")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 19
Physicians’ Knowledge of Pulmonary Rehabilitation in China: A Cross-Sectional Study
Authors Pan F , Lu AT , Mao X , Hu F, Zhang H, Han B
Received 15 August 2023
Accepted for publication 13 November 2023
Published 16 January 2024 Volume 2024:19 Pages 121—131
DOI https://doi.org/10.2147/COPD.S429517
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jill Ohar
Feng Pan,1,* Ai-ting Lu,1,2,* Xiaowei Mao,1,* Fang Hu,1 Hai Zhang,1 Baohui Han1
1Department of Pulmonary Medicine, Shanghai Chest Hospital, Shanghai Jiaotong University, Shanghai, People’s Republic of China; 2Department of Pulmonary and Critical Care Medicine, Regional Medical Center for National Institute of Respiratory Diseases, Sir Run Run Shaw Hospital, School of Medicine, Zhejiang University, Hangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Baohui Han, Email [email protected]
Objective: To investigate the knowledge of pulmonary rehabilitation (PR) among physicians involved in pulmonary disease management.
Methods: This multi-regional cross-sectional survey was conducted from December 12, 2019 to January 22, 2020. The participants were enrolled and an electronic questionnaire was exclusively sent to the members of the Lung Cancer Special Committee of the China Medicine Education Association through the WeChat platform. Multivariable logistic regression analysis was performed to explore the associated factors of high PR knowledge scores (≥ 18 points).
Results: From the 858 valid questionnaires, the routine implementation of PR was only reported for 16.95% of physicians. The main reason hindering the implementation of PR for patients was the limited knowledge and awareness of PR among the physicians involved (69.1%). A total of 618 and 240 physicians had high and low knowledge scores, respectively. Multivariable analysis suggests that the self-perception of PR knowledge (OR = 1.89, 95% CI: 1.32– 2.771, P = 0.001) was independently associated with high knowledge scores, while having no theoretical knowledge of PR was associated with poor knowledge scores (OR = 0.43, 95% CI: 0.26– 0.72, P = 0.001).
Conclusion: Inadequate knowledge of pulmonary rehabilitation is evident among physicians who are involved in pulmonary disease management in China. This underscores the need for more comprehensive and standardized training to bolster their awareness and effective utilization of pulmonary rehabilitation.
Keywords: chronic obstructive pulmonary disease, pulmonary rehabilitation, lung cancer, knowledge, oncologists
Introduction
Chronic obstructive pulmonary disease (COPD) commonly affects adults >40 years old who experience significant exposure to combusted tobacco,1,2 with an estimated worldwide prevalence of about 11%, with about 14.3% in males and 7.6% in females.3 It is the third leading cause of mortality worldwide,4 with 4-year mortality rates ranging from 28% to 62%,1,2 and up to 90% of COPD deaths are reported in low- and middle-income countries.1,2 According to a cross-sectional study in mainland China, the standardized prevalence of COPD was estimated at 13.6%.5 Exacerbations in COPD are crucial events characterized by a sudden worsening of symptoms, particularly breathlessness, cough, and mucus production. These exacerbations significantly impact the health status, rate of hospital admissions, and mortality in individuals with COPD.6 Furthermore, the long-term decline in lung function and physical function has a substantial and lasting impact on the quality of life (QoL) among survivors.7,8 Hence, it is of great importance to implement strategies to optimize health-related QoL for patients with COPD.
Pulmonary rehabilitation, a comprehensive intervention based on patient assessment, encompasses exercise, education, and behavioral changes.1,9,10 Defined rigorously by the ACCP/ACCVP’s evidence-based guidelines, it aims to enhance the physical and psychological state of patients with chronic respiratory diseases and promote sustained healthy behaviors.11 This rehabilitation has been shown to minimize postoperative complications, expedite recovery, manage functional impairments, increase patients’ daily life activity endurance, and even enhance the potential for surgical intervention in patients initially deemed inoperable due to compromised lung function.12–15 Its benefits, recognized by an array of healthcare professionals, extend from improved dyspnea, mental health, and exercise tolerance to reduced hospitalizations, especially in patients with COPD. The core elements of pulmonary rehabilitation include personalized programs, multidisciplinary teams, and comprehensive disease understanding. A thorough patient assessment is vital to curate an individualized plan, involving a collaborative effort from physicians, nurses, therapists, dietitians, and community workers.16 Notably, COPD patients undergoing pulmonary rehabilitation experience enhanced walking distances, muscle strength, fewer exacerbations, and shorter hospital stays.17,18 Furthermore, its benefits are acknowledged for patients with other respiratory conditions like restrictive lung diseases, pulmonary hypertension, and lung cancer.19–22
While the benefits of pulmonary rehabilitation are well-established, its implementation remains a challenge across the global healthcare landscape. Several studies have shown that despite its proven efficacy, pulmonary rehabilitation remains considerably underutilized.23,24 Specifically, in China, a rapidly developing nation with a vast population, only about 27% of hospitals offer pulmonary rehabilitation services.25 This underutilization is not just a product of limited resources; often, the lack of its integration into COPD care pathways plays a significant role.26 Alarmingly, many patients remain deprived of the benefits of pulmonary rehabilitation due to inadequate referrals, a situation rooted in the limited knowledge and awareness among physicians involved in pulmonary disease management.26 This lack of awareness is not isolated to a few regions; even in developed regions of China, physicians remain relatively unaware of the importance and procedures related to pulmonary rehabilitation.27 Recent studies have indicated that the education level of the physician, their region of practice, and the duration of their professional practice were significant determinants influencing their awareness and subsequent referral rates for pulmonary rehabilitation.27 Thus, while the need for pulmonary rehabilitation is universally acknowledged, the gap in knowledge among healthcare professionals poses a significant challenge. There’s a need for comprehensive data to understand the dimensions of this challenge better, enabling the design of interventions for enhanced physician awareness and patient care.
Therefore, this multi-regional cross-sectional study aimed to investigate the perception of pulmonary rehabilitation among physicians involved in pulmonary disease management and explore associated factors of knowledge of pulmonary rehabilitation.
Methods
Study Design and Participants
This multi-regional cross-sectional survey was conducted from December 12, 2019 to January 22, 2020. The participants were enrolled through the WeChat platform. The electronic questionnaire was sent to a chat group exclusive to members of the Lung Cancer Special Committee of the China Medicine Education Association. The members were asked to spread the questionnaire to the related department at their hospital. The target population was physicians at all levels of hospitals in China who were engaged in work related to pulmonary disease. The study was approved by the ethics committee and all participants provided written informed consent before the survey.
Survey
Referring to the pulmonary rehabilitation-related literature, the authors developed the pulmonary rehabilitation knowledge survey. The questions were discussed and revised at a consensus meeting attended by experts in pulmonary disease. The questionnaire was administered through the WeChat platform using the software “WJX”. The physicians’ self-perception, knowledge of pulmonary rehabilitation, and implementation were investigated. The term “self-perception” refers to a subjective evaluation by physicians regarding their own understanding and familiarity with pulmonary rehabilitation. Knowledge of pulmonary rehabilitation represents an objective measurement derived from the responses of physicians to questions centered around their professional knowledge and awareness of pulmonary rehabilitation. The term “implementation” relates to the actual execution or application of pulmonary rehabilitation in clinical practice. It’s gauged based on the feedback from physicians in the survey concerning the prevalence and routine of pulmonary rehabilitation deployment in their respective healthcare settings.
The first part of the questionnaire was about the general information of the participants (including gender, age, occupation, title, education, department, years of work, and position). The second part of the questionnaire was about the self-perception (rated 0–10, with 10 being full perception) and previous theoretical study of pulmonary rehabilitation. The third part of the questionnaire was about the knowledge of pulmonary rehabilitation in three aspects: the role, content, and indications of pulmonary rehabilitation to assess the perception of the surveyed physicians. The fourth part of the questionnaire was about the implementation of pulmonary rehabilitation, including the current situation, physician’s willingness, and main obstacles.
There were 10 options for each of the three aspects of the third part. The role of pulmonary rehabilitation was set in the questionnaire with 10 options: (1) reduce hospitalization and mortality, (2) limit exercise capacity, (3) increase dyspnea and lower extremity discomfort, (4) improve upper extremity muscle strength and endurance, (5) improve quality of life, (6) limit mobility (eg, daily activities), (7) regulate emotions, (8) enhance self-care and cognition, (9) increase self-management, and (10) decreasing physical activity level. (1), (4), (5), (7), (8), and (9) are correct; (2), (3), (6), and (10) are incorrect. One point was given for each correct judgment. The content of pulmonary rehabilitation included 10 options: (1) exercise, (2) respiratory muscle exercise, (3) home oxygen therapy, (4) health education, (5) traditional Chinese medicine (TCM) rehabilitation, (6) telemedicine rehabilitation (rehabilitation through IoT, APP, WeChat platform, etc.), (7) neuromuscular electrical stimulation, (8) non-invasive ventilation, (9) self-management (adherence to medication, change of poor living environment, diet therapy, behavior change), and (10) psychological intervention. The physicians were surveyed to see if they understood these 10 items, and one point was given for each positive answer. There were 10 indications for pulmonary rehabilitation, including (1) chronic obstructive pulmonary disease, (2) asthma, (3) chronic bronchitis, (4) pulmonary hypertension/pulmonary heart disease, (5) interstitial lung disease, (6) bronchiectasis, (7) lung cancer, (8) perioperative chest surgery, (9) cardiovascular disease, and (10) others. One point was scored for each item selected.
The total score of pulmonary rehabilitation knowledge was 30 points, including 10 points for pulmonary rehabilitation role, 10 points for pulmonary rehabilitation content, and 10 points for pulmonary rehabilitation indications. A questionnaire was considered valid if all questions were answered.
An English version of the questionnaire is available in Figure S1.
Statistical Analysis
SPSS, version 18.0 (IBM, Armonk, NY, USA) was used for data processing and analysis. Continuous variables were presented as mean ± standard deviation or median (Q1, Q3), and categorical variables were presented as frequency (percentage). Comparisons between groups were performed using the chi-square test and t-test. The variables with P<0.05 in comparison were included in the multivariable logistic regression analysis to explore the associated factors of high pulmonary rehabilitation knowledge scores. The total score of pulmonary rehabilitation knowledge was divided at the 60% threshold, with 0–17 points being a low score and 18–30 points being a high score. The 60% threshold was determined based on a consensus achieved during meetings with experts in pulmonary disease. This threshold was considered to effectively represent a distinction in the level of expertise among the responders. P-values <0.05 were considered statistically significant.
Results
Characteristics of the Participants
A total of 858 valid questionnaires were collected in the study. The top five provinces and municipalities were Shanghai (n = 496, 57.8%), Jiangsu (n = 97, 11.3%), Zhejiang (n = 37, 4.3%), Anhui (n = 26, 3.0%), and Hebei (n = 24, 2.8%).
Among the 858 surveyed participants, 398 (46.4%) were male, and 460 (53.6%) were female. Thirty-six (4.2%) were <25 years old, 506 (59.0%) were 25–40 years old, 240 (28.0%) were 40–50 years old, and 74 (8.6%) were ≥50 years old. In addition, 365 (42.5%) worked in departments directly related to pulmonary disease (including respiratory medicine, thoracic surgery, oncology, radiotherapy, etc.), and 493 (57.5%) worked in other departments generally related to pulmonary disease (such as general medicine or major internal medicine) (Table 1).
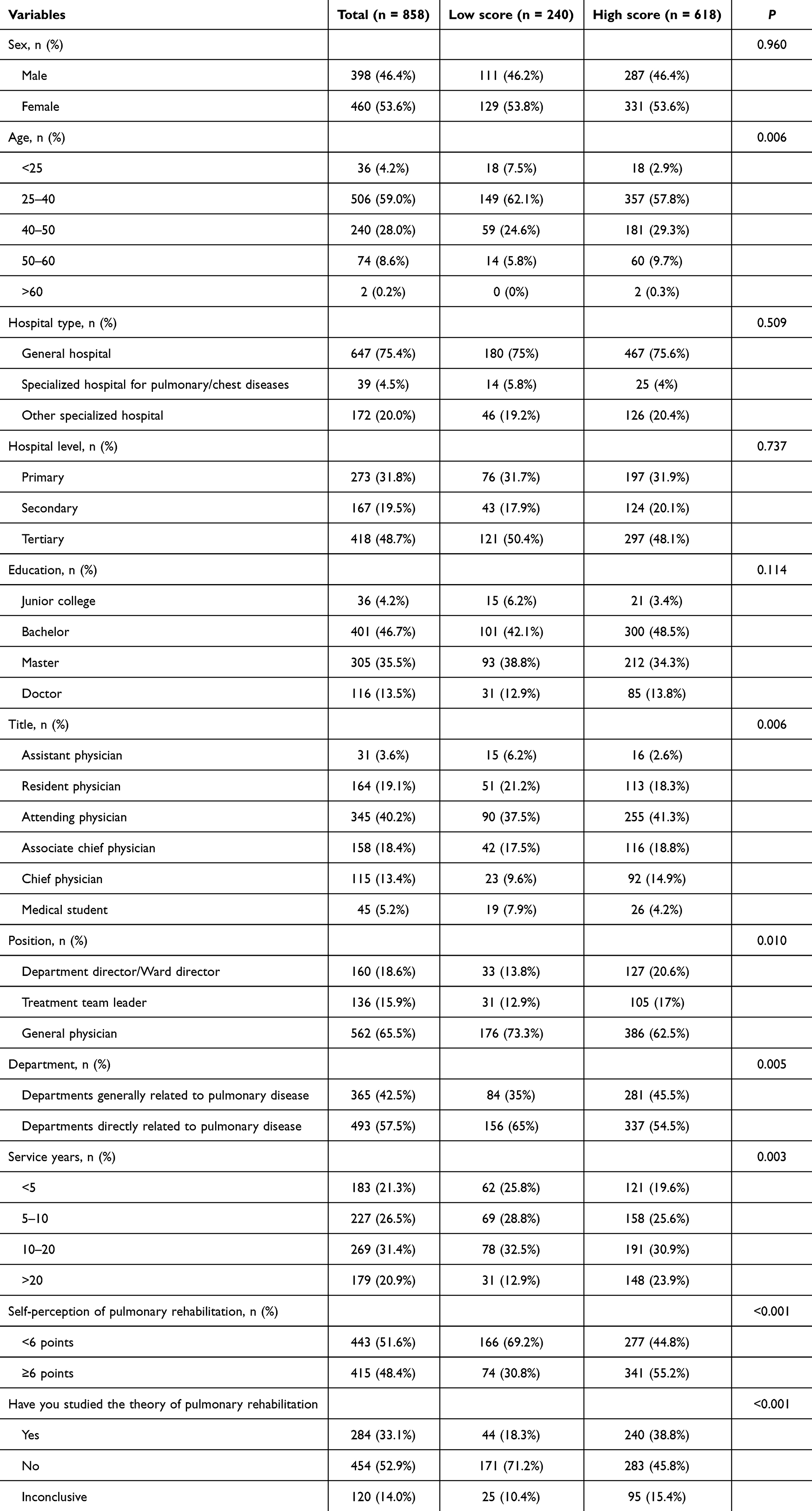 |
Table 1 Participants’ Characteristics |
Self-Perception and Implementation of Pulmonary Rehabilitation
Among all participants, 443 (51.6%) rated less than 6 points regarding self-perception of pulmonary rehabilitation, while only 284 (33.1%) have studied the theory of pulmonary rehabilitation. The routine implementation of pulmonary rehabilitation was only reported for 16.95% of physicians and 60.14% of the participants never had any implementation at their department. Nevertheless, most of the physicians (85.31%) were willing to provide the treatment of pulmonary rehabilitation.
The main reason reported to hinder the implementation of pulmonary rehabilitation for patients was the limited knowledge and awareness of pulmonary rehabilitation among the physicians involved (69.1%), followed by the lack of professional pulmonary rehabilitation techniques and equipment (54.8%).
Pulmonary Rehabilitation Knowledge, Perception, Indications Scores
The rate of high knowledge score was 72.0% (n = 618). The total knowledge score for pulmonary rehabilitation and the perception scores in the three components are shown in Table 2 and Figure 1.
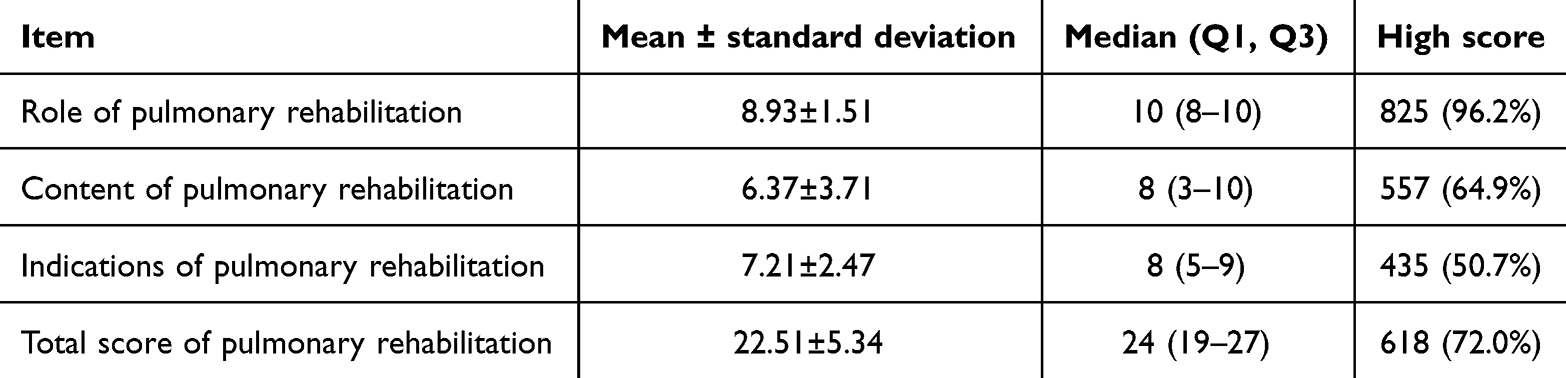 |
Table 2 Pulmonary Rehabilitation Knowledge Scores (n = 858) |
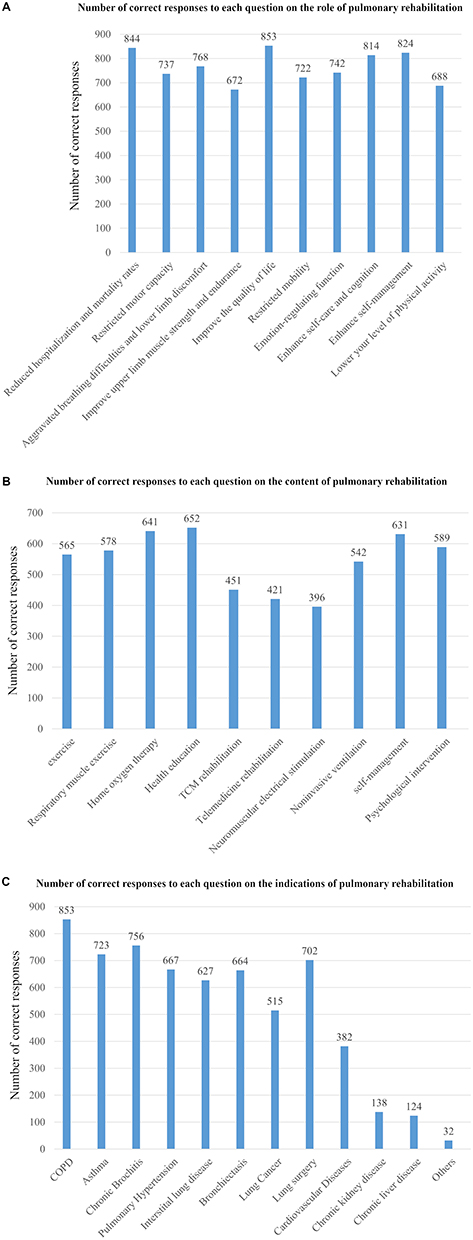 |
Figure 1 Scores of the perception of the role (A), content (B) and indications (C) of pulmonary rehabilitation by physicians involved in pulmonary disease management in China. The y-axis indicates the number of physicians who answered correctly. |
Compared with the low knowledge group, the participants with high knowledge belonged to older age groups (P = 0.006), higher professional titles (P = 0.006), higher hospital positions (P = 0.010), departments directly related to pulmonary disease (P = 0.005), and groups with longer experience (P = 0.003). The participants in the high-knowledge group also had a higher appreciation of their knowledge (P < 0.001) and received training in pulmonary rehabilitation (P < 0.001).
Associated Factors of High Pulmonary Rehabilitation Knowledge Scores
The multivariable analysis suggested that the self-perception of pulmonary rehabilitation knowledge (OR = 1.89, 95% CI: 1.32–2.771, P = 0.001) was independently associated with high knowledge scores, while having learned no theoretical knowledge of pulmonary rehabilitation was associated with poor knowledge scores (OR = 0.43, 95% CI: 0.26–0.72, P = 0.001) (Table 3).
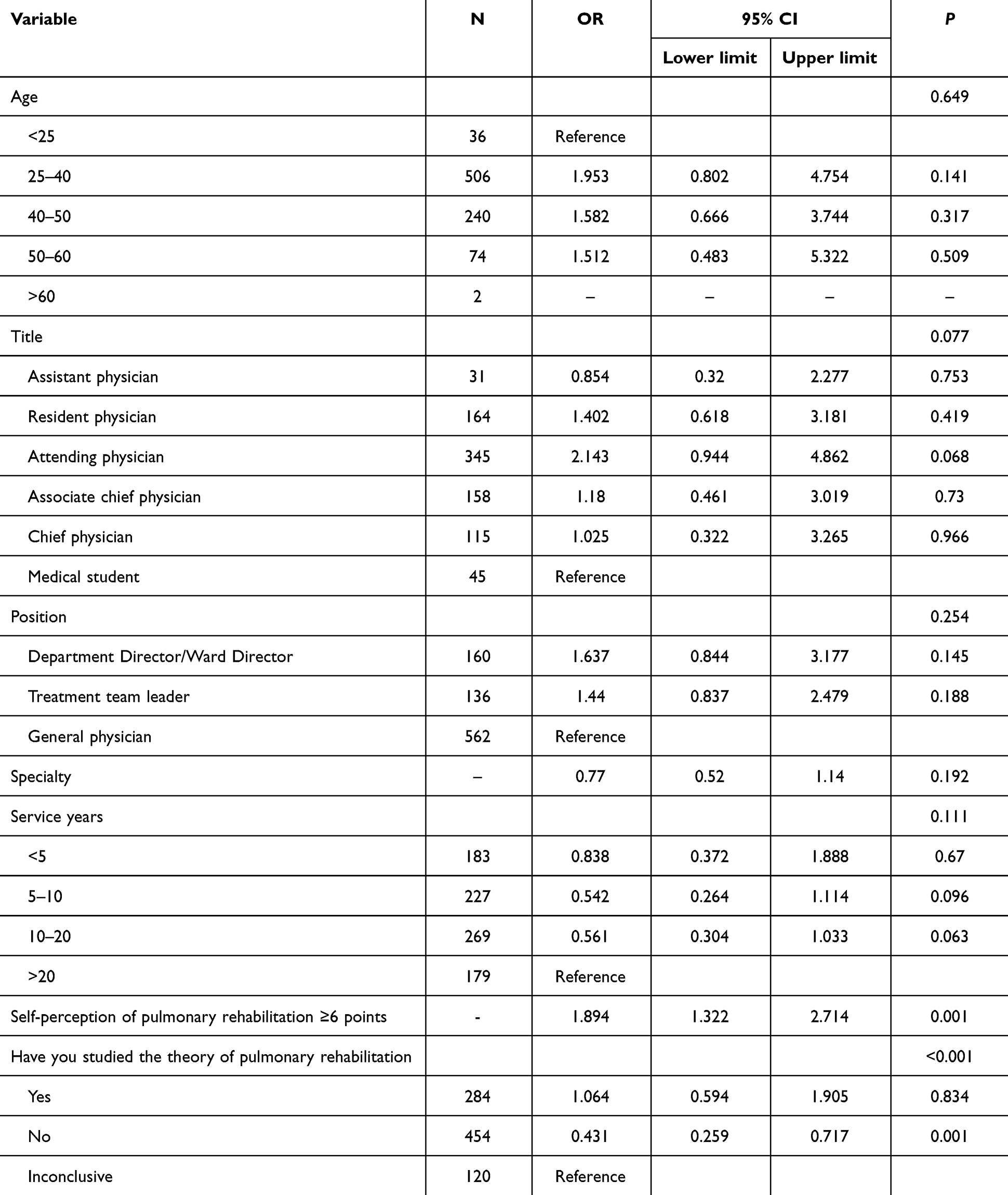 |
Table 3 Logistic Regression Analysis of Associated Factors of High Pulmonary Rehabilitation Knowledge |
Discussion
Due to differences in physicians’ characteristics, it is unclear whether clinicians have consistent knowledge of pulmonary rehabilitation. Therefore, this multi-regional cross-sectional study investigated the perception of pulmonary rehabilitation among physicians involved in pulmonary disease management. The results suggest that inadequate knowledge of pulmonary rehabilitation was observed among physicians. The self-perception and learning of theoretical knowledge were associated with better knowledge of pulmonary rehabilitation. The findings of this study revealed the current situation of knowledge of pulmonary rehabilitation and provided evidence for further implementation of education programs among physicians involved in pulmonary disease management in China.
Despite its described benefits, pulmonary rehabilitation is not popular among physicians, surveys conducted in hospitals abroad showed vast disparities in recommendations or implementation among continents and areas but relatively low referral rates.23,24 A study in China by Hao et al27 surveying 520 respiratory physicians showed that the physicians’ knowledge of pulmonary rehabilitation for COPD, as well as the referral rate of pulmonary rehabilitation in patients with COPD, was rather low. In addition, the low referral rates were influenced by education, area of China, and work experience, while the lack of facilities was the main barrier.27 Also in China, Xie et al28 showed a poor perception and disbelief in the need for pulmonary rehabilitation among patients with COPD. Such a poor perception of pulmonary rehabilitation will not encourage the patients to discuss pulmonary rehabilitation with their physician but also suggests that physicians do not promote pulmonary rehabilitation enough. In this study, 85.3% of the physicians were willing to provide pulmonary rehabilitation treatment to their patients. The main reason reported to hinder the implementation of pulmonary rehabilitation for patients was the limited knowledge and awareness of pulmonary rehabilitation among the physicians, technique, and equipment, which was supported by the literature, ie, that the main barriers to referral to pulmonary rehabilitation are a lack of knowledge and facilities.27 Of course, a lack of knowledge will not incite the physicians to request proper facilities from their hospital management and a lack of facilities will not encourage physicians to take an interest in pulmonary rehabilitation. Therefore, training in pulmonary rehabilitation should be standardized, and on-the-job training should be carried out so that continuing education in pulmonary rehabilitation can be implemented in daily work. While earlier studies have shed light on the general awareness and implementation of pulmonary rehabilitation among respiratory physicians, our investigation offers a more comprehensive exploration by encompassing a diverse range of medical specialists. Unlike prior research that predominantly centered on respiratory physicians,27 our study uniquely incorporates perspectives from physicians in departments directly related to pulmonary disease and departments generally related to pulmonary disease. This holistic approach provides a richer understanding of the landscape of pulmonary rehabilitation awareness and its implementation across varying medical fields. Additionally, the robust sample size of our study (n = 858) further reinforces the significance and validity of our findings. Together, these aspects underscore our study’s unique positioning in contributing fresh insights to the existing body of evidence on this subject.
In the broader context of our findings, it’s crucial to consider the environmental milieu in which the surveyed physicians operate. Urban healthcare settings, typically endowed with enhanced resources and access to contemporary medical practices, may inherently facilitate a physician’s exposure to pulmonary rehabilitation and its nuances. Conversely, physicians in rural settings might grapple with limited access to advanced training or pulmonary rehabilitation facilities.29 Notably, physicians embedded in specialized respiratory departments or tertiary care hospitals might naturally possess a more refined perspective on pulmonary rehabilitation, attributed to their frequent interactions with COPD patients and the interdisciplinary nature of such settings.27 Recognizing these environmental and cultural disparities can aid in designing bespoke educational interventions, ensuring a holistic propagation of pulmonary rehabilitation practices across varied healthcare terrains.
While our study has shed light on the knowledge gap among physicians, it is equally crucial to discern the underlying barriers and facilitators that influence the actual implementation of pulmonary rehabilitation. Factors such as existing healthcare infrastructure, availability of skilled professionals, socio-cultural attitudes towards rehabilitation, and economic constraints play a pivotal role. On the other hand, facilitators might include successful case studies, patient testimonials, increased awareness campaigns, and institutional support, which collectively bolster the advocacy for pulmonary rehabilitation.30 In the evolving landscape of pulmonary care, the findings of our study underscore the urgency to enhance the understanding and implementation of pulmonary rehabilitation among physicians. Central to this transformative journey is the necessity for robust physician education and training modules that intricately weave the principles and practices of pulmonary rehabilitation into the medical curriculum.31 Periodic workshops and continual medical education sessions can serve as reinforcement tools, ensuring that physicians remain updated on the latest methodologies and practices in pulmonary rehabilitation. Additionally, fostering a culture of interdisciplinary collaboration becomes paramount.32 By bridging the knowledge gaps and encouraging synergies between physicians, physiotherapists, respiratory therapists, and other allied healthcare professionals, a comprehensive, patient-centric approach to pulmonary rehabilitation can be realized. This holistic approach, however, warrants a robust policy and resource backbone. Governments and healthcare institutions must invest judiciously in infrastructure, policies, and training programs that prioritize pulmonary rehabilitation.31 Such endeavors, while resource-intensive, pave the way for a healthcare paradigm that is truly responsive to the needs of patients with pulmonary conditions, ensuring their improved quality of life and healthcare outcomes.
This study had limitations. Although the questionnaire was designed and revised by experts, it was not formally validated. Although the sample size was large, it represents only a fraction of the physicians involved in pulmonary disease management in China, and only a few geographical regions were covered. A further larger-scale cross-sectional study is warranted to verify the findings of this study.
Conclusion
Inadequate knowledge of pulmonary rehabilitation is evident among physicians involved in pulmonary disease management in China. Besides the self-perception and formal theoretical knowledge, understanding referral systems and access to pulmonary rehabilitation programs play a pivotal role. This underscores the need for more comprehensive and standardized training to bolster their awareness and effective utilization of pulmonary rehabilitation.
Ethics Approval and Informed Consent
The study was approved by the ethics committee and all participants provided written informed consent before the survey.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was supported by Zhejiang Medical and Health Science and Technology program (2023RC034); the Medical Engineering Cross Research Foundation of Shanghai Jiao Tong University (ZH2018QNA67); Scientific Research Project of Shanghai Municipal Health Commission (20194Y0168). The funders had no role in the study design, data collection, data analysis and interpretation, writing of the report, or the decision to submit the article for publication.
Disclosure
All authors declare that they have no competing interests.
References
1. Global Initiative for Chronic Obstructive Lung Disease (GOLD) Global strategy for the diagnosis, management, and prevention of COPD; 2022. https://goldcopd.org/wp-content/uploads/2021/11/GOLD-REPORT-2022-v1.0-12Nov2021_WMV.pdf.
2. Qaseem A, Wilt TJ, Weinberger SE, et al. Diagnosis and management of stable chronic obstructive pulmonary disease: a clinical practice guideline update from the American College of Physicians, American College of Chest Physicians, American Thoracic Society, and European Respiratory Society. Ann Intern Med. 2011;155(3):179–191. doi:10.7326/0003-4819-155-3-201108020-00008
3. Adeloye D, Chua S, Lee C, et al. Global and regional estimates of COPD prevalence: systematic review and meta-analysis. J Glob Health. 2015;5(2):020415. doi:10.7189/jogh.05.020415
4. Ford ES, Croft JB, Mannino DM, Wheaton AG, Zhang X, Giles WH. COPD surveillance--United States, 1999-2011. Chest. 2013;144(1):284–305. doi:10.1378/chest.13-0809
5. Fang L, Gao P, Bao H, et al. Chronic obstructive pulmonary disease in China: a nationwide prevalence study. Lancet Respir Med. 2018;6(6):421–430. doi:10.1016/S2213-2600(18)30103-6
6. Aaron SD. Management and prevention of exacerbations of COPD. BMJ. 2014;349(sep22 3):g5237. doi:10.1136/bmj.g5237
7. Stober A, Lutter JI, Schwarzkopf L, et al. Impact of Lung Function and Exacerbations on Health-Related Quality of Life in COPD Patients Within One Year: real-World Analysis Based on Claims Data. Int J Chron Obstruct Pulmon Dis. 2021;16:2637–2651. doi:10.2147/COPD.S313711
8. Guo J, Chen Y, Zhang W, Tong S, Dong J. Moderate and severe exacerbations have a significant impact on health-related quality of life, utility, and lung function in patients with chronic obstructive pulmonary disease: a meta-analysis. Int J Surg. 2020;78:28–35. doi:10.1016/j.ijsu.2020.04.010
9. Spruit MA, Singh SJ, Garvey C, et al. An official American Thoracic Society/European Respiratory Society statement: key concepts and advances in pulmonary rehabilitation. Am J Respir Crit Care Med. 2013;188(8):e13–64. doi:10.1164/rccm.201309-1634ST
10. Bolton CE, Bevan-Smith EF, Blakey JD, et al. British Thoracic Society guideline on pulmonary rehabilitation in adults. Thorax. 2013;68(Suppl 2):1–30. doi:10.1136/thoraxjnl-2013-203808
11. Ries AL, Carlin BW, Carrieri-Kohlman V. Pulmonary rehabilitation: joint ACCP/AACVPR evidence-based guidelines. ACCP/AACVPR Pulmonary Rehabilitation Guidelines Panel. American College of Chest Physicians. American Association of Cardiovascular and Pulmonary Rehabilitation. Chest. 1997;112(5):1363–1396. doi:10.1378/chest.112.5.1363
12. Burge AT, Cox NS, Abramson MJ, Holland AE. Interventions for promoting physical activity in people with chronic obstructive pulmonary disease (COPD). Cochrane Database Syst Rev. 2020;4(4):CD012626. doi:10.1002/14651858.CD012626.pub2
13. McCarthy B, Casey D, Devane D, Murphy K, Murphy E. Pulmonary rehabilitation for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2015;2(2):CD003793. doi:10.1002/14651858.CD006927.pub4
14. Vooijs M, Siemonsma PC, Heus I, Sont JK, Rovekamp TA, van Meeteren NL. Therapeutic validity and effectiveness of supervised physical exercise training on exercise capacity in patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis. Clin Rehabil. 2016;30(11):1037–1048. doi:10.1177/0269215515609413
15. van Wetering CR, Hoogendoorn M, Mol SJ, Rutten-van molken MP, Schols AM. Short- and long-term efficacy of a community-based COPD management programme in less advanced COPD: a randomised controlled trial. Thorax. 2010;65(1):7–13. doi:10.1136/thx.2009.118620
16. Wang H, Liu X, Rice SJ, Belani CP. Pulmonary Rehabilitation in Lung Cancer. PM R. 2016;8(10):990–996. doi:10.1016/j.pmrj.2016.03.010
17. van Ranst D, Stoop WA, Meijer JW, Otten HJ, van de Port IG. Reduction of exacerbation frequency in patients with COPD after participation in a comprehensive pulmonary rehabilitation program. Int J Chron Obstruct Pulmon Dis. 2014;9:1059–1067. doi:10.2147/COPD.S69574
18. Ho SC, Lin HC, Kuo HP, et al. Exercise training with negative pressure ventilation improves exercise capacity in patients with severe restrictive lung disease: a prospective controlled study. Respir Res. 2013;14(22). doi:10.1186/1465-9921-14-22
19. Varadi RG, Goldstein RS. Pulmonary rehabilitation for restrictive lung diseases. Chest. 2010;137(2):247–248. doi:10.1378/chest.09-1857
20. Arena R, Cahalin LP, Borghi-Silva A, Myers J. The effect of exercise training on the pulmonary arterial system in patients with pulmonary hypertension. Prog Cardiovasc Dis. 2015;57(5):480–488. doi:10.1016/j.pcad.2014.03.008
21. Jastrzebski D, Maksymiak M, Kostorz S, et al. Pulmonary Rehabilitation in Advanced Lung Cancer Patients During Chemotherapy. Adv Exp Med Biol. 2015;861:57.
22. Maeda K, Higashimoto Y, Honda N, et al. Effect of a postoperative outpatient pulmonary rehabilitation program on physical activity in patients who underwent pulmonary resection for lung cancer. Geriatr Gerontol Int. 2016;16(5):550–555. doi:10.1111/ggi.12505
23. Spruit MA, Pitta F, Garvey C, et al. Differences in content and organisational aspects of pulmonary rehabilitation programmes. Eur Respir J. 2014;43(5):1326–1337. doi:10.1183/09031936.00145613
24. Garvey C, Fullwood MD, Rigler J. Pulmonary rehabilitation exercise prescription in chronic obstructive lung disease: US survey and review of guidelines and clinical practices. J Cardiopulm Rehabil Prev. 2013;33(5):314–322. doi:10.1097/HCR.0b013e318297fea4
25. Gao LJ, Zhao HM. [A nationwide online questionnaire survey of the understanding and implementation of pulmonary rehabilitation at all levels of medical institutions in China in 2017]. Zhonghua Jie He He Hu Xi Za Zhi. 2019;42(4):275–278. Chinese. doi:10.3760/cma.j.issn.1001-0939.2019.04.006
26. Johnston KN, Young M, Grimmer KA, Antic R, Frith PA. Barriers to, and facilitators for, referral to pulmonary rehabilitation in COPD patients from the perspective of Australian general practitioners: a qualitative study. Prim Care Respir J. 2013;22(3):319–324. doi:10.4104/pcrj.2013.00062
27. Hao S, Xie L, Wang H, et al. Respiratory physicians’ awareness and referral of pulmonary rehabilitation in China: a cross-sectional study. J Thorac Dis. 2021;13(8):4753–4761. doi:10.21037/jtd-20-2587
28. Xie L, Liu Z, Hao S, et al. Assessment of knowledge, attitude, and practice towards pulmonary rehabilitation among COPD patients: a multicenter and cross-sectional survey in China. Respir Med. 2020;174:106198. doi:10.1016/j.rmed.2020.106198
29. Etruw E, Fuhr D, Huynh V, et al. Short-Term Health Outcomes of a Structured Pulmonary Rehabilitation Program Implemented Within Rural Canadian Sites Compared With an Established Urban Site: a Pre-Post Intervention Observational Study. Arch Phys Med Rehabil. 2023;104(5):753–760. doi:10.1016/j.apmr.2022.10.011
30. Rochester CL, Spruit MA, Holland AE. Pulmonary Rehabilitation in 2021. JAMA. 2021;326(10):969–970. doi:10.1001/jama.2021.6560
31. Vogiatzis I, Rochester CL, Spruit MA, Troosters T, Clini EM. American Thoracic Society/European Respiratory Society Task Force on Policy in Pulmonary R Increasing implementation and delivery of pulmonary rehabilitation: key messages from the new ATS/ERS policy statement. Eur Respir J. 2016;47(5):1336–1341. doi:10.1183/13993003.02151-2015
32. Liang J, Abramson MJ, Russell G, et al. Interdisciplinary COPD intervention in primary care: a cluster randomised controlled trial. Eur Respir J. 2019;53(4):1801530. doi:10.1183/13993003.01530-2018
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.