Back to Journals » Patient Preference and Adherence » Volume 20
Polypharmacy Experience of Middle-Aged and Elderly Patients with Type 2 Diabetes Comorbidity: A Qualitative Study
Received 27 February 2026
Accepted for publication 15 June 2026
Published 9 July 2026 Volume 2026:20 605584
DOI https://doi.org/10.2147/PPA.S605584
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Emma Veale
Zhu Han, Li Wang
School of Nursing, Liaoning University of Traditional Chinese Medicine, Shenyang, Liaoning, People’s Republic of China
Correspondence: Li Wang, School of Nursing, Liaoning University of Traditional Chinese Medicine, Shenyang, Liaoning, People’s Republic of China, Email [email protected]
Purpose: To reveal the real experience of polypharmacy in middle-aged and elderly patients with type 2 diabetes comorbidity, based on the Common-Sense Model of self-regulation (CSM).
Patients and Methods: With the method of purposive sampling, 15 middle-aged and elderly patients with type 2 diabetes comorbidity hospitalized in the endocrinology department of a tertiary hospital were selected for semi-structured interviews. Using the Colaizzi’s seven-step method to analyze and organize the interview results.
Results: 4 themes and 9 subthemes were identified and organized based on the Common-Sense Model of self-regulation: cognitive representation (cognitive struggle in coexistence with medicines, physical discomfort and adjustment, expectations for treatment methods); emotional representation (memory burden, space management burden); coping strategies - negative and positive responses (negative emotions related to polypharmacy, self driven); external factors (family support feels helpful, medical staff support feels relieved).
Conclusion: The psychological experience of middle-aged and elderly patients with type 2 diabetes comorbidity in the course of taking medicine includes the interaction of cognitive and emotional representation, coping strategies and external support system at all levels. Medical personnel should clarify patients’ treatment burden, polypharmacy burden, self-management workload, coping strategies and effective support system during the medication process, in order to provide patient-centered medicine care and achieve more ideal emotional and health outcomes.
Keywords: diabetes mellitus, comorbidity, polypharmacy, qualitative research, common-sense model of self-regulation
Introduction
The comorbidity of diabetes has become a serious health problem. Comorbidity refers to the same patient having two or more diseases simultaneously.1 In the group of diabetes patients, comorbidity is extremely common. Related large sample research results show that 83.3% of middle-aged and elderly patients with type 2 diabetes are comorbidity.2 Compared with single disease, comorbidity of diabetes is one of the key factors threatening health aging. The presence of comorbidities can greatly shorten the life expectancy of patients, with an average loss of life of 5.4 to 6.8 years per person.3 And often face greater challenges in disease management. These patients have relatively poor physical function, usually requiring the use of multiple medications, and the frequency of medical resource utilization is also higher.4,5 In addition, comorbidities can further exacerbate the economic pressure and treatment burden on patients.6 Therefore, comorbidities have a profound impact on the clinical prognosis, psychological state, and treatment burden of patients.
Medication management is a crucial part of daily health management. Regular medication can enable patients to more effectively control their blood glucose levels, thereby avoiding the occurrence of complications.7 However, the complexity of medication regimens not only increases the risk of side effects and medicine interaction events,8,9 but also increase the medication burden on patients, reduce their quality of life and medication adherence.10,11 Furthermore, it affects the patient’s blood glucose control level and re-hospitalization rates.10,12
In the research field of medication adherence of diabetes patients, cross-sectional research currently occupies a leading position. For example, Ahmed et al13 investigated many influencing factors of medication adherence of patients with diabetes through cross-sectional study. Qualitative research can reveal the true feelings of nursing objects that are difficult to quantify numerically in nursing practice, and providing strong support for developing personalized nursing plans.
The Common Sense Model of illness self-regulation14 suggests that when individuals face health threats, they will form two relatively independent self-regulation systems: cognitive representation (including their experiences with medication and the degree to which diseases affect their lives) and emotional representations (emotional reactions caused by health threats) and coping processes, the patient’s cognitive and emotional representation will directly or indirectly affect the emotional outcome and disease outcome through coping style, at the same time, the social and cultural environment in which an individual operates will also play a regulatory role throughout the entire process.
This study adopts descriptive phenomenological research methods, based on the Common Sense Model of self-regulation, through semi-structured interviews with middle-aged and elderly patients with type 2 diabetes comorbidity with a wide variety of medication types, to deeply explore the emotional outcomes and disease outcomes related to the emotional outcomes in the Common Sense Model of self-regulation, that is, patients’ experience in the process of polypharmacy and medication adherence affected by emotional outcomes and directly related to disease outcomes. To provide scientific recommendations for establishing a comprehensive and effective medication treatment nursing model, in order to reduce the difficulties and negative pain experiences faced during the polypharmacy process, effectively leverage promoting factors, and thereby improve patients’ medication compliance and health outcomes.
Methods
Design
The core of descriptive phenomenology lies in exploring the essence of lived experience. Through multiple interviews and in-depth analysis, researchers have taken the patient’s perspective and comprehensively grasped the subjective feelings in the process of polypharmacy, covering multiple dimensions such as cognition, emotion, and behavior. Therefore, this study adopts descriptive phenomenological research and focuses on Interpretivism philosophical orientation to deeply understand the inner experience of polypharmacy in middle-aged and elderly patients with type 2 diabetes comorbidity. Follow COREQ’s standards in the design and reporting process.15
Setting and Participant
The data collection was conducted in the endocrinology ward of a tertiary hospital in Liaoning Province, China. Due to the complexity of medication regimens for hospitalized patients, the ability to maximize the presentation of the emotional experience of “polypharmacy” constitutes the phenomenon explored in this study, which is conducive to obtaining a “thick description” for more comprehensive consideration of the types of polypharmacy experiences of patients in the future. The hospital has a large number of patients and is concentrated, and the research team has a cooperative relationship with the hospital. Therefore, this hospital was selected as the recruitment point.
Through the purposive sampling method, the principle of maximum differentiation is followed to ensure the diversity of patients in terms of age, gender, education level, residence, course of diabetes, types of combined diseases. Inclusion criteria include (1) patients with type 2 diabetes diagnosed by doctors, (2) patients with one or more chronic diseases besides type 2 diabetes, (3) patients over 45 years of age, and (4) patients taking five or more medications. Excluded patients who are unable to communicate normally.
Data Collection
The interviewer is a female nursing graduate student who has obtained the English CET-6 and nursing qualification certificate, and has received systematic training in qualitative research methodology and has a dual identity as an student nurse in the endocrinology department and a qualitative researcher. The identity of an student nurse familiarizes researchers with the patient’s condition, and also establishes a good trust relationship. At the same time, in order to avoid desirability bias and power imbalance caused by participants viewing the interviewer as a member of the medical team, the researcher clearly informed the participants before the interview that I am currently a researcher, and the answers to the interview will not have any impact, in order to reduce the medical authority effect. During the interview process, the first author conducted semi-structured interviews in a face-to-face manner. Another researcher observed and recorded the interviewee’s non-verbal information such as tone, intonation, facial expressions, and changes in body movements in detail. The final interview outline was presented in Table 1.
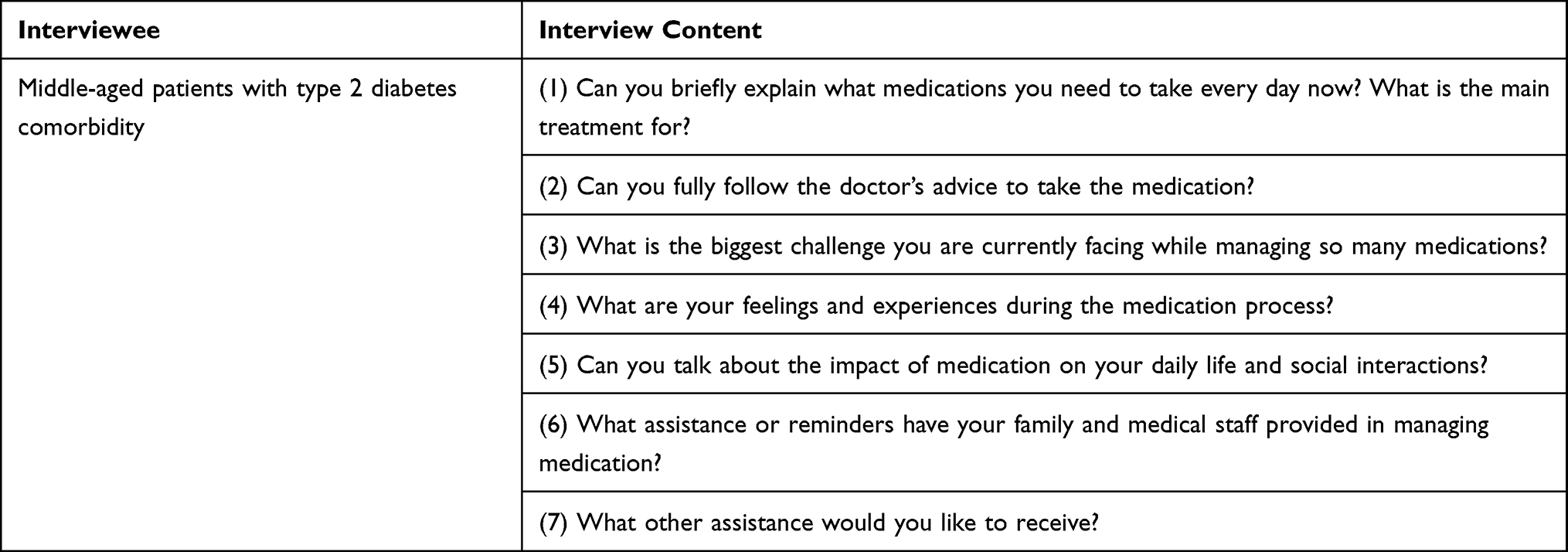 |
Table 1 Semi-Structured Interview Outline |
Data Analysis
After the interview, the researcher transcribed the interview data into text within 24 hours and supplemented it with on-site notes to verify the interviewee’s facial expressions, silence time, and body movements at that time, forming a written document. And use the Colaizzi’s seven-step method for data analysis.16
Two researchers independently and repeatedly read the transcribed text, extracted meaningful statements, constructed them into meaning units, and preliminary classified and integrated the codes into themes. Further, each theme will be described in detail to form the essential structure of polypharmacy use experience of patients, and be improved and optimized. Due to the clear viewpoints expressed by some patients during the interview process or their discharge and loss to follow-up, after a detailed description of the themes, this study will return to participants for formal member checking when necessary and feasible to confirm that the theme is in line with its original intention. The analysis results were not returned to all participants for formal member verification, but the core viewpoints were immediately reiterated to the participants after the interview, obtaining their initial confirmation.
During this process, the two researchers continuously discussed; return to the original text for inconsistent codes and discuss it again in context; timely resolution of differences to reach consensus. Throughout the entire data analysis process, the two researchers maintained an open and inclusive attitude, constantly reflecting on whether their personal values and identities had any potential interference or impact on the research results.
Ethical Considerations
Before the formal interview, the research team explained in detail the purpose and process of the study to the patients, promised to strictly follow the principle of confidentiality, and after obtaining the patient’s consent, guided the interviewees to fill out the general information questionnaire (Figure 1) and informed consent form. After obtaining the patient’s consent, the recording was made.
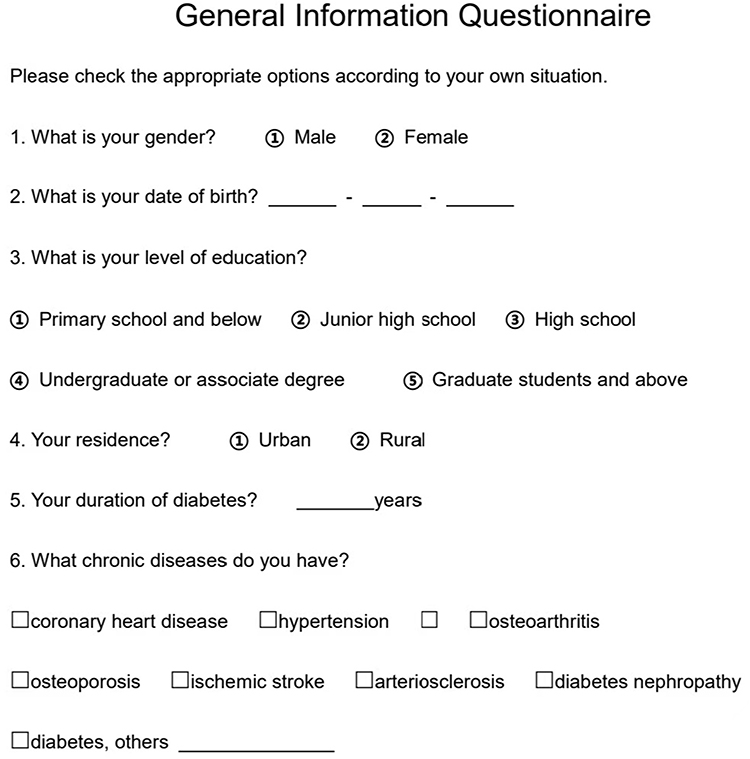 |
Figure 1 General Information Questionnaire. |
In order to protect the anonymity and privacy of participants, all identification information that may involve personal identity in the research results was replaced with numbers (such as N1, N2, etc).
Rigor
In the research design phase, this study first conducted pre interviews, and then modified the interview outline based on the interview results and research group discussion results to determine the final interview outline, ensuring that the interview outline can cover the questions of this study.
During the interview process, the first author act as a researcher and maintains a neutral attitude and does not interrupt the interviewee’s response to ensure that the research subjects can express their true experiences without reservation and avoid power desirability bias. A triangulation method of questioning participants and reviewing medical records to ensure the accuracy of data collection was used.
In the data analysis stage: After the interview, the research team promptly transcribed and reviewed the interview data. As the analysis deepens, constantly reflecting and adjust the codes.
Results
Participant Characteristics
This study interviewed a total of 15 patients who met the inclusion criteria and completed the interview. After interviewing the 11th participant, the explanatory dimensions of each code or theme began to reappear, and no other explanations were found. The depth of meaning of the code and theme was fully explored, the data has reached meaning saturation.17 Table 2 provides detailed data.
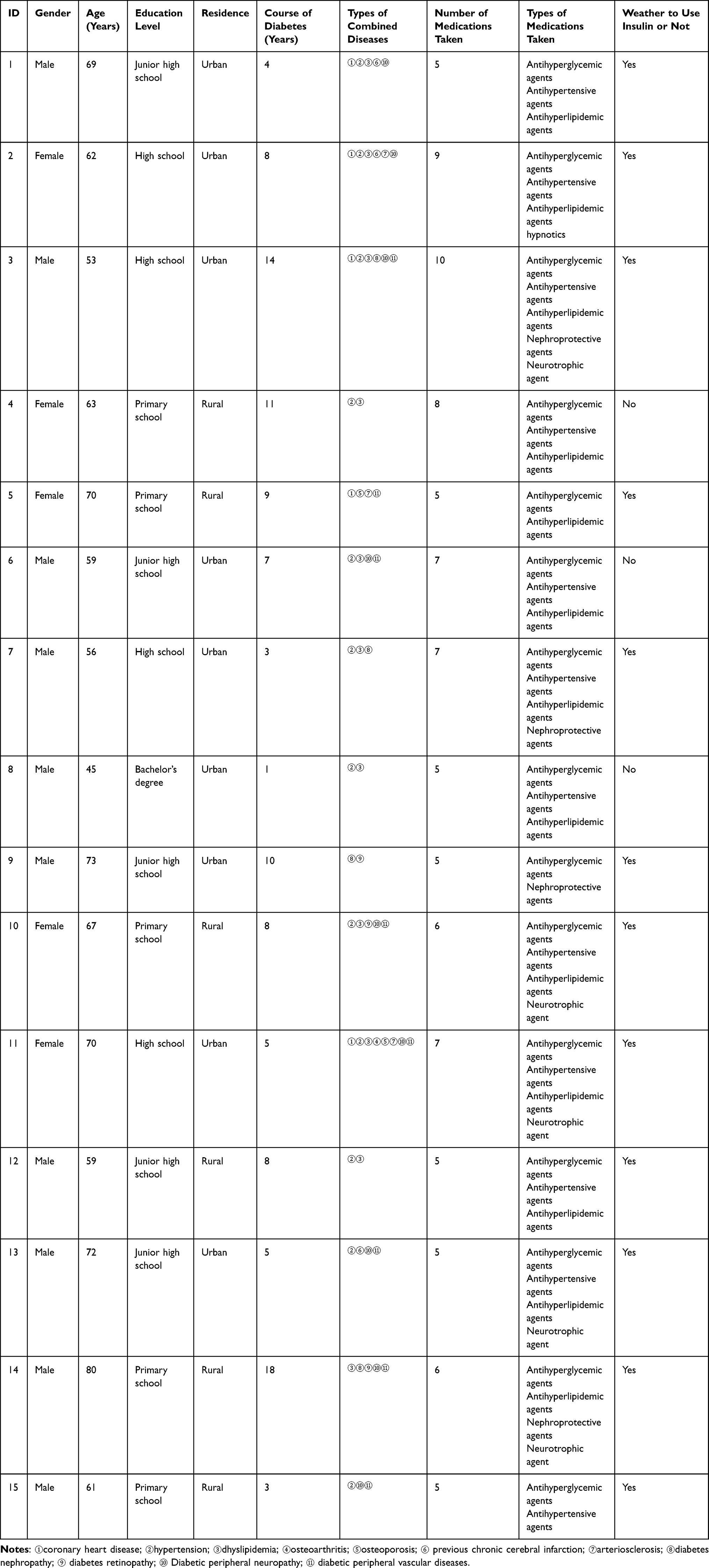 |
Table 2 Demographic Characteristics of the Participants |
Key Themes
Table 3 shows the themes and subthemes formed based on the interview results.
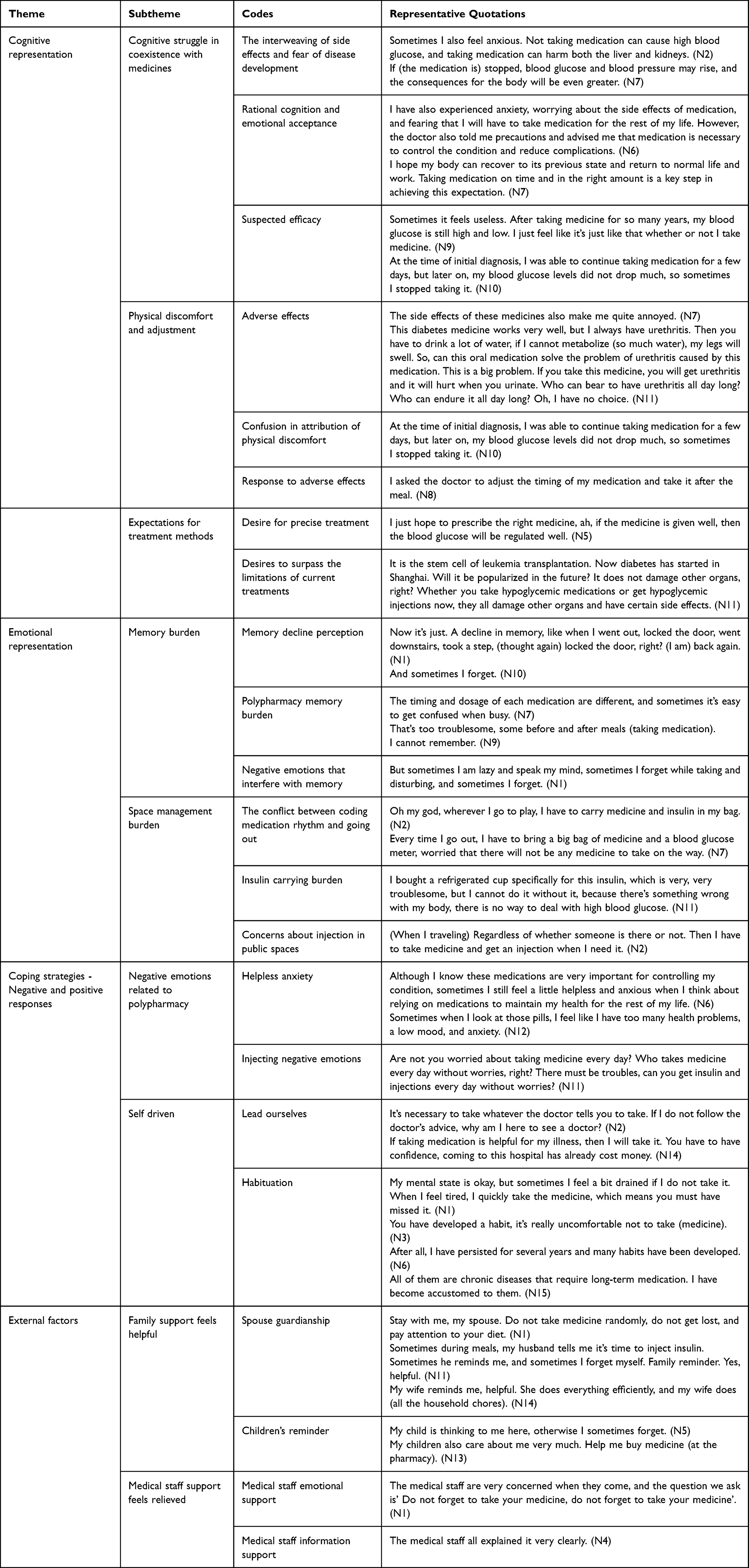 |
Table 3 Themes and Subthemes |
Theme 1: Cognitive Representation
Cognitive Struggle in Coexistence with Medicines
Patients’ understanding of medicines is a dynamic cognitive process constantly constructed in their daily polypharmacy experience. Patients often worry about side effects during the treatment process, and this fear and anxiety caused by not taking medication lead to uncontrolled blood glucose levels, creating a dual pressure. In addition, some patients acknowledge the necessity of medication treatment, but still find it emotionally difficult to fully accept the transition of their life state to “lifelong medication”. Strive to find a balance between worrying about side effects and craving to control the condition. When medicines fail to bring visible improvements as expected, patients question the significance of medicine treatment and even gradually lose patience, no longer strictly following medical advice.
Sometimes I also feel anxious. Not taking medication can cause high blood glucose, and taking medication can harm both the liver and kidneys. (N2)
If (the medication is) stopped, blood glucose and blood pressure may rise, and the consequences for the body will be even greater. (N7)
I have also experienced anxiety, worrying about the side effects of medication, and fearing that I will have to take medication for the rest of my life. However, the doctor also told me precautions and advised me that medication is necessary to control the condition and reduce complications. (N6)
At the time of initial diagnosis, I was able to continue taking medication for a few days, but later on, my blood glucose levels didn’t drop much, so sometimes I stopped taking it. (N10)
Physical Discomfort and Adjustment
Side effects constitute one of the most direct and troubling components of a patient’s physical experience. The patient feels a sense of powerlessness between efficacy dependence and side effects. Faced with physical discomfort, patients undergo a complex attribution process, and this attribution confusion directly affects their medication behavior. Faced with the dilemma of side effects, some patients actively seek coping methods.
This diabetes medicine works very well, but I always have urethritis. Then you have to drink a lot of water, if I can’t metabolize (so much water), my legs will swell. So, can this oral medication solve the problem of urethritis caused by this medication. This is a big problem. If you take this medicine, you will get urethritis and it will hurt when you urinate. Who can bear to have urethritis all day long? Who can endure it all day long? Oh, I have no choice. (N11)
At the time of initial diagnosis, I was able to continue taking medication for a few days, but later on, my blood glucose levels didn’t drop much, so sometimes I stopped taking it. (N10)
I asked the doctor to adjust the timing of my medication and take it after the meal. (N8)
Expectations for Treatment Methods
When faced with diseases and side effects, patients also shift from passive acceptance to active seeking, hoping that doctors can accurately use medication to treat diseases more effectively. In addition, patients have become aware of the limitations of the current treatment model (side effects, lifelong dependence), which has given rise to deep expectations for medical breakthroughs. New technologies such as stem cell therapy have become symbols of hope for breaking free from medicine constraints.
I just hope to prescribe the right medicine, ah, if the medicine is given well, then the blood glucose will be regulated well. (N5)
It is the stem cell of leukemia transplantation. Now diabetes has started in Shanghai. Well, will it be popularized in the future? It doesn’t damage other organs, right? Whether you take hypoglycemic medications or get hypoglycemic injections now, they all damage other organs and have certain side effects. (N11)
Theme 2 Emotional Representation
Memory Burden
The patient attributed the missed medication to the use of a variety of medicines, feeling a decrease in memory, and negative emotional interference related to medication, complex medication plans often exceed their memory load. Therefore, experiencing the prominent dilemma of memory burden during the medication process.
Now it’s just. a decline in memory, like when I went out, locked the door, went downstairs, took a step, (thought again) locked the door, right? (I’m) back again. (N1)
The timing and dosage of each medication are different, and sometimes it’s easy to get confused when busy. (N7)
But sometimes I am lazy and speak my mind, sometimes I forget while taking and disturbing, and sometimes I forget. (N1)
Space Management Burden
For patients with diabetes comorbidity, they need to carry a variety of medicines when they leave their regular living space. The patients feel faced with many challenges, including the conflict between the fixation of medication time and going out activities. For patients who use insulin therapy, the special requirements of carrying insulin preservation when going out increase the space management burden. Moreover, performing injection activities in public spaces puts patients under social and psychological pressure.
Oh my god, wherever I go to play, I have to carry medicines and insulin in my bag. Regardless of whether someone is there or not. Then I have to take medicines and get an injection when I need it. (N2)
I bought a refrigerated cup specifically for this insulin, which is very, very troublesome, but I can’t do it without it, because there’s something wrong with my body, there is no way to deal with high blood glucose. (N11)
Theme 3 Coping Strategies – Negative and Positive Responses
Negative Emotions Related to Polypharmacy
Comorbidity patients face the challenge of long-term polypharmacy, which leads to negative psychological reactions. When patients realize the coexistence of multiple diseases, the complexity of the disease, the long-term nature of treatment while taking medication, they may fall into negative emotions. For insulin treated patients, injection therapy, as an important means of diabetes management, brings emotional burden to patients by repeated injections every day.
Although I know these medications are very important for controlling my condition, sometimes I still feel a little helpless and anxious when I think about relying on medications to maintain my health for the rest of my life. (N6)
Sometimes when I look at those pills, I feel like I have too many health problems, a low mood, and anxiety. (N12)
Aren’t you worried about taking medicine every day? Who takes medicine every day without worries, right? There must be troubles, can you get insulin and injections every day without worries? (N11)
Self Driven
Sometimes patients choose to actively respond rather than passively taking medication under external coercion. Driven by a sense of responsibility, patients believe that only by actively cooperating can the effectiveness of the treatment plan be maximized, prompting them to strictly follow medical advice. When taking medication becomes a habit in patients’ daily lives and integrated into their health behaviors, physical discomfort can serve as a physical signal of missed medication, and patients feel a reduced burden on memory.
It’s necessary to take whatever the doctor tells you to take. If I don’t follow the doctor’s advice, why am I here to see a doctor? (N2)
My mental state is okay, but sometimes I feel a bit drained if I don’t take it. When I feel tired, I quickly take the medicine, which means you must have missed it. (N1)
You’ve developed a habit, it’s really uncomfortable not to take (medicine). (N3)
All of them are chronic diseases that require long-term medication. I have become accustomed to them. (N15)
Theme 4 External Factors
Family Support Feels Helpful
Reminders and support from family members can help patients avoid forgetting to take medication or inject insulin, making them feel that they are not facing it alone. Most respondents stated that family support can help them cope with complex medication plans, and through specific behaviors such as reminders, supervision, and sharing of dietary management, family members directly reduce their implementation burden.
Stay with me, my spouse. Don’t take medicine randomly, don’t get lost, and pay attention to your diet. (N1)
My child is thinking to me here, otherwise I sometimes forget. (N5)
Sometimes during meals, my husband tells me it’s time to inject insulin. Sometimes he reminds me, and sometimes I forget myself. Family reminder. Yes, helpful. (N11)
Medical Staff Support Feels Relieved
When medical staffs explain medication plans in a detailed and clear manner, patients not only experience information acquisition, but also a sense of existential “comfort” - this comfort comes from the “seeing” and “responding” of professional others, which relieves patients’ uncertainty and anxiety when facing complex treatment plans.
The medical staff are very concerned when they come, and the question we ask is’ Don’t forget to take your medicine, don’t forget to take your medicine’. (N1)
Discussion
This study is based on the Common Sense Model of self-regulation and clarifies the four core dimensions of cognitive representation, emotional representation, coping strategies, and external factors that affect patients’ emotional and health outcomes when facing health threats.
When patients face the health threats of comorbidities and polypharmacy, they develop cognitive representation (cognitive struggle in coexistence with medicines, physical discomfort and adjustment, expectations for treatment methods), as well as emotional representation (memory burden, space management burden). This leads to positive or negative coping strategies, which in turn affect the emotional outcomes (polypharmacy experience) and disease outcomes (medication adherence) related to the emotional outcomes. During this process, external support from families and medical staff played a moderating role.
Main Findings at Cognitive Representation Level
The patient’s cognitive representation of medication affects their polypharmacy experience. This cognition is mainly reflected in the understanding of medication side effects, perception of diseases and medication effects. As mentioned, for patients who require long-term medication, worrying about the potential side effects of the medication is a common psychological state. However, some patients believe that reducing medication to avoid side effects may further worsen the condition. At the same time, they also hope to restore their health through rational medication use, so they need to seek a balance between medication efficacy and side effects. On the contrary, patients who are skeptical about the efficacy of medication often lack confidence in treatment.
Related Research Support
In terms of medication side effect cognition and treatment confidence, Wu’s18 research found that Chinese elderly patients with type 2 diabetes who have low general harm beliefs often have a high sense of self-efficacy, which makes their medication adherence level higher. According to the theoretical framework of the health belief model, patients’ decisions about their health behaviors can be influenced by two important cognitive factors: the assessment of the potential serious consequences of diseases, such as death, disability, and long-term health problems, and the perception of the advantages of adopting healthy behaviors, these cognitive aspects affect patients’ long-term treatment adherence.19 Perceived susceptibility, perceived medication benefits, and self-efficacy were significant health belief model predictors for medication adherence in the population of type 2 diabetes patients.20,21 Abdelhamid et al22 and Bilondi et al23 further shows that disease cognition is an important predictor of medication adherence of diabetes patients.
Clinical Implications
It has been reported that the efficacy and side effects affect patients’ polypharmacy experience. Therefore, patients can be guided to correctly view the efficacy and side effects of medicines and actively observe the positive changes that occur in their bodies after regular medication adherence, which may effectively improve their medication self-management level.
Main Findings at Emotional Representation Level
Emotional representation is an important component of the Common Sense Model of self-regulation, which directly affects patients’ coping behaviors and emotional outcomes. From the perspective of emotional representation, this study found that the burden of memory and space management in the polypharmacy experience of diabetes comorbidity patients were the core variables. It is worth noting that this burden is not only due to the complexity of the medicine regime,24 but also closely related to the interference of negative emotions on cognitive function. The “spatial management burden” in this study reveals the multiple challenges faced by patients in outdoor situations. From the perspective of emotional representation, these spatial management dilemmas essentially trigger patients’ stigma and constitute a strong negative emotional experience.
Related Research Support
The self-regulation theory regards medication adherence as a health behavior that requires self-regulation.25 Negative emotional states can consume an individual’s self-control resources, leading to impaired memory in patients. For patients who inject insulin in public places, frequent feeling embarrassed or criticized is one of the difficulties faced by patients.26,27
Clinical Implications
Actively evaluating the emotional representation status of patients, paying attention to the regulatory effect of emotional status on behavior, identifying the emotional context behind behavior, and thereby helping patients establish emotional regulation ability to alleviate the burden of polypharmacy can be considered by nursing staffs.
Main Findings at Coping Strategies Level
In the coping style dimension of the Common Sense Model of self-regulation, individuals will develop coping strategies based on their cognitive and emotional responses, and actively adopt regulatory behaviors. This study found that it includes negative coping with negative emotions caused by the disease itself, as well as polypharmacy and insulin injections, and promoting medication as a habit to maintain treatment adherence or positive coping driven by a sense of responsibility without consuming cognitive resources. These coping strategies reflect patients’ negative and positive cognitive evaluations of cognitive and emotional representations.
Related Research Support
The relevant survey shows that there is a significant difference between positive and negative coping style of diabetes patients, and the number of patients who choose negative coping style is higher than that of positive coping style.28 Problem solving positive coping style help improve medication adherence, while negative coping strategies are negatively correlated with medication adherence.29 And patients on insulin therapy were associated with an increased risk of depression compared with those on non-insulin treatment.30
Clinical Implications
Based on this, there is a complex interaction between diabetic trouble and coping mechanism, and patients may strictly follow the treatment plan on the surface, but bear a huge emotional burden on the heart. Patients may beneficial for nursing staffs to go beyond the behavioral level of adherence assessment, pay attention to the coping style dimension of patients’ polypharmacy experience, provide emotional support and cognitive reconstruction for those patients who are “highly dependent and suffering”, to promote their transformation from “painful persistence” to “active management”.
Main Findings at External Factors Level
For external support systems, the Common Sense Model of self-regulation suggests that an individual’s social environment will also affect their perception and coping strategies towards diseases, and further influence emotional and disease outcomes. The supports from family members or medical staff serve as external environmental factors, helping patients feel embedded in the meaning network of family relationships and feel a sense of security and belonging in the reality of multiple diseases coexisting and polypharmacy.
Related Research Support
According to social support theory, information or emotional support networks from families or healthcare professionals can buffer the negative impact of adverse events on emotions.31 Research has found that the quality of social support is the core mechanism for improving polypharmacy experience. Patients with informal caregivers such as friends and family have significantly higher levels of medication adherence.32 Further research by Olagbemide has shown that good family support can significantly improve patients’ medication adherence, thereby promoting better blood glucose control, in the strong family support group, 69.5% achieved medium/high medication adherence, and 65.7% achieved good blood glucose control.33
Clinical Implications
Therefore, there is evidence supporting the active effects of external factors. Providing professional and emotional support and guide family members to actively participate in medication management is recommended to nursing staffs to improve patients’ polypharmacy experience and more effectively manage related diseases.
Limitations
Due to the lack of longitudinal research in this study, it is difficult to clarify the changes in polypharmacy experience and adherence among patients at different stages of the disease. In view of this, future research can fully consider the differences in economic, cultural, and medical levels among different regions in China, further expand the scope of research subjects, extend follow-up time, and conduct multi center patient journey map research, in order to have a more comprehensive and in-depth understanding of patient conditions, further enrich research results, and provide more valuable reference for related research and practice.
Conclusion
Based on the Common Sense Model of self-regulation, this study focuses on the polypharmacy experience of middle-aged and elderly patients with type 2 diabetes comorbidity, to provide reference for targeted nursing measures. The research results show that the middle-aged and elderly patients with type 2 diabetes comorbidity have complex perceptions of diseases and medicines, management burdens, positive and negative coping style, and needs and recognition of external support systems in the process of polypharmacy. Medical staff can identify the polypharmacy experience of middle-aged and elderly patients with type 2 diabetes comorbidity from multiple perspectives, actively explore personalized nursing intervention strategies, improve patients’ medication emotional experience, and then promote patients to adopt health behaviors to improve adherence, thus promoting patients’ health outcomes.
Ethics Approval and Informed Consent
The first author of this study is a current graduate student at Liaoning University of Traditional Chinese Medicine, and the corresponding author is a supervisor at Liaoning University of Traditional Chinese Medicine. A cooperative relationship was established with Tieling Central Hospital in Liaoning Province, and this study has been reviewed and approved by the Ethics Committee of Tieling Central Hospital (2025-40). This study was conducted in accordance with the Helsinki Declaration, ensuring that all ethical standards were followed throughout the research process. All the participants informed consent included publication of anonymized responses/direct quotes.
Acknowledgments
We sincerely thank every patient who participated in the study. They patiently shared their experiences and feelings, providing a foundation for the progress of this study. At the same time, we also very grateful to Director Han from the Nursing Department of Tieling Central Hospital for her support throughout the recruitment and research implementation process.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no relevant funding support for this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chang F, Zhang R, Lu Y, et al. Analysis and design of the concept system of comorbidity. Chin J Gen Pract. 2018;21(3):256–15. doi:10.3969/j.issn.1007-9572.2017.00.219
2. Yan ZY, Gao R, Sun MY, et al. Analysis of comorbidity pattern of elderly patients with type 2 diabetes based on outpatient electronic medical record data. China Public Health. 2022;38(12):1576–1581. doi:10.11847/zgggws1138135
3. Compile the clinical guidelines for the prevention and treatment of senile diabetes in China. Chinese clinical guidelines for the prevention and treatment of elderly type 2 diabetes (2022 Edition). Chin J Diabet. 2022;30(1):2–51. doi:10.3969/j.issn.1006-6187.2022.01.002
4. Skou ST, Mair FS, Fortin M, et al. Multimorbidity. Nat Rev Dis Primers. 2022;8(1):48. doi:10.1038/s41572-022-00376-4
5. Nowakowska M, Zghebi SS, Ashcroft DM, et al. The comorbidity burden of type 2 diabetes mellitus: patterns, clusters and predictions from a large English primary care cohort. BMC Med. 2019;17(1):145. doi:10.1186/s12916-019-1373-y
6. Religioni U, Barrios-Rodríguez R, Requena P, Borowska M, Ostrowski J. Enhancing Therapy Adherence: impact on Clinical Outcomes, Healthcare Costs, and Patient Quality of Life. Medicina. 2025;61(1):153. doi:10.3390/medicina61010153
7. Piragine E, Petri D, Martelli A, Calderone V, Lucenteforte E. Adherence to oral antidiabetic drugs in patients with type 2 diabetes: systematic review and meta-analysis. J Clin Med. 2023;12(5):1981. doi:10.3390/jcm12051981
8. Indu R, Adhikari A, Maisnam I, Basak P, Sur TK, Das AK. Polypharmacy and comorbidity status in the treatment of type 2 diabetic patients attending a tertiary care hospital: an observational and questionnaire-based study. Perspect Clin Res. 2018;9(3):139–144. doi:10.4103/picr.PICR_81_17
9. Polonsky WH, Henry RR. Poor medication adherence in type 2 diabetes: recognizing the scope of the problem and its key contributors. Patient Prefer Adherence. 2016;10:1299–1307. doi:10.2147/PPA.S106821
10. Boye KS, Mody R, Lage MJ, Douglas S, Patel H. Chronic medication burden and complexity for US patients with type 2 diabetes treated with glucose-lowering agents. Diabetes Ther. 2020;11(7):1513–1525. doi:10.1007/s13300-020-00838-6
11. Tamene FB, Zeleke TK, Desalew AF, et al. Polypharmacy and associated factors among patients with type two diabetes mellitus with comorbidity: a multicenter cross-sectional study in Northwest Ethiopia. BMC Endocr Disord. 2025;25(1):188. doi:10.1186/s12902-025-02011-1
12. Alves-Conceição V, Rocha KSS, Silva FVN, Silva ROS, Silva DTD, Lyra-Jr DP. Medication regimen complexity measured by MRCI: a systematic review to identify health outcomes. Ann Pharmacother. 2018;52(11):1117–1134. doi:10.1177/1060028018773691
13. Ahmed S, Saif-Ur-Rahman KM, Dhungana RR, et al. Medication adherence and health-related quality of life among people with diabetes in Bangladesh: a cross-sectional study. Endocrinol Diabet Metab. 2023;6(5):e444. doi:10.1002/edm2.444
14. Hagger MS, Orbell S. The common sense model of illness self-regulation: a conceptual review and proposed extended model. Health Psychol Rev. 2022;16(3):347–377. doi:10.1080/17437199.2021.1878050
15. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
16. Liu M. Application of Colaizzi’s seven steps in phenomenological research data analysis. J Nurs. 2019;34(11):90–92. doi:10.3870/j.issn.1001-4152.2019.11.090
17. Rahimi S, Khatooni M. Saturation in qualitative research: an evolutionary concept analysis. Int J Nurs Stud Adv. 2024;6:100174. doi:10.1016/j.ijnsa.2024.100174
18. Wu J, Shen J, Tao Z, Song Z, Chen ZL. Self-efficacy as moderator and mediator between medication beliefs and adherence in elderly patients with type 2 diabetes. Patient Prefer Adherence. 2023;17:217–226. doi:10.2147/PPA.S382362
19. Alyafei A, Easton-Carr R. The health belief model of behavior change. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2024.
20. Alatawi YM, Kavookjian J, Ekong G, Alrayees MM. The association between health beliefs and medication adherence among patients with type 2 diabetes. Res Social Adm Pharm. 2016;12(6):914–925. doi:10.1016/j.sapharm.2015.11.006
21. Xie Z, Liu K, Or C, Chen J, Yan M, Wang H. An examination of the socio-demographic correlates of patient adherence to self-management behaviors and the mediating roles of health attitudes and self-efficacy among patients with coexisting type 2 diabetes and hypertension. BMC Public Health. 2020;20(1):1227. doi:10.1186/s12889-020-09274-4
22. Abdelhamid ZG, Abdel-Salam DM, Mohamed GA, El-Megeed HSA. Medication adherence and illness perception among diabetic patients in Upper Egypt. BMC Endocr Disord. 2025;25(1):223. doi:10.1186/s12902-025-01966-5
23. Bilondi SS, Noghabi AD, Aalami H. The relationship between illness perception and medication adherence in patients with diabetes mellitus type II: illness perception and medication adherence. J Prev Med Hyg. 2022;62(4):E966–E971. doi:10.15167/2421-4248/jpmh2021.62.4.2277
24. Curkendall SM, Thomas N, Bell KF, Juneau PL, Weiss AJ. Predictors of medication adherence in patients with type 2 diabetes mellitus. Curr Med Res Opin. 2013;29(10):1275–1286. doi:10.1185/03007995.2013.821056
25. Newbern VB. Application of self-regulation theory to the year of denouement for an insulin-dependent diabetic. Holist Nurs Pract. 1990;5(1):36–44. doi:10.1097/00004650-199010000-00010
26. Eitel KB, Pihoker C, Barrett CE, Roberts AJ. Diabetes stigma and clinical outcomes: an international review. J Endocr Soc. 2024;8(9):bvae136. doi:10.1210/jendso/bvae136
27. Bermeo-Cabrera J, Almeda-Valdes P, Riofrios-Palacios J, Aguilar-Salinas CA, Mehta R. Insulin adherence in type 2 diabetes in mexico: behaviors and barriers. J Diabetes Res. 2018;2018:3190849. doi:10.1155/2018/3190849
28. Verma M, Sidana S, Kumar P, et al. Distress and coping mechanisms among people with diabetes: cross-sectional assessment from an NCD screening clinic of a tertiary care hospital in North India. Diabetol Metab Syndr. 2025;17(1):34. doi:10.1186/s13098-025-01603-0
29. Chatoo A, Lee S. Association of coping strategies and medication adherence: a systematic review. Innov Pharm. 2022;13(3):10. doi:10.24926/iip.v13i3.4991
30. Mendes R, Martins S, Fernandes L. Adherence to medication, physical activity and diet in older adults with diabetes: its association with cognition, anxiety and depression. J Clin Med Res. 2019;11(8):583–592. doi:10.14740/jocmr3894
31. Acoba EF. Social support and mental health: the mediating role of perceived stress. Front Psychol. 2024;15:1330720. doi:10.3389/fpsyg.2024.1330720
32. Bouldin ED, Trivedi RB, Reiber GE, et al. Associations between having an informal caregiver, social support, and self-care among low-income adults with poorly controlled diabetes. Chronic Illn. 2017;13(4):239–250. doi:10.1177/1742395317690032
33. Olagbemide OJ, Omosanya OE, Ayodapo AO, Agboola SM, Adeagbo AO, Olukokun TA. Family support and medication adherence among adult type 2 diabetes: any meeting point? Ann Afr Med. 2021;20(4):282–287. doi:10.4103/aam.aam_62_20
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Development of Schematics to Illustrate Women’s Experiences with Adjuvant Hormone Therapy in the Treatment of Breast Cancer
AlOmeir O, Patel N, Donyai P
Patient Preference and Adherence 2022, 16:2639-2647
Published Date: 23 September 2022
Acne Comorbidities
Wang Y, Zhu M, Wu S, Zheng H
Clinical, Cosmetic and Investigational Dermatology 2022, 15:2415-2420
Published Date: 10 November 2022
Trends and Comparisons of Blood Pressure and Fasting Plasma Glucose in Patients with Hypertension, Diabetes, and Comorbidity: 4-Year Follow-Up Data
Xu L, Wen X, Yang Y, Cui D
Risk Management and Healthcare Policy 2022, 15:2221-2232
Published Date: 25 November 2022
Prevalence and Associated Factors of Diabetes Mellitus Among Newly Enrolled Tuberculosis Patients in Lubumbashi (DRC)
Kakisingi C, Mwamba C, Muteba MK, Kasamba E, Kabamba M, Tanon A, Situakibanza H
Risk Management and Healthcare Policy 2024, 17:171-180
Published Date: 17 January 2024
Perspectives of People with Type 2 Diabetes Mellitus Towards a Decision Aid Assessing Preferences of Glucose-Lowering Drugs: The Dilemma of Choosing
Roldan Munoz S, Mol PGM, de Vries F, van Dijk PR, Hillege H, Postmus D, de Vries ST
Patient Preference and Adherence 2025, 19:215-234
Published Date: 25 January 2025