")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
Physical Therapists’ Role in Health and Wellness Promotion for People with Musculoskeletal Disorders: A Cross-Sectional Description Study Conducted in Saudi Arabia
Authors Alodaibi FA , Alotaibi MA , Almohiza MA, Alhowimel AS
Received 14 January 2022
Accepted for publication 18 March 2022
Published 29 March 2022 Volume 2022:15 Pages 567—576
DOI https://doi.org/10.2147/JMDH.S356932
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Faris A Alodaibi,1 Mazyad A Alotaibi,2 Mohammad A Almohiza,1 Ahmed S Alhowimel2
1Health Rehabilitation Science, College of Applied Medical Sciences, King Saud University, Riyadh, Saudi Arabia; 2Department of Health and Rehabilitation Science, Sattam Bin Abdulaziz University, Al-Kharj, Saudi Arabia
Correspondence: Faris A Alodaibi, Health Rehabilitation Sciences, College of Applied Medical Sciences, King Saud University, PO Box 22480, Riyadh, 11495, Kingdom of Saudi Arabia, Tel +966 14676176, Fax +966 14676162, Email [email protected]
Background: Chronic non-communicable diseases and musculoskeletal disorders are primarily associated with poor lifestyle behaviors and underestimated public health issues. Physical therapists have an essential role in promoting health. Still, few studies have described the current role of physical therapy in health promotion to lessen the impact of public health issues and chronic musculoskeletal conditions. Therefore, this study aimed to explore physical therapists’ health promotion in the musculoskeletal practice setting and investigate potential barriers and needed education.
Design and Methods: A cross-sectional descriptive study was conducted, using an electronic survey distributed among physical therapists practicing in Saudi Arabia who managed patients with musculoskeletal disorders.
Results: A total of 150 physical therapists participated in this survey. The physical therapists dealing with musculoskeletal disorders were, to a fair degree, aware of the importance of lifestyle risk factors related to health and wellness, particularly those relating to physical aspects. However, participants’ knowledge and experience (according to their report) were relatively limited in other lifestyle behaviors such as smoking, nutrition, sleep, and stress management. Participants believed further education/training would be needed to address these behaviors.
Conclusion: The participants appreciated the importance of addressing lifestyle factors. Nonetheless, knowledge and experience in health promotion were limited. To optimize the outcome of musculoskeletal patients through health promotion, more training will be needed.
Keywords: lifestyle behaviors, health promotion, physical therapy, education and training, musculoskeletal disorders
Introduction
Chronic non-communicable diseases (NCDs) pose a significant threat to the public health and quality of life of people of all ages and nationalities.1–3 The burden of NCDs is projected to increase due to several factors, including a longer average life span and an increasing prevalence of unhealthy lifestyles. Many of the underlying risk factors for NCDs, particularly the unhealthy lifestyle behaviors, are modifiable, and therefore NCDs may be amenable to behavior modification.4 Chronic musculoskeletal disorders, including back pain, are similar to NCDs in that they are a significant reason for seeking care, and they share many of the modifiable lifestyle behaviors and risk factors.5 Physical inactivity, smoking, an unhealthy diet, obesity, poor sleep, and stress are the main lifestyle behaviors associated with NCDs and chronic musculoskeletal disorders.6 Therefore, targeting these lifestyle behaviors may manage these conditions and improve general health and wellness. Healthcare professionals have an excellent opportunity to lessen the impact of chronic pain through incorporating health promotion into their clinical practice and thereby changing the lifestyle of their patients, which may help reduce the burden of such cases.7
Health promotion has been defined as “the process of enabling people to increase control over, and to improve, their health.”.8 Assessment, communication, and improving health literacy are among the main ways to promote health.9 According to the World Physiotherapy (formerly known as the World Confederation for Physical Therapy), “Physical therapists provide services that develop, maintain and restore people’s maximum movement and functional ability”. From physical, psychological, emotional, and social well-being, physical therapists help people maximize their quality of life. Physical therapists dealing with musculoskeletal disorders encounter many patients with chronic conditions and unhealthy lifestyle behaviors and therefore are well-positioned to promote health and wellness with their patients.10 Through this, physical therapists could have a vital role in reducing the burden of NCDs and chronic musculoskeletal disorders. However, health and wellness promotion has not yet been recognized as a core physical therapist competency, and few studies have looked at the current assessment, management, and barriers to physical therapists incorporating health and wellness promotion into their clinical practice.11–14 To support enhancing the health promotion practice in Saudi Arabia, current physical therapy services need to be explored in assessing and managing lifestyle behaviors.
Therefore, this study aimed to explore the current role of physical therapists practicing in Saudi Arabia in assessing and managing lifestyle behaviors of patients presenting with musculoskeletal disorders. Additionally, we aimed to examine physical therapists’ beliefs regarding the perceived barriers and training needs required to provide health and wellness promotion in the musculoskeletal physical therapy practice setting.
Design and Methods
Study Design
A cross-sectional study was undertaken, utilizing an online survey to explore physical therapists’ current role in assessing and managing lifestyle behaviors and risk factors from June 2019 to September 2019. Ethical approval was obtained from the King Fahad Medical City Research Ethics Committee.
Eligibility Criteria
We targeted a convenience sample of physical therapists in Saudi Arabia whose clinical practice involves managing individuals with musculoskeletal disorders. The advertisement for participating in the study was distributed through social media and direct invitations with the help of the Saudi physical therapy association and other physical therapy clubs and individuals practicing in Saudi Arabia. Informed consent was included in the first page of the web-based survey (describing the study and asking for the willingness to participate). To be included, participants had to consent to be part of the study before starting.
Outcome Measure
A survey was purpose-designed and based on previous studies.12–14 The survey was organized into several sections that included: demographic and background descriptive data (including personal adherence to healthy lifestyle factors), assessment and confidence level in assessing lifestyle behaviors and readiness to change, the priority level of addressing lifestyle risk factors, and perceived effectiveness of such practice, barriers to providing health and wellness promotion, and education needed to be able to provide health and wellness promotion. The electronic survey was distributed to physical therapists practicing in Saudi Arabia who work with musculoskeletal disorders. Since English is the formal language in physical therapy education and practice in Saudi Arabia, the survey was conducted in English.
Sample Size
According to the Saudi Commission for Health Specialties (SCFHS), there were 1618 licensed physical therapists in 2018.15 With a population of 1618 and a margin of error of 5%, the required sample size was computed by setting the statistical power at an 80% confidence interval. As a result, a sample size of 150 people was necessary for this study.
Data Analyses
Data were described using absolute and relative frequencies. We examined the effects of age, gender, and experience on the likelihood that therapist report assessing smoking, diet, sleep, stress/psychological status, and physical activity/exercise. Analyses were conducted using the Statistical Package for the Social Sciences (SPSS, Version 25) and the significance level was set at 0.05.
Results
A total of 153 physical therapists participated in the online survey; however, three were excluded since they were still students. Thus, we analyzed the data of 150 physical therapists who managed musculoskeletal disorders.
Participants’ Characteristics
As summarized in Table 1, most of the participants were 30 years old or less and had five years or less of work experience. Rating their adherence to healthy lifestyle factors, the majority reported being non-smokers and having “correct posture and lifting techniques”, but only a minority thought they were physically active and had a healthy diet and sleep routine (Table 1).
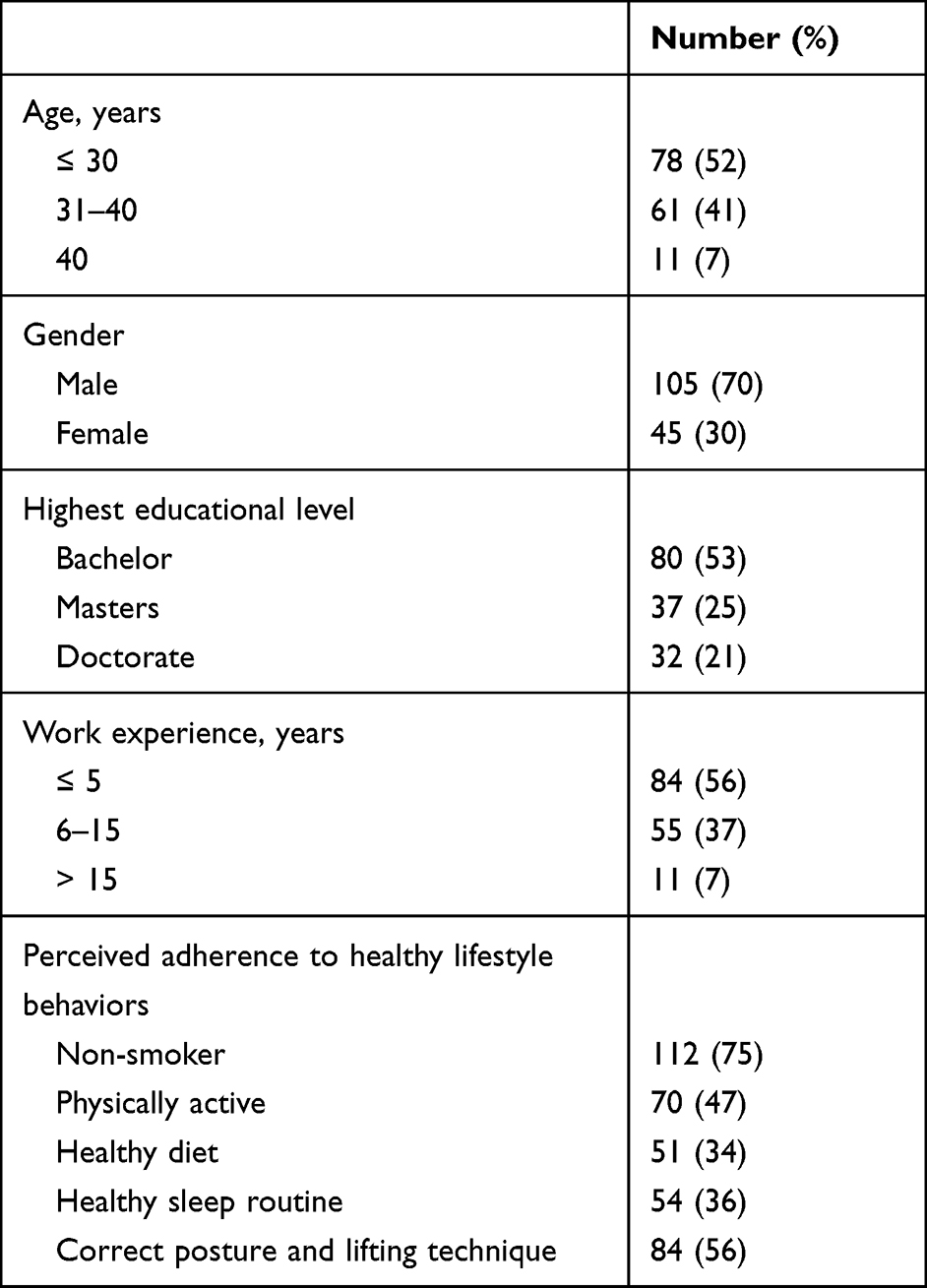 |
Table 1 Demographic and Descriptive Data for the 150 Participants |
Education/Training and Assessment of Lifestyle Behaviors and Risk Factors
When asked about whether they had received any education or training specifically in the management of lifestyle behaviors and risk factors or learning strategies for helping patients change their behaviors, as summarized in Table 2, the majority reported receiving some concerning physical activity. Still, the percentages were considerably lower for the other behaviors and factors listed. Similarly, the majority reported usually or always assessing physical activity levels and correct posture, but markedly fewer reported “usually or always” assessing the other lifestyle behaviors and risk factors (Table 2).
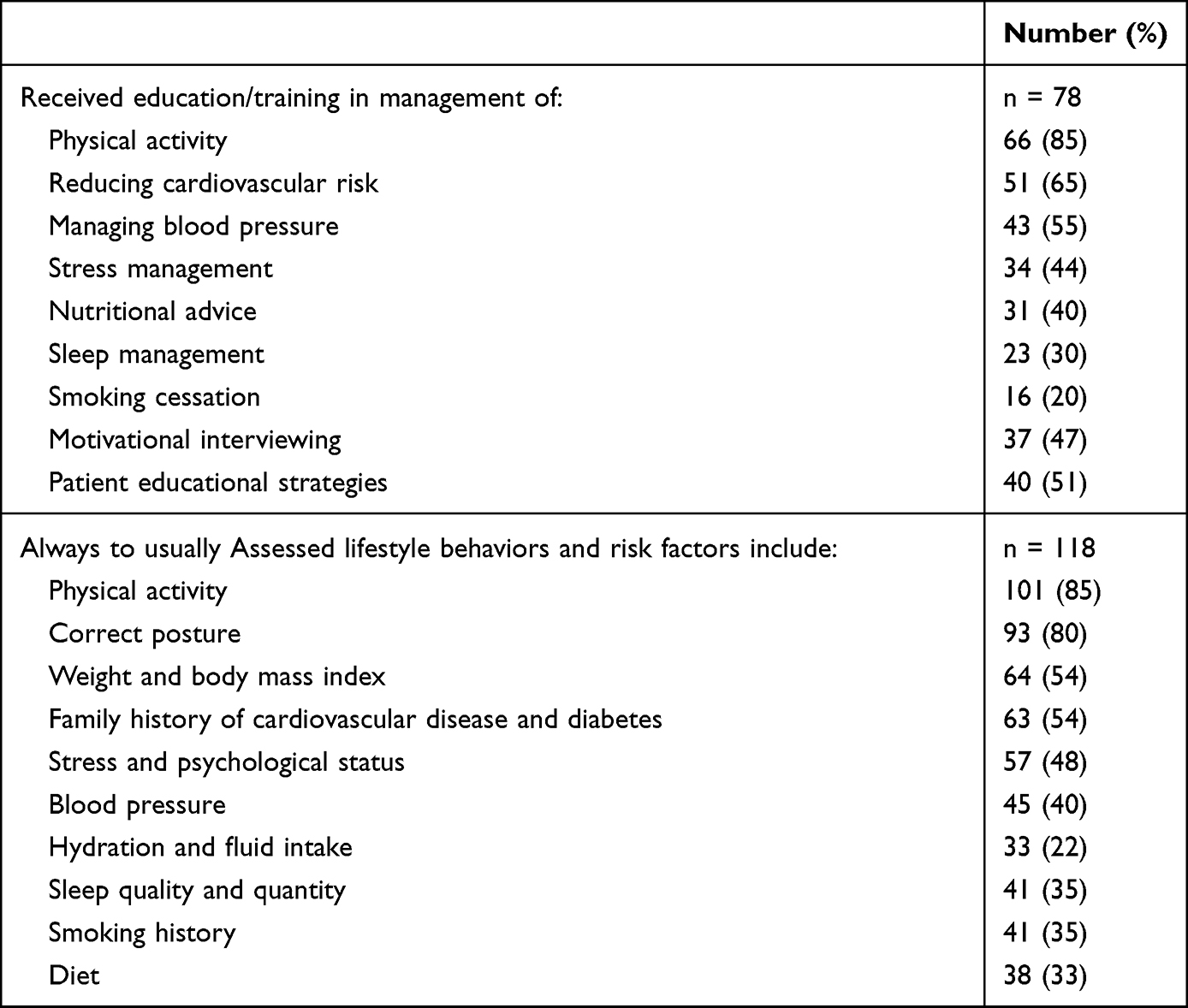 |
Table 2 Education/Training the Participants Had Received and Assessments Undertaken Regarding Lifestyle Behaviors and Risk Factors |
Participants were also asked about their level of confidence in assessing lifestyle behaviors and risk factors. As shown in Figure 1, this varied widely across the factors, with higher levels of confidence seen for assessing posture/lifting and physical inactivity but much lower levels for the other factors.
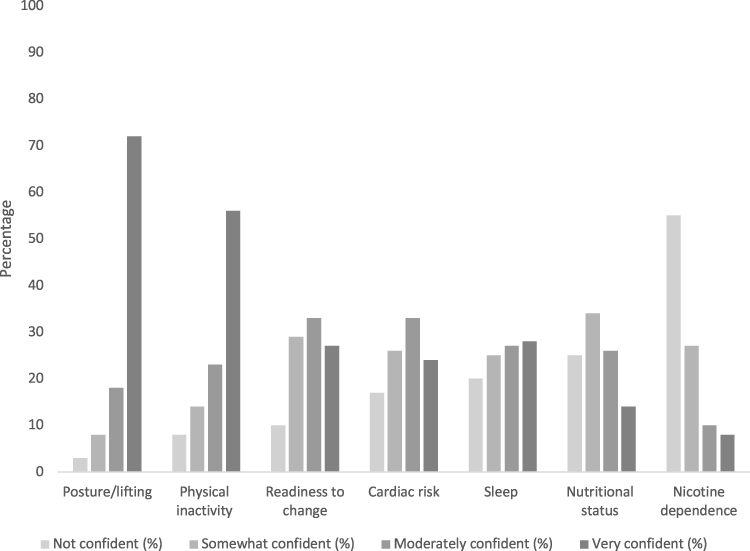 |
Figure 1 Participants’ (n = 118) level of confidence level at assessing lifestyle behaviors and risk factors. |
Advice Regarding Lifestyle Behaviors and Risk Factors: Frequency, Effectiveness, Priority, and Acceptability
As summarized by the 98 participants who responded to this survey item, correct posture, correct lifting, and taking regular exercise and physical activity were the most frequent behaviors and risk factors the participants counseled their patients about according to their report (Figure 2). In terms of the perceived effectiveness of this advice, the advice about correct posture, lifting, and physical activity was rated as being the most effective. Of the 85 participants who responded to the question about the priority of addressing lifestyle behaviors and risk factors as part of their usual clinical workload, addressing physical activity, correct posture, and lifting were given the highest priority (Figure 3). Similarly, the participants rated their counseling about physical activity, correct posture, and lifting as most acceptable to their patients.
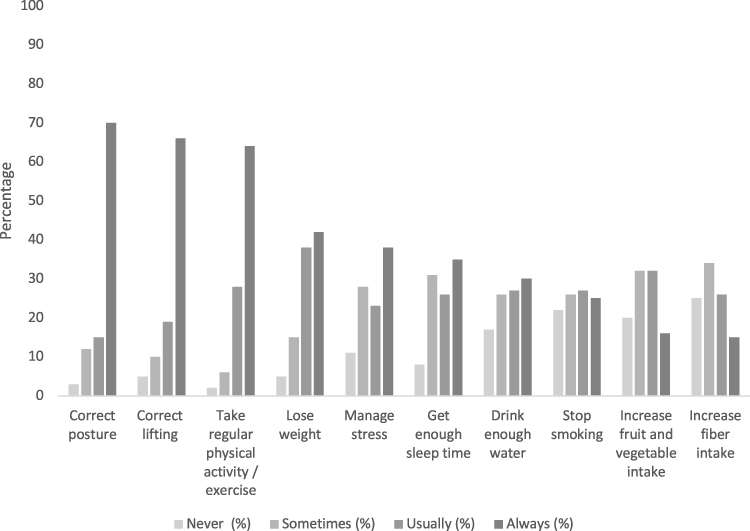 |
Figure 2 Participants’ (n = 98) frequency of advising patients about lifestyle behaviors and risk factors. |
 |
Figure 3 Participants’ (n = 85) perception of priority of addressing lifestyle behaviors and risk factors. |
Availability and Sources of Patient Educational Materials
Participants reported that educational materials about physical activity and exercise were the most readily available, whereas more than 50% of participants reported having no educational materials about smoking cessation.
As physical therapists may need to refer their patients to other providers, services, or support groups to provide assessment, advice, and education on lifestyle behaviors and risk factors, participants were asked to rate how often they were able to find this accessible concerning five lifestyle behaviors. This was reported as never being available, in descending order, by 54 (55%) for smoking cessation, 39 (40%) for diet and sleep disorder, 36 (37%) for stress management, and 14 (14%) for physical activity and exercises.
Perceived Barriers to Health and Wellness Promotion and Required Training
A summary of the participants’ rating of the perceived importance of potential barriers to providing health and wellness promotion is shown in Figure 4. As can be seen, the highest-rated potential barriers were a lack of access to health promotion staff and counselors, lack of interest from the patient, and lack of proper patient educational materials. Finally, participants were asked if they would like more training in health and wellness promotion. While only 78 participants answered this question, 67 (86%) responded that they would like more training, and the most frequent form of education the participants chose was workshops.
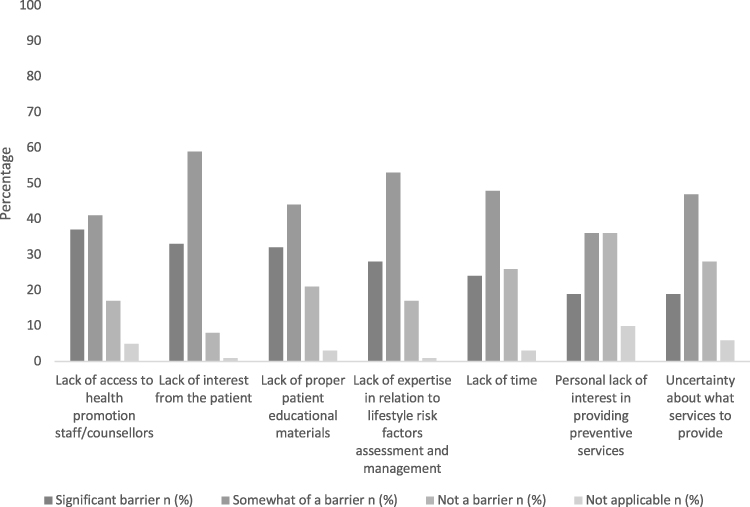 |
Figure 4 Rating of the significance of potential barriers to providing health and wellness promotion (n=78). |
Simple logistic regression models were performed to examine the effects of age, gender, and experience on the likelihood that participants report assessing smoking, diet, sleep, stress/psychological status, and physical activity/exercise. None of the demographic variables were significant (P<0.05). Table 3 present the odds ratios, 95% CI, and their p-values.
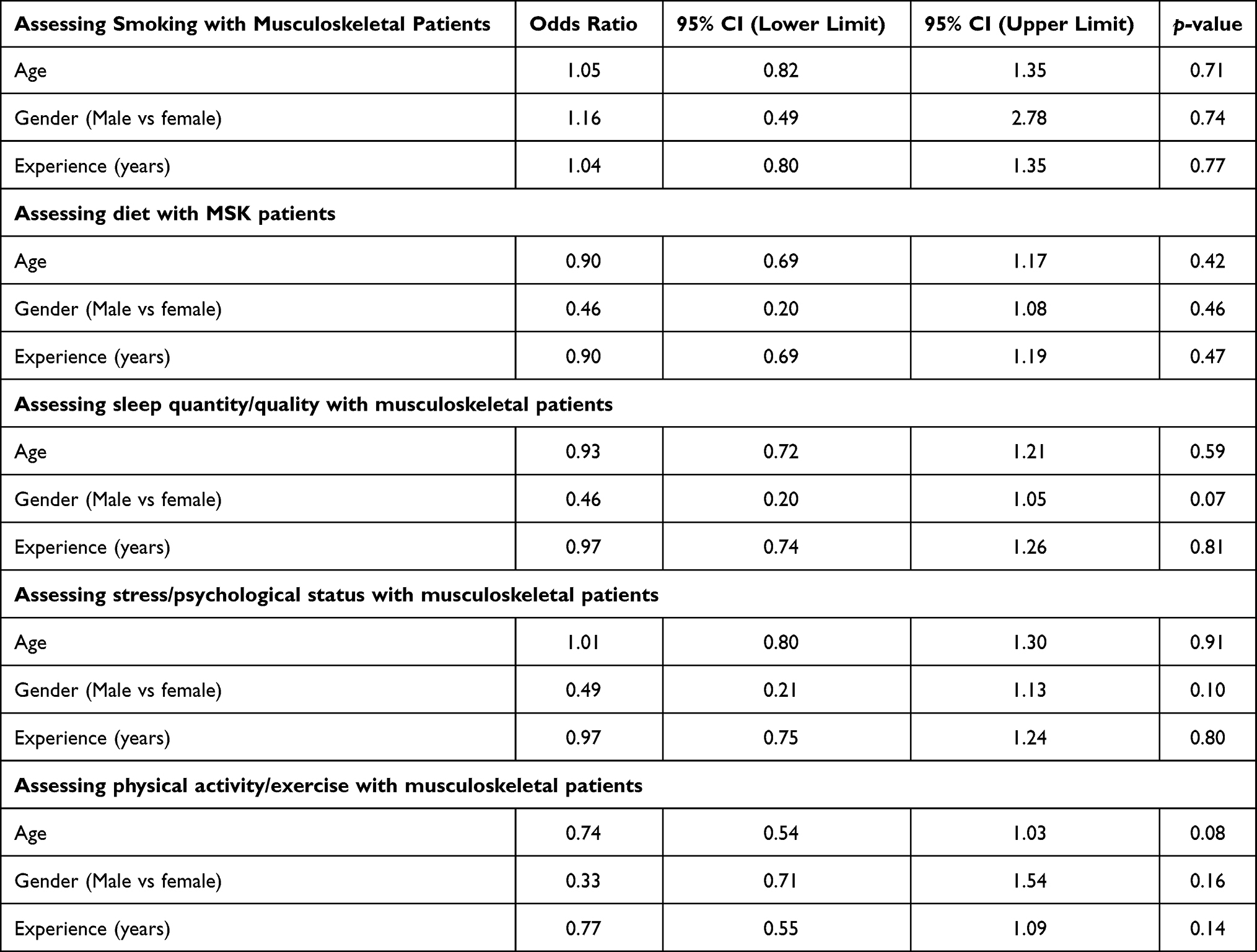 |
Table 3 Simple Logistic Regressions for the Effect of Age, Gender, and Experience on the Likelihood That Participants Assess Smoking, Diet, Sleep, Stress/Psychological Status, and Physical Activity/Exercise |
Discussion
To the best of our knowledge, this is the first study undertaken in Saudi Arabia, and indeed the Middle East, that has investigated the current role of physical therapists regarding the assessment and management of lifestyle risk factors in patients presenting with musculoskeletal disorders, and the perceived barriers and training that would be required to provide health and wellness promotion. We found that the physical therapists who participated in this study frequently assessed patients’ level of physical activity/exercise, posture, and lifting according to their report. However, their assessment of other lifestyle risk factors was lower based on their answers, such as anthropometric measures, stress and psychological status, and family history of cardiovascular disease and diabetes.
Our study findings whereby physical therapists reported being confident to provide advice regarding posture, lifting, and physical activity/exercise but less confident with other lifestyle risk factors were similar to those of O’Donoghue et al13 and Abaraogu et al.14 These studies investigated the practice of lifestyle assessment among physical therapists in Ireland13 and Nigeria14 and found that the majority of physical therapists provided advice to increase physical activity, perceived this advice as being very effective, and referred physically inactive patients to other providers or resources. The study by O’Donoghue et al13 among primary care physical therapists, found that most of the physical therapists in their sample assessed patients’ physical activity level, and most of them reported having received training about the management of the risk of physical inactivity.
While it could be argued that the other lifestyle risk factors may not be overly relevant in the setting of musculoskeletal, they have been shown to be associated with musculoskeletal pain and disability. In a meta-analysis of 40 studies examining the relationship between low back pain and smoking, Shiri et al, concluded that smokers have a higher prevalence and incidence of developing low back pain than non-smokers.16 Nutrition is linked to obesity, inflammatory process, and nerve sensitization and therefore, leads to the development of musculoskeletal pain.17 Moreover, insomnia has been shown to increase the risk of developing musculoskeletal pain18,19 and emotional distress and cognitive-behavioral factors are strong indicators for chronic musculoskeletal pain and disability.20
The sample of physical therapists who participated in our study reported moderate to low awareness regarding their potential role in assessing and managing lifestyle behaviors other than the physical activity/exercise advice. Therefore, participants appeared to use a reductionist approach when managing lifestyle behaviors by adopting a biomedical model instead of a holistic approach to managing patients with musculoskeletal pain.21 This approach might miss important contributors to pain chronicity development and persistence that in turn might influence function and physical therapy intervention outcomes.
The most frequently reported perceived barriers to assessing and managing lifestyle behaviors seen in our study included lack of patients’ interest, lack of expertise about lifestyle risk factors assessment and management, lack of access to health promotion staff/counselors, lack of proper patient education materials, lack of time, and uncertainty about what services to provide. Addressing these barriers by educating and training physical therapists in health and wellness promotion and providing enough time for each patient to be able to provide such holistic interventions could enhance clinical practice and patient outcomes and overall health.
We also explored the relationship between the effects of age, gender, and experience on the likelihood that participants report assessing smoking, diet, sleep, stress/psychological status, and physical activity/exercise. While we found no statistically significant relationships and given the small sample size, some links may be drawn from these findings. Although not no statistically significant, females tend to have higher odds than males in reporting assessment of stress/psychological status and physical activity/exercise with MSK patients. Also, younger participants tend to have higher odds than older counterparts in reporting assessment of physical activity/exercise with MSK patients. Future studies with larger sample size should be conducted to further examine the relationships between gender and age and the assessment of these health promotion areas.
Some limitations need to be considered when interpreting the findings of this study. While we received over a hundred responses, the generalizability of the findings is still limited because participation was voluntary, limited in some questions, and selection bias may have been introduced. Because of the nature of the cross-sectional design, we might have introduced selection bias, meaning that our timing of accepting the participation for the study may not reflect actual practice and therefore it is recommended to examine this in a longer period and larger sample size. Moreover, because we had more than 15 questions in our survey, our completion rate decreased with the survey progression and this may led to losing more participants. However, we maintained a completion rate of above 50% in all questions. Although the findings was similar to other related studies,13,14 caution should be taken when interpreting these results taking considering the missing data. Another limitation relates to the utilized survey. Although it was based on previous studies,12–14 the validity was not examined, and self-report results need to be interpreted with caution. The participants report may not reflect actual practice and future study should examine the assessment and management behaviors with more objective tools. Nonetheless, these findings provide preliminary data of the health promotion and wellness practice adopted by physical therapists with their musculoskeletal patients in Saudi Arabia.
This study was the first one in the Saudi Arabia and Middle-East to highlight that the knowledge and experience of the participants practicing in Saudi Arabia were limited in assessing, managing lifestyle behaviors and health promotion, so further education/training would be needed to optimize the outcome of musculoskeletal patients through health promotion. To advance health promotion practice in the musculoskeletal physical therapy, future research needs to explore the impact of providing training in this contemporary physical therapy practice on the general health of musculoskeletal patients. It is recommended that physical therapists should be empowered to fulfill a health promotion role through educational activities, training courses, and incorporating basic education and training about the role of physical therapists in health and wellness promotion into the undergraduate physical therapy curricula. It is assumed that adopting health promotion practice, considering all relevant lifestyle factors, by physical therapy could optimize clinical outcomes and general health of musculoskeletal patients.
Conclusions
This study found that physical therapists dealing with musculoskeletal disorders were mostly aware of the importance of lifestyle risk factors related to health and wellness. However, their knowledge and experience in health and wellness promotion were relatively limited and tended to be focused on posture, lifting, and physical activity. To optimize the outcome of patients with musculoskeletal disorders, more training in health and wellness promotion would be needed.
Significance for Public Health
In the twenty-first century, chronic non-communicable diseases (NCDs) pose a significant threat to public health, closely related to poor lifestyle. To decrease the burden of NCDs, health promotion efforts from different healthcare providers are needed. This study explored physical therapists’ health promotion in the musculoskeletal practice setting and investigated potential barriers and required education. The results of this can help advance health promotion practice in musculoskeletal physical therapy by providing current perspectives in current practice and perceived barriers and needed training areas.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethical Approval
This study complies with the Declaration of Helsinki and has been reviewed and approved by the Institutional Review Board of KFMC. (IRB Approval Number 18-384E).
Acknowledgments
We gratefully acknowledge financial support from King Abdulaziz City for Science and Technology, Saudi Arabia (Grant research number (05-18-03-001-0001). The funding source had nothing to do with the conduction of the research or the results.
Disclosure
The authors declare no conflicts of interest for this work. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
References
1. Daar AS, Singer PA, Persad DL, et al. Grand challenges in chronic non-communicable diseases. Nature. 2007;450(7169):494–496. doi:10.1038/450494a
2. Beaglehole R, Bonita R, Horton R, et al. Priority actions for the non-communicable disease crisis. Lancet. 2011;377(9775):1438–1447. doi:10.1016/S0140-6736(11)60393-0
3. Alzeidan R, Rabiee F, Mandil A, Hersi A, Fayed A. Non-communicable disease risk factors among employees and their families of a Saudi university: an epidemiological study. PLoS One. 2016;11(11):e0165036. doi:10.1371/journal.pone.0165036
4. World Health Organization. The world health report 2002: reducing risks, promoting healthy life. World Health Organization; 2002.
5. Woolf AD, Akesson K. Understanding the burden of musculoskeletal conditions. The burden is huge and not reflected in national health priorities. BMJ. 2001;322(7294):1079–1080. doi:10.1136/bmj.322.7294.1079
6. Dean E, Söderlund A. What is the role of lifestyle behaviour change associated with non-communicable disease risk in managing musculoskeletal health conditions with special reference to chronic pain? BMC Musculoskelet Disord. 2015;16(1):1–7. doi:10.1186/s12891-015-0545-y
7. van Hecke O, Torrance N, Smith BH. Chronic pain epidemiology–where do lifestyle factors fit in? Br J Pain. 2013;7(4):209–217. doi:10.1177/2049463713493264
8. Nutbeam D. Health promotion glossary. Health Promot Int. 1998;13(4):349–364. doi:10.1093/heapro/13.4.349
9. Nutbeam D. Health literacy as a public health goal: a challenge for contemporary health education and communication strategies into the 21st century. Health Promot Int. 2000;15(3):259–267. doi:10.1093/heapro/15.3.259
10. Bezner JR. Promoting health and wellness: implications for physical therapist practice. Phys Ther. 2015;95(10):1433–1444. doi:10.2522/ptj.20140271
11. Dean E, Skinner M, Myezwa H, et al. Health competency standards in physical therapist practice. Phys Ther. 2019;99(9):1242–1254. doi:10.1093/ptj/pzz087
12. Alodaibi F AA, Alotiabi M, ALMohiza M. Perception of physiotherapists practicing in Saudi Arabia about their role in health and wellness promotion for patients with musculoskeletal conditions: a qualitative study; 2021.
13. O’Donoghue G, Cunningham C, Murphy F, Woods C, Aagaard-Hansen J. Assessment and management of risk factors for the prevention of lifestyle-related disease: a cross-sectional survey of current activities, barriers and perceived training needs of primary care physiotherapists in the Republic of Ireland. Physiotherapy. 2014;100(2):116–122. doi:10.1016/j.physio.2013.10.004
14. Abaraogu UO, Ogaga MO, Dean E. Practices of Nigerian physiotherapists with respect to lifestyle risk factor assessment and intervention: a national cross-sectional survey. Physiother Theory Pract. 2017;33(6):497–507. doi:10.1080/09593985.2017.1318421
15. Saudi Commission for Health Specialties. Health Workforce. 2018. Available from: https://www.scfhs.org.sa/Media/DigitalLibrary/DocumentLibrary/OtherPublications/Pages/default.aspx.
16. Shiri R, Karppinen J, Leino-Arjas P, Solovieva S, Viikari-Juntura E. The association between smoking and low back pain: a meta-analysis. Am J Med. 2010;123(1):
17. Elma Ö, Yilmaz ST, Deliens T, et al. Chronic musculoskeletal pain and nutrition: where are we and where are we heading? Pm&r. 2020;12(12):1268–1278. doi:10.1002/pmrj.12346
18. Mork PJ, Vik KL, Moe B, Lier R, Bardal EM, Nilsen TI. Sleep problems, exercise and obesity and risk of chronic musculoskeletal pain: the Norwegian HUNT study. Eur J Public Health. 2014;24(6):924–929. doi:10.1093/eurpub/ckt198
19. Smith MT, Quartana PJ, Okonkwo RM, Nasir A. Mechanisms by which sleep disturbance contributes to osteoarthritis pain: a conceptual model. Curr Pain Headache Rep. 2009;13(6):447–454. doi:10.1007/s11916-009-0073-2
20. Tseli E, Boersma K, Stalnacke BM, et al. Prognostic factors for physical functioning after multidisciplinary rehabilitation in patients with chronic musculoskeletal pain: a systematic review and meta-analysis. Clin J Pain. 2019;35(2):148–173. doi:10.1097/AJP.0000000000000669
21. Remde A, DeTurk S, Wojda T. Teaching balanced patient care using principles of reductionism and holism: the example of chronic low back pain. In: Contemporary Topics in Graduate Medical Education. IntechOpen; 2018.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.