")
Back to Journals » Drug Design, Development and Therapy » Volume 16
Platelet Rich Plasma and Its Use in Hair Regrowth: A Review
Authors Paichitrojjana A , Paichitrojjana A
Received 2 January 2022
Accepted for publication 4 March 2022
Published 10 March 2022 Volume 2022:16 Pages 635—645
DOI https://doi.org/10.2147/DDDT.S356858
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Tuo Deng
Anon Paichitrojjana,1 Anand Paichitrojjana2
1School of Anti-Aging and Regenerative Medicine, Mae Fah Luang University, Bangkok, Thailand; 2Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok, Thailand
Correspondence: Anon Paichitrojjana, School of Anti-Aging and Regenerative Medicine, Mae Fah Luang University, 36/87-88 PS Tower 25Fl, Asoke Road, Sukhumvit 21, Klong Toey Nua, Wattana, Bangkok, 10110, Thailand, Tel +66 81-9343050, Email [email protected]
Abstract: Platelet rich plasma (PRP) was described as a small volume of plasma containing higher concentrations of platelets than those found in peripheral blood and initially used as a transfusion product for treatment of thrombocytopenia. To date, it was discovered that there are several growth factors and cytokines that can accelerate wound healing and tissue regeneration, leading to a wider range of applications in the medical field, such as in sport medicine, regenerative medicine, and aesthetic medicine. Several studies have shown that PRP can be used effectively for treatment of hair loss. Although it has been widely used, the exact mechanism of action of PRP is still not fully elucidated. In this article, we aim to review and update current information on the definition, classification, mechanism of action, clinical efficacy in hair regrowth, and adverse events of PRP.
Keywords: platelet rich plasma, androgenetic alopecia, female pattern hair loss, alopecia areata, cicatricial alopecia, hair transplantation
Introduction
Platelet rich plasma (PRP) was first described in Hematology as a small volume of plasma containing higher concentrations of platelets than those found in peripheral blood and initially used as a transfusion product for treatment of thrombocytopenia since 1970.1 Nowadays, PRP has become a popular treatment for many conditions in sport medicine,2 regenerative medicine,2,3 aesthetic medicine4 and hair loss treatment5,6 as it contains a variety number of growth factors and cytokines that can accelerate wound healing and tissue restoration. Both the device used to separate platelets and the subsequent use of the PRP product fall under the regulation of the US Food and Drug Administration (FDA).7 Any use of PRP other than blood transfusion is an “off label use” which is not prohibited by the FDA regulation if performed by a physician with the intent to practice medicine. Despite its widely application, the mechanism underlying the hair regrowth effects of PRP remains to be fully explored. We aim to review the effectiveness of PRP as a treatment for hair loss including definition, classification, mechanism of action, clinical efficacy in hair regrowth, and adverse effects.
Definition
Platelet-rich plasma, also known as platelet-rich growth factors or platelet concentrate, is a concentrate of platelet-rich plasma protein derived from whole blood, centrifuged to remove red blood cells. In addition to the main component that contains high concentrations of platelets, there are also other components, such as, the presence or absence of leucocytes and platelet-activating agents, which used to define different types of PRP. The effectiveness of stimulating tissue regeneration depends on the concentration of platelets present in the plasma, several studies have shown that concentrations two to six times higher than normal platelet count is required for optimal outcomes.8
Preparation
Due to the lack of a standardized method of preparation and application of PRP, there is a wide variety method of preparation. However, the main principle is to prepare concentrated platelets from the patient’s own blood. All PRP preparation protocols follow a generic method, started with collecting venous blood approximately 10 to 60 mL from the patient and placing it into tubes containing an Anticoagulant, either acid citrate dextrose or sodium citrate solution to prevent coagulation and premature secretion of the alpha granules. Subsequently, whole blood is centrifuged and divided into 3 layers based on specific gravity, the bottom layer contains red blood cells (RBCs) with leukocytes the middle layer is the PRP, and the top layer is platelet-poor plasma (PPP).9 There are several types of commercial PRP kits that simplify the PRP preparation. These kits differed in platelet concentrations, the presence of leukocytes and platelet activator leading to the diversity of growth factors concentration. All of these explain the variability in the clinical benefits of PRP reported in the literature. Some studies induced growth factor secretion and degradation of alpha granules by adding calcium gluconate, calcium chloride, or thrombin before administration (activated PRP). There is no consensus as to whether platelets must be activated exogenously or use host thrombin as endogenous activator in order to maximize the therapeutic effect.10–12 The platelet alpha granules secrete growth factors within 10 minutes after clotting or activation, so PRP should be used within 10 minutes of activation for maximum benefits.13
Classification of Platelet Rich Plasma
There are many variations in PRP preparations, from the type of collection tubes, power used, the number of cycles and the duration of centrifugation, components of PRP and an activation method was applied. A standardized classification of PRP called DEPA was proposed by Magalon et al, based on four components: dose of injected platelets (baseline concentration of platelets at 200×109/L), efficiency of the process (platelet recovery rate %), purity of PRP (relative composition in platelets %) and activation process,14 as shown in Table 1. From this classification, an “AAA” DEPA score is referred to a high-concentration platelet injection (>5 billion) with minimal red blood cell contamination and well prepared with a proper method resulting in minor loss of platelets from whole blood. The last category in the DEPA classification is reporting the presence or absence of any exogenous activator, such as thrombin or calcium chloride.
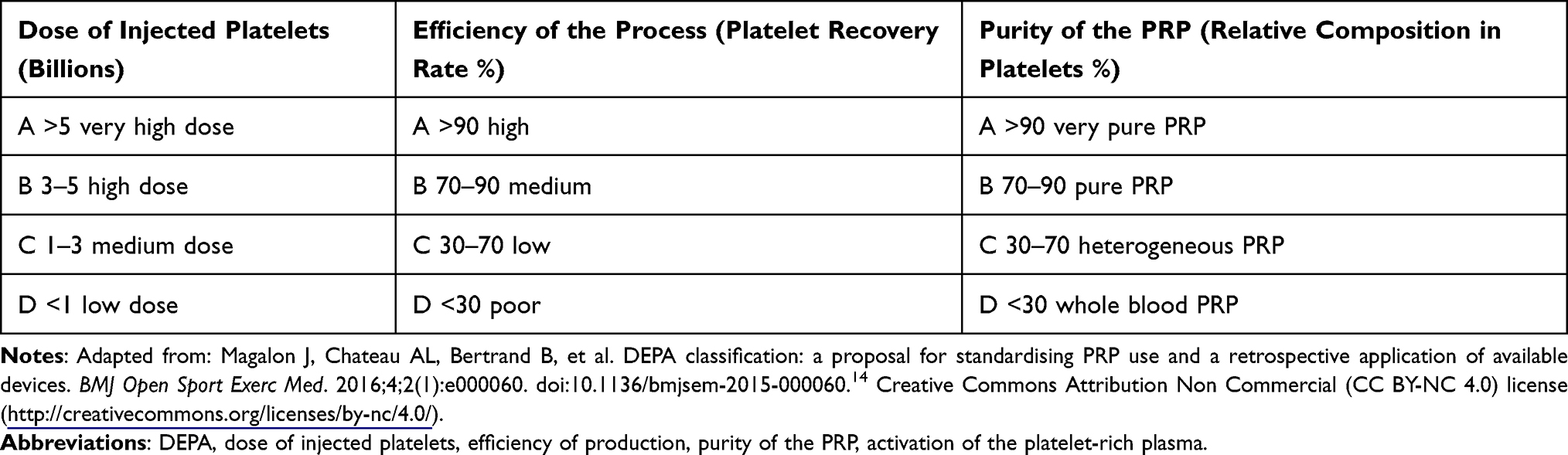 |
Table 1 DEPA Score is Categorized in Order from A to D |
Mechanism of Action
Currently, many studies have demonstrated that platelets not only affect hemostatic system, but also affect inflammatory system, angiogenesis, stem cell induction, and cell proliferation through the release of many different growth factors and cytokines.15–17 Activated platelets in PRP release numerous growth factors and cytokines from their alpha granules, including platelet-derived endothelial growth factor (PDGF), transforming growth factor β (TGF-β), fibroblast growth factor-2 (FGF-2), vascular endothelial growth factor (VEGF), epidermal growth factor (EGF), insulin-like growth factor-1 (IGF-1), glial cell line–derived neurotrophic factor (GDNF), which play a major role in stimulating hair growth through cell proliferation, differentiation and angiogenesis.18–22 GDNF can stimulate cell proliferation and protect hair follicle from premature catagen transition.23,24 VEGF play a major role as a potent hair growth stimulator via an angiogenesis induction.25,26 While IGF-1 stimulates proliferation of cycling Ki67+ basal keratinocytes, induce and prolong the anagen phase of the hair growth cycle.27–29 In addition, PRP can induce the proliferation of dermal papilla (DP) cells by activating extracellular signal-related kinase (ERK), fibroblast growth factor 7 (FGF-7), beta-catenin, and Akt signaling (an anti-apoptotic signaling molecule). There is also an increase in expression of Bcl-2 protein (an anti-apoptotic protein) in vitro human dermal papilla cells cultured with PRP. Thus, it was clearly illustrated that PRP can increase the survival of hair follicle cells through anti-apoptotic effects and stimulate hair growth by extending the anagen phase of the hair cycle.30 This theory was further supported by the results of microscopic examination which demonstrated an increase in number of follicular bulge cells, hair follicles, epidermal thickening, vascularization, and a higher number of Ki67+ basal keratinocytes in PRP-treated scalp tissue compared with placebo.31
Contraindication
Although PRP is a safe treatment with minimal side effects, there are some contraindications that need to be considered. Absolute contraindication for PRP include critical thrombocytopenia, platelet dysfunction, hemodynamic instability, sepsis, local infection (site PRP) and patient with unwilling to accept risk. Relative contraindications include NSAIDs use in 48 hours, glucocorticoid injection at treatment site within one-month, systemic glucocorticoid within 2 weeks, recent illness or fever, cancer especially bone or hematolymphoid, anemia (hemoglobin less than 10 grams per deciliter), thrombocytopenia (platelets less than 150,000 per microliter) and tobacco use.32
Use of Platelet Rich Plasma in Hair Disorders
Androgenetic Alopecia
Androgenetic alopecia (AGA) is a non-scarring alopecia characterized by a shortened anagen phase and progressive miniaturization of terminal hairs into vellus hairs.33 This condition is found in approximately 50% of Caucasian men by the age of 50 years, and in women, it can be as much as 50% over the course of their lifetime.34 In men, baldness started with frontal recession and thinning of hair on vertex area (MPHL), while in women, hair loss is characterized by less hair density and smaller hair shaft diameter over the crown without frontal hairline recessions (FPHL). FDA has approved oral finasteride (for men only) and topical minoxidil for the treatment of AGA.35
A meta-analysis from six studies (four studies were randomized controlled trials, while the other two were retrospective studies) involving 177 patients, showed a significant increase in number of hairs per cm2 after PRP injections compared to control (mean difference (MD) 17.90, 95% CI 5.84–29.95, P=0.004) and the tendency to increase in number of hairs and the percentage of hair thickness.36 Similar result was confirmed by another two meta-analysis studies which showed a significantly increased hair numbers per cm2 after PRP injections in the treatment group versus the control group with MD 38.75, 95% CI 22.22–55.28, P <0.00001 and MD 30.35, 95% CI 1.77–58.93, P <0.00001, respectively.37,38 Compared to minoxidil, finasteride, and adult stem cell-based therapy, 84% of all studies reported a positive effect of PRP, 50% demonstrated a statistically significant improvement while 34% showed hair density and hair thickness improvement, although no P values or statistical analysis was described.39
Despite several clinical trials showed the success of PRP therapy in AGA, there is no standard practice for PRP preparation and administration as well as a method to evaluate results. Attempts have been made to standardize PRP treatment for AGA patients. A standard PRP procedure was proposed by Stevens et al, employing a single spin centrifugation method to produce pure PRP with a platelet enrichment of 3 to 6 times the mean concentration of whole blood and adding a platelet activator such as calcium chloride or calcium gluconate before administration of PRP as subdermal injections. Treatment intervals should include monthly sessions for the first 3 months, then every 3 months for the first year.27
However, there is still debate in the literature about the standardization of PRP preparation. A split scalp prospective comparative clinical study included 15 females with AGA was performed by intradermal injection of double-spin prepared PRP into the right half of the scalp and single-spin prepared PRP into the left half of the scalp of each patient for three treatment sessions, 3 weeks apart. Results showed clinical improvement in both sides of scalp while hair density measured by trichoscan revealed that the right half of the scalp was significantly higher in median terminal hair density than the left half (P = 0.031), which illustrated that double-spin method could yield better results than single-spin method.40 In addition, there was a comparative study demonstrated that patients treated with non-activated PRP were found to have greater increase in hair count and total hair density (31% ± 2% versus 19% ± 3%, P= 0.0029) than patients treated with activated-PRP, leading to the conclusion that PRP does not require activation before injection.31
The important factors that affect the effectiveness of PRP is the number of platelets. Higher numbers of platelets have a greater effect than lower numbers of platelets in terms of hair density, follicle diameter, and terminal hair density.41 In AGA, action of dihydrotestosterone on dermal papilla cells suppressed canonical WNT signaling, resulting in defective hair growth and retarding hair cycling. PRP promoting hair growth by activating WNT/β-Catenin signaling lead to proliferation and differentiation of hair follicle cells and triggering new hair cycle.42
Some studies have reported ineffectiveness of PRP in AGA treatment, which may be caused by low platelet concentration, low volume of PRP injected, and inadequate frequency of treatment.9 The treatment response to PRP in AGA patients can be predicted by measuring pro-inflammatory cytokine IL-1α polymorphism from peripheral blood. A study has reported significantly higher frequency of C/C genotype of IL-1α in responder (66%) than in non-responder patients (22%) with odds ratio (OR) 6.68, 95% CI 0.99–72.95 (p<0.05).43
Evidence from randomized controlled trials of PRP in AGA is summarized in Table 2.
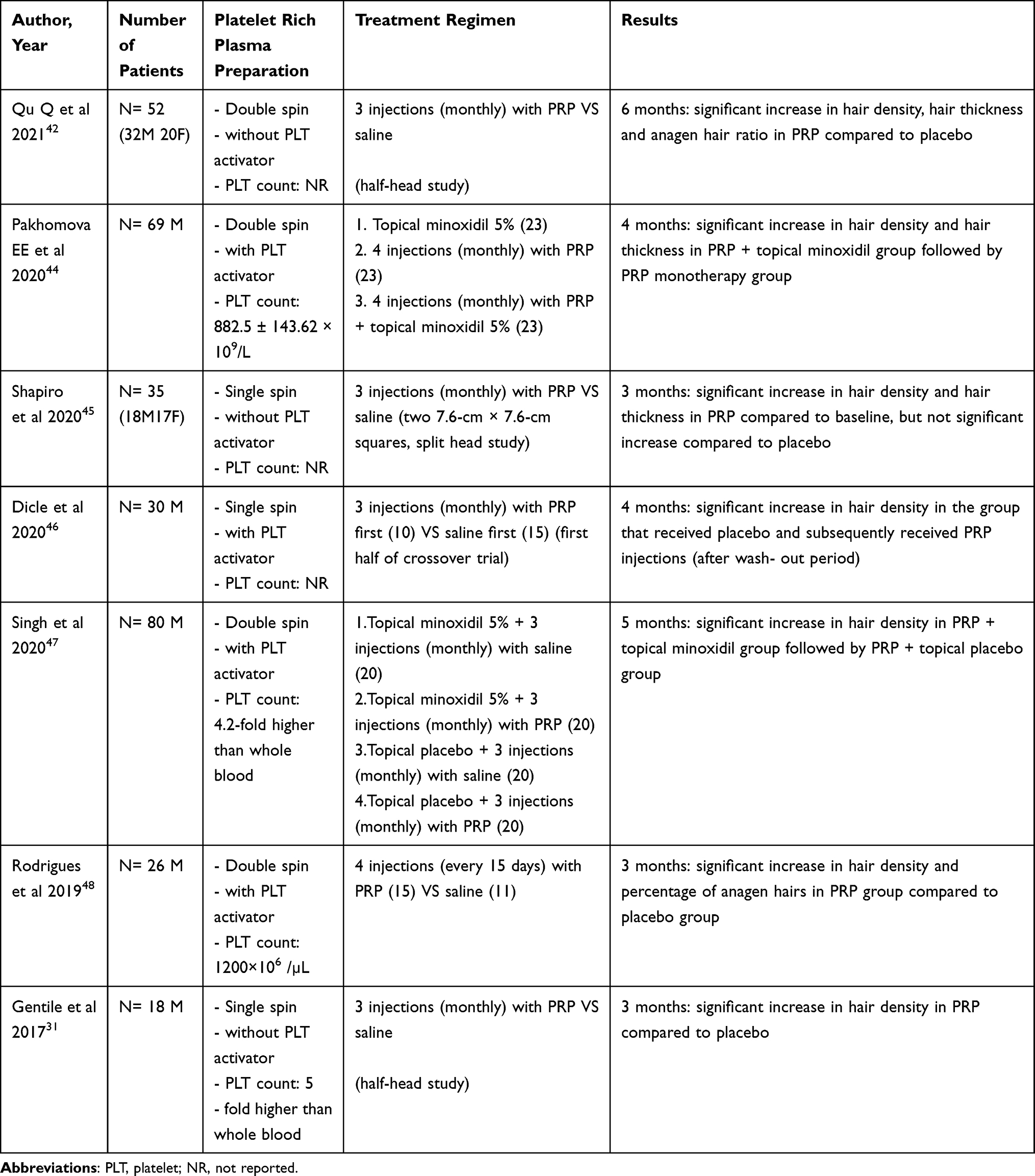 |
Table 2 Randomized Controlled Trials of PRP in Male Androgenic Alopecia |
Female Pattern Hair Loss
Female pattern hair loss (FPHL) is the most common cause of hair loss in middle-aged women, characterized by progressive follicular miniaturization and conversion of terminal follicles into vellus-like follicles, leading to a decrease in hair density, thinning of hair and diffuse non scarring alopecia especially in the central, frontal and parietal regions of the scalp. The cause of this problem is unknown, but it is related to genetics, hormones, and environmental conditions.49
A systemic review study evaluating the efficacy of PRP in the treatment of FPHL comprising 92 patients from 6 randomized controlled clinical trials showed that PRP has a positive effect on FPHL treatment by increasing hair thickness and hair density.50 Recently, two meta-analysis studies have confirmed the efficacy of FPHL treatment with PRP. The first study consisted of 776 female participants covering 16 randomized controlled trials and 26 observational trials, demonstrated that PRP has a good therapeutic effect on FPHL in hair density compared to the control groups with OR 1.61, 95% CI 0.52–2.70, and compared to baseline with OR 1.11, 95% CI 0.86–1.37.51 The second study from 8 clinical studies and a total of 197 subjects showed a significant increase in hair count and hair diameter in 4 studies after PRP treatment. Moreover, PRP has been shown to produce high levels of satisfaction and improvement in the quality of life in patients affected by FPHL.52
Differences in the treatment efficacy for AGA with PRP between men and women was discovered by a meta-analysis study, which revealed that PRP significantly increased both hair density (N = 250, MD = 25.83, 95% CI: 15.48–36.17, P < 0.00001) and hair diameter (N = 123, MD = 6.66, 95% CI: 2.37–10.95, P = 0.002) in men while significantly increased hair diameter (N = 95, MD = 31.22, 95% CI: 7.52–54.91, P = 0.01), but did not increase hair density (N = 92, MD = 43.54, 95% CI: −1.35–88.43, P = 0.06) in women.53 However, PRP effectiveness in the treatment of AGA is influenced by gender is still controversial because of the differences in several reports listed, many of the analyzed studies were non-randomized, uncontrolled, and had small sample size.
Evidence from randomized controlled trials of PRP in FPHL is summarized in Table 3.
 |
Table 3 Randomized Controlled Trials of PRP in Female Pattern Hair Loss |
Alopecia Areata
Alopecia areata (AA) is a common autoimmune disorder that causes nonscarring alopecia in males and females at any age. The estimated lifetime risk of AA is around 2% of population, with no difference in incidence between genders. Most patients have only one lesion of alopecia and spontaneous hair regrowth can occur within months to years. However, there are many patients who may develop multiple lesions and turn into chronic hair loss.58
PRP was discovered to have a potent anti-inflammatory effect. It suppresses cytokine release and decreases local tissue inflammation, which makes PRP potentially beneficial in treating inflammatory hair loss such as AA.59,60 PRP was initially tested in patients with AA by a randomized, double-blind, placebo controlled, half-head study. Forty-five patients with AA were randomized to receive intralesional injections of PRP or triamcinolone acetonide or placebo on one half of their scalp, while the other half was untreated. The results showed that PRP significantly increased hair regrowth and Ki-67 level (marker for cell proliferation) compared with triamcinolone acetonide or placebo injection.61 Collectively, many randomized controlled trials demonstrated that treatment with PRP can stimulate hair regrowth to the same extent as intralesional injection of triamcinolone acetonide in the treatment of AA.62–65 Two recent studies compared the therapeutic effect of intralesional injections of PRP with triamcinolone acetonide in AA. One study found that final severity of alopecia tool (SALT) score showed significant lower levels in both groups compared to baseline levels (P = 0.025 and P = 0.008) with no significant difference between both treatment modalities in term of clinical improvement, while final alopecia areata symptom impact scale (AASIS) showed significant decrease in PRP group (P = 0.006) but not in triamcinolone group (P = 0.062).62 Similar results were found in the other study by showing that there was no statistically significant difference in SALT score reduction and hair regrowth scale between these two groups.63
On the contrary, different results were found in three randomized controlled clinical trials which demonstrated that PRP was significantly less effective than intralesional steroid injection based on Mac Donald Hull and Norris grading system, percentage of hair regrowth and reduction in SALT score from baseline, respectively.66–68 All these results could explain that steroid is more potent than PRP in terms of having immunosuppressive and strong inhibitory effect on T lymphocyte activation.
A beneficial effect of combination therapy with PRP was reported in a patient with long standing AA treated with a combination of intralesional injection of triamcinolone acetonide and PRP in one half of the scalp while the other half of the scalp was treated with intralesional triamcinolone acetonide only. The half head treated with the combined therapy showed greater hair regrowth and larger hair fiber diameter.69 Furthermore, there was a prospective study on the efficacy of PRP treatment in 20 cases of chronic AA who had not responded to conventional therapy for 2 years, demonstrated that all patients with chronic AA were successfully treated with PRP, only one patient had a relapse after one year of follow-up.70 The successful treatment with PRP was also reported in a patient with corticosteroid-resistant ophiasis AA who experienced hair regrowth after PRP injections71 and a patient who suffering from alopecia areata barbae.72 Hence, PRP can be used as an alternative therapy in patients unresponsive to conventional therapy or patients who do not want to be treated with steroids and can also be used as an adjuvant therapy for alopecia areata.
Evidence from randomized controlled trials of PRP in AA is summarized in Table 4.
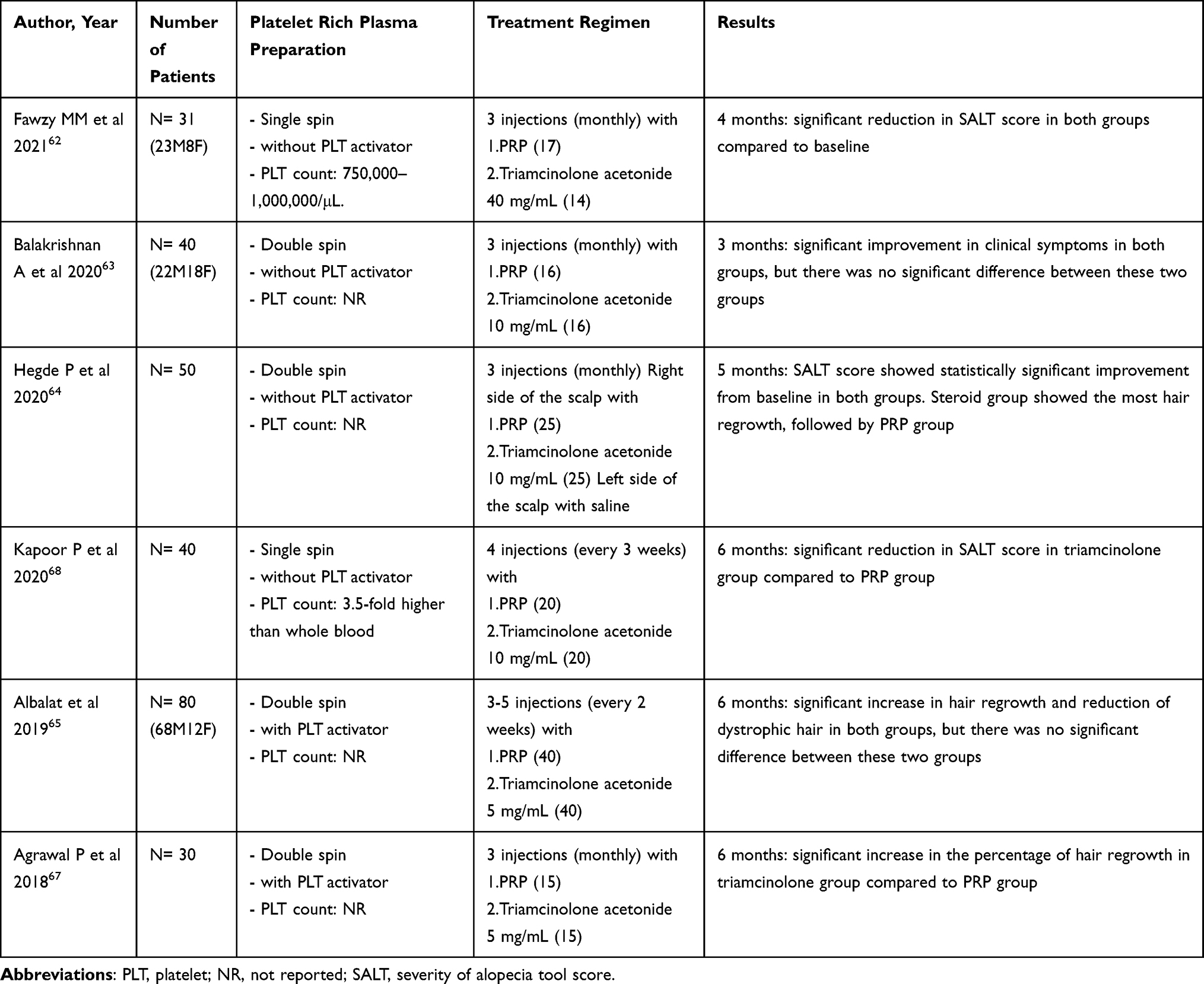 |
Table 4 Randomized Controlled Trials of PRP in Alopecia Areata |
Cicatricial Alopecia
Cicatricial alopecia is a type of scarring alopecia, caused by different inflammatory conditions, physical trauma, burn, or severe infections that lead to the destruction of the hair follicles and subsequent scarring. The goal of treatment is to stop the disease progression, prevent further hair loss and scarring by using different anti-inflammatory drugs, such as topical steroid, intralesional triamcinolone acetonide injection and immunomodulating agents. However, there is no effective treatment to stimulate hair regrowth in fibrotic area.73
Frontal fibrosing alopecia (FFA), a variant of lichen planopilaris, is currently the most common type of cicatricial alopecia characterized by progressive recession of the frontal and temporoparietal hairline along with perifollicular erythema and papules leading to band-shaped scarring alopecia in the frontotemporal area.74 The satisfactory treatment outcome with five consecutive PRP injections was reported in a 44-year-old female with FFA, who had a history of unresponsive to conventional intralesional steroid therapy. Only one month after treatment, perifollicular erythema, scaling, and lichenoid papules on the frontotemporal hairline were improved, and no further hair loss was seen after 5 months.75
Lichen planopilaris (LPP) is a chronic inflammatory scarring alopecia characterized by follicular hyperkeratosis, perifollicular erythema, and loss of follicular orifices on vertex and parietal area of the scalp. Bolanča et al have reported for the first time the efficacy of PRP therapy in a case of LPP diagnosed by histopathology and unresponsive to any previous treatments. After 3 consecutive treatments of PRP and followed up for 6 months, patients experienced complete regression of scalp itching and hair shedding, confirmed by undetectable perifollicular erythema and scaling on trichoscopic examination.76 Subsequently, two patients with central centrifugal cicatricial alopecia (CCCA) and one patient with LPP were reported on the success of PRP treatment, resulting in a significant increase in hair density despite a history of unresponsiveness to conventional therapy before.77,78
Effective treatment of cicatricial alopecia with PRP is possible due to various cytokines and growth factors such as TGFβ, TGFβ1 in platelet granules, which have anti-inflammatory and proangiogenic effects.79 Although there is evidence that PRP can be used as an effective treatment for some types of cicatricial alopecia, more clinical trials are needed to produce further evidence.
Hair Transplantation
Several studies have shown a beneficial effect of using PRP in combination with hair transplantation. The first report was an experimental study in a group of 20 patients with male pattern baldness demonstrated a 15% greater hair yield in follicular unit density in areas pretreated the harvested donor with platelet plasma growth factors obtained from the patient’s autologous plasma as compared with normal saline (18.7 follicular units per cm2 vs 16.4 follicular units per cm2).22 Similar results were found in another two studies, the first was a comparative study showed that transplanted follicular unit grafts in conjunction with platelet lysate (PL) or activated PRP (AA–PRP) resume growth faster than normal saline at 4 months after operation, 99%, 75%, and 71% of follicle regeneration had occurred in the PL, AA–PRP, and saline treatment areas, respectively.80 The second was a randomized controlled study demonstrated that preserving hair grafts in PRP before implantation enhances the hair density, the graft uptake, and the hair thickness compared with preserving in normal saline.81
Furthermore, PRP can also be used as a combination treatment with the follicular unit extraction (FUE) hair transplantation as shown in a single-blind, prospective randomized study in 40 FUE hair transplant patients. The patients were divided into two groups, PRP was injected intra-operatively immediately after creating slits over the recipient area in PRP group while normal saline was injected in non-PRP group. It was clearly seen that intra-operative PRP therapy is profitable in giving significantly improved density and quality of hair growth, reducing the catagen loss of transplanted hair, early recovery of the skin and faster appearance of new anagen hair in FUE transplant patients.82 Thus, PRP is not only an effective hair loss treatment, but it can also be used as an adjunct to hair transplantation.
Adverse Effects of Platelet Rich Plasma
PRP is an autologous preparation of plasma with a high concentration of platelets. It is relatively safe intervention with minimal adverse effects, including temporary and tolerable pain during treatment, mild headache, minimal itching, transient erythema and edema on treated area. No major side effects such as scarring, infections, panniculitis, hematoma or allergic reaction have been documented following PRP treatment.39,83,84 After treatment, patients can resume normal daily activities, no antibiotics are needed to prevent infection. Most patients can return to work the following day.
Conclusion
PRP can be used as a new therapeutic option for hair loss including androgenetic alopecia and female pattern hair loss, either as a monotherapy or an adjuvant to conventional therapy or hair transplantation. PRP is also considered a safe, effective, steroid sparing, and alternative treatment for alopecia areata. Moreover, there was evidence showing that PRP can improve clinical symptoms in some types of cicatricial alopecia. However, further studies are needed to determine the standard of PRP treatment preparation, treatment regimen, including dosing protocols, injection technique, number and interval of optimal treatment sessions in order to achieve the maximum therapeutic efficiency.
Data Sharing Statement
The reader can personally request to access the data via Dr. Anon Paichitrojjana; E-mail: [email protected].
Acknowledgments
The authors would like to thank the School of AntiAging and Regenerative Medicine, Mae Fah Luang University for research facilities.
Funding
This study did not receive any funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Matras H. Effect of various fibrin preparations on reimplantation in the rat skin. Osterr Z Stomatol. 1970;67(9):338–359.
2. Sclafani AP, Azzi J. Platelet preparations for use in facial rejuvenation and wound healing: a critical review of current literature. Aesthetic Plast Surg. 2015;39(4):495–505. doi:10.1007/s00266-015-0504-x
3. Marx RE, Carlson ER, Eichstaedt RM, et al. Platelet rich plasma: growth factor enhancement for bone grafts. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1998;85:638–646. doi:10.1016/s1079-2104(98)90029-4
4. Sand JP, Nabili V, Kochhar A, et al. Platelet-rich plasma for the aesthetic surgeon. Facial Plast Surg. 2017;33(04):437–443. doi:10.1055/s-0037-1604240
5. Kang J-S, Zheng Z, Choi MJ, et al. The effect of CD341 cell-containing autologous platelet-rich plasma injection on pattern hair loss: a preliminary study. J Eur Acad Dermatol Venereol. 2014;28(1):72–79. doi:10.1111/jdv.12062
6. JusticzN, DerakhshanA, ChenJX, et al.Platelet-rich plasma for hair restoration.Facial Plas Surg Clin North Am. 2020;28(2):181–187. doi:10.1016/j.fsc.2020.01.009
7. Beitzel K, Allen D, Apostolakos J, et al. US definitions, current use, and FDA stance on use of platelet-rich plasma in sports medicine. J Knee Surg. 2015;28(1):29–34. doi:10.1055/s-0034-1390030
8. Weibrich G, Hansen T, Kleis W, et al. Effect of platelet concentration in platelet-rich plasma on peri-implant bone regeneration. Bone. 2004;34(4):665–671. doi:10.1016/j.bone.2003.12.010
9. Gupta AK, Renaud HJ, Rapaport JA. Platelet-rich plasma and cell therapy the new horizon in hair loss treatment. Dermatol Clin. 2021;39(3):429–445. doi:10.1016/j.det.2021.04.001
10. Wroblewski AP, Melia HJ, Wright VJ. Application of platelet-rich plasma to enhance tissue repair. Oper Tech Orthop. 2010;20:98–105. doi:10.1080/14787210.2021.1858801
11. Dhurat R, Sukesh MS. Principles and methods of preparation of platelet-rich plasma: a review and author’s perspective. J Cutan Aesthet Surg. 2014;7(4):189–197. doi:10.4103/0974-2077.150734
12. Leo MS, Kumar AS, Kirit R, et al. Systematic review of the use of platelet-rich plasma in aesthetic dermatology. J Cosmet Dermatol. 2015;14:315–323. doi:10.4103/0974-2077.150734
13. Cole B, Seroyer S, Filardo G, Bajaj S, Fortier LA. Platelet-rich plasma: where are we now and where are we going? Sports Health. 2010;2(3):203–210. doi:10.1177/1941738110366385
14. Magalon J, Chateau AL, Bertrand B, et al. DEPA classification: a proposal for standardising PRP use and a retrospective application of available devices. BMJ Open Sport Exerc Med. 2016;2(1):e000060. doi:10.1136/bmjsem-2015-000060
15. Alves R, Grimalt R. A review of platelet-rich plasma: history, biology, mechanism of action, and classification. Skin Appendage Disord. 2018;4(1):18–24. doi:10.1159/000477353
16. Xu P, Wu Y, Zhou L, et al. Platelet-rich plasma accelerates skin wound healing by promoting re-epithelialization. Burns Trauma. 2020;8:tkaa028. doi:10.1093/burnst/tkaa028
17. Sakata R, Reddi AH. Platelet-rich plasma modulates actions on articular cartilage lubrication and regeneration. Tissue Eng Part B Rev. 2016;22(5):408–419. doi:10.1089/ten.TEB.2015.0534
18. Siah TW, Guo H, Chu T, et al. Growth factor concentrations in platelet-rich plasma for androgenetic alopecia: an intra-subject, randomized, blinded, placebo-controlled, pilot study. Exp Dermatol. 2020;29(3):334–340. doi:10.1111/exd.14074
19. Gupta AK, Carviel J. A mechanistic Model of platelet-rich plasma treatment for androgenetic alopecia. Dermatol Surg. 2016;42(12):1335–1339. doi:10.1097/DSS.0000000000000901
20. Hom DB, Maisel RH. Angiogenic growth factors: their effects and potential in soft tissue wound healing. Ann Otol Rhinol Laryngol. 1992;101(4):349–354. doi:10.1177/000348949210100411
21. Kim DH, Je YJ, Kim CD, et al. Can platelet-rich plasma be used for skin rejuvenation? Evaluation of effects of platelet-rich plasma on human dermal fibroblast. Ann Dermatol. 2011;23(4):424–431. doi:10.5021/ad.2011.23.4.424
22. Uebel CO, da Silva JB, Cantarelli D, et al. The role of platelet plasma growth factors in male pattern baldness surgery. Plast Reconstr Surg. 2006;118(6):1458–1466. doi:10.1097/01.prs.0000239560.29172.33
23. Botchkareva NV, Botchkarev VA, Welker P, et al. New roles for glial cell line-derived neurotrophic factor and neurturin: involvement in hair cycle control. Am J Pathol. 2000;156(3):1041–1053. doi:10.1016/S0002-9440(10)64972-3
24. Adly MA, Assaf HA, Pertile P, et al. Expression patterns of the glial cell line-derived neurotrophic factor, neurturin, their cognate receptors GFRalpha-1, GFRalpha-2, and a common signal transduction element c-Ret in the human skin hair follicles. J Am Acad Dermatol. 2008;58(2):238–250. doi:10.1016/j.jaad.2007.10.014
25. Yano K, Brown LF, Detmar M. Control of hair growth and follicle size by VEGF-mediated angiogenesis. J Clin Invest. 2001;107(4):409–417. doi:10.1172/JCI11317
26. Ozeki M, Tabata Y. Promoted growth of murine hair follicles through controlled release of vascular endothelial growth factor. Biomaterials. 2002;23(11):2367–2373. doi:10.1016/s0142-9612(01)00372-6
27. Stevens J, Khetarpal S. Platelet-rich plasma for androgenetic alopecia: a review of the literature and proposed treatment protocol. Int J Womens Dermatol. 2018;5(1):46–51. doi:10.1016/j.ijwd.2018.08.004
28. Hodak E, Gottlieb AB, Anzilotti M, et al. The insulin-like growth factor 1 receptor is expressed by epithelial cells with proliferative potential in human epidermis and skin appendages: correlation of increased expression with epidermal hyperplasia. J Investig Dermatol. 1996;106:564–570. doi:10.1111/1523-1747.ep12344044
29. Ristow HJ, Messmer TO. Basic fibroblast growth-factor and insulin-like growth factor-I are strong mitogens for cultured mouse keratinocytes. J Cell Physiol. 1988;137:277–284. doi:10.1002/jcp.1041370210
30. Li ZJ, Choi HI, Choi DK, et al. Autologous platelet-rich plasma: a potential therapeutic tool for promoting hair growth. Dermatol Surg. 2012;38(7 Pt 1):1040–1046. doi:10.1111/j.1524-4725.2012.02394
31. Gentile P, Cole JP, Cole MA, et al. Evaluation of not-activated and activated PRP in hair loss treatment: role of growth factor and cytokine concentrations obtained by different collection systems. Int J Mol Sci. 2017;18(2). doi:10.3390/ijms18020408
32. Hesseler MJ, Shyam N. Platelet-rich plasma and its utilities in alopecia: a systematic review. Dermatol Surg. 2020;46(1):93–102. doi:10.1097/DSS.0000000000001965
33. Blumeyer A, Tosti A, Messenger A, et al. Evidence-based (S3) guideline for the treatment of androgenetic alopecia in women and in men. J Dtsch Dermatol Ges. 2011;9:S1–S57. doi:10.1111/j.1610-0379.2011.07802
34. Rogers NE, Avram MR. Medical treatments for male and female pattern hair loss. J Am Acad Dermatol. 2008;59:
35. Lee SW, Juhasz M, Mobasher P, et al. A systematic review of topical finasteride in the treatment of androgenetic alopecia in men and women. J Drugs Dermatol. 2018;17(4):457–463.
36. Giordano S, Romeo M, Lankinen P. Platelet-rich plasma for androgenetic alopecia: does it work? Evidence from meta analysis. J Cosmet Dermatol. 2017;16(3):374–381. doi:10.1111/jocd.12331
37. Mao G, Zhang G, Platelet-Rich FW. Plasma for treating androgenic alopecia: a systematic review. Aesthetic Plast Surg. 2019;43(5):1326–1336. doi:10.1007/s00266-019-01391-9
38. Dervishi G, Liu H, Peternel S, et al. Autologous platelet-rich plasma therapy for pattern hair loss: a systematic review. J Cosmet Dermatol. 2020;19(4):827–835. doi:10.1111/jocd.13113
39. Gentile P, Garcovich S. Systematic review of platelet-rich plasma use in androgenetic alopecia compared with Minoxidil®, Finasteride®, and adult stem cell-based therapy. Int J Mol Sci. 2020;21(8):2702. doi:10.3390/ijms21082702
40. El-Husseiny RM, Saleh HM, Moustafa AA, et al. Comparison between single- versus double-spin prepared platelet-rich plasma injection in treatment of female pattern hair loss: clinical effect and relation to vascular endothelial growth factor. Arch Dermatol Res. 2021;313(7):557–566. doi:10.1007/s00403-020-02134-6
41. Sasaki GH. The effects of lower vs higher cell number of Platelet-Rich Plasma (PRP) on hair density and diameter in Androgenetic Alopecia (AGA): a randomized, double-blinded, placebo, parallel-group half-scalp IRB-approved study. Aesthet Surg J. 2021;41(11):NP1659–NP1672. doi:10.1093/asj/sjab236
42. Qu Q, Zhou Y, Shi P, et al. Platelet-rich plasma for androgenic alopecia: a randomized, placebo-controlled, double-blind study and combined mice model experiment. J Cosmet Dermatol. 2021;20(10):3227–3235. doi:10.1111/jocd.14089
43. Rossano F, Di Martino S, Iodice L, et al. Correlation between individual inflammation genetic profile and platelet rich plasma efficacy in hair follicle regeneration: a pilot study reveals prognostic value of IL-1α polymorphism. Eur Rev Med Pharmacol Sci. 2017;21(22):5247–5257. doi:10.26355/eurrev_201711_13848
44. Pakhomova EE, Smirnova IO. Comparative evaluation of the clinical efficacy of PRP-therapy, minoxidil, and their combination with immunohistochemical study of the dynamics of cell proliferation in the treatment of men with androgenetic alopecia. Int J Mol Sci. 2020;21(18):6516. doi:10.3390/ijms21186516
45. Shapiro J, Ho A, Sukhdeo K, et al. Evaluation of platelet-rich plasma as a treatment for androgenetic alopecia: a randomized controlled trial. J Am Acad Dermatol. 2020;83(5):1298–1303. doi:10.1016/j.jaad.2020.07.006
46. Dicle O, Bilgic Temel A, Gu¨lkesen KH. Platelet-rich plasma injections in the treatment of male androgenetic alopecia: a randomized placebo-controlled crossover study. J Cosmet Dermatol. 2020;19(5):1071–1077. doi:10.1111/jocd.13146
47. Singh SK, Kumar V, Rai T. Comparison of efficacy of platelet-rich plasma therapy with or without topical 5% minoxidil in male-type baldness: a randomized, double-blind placebo control trial. Indian J Dermatol Venereol Leprol. 2020;86(2):150–157. doi:10.4103/ijdvl.IJDVL_589_18
48. Rodrigues BL, Montalvão SA, Cancela RBB, et al. Treatment of male pattern alopecia with platelet-rich plasma: a double-blind controlled study with analysis of platelet number and growth factor levels. J Am Acad Dermatol. 2019;80(3):694–700. doi:10.1016/j.jaad.2018.09.033
49. Ramos PM, Miot HA. Female pattern hair loss: a clinical and pathophysiological review. An Bras Dermatol. 2015;90(4):529–543. doi:10.1590/abd1806-4841.20153370
50. Torabi P, Behrangi E, Goodarzi A, et al. A systematic review of the effect of platelet-rich plasma on androgenetic alopecia of women. Dermatol Ther. 2020;33(6):e13835. doi:10.1111/dth.13835
51. Zhou S, Qi F, Gong Y, et al. Platelet-rich plasma in female androgenic alopecia: a comprehensive systematic review and meta-analysis. Front Pharmacol. 2021;12:642980. doi:10.3389/fphar.2021.642980
52. Mercuri SR, Paolino G, Di Nicola MR, et al. Investigating the safety and efficacy of Platelet-Rich Plasma (PRP) treatment for female androgenetic alopecia: review of the literature. Medicina (Kaunas). 2021;57(4):311. doi:10.3390/medicina57040311
53. Gupta AK, Renaud HJ, Bamimore M. Platelet-rich plasma for androgenetic alopecia: efficacy differences between men and women. Dermatol Ther. 2020;33(6):e14143. doi:10.1111/dth.14143
54. Dubin DP, Lin MJ, Leight HM, et al. The effect of platelet-rich plasma on female androgenetic alopecia: a randomized controlled trial. J Am Acad Dermatol. 2020;83(5):1294–1297. doi:10.1016/j.jaad.2020.06.1021
55. Bruce AJ, Pincelli TP, Heckman MG, et al. A randomized, controlled pilot trial comparing platelet-rich plasma to topical minoxidil foam for treatment ofandrogenic alopecia in women. Dermatol Surg. 2020;46(6):826–832. doi:10.1097/DSS.0000000000002168
56. Tawfik AA, Osman MAR. The effect of autologous activated platelet-rich plasma injection on female pattern hair loss: a randomized placebo-controlled study. J Cosmet Dermatol. 2018;17:47–53. doi:10.1111/jocd.12357
57. Lee SH, Zheng Z, Kang JS, et al. Therapeutic efficacy of autologous platelet-rich plasma and polydeoxyribonucleotide on female pattern hair loss. Wound Repair Regen. 2015;23(1):30–36. doi:10.1111/wrr.12250
58. MadaniS, ShapiroJ.Alopecia areata update. J Am Acad Dermatol. 2000;42(4):
59. El-Sharkawy H, Kantarci A, Deady J, et al. Platelet-rich plasma: growth factors and pro- and anti-inflammatory properties. J Periodontol. 2007;78(4):661–669. doi:10.1902/jop.2007.060302
60. Pratt CH, King LE, Messenger AG, Christiano AM, Sundberg JP. Alopecia areata. Nat Rev Dis Primers. 2017;16(3):17011. doi:10.1038/nrdp.2017.11
61. Trink A, Sorbellini E, Bezzola P, et al. A randomized, double-blind, placebo- and active-controlled, half-head study to evaluate the effects of platelet-rich plasma on alopecia areata. Br J Dermatol. 2013;169(3):690–694. doi:10.1111/bjd.12397
62. Fawzy MM, Abdel Hay R, Mohammed FN, et al. Trichoscopy as an evaluation method for alopecia areata treatment: a comparative study. J Cosmet Dermatol. 2021;20(6):1827–1836. doi:10.1111/jocd.13739
63. Balakrishnan A, Joy B, Thyvalappil A, et al. A comparative study of therapeutic response to intralesional injections of platelet-rich plasma versus triamcinolone acetonide in alopecia areata. Indian Dermatol Online J. 2020;11(6):920–924. doi:10.4103/idoj.IDOJ_6_20
64. Hegde P, Relhan V, Sahoo B, et al. A randomized, placebo and active controlled, split scalp study to evaluate the efficacy of platelet-rich plasma in patchy alopecia areata of the scalp. Dermatol Ther. 2020;33(6):e14388. doi:10.1111/dth.14388
65. Albalat W, Ebrahim HM. Evaluation of platelet-rich plasma vs intralesional steroid in treatment of alopecia areata. J Cosmet Dermatol. 2019;18:1456–1462. doi:10.1111/jocd.12858
66. Ranpariya RH, Gupta SB, Deora MS, et al. Intralesional triamcinolone acetonide versus platelet rich plasma: a comparative study in the treatment of alopecia areata of scalp. Int J Res Dermatol. 2019;5(3):521–527. doi:10.18203/issn.2455-4529.IntJResDermatol20193223
67. Agrawal P, Jerajani HR, Jindal S. Intralesional platelet rich plasma therapy vs intralesional triamcinolone acetonide for the treatment of alopecia areata. MGM J Med Sci. 2018;5(2):68–75. doi:10.5005/jp-journals-10036-1187
68. Kapoor P, Kumar S, Brar BK, et al. Comparative evaluation of therapeutic efficacy of intralesional injection of triamcinolone acetonide versus intralesional autologous platelet-rich plasma injection in alopecia areata. J Cutan Aesthet Surg. 2020;13(2):103–111. doi:10.4103/JCAS.JCAS_16_19
69. Mubki T. Platelet-rich plasma combined with intralesional triamcinolone acetonide for the treatment of alopecia areata: a case report. J Dermatol Dermatol Surg. 2016;20:87–90. doi:10.1016/j.jdds.2015.11.002
70. Singh S. Role of platelet-rich plasma in chronic alopecia areata: our centre experience. Indian J Plast Surg. 2015;48(1):57–59. doi:10.4103/0970-0358.155271
71. Donovan J. Successful treatment of corticosteroid-resistant ophiasis-type alopecia areata (AA) with platelet-rich plasma (PRP). JAAD Case Rep. 2015;1(5):305–307. doi:10.1016/j.jdcr.2015.07.004
72. Pototschnig H, Madl MT. Successful treatment of alopecia areata barbae with platelet-rich plasma. Cureus. 2020;12(4):e7495. doi:10.7759/cureus.7495
73. KantiV, Röwert-HuberJ,VogtA, et al.Cicatricial alopecia.J Dtsch Dermatol Ges. 2018;16(4):435–461. doi:10.1111/ddg.13498
74. Litaiem N, Idoudi S. Frontal fibrosing alopecia. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2021.
75. Özcan D, Tunçer Vural A, Özen Ö. Platelet-rich plasma for treatment resistant frontal fibrosing alopecia: a case report. Dermatol Ther. 2019;32(5):e13072. doi:10.1111/dth.13072
76. Bolanča Ž, Goren A, Getaldić-švarc B, et al. Platelet-rich plasma as a novel treatment for lichen planopillaris. Dermatol Ther. 2016;29(4):233–235. doi:10.1111/dth.12343
77. DinaY, AguhC.Use of platelet-rich plasma in cicatricial alopecia.Dermatol Surg. 2019;45(7):979–981. doi:10.1097/DSS.0000000000001635
78. Jha AK. Platelet-rich plasma as an adjunctive treatment in lichen planopilaris. J Am Acad Dermatol. 2019;80(5):e109–e110. doi:10.1016/j.jaad.2018.09.013
79. Alves R, Grimalt R. Platelet-rich plasma and its use for cicatricial and non-cicatricial alopecias: a narrative review. Dermatol Ther (Heidelb). 2020;10(4):623–633. doi:10.1007/s13555-020-00408-5
80. ColeJP,ColeMA,InsalacoC, et al.Alopecia and platelet-derived therapies. Stem Cell Investig. 2017;4:88. doi:10.21037/sci.2017.11.01
81. Abdelkader R, Abdalbary S, Naguib I, et al. Effect of platelet rich plasma versus saline solution as a preservation solution for hair transplantation. Plast Reconstr Surg Glob Open. 2020;8(6):e2875. doi:10.1097/GOX.0000000000002875
82. Garg S. Outcome of intra-operative injected platelet-rich plasma therapy during follicular unit extraction hair transplant: a prospective randomised study in forty patients. J Cutan Aesthet Surg. 2016;9(3):157–164. doi:10.4103/0974-2077.191657
83. Cervantes J, Perper M, Wong LL, et al. Effectiveness of platelet-rich plasma for androgenetic alopecia: a review of the literature. Skin Appendage Disord. 2018;4(1):1–11. doi:10.1159/000477671
84. Almohanna HM, Ahmed AA, Griggs JW, et al. Platelet-rich plasma in the treatment of alopecia areata: a review. J Investig Dermatol Symp Proc. 2020;20(1):S45–S49. doi:10.1016/j.jisp.2020.05.002
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.