Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Photodynamic Therapy Combined with Cryotherapy and Surgery for Multiple Actinic Keratoses and Well-Differentiated Cutaneous Squamous Cell Carcinoma: A Two-Case Report
Authors He X, Gao Y, Jiang S, Tang X, Wang D, Lin L, Deng Y
Received 27 January 2026
Accepted for publication 1 July 2026
Published 16 July 2026 Volume 2026:19 596319
DOI https://doi.org/10.2147/CCID.S596319
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Michela Starace
Xueyang He,1 Yunfeng Gao,2 Shali Jiang,1 Xinyue Tang,1 Dan Wang,1 Li Lin,3 Yongqiong Deng1
1Department of Dermatology, Chengdu First People’s Hospital, Chengdu, Sichuan, People’s Republic of China; 2Department of Urology, Chengdu Second People’s Hospital, Chengdu, Sichuan, People’s Republic of China; 3Department of Pathology, Chengdu First People’s Hospital, Chengdu, Sichuan, People’s Republic of China
Correspondence: Yongqiong Deng, Email [email protected]
Abstract: Multiple actinic keratoses(AK)with field cancerization and cutaneous squamous cell carcinoma(cSCC) are difficult to treat in dermatology. These diseases represent different stages of keratinocyte damage and have common treatment approaches. Available treatment methods include drug therapy, surgery, cryotherapy, and photodynamic therapy (PDT). However, in elderly patients with extensive and multiple lesions, it is difficult to completely clear the lesions with a single therapy. This article presents two elderly patients with multiple actinic keratoses, one of whom was also diagnosed with well-differentiated cSCC. PDT combined with cryotherapy and surgery was applied to the two patients, respectively, achieving favorable therapeutic and cosmetic outcomes with good patient tolerance.
Keywords: actinic keratosis, squamous cell carcinoma, field cancerization, photodynamic therapy, cryotherapy, surgery, ALA
Introduction
Actinic keratosis (AK) is a common skin disorder characterized by dysplastic proliferation of epidermal keratinocytes. AK is defined by the World Health Organization(WHO) as a precancerous lesion that may progress into cutaneous squamous cell carcinoma(cSCC). Global prevalence of AK is approximately 14%, with the highest rates reported in Australia.1 Factors associated with an increased risk of developing AK include male sex, an age exceeding 45 years, fair skin type, light hair, light eye color, facial or arm freckles, a positive history of non - melanoma skin cancer (NMSC), sunburn during childhood and adulthood, severe sunburn, long - term occupational and/or recreational sun exposure, baldness, and the utilization of potentially photosensitizing thiazide diuretics or other photosensitizing cardiac medications.2 In several Danish studies, a cumulative exposure to hydrochlorothiazide (HCTZ) of 50,000 mg or more was associated with a fourfold increase in the risk of SCC.3 Repeated and prolonged sun exposure is the main risk factor for AK development, with reported progression rates to invasive SCC ranging from 0.025% to 16%.4 Immunosuppressed individuals, especially organ transplant recipients, have a higher risk of AK and cSCC.5
The concept of field cancerization was first proposed by Slaughter et al in 1953, based on histological findings of atypical cells surrounding oral SCC.6 A recent European consensus proposed that field cancerization refers to the region of subclinical change at the edge of clinically visible AK lesions, which has a similar genetic change to those of macroscopic AKs.7 Clinically, field cancerization comprises adjacent anatomical regions of AK and sun - damaged skin, which may display at least two of the following features: telangiectasia, atrophy, abnormal pigmentation, and a sandpaper - like appearance.2
Field-directed treatment is recommended by the European consensus for multiple or extensive AK lesions and for subclinical field cancerization area resulting from chronic sun damage. Agents such as 5-fluorouracil and imiquimod, as well as PDT, are used as field-directed options.2 For patients with multiple AKs and well-differentiated cSCC, given the large and widespread area of skin involvement, surgery combined with PDT-based field-directed treatment can be used as the first choice and can improve the clearance rate. Given the non-invasive nature, high clearance rates, tolerability, and cosmetic benefits of ALA-PDT, we used ALA-PDT in combination with cryotherapy and surgery to treat two elderly patients with multiple AKs respectively, one of the two patients also had well-differentiated cSCC.
Case Report
Case 1
An 84-year-old female presented with multiple areas of erythema and plaques on the scalp that had developed progressively over two years. The initial sporadic lesions were asymptomatic but increased in number and size, with the larger lesions causing pain. The patient reported no history of hypertension, diabetes, or coronary heart disease. Dermatological examination revealed erythema and brown plaques on the scalp with surface keratosis, visible capillary dilation, atrophy, and pigmentation, but no exudation or ulceration (Figure 1A). Dermoscopy showed a diffuse erythematous background characterized by glomerular and linear vessels, prominent shiny white streaks, yellow-white keratin plugs within the hair follicles, and superficial yellowish-white scales (Figure 2A and B). Histopathology confirmed hyperkeratosis with parakeratosis of the epidermis, atypical squamous epithelial cell hyperplasia, band-like lymphocyte infiltration, and degeneration of elastic fibers in the superficial dermis (Figure 2E–G). Based on the clinical features, dermoscopy, and histopathological examination, a diagnosis of multiple AKs with field cancerization was made.
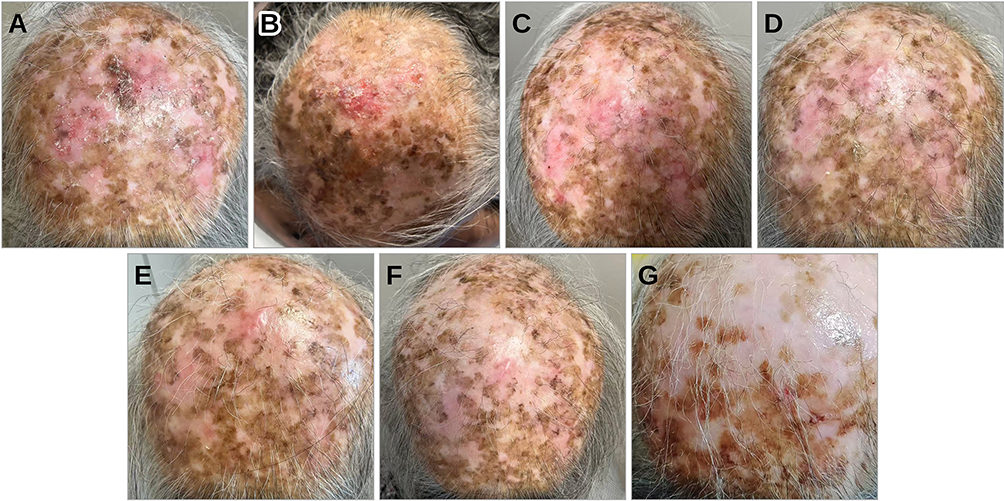 |
Figure 1 Images of the patient before and after photodynamic therapy. (A) The scalp lesion before ALA-PDT. (B–F) The lesion before the first to fifth sessions of cryotherapy combined with ALA-PDT, performed at two-week intervals. (G) One year after five sessions of ALA-PDT. |
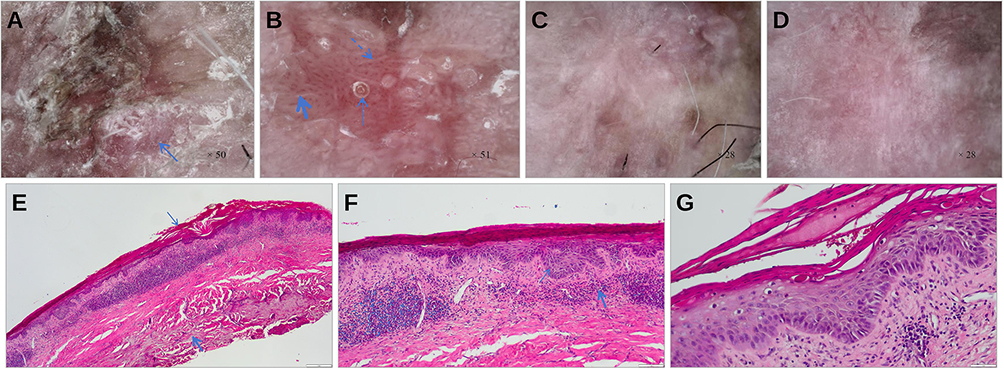 |
Figure 2 Dermoscopic and histopathological findings of the scalp lesion. (A and B) Dermoscopic images of the scalp lesion before ALA-PDT. (A) An erythematous background with surface keratinization (thin solid arrow). (B) A typical erythematous background characterized by glomerular and linear vessels (thick solid arrow), prominent shiny white streaks (dashed arrow), yellow-white keratin plugs within the hair follicles (thin solid arrow),and superficial yellowish-white scales. (C and D) Dermoscopic images of the scalp lesion after three sessions of ALA-PDT; the erythematous background faded, the yellow-white follicular plugs decreased, and the linear and glomerular vessels and shiny white streaks diminished. (E–G) Histopathological findings of the lesions (hematoxylin and eosin staining; (E) ×40; (F) ×100; (G) ×200), showing hyperkeratosis with parakeratosis of the epidermis (thin solid arrow in (E)), atypical squamous epithelial cell hyperplasia (thin solid arrow in (F)), band-like lymphocytic infiltration (thick solid arrow in (F)), and degeneration of elastic fibers in the superficial dermis (thick solid arrow in (E)). All arrows are blue. |
Considering the patient’s age and the extent of the lesions, PDT-based field-directed treatment was adopted. To facilitate the penetration of the photosensitizer, the lesions were initially treated with cryotherapy, and the hypertrophic and hyperkeratotic regions within the lesions were curetted before PDT. Freshly prepared 20% ALA cream (Shanghai FudanZhangjiang Bio-Pharmaceutical company, located in Shanghai,China) was then applied to the AK lesions and to areas showing signs of field cancerization, extending up to 1 cm beyond their margins. The treated skin was covered with a light-shielding dressing for four hours. Photodynamic diagnosis (PDD) confirmed the treatment area, and PDT was performed with a 635 nm LED red light at an initial output of 60 mW/cm2 for five minutes, which was increased to 80 mW/cm2 for 30 minutes as the patient’s pain tolerance improved (LD600-C, Wuhan Yage Optic and Electronic Technique Co., Ltd., Wuhan, China). PDD confirmed the absence of residual fluorescence after irradiation. Treatment was repeated every two weeks for five consecutive sessions.
Significant improvement in clinical symptoms, photoaging scores, and dermoscopic findings was observed after the treatment (Figure 1B–F; Figure 2C and D; Table 1). The pain during treatment was tolerable. A 5% imiquimod ointment was applied every other day after the five ALA-PDT sessions; however, after one week, the patient reported local skin pain and erosion, so imiquimod was discontinued and not resumed. One-year follow-up showed no new lesions, and clinical follow-up is still in progress (Figure 1G).
 |
Table 1 Photoaging Scores in Case One |
Case 2
A 79-year-old female presented with a 6-year history of a papule at the left inner canthus and gradually enlarging lesions on the left cheek and left temporal region over the previous five years. The patient reported no history of hypertension, diabetes, or coronary heart disease. On dermatological examination, the left inner canthus showed a round keratotic papule measuring 1 cm in diameter without surface ulceration (Figure 3A). The left cheek showed a circular keratotic papule approximately 0.8 cm in diameter, while the left temporal region showed a plaque about 5 cm in diameter with overlying hyperkeratosis (Figure 3B). Histopathological examination of the left inner canthus showed atypical epidermal hyperplasia and structural disorder with hyperkeratosis and keratin pearl formations, together with basophilic degeneration of the dermal collagen fibers and lymphocyte infiltration (Figure 4A and B). Histopathological examination of the left temporal lesion showed squamous epithelium with full-thickness atypical hyperplasia, a small amount of lymphocyte infiltration in the superficial dermis, and significant solar degeneration of elastic fibers (Figure 4C and D). Histopathology of the left cheek was consistent with AK. Based on the clinical features and histopathological examination, the diagnosis of multiple AKs with well-differentiated cSCC was made.
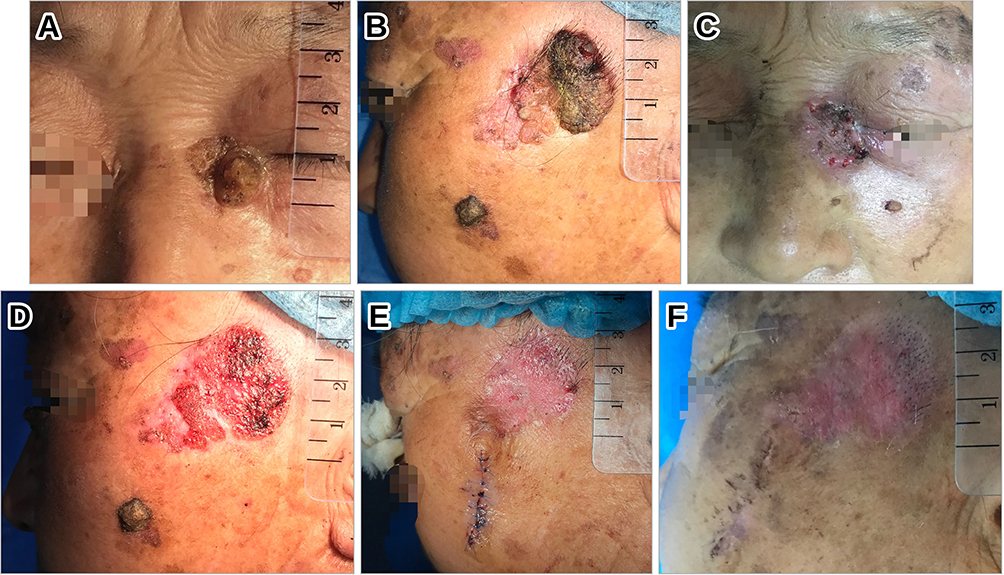 |
Figure 3 Images of the patient before and after treatment. (A) The left inner canthal lesion before treatment. (B) The left cheek and temporal lesions before treatment. (C) The left inner canthus lesion after surgical excision and skin grafting. (D) The left temporal region after laser ablation during the first photodynamic therapy session. (E) The left temporal lesion before the second photodynamic therapy session. (F) The left temporal lesion before the third photodynamic therapy session. |
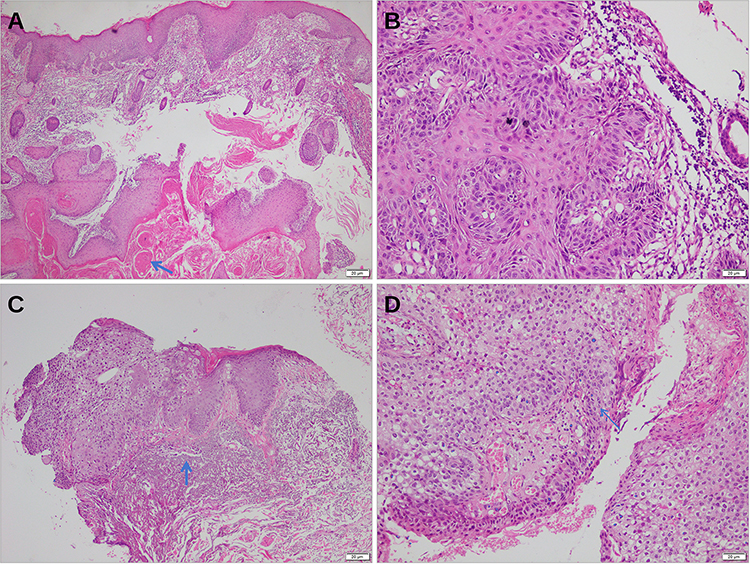 |
Figure 4 Histopathological features of the left inner canthal and left temporal lesions. (A and B) Histopathology of the left inner canthus (hematoxylin and eosin staining; (A) ×40; (B) ×200): atypical epidermal hyperplasia and structural disorder with hyperkeratosis and keratin pearl formation (arrow in (A)), together with basophilic degeneration of the dermal collagen fibers and lymphocytic infiltration. (C and D) Histopathology of the left temporal lesion (hematoxylin and eosin staining; (C) ×100; (D) ×200): squamous epithelium with full-thickness atypical hyperplasia (arrow in (D)), a small amount of lymphocyte infiltration in the superficial dermis, and significant solar degeneration of elastic fibers (arrow in (C)). All arrows are blue. |
Considering the patient’s advanced age and extensive lesions, a combination of PDT and surgery was determined to be the optimal approach. The left inner canthal lesion was treated by wide local excision combined with skin grafting; histopathological examination of the surgical margins showed no residual tumor tissue (Figure 3C). The left cheek lesion was completely excised surgically. For the extensive lesion in the left temporal region, PDT was performed. To promote photosensitizer penetration, 20% ALA (Shanghai Fudan Zhangjiang Bio-Pharmaceutical Co., Shanghai, China) was applied to the AK lesions and the surrounding 1 cm after carbon dioxide laser ablation of the hyperkeratotic lesions (Figure 3D). The specific treatment options of ALA-PDT procedure refer case 1. After three ALA-PDT sessions (Figure 3E and F), the patient discontinued treatment for personal reasons. A 5% imiquimod ointment was subsequently applied to the lesions for two weeks. Six-month follow-up examinations showed no evidence of recurrence or new lesions.
Discussion
AK is a precancerous lesion showing many similar cytological and molecular characteristics with cSCC. Chronic UVB radiation induces the mutations and decreases of tumor suppressor proteins such as p53, p16INK4a, and PTEN, which is considered to be the key molecular mechanism of AK and cSCC.8,9 These mutations occur both in visible lesions and in the subclinical sun-exposed areas beside the AK lesions, gradually forming field cancerization. Dermoscopy also detects the early signs of progression from AK to SCC, such as curly, glomerular, or pleomorphic vessels and white halo, which are rarely observed in AK.10 In addition, dermoscopy can help in the assessment of treatment response and differential grade diagnosis of AK.
The selection of optimal treatment depends on multiple factors, including lesion severity, location, quantity, prior medical history, patient tolerance, immune status, and age. For mild AK lesions, lesion-directed therapies such as surgical excision, cryotherapy, and laser ablation are commonly employed. Surgical intervention is particularly recommended for lesions necessitating biopsy—especially those unresponsive to treatment, recurrent, or exhibiting concerning features like hypertrophy, pain, or bleeding. Field-directed therapy is more appropriate for cases involving multiple, widespread AKs or field cancerization.2 Available field-directed therapies include surgical excision, cryotherapy, curettage, PDT, and radiotherapy, as well as topical agents such as 5-fluorouracil, imiquimod, ingenol mebutate, tirbanibulin, and diclofenac.11 Recently, immune checkpoint inhibitors, particularly anti-PD-1 therapies such as cemiplimab, have been approved for adjuvant use in patients with high-risk SCC following surgery and radiotherapy.12 Field-directed treatment reduces the incidence of cSCC by preventing subclinical lesions from progressing to visible AK.13 Pre-treatment with cryotherapy, curettage, or laser before field therapy is essential for hyperkeratotic lesions.
As a non-invasive, effective, and cosmetic treatment, PDT is the preferred field-directed option for AK and cSCC. Research has demonstrated that PDT inhibits the progression of precancerous lesions while offering superior cosmetic results.14 Histologically, PDT reduces keratinocyte abnormalities, increases collagen production, and decreases the degeneration of solar elastotic fibers in the field-cancerized skin.15 Clinical studies have further confirmed the high efficacy and safety of PDT for mild to severe thick AK and field cancerization,16 particularly BF-200 ALA-PDT, which achieved up to 90% clearance after 12 weeks in mild to moderate AK.17 Combined treatment is suitable for patients with extensive, hyperkeratotic, treatment-resistant, or multifocal lesions at different sites, achieving a higher clearance rate than monotherapy.7,18 PDT combined with other therapies, such as surgery, cryotherapy, laser and microneedling, can enhance efficacy without obvious adverse reactions. Daylight PDT offers comparable efficacy with improved patient tolerance.19 In organ transplant recipients, PDT may be used to prevent cutaneous field cancerization after transplantation.20
This report describes two elderly patients with multiple and extensive skin lesions that were difficult to clear completely with a single treatment approach. The first case involved multiple AKs with field cancerization. Considering the high clearance rate and good cosmetic outcome of PDT, PDT-based field-directed treatment was adopted. Combining PDT with cryotherapy enhanced photosensitizer penetration and improved the therapeutic effect. The second case presented with multiple AKs accompanied by well-differentiated cSCC and a prolonged disease course. Pathological examination revealed different findings across the lesion sites, indicating distinct stages of disease progression—including sun damage, AK, and cSCC—necessitating prompt intervention. Considering that excessive hyperkeratosis of AK is a risk factor for early progression to SCC, we performed surgical resection of the well-demarcated cSCC and the markedly hyperkeratotic AK lesions. For the lesions of extensive, unclear boundaries in the left temporal region, a combination of photodynamic and laser therapy was utilized. The two cases reflect the advantages of PDT in the management of AK and well-differentiated cSCC.
For the follow-up of AK, there is no standard and unified method. The frequency of follow-up needs to be based on the number and activity of AK lesions previously, the history of keratinocyte carcinoma, as well as the individual’s immune status and medication situation. Guidelines suggest that for patients with multiple AKs and a history of cSCC, the follow-up schedule should follow the cSCC guidance.
Conclusion
In conclusion, PDT is particularly suitable as a first-line field treatment for patients with extensive multiple AKs, AKs associated with field cancerization, and AKs with well-differentiated cSCC, especially for elderly patients and those who cannot tolerate surgery. In this report, ALA-PDT combined with cryotherapy and surgery successfully treated multiple AKs associated with field cancerization and AKs with well-differentiated cSCC, respectively, with excellent efficacy and cosmetic results. At present, the diagnosis of field cancerization relies on clinical symptom and photodynamic fluorescence diagnosis. We hope that more methods to detect field-cancerized lesions will become available in the future, and that multiple biopsies will be taken from multiple or cSCC-suspicious lesions, so as to achieve early diagnosis and early treatment. Long-term follow-up remains essential after treatment.
Ethical Approval and Consent to Publish
The publication of this case report did not require approval from the Ethics Committee of Chengdu First People’s Hospital. Informed consent was obtained from the patients for publication of the two case reports and any accompanying images.
Funding
This study was not supported by any funding.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. George CD, Lee T, Hollestein LM, et al. Global epidemiology of actinic keratosis in the general population: a systematic review and meta-analysis. Br J Dermatol. 2024;190(4):465–7. doi:10.1093/bjd/ljad371
2. Kandolf L, Peris K, Malvehy J, et al. European consensus-based interdisciplinary guideline for diagnosis, treatment and prevention of actinic keratoses, epithelial UV-induced dysplasia and field cancerization on behalf of European Association of Dermato-Oncology, European Dermatology Forum, European Academy of Dermatology and Venereology and Union of Medical Specialists (Union Européenne des Médecins Spécialistes). J Eur Acad Dermatol Venereol. 2024;38(6):1024–1047. doi:10.1111/jdv.19897
3. Pedersen SA, Gaist D, Schmidt SAJ, et al. Hydrochlorothiazide use and risk of nonmelanoma skin cancer: a nationwide case-control study from Denmark. J Am Acad Dermatol. 2018;78(4):673–681. doi:10.1016/j.jaad.2017.11.042
4. Guorgis G, Anderson CD, Lyth J, et al. Actinic keratosis diagnosis and increased risk of developing skin cancer: a 10-year cohort study of 17,651 patients in Sweden. Acta Derm Venereol. 2020;100(8):adv00128. doi:10.2340/00015555-3486
5. Roewert-Huber J, Stockfleth E, Kerl H. Pathology and pathobiology of actinic (solar) keratosis - an update. Br J Dermatol. 2007;157:18–20. doi:10.1111/j.1365-2133.2007.08267.x
6. Slaughter DP, Southwick HW, Smejkal W. Field cancerization in oral stratified squamous epithelium; clinical implications of multicentric origin. Cancer. 1953;6(5):963–968. doi:10.1002/1097-0142(195309)6:5<963::AID-CNCR2820060515>3.0.CO;2-Q
7. Jetter N, Chandan N, Wang S, et al. Field cancerization therapies for management of actinic keratosis: a narrative review. Am J Clin Dermatol. 2018;19:543–557. doi:10.1007/s40257-018-0348-7
8. Ming M, Han W, Maddox J, et al. UVB-induced ERK/AKT-dependent PTEN suppression promotes survival of epidermal keratinocytes. Oncogene. 2010;29:492–502. doi:10.1038/onc.2009.357
9. Kanellou P, Zaravinos A, Zioga M, et al. Genomic instability, mutations and expression analysis of the tumour suppressor genes p14ARF, p15INK4b, p16INK4a and p53 in actinic keratosis. Cancer Lett. 2008;264:145–161. doi:10.1016/j.canlet.2008.01.042
10. Zalaudek I, Giacomel J, Schmid K, et al. Dermatoscopy of facial actinic keratosis, intraepidermal carcinoma, and invasive squamous cell carcinoma: a progression model. J Am Acad Dermatol. 2012;66:589–597. doi:10.1016/j.jaad.2011.02.011
11. Braathen LR, Morton CA, Basset-Seguin N, et al. Photodynamic therapy for skin field cancerization: an international consensus. J Eur Acad Dermatol Venereol. 2012;26(9):1063–1066. doi:10.1111/j.1468-3083.2011.04432.x
12. Chedid MF, Tregnago AC, Riva F, et al. Indications and mechanisms of action of the main treatment modalities for non-melanoma skin cancer. Life (Basel). 2025;15(9):1447. doi:10.3390/life15091447
13. Weinstock MA, Thwin SS, Siegel JA, et al. Chemoprevention of basal and squamous cell carcinoma with a single course of fluorouracil, 5%, cream: a randomized clinical trial. JAMA Dermatol. 2018;154(2):167–174. doi:10.1001/jamadermatol.2017.3631
14. Heppt MV, Leiter U, Steeb T, et al. S3 guideline for actinic keratosis and cutaneous squamous cell carcinoma - short version, part 1: diagnosis, interventions for actinic keratoses, care structures and quality-of-care indicators. J Dtsch Dermatol Ges. 2020;18:275–294.
15. Szeimies RM, Torezan L, Niwa A, et al. Clinical, histopathological and immunohistochemical assessment of human skin field cancerization before and after photodynamic therapy. Br J Dermatol. 2012;167(1):150–159. doi:10.1111/j.1365-2133.2012.10887.x
16. Piacquadio D, Houlihan A, Ferdon MB, et al. A randomized trial of broad area ALA-PDT for field cancerization mitigation in high-risk patients. J Drugs Dermatol. 2020;19(5):452–458. doi:10.36849/JDD.2020.4930
17. Reinhold U, Dirschka T, Ostendorf R, et al. A randomized, double-blind, Phase III, multicentre study to evaluate the safety and efficacy of BF-200 ALA (Ameluz®) vs. placebo in the field-directed treatment of mild-to-moderate actinic keratosis with photodynamic therapy (PDT) when using the BF-RhodoLED® lamp. Br J Dermatol. 2016;175(4):696–705. doi:10.1111/bjd.14498
18. Heppt MV, Steeb T, Leiter U, et al. Efficacy of photodynamic therapy combined with topical interventions for the treatment of actinic keratosis: a meta-analysis. J Eur Acad Dermatol Venereol. 2019;33:863–873. doi:10.1111/jdv.15459
19. Lacour JP, Ulrich C, Gilaberte Y, et al. Daylight photodynamic therapy with methyl aminolevulinate cream is effective and nearly painless in treating actinic keratoses: a randomised, investigator-blinded, controlled, Phase III study throughout Europe. J Eur Acad Dermatol Venereol. 2015;29(12):2342–2348. doi:10.1111/jdv.13228
20. Togsverd-Bo K, Omland SH, Wulf HC, et al. Primary prevention of skin dysplasia in renal transplant recipients with photodynamic therapy: a randomized controlled trial. Am J Transplant. 2015;15(11):2986–2990. doi:10.1111/ajt.13358
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Clinical Staging and Histopathological Grading of Inguinal Squamous Cell Carcinoma in Dogs: A Case Series Study
Jiménez-Alonso AA, Pérez-Santana CG, Cazorla-Rivero SE, Rodríguez-Esparragón F, Rodríguez Grau-Bassas E
Veterinary Medicine: Research and Reports 2025, 16:1-8
Published Date: 28 May 2025
Photodynamic Therapy Combined with Surgery: An Effective Treatment for Keloids via the YAP/Engrailed-1 Signaling Pathway
Ren Y, Zhang J, Jiang H, Wang Y, Lu Y
Clinical, Cosmetic and Investigational Dermatology 2026, 19:550493
Published Date: 25 March 2026