Back to Journals » Journal of Pain Research » Volume 12
Physical functioning and mindfulness skills training in chronic pain: a systematic review
Authors Jackson W ![]() , Zale EL, Berman SJ, Malacarne A, Lapidow A, Schatman ME
, Zale EL, Berman SJ, Malacarne A, Lapidow A, Schatman ME ![]() , Kulich R
, Kulich R ![]() , Vranceanu AM
, Vranceanu AM ![]()
Received 1 May 2018
Accepted for publication 2 October 2018
Published 3 January 2019 Volume 2019:12 Pages 179—189
DOI https://doi.org/10.2147/JPR.S172733
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Katherine Hanlon
William Jackson,1 Emily L Zale,2 Stanley J Berman,3 Alberto Malacarne,1 Amy Lapidow,4 Michael E Schatman,5,6 Ronald Kulich,1,7,* Ana-Maria Vranceanu2,*
1Department of Diagnostic Sciences, Tufts University School of Dental Medicine, Boston, MA, USA; 2Department of Psychiatry, Massachusetts General Hospital, Harvard School of Medicine, MA, USA; 3Department of Clinical Health Psychology, William James College, MA, USA; 4Department of Health Sciences Library, Tufts University School of Dental Medicine, Boston, MA, USA; 5Department of Public Health and Community Medicine, Tufts University School of Medicine, Boston, MA, USA; 6Research and Network Development, Boston PainCare, Waltham, MA, USA; 7Department of Anesthesia, Massachusetts General Hospital, Harvard School of Medicine, MA, USA
*These authors contributed equally to this work
Purpose: The importance of improved physical function as a primary outcome in the treatment of chronic pain is widely accepted. There have been limited attempts to assess the effects mindfulness skills training (MST) has on objective outcomes in chronic pain care.
Methods: This systematic review evaluated published reports of original randomized controlled trials that described physical function outcomes after MST in the chronic pain population and met methodological quality according to a list of predefined criteria. PRISMA criteria were used to identify and select studies, and assess their eligibility for inclusion. The established guidelines for best practice of systematic reviews were followed to report the results.
Results: Of the 2,818 articles identified from the original search of four electronic databases, inclusionary criteria were met by 15 studies published as of August 10, 2015, totaling 1,199 patients. All included studies used self-report measures of physical function, and only two studies also employed performance-based measures of function. There were wide variations in how physical function was conceptualized and measured. Although the quality of the studies was rated as high, there was inconclusive evidence for improvement in physical function assessed by self-report due to contradiction in individual study findings and the measures used to assess function. Strong evidence for lack of improvement in physical function assessed via performance-based measures was found.
Conclusion: This review draws attention to the importance of having a unified approach to how physical function is conceptualized and assessed, as well as the importance of using quality performance-based measures in addition to subjective self-reports that appropriately assess the physical function construct within MSTs for chronic pain.
Keywords: mindfulness, chronic pain, physical functioning, systematic review, outcome measures, activity trackers
Introduction
Pain is a complex and multidimensional construct, and evidence supporting the biopsychosocial model indicates that psychological factors are unique determinants of the pain experience, above and beyond medical diagnosis.1,2 For example, for many chronic pain conditions, tissue damage is often uncorrelated with self-reported disability and pain intensity.3 Conversely, psychosocial factors, such as pain-related fear, have consistently been associated with pain intensity, disability, and the worsening of chronic pain over time.4 Researchers and clinicians have also come to recognize that achieving pain relief may be less important than improving physical functioning as a means of reducing health care costs and utilization and improving productivity and quality of life among pain patients.3,5 Thus, over the last decade, and in an effort to improve long-term chronic pain outcomes, psychosocial treatments have evolved toward acceptance of pain and increased function regardless of reported pain intensity. These interventions show durability in follow-up assessments and target key outcome variables with greater patient satisfaction.6–8
Cognitive behavioral approaches to pain treatment are efficacious in the treatment of chronic pain, producing short-term improvements in reported pain intensity and disability (small effect sizes), mood and pain catastrophizing with moderate effect sizes.9 Although psychosocial approaches to pain care have had an effect on key outcomes including physical functioning, a limitation of cognitive behavioral approaches has been that effects on pain and physical functioning tend to dissipate within 6–12 months after treatment concludes.10
More recently, acceptance and mindfulness-based interventions have been developed for the treatment of chronic pain. A primary goal of these interventions, including Acceptance and Commitment Therapy and Mindfulness Based Stress Reduction (MBSR), is to cultivate the patient’s ability to accept and observe experiences in the present moment (eg, pain) in a nonjudgmental manner (eg, without reactive cognitions and resulting negative affect). As such, acceptance and mindfulness-based interventions focus on improving overall well-being and psychological outcomes through developing accepting and stable, nonreactive states of mind.7,8,11,12
Although mindfulness-based interventions show considerable promise for the treatment of chronic pain, to our knowledge, no systematic reviews have sought to address the effects of MST on physical functioning. This represents an important gap in the literature for several reasons. First, the IMMPACT has identified physical function as a necessary outcome in clinical trials involving chronic pain.13 This is consistent with the growing emphasis on improving function and reducing pain-related disability rather than focusing solely on pain reduction as a primary treatment target. Second, prior reviews of psychosocial pain interventions have tended to focus on psychological outcomes or general health outcomes, neglecting a detailed analysis of physical function.14 Indeed, the construct of physical function is multidimensional and includes both objective (eg, impairment in range of motion) and subjective (eg, self-reported disability) measures of functioning.15 Although researchers tend to rely on subjective, self-report measures of physical function, there is evidence to suggest that objective measures (eg, accelerometer tracking) have the potential to more accurately capture physical activity and performance.16 Therefore, a systematic review that examines the effects of MSTs on both self-report and objective measures of physical function is needed to advance the field and inform future intervention development.
The purpose of this systematic review was to identify the effects of MSTs on physical functioning using findings derived from RCTs conducted among persons with chronic pain. This review also aimed to summarize the instruments used to assess physical function in the current literature and reveal the suspected lack of objective or performance-based measures of physical function compared to the more commonly used self-report measures.
The range of studies included in this systematic review was initially limited to those conducted before 2016. Since the original search, there has been no adaptation of performance-based measures used in the chronic pain literature. A brief review of current studies revealed that the data discovered in the original search has maintained its relevance. To address the limitations of the original search and highlight the continued lack of adaptation to a more comprehensive assessment of physical function, the results of a representative number of recent systematic reviews performed after the original search have been summarized.
Methods
We followed the PRISMA criteria17,18 to identify and select studies, and assess their eligibility for inclusion in this systematic review. We followed recommendations for establishing best practice evidence in chronic pain systematic reviews18 to report the results.
Search strategy
Reports of original research studies investigating the effects of MSTs on physical function in the chronic pain population were identified for the review. Articles published in peer-reviewed journals as of August 10, 2015 were identified via searches of four electronic databases (ie, PubMed, PsychINFO, EMBASE, and Web of Science). Two health science librarians with expertise in complex electronic database searches were consulted to develop a comprehensive search for individual databases, and complete search criteria are available on request. A total of 2,818 study abstracts were initially retrieved. A total of 706 duplicate records were identified, resulting in the removal of 353 study records in order to retain each study only once. One study was eliminated because no abstract was available, resulting in 2,464 studies that were screened by abstract for selection criteria.
Inclusion/exclusion criteria
Inclusion and exclusion criteria were determined a priori by the study authors. Studies were required to report results of an RCT of an MST vs a control intervention. Inclusion criteria for MSTs were that 1) the intervention lasted at least 4 weeks; 2) the intervention provided MST in which regular mindfulness practice was expected (eg, MBSR, mindfulness-based cognitive therapy); 3) participants were at least 18 years of age; and 4) participants had chronic non-cancer pain. Studies were excluded if they did not report at least one measure of physical function pre- and post-intervention.
Study selection
The study selection process is presented in Figure 1. Abstracts were evaluated independently for eligibility by two reviewers who are authors on the paper (WJ and AM), and disagreements were resolved upon discussion (κ=0.93). Because many studies could have been excluded for more than one reason, a hierarchy of exclusion criteria was used to enhance interrater reliability. Studies were excluded by predefined population, intervention, outcome, study design, and other criteria (ie, systematic reviews, commentary, etc). A log of excluded studies along with reasons for their rejection is available upon request. Review of retrieved abstracts resulted in exclusion of 2,406 studies. Primary reasons for exclusion were that the studies were not RCTs of MSTs (K=1,102) or were not conducted in an adult non-cancer chronic pain population (K=1,100). A total of 58 articles were retrieved for full-text review, and 43 additional articles were subsequently excluded. The most common reason for exclusion after full-text review was that the study did not provide a measure of physical function (K=29). A total of 15 articles were included in the final analysis (Table 1).
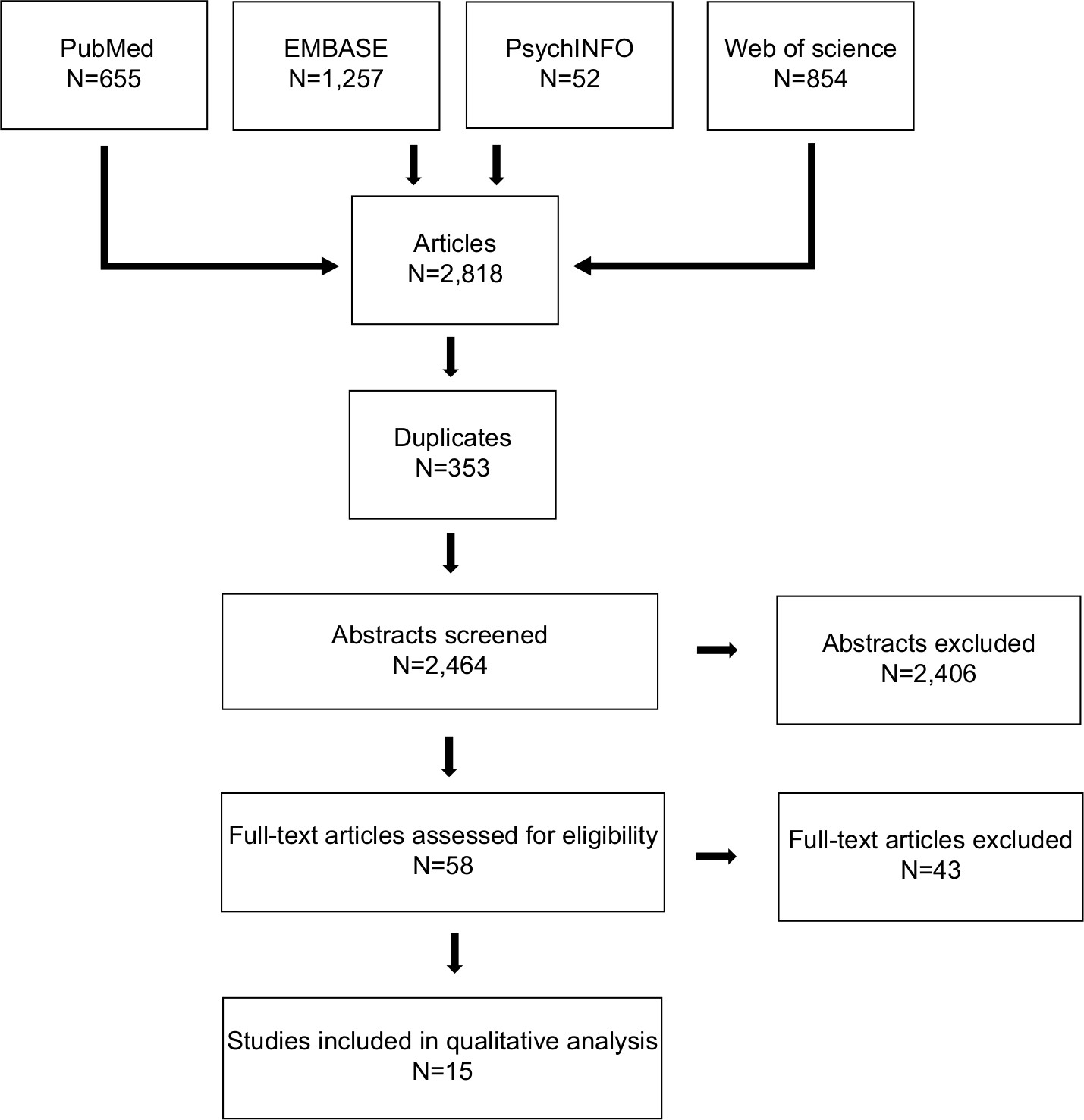 | Figure 1 Flowchart of this systematic review showing the process of search, exclusion of studies, and inclusion of studies for quality assessment and extraction of data. |
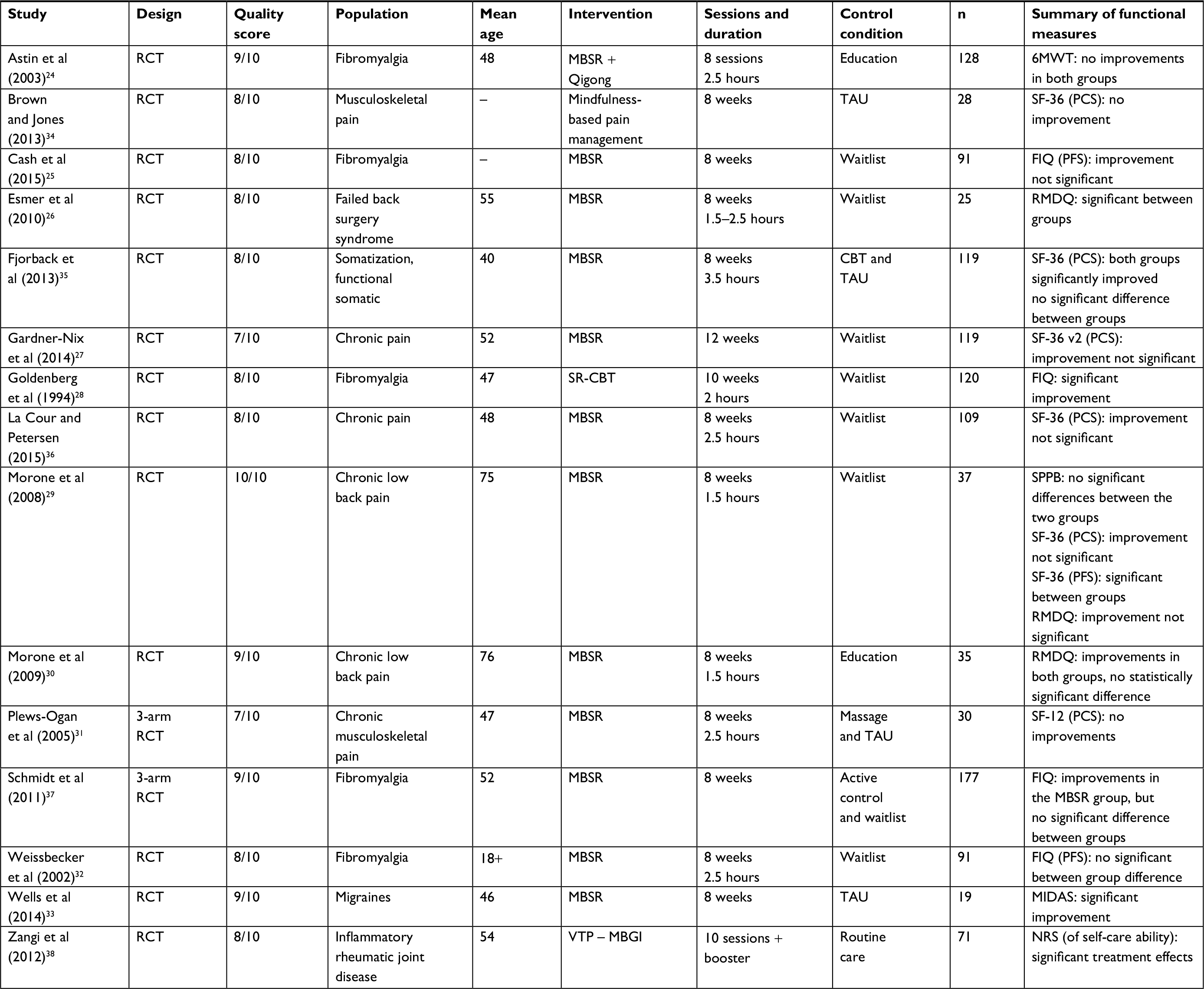 | Table 1 Characteristics of selected studies Note: Quality rating was based on predefined 10-point criteria. Abbreviations: CBT, cognitive behavioral therapy; FIQ, Fibromyalgia Impact Questionnaire; FIQ (PFS), physical functioning scale of FIQ; MBSR, mindfulness-based stress reduction; MIDAS, migraine disability assessment; NRS, 10-point numeric rating scale; RCT, randomized controlled trial; RMDQ, Roland Morris Disability Questionnaire; SF-36 (PCS), physical component scale of SF-36; SF-36 v2 (PCS), physical component scale of SF-36 version 2; SF-36 (PFS), physical functioning scale of SF-36; SPPB, short physical performance battery; SR-CBT, stress reduction cognitive behavioral therapy; TAU, treatment as usual; VTP – MBGI, vitality training programme – mindfulness-based group intervention. |
Data extractions and quality assessment
Two independent reviewers (WJ and AM) extracted the following variables: study design, population, study location, participant age, type of intervention, duration of treatment, control condition, sample size, physical function measure, and changes in physical function from pre- to post-intervention. Complete study characteristics are presented in Table 1. Methodological quality was assessed with a standardized 10-item checklist using previously established criteria for systematic reviews,19,20 which were modified by the authors for the chronic pain population. Complete criteria for quality assessment are presented in Table 2. Each criterion was worth 1 point if fulfilled. Each criterion that was not fulfilled or sufficiently addressed in the manuscript was awarded 0 point. A total quality score was generated by summing the number of points awarded and dividing by 10. The maximum score was 100%. Studies that scored 70% or more were considered to be of “high quality”, studies that scored 50% or 60% were considered to be of “moderate quality”, and studies that scored 40% or below were considered to be of “low quality”. Findings regarding functional assessment and outcomes were summarized according to level of evidence.19 Consistent with previously determined criteria,21 and prior systematic reviews,22,23 level of evidence is considered “strong” when findings are consistent in at least two high-quality studies. The level of evidence is considered “moderate” if findings are consistent in one high-quality study and at least one moderate- or low-quality study. The level of evidence is considered “weak” if findings are present in one high-quality study or at least three or more low-quality studies and “inconclusive” if findings are inconsistent or less than three low-quality studies are available.
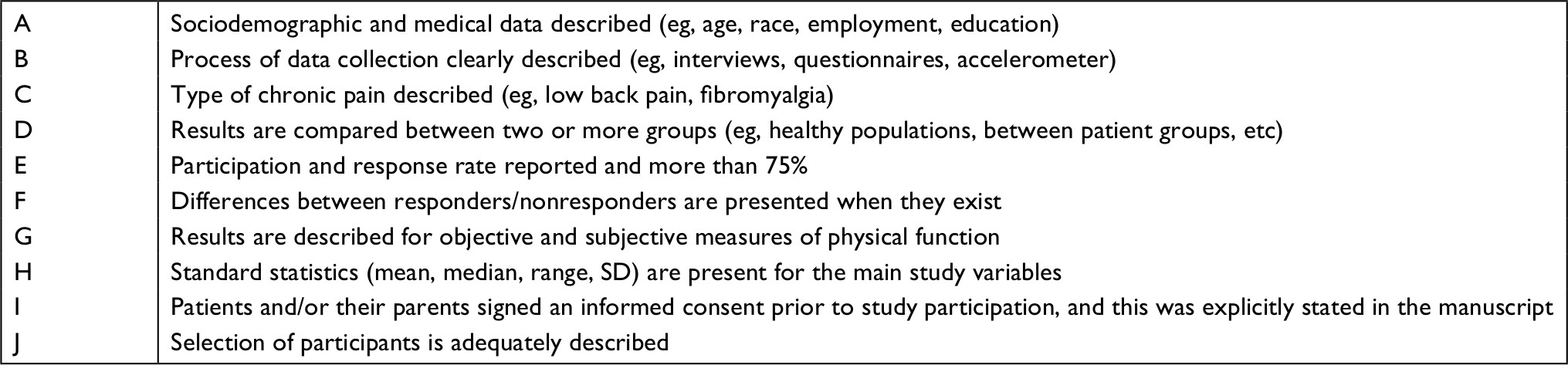 | Table 2 10-Item quality assessment Notes: The studies that have met inclusion criteria for this systematic review were assessed for quality using the above criteria. A study that meets criteria for a particular category was given 1 point with 10 points (100%) being the maximum score. This quality assessment was Adapted by permission from Springer Nature Customer Service Centre GmbH: Springer Nature Journal of Neuro-Oncology Vranceanu AM, Merker VL, Park E, Plotkin SR. Quality of life among adult patients with neurofibromatosis 1, neurofibromatosis 2 and schwannomatosis: a systematic review of the literature. J Neurooncol. 2013;114(3):257–262, © 2013.22 |
Results
Characteristics of included studies
A total of 15 studies were included (Table 1). All studies were RCTs published between 1994 and 2015. Studies were conducted in several countries including 10 in the USA,24–33 one in the UK,34 two in Denmark,35,36 one in Germany,37 and one in Norway.38 Of the 15 studies, five included participants with fibromyalgia,24,25,28,32,37 two included participants with mixed “chronic pain”,27,36 three included participants with chronic back pain,26,29,30 two included participants with unspecified chronic musculoskeletal pain,31,34 one included participants with chronic migraine,33 one included participants with somatization and functional somatic disorders,35 and one included participants with inflammatory rheumatic joint disease.38 Sample sizes varied considerably across studies such that the smallest sample size was 1933 and the largest was 177.37 Nearly half (K=7) of the studies compared a mindfulness-based intervention to a waitlist control,25–29,32,36 two studies utilized a TAU control condition,33,34 three studies utilized a three-arm design with an active control condition (eg, massage) and either a TAU control or waitlist condition,31,35,37 and two studies used an education control condition.24,30
Quality of included studies
All studies included were considered to be of high quality, with scores of 100% (one study),29 90% (four studies),24,30,33,37 80% (eight studies),25,26,28,32,34–36,38 and 70% (two studies).27,31 Examination of individual criteria indicated that only two studies24,29 included both performance-based and self-report measures of physical functioning, whereas all remaining studies (K=13) included only subjective physical function measures (criterion G). Although most studies addressed some aspect of patient demographics (criterion A), two studies did not do so.25,34 Four of the included studies did not reach a participation response rate of 75% or above (criterion E).24,26,27 Three studies did not report differences between responders and nonresponders (criterion F).31–33
Use of self-report measures of physical functioning
All 15 studies had at least one measure of self-reported physical function. The most frequently utilized self-report measures of physical function were derived from three versions of the Short-Form Health Survey, which was designed to assess general health-related quality of life and has been validated for use across broad populations.39 The 36-item measure (SF-36) yields a PCS, which comprises 21 items that assess role limitations due to physical problems, energy/fatigue, bodily pain, and general health perceptions,39–41 and a PFS, which comprises 10 items that assess limitations in physical function.39 The 12-item abbreviated measure (SF-12) also yields a PCS, which assess abilities to accomplish activities of daily living. Five studies used the SF-36 (PCS),27,29,34–36 one study used the SF-36 (PFS),29 and one study used the SF-12 (PCS).31
Whereas the SF-36 and SF-12 are generic measures that can be utilized across populations with various diseases or conditions, several studies used disease-specific measures to assess the impact of a specific disease on participants’ physical functioning. Four studies assessed physical functioning among participants with fibromyalgia using either the FIQ total score28,37 or the PFS score.25,32 The RMDQ was used in three studies26,29,30 to assess limitations in physical functioning related to low back pain.42 Finally, the Migraine Disability Assessment43 was used in one study33 to assess limitations in physical functioning due to migraines. Although IMMPACT guidelines recommend use of both generic and disease-specific measures, only two studies used both a generic measure and a disease-specific measure.24,30
Use of performance-based measures of physical functioning
Only two studies assessed physical function using performance-based measures.24,29 Specifically, one study utilized the 6MWT,24 which measures the maximum distance a patient can walk during a 6-minute interval and has been validated for use across broad populations.44–47 The other study that included a performance-based measure utilized the SPPB,29 which assesses patients’ standing balance, gait speed, and ability to rise from a chair. The test can be reliably performed by a trained lay observer and takes approximately 10–15 minutes to administer.48
Description of MST interventions
The majority of studies (11/15) tested the MBSR25–27,29–33,35–37 intervention. Ten of the MBSR studies utilized eight sessions,25,26,29–33,35–37 while one27 was conducted over 12 sessions. MBSR defines the practice of mindfulness as “the awareness that emerges through paying attention on purpose, in the present moment, and nonjudgmentally to the unfolding of experience moment by moment”.49 When applied to the treatment of chronic pain conditions, MBSR teaches skills for acceptance of pain sensations and pain-related thoughts.8 MBSR is traditionally delivered in groups, and includes 30 hours of in-session experiential learning, including sitting meditation and mindfulness movement with intensive meditation practice between group sessions (at least 45 minutes per day, 6 days per week).50 One study24 utilized MBSR + Qigong, which is an ancient Chinese practice of performing gentle, non-aerobic movements with mindfulness. One study28 utilized an SR-CBT program modeled after the MBSR curriculum with ten 2-hour education and practice sessions and 40 minutes of daily home meditation practice.28 One study38 utilized a mindfulness-based pain management group intervention, the VTP, consisting of a 11-session mindfulness-based curriculum that required participants to practice mindfulness-based meditations between sessions.
Effect of MST on self-reported physical functioning
Five studies demonstrated greater improvement in self-reported physical functioning among participants who received an MST vs control.26,28,29,33,38 Three of the five studies26,28,29 utilized a waitlist control group, whereas the other two studies33,38 utilized a usual care control group. Three studies26,29,30 were conducted among patients with back pain, one study28 was conducted among patients with fibromyalgia, one study33 was conducted among patients with migraines, and one study was conducted among patients with inflammatory rheumatic joint disease.38 Four studies utilized an 8-week MBSR intervention as their active condition,26,29,30,33 while one study utilized a 10-week SR-CBT program28 and one study utilized an 11-session VTP – Mindfulness-Based Group Intervention.38 The self-report assessments were not consistent across studies, with three reporting improvements in disease-specific physical functioning26,28,33 and two reporting improvements in general physical function.29,38 Of note, one study29 utilized both general and disease-specific measures of physical functioning, and found only a significant improvement in physical functioning when measured with the SF-36 (PFS).
Ten studies did not observe significant differences in physical functioning when MST was compared to the control group.24,25,27,30–32,34–37 Examination of within-group changes revealed that patients who received MST demonstrated improvements in physical functioning from pre- to post-intervention in six studies.25,27,30,35–37 All six studies that observed within-group improvements in self-reported physical functioning tested an 8-week MBSR intervention, with three of these studies utilizing a waitlist control,25,27,36 two studies utilized an active control,30,35 and one study37 utilized a three-arm design that included both an active and a waitlist control. Three studies utilized the SF-36 as a general measure of physical functioning.27,35,36 Three studies were conducted among patients with chronic pain,27,30,36 two studies were conducted among patients with fibromyalgia,25,37 and one study was conducted among patients with chronic discomfort categorized as “functional somatic disorder”.35 Taken together, these findings show inconclusive evidence for the effects of MST on self-reported physical function.
Effect of MST on performance-based measures of physical functioning
Of the two studies that utilized performance-based assessments of physical function, neither observed improvement in physical function when MST was compared to a control.24,29 Specifically, one study conducted among patients with fibromyalgia did not observe differences in the 6MWT among patients who completed eight sessions of MBSR + Qigong vs Education. Although Morone et al29 observed improvements in self-reported functioning (SF-36) after eight sessions of MBSR (vs waitlist control) in patients with chronic low back pain, these results were not replicated by the SPPB. Thus, no RCTs in the current study demonstrated a significant effect of MST on performance-based measures of physical functioning.
Discussion
This systematic review summarized RCTs that tested the effects of MSTs on self-reported and performance-based measures of physical function. As evidenced by the large number of studies extracted for this review, mindfulness approaches clearly have a major presence in the research and clinical pain literature. However, we identified only 15 RCTs that assessed physical functioning. The absence of attention to physical functioning across RCTs of MSTs was surprising given the critical importance of physical functioning as a pain management outcome.2,51,52 Indeed, IMMPACT recommendations53 indicate that all RCTs for chronic pain should assess physical functioning, yet less than 1% of MST RCTs were eligible for inclusion in this review, suggesting inherent weaknesses in the investigations on this topic conducted to date.
Recent systematic reviews of mindfulness and chronic pain have conflicting results. As of August 5, 2018, the most recent systematic reviews on mindfulness with chronic pain54–58 reveal one review reporting no clinically significant effect of MST on physical quality of life in a mixed chronic pain population,57 one reporting time-limited subminimal clinically significant difference with low back population,55 and one reporting a significant effect on physical health-related quality of life.58 Other reviews neglected to report on physical function or summarize the results.54,56 More to the point of this review, as of 2018, a brief review of these five systematic reviews54–58 of mindfulness interventions in chronic pain published after our original search reveals no new RCTs that include functional measures beyond that assessed by questionnaires such as the RMDQ and the Owestry Disability Questionnaire. No new studies included performance-based measures or tracking of physical activity despite the widespread use of activity trackers such as the Fitbit.
Results of the current review provide inconclusive evidence for the efficacy of MSTs for improving physical functioning. Although five studies found that MST improved physical functioning compared to waitlist control (K=3) or usual care (K=2), 10 studies did not observe significant differences in MST vs control interventions. Potential explanations for these inconsistent findings include small sample sizes and variations in assessment tools. Prior research has demonstrated that at least 30 participants are needed per group in order to generate stable estimates of change.59–62 However, sample sizes of six studies were less than 40. Likewise, there was no measure of physical function that was used consistently across studies. Even studies that assessed general physical function via the Short-Form Health Survey (K=7) did not consistently utilize the same version or subscale.
Among studies that observed significant improvement in physical functioning after MST, results indicate that patients with multiple pain conditions, including chronic back pain, fibromyalgia, migraines, and inflammatory rheumatic diseases, may benefit from MST. Additional research is needed to better understand potential moderators that could influence the efficacy of MST interventions for improving physical functioning. As noted above, studies were not consistent in their evaluations of physical functioning, and only two studies utilized performance-based measures. Additional research is needed to assess whether MSTs improve some aspects of physical functioning over others. Although a single study did not observe an effect of MST on performance during a 6MWT among patients with fibromyalgia, it is possible that the 6MWT did not capture changes in functioning which could have otherwise been observed via other measures. For example, the 6MWT may have been limited by other factors, such as participants’ cardiovascular endurance or motivation to perform optimally, which would not have been targeted by an MST. It is also not clear to what extent performance on laboratory-based physical activity assessments reflect abilities to complete activities of daily living. It is possible that ongoing measures of activity in natural environments (eg, via Actigraph recordings of physical activity) may provide the best assessment of real-time changes in physical activity following MSTs. Indeed, real-time digital monitoring devices like the Fitbit also show adherence rates as high as 95%63 and an error rate as low as 10.1%.64
Consistent with IMPAACT recommendations,53 future research should utilize a comprehensive assessment battery comprising general and disease-specific self-report measures as well as performance-based assessment of physical function. A recent systematic review16 of 187 studies indicated that self-reported activity is only moderately correlated with performance-based measurement (eg, activity measured via accelerometer). Of note, only one study included in the current review administered both self-report and performance-based physical functioning assessments. In that study, MST significantly improved physical functioning as measured by the SF-36 (PFS), but not the 6MWT. Although conclusions cannot be drawn from a single study, the lack of concordance between self-report and performance-based measures should receive future attention. In a 2013 systematic review, the authors noted that false-negative diagnoses of submaximal capacities in FCEs highlight the need for multimodal assessment.65 Argument against using certain FCEs and other performance measures in research (as well as, perhaps, clinically) can be made from results of a very recent systematic review that noted considerable variance in the psychometric properties of the different FCE systems.66 However, a multimodal approach with validated measures in future research has a degree of potential to fully capture any effects of MSTs on physical functioning.
Conclusion
Given the inconsistent findings observed in the current review, it is possible that MSTs do not effectively target physical behavior change,8,67 and should be adapted to explicitly address physical functioning among patients with chronic pain. Mindfulness can be conceptualized as a primarily cognitive practice, in that it involves the purposeful control of attention to foster nonjudgmental awareness of the present moment. Patients are encouraged to use mindfulness in order to participate fully in the present moment, which may involve mindful participation in physical activities. Although MSTs teach patients to observe negative pain thoughts (eg, “I can’t move because it hurts”) without acting on them, it is possible that additional skills training is necessary to further change patients’ behavior after mindfully observing maladaptive pain thoughts.
Results of the current review should be interpreted in light of several limitations. Although the studies included in this review were of high quality based on established criteria for systematic reviews,22 there were several study limitations that may not have been captured by our quality rating scale. Three of the studies that showed improvement in functioning had a relatively small sample size (n≤37) with less than 15 completers in each group. Means and standard errors were not stable with such small samples,59–62 decreasing confidence that results would be maintained in a properly powered larger study. The remaining studies used measures that may have been less accurate for assessing physical function. For example, the FIQ assesses physical functioning as part of the larger construct of quality of life, and the measure includes psychological items as well.28 A second study used a measure of physical function (10-point Numeric Rating Scale of self-care ability) that had not been previously validated.10 Additionally, there were only two studies that assessed performance-based measures of physical function, and neither study utilized the same measure. Thus, we are unable to draw conclusions about effects of MSTs on specific areas of functioning.
IMMPACT guidelines recommend a move toward common, validated self-reported outcome measures. As evidenced by the variety of self-report measures used for physical function in this review, the transition has been slow. The PROMIS, an initiative funded by the National Institutes of Health, has made progress toward creating common, self-report measures that can be used and compared across populations, but none of the studies included in this review used PROMIS measures. Common measures with sufficient reliability and validity of this sort may provide opportunities for comparisons across studies and ease aggregation of data to support clinical decision making.
Given the increased focus on mindfulness approaches in the management of chronic pain and the strong evidence supporting the importance of improved physical function in pain treatment, the field of mindfulness-based treatment has an opportunity to better target function and systematically measure objective performance outcomes. Findings from this study show that the effects of MSTs on physical function in chronic pain have not been thoroughly assessed and need to be evaluated in future RCTs. With improving cost-effective technology, opportunities to employ interactive measures that reinforce function and measure objective improvement are increasingly available. Future research should examine the effects of MST on self-reported and performance-based outcome measures, and studies that assess MSTs adapted to target physical functioning are also warranted.
Abbreviations
FCEs, functional capacities evaluations
FIQ, Fibromyalgia Impact Questionnaire
IMMPACT, Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials
MBSR, Mindfulness-Based Stress Reduction
MST, mindfulness skills training
PCS, physical component scale
PFS, physical functioning scale
PROMIS, Patient Reported Outcome Measurement Information System
RCT, randomized controlled trial
RMDQ, Roland Morris Disability Questionnaire
SPPB, short physical performance battery
SR-CBT, stress reduction-cognitive behavioral therapy
TAU, treatment as usual
VTP, Vitality Training Programme
Acknowledgments
Frederick Jackson provided copy editing support. David Haddad Psy.D. provided conceptual support. Consulting scientific librarian Matthew Kramer, MLIS, aided in the organization of search strategy and research data, and access to electronic databases. The abstract of this paper was presented at the American Pain Society Annual Meeting in Austin, TX, USA, on May 11–14, 2016, as a poster presentation with interim findings. The poster’s abstract was published in “Poster Abstracts” in the Journal of Pain: https://www.jpain.org/article/S1526-5900(16)00334-5/pdf.
Disclosure
The authors report no conflicts of interest in this work.
References
Den Boer JJ, Oostendorp RA, Beems T, Munneke M, Evers AW. Continued disability and pain after lumbar disc surgery: the role of cognitive-behavioral factors. Pain. 2006;123(1–2):45–52. | ||
Turk DC, Okifuji A. Psychological factors in chronic pain: evolution and revolution. J Consult Clin Psychol. 2002;70(3):678–690. | ||
Severeijns R, Vlaeyen JW, van den Hout MA, Weber WE, Severeijns R. Pain catastrophizing predicts pain intensity, disability, and psychological distress independent of the level of physical impairment. Clin J Pain. 2001;17(2):165–172. | ||
Eccleston C. Role of psychology in pain management. Br J Anaesth. 2001;87(1):144–152. | ||
Pincus T, Burton AK, Vogel S, Field AP. A systematic review of psychological factors as predictors of chronicity/disability in prospective cohorts of low back pain. Spine (Phila Pa). 1976;27(5):109–120. | ||
Cherkin DC, Sherman KJ, Balderson BH, et al. Effect of mindfulness-based stress reduction vs cognitive behavioral therapy or usual care on back pain and functional limitations in adults with chronic low back pain: a randomized clinical trial. JAMA. 2016;315(12):1240. | ||
Veehof MM, Oskam MJ, Schreurs KM, Bohlmeijer ET. Acceptance-based interventions for the treatment of chronic pain: a systematic review and meta-analysis. Pain. 2011;152(3):533–542. | ||
Wetherell JL, Afari N, Rutledge T, et al. A randomized, controlled trial of acceptance and commitment therapy and cognitive-behavioral therapy for chronic pain. Pain. 2011;152(9):2098–2107. | ||
Astin JA, Beckner W, Soeken K, Hochberg MC, Berman B. Psychological interventions for rheumatoid arthritis: a meta-analysis of randomized controlled trials. Arthritis Rheum. 2002;47(3):291–302. | ||
Williams AC, Eccleston C, Morley S. Psychological therapies for the management of chronic pain (excluding headache) in adults. Cochrane Database Syst Rev. 2012;11:CD007407. | ||
Grabovac AD, Lau MA, Willett BR. Mechanisms of mindfulness: A Buddhist psychological model. Mindfulness. 2011;2(3):154–166. | ||
Hölzel BK, Lazar SW, Gard T, Schuman-Olivier Z, Vago DR, Ott U. How does mindfulness meditation work? Proposing mechanisms of action from a conceptual and neural perspective. Perspect Psychol Sci. 2011;6(6):537–559. | ||
Turk DC, Dworkin RH, Allen RR, et al. Core outcome domains for chronic pain clinical trials: IMMPACT recommendations. Pain. 2003;106(3):337–345. | ||
Gotink RA, Chu P, Busschbach JJ, Benson H, Fricchione GL, Hunink MG. Standardised mindfulness-based interventions in healthcare: an overview of systematic reviews and meta-analyses of RCTs. PLoS One. 2015;10(4):e0124344. | ||
WHO. World Report on Disability. Geneva: WHO; 2011. | ||
Prince SA, Adamo KB, Hamel ME, Hardt J, Connor Gorber S, Tremblay M. A comparison of direct versus self-report measures for assessing physical activity in adults: a systematic review. Int J Behav Nutr Phys Act. 2008;5(1):56. | ||
Moher D, Liberati A, Tetzlaff J, Altman DG, Group TP, PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097. | ||
Moore RA, Eccleston C, Derry S. AWG of the ISIG on SR in PR and others. Palliative and supportive care systematic review group editors:“Evidence” in chronic pain-establishing best practice in the reporting of systematic review. Pain. 2010;150:386–389. | ||
Kuijpers T, van der Windt DA, van der Heijden GJ, Bouter LM. Systematic review of prognostic cohort studies on shoulder disorders. Pain. 2004;109(3):420–431. | ||
Scholten-Peeters GG, Verhagen AP, Neeleman-van der Steen CW, Hurkmans JC, Wams RW, Oostendorp RA. Randomized clinical trial of conservative treatment for patients with whiplash-associated disorders: considerations for the design and dynamic treatment protocol. J Manipulative Physiol Ther. 2003;26(7):412–420. | ||
Ariëns GA, van Mechelen W, Bongers PM, Bouter LM, van der Wal G, van MW, der Wgvan. Physical risk factors for neck pain. Scand J Work Environ Health. 2000;26(1):7–19. | ||
Vranceanu AM, Merker VL, Park E, Plotkin SR. Quality of life among adult patients with neurofibromatosis 1, neurofibromatosis 2 and schwannomatosis: a systematic review of the literature. J Neurooncol. 2013;114(3):257–262. | ||
Vranceanu AM, Merker VL, Park ER, Plotkin SR. Quality of life among children and adolescents with neurofibromatosis 1: a systematic review of the literature. J Neurooncol. 2015;122(2):219–228. | ||
Astin JA, Berman BM, Bausell B, Lee WL, Hochberg M, Forys KL. The efficacy of mindfulness meditation plus Qigong movement therapy in the treatment of fibromyalgia: a randomized controlled trial. J Rheumatol. 2003;30(10):2257–2262. | ||
Cash E, Salmon P, Weissbecker I, et al. Mindfulness meditation alleviates fibromyalgia symptoms in women: results of a randomized clinical trial. Ann Behav Med. 2015;49(3):319–330. | ||
Esmer G, Blum J, Rulf J, Pier J. Mindfulness-based stress reduction for failed back surgery syndrome: a randomized controlled trial. J Am Osteopath Assoc. 2010;110(11):646–652. | ||
Gardner-Nix J, Barbati J, Grummitt J, Pukal S, Raponi Newton R. Exploring the effectiveness of a mindfulness-based chronic pain management course delivered simultaneously to on-site and off-site patients using telemedicine. Mindfulness. 2014;5(3):223–231. | ||
Goldenberg DL, Kaplan KH, Nadeau MG, Brodeur C, Smith S, Schmid CH. A controlled study of a stress-reduction, cognitive-behavioral treatment program in fibromyalgia. J Musculoskelet Pain. 1994;2(2):53–66. | ||
Morone NE, Greco CM, Weiner DK. Mindfulness meditation for the treatment of chronic low back pain in older adults: a randomized controlled pilot study. Pain. 2008;134(3):310–319. | ||
Morone NE, Rollman BL, Moore CG, Li Q, Weiner DK. A mind-body program for older adults with chronic low back pain: results of a pilot study. Pain Med. 2009;10(8):1395–1407. | ||
Plews-Ogan M, Owens JE, Goodman M, Wolfe P, Schorling J. A pilot study evaluating mindfulness-based stress reduction and massage for the management of chronic pain. J Gen Intern Med. 2005;20(12):1136–1138. | ||
Weissbecker I, Salmon P, Studts JL, Floyd AR, Dedert EA, Sephton SE. Mindfulness-based stress reduction and sense of coherence among women with fibromyalgia. J Clin Psychol Med Settings. 2002;9(4):297–307. | ||
Wells RE, Burch R, Paulsen RH, Wayne PM, Houle TT, Loder E. Meditation for migraines: a pilot randomized controlled trial. Headache. 2014;54(9):1484–1495. | ||
Brown CA, Jones AK. Psychobiological correlates of improved mental health in patients with musculoskeletal pain after a mindfulness-based pain management program. Clin J Pain. 2013;29(3):233–244. | ||
Fjorback LO, Carstensen T, Arendt M, Ørnbøl E, Walach H, Rehfeld E. Mindfulness therapy for somatization disorder and functional somatic syndromes: analysis of economic consequences alongside a randomized trial ✩. J Psychosom Res. 2013:1–8. | ||
La Cour P, Petersen M. Effects of mindfulness meditation on chronic pain: a randomized controlled trial. Pain Med. 2015;16(4):641–652. | ||
Schmidt S, Grossman P, Schwarzer B, Jena S, Naumann J, Walach H. Treating fibromyalgia with mindfulness-based stress reduction: results from a 3-armed randomized controlled trial. Pain. 2011;152(2):361–369. | ||
Zangi HA, Mowinckel P, Finset A, et al. A mindfulness-based group intervention to reduce psychological distress and fatigue in patients with inflammatory rheumatic joint diseases: a randomised controlled trial. Ann Rheum Dis. 2012;71(6):911–917. | ||
Ware JE, Kosinski M, Keller SD. SF-36 Physical and Mental Health Summary Scales: A User’s Manual. Boston, MA: Heath Institute, New England Medical Center; 1994. | ||
Ware J, Kosinski M, Keller SD. A 12-Item Short-Form Health Survey: construction of scales and preliminary tests of reliability and validity. Med Care. 1996;34(3):220–233. | ||
John E. WJP. SF-36 health survey update. Spine. 2000;25(24):31303139. | ||
Roland M, Fairbank J. The roland–morris disability questionnaire and the oswestry. Spine. 2000;25(24):3115–3124. | ||
Stewart WF, Lipton RB, Dowson AJ, Sawyer J. Development and testing of the Migraine Disability Assessment (MIDAS) Questionnaire to assess headache-related disability. Neurology. 2001;56(6 Suppl 1):S20 LP-S28. | ||
Gibbons WJ, Fruchter N, Sloan S, Levy RD. Reference values for a multiple repetition 6-minute walk tes. J Cardiopulm Rehabil Prev. 2001;21(2):87–93. | ||
Balke B. A simple field test for the assessment of physical fitness. Oklahoma, OK: Civil Aeromedical Research Institute; 1963. Available from: https://rosap.ntl.bts.gov/view/dot/20899. Accessed March 19, 2018. | ||
Bohannon RW, Test S-Minutewalk. Top Geriatr Rehabil. 2007;23(2):155–160. | ||
King SJ, Wessel J, Bhambhani Y, Sholter D, Maksymowych W. The effects of exercise and education, individually or combined, in women with fibromyalgia. J Rheumatol. 2002;29(12):2620–2627. | ||
Guralnik JM, Simonsick EM, Ferrucci L, et al. A short physical performance battery assessing lower extremity function: association with self-reported disability and prediction of mortality and nursing home admission. J Gerontol. 1994;49(2):M85–M94. | ||
Kabat-Zinn J. Mindfulness-based interventions in context: past, present, and future. Am Psychol Assoc. 2003;10(N2):144–156. | ||
Santorelli SF. Mindfulness-based stress reduction standards of practice. 2014. Available from: https://www.umassmed.edu/contentassets/24cd221488584125835e2eddce7dbb89/mbsr_standards_of_practice_2014.pdf. Accessed November 11, 2018. | ||
Dworkin RH, Turk DC, Farrar JT, et al. Core outcome measures for chronic pain clinical trials: IMMPACT recommendations. Pain. 2005;113(1):9–19. | ||
Simmonds MJ, Olson SL, Jones S. Psychometric characteristics and clinical usefulness of phys. Spine. 1998;23(22):2412–2421. | ||
Dworkin RH, Turk DC, Farrar JT, et al. Core outcome measures for chronic pain clinical trials: IMMPACT recommendations. Pain. 2005;113(1–2):9–19. | ||
Ball EF, Nur Shafina Muhammad Sharizan E, Franklin G, Rogozin´ska E. Does mindfulness meditation improve chronic pain? A systematic review. Curr Opin Obstet Gynecol. 2017;29(6):359–366. | ||
Anheyer D, Haller H, Barth J, Lauche R, Dobos G, Cramer H. Mindfulness-based stress reduction for treating low back pain. Ann Intern Med. 2017;166(11):799. | ||
Hilton L, Hempel S, Ewing BA, et al. Mindfulness Meditation for Chronic Pain: Systematic Review and Meta-analysis. Ann Behav Med. 2017;51(2):199–213. | ||
Anheyer D, Leach MJ, Klose P, Dobos G, Cramer H. Mindfulness-based stress reduction for treating chronic headache: a systematic review and meta-analysis. Cephalalgia. 2018;333102418781795:333102418781795. | ||
Majeed MH, Ali AA, Sudak DM. Mindfulness-based interventions for chronic pain: evidence and applications. Asian J Psychiatr. 2018;32:79–83. | ||
Browne RH. On the use of a pilot sample for sample size determination. Stat Med. 1995;14(17):1933–1940. | ||
Lancaster GA, Dodd S, Williamson PR. Design and analysis of pilot studies: recommendations for good practice. J Eval Clin Pract. 2004;10(2):307–312. | ||
Shih WJ, Ohman-Strickland PA, Lin Y. Analysis of pilot and early phase studies with small sample sizes. Stat Med. 2004;23(12):1827–1842. | ||
Whitehead AL, Julious SA, Cooper CL, Campbell MJ. Estimating the sample size for a pilot randomised trial to minimise the overall trial sample size for the external pilot and main trial for a continuous outcome variable. Stat Methods Med Res. 2016;25(3):1057–1073. | ||
Cadmus-Bertram LA, Marcus BH, Patterson RE, Parker BA, Morey BL. Randomized trial of a fitbit-based physical activity intervention for women. Am J Prev Med. 2015;49(3):414–418. | ||
Lee J, Welk GJ. Validity of consumer-based physical activity monitors under free-living: 2549. Med Amp. 2011;43(5):700. | ||
van der Meer S, Trippolini MA, van der Palen J, Verhoeven J, Reneman MF. Which instruments can detect submaximal physical and functional capacity in patients with chronic nonspecific back pain? A systematic review. Spine. 2013;38(25):E1608–E1615. | ||
De Baets S, Calders P, Schalley N. Updating the evidence on functional capacity evaluation methods: a systematic review. J Occup Rehabil. 2017:1–11. | ||
Mccracken LM, Sato A, Taylor GJ. A trial of a brief group-based form of acceptance and commitment therapy (ACT) for chronic pain in general practice: pilot outcome and process results. J Pain. 2013;14(11):1398–1406. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.