Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Photodynamic Therapy Combined with Surgery: An Effective Treatment for Keloids via the YAP/Engrailed-1 Signaling Pathway
Authors Ren Y, Zhang J, Jiang H, Wang Y, Lu Y
Received 30 June 2025
Accepted for publication 1 February 2026
Published 25 March 2026 Volume 2026:19 550493
DOI https://doi.org/10.2147/CCID.S550493
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Yuan Ren,* Junbo Zhang,* Hao Jiang, Yuanyuan Wang, Yuangang Lu
Department of Plastic and Cosmetic Surgery, Daping Hospital, Army Medical University, Chongqing, 400042, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yuangang Lu, Department of Plastic and Cosmetic Surgery, Daping Hospital, Army Medical University, Chongqing, 400042, People’s Republic of China, Email [email protected]
Objective: Keloid, a unique human ailment, poses challenges in scar treatment due to variable efficacy and lengthy therapy and follow-up periods. Therefore, there is a need for a novel approach to address all forms of abnormal scarring. Photodynamic therapy (PDT), although slow-acting, shows promise, particularly when combined with surgery. This study aims to assess the efficacy and potential mechanism of PDT in conjunction with surgery for keloid treatment.
Methods: Keloid patients were identified through pathological examination, and the expression of YAP and Engrailed-1 in keloid tissue was determined via immunohistochemistry. Initially, all keloids underwent treatment with 20% ALA-PDT as the initial therapeutic step (the preoperative photodynamic therapy margin extends 0.5 cm beyond the visible lesion edge to ensure full target tissue coverage), using red LED light with specific parameters. Subsequently, keloids were surgically excised 24 hours post-PDT, followed by another PDT session.
Results: Immunohistochemistry assays revealed a significant reduction in YAP and Engrailed-1 levels in keloid tissues post-PDT. Over a minimum 6-month follow-up period, no infections, scar exacerbations, or recurrences were observed, except for postoperative hyperpigmentation.
Conclusion: The combination of PDT and surgical therapy demonstrates promising results for keloid treatment. The suppression of YAP leading to reduced Engrailed-1 expression may represent a mechanism underlying the successful treatment of keloids with PDT.
Keywords: keloid, photodynamic therapy, surgery, YAP and Engrailed-1
Introduction
Keloids are benign skin conditions characterized by excessive fibrous tissue growth, resulting from persistent and abnormal inflammation at the site of a wound.1 Keloid scars exhibit overgrowth beyond the original wound boundaries, contrasting with hypertrophic scars that remain confined to the incision area.2 Both types of scars stem from impaired fibroblast proliferation and collagen deposition post-injury.3 Symptoms such as discomfort, itching, red discoloration, and uncontrollable spreading can significantly impact patients’ quality of life and mental well-being.4 Current treatment modalities for keloids encompass surgical removal and local corticosteroid injections;5 however, monotherapies are associated with high relapse rates. While combination therapies can yield favorable outcomes, they often necessitate prolonged treatment durations and follow-up periods. Consequently, there is a pressing need for innovative therapeutic strategies to consistently and effectively improve keloid healing.
Nie et al were the pioneers in demonstrating the effectiveness of combining photodynamic therapy with surgical intervention for keloid treatment.6 PDT is a feasible option. This treatment is non-invasive and secure. The process involves applying a chemical known as a photosensitizer to a lesion and then exposing it to light in the presence of molecular oxygen.7,8 In dermatology, topical PDT today employs several light sources, such as lasers, intense pulsed light, light-emitting diodes, blue light, red light, and other visible light, including natural light.9 The current photosensitizers include 5-aminolevulinic acid (ALA), an intermediate naturally occurring in the heme biosynthesis pathway, and its methyl ester, methylaminolevulinic acid (MAL).10,11 ALA and MAL do not possess intrinsic photosensitizing characteristics. They serve as pro-drugs, processed by enzymes in the heme pathway to generate protoporphyrin IX, a very potent endogenous photosensitizer.12 Upon light exposure, protoporphyrin IX is activated and interacts with molecular oxygen in the surrounding tissue, leading to the generation of fatal reactive oxygen species (ROS) and free radicals. These agents selectively eradicate quickly dividing cells.13 Topical PDT is an established treatment for malignancies including actinic keratosis, Bowen’s disease, and superficial basal cell carcinoma.14 PDT has shown effectiveness in addressing many non-neoplastic dermatological disorders, including photoaged skin, leishmaniasis, pyogenic sweat adenitis, sebaceous gland hyperplasia, and acne vulgaris.15 Research examining the molecular mechanisms underlying the anti-tumor effects of topical PDT suggests its capacity to inhibit bacterial proliferation, diminish inflammation, and regulate the immune response in various skin cell types, including keratinocytes, fibroblasts, mast cells, sebaceous glands, and hair follicles.16 Moreover, several studies suggest that topical PDT has beneficial effects on keloids. A case report shown that PDT effectively cured a persistent keloid unresponsive to many conventional therapies.17 This study seeks to combine PDT with surgical intervention for keloid treatment, while also exploring the underlying processes of PDT’s impact on keloid development.
Materials and Methods
Patients
Ten patients, aged 20 to 70, diagnosed with keloid, were randomly chosen and enrolled for our study based on histological examination performed at our hospital (Table 1). Patients get detailed information on ALA-PDT, including its indications, treatment principles, therapeutic results, possible complications, and preventive strategies. Patients were obligated to provide written informed consent.
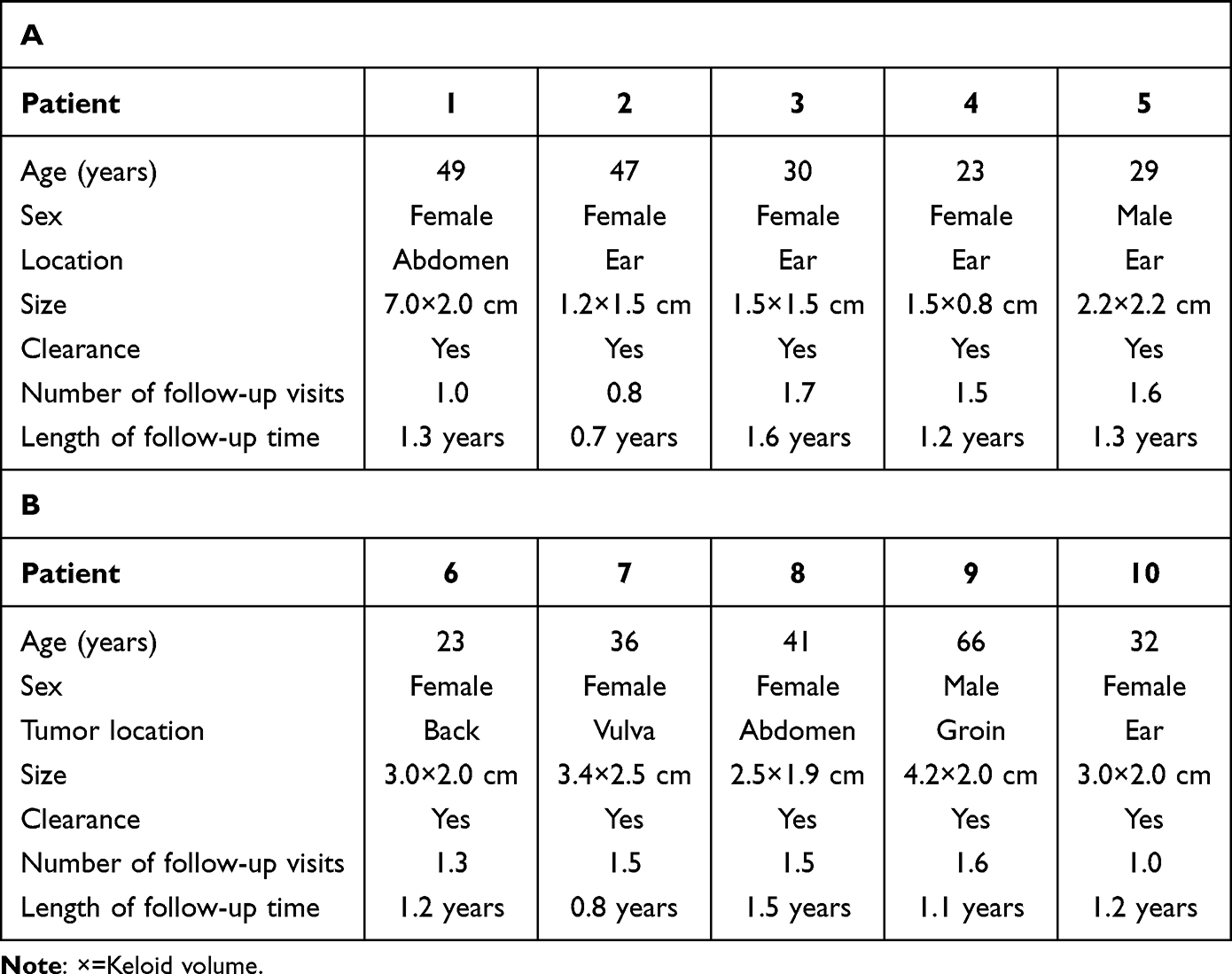 |
Table 1 Clinical Data and Follow-Up Information |
The following criteria were used to evaluate eligibility for inclusion: (1) Keloids identified by skilled plastic surgeons; (2) Participants aged 18 to 75 years; (3) Absence of prior keloid treatments, including laser therapy, radiation, or injectable therapies, during the six months before participation. The exclusion criteria included the subsequent: (1) individuals with malignant neoplasms or systemic immunological disorders; (2) pregnant or lactating women; (3) patients with substantial cardiac, hepatic, or renal impairment, in addition to coagulation abnormalities or platelet disorders.
The Procedure of ALA-PDT Treatment
Following the acquisition of the patient’s permission for treatment, the keloid underwent a solitary session of PDT. The keloid was surgically removed 24 hours after confirming the patient’s lack of any apparent adverse responses, followed by immediate PDT on the afflicted region once again (applying a wet compress of 5-ALA to the keloid lesion, extending 0.5–1 cm beyond the visible margins, before photodynamic therapy. cover with moist gauze and shield from light for 3–4 hours), then the surgical incision is meticulously closed using standard protocols to ensure optimal healing and minimize postoperative complications. The lesions situated in the region of interest and extending 0.5 cm beyond the visible lesions were treated with benzalkonium bromide for decontamination. The injury was addressed with a saline solution including 20% ALA (0.5 mL: 118 mg), produced by Fudan Zhang Jiang Biomedical Corp. in Shanghai, China. The specified area was covered with a plastic sheet and protected from all light sources for a period of 4 hours. The XD-635AB diode laser, produced by Xingda Photoelectricity Medical Equipment Corp. in Guilin, China, generated laser beams at a wavelength of 635nm once the plastic coating was removed. The laser beams were aimed at the treatment region, ensuring a uniform energy density of 120 J/cm2. The exposure length for each 3 cm2 spot size was set at 15 minutes. Numerous sources were used to light the impacted region for extensive lesions. The power output was modified to 100 milliwatts per square centimeter. The light exposure was adjusted to provide a uniform vertical distance of 5 cm from the lesions.18
Histopathologic Biopsy and Immunohistochemistry
All patients who met the stated criteria and were identified with keloids were sent to the plastic surgery department for surgical intervention. The surgical procedure was conducted following recognized guidelines, culminating in the preparation of histology slides. The surgical specimens were processed for hematoxylin and eosin staining and immunohistochemistry. The approach may be concisely articulated as follows: The study included analyzing the tissue material microscopically at a magnification of ×40, thereafter doing a more detailed inspection at a magnification of ×100. Two skilled pathologists performed independent analyses of the tissue and surgical specimens using slides. The immunohistochemical approach used primary antibodies, namely rabbit anti-YAP (Cat # 14074S, 1:200, CST) and rabbit anti-Engrailed-1 (Cat # ab108598, 1:200, Abcam). The tissue sections were processed to eliminate paraffin and then incubated with antibodies for a prolonged duration at 4°C. The samples were washed with PBS and then stained with donkey anti-rabbit IgG antibodies. The sections underwent counterstaining with hematoxylin. The intensity of positive expression in immunohistochemistry (IHC) is represented by the integrated optical density (IOD), calculated by dividing the total IOD values by the aggregate of the relevant regions.
Visual Analogue Scale
The patients’ discomfort throughout the PDT session was assessed using the Visual Analog Scale (VAS).19 The VAS is a technique used to measure the level of pain perceived by people. The process is measuring the distance in millimeters on a 10-centimeter line, with each millimeter denoting one unit, from the reference point of “no pain” to the mark specified by the patient. The approach produces ratings ranging from 0 to 10.
Statistical Analysis
Statistical analysis was conducted with GraphPad Prism 5 software created by GraphPad (USA). The statistical data were presented as the mean value with the standard error of the mean (SEM) indicated as plus or minus. The data were analyzed using Student’s t-test to compare the two groups or a one-way analysis of variance (ANOVA), followed by Tukey’s post hoc test. A P value under 0.05 was considered statistically significant.
Result
Histological analysis confirmed the diagnosis of keloids in all 10 cases, and requisite MRI or X-ray examinations were conducted. All patients had keloids measuring between 0.5 and 3 cm. The patients exhibited no notable wound infections, and no drug-resistant bacteria, including Pseudomonas, Citrobacter freundii, Staphylococcus aureus, or Serratia marcescens, were identified in the secretions.
All 10 patients had surgical excision of the keloid, with adjunctive photodynamic therapy delivered both before to and during the treatment. All surgical wounds demonstrated good healing without any occurrences of keloid recurrence or wound infections (Table 1).
Figure 1a depicts the hyperplasia of a keloid in the patient’s earlobe, which has significantly hindered everyday activities including social interactions, academic performance, and vocational functioning. This ailment has significantly impacted the patient’s psychological state. The findings indicated a significant enhancement in earlobe keloid after one year of photodynamic therapy combined with surgical surgery (Figure 1b). The pathological findings indicated that the collagen fibers in normal skin were well-structured and systematically ordered. The collagen fibers in keloids exhibit variability in size, are densely coiled, possess indistinct borders, and display disorganization, lacking adjacent skin appendages such as sweat glands, sebaceous glands, and hair follicles. Consequently, the therapeutic efficacy of the aforementioned approaches is significant and noteworthy (Figure 2a and b). Thus, the instances that underwent the aforementioned approach had favorable treatment results with notable impacts.
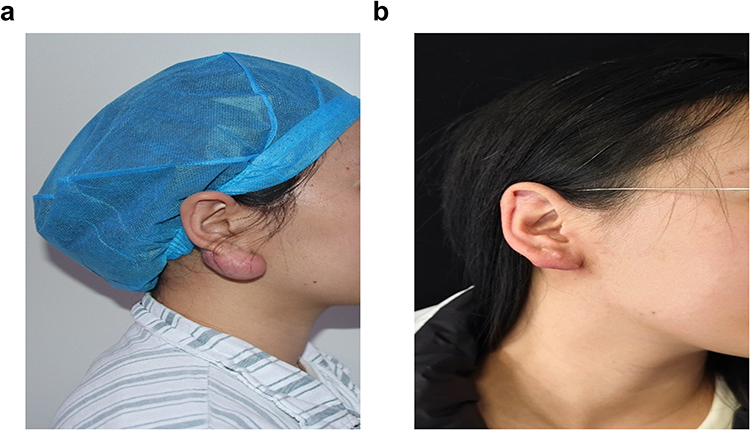 |
Figure 1 The effect of the combination of ALA-PDT and surgical excision on keloid. (a) Patients before photodynamic therapy. (b) 1 year follow-up after the whole treatment showed no local recurrence. |
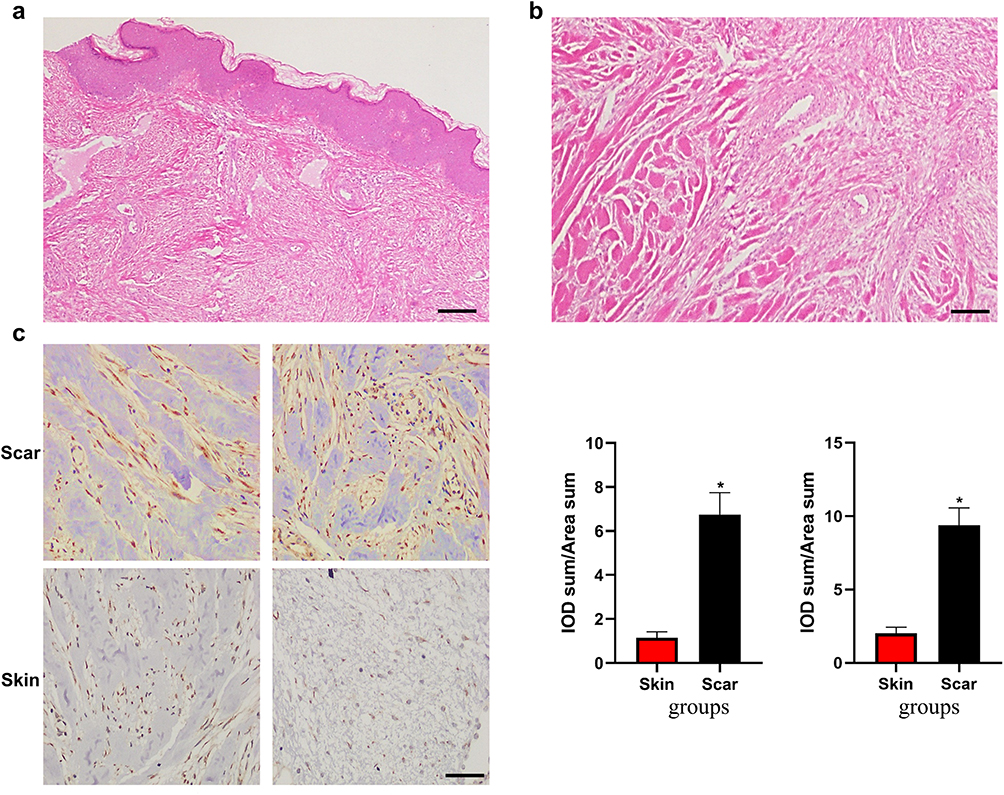 |
Figure 2 Histological analysis of normal skin and keloid using H&E staining. (a) Normal skin with thin epidermis, organized fine collagen and reduced cellularity in normal skin. (b) Whorls of haphazard hyalinized thickened collagen and increased cellularity in keloid. (c) Immunohistochemical staining revealed the expression of YAP and Engrailed-1 in keloid and skin (Scale bar, 200 μm. n=3; *P < 0.05, n=5). |
Studies have shown that scar repair in skin wounds often include the development of fibrous tissue, regulated by a distinct fibroblast lineage known as Engrailed-1 (En1). The YAP protein pathway, integral to mechanosignaling, is essential for modulating the expression of En1.20 Immunohistochemistry results demonstrated a significant elevation in the expression of En1 and YAP in keloid tissue relative to normal skin tissue (Figure 2c). Subsequently, after two sessions of photodynamic treatment, immunohistochemistry examination demonstrated a significant decrease in the expression levels of YAP and Engrailed-1 proteins in keloid cells, as well as in the surrounding skin tissues. This discovery indicates a possible new therapeutic target for photodynamic therapy in keloid treatment (Figure 3a and b). Post-PDT, some patients may have temporary localized adverse effects, such as dermal burning, heightened wound exudation, erythema, pigmentation changes, sharp pain, and infection (Table 2), often linked to the procedure’s execution. Subsequent to PDT, the Visual Analog Scale (VAS), a validated instrument for measuring subjective pain intensity, was used to assess patient-reported pain levels. Table 3 delineates the VAS ratings for all patients subsequent to each PDT session. When the VAS score above 3,18 patients received a 5 mL (50 mg) injection of flurbiprofen axetil.
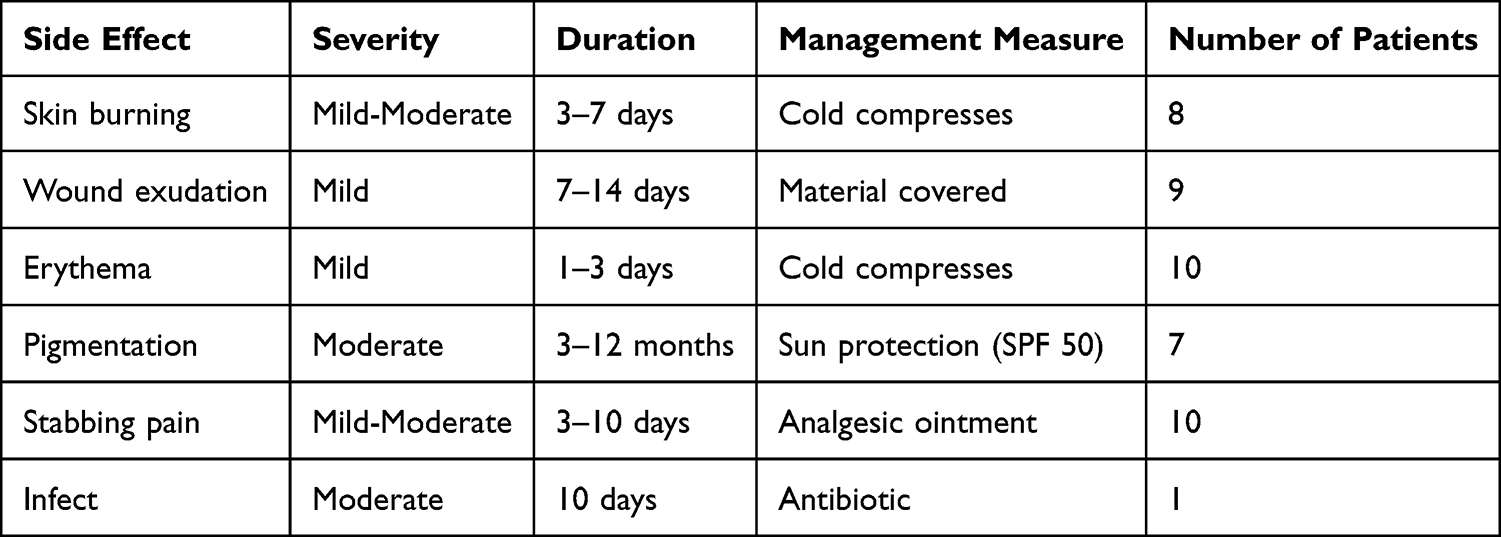 |
Table 2 PDT Treatment of Keloid Side Effects and Management Measures |
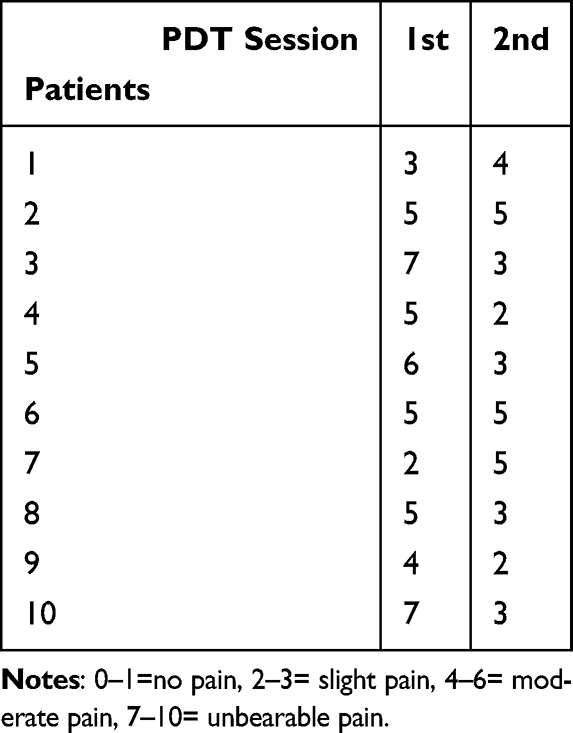 |
Table 3 VAS Score of Patients |
 |
Figure 3 (a) Immunohistochemical staining revealed YAP-positive cells in keloid tissues. (b) Immunohistochemical staining revealed Engrailed-1-positive cells in keloid tissues (Scale bar, 200 μm. n=3; **P < 0.01, n=5). |
Discussion
Keloids develop as a result of abnormal wound healing and manifest as red, hard, raised lesions. They are characterized by chronic inflammation and the overproduction of fibrous tissue.21 Their development is gradual and accompanied by significant pain, pruritus, and aesthetic concerns. The origin of keloid or hypertrophic scar development is unclear. Both disorders include an overproduction of extracellular matrix constituents, including collagen. Keloids generate around 20 times more collagen (notably collagen I and III) and 4 times more fibronectin than normal skin. The fibroblasts inside these scars are also activated. Keloid fibroblasts demonstrate increased concentrations of growth factors, including vascular endothelial growth factor, transforming growth factor-β1 and -β2, and platelet-derived growth factor-α1. The cells have a vigorous reaction to these growth factors.
It is believed that 5% to 15% of all wounds develop into keloids and hypertrophic scars, particularly in persons of Asian or African origin. The lack of animal models for these scars has resulted in a scarcity of specific drugs and treatments for them.22 Numerous cures have been identified via empirical investigation and conjecture. The most efficacious therapy now include topical-steroid injection, steroid-impregnated tape, surgical intervention, irradiation, silicone-gel sheeting, imiquimod, fluorouracil cream, and intralesional injection of bleomycin.23 Nonetheless, certain restrictions are connected with these therapies. The medications used are not just aimed at keloids and hypertrophic scars. Moreover, both steroid injections and radiation may result in adverse consequences, including skin shrinkage and telangiectasia. Moreover, dependence only on keloid surgery correlates with a significant recurrence rate, often resulting in new scars that are more severe than the initial ones. Moreover, combination medications naturally need prolonged treatment durations or follow-up. Therefore, it is important to create a very effective and consistent innovative treatment for keloids and hypertrophic scars that swiftly resolves them.
Our study results suggest that the integration of PDT with surgery for keloid treatment is a very promising therapeutic approach. This integrated method has shown significant clinical efficacy in reducing scar recurrence, improving texture and pigmentation, and increasing patient satisfaction. This treatment method had a satisfactory safety profile, marked by few side effects. Another study group showed the effectiveness and safety of combining photodynamic therapy with surgery for scar repair, with a mean follow-up period of 2.7 years.24
The specific mechanisms by which topical PDT improves abnormal scarring are mostly unknown. Nonetheless, these responses probably include reactions to the reactive oxygen species (ROS) produced by the photodynamic process. Reactive oxygen species (ROS) inflict damage on the cell membrane and mitochondria, triggering the activation of signaling molecules such as TNF-α and interleukins 1 and 6, which eventually culminates in cell death.25 Cellular demise may transpire by apoptosis, necrosis, and/or autophagy. These modifications may impact the expression of growth factors and cytokines inside the lesion, thus affecting collagen synthesis and the arrangement of the extracellular matrix. The findings indicates that ALA-PDT given to cultured normal fibroblasts significantly reduces their formation of type I collagen while enhancing the activity of collagen-degrading enzymes.26 This may explain the finding of the Bayat group that PDT induced a rearrangement of the extracellular matrix components in both hypertrophic scars and keloids.27 Moreover, several studies have shown that the photodynamic response inhibits the proliferation and motility of normal cutaneous fibroblasts cultured in a gel matrix. Moreover, it was shown that PDT markedly diminishes the expression of TGF-β1 and basic fibroblast growth factor mRNA in fibroblasts.28
The mechanical signaling factor termed yes-associated protein (YAP) has been connected with En1-lineage positive fibroblasts (EPFs), a specific fibroblast lineage that facilitates scarring. This association connects the conversion of mechanical impulses into biochemical signals (mechanotransduction) with the progression of fibrosis.29 Our results demonstrated a decrease in Engrailed-1 and YAP positive fibroblasts in keloids after PDT treatment. By inhibiting the manufacture of EPFs cells, PDT may provide a novel strategy for treating keloids by diminishing tissue fibrosis.
Nevertheless, it is important to acknowledge several limitations of our research. The results may have restricted relevance owing to the minimal sample size. Furthermore, to validate the post-PDT process for keloid therapy, it is essential to separate it from surgical intervention to ascertain the precise mechanism by which PDT alone inhibits keloid development.
Our research definitively demonstrates the effectiveness of PDT when combined with surgery for keloid therapy. The combination therapy shown significant clinical effectiveness in reducing scar size, improving texture and pigmentation, and elevating patient satisfaction. This medicine has superior safety, with a minimal incidence of adverse effects. We propose that PDT may effectively treat keloids by inhibiting the Yap tension signaling system. This would inhibit the expression of En1 in keloid tissue, resulting in the reversal of tissue fibrosis and eliciting an anti-scar action.
Data Sharing Statement
The data generated in the present study may be requested from the corresponding author.
Ethics Statement
Tissue samples of human skin were obtained from willing patients at Daping Hospital, Army Medical University (Chongqing, China). The human participant research was approved by the Research Committee and Ethics Committee of the General Hospital (Daping Hospital) of the Army Medical University, with clearance number DP2019‑46.
Patient Consent for Publication
All patients consented to the publishing of this paper and provided written informed consent.
Acknowledgments
We gratefully acknowledge Dr. Jinlong Qiu for his instrumental technical and financial support in facilitating the experimental work, and Dr. Weijie Xia for his valuable contributions to data organization.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was supported by the Chongqing Science and Health Joint Medical Research Project (2023MSXM073), Natural Science Foundation of Chongqing, China (No. CSTB2022NSCQ-MSX1681), and the Chongqing Technology Innovation and Application Development Project (Grant No. CSTB2023YSZX-JSX0003).
Disclosure
No potential conflict of interest was reported by the authors.
References
1. Steiner JE, Cottrell CE, Streicher JL, et al. Scarring in patients with PIK3CA-related overgrowth syndromes. JAMA Dermatol. 2018;154(4):452–9. doi:10.1001/jamadermatol.2017.6189
2. Kim H, Anggradita LD, Lee SJ, et al. Ameliorating fibrotic phenotypes of keloid dermal fibroblasts through an epidermal growth factor-mediated extracellular matrix remodeling. Int J Mol Sci. 2021;22(4):2198. doi:10.3390/ijms22042198
3. Zhao B, Guan H, Liu JQ, et al. Hypoxia drives the transition of human dermal fibroblasts to a myofibroblast-like phenotype via the TGF-β1/Smad3 pathway. Int J Mol Med. 2017;39(1):153–159. doi:10.3892/ijmm.2016.2816
4. Wang Q, Wang P, Qin Z, et al. Altered glucose metabolism and cell function in keloid fibroblasts under hypoxia. Redox Biol. 2021;38:101815. doi:10.1016/j.redox.2020.101815
5. Yamawaki S, Naitoh M, Kubota H, et al. HtrA1 is specifically up-regulated in active keloid lesions and stimulates keloid development. Int J Mol Sci. 2018;19(5):1275. doi:10.3390/ijms19051275
6. Nie Z, Bayat A, Behzad F, Rhodes LE. Positive response of a recurrent keloid scar to topical methyl aminolevulinate-photodynamic therapy. Photodermatol Photoimmunol Photomed. 2010;26(6):330–332. PMID: 21140993. doi:10.1111/j.1600-0781.2010.00539.x
7. Song C, Xu W, Wu H, et al. Photodynamic therapy induces autophagy-mediated cell death in human colorectal cancer cells via activation of the ROS/JNK signaling pathway. Cell Death Dis. 2020;11(10):938. doi:10.1038/s41419-020-03136-y
8. Zhao H, Sun J, Yang Y. Research progress of photodynamic therapy in wound healing: a literature review. J Burn Care Res. 2023;44(6):1327–1333. doi:10.1093/jbcr/irad146
9. Mollaeva MR, Nikolskaya E, Beganovskaya V, et al. Oxidative damage induced by phototoxic pheophorbide a 17-Diethylene glycol ester encapsulated in PLGA nanoparticles. Antioxidants. 2021;10(12):1985. doi:10.3390/antiox10121985
10. Xie Y, Hu Y, Smith DE. The proton-coupled oligopeptide transporter 1 plays a major role in the intestinal permeability and absorption of 5-aminolevulinic acid. Br J Pharmacol. 2016;173(1):167–176. doi:10.1111/bph.13356
11. Dogra Y, Ferguson DCJ, Dodd NJF, et al. The hydroxypyridinone iron chelator CP94 increases methyl-aminolevulinate-based photodynamic cell killing by increasing the generation of reactive oxygen species. Redox Biol. 2016;9:90–99. doi:10.1016/j.redox.2016.07.002
12. Richter AS, Banse C, Grimm B. The GluTR-binding protein is the heme-binding factor for feedback control of glutamyl-tRNA reductase. Elife. 2019;8:e46300. doi:10.7554/eLife.46300
13. Park W, Cho S, Kang D, et al. Tumor microenvironment targeting nano-bio emulsion for synergistic combinational X-Ray PDT with oncolytic bacteria therapy. Adv Healthc Mater. 2020;9(13):e1901812. doi:10.1002/adhm.201901812
14. Wang X, Shi L, Tu Q, et al. Treating cutaneous squamous cell carcinoma using 5-aminolevulinic acid polylactic-co-glycolic acid nanoparticle-mediated photodynamic therapy in a mouse model. Int J Nanomed. 2015;10:347–355. doi:10.2147/IJN.S71245
15. An J, Tang S, Hong G, et al. An unexpected strategy to alleviate hypoxia limitation of photodynamic therapy by biotinylation of photosensitizers. Nat Commun. 2022;13(1):2225. doi:10.1038/s41467-022-29862-9
16. Ortel B, Shea CR, Calzavara-Pinton P. Molecular mechanisms of photodynamic therapy. Front Biosci. 2009;14(11):4157–4172. doi:10.2741/3520
17. Chiu LL, Sun CH, Yeh AT, et al. Photodynamic therapy on keloid fibroblasts in tissue-engineered keratinocyte-fibroblast co-culture. Lasers Surg Med. 2005;37(3):231–244. doi:10.1002/lsm.20213
18. Zhao H, Ren Y, Kou H, Zhang J, Zhang X. Increased CD56 expression after photodynamic therapy indicates an increased natural killer cell count following early photodynamic therapy for cutaneous squamous cell carcinoma. Oncol Lett. 2024;28(2):372. doi:10.3892/ol.2024.14505
19. Lissek M, Boeker M, Happe A. How thick is the oral mucosa around implants after augmentation with different materials: a systematic review of the effectiveness of substitute matrices in comparison to connective tissue grafts. Int J Mol Sci. 2020;21(14):5043. doi:10.3390/ijms21145043
20. Mascharak S, desJardins-Park HE, Davitt MF, et al. Preventing Engrailed-1 activation in fibroblasts yields wound regeneration without scarring. Science. 2021;372(6540):eaba2374. doi:10.1126/science.aba2374
21. Li K, Nicoli F, Xi WJ, et al. The 1470 nm diode laser with an intralesional fiber device: a proposed solution for the treatment of inflamed and infected keloids. Burns Trauma. 2019;7:5. doi:10.1186/s41038-019-0143-6
22. Li J, Li Z, Wang S, et al. Exosomes from human adipose-derived mesenchymal stem cells inhibit production of extracellular matrix in keloid fibroblasts via downregulating transforming growth factor-β2 and Notch-1 expression. Bioengineered. 2022;13(4):8515–8525. doi:10.1080/21655979.2022.2051838
23. Wang CH, Shan MJ, Liu H, et al. Hyperbaric oxygen treatment on keloid tumor immune gene expression. Chin Med J. 2021;134(18):2205–2213. doi:10.1097/CM9.0000000000001780
24. Lu Z, Zhu D, Yang Y, Kou H, Li X, Zhang J. Assessment of the efficacy and safety of auricular keloids excision followed by 5-aminolevulinic acid photodynamic therapy. Photodiagnosis Photodyn Ther. 2024;50:104335. doi:10.1016/j.pdpdt.2024.104335
25. Zhang X, Wang B, O’Callaghan P, et al. Heparanase overexpression impairs inflammatory response and macrophage-mediated clearance of amyloid-β in murine brain. Acta Neuropathol. 2012;124(4):465–478. doi:10.1007/s00401-012-0997-1
26. Liu T, Ma X, Ouyang T, et al. Efficacy of 5-aminolevulinic acid-based photodynamic therapy against keloid compromised by downregulation of SIRT1-SIRT3-SOD2-mROS dependent autophagy pathway. Redox Biol. 2019;20:195–203. doi:10.1016/j.redox.2018.10.011
27. Aoki M, Matsumoto NM, Dohi T, et al. Direct delivery of apatite nanoparticle-encapsulated siRNA targeting TIMP-1 for intractable abnormal scars. Mol Ther Nucleic Acids. 2020;22:50–61. doi:10.1016/j.omtn.2020.08.005
28. George J, Tsutsumi M, Tsuchishima M. MMP-13 deletion decreases profibrogenic molecules and attenuates N-nitrosodimethylamine-induced liver injury and fibrosis in mice. J Cell Mol Med. 2017;21(12):3821–3835. doi:10.1111/jcmm.13304
29. Wu M, Matar DY, Yu Z, et al. Continuous NPWT regulates fibrosis in murine diabetic wound healing. Pharmaceutics. 2022;14(10):2125. doi:10.3390/pharmaceutics14102125
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Photodynamic Therapy Combined with Cryotherapy and Surgery for Multiple Actinic Keratoses and Well-Differentiated Cutaneous Squamous Cell Carcinoma: A Two-Case Report
He X, Gao Y, Jiang S, Tang X, Wang D, Lin L, Deng Y
Clinical, Cosmetic and Investigational Dermatology 2026, 19:596319
Published Date: 16 July 2026