Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 13
Physical Activity Interventions in Children with Juvenile Idiopathic Arthritis: A Systematic Review of Randomized Controlled Trials
Authors Iversen MD, Andre M, von Heideken J
Received 17 December 2021
Accepted for publication 25 March 2022
Published 14 April 2022 Volume 2022:13 Pages 115—143
DOI https://doi.org/10.2147/PHMT.S282611
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Roosy Aulakh
Maura D Iversen,1– 3 Marie Andre,2 Johan von Heideken2
1College of Health Professions, Sacred Heart University, Fairfield, CT, USA; 2Department of Women’s and Children’s Health, Karolinska Institutet, Stockholm, Sweden; 3Section of Clinical Sciences, Division of Immunology, Rheumatology & Immunity, Brigham & Women’s Hospital, Harvard Medical School, Boston, MA, USA
Correspondence: Maura D Iversen, College of Health Professions, Sacred Heart University, 5151 Park Avenue, Fairfield, CT, 06825, USA, Tel +1 203 396-8024, Fax +1 203-396-8025, Email [email protected]
Introduction: Children with juvenile arthritis (JA) experience pain, stiffness, fatigue, and decreased motion leading to difficulties with daily activities and low physical activity (PA). PA is critical to improve health and function and mitigate JA-associated symptoms. This study evaluated the evidence for PA interventions in children with JA.
Materials and Methods: A systematic review of randomized controlled trials (RCTs) of PA interventions in children with JA was conducted. Ovid (Medline), Cochrane Library, EMBASE, and CINAHL databases were searched for papers published in English between 1/1/1946 and 9/1/2021. Studies which concurrently assessed medical interventions were excluded. Participant and intervention characteristics and outcomes were extracted. Study internal validity and intervention attributes were assessed.
Results: A total of 555 studies were identified, with 13 studies from 10 countries included. Data from 672 children diagnosed with juvenile idiopathic arthritis (JIA) (range of mean ages, 8.7 to 16.1 years) were analyzed. Fifty-two percent of intervention arms incorporated strengthening exercise alone or combined with other exercise, with 61.9% performed 3x/week. About 43.5% of sessions lasted > 45 to ≤ 60 minutes and 65.2% of programs were ≥ 12 to < 28 weeks. PA interventions improved function and symptoms without adverse events. Intervention details were missing especially regarding PA intensity, reasons for dropouts, and adherence. Only two studies incorporated strategies to promote adherence.
Discussion: RCTs of PA interventions in JA only include JIA. Available RCTs used mixed modes of interventions. Reporting of PA interventions lacks sufficient detail to discern the dose-response relationship. Strategies to motivate engagement in PA and to support families to promote PA are lacking, as are studies of long-term outcomes.
Conclusion: There are limited RCTs of PA interventions in JIA. Adherence was better with low intensity programs. PA interventions for JIA yield positive health benefits but better reporting of PA intervention details is needed to generate more high-quality evidence and inform clinical practice.
Prospero Registration: Maura Iversen, Johan von Heideken, Marie Andre. Physical Activity in Children with Rheumatic Diseases: a systematic review. PROSPERO 2021 CRD42021274634 Available from: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42021274634.
Keywords: physical activity, juvenile idiopathic arthritis, exercise
Plain Language Summary
- Physical activity (PA) is an important component of juvenile idiopathic arthritis (JIA) management and may prevent long-term consequences of the disease.
- We reviewed studies which evaluated PA interventions for children with JIA to determine whether PA interventions provide positive health benefits.
- There is limited number of RCTs of PA in children with JIA and the majority of studies included children with polyarticular or oligoarthritis JIA subtypes.
- Most studies incorporated strengthening exercises alone or in combination with other forms of exercise.
- Studies noted improved physical function and mental health and programs were well tolerated with no adverse events.
- Adherence was generally better with lower intensity exercise compared to high intensity. Identifying strategies to motivate children to adhere is needed.
- Better reporting of PA interventions may inform clinical practice and research.
Introduction
Juvenile idiopathic arthritis (JIA), the most prevalent rheumatic disease in children, has many subtypes including: oligoarthritis, polyarthritis, systemic, psoriatic arthritis, enthesitis-related or spondyloarthritis, and undifferentiated.1 JIA-associated symptoms include joint pain, stiffness and movement restrictions, fatigue, fever and muscle weakness.1 These symptoms and some forms of medical therapy used to manage JIA, place children at increased risk of sub-optimal bone mineralization and osteoporosis, undernutrition, muscle weakness, mobility impairments, and limitations in activities of daily living such as play.1–5 JIA also leads to reduced quality of life and the potential for increased mortality in adulthood.1 Physical activity (PA) and exercise are important components of a healthy lifestyle for all children including children with JIA.6–10 Current PA recommendations for children include participation in 60 minutes of moderate to vigorous activity per day, with vigorous activity completed on at least 3 days per week.11–13
Studies of PA participation in children with JIA show these children are considerably less active than their peers.6,14 Bos et al found children with JIA spent substantial time in sedentary behaviors and less time in moderate to vigorous activity compared to health controls, adjusting for age, gender, body mass index and season.15 Children with JIA also demonstrate reduced aerobic and anaerobic exercise capacity.6 These factors lead to a higher rate of disability, especially among adolescent girls with polyarticular rheumatoid factor-positive subtype.16
Earlier investigative studies of children with JIA suggest weight-bearing PA and muscle strengthening are positively associated with a number of health outcomes.2,17 Farpour-Lambert et al reported weight-bearing and strengthening exercises can improve bone health.2 Sandstedt et al found a 12-week exercise program of weight-bearing exercise plus standardized muscle strengthening exercises for children with JIA led to significant improvements in bone mineral density, bringing measurements for children with JIA within the reference range of healthy children.3 Physical activity and exercise (both aerobic and low intensity resistance exercise) also increase exercise capacity, muscle strength and composition, enhance mood, and improve quality of life.18 Studies indicate these benefits lead to reduced disability in adulthood.19 Among children with JIA, the goal is to achieve recommended PA levels, accounting for baseline PA levels, disease status, and JIA-associated symptoms.20 Treatment guidelines indicate a comprehensive approach to JIA management includes a combination of pharmacologic interventions plus moderate, consistent exercise and/or a more active lifestyle.10
Despite the evidence suggesting the positive impact of many forms of PA participation on health outcomes in children with JIA, parents and their children still fear exercise will exacerbate symptoms. This fear coupled with the vagueness of exercise prescriptions provided in clinical encounters leads to hesitancy and uncertainty regarding the best exercise and PA recommendations for children with JIA. This systematic review evaluated randomized controlled trials (RCTs) of PA interventions, including exercise, for children with JIA in terms of the breadth and quality of studies and synthesized these data to provide more detailed PA recommendations for children with JIA and their families.
Materials and Methods
Data and Data Sources
The research team conducted a systematic review of RCTs of PA and exercise in children with Juvenile Arthritis (JA) including JIA, following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines21 and registered in the International Prospective Register of Systematic Reviews (PROSPERO)22 prior to beginning the search. The Ovid (Medline), Cochrane Library, EMBASE and CINAHL databases were searched for articles published in English between 1/1/1946 to 9/1/2021. Two reference librarians (JP and SG) conducted the literature search using our pre-specified criteria and search terms, see Supplementary Materials (Figure S1–4).
Eligibility Criteria: Studies were included if they: (1) evaluated exercise or PA interventions, or evaluated PA interventions which combined exercise with a modality (inferential current, hot packs) or (2) employed an interactive digital intervention (eg via computers, handheld devices, web-based programs, wearable technology or applications (apps)) which aimed to measure and promote PA, as long as a PA was incorporated into the intervention. The constructs exercise and physical activity are related but different. Exercise is defined as planned, structured behavior and is a subset of physical activity. Thus, to be comprehensive, this review included studies of PA including exercise interventions.23 This study includes only RCTs as non-randomized studies have an inherently greater risk of bias than RCTs and most observational cohorts studies use large databases which present data estimates than may appear to be more precise than they really are. Studies were excluded if they examined PA in adults with JA, were secondary analyses of a primary PA intervention in children with JA and were not published in English.
Study Selection: Two librarians (JP and SG) compiled all citations identified from the searches using Endnote bibliographic software (EndNote X9, Clarivate Analytics, Philadelphia, PA) and removed duplicate records. The team members (MDI and JvH) individually examined the title and abstract of each study applying a screening process used in prior publications24,25 and eliminated studies that did not meet the inclusion criteria. The team was not masked to the name(s) of the study author(s), institution(s) or publication source. If study eligibility was unclear, they deliberated whether or not the study met inclusion/exclusion criteria and came to a consensus regarding inclusion. Next, the team excluded conference abstracts and individually reviewed the full text articles to determine whether the study met the inclusion criteria. The search results and process of study elimination are summarized in the PRISMA flow diagram portrayed in Figure 1. For a list of excluded full text manuscripts and the reason for exclusions, please see Supplementary Materials (Table S1).
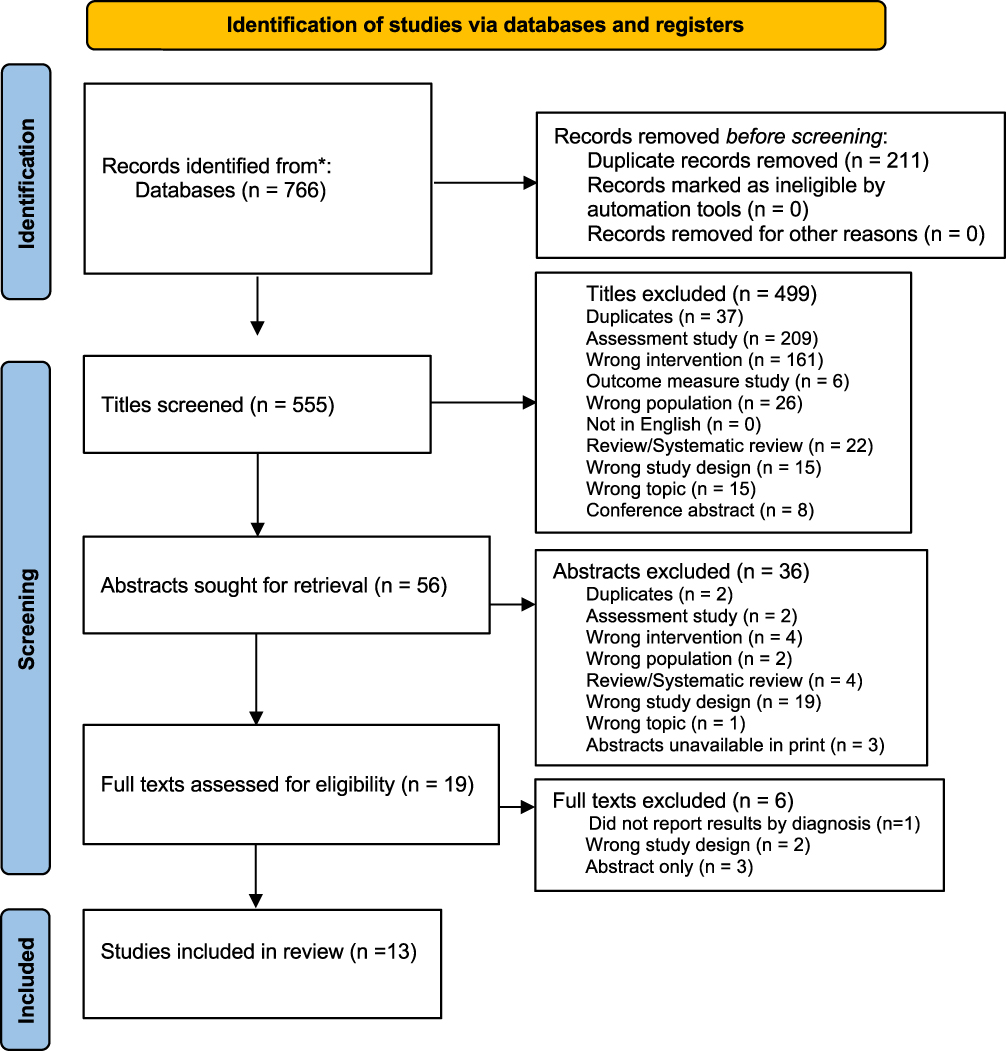 |
Figure 1 PRISMA flow diagram of randomized studies of PA and exercise in children with Juvenile Arthritis. Notes: Adapted From: Page MJ, McKenzie JE, Bossuyt PM et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. I. 2021;372:n71. doi: 10.1136/bmj.n71. This paper was published under Open Access, Creative Commons. For more information, visit: http://www.prisma-statement.org/. |
Data Extraction and Risk of Bias
After identifying all studies that met the inclusion criteria, data were extracted using a standardized form. Specific data elements included: author; year of publication; source of funding; country where study was conducted; total number of participants in PA arms and comparison/control arms; participant demographics and clinical characteristics (eg diagnosis, subtype, age, sex); program attributes such as setting, program length in weeks; type of intervention, frequency, duration, intensity, and the amount and type of supervision; whether there was a clear statement of adverse events (AEs) and drop outs (DOs) and the severity of AEs related to the intervention. The aim was to classify AEs as severe (fracture, permanent damage, disability, or death) or non-serious (muscle strain, soreness, or a fall not related to the exercise program).26
The team (JvH, MDI) used the Physiotherapy Evidence Database (PEDro) scoring method to independently assess the risk of bias in the included studies.27 The PEDro scale consists of 11 items to rate the internal validity and sufficiency of statistical information provided in the RCTs to inform clinical decisions. Allocation of points for each item are as follows: one or no points for the presence or absence of random allocation, concealed allocation, baseline comparability, participant blinded to allocation, therapist blinded to allocation, assessor blinded to allocation, measures of key outcomes, intention to treat analysis, comparison of study arm results, and reporting of point estimates of variability. Reporting subject eligibility criteria is acquired but not included in the total score. Points across the items are summarized to create a single score for each study ranging from 0 to 10. PEDro scores traditionally are reported as a range versus a mean or median. If the researchers disagreed on the PEDro score of a study, a normative group process was used to reach a consensus.
Sources of Funding for Included Studies
Following the recommendations of the critical appraisal tool “A MeaSurement Tool to Assess Systematic Reviews” (AMSTAR 2), the researchers examined all included studies to determine the source of funding for the project and recorded the source of funding. If no source of funding was mentioned, this fact was recorded as well.28 Recording of funding is recommended as bias may be present with commercial funding.
Quality of PA Intervention Reporting
The team used the Consensus for Exercise Reporting Template (CERT) checklist to assess the quality of the PA interventions. This checklist provides a best practice for reporting and replicating interventions in research to address deficiencies noted in PA studies. The checklist includes 16 items within seven domains such as: what (materials, exercises), who (provider), how (delivery including supervision), where (location), when, how much (dosage), tailoring of exercise (what, how), and how well the program was implemented (compliance/planned and actual), with a maximal attainable score of 19.29
Outcome Measures
The primary outcome measures typically used were PA level, physical function, or exercise capacity assessed from baseline to the end of the intervention. Assessment of PA level, physical function, or exercise capacity could be conducted using physical examination measures (such as Metabolic equivalent of task (METS), maximal aerobic capacity (VO2 Max), device-acquired data such as pedometer step counts, accelerometry measures of PA levels, time spent in various activities, level of achievement of PA guideline recommendations, and/or self-reported PA levels via a validated questionnaire or diary.30 Examples of secondary outcomes included health-related quality of life (HRQoL) pain, fatigue, joint stiffness, range-of-motion (ROM), muscle integrity (eg strength, mass etc), and mental health using validated generic or disease-specific outcome measures. Intervention timeframe was documented for each study.
Data Synthesis and Analysis
The team conducted a narrative synthesis of the included studies such as subject characteristics, the country where the study was conducted, PA or exercise intervention attributes (eg frequency of PA (days/week), program intensity, duration of individual sessions (minutes), total program duration (weeks), PA modes, and level of supervision (partial or complete). Modes of PA interventions were categorized as follows: strengthening alone; strengthening plus flexibility, a combination of strengthening, balance, flexibility and/or range of motion (ROM) or Pilates; aerobic exercise alone, conventional physical therapy alone or with an emphasis on a specific mode of PA, Qi Gong, or aquatic exercise. In cases where a range of time, frequency or intensity was reported for any PA intervention, the team calculated the average or rounded up the number to the next category. The team also identified whether the authors included a statement of AEs or DOs. The outcomes were then synthesized (eg function, pain, adherence etc), along with the number and type of AEs and DOs and reported across study arms. Data heterogeneity with respect to modes to intervention, duration and patient demographics and disease type, duration and activity level coupled with lack of information on intervention intensity, prohibited the use of meta-analysis. The results were presented in a descriptive analysis, and all data were analyzed using IBM SPSS Statistics version 26 (SPSS Inc., Chicago, USA).
Results
Study Characteristics
The initial literature search yielded 555 studies. Of these, 13 studies met the inclusion criteria (Figure 1).17,31–42 These studies were conducted in 10 countries, with 4 studies31–33,42 (31%) conducted in Turkey. All studies included children with JIA. There were 672 participants randomized. Of these, 579 were analyzed; 494 participants in the PA intervention arms and 85 in non-physical activity groups. The participant demographic and clinical characteristics are similar to a typical population of children with JIA. For example, the mean age across studies ranged from 8.7 to 16.1 years, with a higher prevalence of oligoarthritis and polyarticular arthritis diagnoses and a higher prevalence of female patients (Table 1).
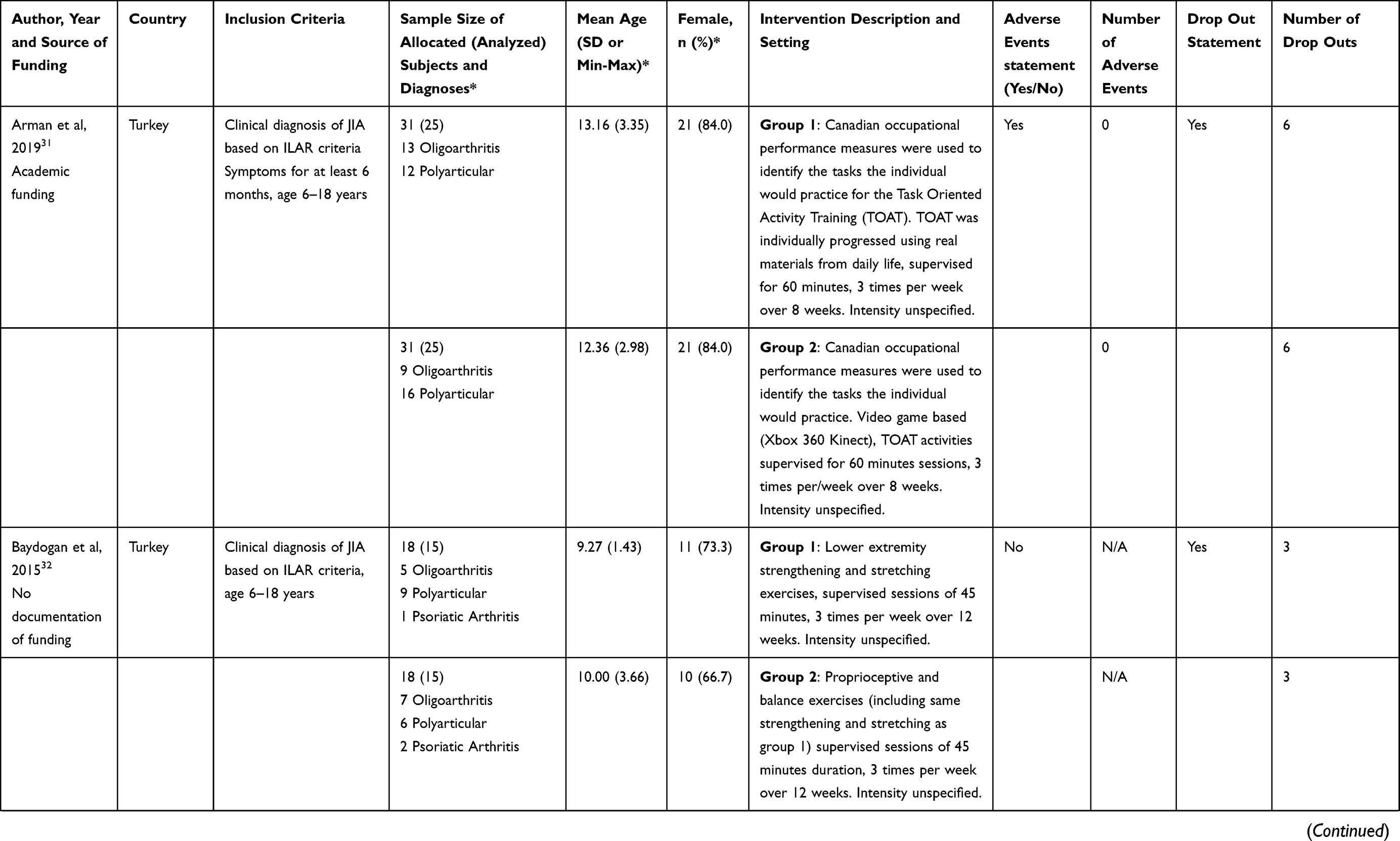 | 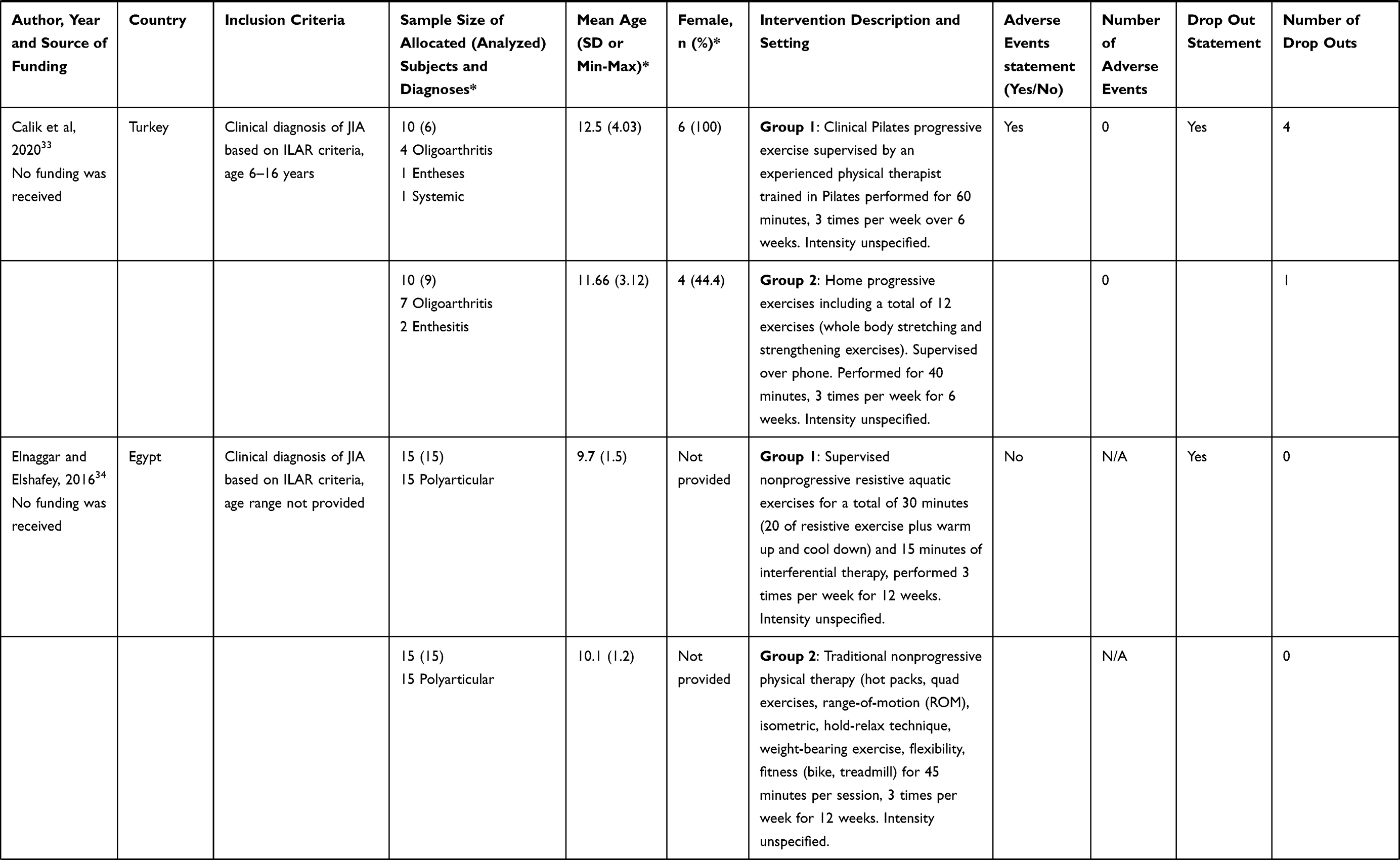 | 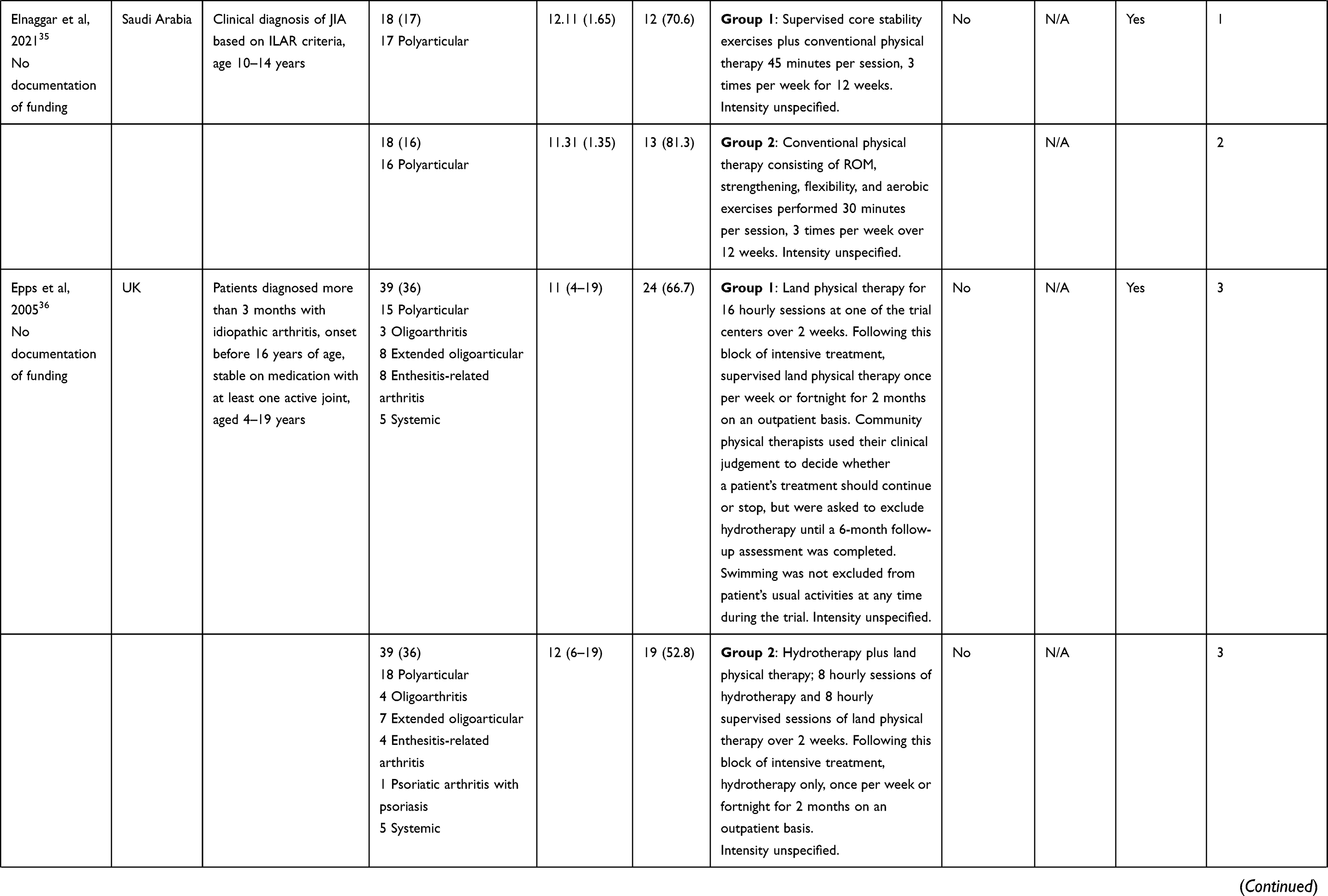 | 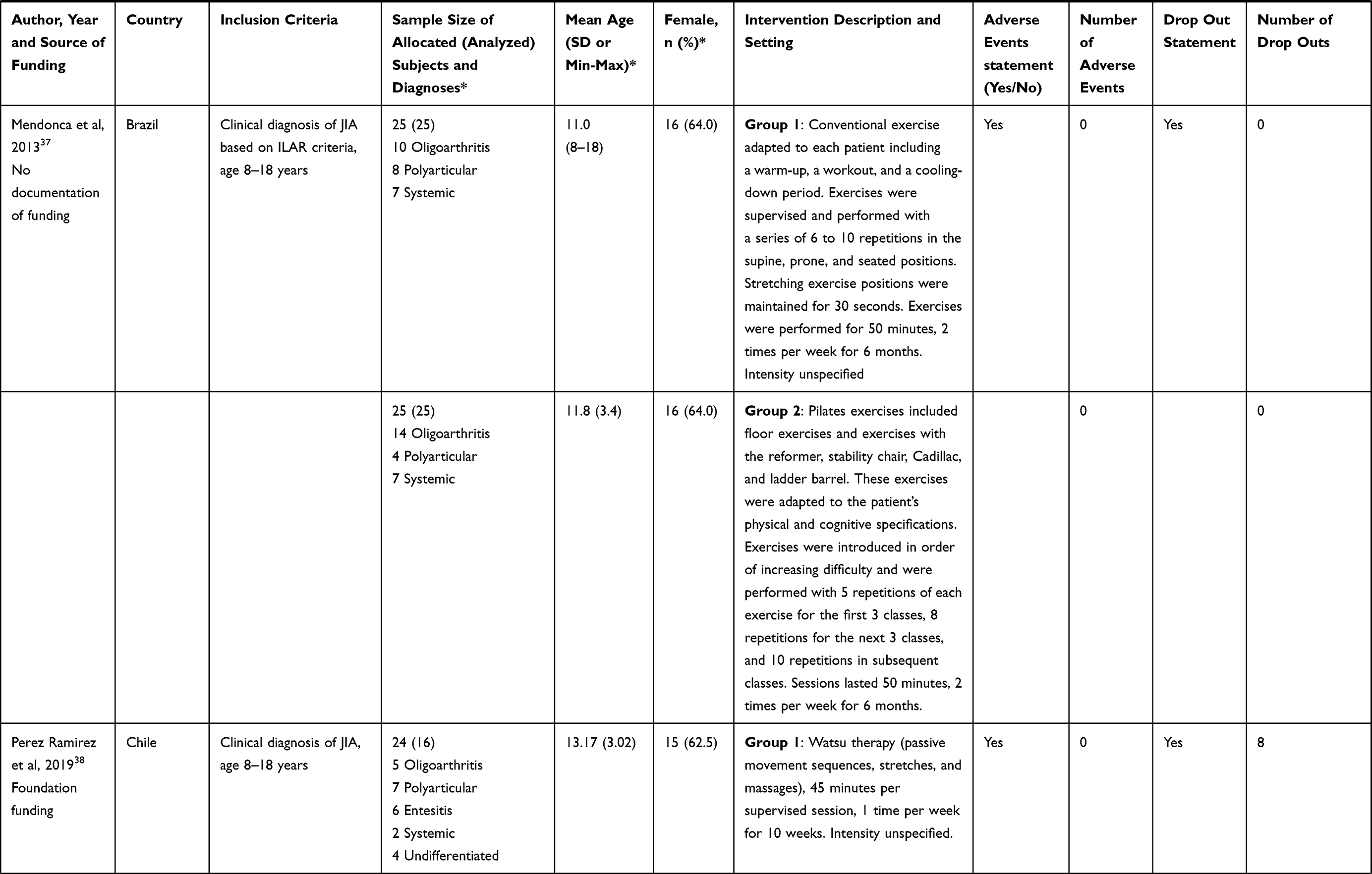 | 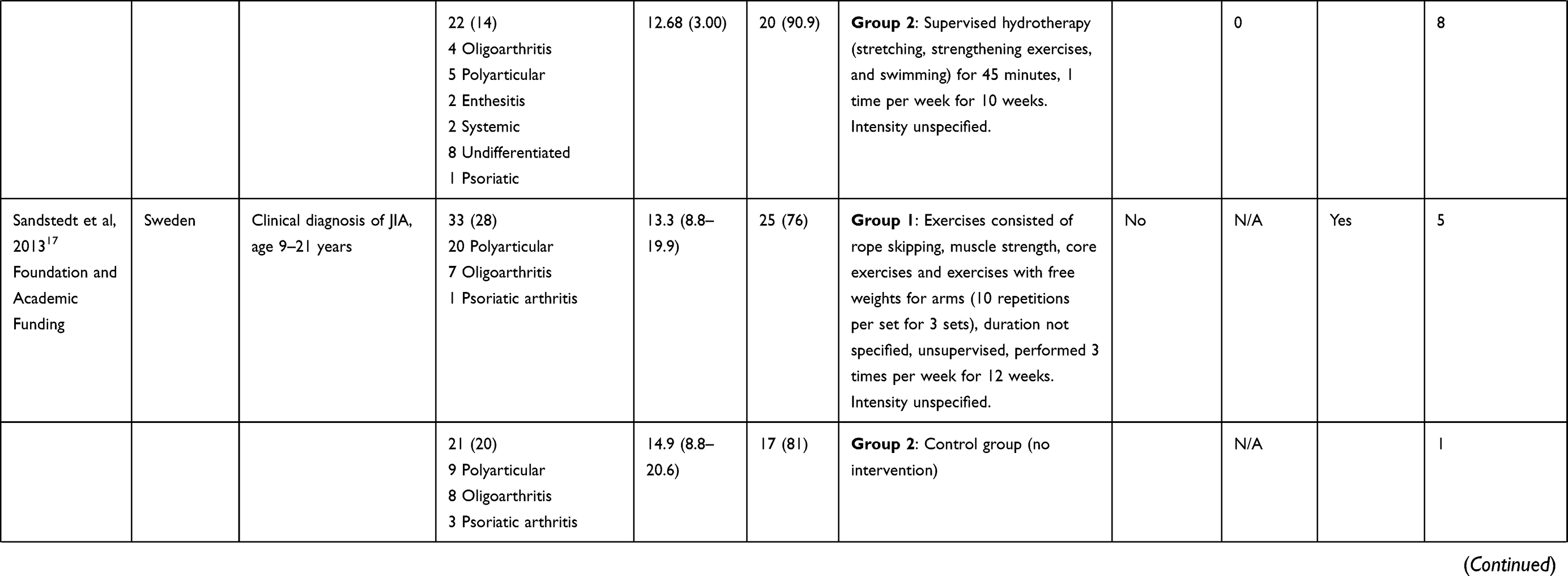 | 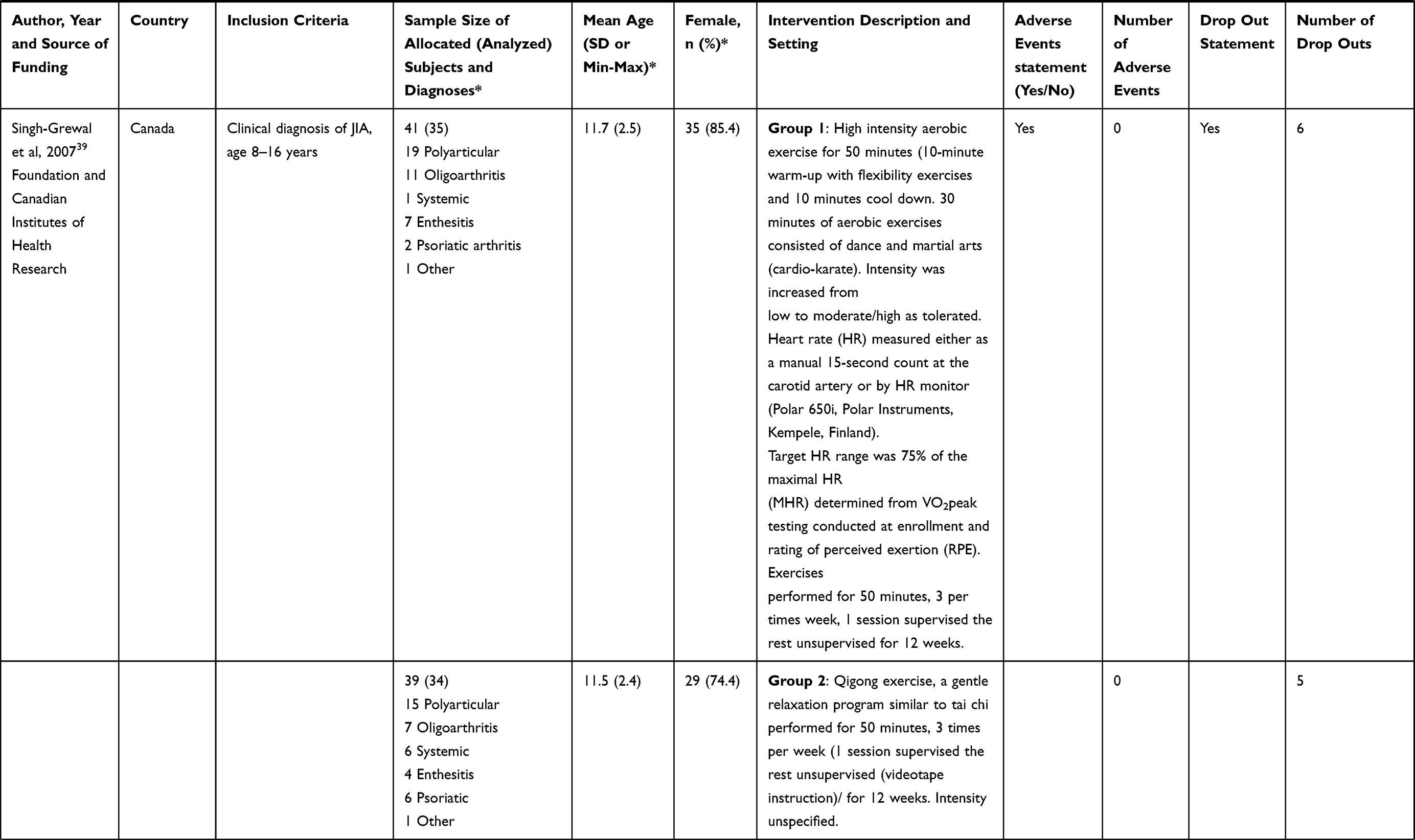 | 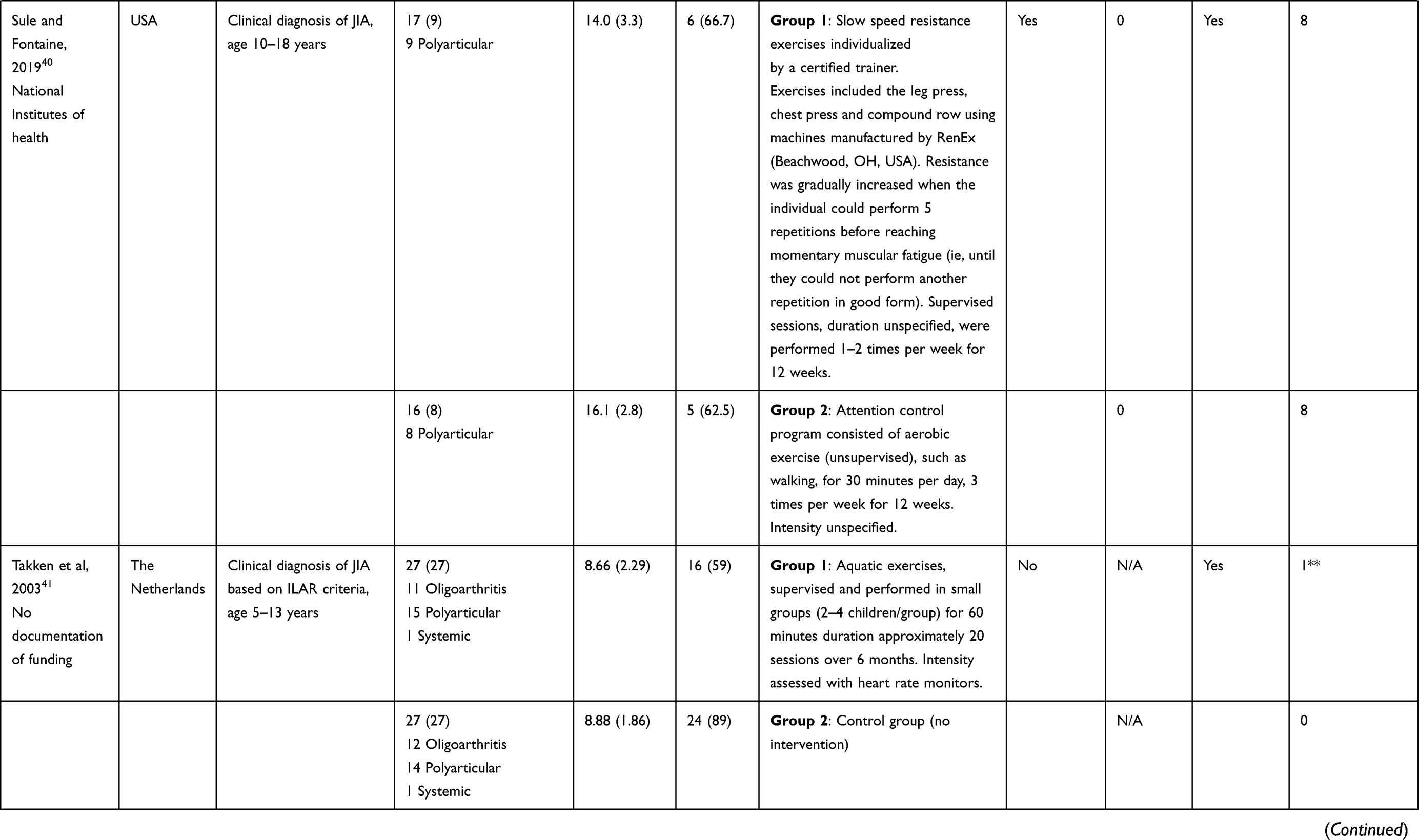 |
Table 1 Characteristics of Study Participants, Physical Activity Interventions, Adverse Events, and Dropouts in Randomized Controlled Trials of Physical Activity Interventions in Children with Juvenile Idiopathic Arthritis |
Risk of Bias
The PEDro scores of included studies ranged from 4 to 8, out of a possible 10 points. Only one study (7.7%) did not use concealed allocation.40 In most studies, subjects and interventionists were not blinded to the intervention due to the nature of the interventions provided. In two studies (15.3%), assessors were also not blinded (84.6%).34,40 Regarding measurement of key outcomes, five studies31–33,38,40 (38.4%) had less than the required 85% threshold for measurement of key outcomes and four studies (30.7%) used an intention-to-treat analysis36,38,39,41 (Table 2). No studies were funded by a commercial source (Table 1).
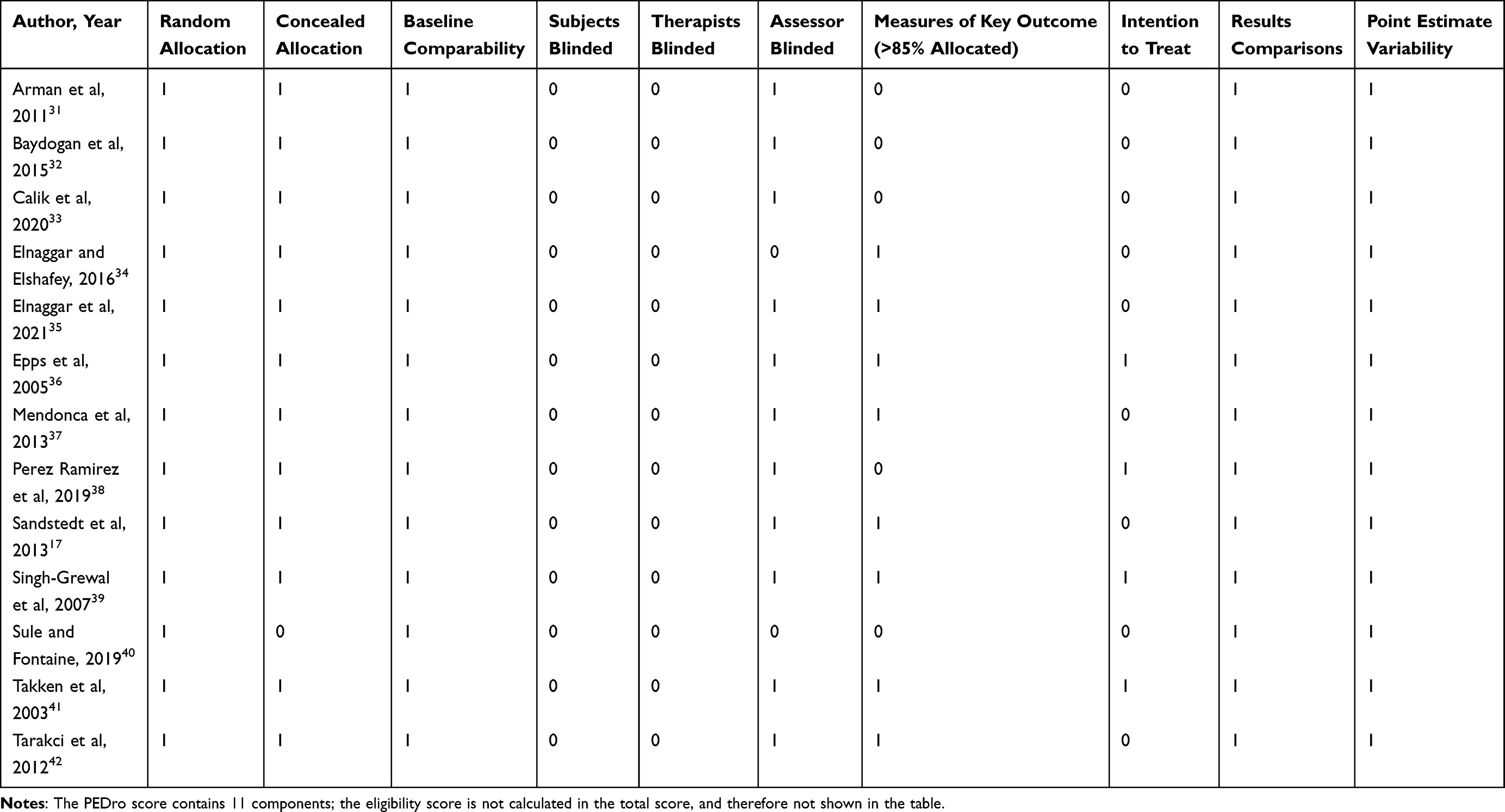 |
Table 2 Risk of Bias Assessment of Included Randomized Trials Using the PEDro Scoring Format; Measures of at Least One Key Outcome Were Obtained from More Than 85% of the Subjects Initially Allocated to Groups |
Attributes of Therapeutic Exercise and Physical Activity Interventions
Studies included a mix of PA interventions such as strengthening exercises, task-based activities, aquatic or hydrotherapy, Watsu, Pilates, Qigong or a combination of modes of exercise. The most common form of PA intervention was strengthening exercise plus some combination of other exercise modes. Among the 23 intervention arms, five arms (21.7%) included physical therapy.33–36 The mean number of participants per intervention arm and comparison arms was 21.5 (range 6 to 43) and 28.3 (range 20–38), respectively Three studies included a true control or wait list arm (Table 3).17,41,42
 |
Table 3 Summary of Physical Activity Intervention Durations, Frequencies, Intensities, Modes, and Levels of Supervision Among the Exercise Arms (n = 23) Included in the 13 Studies |
The duration of most interventions (65.2%) lasted more than 12 weeks and up to 28 weeks and interventions were often scheduled three times per week (60.9%). Intervention sessions typically lasted more than 45 minutes, up to and including 60 minutes (43.5%). Intervention arms typically incorporated in-person supervision (78.2%) or partial supervision (13.1%) to ensure proper performance of PA intervention. Program intensity was not specified in 15 intervention arms (65.2%). In six intervention arms,31,33,37,40,42 the authors stated a trained person was individualizing and progressing the PA, but details regarding how the intervention was tailored and progressed were not provided. In two intervention arms,39,41 heart rate monitors or heart rate monitors plus perceived exertion scales were used to assess PA intensity.
The CERT scoring method was used to evaluate the quality of the reporting of PA interventions.29 The CERT scores ranged from 5 to 17, out of a possible 19 points. Only one study31 used motivational strategies to promote intervention adherence. Other areas where studies lacked information and did not receive CERT points pertained to the threshold at which PA was initiated, details regarding PA progression, and the measurement and reporting of adherence. Table 4 shows CERT scores and details for all interventions.
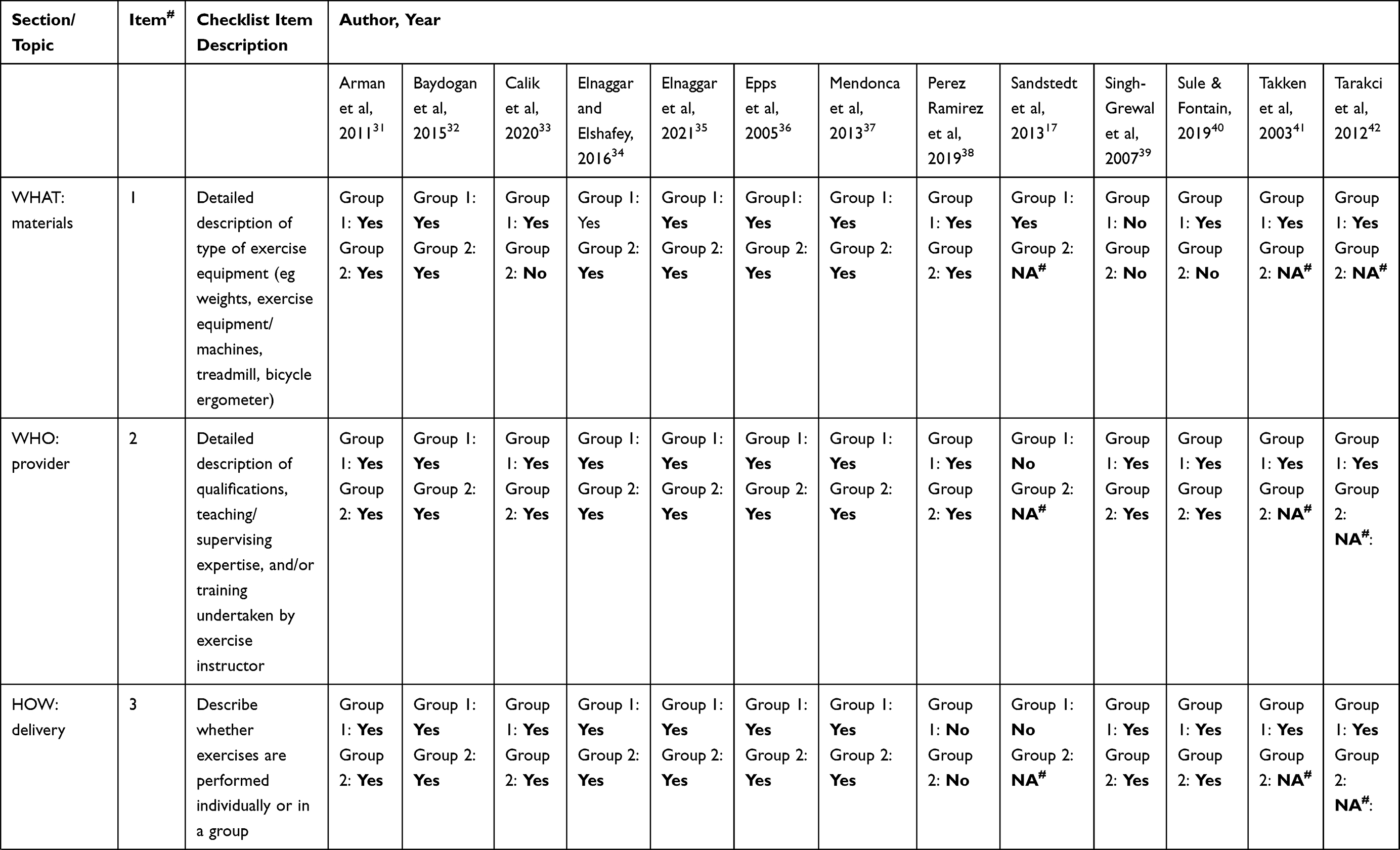 | 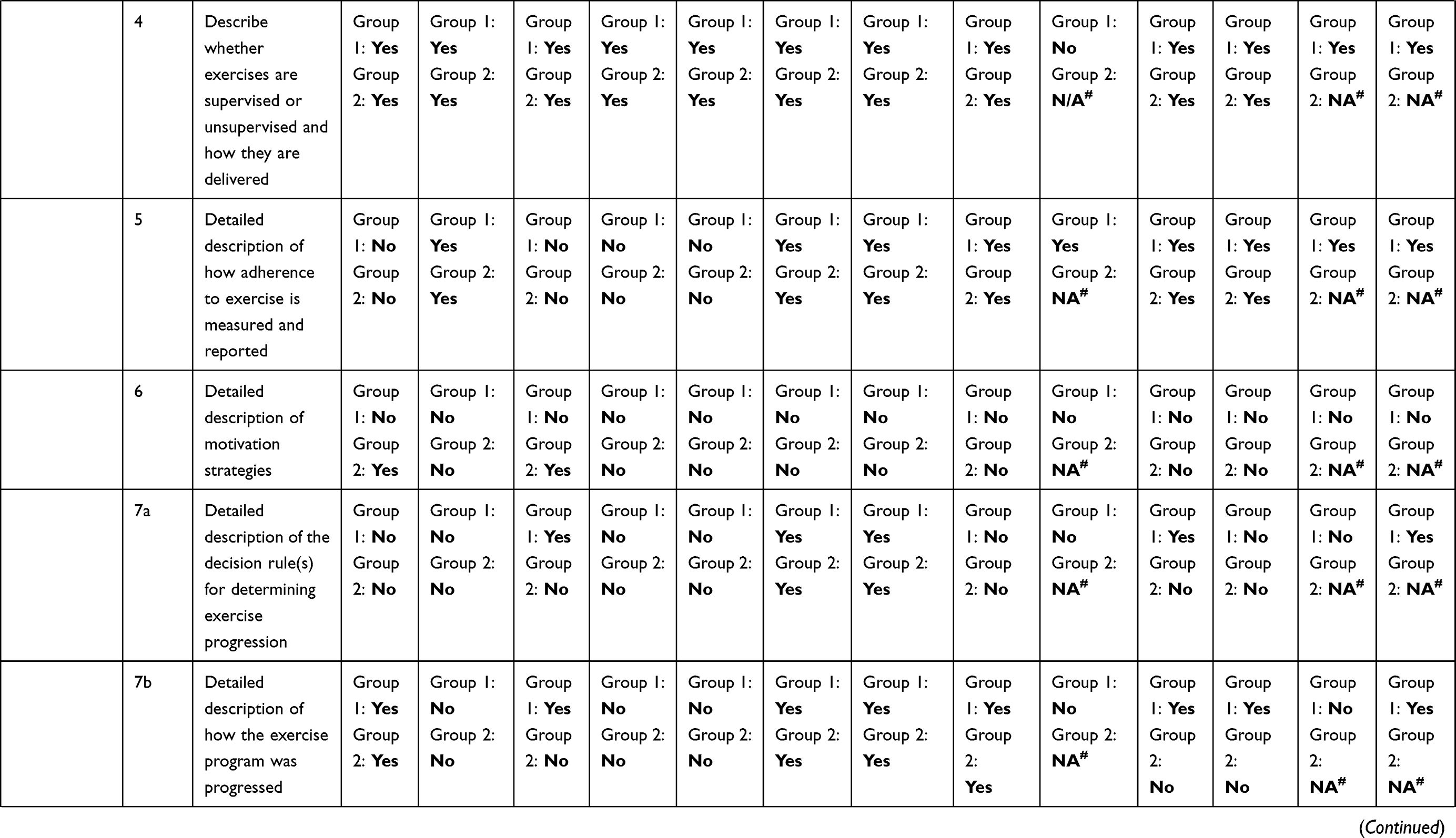 | 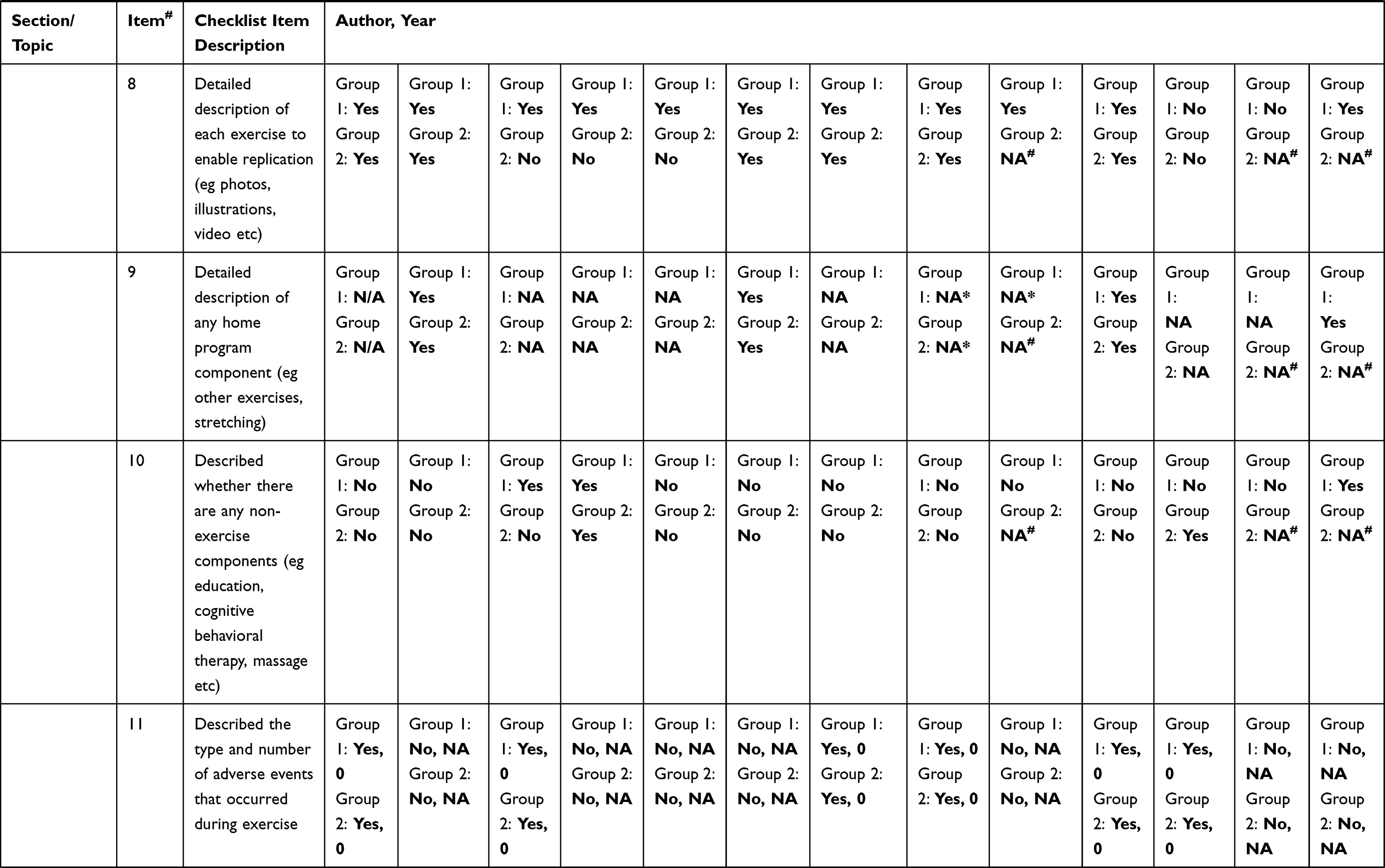 | 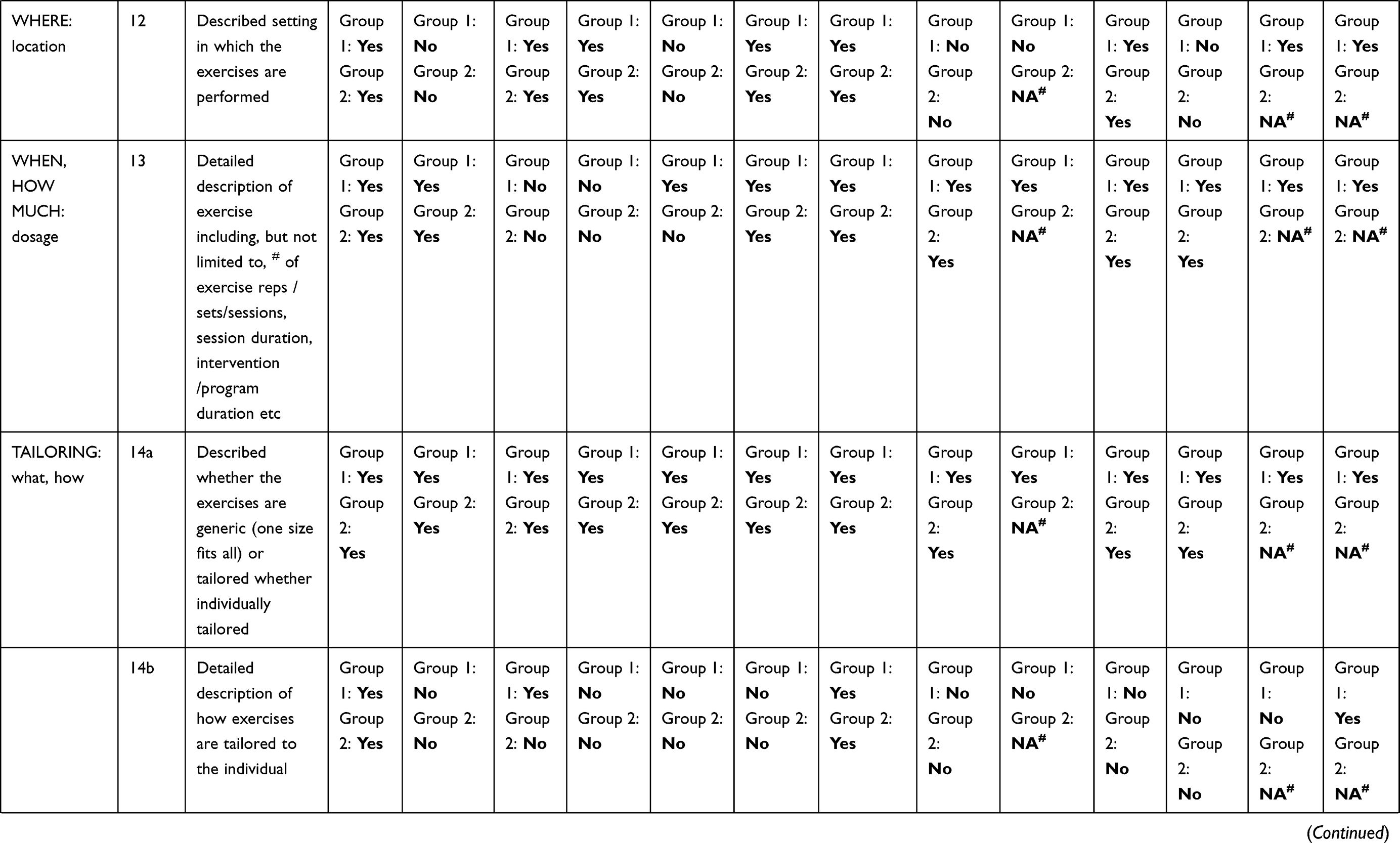 |
Table 4 Key Items of Exercise Interventions of Included Randomized Trials Using the Consensus on Exercise Reporting Template (CERT) Scoring Format |
Reporting of Adverse Events (AEs) and Dropouts (DOs)
Table 1 summarizes the information on the number of AEs and DOs reported. No studies included an a priori definition for AEs, nor information on the threshold for reporting AEs or methods for collecting AEs (ie patient-report log and online survey at the end of the intervention). Only six studies (46.1%) included a statement of AEs and no AEs were reported in any study.31,33,37–40
All 13 studies included a clear statement regarding DOs. Two studies34,37 reported no DOs during the study. One study41 reported a single DO but the researchers included the subject in the analysis, as the subject met their threshold for program adherence. In total, there were 94 (16.3%) DOs across the 23 intervention arms and 9 DOs (1.5%) across the 3 control arms.17,41,42 Fifty-eight DOs were non-exercise related, with 45 dropouts (77.6%) recorded as providing no reason for stopping the study, providing an unspecified personal reason or were lost to follow up. The remainder of the DOs were recorded as either ineligible or having family issues. Among the 36 exercise-related DOs, 34 (94.4%) dropped out due to lack of time or scheduling issues.
Outcomes of Study
Within the 13 RCTs of PA interventions, all studies used a generic or disease-specific functional outcome measure. Eleven studies17,31–35,37–40,42 (84.6%) included a measure of pain, seven studies17,32,34–36,39,41,42 (53.8%) incorporated measures of aerobic capacity, fitness or functional performance, 8 studies17,32,36–41 (61.5%) measured ROM and 7 studies17,33,36–38,40–42 (53.8%) assessed quality of life. Only one study assessed fatigue40 and one study measured balance32 (Table 5).
 | 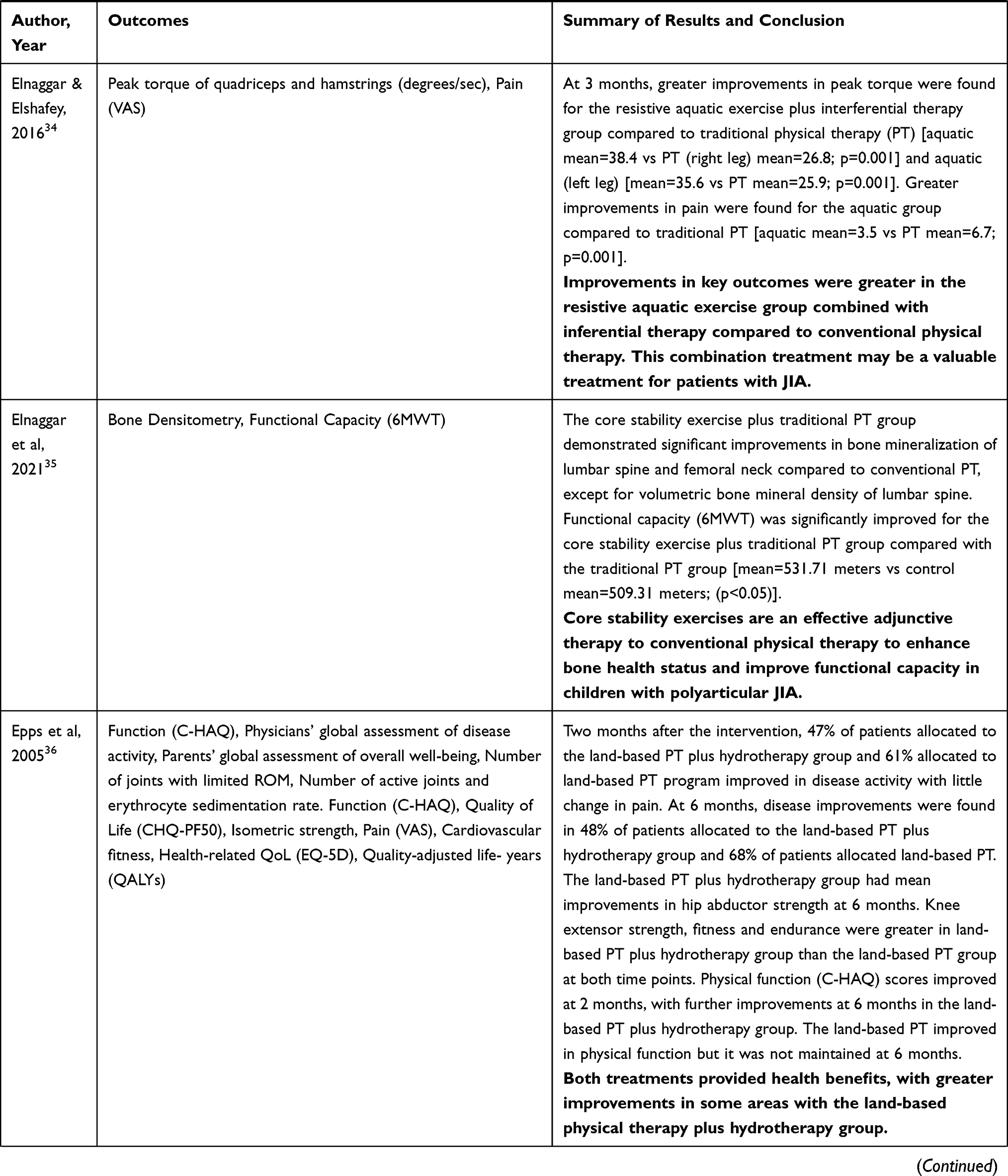 | 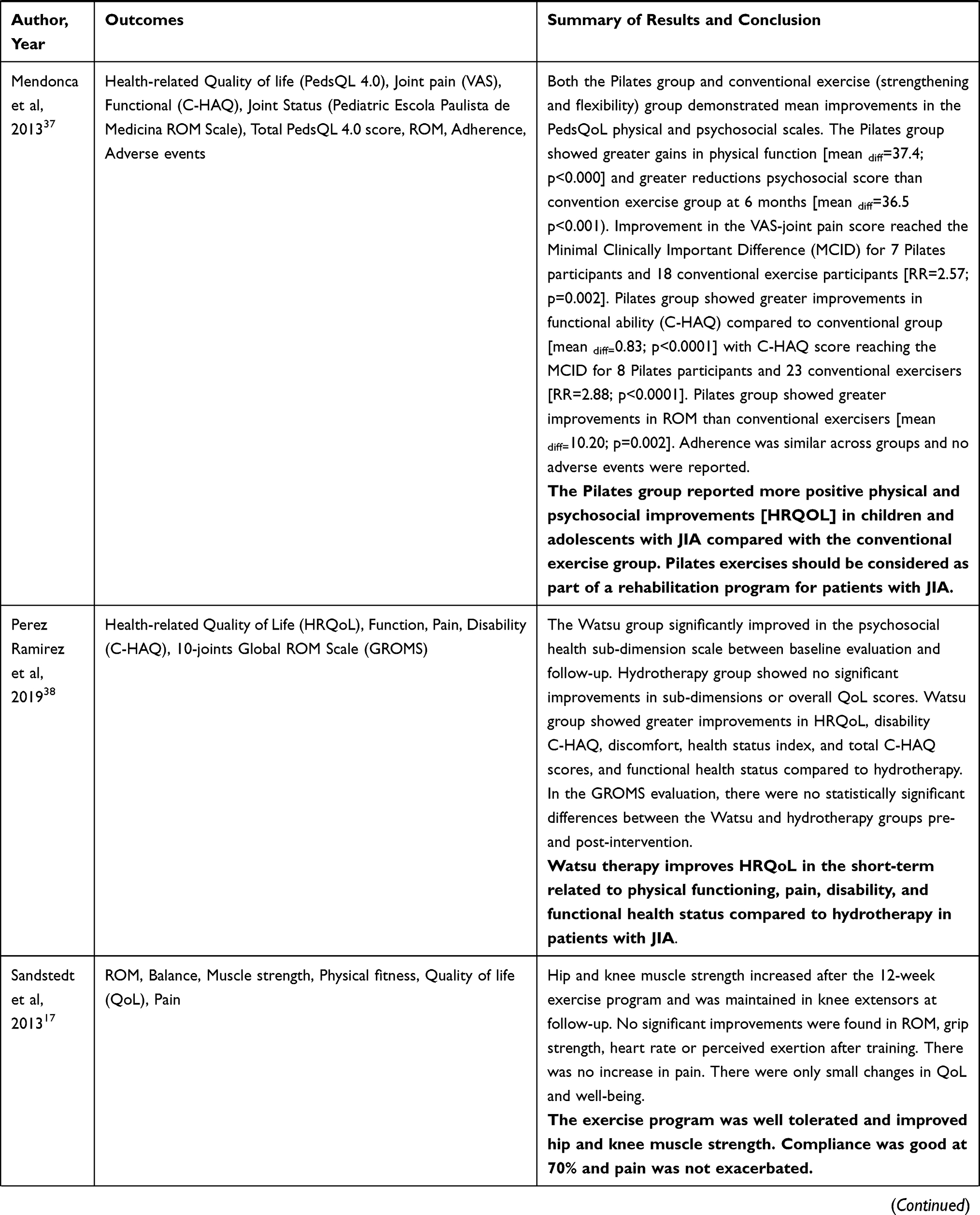 | 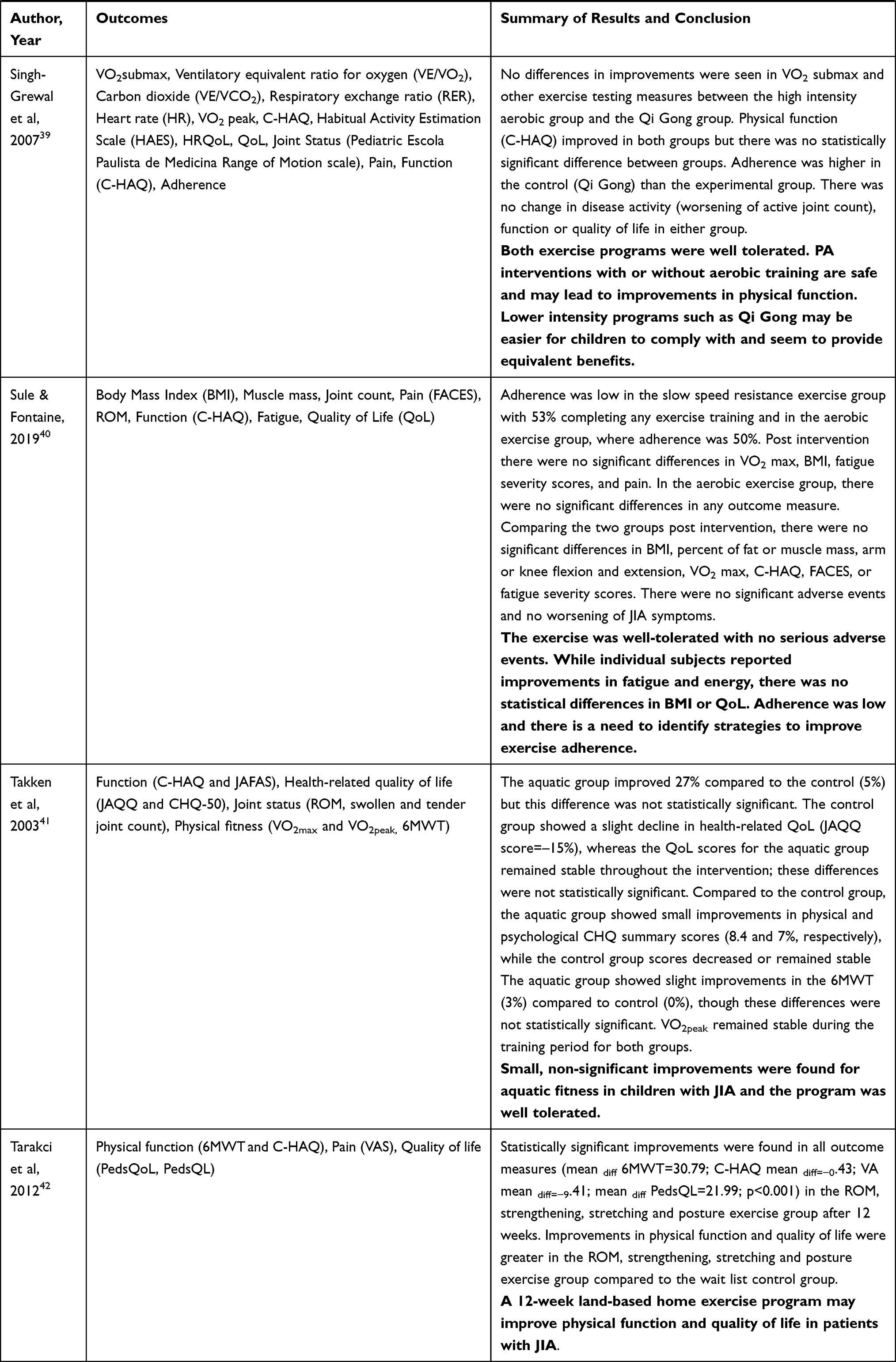 |
Table 5 Summary of Study Outcome Measures and Results Among Included Randomized Controlled Trials of Physical Activity in Children with Juvenile Idiopathic Arthritis |
In all studies, health outcomes improved across a variety of domains. In the study by Arman et al,31 data indicated that a video-based task-oriented training program resulted in similar health benefits to a traditional task-oriented training program, but the video games appeared to have a greater motivating effect on patient behavior. The use of Pilates33,37 and Watsu38 and Qigong39 exercises appeared to be effective, and in the case of Qigong,39 this PA format was better tolerated than high intensity PA. Additionally, the use of conventional physical therapy with focused attention on core stability exercises appeared to yield additional benefits than conventional physical therapy.35
Intervention Adherence: Four studies (30.7%) made no mention of assessing adherence.31,33–35 The remaining studies measured adherence as either a percent of sessions attended, via a questionnaire, or defined adherence as the number of completed repetitions of all exercises performed in the program. In five studies,17,39–42 an a priori threshold for adherence was defined (ranging from 70% to greater than 75% adherence) and two studies32,37 reported the mean number of sessions attended out of all possible sessions.
Discussion
This systematic review aimed to evaluate the literature regarding PA interventions for children with JIA. The review focused on the breadth of the studies (PA intervention attributes such as the mode(s), frequency, intensity, duration etc) and study quality, in order to ascertain detailed recommendations and perspectives on PA interventions for children with JIA and their families. This issue is important as PA guidelines are most often nonspecific. Current recommendations published by the US Centers for Disease Control recommend school-aged children should participate in ≥ 60 minutes of moderate to vigorous PA daily, noting that activities be enjoyable, variable (eg aerobic, muscle and bone strengthening exercises), and developmentally appropriate.12 Similar recommendations are published across other countries.11,13 Organizations that represent healthcare providers who work with children diagnosed with JIA suggest these recommendations be tailored to address health-specific changes associated with JIA disease.8–10
Our search found 555 published studies of PA interventions for children with JA. However, the number of RCTs of PA interventions was considerably low, at 13 studies. These studies included only children with JIA and then limited to certain subtypes of JIA. Included studies provided a mix of interventions (eg strengthening, aerobic) which is reflective of current recommendations and clinical practice.11,12 Using a mix of PA interventions helps to address the various manifestations of JIA-associated symptoms and has the added benefit providing a variety PA interventions which may be more appealing to children.
To provide the best interventions, clinicians and families need detailed information such as how, when, and why to engage in PA and what interventions are most effective. The CERT checklist provides a guideline to help researchers describe in detail the attributes of the interventions they have tested so that the results can be readily transferrable to clinical practice and to enable other researchers to replicate their findings.29 Using the CERT, we found a number of deficiencies in the reporting of the interventions employed in these studies. Most notable, was the lack of detail regarding the starting point for PA programs (eg amount of resistance within the activity, speed etc). Most studies did not indicate that the program was tailored to the patient’s health status and a number of studies did not provide specific details on how to the intervention was progressed. Whereas, Taracki et al, engaged physical therapists with expertise in JIA to design the PA program.42 These physical therapists established the baseline components of the PA program, progressed the repetitions of exercise per patient tolerance, and provided a detailed list of activities for patients and families. The study incorporated patient diaries and supervision help to patients understand the PA progression.
Since the ability to determine dose-response effects of PA interventions on health outcomes is contingent upon detailed reporting of interventions in PA studies, further attention to these factors and use of the CERT when reporting results of PA interventions is necessary. For children and parents of children with JIA who may be fearful of PA, it is difficult to initiate and maintain engagement in a PA program without the requisite information to properly perform the activities. Fear avoidance is a cognitive construct that can have lifelong implications and is important to address in young children. Children’s fear of movement coupled with parental protectiveness can lead to a sedentary lifestyle and disability in adulthood. Fear-avoidance beliefs mediate the association between parental protectiveness and PA limitations and are important to address when designing PA interventions for children with chronic pain.43
These 13 RCTs measured different aspects of JIA symptoms and outcomes of PA. For example, typical symptoms of JIA include joint pain, stiffness, loss of range-of-motion, muscle weakness, physical function, fatigue and reduced aerobic capacity. The most common outcomes assessed were pain, aerobic capacity, general function, and range-of-motion. However, fatigue was only measured in one study.40 There was substantial heterogeneity in the outcome measures used which suggests the need for a standardized core set of outcomes measures for studies of PA interventions in this population.
The interventions in this systematic review were generally of a low to moderate intensity. One program compared higher intensity aerobic PA to a lower intensity Qi Gong program, and found children were more adherent to the lower intensity program.39 This study included children with a mix of JIA subtypes ages 8 to 16 years. This sample reflects the heterogeneity of subtypes of JIA. It is important to note that these 13 studies did not measure or report the PA behaviors of children prior to their diagnosis of JIA or inclusion in the study. Thus, we do not know whether children who are very physically active prior to diagnosis may tolerate higher levels of PA.
None of the studies in the systematic review reported any AEs from the short-term PA interventions examined. This result is similar to the data from a 2008 Cochrane Review which included three RCTs.44 However, information on dropouts was lacking in the included studies, so it may be difficult to state that individuals who dropped out did not experience an intervention-related adverse event.
Program adherence was not formally addressed in all studies. Adherence to PA interventions is a complex and multifaceted behavior. Personal factors such as past experience with PA, physical factors such as pain and fatigue and psychosocial factors (eg isolation, motivation) influence PA behaviors and PA programs may be burdensome (eg too much time commitment) and can make increasing PA challenging. Identifying barriers and facilitators to PA adherence is essential for positive health outcomes.45 Favier et al identified barriers and facilitators to PA in children with JIA and reported that forgetting to attend therapy, pain, and the belief that therapy is not necessary were the main barriers to adherence.46 These authors recommended assessing barriers to adherence and actions that facilitate adherence as essential to helping children with JIA achieve a better quality of life. Similarly, Risum et al examined barriers and facilitators to PA in Norwegian children with JIA compared to healthy age and sex matched controls. They found children with JIA reported pain and disease activity as barriers to PA and that fun was the most important facilitator for PA engagement for all children, followed by being with friends.47 Sims-Gould et al in a study of parents and children with JIA reported potential health benefits, fun, and parental support as significant facilitators of PA engagement in these children. Whereas, time pressures and physical symptoms were barriers.48 These data combined with clinical experience indicate the importance of incorporating strategies to motivate children to engage in PA. Potential strategies include the use of fun and engaging smartphone apps, modifying activities at school to enable these children to participate in activities with peers, and strategies to support parents to promote PA with their children. Select smartphone apps and interactive digital interventions combine health education and gaming can be used to promote behavior change. In certain apps, these data can be shared with health care providers.49,50 For example, Wokamon © a commercial application, gamifies walking; the more you walk, the more food the creature eats and the more it grows.51 Such interventions may provide a fun and efficient means of supporting PA behavior in children.
Study quality is an important aspect of research, as lower quality studies are at greater risk of bias. In studies of PA interventions, some mechanisms to reduce bias (blinding the interventionist or subject bias) cannot be addressed in the study design due to the inherent active engagement required of the subject and interventionist. Whereas, other design elements (eg using intention-to-treat analysis, imputing values for missing data, or blinding of the assessor) can be incorporated, regardless of the intervention, to control bias. We found two studies in which the assessor was not blinded,34,40 five studies31–33,38,40 that had less than the required 85% threshold for measurement of key outcomes and only four studies36,38,39,41 that used an intention-to-treat analysis. These data suggest more attention to design elements and reporting of study quality may be warranted in RCTs examining PA interventions for children with JIA.
Limitations and Strengths
There are some limitations to this study. First, there are few published RCTs of PA interventions in children with JIA, this is an area that needs further investigation. This review was restricted to studies published in English, so studies published in other languages are not included. Finally, data heterogeneity prohibited the conduct of a meta-analysis. This study also has a number of strengths. Two research librarians conducted the literature search and the project was submitted to PROSPERO22 for review prior to initiating the search. The team who reviewed the titles, abstracts and full text articles are experienced in systematic reviews and followed the PRIMSA21 guidelines for the conduct of systematic reviews. The study includes both PA and exercise interventions to allow for a greater depth of information. Two validated and accepted measures of study quality were used, the CERT to assess the quality of the PA intervention reporting and PEDro to assess the quality of the study design.27,29
Conclusions
There is a lack of RCTs of PA in children with JA other than in children with JIA. Even among studies of PA in JIA the number of RCTs is relatively small. Additionally, among the studies included in this review, most children with JIA were diagnosed with polyarthritis and oligoarthritis, so there is little data on PA interventions for children with other subtypes of JIA. These studies of PA interventions lacked sufficient details regarding the starting threshold for PA, the tailoring of PA to child-specific needs and PA progression. Several studies examined PA interventions in the short-term and did not evaluate the long-term impact of PA. Thus, there is little evidence for long-term benefits of PA among these children. There was insufficient attention to reporting of adverse events and dropouts, which limits the ability to determine the safety and efficacy of PA interventions in children with JIA. Additionally, the value of individualized PA training, nuanced and dosed by a physical therapist with expertise in the field in JIA cannot be overlooked. Including detailed description of PA evaluated in studies is warranted to determine the best design of PA interventions.
Most programs did not incorporate strategies to address motivation and adherence and relied on family support to ensure the program was followed. There needs to be greater attention to the resources and supports for families to facilitate PA adherence in children with JIA. Developing healthy behaviors early in a child’s life and addressing fear-avoidance behaviors in children with JIA can improve musculoskeletal and cardiovascular health. Given advances in treatments for children with JIA, disease activity can be better controlled with less symptoms and affecting the ability to engage in PA. Children with JIA should be encouraged to participate in habitual PA and age appropriate play and sports to promote overall health.
Future RCTs of PA in children with JIA should: include children with various subtypes of JIA to provide evidence of best practices and benefits and potential harms, if any of PA for these children. We recommend future studies examine the impact of high and low intensity PA programs and include a core set of outcomes measures, along with detailed descriptions of dropouts and adverse events from PA. We also recommend study interventions vary the elements of the PA intervention to target different outcomes (strength, bone health etc) and incorporate strategies to address fear avoidance behaviors and motivate children to encourage active engagement in PA. Finally, more studies which evaluate the benefits of long-term PA engagement are needed.
Abbreviations
JIA, Juvenile idiopathic arthritis; PA, physical activity; RCT, randomized controlled trials; JA, juvenile arthritis; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; PROSPERO, International prospective register for systematic reviews; AEs, adverse events; DOs, drop outs; PEDro, Physiotherapy Evidence Database; AMSTRAM 2, A MeaSurement Tool to Assess systematic Reviews; CERT, Consensus on Exercise Reporting Template; METs, metabolic equivalent of task; VO2 Max, maximal aerobic capacity; HRQoL, health-related quality of life; ROM, range-of-motion.
Data Sharing Statement
The data extracted from these 13 studies are available from the corresponding author on reasonable request.
Acknowledgments
Karolinska Institutet librarians, Jonas Pettersson and Sabina Gillsund assisted with the literature search following the criteria outlined in our PROSPERO application.
Author Contributions
M.D. Iversen and J. von Heideken contributed to the conception of the study, study design, study execution, data collection and synthesis, data interpretation, and all drafts and revisions of the manuscript. M. Andre contributed to data synthesis, clinical relevance of the data and its interpretation, the analysis of results, and writing of the manuscript. All authors reviewed the final draft of the manuscript, agreed on the version to submit to this journal and agreed to take responsibility and be accountable for the contents of the article.
Funding
There was no specific funding for this project.
Disclosure
The authors report no competing interests that could have influenced the conduct of this study.
References
1. Petty RE, Southwood TR, Manners P, et al. International league of associations for rheumatology classification of juvenile idiopathic arthritis: second revision, Edmonton, 2001. J Rheumatol. 2004;31(2):390–392.
2. Farpour-Lambert NJ, Keller-Marchand L, Rizzoli R, et al. [Physical exercise and bone development in chronically ill children]. Exercice physique et developpement osseux de l’enfant malade chronique. Rev Méd Suisse. 2004;124(2):73–75.
3. Sandstedt E, Fasth A, Fors H, Beckung E. Bone health in children and adolescents with juvenile idiopathic arthritis and the influence of short-term physical exercise. Pediatr Phys Ther. 2012;24(2):155–162. doi:10.1097/PEP.0b013e31824cce6e
4. Knops N, Wulffraat N, Lodder S, Houwen R, de Meer K. Resting energy expenditure and nutritional status in children with juvenile rheumatoid arthritis. J Rheumatol. 1999;26(9):2039–2043.
5. Gutierrez-Suarez R, Pistorio A, Cespedes Cruz A, et al. Health-related quality of life of patients with juvenile idiopathic arthritis coming from 3 different geographic areas. The PRINTO multinational quality of life cohort study. Rheumatology. 2007;46(2):314–320. doi:10.1093/rheumatology/kel218
6. Long AR, Rouster-Stevens KA. The role of exercise therapy in the management of juvenile idiopathic arthritis. Curr Opin Rheumatol. 2010;22(2):213–217. doi:10.1097/BOR.0b013e328335d1a2
7. Klepper SE. Exercise in pediatric rheumatic diseases. Curr Opin Rheumatol. 2008;20(5):619–624. doi:10.1097/BOR.0b013e32830634ee
8. Cellucci T, Guzman J, Petty RE, et al. Management of juvenile idiopathic arthritis 2015: a position statement from the pediatric committee of the Canadian rheumatology association. J Rheumatol. 2016;43(10):1773–1776. doi:10.3899/jrheum.160074
9. Davies K, Cleary G, Foster H, et al. BSPAR standards of care for children and young people with juvenile idiopathic arthritis. Rheumatology. 2010;49(7):1406–1408. doi:10.1093/rheumatology/kep460
10. Ringold S, Angeles-Han ST, Beukelman T, et al. 2019 American college of rheumatology/Arthritis foundation guideline for the treatment of juvenile idiopathic arthritis: therapeutic approaches for non-systemic polyarthritis, sacroiliitis, and enthesitis. Arthritis Care Res. 2019;71(6):717–734. doi:10.1002/acr.23870
11. National Health Service (NHS). Physical activity guidelines for children and young people. Available from: https://www.nhs.uk/live-well/exercise/physical-activity-guidelines-children-and-young-people/.
12. US Department of Health and Human Services. Physical Activity Guidelines for School-Aged Children and Adolescents.
13. Bull FC, Al-Ansari SS, Biddle S, et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br J Sports Med. 2020;54(24):1451–1462. doi:10.1136/bjsports-2020-102955
14. Lelieveld OTHM, Armbrust W, Van Leeuwen MA, et al. Physical activity in adolescents with juvenile idiopathic arthritis. Arthritis Care Res. 2008;59(10):1379–1384. doi:10.1002/art.24102
15. Bos J, Armbrust W, Geertzen J, et al. PReS-FINAL-2148: rheumates@work a cognitive behavioural internet based intervention promoting physical activity in children with juvenile idiopathic arthritis: preliminary results of a randomized clinical trail. Pediatric Rheumatology. 2013;11, 160.
16. Bos GJ, Lelieveld OT, Armbrust W, Sauer PJ, Geertzen JH, Dijkstra PU. Physical activity in children with Juvenile Idiopathic Arthritis compared to controls. Pediatr Rheumatol Online J. 2016;14(1):42. doi:10.1186/s12969-016-0102-8
17. Sandstedt E, Fasth A, Eek MN, Beckung E. Muscle strength, physical fitness and well-being in children and adolescents with juvenile idiopathic arthritis and the effect of an exercise programme: a randomized controlled trial. Pediatr Rheumatol Online J. 2013;11(1):7. doi:10.1186/1546-0096-11-7
18. Legerlotz K. The effects of resistance training on health of children and adolescents with disabilities. Am J Lifestyle Med. 2020;14(4):382–396. doi:10.1177/1559827618759640
19. Minden K, Niewerth M, Zink AE, et al. Long-term outcome of patients with juvenile idiopathic arthritis treated with Etanercept results of the biologic register JuMBO. Arthritis Rheum. 2010;62:227.
20. Pedersen BK, Saltin B. Exercise as medicine - evidence for prescribing exercise as therapy in 26 different chronic diseases. Scand J Med Sci Sports. 2015;25(Suppl 3):1–72. doi:10.1111/sms.12581
21. Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ. 2009;339:b2700. doi:10.1136/bmj.b2700
22. Iversen MD, von Heideken J, Andre M Physical activity in children with rheumatic diseases: a systematic review. PROSPERO 2021 CRD42021274634. Available from: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42021274634.
23. Caspersen CJ, Powell KE, Christenson GM. Physical activity, exercise, and physical fitness: definitions and distinctions for health-related research. Public Health Rep. 1985;100(2):126–131.
24. von Heideken J, Chowdhry S, Borg J, James K, Iversen MD. Reporting of harm in randomized controlled trials of therapeutic exercise for knee osteoarthritis: a systematic review. Phys Ther. 2021;101(10). doi:10.1093/ptj/pzab161
25. James KA, von Heideken J, Iversen MD. Reporting of adverse events in randomized controlled trials of therapeutic exercise for hip osteoarthritis: a systematic review. Phys Ther. 2021;101(11). doi:10.1093/ptj/pzab195
26. Vincent KR, Vasilopoulos T, Montero C, Vincent HK. Eccentric and concentric resistance exercise comparison for knee osteoarthritis. Med Sci Sports Exerc. 2019;51(10):1977–1986. doi:10.1249/MSS.0000000000002010
27. Maher CG, Sherrington C, Herbert RD, Moseley AM, Elkins M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys Ther. 2003;83(8):713–721. doi:10.1093/ptj/83.8.713
28. Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. doi:10.1136/bmj.j4008
29. Slade SC, Dionne CE, Underwood M, Buchbinder R. Consensus on Exercise Reporting Template (CERT): explanation and elaboration statement. Br J Sports Med. 2016;50(23):1428–1437. doi:10.1136/bjsports-2016-096651
30. Sylvia LG, Bernstein EE, Hubbard JL, Keating L, Anderson EJ. Practical guide to measuring physical activity. J Acad Nutr Diet. 2014;114(2):199–208. doi:10.1016/j.jand.2013.09.018
31. Arman N, Tarakci E, Tarakci D, Kasapcopur O. Effects of video games-based task-oriented activity training (Xbox 360 Kinect) on activity performance and participation in patients with juvenile idiopathic arthritis: a randomized clinical trial. Am J Phys Med Rehabil. 2019;98(3):174–181. doi:10.1097/PHM.0000000000001001
32. Baydogan SN, Tarakci E, Kasapcopur O. Effect of strengthening versus balance-proprioceptive exercises on lower extremity function in patients with juvenile idiopathic arthritis: a randomized, single-blind clinical trial. Am J Phys Med Rehabil. 2015;94(6):417–418. doi:10.1097/PHM.0000000000000279
33. Calık BB, Gur Kabul E, Korkmaz C, Tekin ZE, Yener GO, Yuksel S. The efficacy of clinical Pilates exercises in children and adolescents with juvenile idiopathic arthritis: a pilot study. Rev Colomb Reumatol. 2020;27(4):269–277. doi:10.1016/j.rcreu.2020.06.015
34. Elnaggar RK, Elshafey MA. Effects of combined resistive underwater exercises and interferential current therapy in patients with juvenile idiopathic arthritis: a randomized controlled trial. Am J Phys Med Rehabil. 2016;95(2):96–102. doi:10.1097/PHM.0000000000000347
35. Elnaggar RK, Mahmoud WS, Moawd SA, Azab AR. Impact of core stability exercises on bone mineralization and functional capacity in children with polyarticular juvenile idiopathic arthritis: a randomized clinical trial. Clin Rheumatol. 2021;40(1):245–253. doi:10.1007/s10067-020-05219-9
36. Epps H, Ginnelly L, Utley M, et al. Is hydrotherapy cost-effective? A randomised controlled trial of combined hydrotherapy programmes compared with physiotherapy land techniques in children with juvenile idiopathic arthritis. Health Technol Assess. 2005;9(39):iii–59. doi:10.3310/hta9390
37. Mendonca TM, Terreri MT, Silva CH, et al. Effects of pilates exercises on health-related quality of life in individuals with juvenile idiopathic arthritis. Arch Phys Med Rehabil. 2013;94(11):2093–2102. doi:10.1016/j.apmr.2013.05.026
38. Perez Ramirez N, Nahuelhual Cares P. San Martin Penailillo P. [Effectiveness of Watsu therapy in patients with juvenile idiopathic arthritis. A parallel, randomized, controlled and single-blind clinical trial]. Efectividad de la terapia Watsu en pacientes con artritis idiopatica juvenil Un ensayo clinico controlado paralelo, aleatorio y simple ciego. Rev Chil Pediatr. 2019;90(3):283–292.
39. Singh-Grewal D, Schneiderman-Walker J, Wright V, et al. The effects of vigorous exercise training on physical function in children with arthritis: a randomized, controlled, single-blinded trial. Arthritis Rheum. 2007;57(7):1202–1210. doi:10.1002/art.23008
40. Sule SD, Fontaine KR. Slow speed resistance exercise training in children with polyarticular juvenile idiopathic arthritis. Open Access Rheumatol. 2019;11:121–126. doi:10.2147/OARRR.S199855
41. Takken T, Van Der Net J, Kuis W, Helders PJM. Aquatic fitness training for children with juvenile idiopathic arthritis. Rheumatology. 2003;42(11):1408–1414. doi:10.1093/rheumatology/keg386
42. Tarakci E, Yeldan I, Baydogan SN, Olgar S, Kasapcopur O. Efficacy of a land-based home exercise programme for patients with juvenile idiopathic arthritis: a randomized, controlled, single-blind study. J Rehabil Med. 2012;44(11):962–967. doi:10.2340/16501977-1051
43. Wilson AC, Lewandowski AS, Palermo TM. Fear-avoidance beliefs and parental responses to pain in adolescents with chronic pain. Pain Res Manag. 2011;16(3):178–182. doi:10.1155/2011/296298
44. Takken T, Van Brussel M, Engelbert RH, Van Der Net J, Kuis W, Helders PJ. Exercise therapy in juvenile idiopathic arthritis: a Cochrane review. Eur J Phys Rehabil Med. 2008;44(3):287–297.
45. Demmelmaier I, Iversen MD. How are behavioral theories used in interventions to promote physical activity in rheumatoid arthritis? A systematic review. Arthritis Care Res. 2018;70(2):185–196. doi:10.1002/acr.23265
46. Favier LA, Taylor J, Loiselle Rich K, et al. Barriers to adherence in juvenile idiopathic arthritis: a multicenter collaborative experience and preliminary results. J Rheumatol. 2018;45(5):690–696. doi:10.3899/jrheum.171087
47. Risum K, Selvaag AM, Molberg Ø, Dagfinrud H, Sanner H. HPR facilitators and barriers for participation in physical activities in juvenile idiopathic arthritis patients and healthy controls. Ann Rheum Dis. 2017;76:1517.
48. Sims-Gould J, Race DL, Macdonald H, et al. “I just want to get better”: experiences of children and youth with juvenile idiopathic arthritis in a home-based exercise intervention. Pediatr Rheumatol Online J. 2018;16(1):59. doi:10.1186/s12969-018-0273-6
49. Iversen MD, Connors ME, Menapace MR, Samson AJ, Tessitore E. Technology applications to improve health outcomes and self-management in patients with arthritis. Int J Clin Rheumtol. 2014;9(5):487. doi:10.2217/ijr.14.35
50. Heale LD, Dover S, Goh YI, Maksymiuk VA, Wells GD, Feldman BM. A wearable activity tracker intervention for promoting physical activity in adolescents with juvenile idiopathic arthritis: a pilot study. Pediatr Rheumatol Online J. 2018;16(1):66. doi:10.1186/s12969-018-0282-5
51. Shikudo. Wokamon. Available from: https://play.google.com/store/apps/details?id=com.wokamon.android&hl=en_US&gl=US.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.