Back to Journals » International Journal of General Medicine » Volume 15
Phototherapy Using Er,Cr:YSGG Laser as a Definitive Treatment for Dentin Hypersensitivity: A Systematic Review
Authors AlHabdan A ![]() , AlAhmari F
, AlAhmari F ![]()
Received 16 January 2022
Accepted for publication 29 April 2022
Published 11 May 2022 Volume 2022:15 Pages 4871—4880
DOI https://doi.org/10.2147/IJGM.S355890
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
AlHanouf AlHabdan,1 Fatemah AlAhmari2
1Department of Restorative Dental Sciences, College of Dentistry, King Saud University, Riyadh, Saudi Arabia; 2Department of Periodontics and Community Sciences, College of Dentistry, King Saud University, Riyadh, Saudi Arabia
Correspondence: AlHanouf AlHabdan, Department of Restorative Dental Sciences, College of Dentistry, King Saud University, Riyadh, Saudi Arabia, Tel +966 556693242, Email [email protected]
Purpose: To assess the efficacy of Er,Cr:YSGG lasers in reducing dentine hypersensitivity (DH).
Methods: Electronic literature were searched through various databases (MEDLINE, SCOPUS, ProQuest, LILACS and EBSCO) up to March 2022 for articles addressing the following focused question: “In patients with dentine hypersensitivity, does an Er,Cr:YSGG laser provide a better outcome in terms of pain reduction than other dentine desensitizer agents?”. The literature was searched using combinations of the following medical subject heading (MeSH) terms and keywords: (laser OR phototherapy OR Er,Cr:YSGG laser) AND (dentine hypersensitivity OR dentine sensitivity OR dental sensitivity).
Results: A total of 486 studies were found, of which 7 randomized controlled trials were included in the review. The Er,Cr:YSGG laser wavelengths, power density and duration of irradiation used in the studies were 2780 nanometers, 0.25– 0.5 watts and 20– 60 seconds, respectively. The follow-up assessments were conducted ranging from immediately to 3 months after treatment. All studies showed that the Er,Cr:YSGG laser was effective in alleviating DH.
Conclusion: This systematic review suggests that the application of an Er,Cr:YSSG laser is effective in alleviating DH and may have limited adverse effects if adequate parameters are followed.
Keywords: phototherapy, dentine hypersensitivity, dentine sensitivity, Er,Cr:YSGG laser
Corrigendum for this paper has been published
Corrigendum for this paper has been published
Introduction
Dentinal hypersensitivity (DH) is known as one of the most irritating clinical conditions.1 DH felt by patients as sharp pain emanating from exposed dentin in reaction to warm, evaporative, material, electrical, osmotic or chemical insult.2 This condition commonly involves the cervical third of canines and premolar facial surfaces.3 Additionally, DH may be the result of dentin exposure due to enamel or cemental loss, the former of which occurs due to improper tooth brushing techniques, dietary erosion, abfraction, and parafunctional habits, while, gingival recession, periodontal disease, root planing and periodontal surgery will result in cemental loss.4–6
Many theories have been proposed to clarify the causes of DH. One among the foremost widely accepted is Braennstroem’s 1984 hydrodynamic theory, which relates the cause of DH to the increase of the fluid flow inside the dentinal tubules after the application of a cold stimulus.7 This fluid movement will elicit the nerve ending within dentinal tubules causing pain.8 Due to its multifactorial nature, DH diagnosis and treatment is complex. Hypersensitive teeth should, therefore, be examined carefully to ensure pulpal and gingival health.9 Dentin with hypersensitivity displays enlarged tubules and more tubules per surface area than dentin without sensitivity, causing discomfort and disrupting quality of life.10
Various methods of treating dentin hypersensitivity were mentioned in the literature and to be utilized they must meet certain criteria at least, such as ease of application, lack of irritability to the pulp, painlessness, rapid action, permanent effects on the dentin, and affordability. Desensitization can be accomplished by blocking pulpal sensory nerves or occluding open dentinal tubules.4,11 Potassium nitrate, silver nitrate, and strontium chloride desensitizing agents work by blocking synapses between nerve cells, thereby reducing nerve activation and pain. Many substances, including sodium fluoride, potassium oxalate, and calcium phosphate, have been shown to occlude dentinal tubules. Varnishes, cements, adhesive materials, and some laser types have also been known to occlude the dentinal tubules.4
Recently, lasers have been used as an alternative for DH treatment and have become a focus of interest for research in recent decades.11,12 There are several types of lasers used in dentistry, which are classified as hard lasers or soft lasers. Carbon dioxide (CO2) lasers, neodymium: yttrium aluminum garnet (Nd: YAG) lasers, and erbium: yttrium aluminum garnet lasers (Er: YAG) are examples of hard lasers. Low-level laser therapy (LLLT) or biostimulation are terms used to describe soft lasers based on semiconductor diode devices.13 Lasers are used for soft tissue as in periodontal treatments, therapy of oral malignancies, orthodontic treatments, and miscellaneous tissue removal in oral medicine. Lasers have also been developed to be used in hard tissue treatment, such as cavity preparation and caries and restorative material removal, along with the treatment of dentinal hypersensitivity.13,14
The erbium, chromium:yttrium, scandium, gallium, garnet laser (Er,Cr:YSGG) has a 2780 nm wavelength15 and provides advantages for both the care provider and recipient. Er,Cr:YSGG is painless, safe and precise laser that is used for hard and soft tissue treatments.12,16 As explained by Yilmaz et al17 in 2011, the Er,Cr:YSGG laser demonstrates increased absorption in water, which results in evaporation of dentinal fluids. This action leads to the insoluble salt deposition in the exposed dentinal tubules to occlude them.17
A systematic review of the literature is required to determine whether lasers are more effective than a placebo or no treatment in reducing DH. As a result, the primary goal of this systematic review is to determine the efficacy of phototherapy, particularly Er,Cr:YSGG laser therapy, in reducing DH.
Materials and Methods
Protocol Registration and Focused PICO Question
This systematic review was registered at the National Institute for Health Research PROSPERO, International Prospective Register of Systematic Reviews, registration number: CRD42021255945. This systematic review was conducted based on the “Preferred Reporting Items for Systematic Review and Meta-Analysis” (PRISMA) guidelines.18 The PICO principle (ie, “Patients” – adults with dentine hypersensitivity; “Interventions” – Er,Cr:YSGG laser “Comparisons” – other dentine desensitizer agent or no treatment group; “Outcomes” – dentine hypersensitivity reduction) was used to develop and answer the following focused question: “In patients with dentine hypersensitivity, does the Er,Cr:YSGG laser provide better outcomes in terms of pain reduction than other dentine desensitizer agents?”
Selection Criteria
The following were the inclusion criteria: (1) randomized controlled trials (RCTs); (2) adult patients (aged 18 years) with DH; (3) comparator group including subjects who were exposed to other dentine desensitizer agents or no treatment. The exclusion criteria included (a) subjects with systemic diseases; (b) studies without quantitative data; (c) studies without a scale or score to measure dentine hypersensitivity; and (d) studies with incomplete irradiation protocols (wavelength, power, energy density, frequency, mode, air and water percentages).
Search Strategy
Electronic literature searches were conducted in various databases (MEDLINE; SCOPUS; ProQuest; LILACS; and EBSCO) up to March 2022 for articles published in English addressing the focused question. The combinations of the following medical subject heading (MeSH) terms and keywords were used to search the literature: MEDLINE (((laser therapy[MeSH Terms]) OR (phototherapy[MeSH Terms]) OR (Er,Cr:YSGG laser[MeSH Terms])) AND ((dentin sensitivity[MeSH Terms]) OR (dentin hypersensitivity[MeSH Terms]))); EBSCO ((laser) Subject AND (dentine sensitivity) Subject OR (dentin hypersensitivity) Subject); SCOPUS (KEY ((laser OR phototherapy)) AND KEY ((dentin sensitivity OR dentin hypersensitivity)); LILACS (dentine sensitivity OR dentin hypersensitivity) [Subject descriptor] AND (laser or phototherapy) [Subject descriptor]); ProQuest ((main subject (dentine sensitivity OR dentin hypersensitivity) AND main subject (phototherapy or laser)).
Screening Methods and Data Extraction
Article titles and abstracts that met the inclusion criteria were screened and evaluated. The information from the included studies was extracted as follows: first author and year of publication, study design (parallel or split‐mouth), type of treatment, number of teeth and subjects, mean difference of pain and percentage of DH reduction, both between baseline and follow‐up, and any recorded adverse effects.
Risk of Bias and Quality Assessments
The quality of RCT methodologies of the included studies was evaluated in accordance with the Cochrane risk-of-bias tool for randomized trials (RoB 2).19 The following domains were evaluated: the process of randomization, deviations from intended interventions, missing outcome data, measurement of the outcome, and selection of the reported result. The bias was then classified into low risk of bias (when all criteria were fulfilled), high risk of bias (when ≥1 criterion was not fulfilled), and some concerns (when ≥1 criterion was partially fulfilled).
Results
Study Selection
The electronic search initially revealed 486 potential studies according to their titles and abstract in the following databases: PubMed (n = 174), LILACS (n = 6), ProQuest (n = 15), SCOPUS (n=187), and EBSCO (n = 104). Fifty-seven studies were removed from the selection process as they were identified as duplicate studies. According to abstract screening results, 369 articles did not meet the objectives of the current review and were therefore excluded. Sixty articles were retrieved and downloaded for full review. Out of these 60 articles, 53 studies were further removed because they did not meet the inclusion criteria. The final selection of studies resulted in the inclusion of 7 RCTs for qualitative assessment.17,20–25 Figure 1 shows the detailed flow diagram of the study selection process according to the PRISMA recommendations and guidelines.26
 |
Figure 1 PRISMA flowchart of the search strategy. Notes: Adapted from Page MJ, McKenzie JE, Bossuyt PM et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71.18 Copyright 2021 Page et al. Creative Commons CC BY 4.0 (https://creativecommons.org/licenses/by/4.0/legalcode). |
General Characteristics of the Included Studies and Laser Parameters
Table 1 presents the general characteristics of all RCTs included. Three studies were conducted in the United States,17,22,25 2 studies were conducted in Iran,20,23 1 study was performed in Brazil21 and 1 study was performed in Turkey.24 Studies included in this review compared one type of laser with a placebo, another desensitizing agent or another type of laser. All publications were in English (Table 1). Four of the included studies20,21,23,24 followed a parallel study design, and the other three17,22,25 adopted a split mouth design. All of the studies were conducted at a university. Generally, all the RCTs included diagnosing dentine hypersensitivity similarly using air stimuli, A visual analog scale (VAS) was used to measure patients’ overall sensitivity, except for Ozlem et al,24 who used a precalibrated Yealp probe, and Aranha and de Paula Eduardo,21 who used slight probe pressure in addition to the air stimulus.
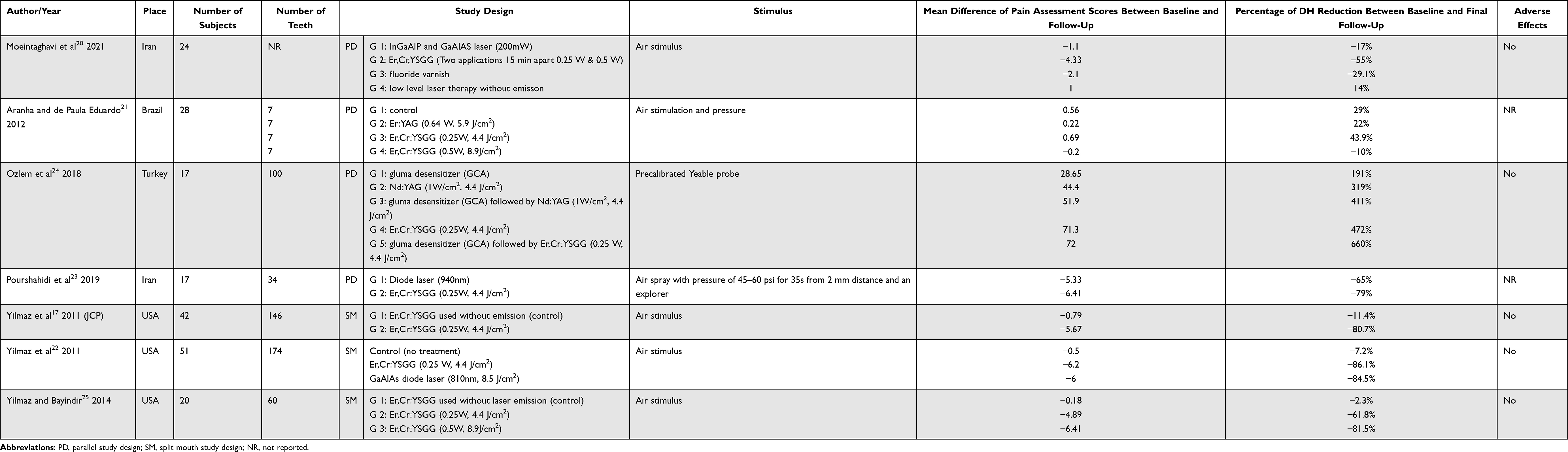 |
Table 1 General Characteristics of the Studies That Were Included in the Review |
The Er,Cr:YSGG laser parameters/settings that were used in the RCTs are shown in Table 2. The follow-up assessments were conducted ranging from immediately to 3 months after treatment. Five of the studies17,20,22,24,25 reported no relevant adverse events after laser application. The other two studies,21,23 no information was disclosed about the occurrence of any adverse events. All the included studies reported that the use of the Er,Cr:YSGG laser decreased the pain level and dentine hypersensitivity.
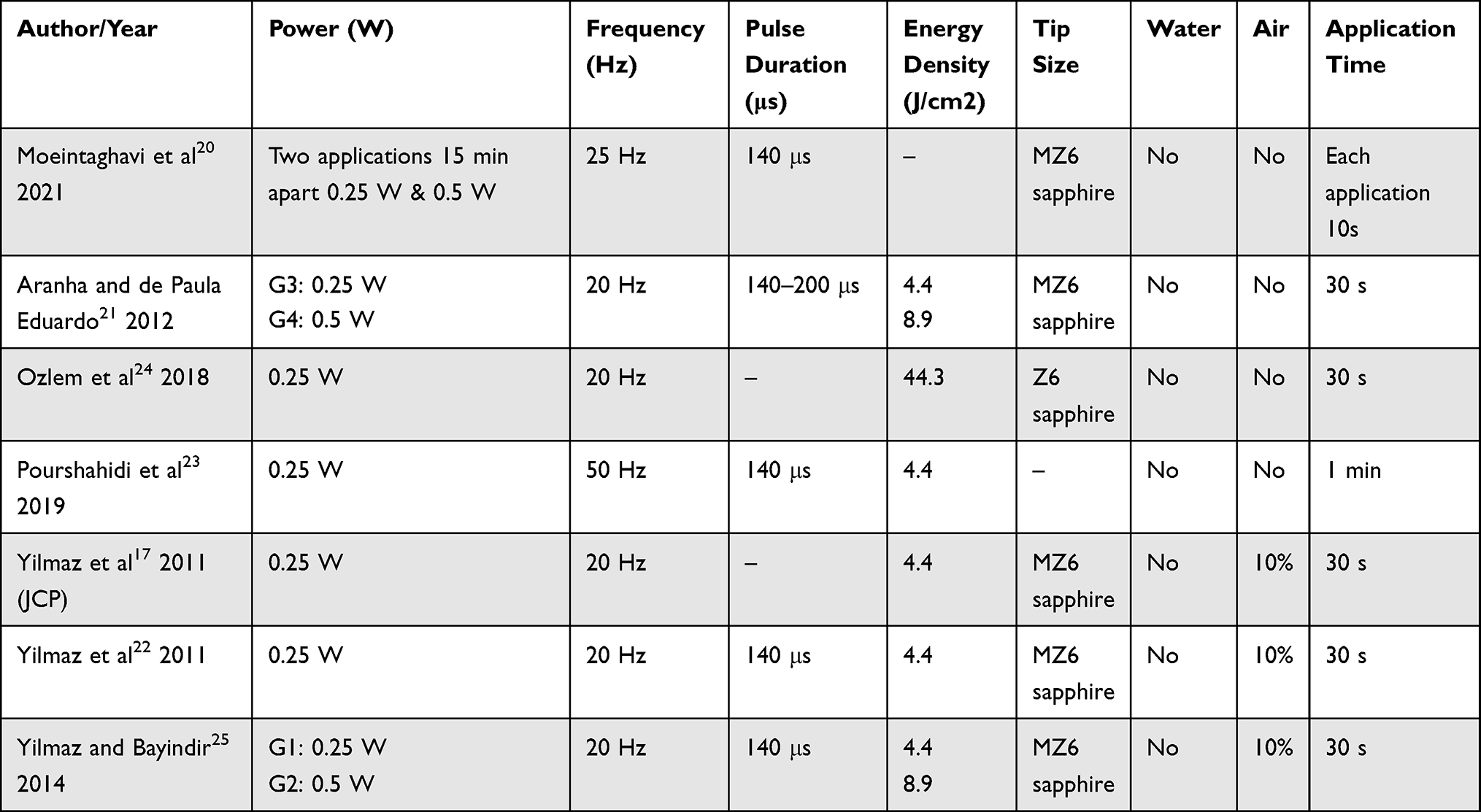 |
Table 2 Er,Cr,YSGG Laser Parameters in the Included Studies |
All included studies17,20–25 presented an appropriate randomization process, outcome measurement, and selection of the reported result. The risk of bias was considered low for all included RCTs in accordance with the recommendation of the Cochrane Handbook for Systematic Reviews of Interventions19 (Table 3).
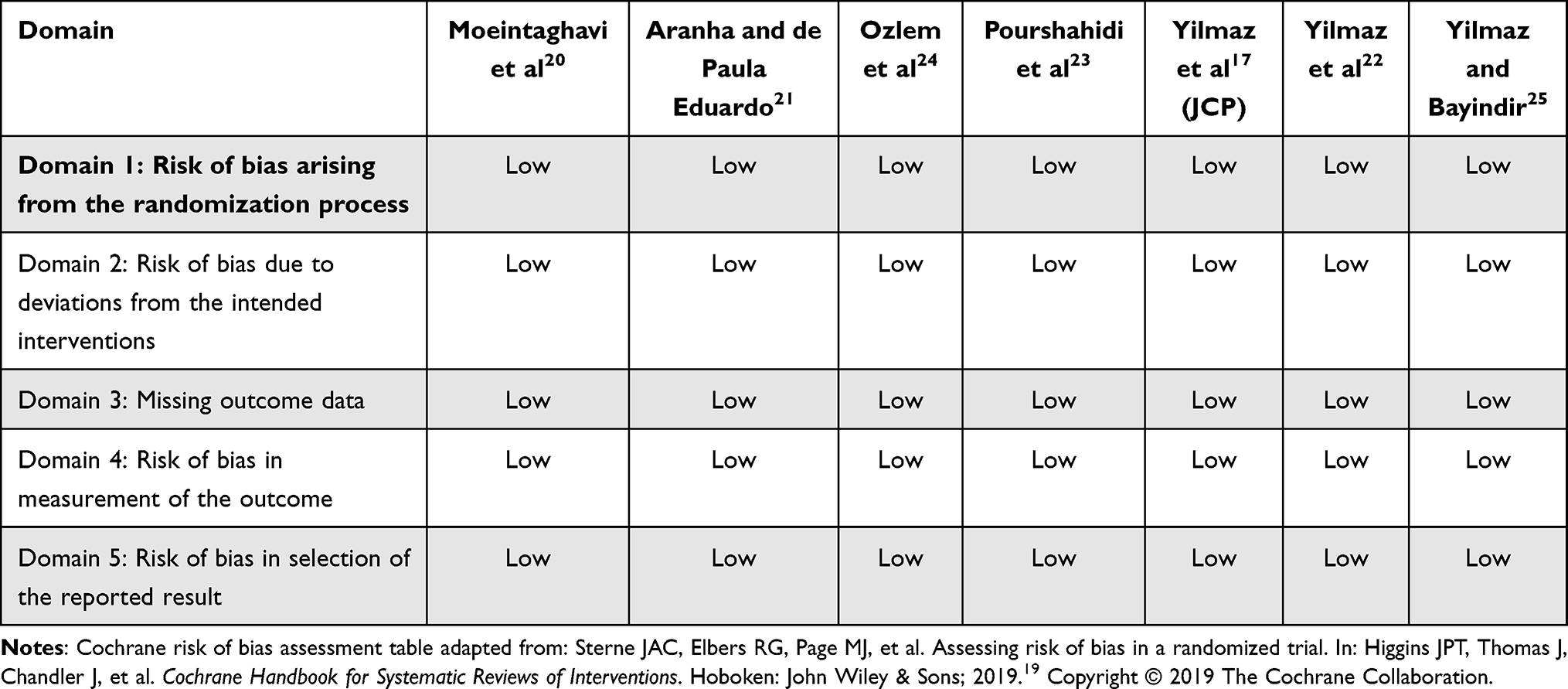 |
Table 3 Results of the Cochrane Risk of Bias Assessment of the Included RCTs |
Discussion
The present systematic review tested the hypothesis that an Er,Cr:YSGG laser is more effective than placebo or other in-office treatments for DH. According to our knowledge, this is the first systematic review to evaluate the effectiveness of an Er,Cr:YSGG laser per se in treating DH. This systematic review revealed that the Er,Cr:YSGG laser reduced DH in all of the studies compared to baseline, demonstrating that this treatment is effective in reducing DH.
Lasers with different power ranges have shown to be an effective treatment of DH.27,28 Er, Cr:YSGG is among the most used lasers in DH treatment and have shown a good result in relieving pain caused by DH.29 The efficacy of Er,Cr:YSGG laser in treating DH is owed to the increased absorption of its wavelengths (2780 nm) by water, which can evaporate dentinal fluid from the exposed tubules.17 Thus, the flow movement is reduced, and insoluble salts are formed that seal the dentinal tubules. Another proposed Er,Cr:YSGG laser mechanism is its impact on transient receptor potential channels (TRPVl), which are known to be affected by thermal stimuli.30,31
Notably, the included studies demonstrated heterogeneity in study design, laser parameters, duration of application, stimulation method, and follow-up time. However, the utilization of Er,Cr:YSGG laser was effective in treating DH without any adverse reactions in most of the protocols used in these studies.
Moeintaghavi et al20 reported that Er,Cr:YSGG laser treatment resulted in a reduction in pain severity immediately and 1 week after treatment that was greater than that produced by Galium, Aluminum, Phosphor (GaAlP) laser therapy, fluoride varnish, and placebo tests. Pourshahidi et al23 also found that pain severity decreased significantly immediately after treatment in comparison with a diode laser, but no further statistically significant decreases at the 1-week or 1-month follow-up were observed. Furthermore, Yilmaz et al22 demonstrated that both Er,Cr:YSGG, and GaAlAs lasers resulted in a reduction in DH immediately after treatment that was maintained throughout the study with no significant differences between the laser groups. Yilmaz et al17,25 reported an immediate pain level reduction following Er,Cr:YSGG use compared with the placebo. Moreover, Aranha and de Paula Eduardo21 found that the Er:YAG and Er,Cr:YSGG treated groups had pain reduction immediately after treatment. However, 0.5 W Er,Cr:YSGG laser radiation showed the most pronounced immediate effect on DH reduction. Similarly, the study by Ozlem et al24 showed that hypersensitivity could be reduced by a range of different interventions, including the use of a glutaraldehyde containing agent and Nd:YAG, and Er,Cr:YSGG lasers. Despite the good results with the other treatment modalities, there seemed to be a better effect when the Er,Cr:YSGG laser is employed.
The results of this systematic review are consistent with those from a previous meta-analysis,29,32 which reported that lasers were more efficient than placebo for DH treatment. Similarly, Rezazadeh et al’s systematic review reported that a high-level laser was effective for the treatment and prevention of DH.33 Additionally, several systematic reviews report that the Er,Cr:YSGG laser is effective in the treatment of DH and maintaining its efficacy over time.27,29,34 However, the results of this systematic review are in contrast to those from that conducted by Sgolastra et al,35 in which the evidence of the effectiveness of laser treatment was weak and the placebo effect could not be ruled out. Notably, only 3 RCTs were included in that review.35 Moreover, a meta-analysis performed by Sgolastra et al36 found a minimal clinical difference between Er,Cr:YSGG laser and placebo treatments. However, because only 3 RCTs using Er,Cr:YSSG laser therapy were included, the capacity to detect significant differences may have been limited.36
The number of studies included in the systematic review, the small sample sizes, little or no follow-up, and the lack of control groups were the study’s main shortcomings. The current systematic review included only English-language papers, which might have resulted in publication bias, with significant studies published in other languages being overlooked.37 Furthermore, due to the methodological heterogeneity of the included papers, no meta-analysis could be performed.
Conclusions
This systematic review suggests that the utilization of an Er,Cr:YSSG laser is efficient in reducing DH and may have limited adverse effects if adequate parameters are followed. However, owing to the considerable heterogeneity and small number of included studies, the current review’s findings should be interpreted with caution. To confirm the beneficial therapeutic effect of the Er,Cr:YSSG laser, a long-term RCT with a large sample size should be performed.
Abbreviations
DH, dentine hypersensitivity; MeSH, medical subject heading; CO2, carbon dioxide; Nd, YAG, neodymium: yttrium, aluminum, garnet; Er: YAG, erbium: yttrium, aluminum, garnet; LLLT, low-level laser therapy; Er,Cr:YSGG, erbium, chromium: yttrium, scandium, gallium, garnet laser; PRISMA, preferred reporting items for systematic review and meta-analysis; RCTs, randomized clinical trials; VAS, visual analog scale; TRPVl, transient receptor potential channels; GaAlP, galium, aluminum, phosphor.
Data Sharing Statement
The data of this review will be shared upon valid request to the corresponding author.
Funding
This review was not funded.
Disclosure
The authors declare no conflicts of interest in relation to this work.
References
1. Porto ICCM, Andrade AKM, Montes MAJR. Diagnosis and treatment of dentinal hypersensitivity. J Oral Sci. 2009;51(3):323–332. doi:10.2334/josnusd.51.323
2. Markowitz K, Pashley DH. Discovering new treatments for sensitive teeth: the long path from biology to therapy. J Oral Rehabil. 2008;35(4):300–315. doi:10.1111/j.1365-2842.2007.01798.x
3. Ozen T, Orhan K, Avsever H, Tunca YM, Ulker AE, Akyol M. Dentin hypersensitivity: a randomized clinical comparison of three different agents in a short-term treatment period. Oper Dent. 2009;34(4):392–398. doi:10.2341/08-118
4. Miglani S, Aggarwal V, Ahuja B. Dentin hypersensitivity: recent trends in management. J Conserv Dent. 2010;13(4):218–224. doi:10.4103/0972-0707.73385
5. Bartold PM. Dentinal hypersensitivity: a review. Aust Dent J. 2006;51(3):212–218. doi:10.1111/j.1834-7819.2006.tb00431.x
6. Addy M, Hunter ML. Can tooth brushing damage your health? Effects on oral and dental tissues. Int Dent J. 2003;53(S3):177–186. doi:10.1111/j.1875-595X.2003.tb00768.x
7. Brannstrom M. Communication between the oral cavity and the dental pulp associated with restorative treatment. Oper Dent. 1984;9(2):57–68.
8. West NX, Lussi A, Seong J, Hellwig E. Dentin hypersensitivity: pain mechanisms and aetiology of exposed cervical dentin. Clin Oral Investig. 2013;17(1):9–19. doi:10.1007/s00784-012-0887-x
9. Longridge NN, Youngson CC. Dental pain: dentine sensitivity, hypersensitivity and cracked tooth syndrome. Prim Dent J. 2019;8(1):44–51. doi:10.1177/205016841900800101
10. Mjör IA. Dentin permeability: the basis for understanding pulp reactions and adhesive technology. Braz Dent J. 2009;20(1):3–16. doi:10.1590/S0103-64402009000100001
11. Lopes AO, Aranha ACC. Comparative evaluation of the effects of Nd: YAG laser and a desensitizer agent on the treatment of dentin hypersensitivity: a clinical study. Photomed Laser Surg. 2013;31(3):132–138. doi:10.1089/pho.2012.3386
12. Asnaashari M, Moeini M. Effectiveness of lasers in the treatment of dentin hypersensitivity. J Lasers Med Sci. 2013;4(1):1–7.
13. Verma SK, Chaudhari P, Maheshwari S, Singh R. Laser in dentistry: an innovative tool in modern dental practice. Natl J Maxillofac Surg. 2012;3(2):124–132. doi:10.4103/0975-5950.111342
14. Luke AM, Mathew S, Altawash MM, Madan BM. Lasers: a review with their applications in oral medicine. J Lasers Med Sci. 2019;10(4):324–329. doi:10.15171/jlms.2019.52
15. Hossain M, Nakamura Y, Yamada Y, Kimura Y, Matsumoto N, Matsumoto K. Effects of Er, Cr: YSGG laser irradiation in human enamel and dentin: ablation and morphological studies. J Clin Laser Med Surg. 1999;17(4):155–159. doi:10.1089/clm.1999.17.155
16. Ramos TM, Ramos-Oliveira TM, Moretto SG, de Freitas PM, Esteves-Oliveira M, de Paula Eduardo C. Microtensile bond strength analysis of adhesive systems to Er: YAG and Er, Cr: YSGG laser-treated dentin. Lasers Med Sci. 2014;29(2):565–573. doi:10.1007/s10103-012-1261-6
17. Yilmaz HG, Cengiz E, Kurtulmus‐Yilmaz S, Leblebicioglu B. Effectiveness of Er, Cr: YSGG laser on dentine hypersensitivity: a controlled clinical trial. J Clin Periodontol. 2011;38(4):341–346. doi:10.1111/j.1600-051X.2010.01694.x
18. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
19. Sterne JAC, Elbers RG, Page MJ, et al. Assessing risk of bias in a randomized trial. In: Higgins JPT, Thomas J, Chandler J, et al, editors. Cochrane Handbook for Systematic Reviews of Interventions. Hoboken: John Wiley & Sons; 2019.
20. Moeintaghavi A, Ahrari F, Nasrabadi N, Fallahrastegar A, Sarabadani J, Rajabian F. Low level laser therapy, Er, Cr: YSGG laser and fluoride varnish for treatment of dentin hypersensitivity after periodontal surgery: a randomized clinical trial. Lasers Med Sci. 2021;36(9):1949–1956. doi:10.1007/s10103-021-03310-4
21. Aranha ACC, de Paula Eduardo C. Effects of Er: YAG and Er, Cr: YSGG lasers on dentine hypersensitivity. Short-term clinical evaluation. Lasers Med Sci. 2012;27(4):813–818. doi:10.1007/s10103-011-0988-9
22. Yilmaz HG, Kurtulmus-Yilmaz S, Cengiz E, Bayindir H, Aykac Y. Clinical evaluation of Er, Cr: YSGG and GaAlAs laser therapy for treating dentine hypersensitivity: a randomized controlled clinical trial. J Dent. 2011;39(3):249–254. doi:10.1016/j.jdent.2011.01.003
23. Pourshahidi S, Ebrahimi H, Mansourian A, Mousavi Y, Kharazifard M. Comparison of Er, Cr: YSGG and diode laser effects on dentin hypersensitivity: a split-mouth randomized clinical trial. Clin Oral Investig. 2019;23(11):4051–4058. doi:10.1007/s00784-019-02841-z
24. Ozlem K, Esad GM, Ayse A, Aslihan U. Efficiency of lasers and a desensitizer agent on dentin hypersensitivity treatment: a clinical study. Niger J Clin Pract. 2018;21(2):225–230. doi:10.4103/njcp.njcp_411_16
25. Yilmaz HG, Bayindir H. Clinical and scanning electron microscopy evaluation of the Er, Cr: YSGG laser therapy for treating dentine hypersensitivity: short‐term, randomised, controlled study. J Oral Rehabil. 2014;41(5):392–398. doi:10.1111/joor.12156
26. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg. 2010;8(5):336–341. doi:10.1016/j.ijsu.2010.02.007
27. Marto CM, Baptista Paula A, Nunes T, et al. Evaluation of the efficacy of dentin hypersensitivity treatments-A systematic review and follow-up analysis. J Oral Rehabil. 2019;46(10):952–990. doi:10.1111/joor.12842
28. Simões TM, Melo KC, Fernandes-Neto JA, et al. Use of high- and low-intensity lasers in the treatment of dentin hypersensitivity: a literature review. J Clin Exp Dent. 2021;13(4):e412–e417.
29. Mendes ST, Pereira CS, Oliveira JL, Santos VC, Gonçalves BB, Mendes DC. Treatment of dentin hypersensitivity with laser: systematic review. BrJP. 2021;11(4):152–160.
30. Matsumoto K, Hossain M, Hossain MI, Kawano H, Kimura Y. Clinical assessment of Er, Cr: YSGG laser application for cavity preparation. J Clin Laser Med Surg. 2002;20(1):17–21. doi:10.1089/104454702753474968
31. Jacboson B, Berger J, Kravitz R, Patel P. Laser pediatric crowns performed without anesthesia: a contemporary technique. J Clin Pediatr Dent. 2003;28(1):11–12. doi:10.17796/jcpd.28.1.t4v16x7757245q64
32. Lin PY, Cheng YW, Chu CY, Chien KL, Lin CP, Tu YK. In‐office treatment for dentin hypersensitivity: a systematic review and network meta‐analysis. J Clin Periodontol. 2013;40(1):53–64. doi:10.1111/jcpe.12011
33. Rezazadeh F, Dehghanian P, Jafarpour D. Laser effects on the prevention and treatment of dentinal hypersensitivity: a systematic review. J Lasers Med Sci. 2019;10(1):1–11. doi:10.15171/jlms.2019.01
34. Kong Y, Lei Y, Li S, Zhang Y, Han J, Hu M. Network meta-analysis of the desensitizing effects of lasers in patients with dentine hypersensitivity. Clin Oral Investig. 2020;24(6):1917–1928. doi:10.1007/s00784-019-03051-3
35. Sgolastra F, Petrucci A, Gatto R, Monaco A. Effectiveness of laser in dentinal hypersensitivity treatment: a systematic review. J Endod. 2011;37(3):297–303. doi:10.1016/j.joen.2010.11.034
36. Sgolastra F, Petrucci A, Severino M, Gatto R, Monaco A. Lasers for the treatment of dentin hypersensitivity: a meta-analysis. J Dent Res. 2013;92(6):492–499. doi:10.1177/0022034513487212
37. Moher D, Fortin P, Jadad AR, et al. Completeness of reporting of trials published in languages other than English: implications for conduct and reporting of systematic reviews. Lancet. 1996;347(8998):363–366. doi:10.1016/S0140-6736(96)90538-3
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.