and beta-thalassemia, all of which are independently associated with sleep disturbances. This concentration of more extreme PSG findings within the MMS subgroup suggests that cohort-level interpretations of sleep fragmentation should be made with caution, as these findings may reflect the combined effects of MMA and underlying comorbidities. Importantly, both patients who underwent MSLT, including the patient diagnosed with narcolepsy, had MMS, indicating that the most clinically significant findings occurred in individuals with conditions known to independently affect sleep-wake regulation. These comorbidities may influence sleep regulation through additional vascular or neurological mechanisms. However, the relative contribution of each factor cannot be determined in this study.
Furthermore, RNF213 mutations were identified in 54.5% of patients, raising the possibility of a genetic contribution to sleep disturbances in MMA. Exploratory comparisons between patients with and without RNF213 mutations did not demonstrate clear differences in sleep-related outcomes, including REM latency and ESS scores. However, these observations are limited by the small sample size and lack of statistical power. While RNF213 mutations are known to be associated with cerebrovascular abnormalities,37 their potential role in sleep regulation remains unclear. Further studies are needed to better understand how genetic factors may interact with cerebrovascular and neurological mechanisms to influence sleep disturbances in this population.
Several limitations should be considered. This study represents a small, retrospective, referral-based case series, which limits generalizability and introduces selection bias toward patients presenting with sleep-related symptoms. The absence of baseline (pre-revascularization) PSG data in most patients limits our ability to determine whether the observed findings reflect the underlying disease process, the effects of surgical intervention, or the natural course of sleep development. In this cohort, neurological symptoms were typically identified earlier in childhood, whereas sleep evaluations were performed later, often following revascularization, reflecting clinical referral patterns. Additionally, the lack of a healthy control group and the absence of matched comparisons for comorbid conditions restrict interpretation, and comparisons with normative data were based on published literature rather than direct statistical analysis. Potential confounders, including first-night effect and night-to-night variability, may also influence PSG findings. In the absence of repeated PSG recordings or an adaptation night, the true prevalence of sleep fragmentation in this cohort cannot be determined with certainty, as first-night effects may have contributed to the observed findings. Finally, mechanistic interpretations, including the potential role of orexin dysfunction, remain speculative in the absence of direct cerebrospinal fluid orexin measurements or related neuronal biomarkers, and no targeted neuroimaging data were available. This hypothesis is supported indirectly by evidence from other cerebrovascular and neurodegenerative conditions, such as ischemic stroke, where post-ischemic changes have been shown to impair hypothalamic orexin pathways and contribute to hypersomnolence.38 Accordingly, the underlying pathophysiology of sleep disturbances in pediatric MMA remains incompletely understood.
From a clinical perspective, these findings suggest that sleep disturbances may be present in pediatric patients with MMA, even in the absence of sleep-disordered breathing. While routine sleep screening cannot be recommended based on current evidence, targeted evaluation using PSG or MSLT may be considered in patients presenting with persistent daytime sleepiness, fatigue, or disrupted sleep. Future studies involving larger, prospective cohorts with pre- and post-operative assessments are needed to better characterize sleep disturbances in this population. Incorporation of objective biomarkers, including CSF orexin levels or advanced neuroimaging, may help clarify underlying mechanisms. Additional tools such as actigraphy, the Pittsburgh Sleep Quality Index (PSQI), cyclic alternating pattern (CAP) analysis,39 may further enhance the assessment of sleep patterns and their clinical implications. A better understanding of the mechanisms underlying sleep disturbances in Moyamoya patients may help refine clinical sleep disorder screening strategies and targeted sleep management for this population.
Conclusion
In this small case series, sleep fragmentation was commonly observed in pediatric patients with MMA who were referred for sleep evaluation, despite the absence of clinically significant sleep-disordered breathing. Polysomnographic findings also demonstrated a trend toward shortened REM latency, suggesting potential alterations in sleep architecture. These findings highlight that sleep dysfunction may represent an underrecognized clinical feature in this population. However, given the retrospective design, small sample size, and lack of pre-revascularization baseline data, the current evidence is insufficient to determine the underlying mechanisms or the impact of surgical intervention on sleep outcomes.
Further prospective studies with larger cohorts, including pre- and post-operative assessments and incorporation of objective biomarkers, are needed to better characterize sleep disturbances and their pathophysiological basis in pediatric MMA. Clinically, targeted sleep evaluation may be considered in patients presenting with persistent daytime sleepiness, fatigue, or disrupted sleep patterns.
Abbreviations
AASM, American Academy of Sleep Medicine; BMI, Body Mass Index; CAHI, Central Apnea-Hypopnea Index; CAP, Cyclic alternating pattern; CSF, cerebrospinal fluid; EEG, Electroencephalography; EMG, Electromyography; EOG, Electrooculography; ESS, Epworth Sleepiness Scale; EtCO2, end-tidal carbon dioxide; IQR, Interquartile Range; MCID, Minimum clinically important difference; MMA, Moyamoya arteriopathy; MMD, Moyamoya disease; MMS, Moyamoya syndrome; MSLT, Multiple Sleep Latency Testing; NF1, Neurofibromatosis type 1; OAHI, Obstructive Apnea-Hypopnea Index; ODI, Oxygen Desaturation Index; PLMI, Periodic Limb Movement Index; PSG, Polysomnography; PSQI, The Pittsburgh Sleep Quality Index; REM, Rapid Eye Movement; RNF213, Ring Finger Protein 213; SD, Standard Deviation; SOREMPs, Sleep-Onset Rapid Eye Movement Periods; SpO2, Oxygen Saturation; TcCO2, Transcutaneous Carbon Dioxide.
Data Sharing Statement
The data of this study are available on request from the corresponding author.
Ethical Approval
The study protocol was approved by the institutional research ethics board at the Hospital for Sick Children (REB No. 3414-33601). This research was performed in accordance with the ethical standards of the Declaration of Helsinki.
Acknowledgments
We would like to thank all health care providers who are involved in the care of the patients. We confirm that permission and licensing has been obtained in order to use the ESS tool as part of this study.
Author Contributions
Sirianansopa K.: conceptualization, data curation, formal analysis, methodology, validation, visualization, writing - original draft, and writing – review and editing.
Chiang J.: conceptualization, validation, visualization, writing – review and editing, and supervision.
Amin R.: conceptualization, validation, visualization, writing – review and editing, and supervision.
All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this article.
References
1. Hertza J, Loughan A, Perna R, Davis AS, Segraves K, Tiberi NL. Moyamoya disease: a review of the literature. Appl Neuropsychol. 2014;21(1):21–11. doi:10.1080/09084282.2012.721147
2. Huang S, Guo ZN, Shi M, Yang Y, Rao M. Etiology and pathogenesis of Moyamoya Disease: an update on disease prevalence. Int J Stroke. 2017;12(3):246–253. doi:10.1177/1747493017694393
3. Kleinloog R, Regli L, Rinkel GJE, Klijn CJM. Regional differences in incidence and patient characteristics of moyamoya disease: a systematic review. J Neurol Neurosurg Psychiatry. 2012;83(5):531–536. doi:10.1136/jnnp-2011-301387
4. Po’ C, Nosadini M, Zedde M, et al. Pediatric moyamoya disease and syndrome in italy: a multicenter cohort. Front Pediatr. 2022;10:892445. doi:10.3389/fped.2022.892445
5. Ibrahimi DM, Tamargo RJ, Ahn ES. Moyamoya disease in children. Childs Nerv Syst. 2010;26(10):1297–1308. doi:10.1007/s00381-010-1209-8
6. Zalonis I, Christidi F, Kararizou E, Triantafyllou NI, Spengos K, Vassilopoulos D. Cognitive deficits presenting as psychiatric symptoms in a patient with moyamoya disease. Psychol Rep. 2010;107(3):727–732. doi:10.2466/02.13.15.22.PR0.107.6.727-732
7. Berteotti C, Liguori C, Pace M. Dysregulation of the orexin/hypocretin system is not limited to narcolepsy but has far-reaching implications for neurological disorders. Eur J Neurosci. 2021;53(4):1136–1154. doi:10.1111/ejn.15077
8. Evans BM. What does brain damage tell us about the mechanisms of sleep? J R Soc Med. 2002;95(12):591–597. doi:10.1177/014107680209501204
9. Ito H, Fukatsu N, Rahaman SM, et al. Deficiency of orexin signaling during sleep is involved in abnormal REM sleep architecture in narcolepsy. Proc Natl Acad Sci. 2023;120(41):e2301951120. doi:10.1073/pnas.2301951120
10. Manorenj S, Sultana Shaik R. Clinical Aspects of Moyamoya Disease. In: Vanaclocha V editor. Moyamoya Disease - a Disease to Count on in Your Daily Practice. IntechOpen;2021:33. doi:10.5772/intechopen.96322
11. Yang J, Kim S-K, Chu MK, Rho Y-I, Phi JH, Lee S-Y. Headache in pediatric moyamoya disease after revascularization surgery. Cerebrovasc Dis. 2023;52(3):266–274. doi:10.1159/000526551
12. Amlie-Lefond C, Ellenbogen RG. Factors associated with the presentation of moyamoya in childhood. J Stroke Cerebrovasc Dis. 2015;24(6):1204–1210. doi:10.1016/j.jstrokecerebrovasdis.2015.01.018
13. Happe S. Excessive daytime sleepiness and sleep disturbances in patients with neurological diseases: epidemiology and management. Drugs. 2003;63(24):24. doi:10.2165/00003495-200363240-00003
14. Ahmad SA, Gatti JR, Peterson RK, Burton N, Malone LA, Sun LR. Patient-reported outcomes in childhood moyamoya arteriopathy. Pediatr Neurol. 2025;162:69–75. doi:10.1016/j.pediatrneurol.2024.10.017
15. Johns MW. A new method for measuring daytime sleepiness: the epworth sleepiness scale. Sleep. 1991;14(6):540–545. doi:10.1093/sleep/14.6.540
16. Berry RB, Brooks R, Gamaldo C, et al. AASM scoring manual updates for 2017 (Version 2.4). J Clin Sleep Med. 2017;13(05):665–666. doi:10.5664/jcsm.6576
17. Soori R, Baikunje N, D’sa I, Bhushan N, Nagabhushana B, Hosmane GB. Pitfalls of AHI system of severity grading in obstructive sleep apnoea. Sleep Sci. 2022;15(S 01):285–288. doi:10.5935/1984-0063.20220001
18. Paruthi S, Chervin RD. Approaches to the assessment of arousals and sleep disturbance in children. Sleep Med. 2010;11(7):622–627. doi:10.1016/j.sleep.2009.11.018
19. Maski KP, Amos LB, Carter JC, Koch EE, Kazmi U, Rosen CL. Recommended protocols for the multiple sleep latency test and maintenance of wakefulness test in children: guidance from the American academy of sleep medicine. J Clin Sleep Med. 2024;20(4):631–641. doi:10.5664/jcsm.10974
20. Ruoff C, Rye D. The ICSD-3 and DSM-5 guidelines for diagnosing narcolepsy: clinical relevance and practicality. Curr Med Res Opin. 2016;32(10):1611–1622. doi:10.1080/03007995.2016.1208643
21. Verhulst SL, Schrauwen N, De Backer WA, Desager KN. First night effect for polysomnographic data in children and adolescents with suspected sleep disordered breathing. Arch Dis Child. 2006;91(3):233–237. doi:10.1136/adc.2005.085365
22. Ahmad M, Klaas JP, Lanzino G, et al. Characteristics of sleep disturbance in Moyamoya disease. Sleep Med. 2026;138:108684. doi:10.1016/j.sleep.2025.108684
23. Castro OL, De Franceschi L, Ganz T, et al. Iron restriction in sickle cell disease: when less is more. Am J Hematol. 2024;99(7):1349–1359. doi:10.1002/ajh.27267
24. Kirov R, Kinkelbur J, Heipke S, et al. Is there a specific polysomnographic sleep pattern in children with attention deficit/hyperactivity disorder? J Sleep Res. 2004;13(1):87–93. doi:10.1111/j.1365-2869.2004
25. Carotenuto M, Messina G, Esposito M, Santoro C, Iacono D, Spruyt K. Polysomnographic study in pediatric neurofibromatosis type 1. Front Neurol. 2023;14:1213430. doi:10.3389/fneur.2023.1213430
26. Busby K, Firestone P, Pivik RT. Sleep patterns in hyperkinetic and normal children. Sleep. 1981;4(4):366–383. doi:10.1093/sleep/4.4.366
27. Mason TBA, Teoh L, Calabro K, et al. Rapid eye movement latency in children and adolescents. Pediatr Neurol. 2008;39(3):162–169. doi:10.1016/j.pediatrneurol.2008.06.011
28. Rao SC, Mansukhani MP, Lloyd RM, Slocumb NL, Kotagal S. Nocturnal polysomnographic characteristics of pediatric narcolepsy: polysomnography characteristics in pediatric narcolepsy. Sleep Biol Rhythms. 2012;10(1):69–71. doi:10.1111/j.1479-8425.2011.00508.x
29. Drakatos P, Suri A, Higgins SE, et al. Sleep stage sequence analysis of sleep onset REM periods in the hypersomnias. J Neurol Neurosurg Psychiatry. 2013;84(2):223–227. doi:10.1136/jnnp-2012-303578
30. Rye DB. Excessive daytime sleepiness and unintended sleep in Parkinson’s disease. Curr Neurol Neurosci Rep. 2006;6(2):169–176. doi:10.1007/s11910-996-0041-8
31. Kamat PK, Khan MB, Smith C, et al. The time dimension to stroke: circadian effects on stroke outcomes and mechanisms. Neurochem Int. 2023;162:105457. doi:10.1016/j.neuint.2022.105457
32. Song J, Kim E, Kim CH, Song HT, Lee JE. The role of orexin in post-stroke inflammation, cognitive decline, and depression. Mol Brain. 2015;8(1):16. doi:10.1186/s13041-015-0106-1
33. Bingeliene A, Shapiro C M. Case report: disturbed sleep in a patient with moyamoya disease. J Sleep Disord Treat Care. 2015;04(04). doi:10.4172/2325-9639.1000164
34. Patel S, Kon SS, Nolan CM, et al. Minimum clinically important difference of the Epworth Sleepiness Scale. Sleep and Control of Breathing. European Respiratory Society; 2017:PA330. doi:10.1183/1393003.congress-2017.PA330
35. Stotesbury H, Kawadler JM, Hales PW, Saunders DE, Clark CA, Kirkham FJ. Vascular instability and neurological morbidity in sickle cell disease: an integrative framework. Front Neurol. 2019;10:871. doi:10.3389/fneur.2019.00871
36. Anastasaki C, Rensing N, Johnson KJ, Wong M, Gutmann DH. Neurofibromatosis type 1 (Nf1)-mutant mice exhibit increased sleep fragmentation. J Sleep Res. 2019;28(4):e12816. doi:10.1111/jsr.12816
37. Kobayashi H, Kabata R, Kinoshita H, et al. Rare variants in RNF213, a susceptibility gene for moyamoya disease, are found in patients with pulmonary hypertension and aggravate hypoxia-induced pulmonary hypertension in mice. Pulm Circ. 2018;8(3):1–13. doi:10.1177/2045894018778155
38. Brown RE, Basheer R, McKenna JT, Strecker RE, McCarley RW. Control of sleep and wakefulness. Physiol Rev. 2012;92(3):1087–1187. doi:10.1152/physrev.00032.2011
39. Parrino L, Grassi A, Milioli G. Cyclic alternating pattern in polysomnography: what is it and what does it mean? Curr Opin Pulm Med. 2014;20(6):533–541. doi:10.1097/mcp.0000000000000100
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.