Back to Journals » Blood and Lymphatic Cancer: Targets and Therapy » Volume 15
Phase II Trial of an Orelabrutinib-Based Combination Therapy in Newly Diagnosed Primary Central Nervous System Lymphoma
Authors Zhao Y ![]() , Liu X, He Q, Yu Y, Xu L, Sun C, Liu G, Wang L
, Liu X, He Q, Yu Y, Xu L, Sun C, Liu G, Wang L ![]() , Ma J
, Ma J
Received 28 July 2025
Accepted for publication 25 November 2025
Published 6 December 2025 Volume 2025:15 Pages 203—216
DOI https://doi.org/10.2147/BLCTT.S556657
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Wilson Gonsalves
Video abstract of “Orelabrutinib-based combination therapy in lymphoma” [556657].
Views: 42
Yajing Zhao,1,* Xinguang Liu,1,* Qiang He,2,* Yafei Yu,1 Lei Xu,3 Caifeng Sun,4 Guoqiang Liu,4 Liang Wang,4 Ji Ma2
1Department of Hematology, Qilu Hospital of Shandong University, Jinan, Shandong, People’s Republic of China; 2Department of Lymphoma, Shandong Cancer Hospital and Institute, Shandong First Medical University and Shandong Academy of Medical Sciences, Jinan, Shandong, People’s Republic of China; 3Department of Imaging, Shengli Oilfield Central Hospital, Dongying, Shandong, People’s Republic of China; 4Department of Hematology, Shengli Oilfield Central Hospital, Dongying, Shandong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ji Ma, Department of Lymphoma, Shandong Cancer Hospital and Institute, Shandong First Medical University and Shandong Academy of Medical Sciences, Jinan, Shandong, People’s Republic of China, Email [email protected] Liang Wang, Department of Hematology, Shengli Oilfield Central Hospital, Dongying, Shandong, People’s Republic of China, Email [email protected]
Purpose: Primary central nervous system lymphoma (PCNSL) is a rare, yet highly aggressive non-Hodgkin lymphoma confined to the central nervous system (CNS). High-dose methotrexate (HD-MTX) remains the baseline chemotherapy for newly-diagnosed PCNSL. Intensive chemotherapies combined with HD-MTX have improved patient outcomes. However, the substantial toxicities limited their applicability, especially among elderly patients with poor physical status. Optimal composition of induction and consolidation treatment are still warranted.
Patients and methods: In this prospective single-arm phase II trial (ChiCTR2200061485), we evaluated the efficacy and safety of HD-MTX combined with rituximab and orelabrutinib, a second-generation BTK inhibitor with high CNS penetration, as induction therapy in newly diagnosed PCNSL. Twenty-two patients received up to six cycles of the combined induction therapy. Patients who achieved remission proceeded to non-randomized consolidation therapies with ASCT (autologous hematopoietic stem cell transplantation), WBRT (whole-brain radiotherapy), or orelabrutinib maintenance, based on patient eligibility and physician discretion. The primary endpoint was the centrally assessed response post-induction. Secondary endpoints included progression free survival (PFS), overall survival (OS), and safety.
Results: Among the 22 enrolled patients, the overall response rate (ORR) at the end of induction therapy was 91.0%, including 9 patients (41.0%) with complete remissions (CRs), and 11 patients (50.0%) with partial remissions (PRs). With a median follow-up of 22.3 months (range 2.3– 42.4 months), the 1-year and 2-year PFS rates were 66.6% and 59.2%, respectively; OS rates were 81.8% and 66.3%, respectively. Consolidation was performed in 15 patients: 5 underwent ASCT, 4 received WBRT, and 6 received maintenance orelabrutinib. The most common adverse effects were grade 1 anemia (45.5%). Grade ≥ 3 events included neutropenia (13.6%) and pneumonia (9.0%).
Conclusion: The combination of HD-MTX, rituximab, and orelabrutinib demonstrates high response rates and manageable toxicity in newly diagnosed PCNSL, supporting further evaluation in randomized trials.
Keywords: primary central nervous system lymphoma, orelabrutinib, high-dose methotrexate, rituximab
Introduction
Primary central nervous system lymphoma (PCNSL) is a subtype of diffuse large B cell lymphoma (DLBCL) occurring exclusively in the brain, leptomeninges, cranial nerves, vitreo-retina, or spinal cord. It is a rare and aggressive lymphoma accounting for 3% of primary CNS neoplasms and 1% of non-Hodgkin lymphomas (NHLs).1 PCNSL is classified in the entity of “primary large B-cell lymphoma of immune-privileged sites” by the 2022 World Health Organization (WHO) classification of hematolymphoid tumors.2 The standard induction strategies for treating DLBCL, such as the combination of rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP), are not suitable for PCNSL due to the low capacity to cross the blood-brain barrier (BBB). While high-dose methotrexate (HD-MTX) has its advantages, there is no consensus on the optimal composition of induction and consolidation treatment for newly diagnosed PCNSL.
To improve efficacy, multi-agent chemotherapy regimens such as MATRix (methotrexate, cytarabine, thiotepa, and rituximab), MARTA (methotrexate, cytarabine, rituximab, and thiotepa), and R-MPV (rituximab, methotrexate, procarbazine, and vincristine) have been developed. The phase II IELSG32 study established the MATRix regimen as a new standard for induction chemoimmunotherapy in fit patients up to age 70, demonstrating a superior complete response rate (49%) and 2-year OS (69%) compared to methotrexate-cytarabine doublet regimens.3 MARTA and R-MPV regimens followed with consolidation therapies yielded similar efficacy, with CR rates ranging 33.3–81.8% and 2-year OS between 63.6–88.0%.4–7 However, the benefits of intensive combined chemotherapies must be weighed against increased toxicity, including hematologic adverse events and treatment-related mortality, particularly for elderly or frail patients who represent a significant proportion of the PCNSL population. Despite consolidations with autologous hematopoietic stem cell transplantation (ASCT) or whole-brain radiotherapy (WBRT), the relapse rate and survival remain suboptimal, emphasizing the persistent unmet need for safer, more effective, and CNS-penetrant therapies for treatment of PCNSL.8
The B-cell receptor (BCR) signaling pathway plays a central role in supporting the survival of B cells. Mutations in MYD88 and CD79B are common genetic alterations in PCNSL, leading to constitutive activation of BCR/toll-like receptor (TLR)-NF-κB signaling via Bruton’s tyrosine kinase (BTK).9 BTK inhibition has yielded promising results in treating mature B cell malignancies and autoimmune disorders.10,11 In patients with PCNSL, 4 BTK inhibitors have been tried and demonstrated encouraging outcomes: ibrutinib, orelabrutinib, zanubrutinib, and tirabrutinib. Ibrutinib was the most frequently used BTK inhibitor. A systematic review indicated that the overall response rate (ORR) of ibrutinib-inclusive regimen ranged from 51.9% to 89% in patients with PCNSL.12 Zanubrutinib and tirabrutinib also showed similar efficacy for the management of PCNSL in several pilot studies, while the long-term response remains to be optimized.13,14
Orelabrutinib is an irreversible, second-generation BTK inhibitor characterized by superior selectivity and higher cerebrospinal fluid (CSF)/plasma ratio compared to first-generation agents.15,16 These properties suggest a potentially improved efficacy and safety profile for CNS lymphoma. Recent clinical studies have demonstrated impressive efficacy of orelabrutinib-rituximab-methotrexate (ORM)–based induction in newly diagnosed PCNSL, with overall response rates of 71.4% to 92.3%, and complete response rates between 35.4% and 87.1% with a favorable safety profile.17–19 Nonetheless, long-term outcomes and optimal integration of orelabrutinib into sequential or consolidation strategies remain to be fully elucidated. This prospective, multicenter, phase II trial aims to address this gap by evaluating the efficacy and safety of orelabrutinib combined with HD-MTX and rituximab (OR+MTX) as induction therapy for newly diagnosed PCNSL. Furthermore, our study design allowed for subsequent consolidation with ASCT, WBRT, or orelabrutinib maintenance based on patient suitability, providing preliminary real-world insights into the feasibility and outcomes of these sequenced approaches.
Methods
Study Design and Participants
This study was a prospective, multicenter, single-arm trial evaluating the efficacy and safety of orelabrutinib, rituximab, and HD-MTX (OR+MTX) induction therapy in newly-diagnosed PCNSL. The study was conducted in 3 tertiary hospitals in China, and was approved by the institutional review board of each participating site. Informed consent was obtained from each patient in accordance with the Declaration of Helsinki. This trial is registered in the Chinese Clinical Trial Registry (ChiCTR2200061485) and the protocol is available online (https://www.chictr.org.cn).
Patients eligible for enrollment were newly diagnosed primary central nervous system lymphoma, aged from 18 to 80 years of both genders, with a histologically proven diagnosis of DLBCL. Disease lesions were exclusively localized to brain, cranial nerves, meningeal, and/or eyes. All the included patients were tolerable to chemotherapies. Patients complicated with other malignancies; those with hepatitis B virus, hepatitis C virus, or human immunodeficiency virus infection; those in pregnancy or lactation; and those with other concurrent regimens including lenalidomide during the induction period were excluded.
Procedures
Eligible patients received 6 cycles (1 cycle = 21 days) of the combined induction therapy (OR+MTX): orelabrutinib of 150 mg/day from day 1 to day 21, rituximab 375 mg/m2 on day 1, and MTX 3.5 g/m2 (0.5 g/m2 in 15min, followed by 3 g/m2 in a 3-hour infusion) on day 2. Fragile patients received a reduced dosage of MTX with no less than 2 g/m2. Patients who achieved response after induction were suggested with consolidation therapy of ASCT, WBRT, or orelabrutinib maintenance, depending on the physician discretion according to patients’ physical conditions and preference. Thiotepa-based conditioning regimen, which includes thiotepa/busulfan/cyclophosphamide (TBC), was applied in ASCT. The total dose of WBRT was 23.4–36 Gy, delivered in 1.8–2.0 Gy fractions. Orelabrutinib maintenance was given at 150 mg once daily continuously until disease progression, unacceptable toxicity, or for a maximum of 2 years in the absence of progression.
Staging and pre-treatment work-up were done at the participating center according to the International Primary CNS Lymphoma Collaborative Group guidelines, which included brain magnetic resonance image (MRI), total spine MRI, ophthalmologic examination, CSF, bone marrow biopsy, and whole-body positron emission tomography CT (PET-CT).20
Supportive Care
Primary prophylaxis with granulocyte colony-stimulating factor (G-CSF) was administered according to institutional guidelines, typically if the absolute neutrophil count (ANC) was expected to fall below 1.0 × 109/L. All patients received anti-infective prophylaxis with sulfamethoxazole and trimethoprim for pneumocystis jirovecii pneumonia and acyclovir for herpes virus reactivation. Dexamethasone (5 mg twice daily) was administered on days 1–5 in the first cycle for control of neurological symptoms and as part of the lymphoma-directed regimen. MTX elimination was monitored by serial serum levels until below 0.1 μmol/L, with leucovorin rescue initiated 24 hours post-MTX start and continued until clearance. Antifungal prophylaxis was not routinely used. Patients with grade 3–4 neutropenia or with previous fungal infection were given prophylactic voriconazole (4 mg/kg twice daily, orally or intravenously). Considering drug interactions through CYP3A4, the dosage of orelabrutinib was reduced by 50% during concomitant voriconazole administration and restored to the standard dose after discontinuation of voriconazole. Adverse events, especially cytopenia, bleeding, hepatic effects, were closely monitored, and no severe drug-related toxicity was observed.
Adverse Event Monitoring
Adverse events (AEs) were assessed clinically and via laboratory tests at the beginning of each treatment cycle and as clinically indicated between cycles. All AEs were graded according to Common Terminology Criteria for Adverse Events (version 5.0) and were recorded with the highest grade for each patient.
Study Outcomes
The primary analysis was performed both in the intention-to-treat (ITT) population and the evaluable population. The ITT population included all enrolled patients who received at least one cycle of induction therapy. The evaluable population was defined as the patients who had completed protocol-defined six cycles of the induction therapy. Patients who dropped out or died were considered non-responders for the primary endpoint analysis unless a response had already been documented. For time-to-event endpoints, data were censored at the last known follow-up date for patients without an event. The primary endpoint was the overall response rate (ORR, including PRs and CRs) after 6 cycles of the induction therapy, which was evaluated according to the International Primary CNS Lymphoma Collaborative Group guidelines.20 Response was assessed in all CNS compartments by MRI imaging, CSF cytology, and flow cytometry. Ophthalmologic examination was performed in case of eye involvement. Secondary endpoints were progression free survival (PFS), overall survival (OS), and safety issues. PFS was calculated from patient enrollment to disease progression, the last disease assessment, or death. OS was defined as the time from enrollment to death of any cause.21
Sample Size Calculation
The sample size was calculated based on a single-arm binomial test comparing the observed response rate to a historical control. According to previous studies of HD-MTX ± rituximab regimens, a historical ORR was estimated at 50%.3,22 A target ORR of 75% was considered clinically meaningful for further evaluation. Using a one-sided alpha level of 0.10 and a desired statistical power of 80%, the calculated sample size is 22 patients. This calculation pertains specifically to the primary endpoint (ORR). The study was not powered for formal hypothesis testing on secondary survival endpoints (PFS, OS), for which the analyses are considered descriptive and exploratory in this study.
Statistical Analysis
Descriptive statistics were used to summarize demographic and baseline clinical characteristics of the enrolled patients. All continuous values were expressed as medians with ranges. Comparisons among groups were performed using Kruskal-wallis test. Categorical variables were analyzed using the chi-square test or Fisher’s exact test. We used the Kaplan-Meier method to generate the survival curves. Comparisons of survival curves were done through the Log rank test. Data management and statistical analyses were performed using SPSS, version 23.0.
Results
Study Population
Between October 2019 and April 2024, 48 patients were screened for eligibility from 3 participating centers. Two patients exited the study due to consent withdrawal, and 24 patients were excluded due to simultaneous administration of lenalidomide. There were 22 patients enrolled and treated with OR+MTX. During the treatment cycles, 1 patient (#20) achieved a PR after 2 cycles of induction, but died of severe pneumonia before the next cycle of therapy; 2 patients (#21, #22) dropped out with consent withdrawal, who achieved PRs after 3 and 5 cycles of treatments, respectively—these 2 patients received thiotepa-based therapies afterwards and remained PRs until the last follow-up. Finally, 19 patients finished the 6 cycles of OR+MTX therapies as planned (Figure 1). Efficacy was assessed in intention-to-treat (ITT) population—the 22 patients who received at least one cycle of induction therapy; and in the evaluable population—the 19 patients who finished the 6 cycles of induction therapy. Demographics and baseline characteristics of the ITT population were shown in Table 1. The median age of the ITT group was 59.5 years (range 35–79), and 11 patients (50%) were female. The median Eastern cooperative oncology group (ECOG) performance status score was 1 (range 0–4). Parenchymal brain lesions were found in 18 patients, and 1 patient had spinal and eye involvement. The median Karnofsky Performance Status (KPS) score was 80 (range 40–100). The mini-mental state examination (MMSE) score at baseline was 28 (range 17–30). The median International Extra-nodal Lymphoma Study Group (IELSG) prognostic score was 3 (range 2–4). According to the Memorial Sloan-Kettering Cancer Center (MSKCC) prognostic score, there were 2 patients in low risk, 13 in moderate risk, and 7 in high risk.
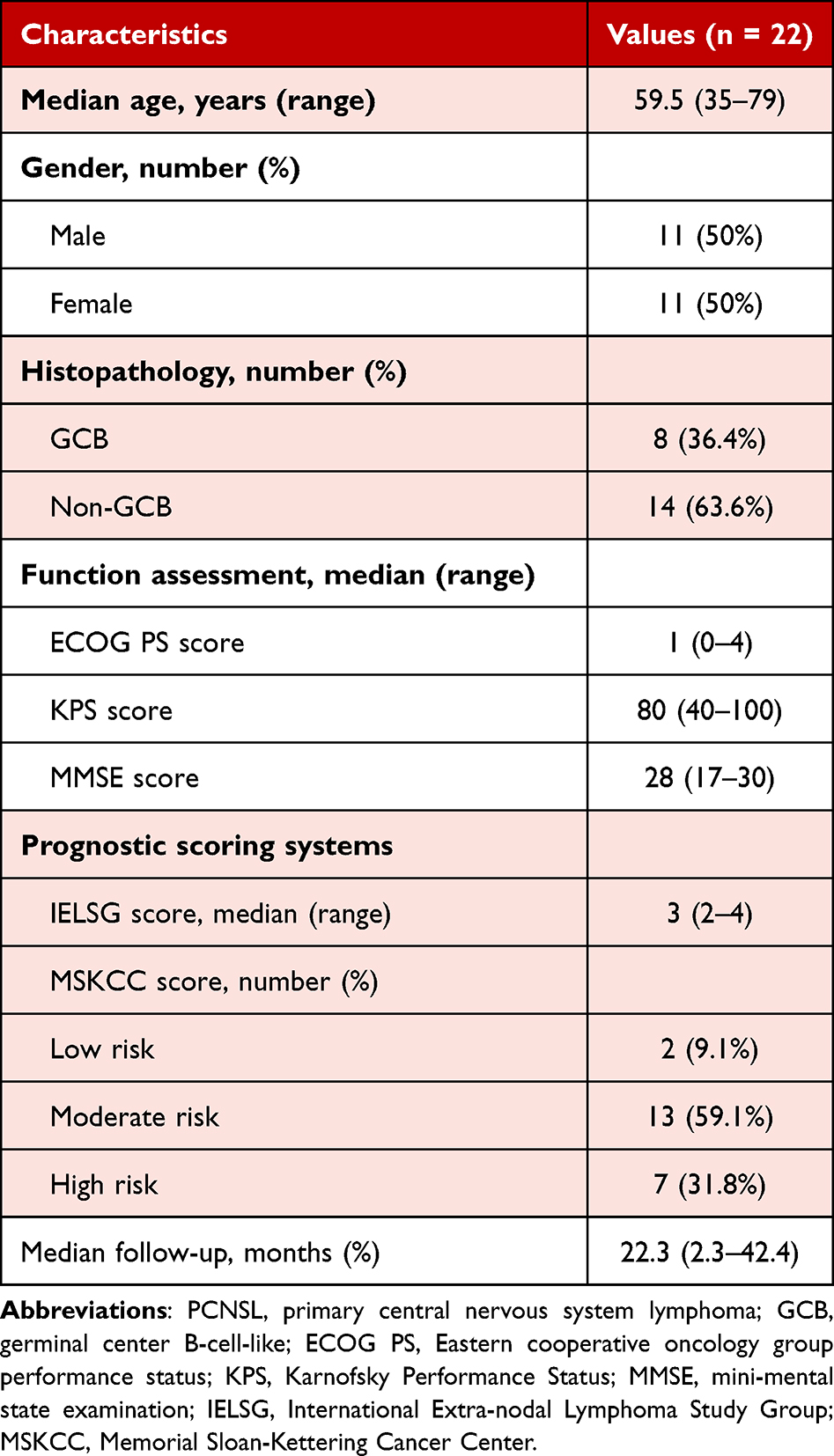 |
Table 1 Characteristics of PCNSL Patients |
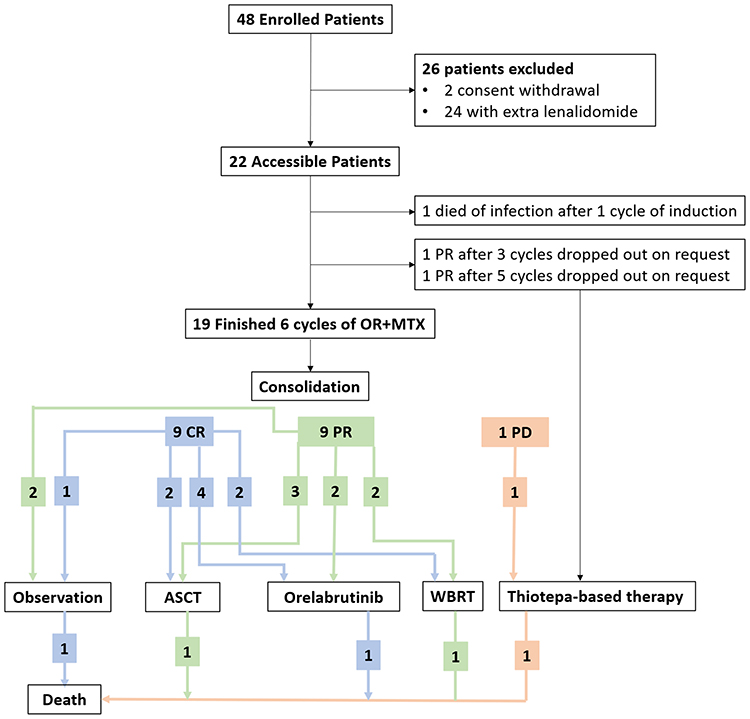 |
Figure 1 Flow diagram of study design. A total of 48 patients were screened for eligibility, with 26 patients excluded due to consent withdrawal or simultaneous administration of lenalidomide. Among the 22 patients enrolled, 1 patient died of infection and 2 patients dropped out with consent withdrawal. Finally, 19 patients (9 CRs, 9 PRs, 1 PD) finished the 6 cycles of OR+MTX therapies and entered the consolidation period. Patients with CR are shown in blue, PR in green, and PD in Orange. Abbreviations: OR+MTX, orelabrutinib, high-dose methotrexate, and rituximab induction regimen; ASCT, autologous hematopoietic stem cell transplantation; WBRT, whole-brain radiotherapy. |
After 6 cycles of induction therapy, 15 patients received consolidation therapies including ASCT, WBRT, or orelabrutinib monotherapy, based on patients’ physical conditions and preference. Three patients (#15, #16, #18) refused consolidation and then received close observations. One patient (#8) with progression disease (PD) chose thiotepa-based further chemotherapies (Figure 1). The baseline characteristics of the patients in different consolidation groups were comparable (Table 2).
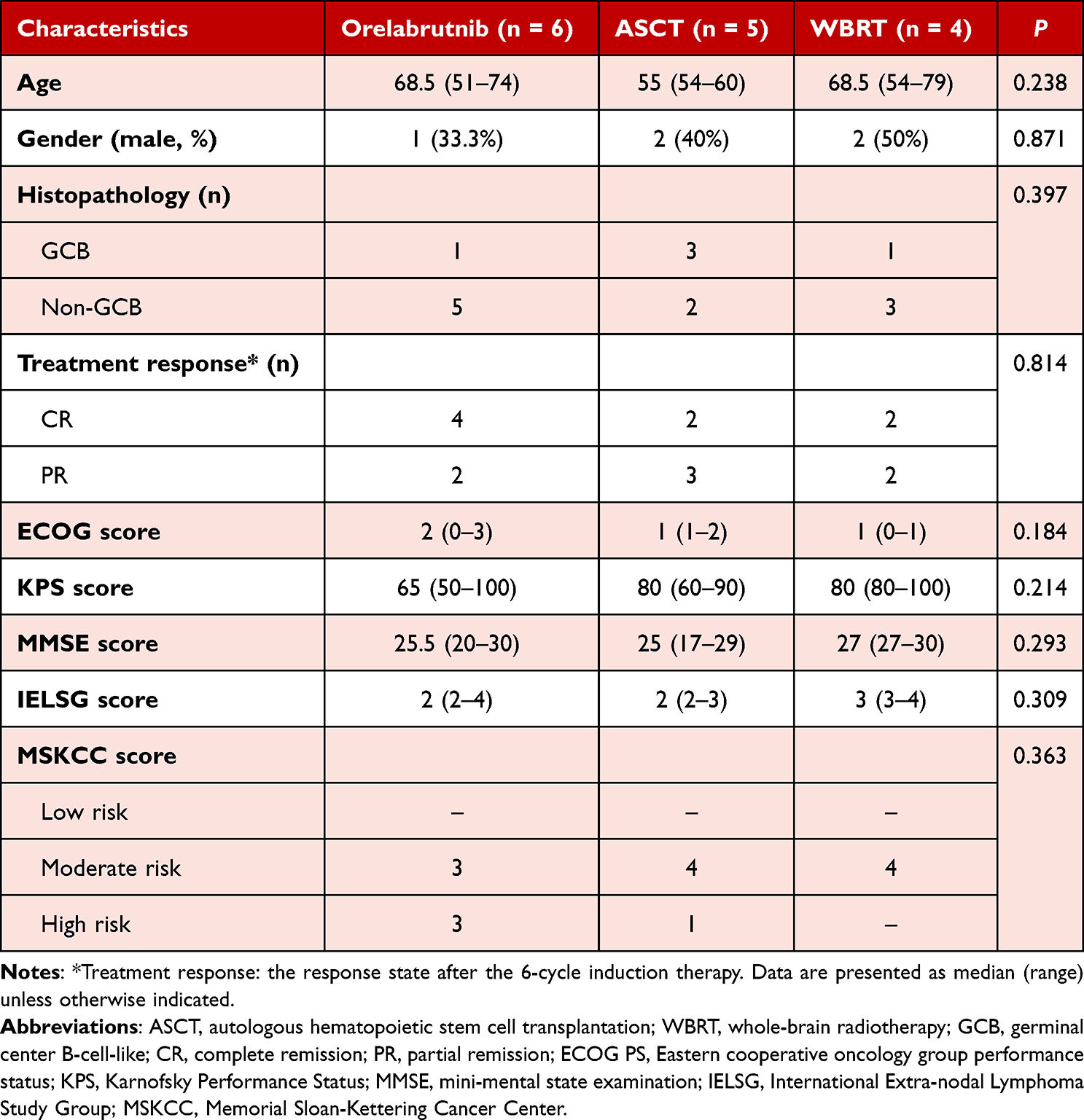 |
Table 2 Baseline Characteristics of the Patients Receiving Maintenance Therapies |
Efficacy
At a median follow-up of 22.3 months (range 2.3–42.4 months) of the ITT population, the ORR after 6 cycles was 91.0%, including 9 patients (41.0%) with CRs, and 11 patients (50.0%) with PRs. The best responses included 11 CRs (50.0%) and 11 PRs (50.0%) with a best response rate of 100% (Figure 2A). More specifically, at the end of 2 and 4 cycles of induction treatment, the CR rates were 9.1% and 41.0%, and the PR rates were 90.9% and 54.5%, respectively (Figure 2B). For the evaluable group of 19 patients who finished the 6 cycles of induction therapy, the median follow-up time was 25.9 months (range 6.3–42.4 months), the ORR was 94.7%, with 9 patients with CRs, and 9 patients with PRs. The best responses included 11 CR (52.6%) and 8 PR (47.4%) with an ORR of 100% (Figure S1A). At the end of two and four cycles of induction treatment, the CR rates were 10.5% and 47.4%, and the PR rates were 89.5% and 52.6%, respectively (Figure S1B). Fifteen patients received following consolidation therapies, among whom, 2 patients with CRs (#6, #19) and 3 patients with PRs (#11, #12, #13) received ASCT. During the follow-up, 1 patient (#12) progressed on 16.4 months, and 1 patient (#11) died of pneumonia on 8.8 months, while others remained stable disease after ASCT. Two patient (#14, #17) with CRs, 1 patient (#10) with a PR, and 1 patient (#7) with a PR but progressed at 9.7 months received WBRT consolidation. The patient (#7) with PD achieved a CR after WBRT, which maintained 10.2 months before the progression again, and died at 25.9 months of follow-up. The other 3 patients remained progression-free on the last follow-up. Orelabrutinib maintenance was carried out in 6 patients—4 patients with CRs (#3, #4, #5, #9) and 2 patients with PRs (#1, #2) after the 6 cycles of induction. One patient (#9) discontinued orelabrutinib after 6 months of maintenance therapy and relapsed at 22.3 months of follow-up, subsequently resulting in death 3 months later. Up to the last follow-up, all the other 5 patients were alive without newly-onset progression (Figure 3).
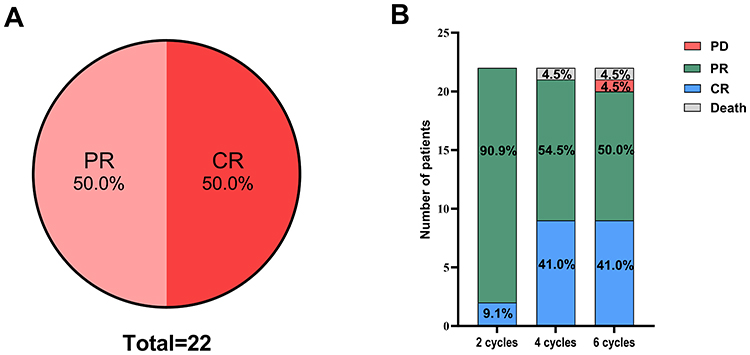 |
Figure 2 Outcomes after induction therapy. (A) The best outcomes during the induction therapy. (B) Outcomes after 2, 4, and 6 cycles of induction therapy. Abbreviations: PR, partial remission; CR, complete remission; PD, progressive disease. |
 |
Figure 3 Swim-lane plots of the corresponding responses. The swim-lane plot shows the treatment responses during the induction and consolidation period of every individual patient enrolled. Abbreviations: PR, partial remission; CR, complete remission; PD, progressive disease; SD, stable disease; ASCT, autologous hematopoietic stem cell transplantation; WBRT, whole-brain radiotherapy. |
The median PFS for all 22 patient was not reached (range: 2.3–no upper limit). The 1-year PFS rate was 66.6% (95% CI, 56.2–77.0%) and the 2-year PFS rate was 59.2% (95% CI, 47.6–70.8%). The median OS was not reached until the last follow-up (16/22 subjects alive). The 1-year OS rate was 81.8% (95% CI, 72.5–89.7%), and the 2-year OS rate was 66.3% (95% CI, 54.6–78.0%) (Figure 4A). The median PFS for the evaluable population was not reached (range: 3.7–no upper limit). The 1-year PFS rate was 66.2% (95% CI, 54.8–77.6%), and the 2-year PFS rate was 58% (95% CI, 45.4–70.6%). The median OS was not reached until the last follow-up (14/19 subjects alive). The 1-year OS rate was 83.2% (95% CI, 74.3–92.1%), and the 2-year OS rate was 66.6% (95% CI, 53.9–79.3%) (Figure S2). At the last follow-up, 3 patients (60%) in the ASCT group, 3 patients (75%) in the WBRT group, and 5 patients (83.3%) in the orelabrutinib group remained progression-free. All the patients with progressed disease died except for one patient (#12) in the ASCT group, who were still alive on the last follow-up at 18.7 months. The 2-year PFS rate was 53.3% (95% CI, 28.5–78.1%) in the ASCT group, 85.7% (95% CI, 72.5–98.9%) in the orelabrutinib, and 92.9% (95% CI, 86.0–99.8%) in the WBRT group (Figure 4B). The 2-year OS rate was 80% (95% CI, 62.1–97.9%) in the ASCT group, and 87.5% (95% CI, 75.8–99.2%) in the orelabrutinib/WBRT group (Figure 4C). The median duration of response (DOR) was 17.9 months in all patients (range: 2.3–42.4), 24.4 months (range: 17.7–42.4) in the orelabrutinib group, 16.5 months (range: 4–42.3) in the ASCT group, 10.5 months (range: 10.3–38.9) in the WBRT group, and 6 months (range: 5.8–31.9) in those who finished 6 cycles of induction therapy without further consolidation. No significant differences were observed among the consolidation groups in PFS, OS, or DOR.
 |
Figure 4 Kaplan–Meier survival curves. (A) The progression-free survival (PFS) and overall survival (OS) curves of the entire cohort. The PFS (B) and OS (C) curves stratified by consolidation therapies of autologous hematopoietic stem cell transplantation (ASCT), whole-brain radiotherapy (WBRT), or orelabrutinib. |
Causes of Death
Among the 6 recorded deaths in the study, the primary causes were disease progression (n = 4) and infection (n = 2). Specifically, patient #7 and #18 died from progressive lymphoma, #8 from PD after receiving further chemotherapies, and #9 from relapse after discontinuing orelabrutinib maintenance. The 2 infection-related deaths included patient #11 (sepsis after ASCT) and #20 (grade 4 pneumonia during induction).
Assessment of Potential Selection Bias
A total of 48 patients were screened for this study. To assess potential selection bias, we compared the baseline characteristics of the 22 enrolled patients with the 24 patients who were excluded due to the simultaneous administration of lenalidomide (a non-protocol therapy). The two groups were comparable in terms of median age (59.5 vs 61 years, P = 0.45), sex distribution (50% vs 54% female, P = 0.78), and median KPS score (80 vs 75, P = 0.12), suggesting that the enrolled cohort was broadly representative of the screened population.
Safety and Adverse Events
Most of the adverse events observed were tolerable and resolved after interventions. There was no treatment discontinuation because of adverse events with OR+MTX induction therapies. One patient with grade 3 renal dysfunction reduced the dosage of HD-MTX to 2 g/m2 after the first cycle of induction. Orelabrutinib was given on a median of 19 days (range, 17–21) per cycle. One patient developed grade 4 neutropenia accompanied by grade 3 pneumonia and recovered after anti-infection and supporting therapies. Another patient, who achieved a PR after two cycles of induction therapy, died from infection including grade 4 pneumonia. Other grade 3 adverse events included neutropenia (9.1%), febrile neutropenia (4.5%), hyperlipidemia (4.5%), liver dysfunction (4.5%), and renal dysfunction (4.5%). Five patients had grade 2 thrombocytopenia (22.7%), and other grade 2 adverse effects include neutropenia (4.5%), liver dysfunction (4.5%), renal dysfunction (9.1%), hypoproteinemia (4.5%), pneumonia (4.5%), and nausea (9.1%). The common grade 1 adverse events were anemia (45.5%), hypokalemia (22.7%), pneumonia (22.7%), thrombocytopenia (18.2%), and nausea (18.2%) (Table 3). No fungal infections were observed. Neutropenia and pneumonia were consistent with the reported common adverse effects of BTK inhibitors, including orelabrutinib, and may reflect its immunomodulatory profile.23 However, causality cannot be definitively established due to combination therapy with HD-MTX and rituximab.
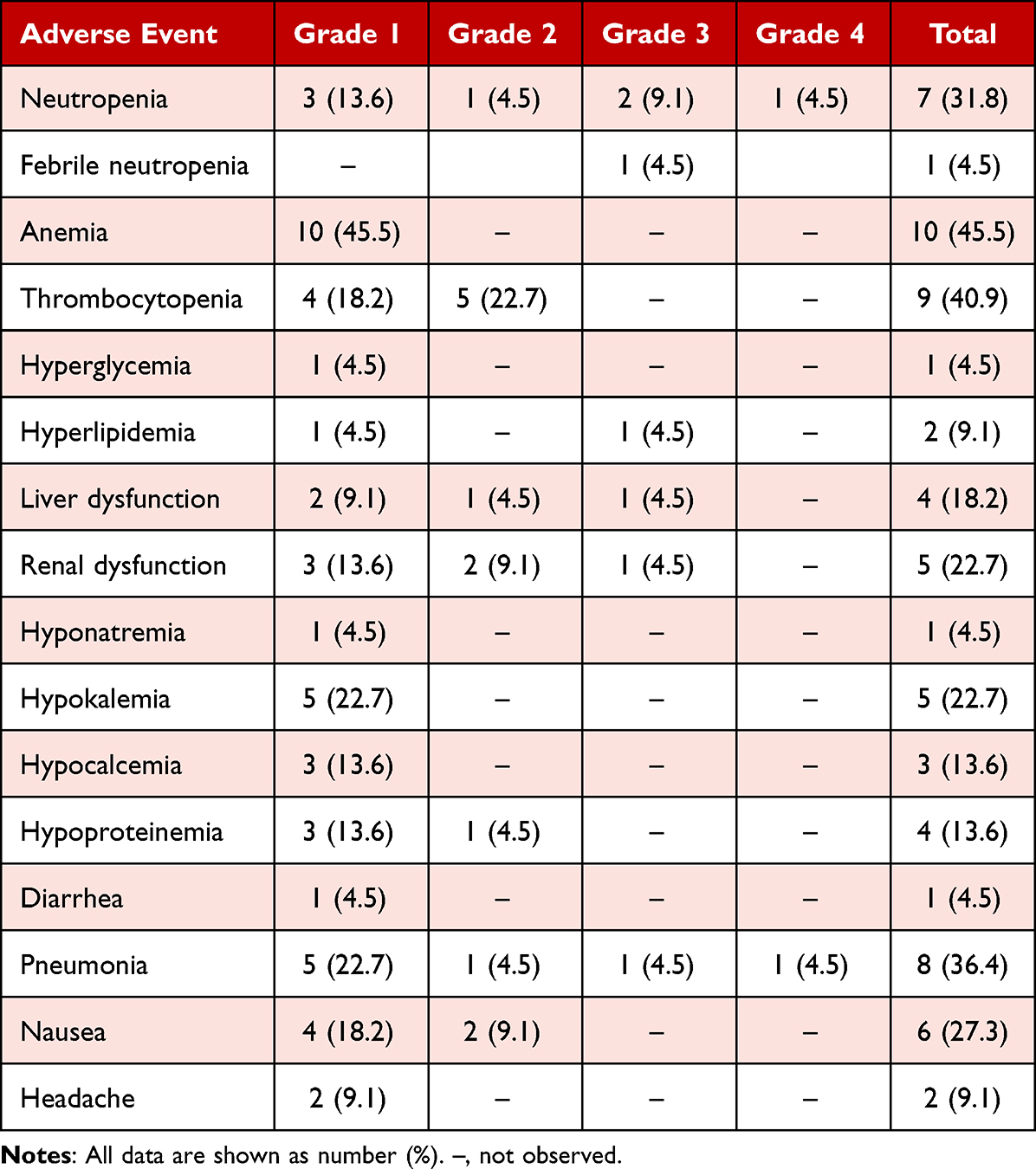 |
Table 3 Adverse Events |
Discussion
The incidence of PCNSL has steadily increased, particularly in elderly patients.12 The rarity of the disease, the highly aggressive biological behavior, the physical barrier in the CNS system, and the overall vulnerability of the patients diagnosed all collectively present substantial challenges in the management of PCNSL.24 Although initially responsive to first-line chemotherapy and radiotherapy, approximately 50% of patients experience relapse or develop refractory disease within 1 year, when the median OS is reduced to 8.4 months despite salvage interventions.24,25
The BTK inhibitor, ibrutinib, which target the BCR pathway, has demonstrated promising effects in combination regimens for relapsed/refractory (r/r) PCNSL in several clinical studies.26–28 Nevertheless, as a first generation of BTK inhibitor, ibrutinib exhibits off-target inhibition on multiple kinases, leading to nonnegligible adverse effects in clinical applications, especially atrial fibrillation.29 In contrast, orelabrutinib, a second-generation irreversible BTK inhibitor, has been approved for the treatment of r/r mantel cell lymphoma and chronic lymphocytic leukemia with high efficacy and more favorable safety profile.29,30 As the cornerstone in the management of PCNSL, HD-MTX often induce rapid initial remission. However, combination therapies are necessary to achieve more durable and profound responses, as outcomes with HD-MTX monotherapy remain suboptimal.31 Rituximab often serves as a backbone agent in the treatment of lymphoma. Emerging evidence suggested that orelabrutinib could enhance the antitumor activity of rituximab in DLBCL, compared to ibrutinib.32
In this prospective phase II trial, we demonstrated that the combination of orelabrutinib, HD-MTX, and rituximab (OR+MTX) is an effective and well-tolerated induction regimen for newly diagnosed PCNSL, achieving an ORR of 91.0% and encouraging survival outcomes with a manageable safety profile. When contextualizing our results within the current therapeutic landscape, it is informative to compare the OR+MTX regimen with established intensive chemotherapy protocols (Table 4). The benchmark MATRix regimen, as established in the IELSG32 trial, yielded a CR rate of 49% and a 2-year OS of 69%.3 While our observed CR rate (41.0%) and 2-year OS (66.3%) appear numerically comparable, such cross-trial comparisons must be interpreted with caution due to differences in study populations and design. MARTA and R-MPV regimens followed with consolidation therapies yield variable efficacies among studies, with CR rates ranging 33.3–81.8% and 2-year OS between 63.6–88%.4–7 The key distinction lies in the toxicity profile. Intensive regimens like MATRix, MARTA, and R-MPV were associated with high rates of grade 3–4 hematologic toxicity, often mandating mandatory G-CSF support and prolonged hospitalization.3–7,33 In contrast, the OR+MTX regimen was associated with a lower incidence of severe hematologic events in our cohort, suggesting a potentially more favorable tolerability that could be particularly advantageous for elderly or less fit patients ineligible for maximal-intensity chemotherapy. Due to the limited sample size, larger cohort studies are warranted for further comparisons of consolation therapies. Nevertheless, orelabrutinib, as an oral regimen, offers a convenient option for prolonged maintenance therapy—especially for elderly or frail patients.
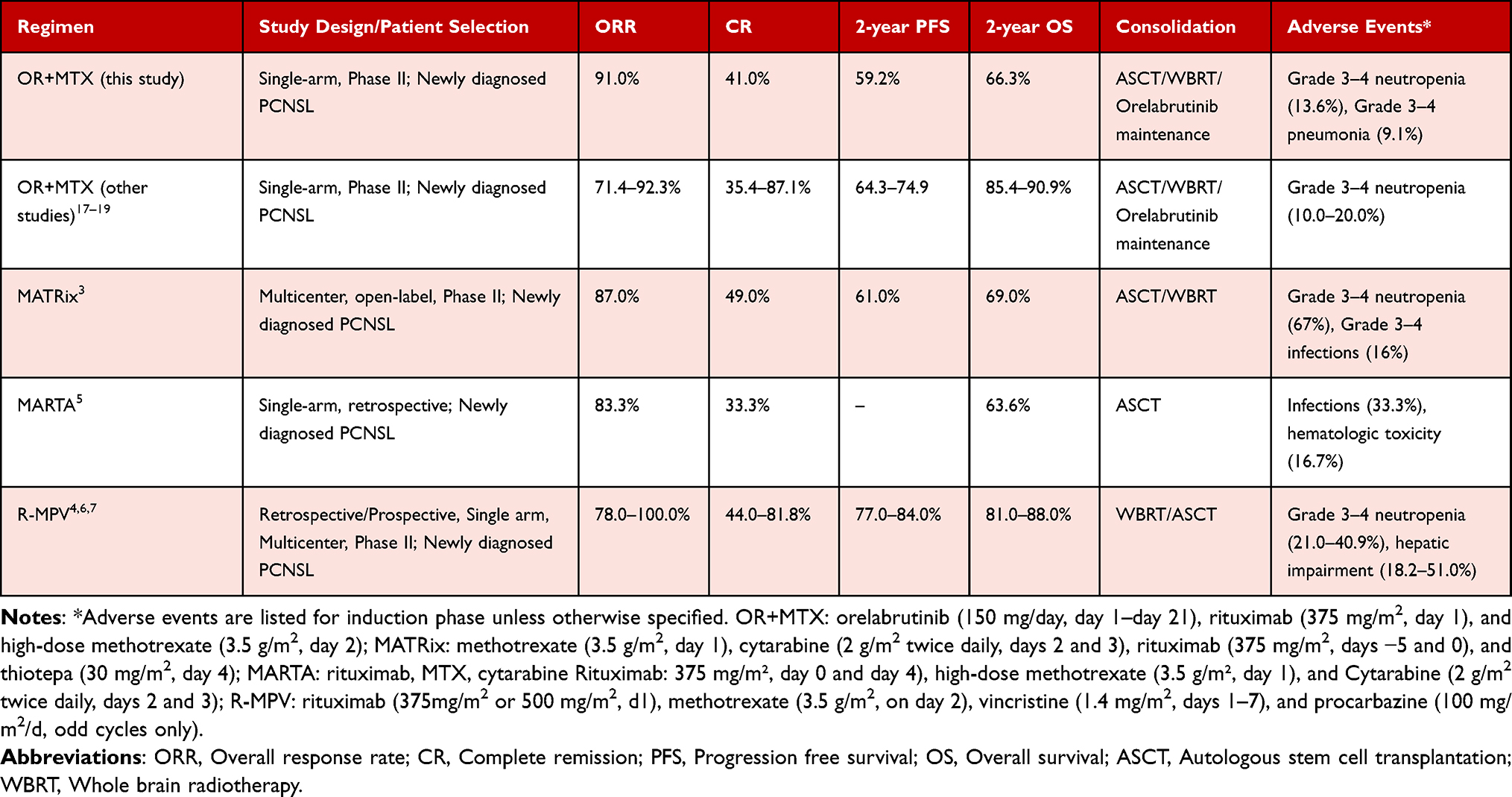 |
Table 4 Summary of Efficacy and Safety Outcomes in Selected First-Line Regimens for Newly Diagnosed PCNSL |
Our findings align with and extend the emerging evidence for orelabrutinib in PCNSL. A retrospective study investigating a combination of rituximab, HD-MTX, temozolomide, orelabrutinib, and lenalidomide in r/r PCNSL patients reported an ORR of 86.7%.34 Another retrospective analysis of orelabrutinib combined with HD-MTX and thiotepa, with or without rituximab, in PCNSL and secondary CNS lymphoma demonstrated an ORR of 92.3%, with the 1-year PFS and OS rates of 60% and 70%, respectively.31 Recent multicenter prospective phase II studies reported promising outcomes of orelabrutinib plus HD-MTX and rituximab in newly diagnosed PCNSL patients, with 2-year PFS rate of 64.3–74.9% and 2-year OS rate of 85.4–90.9% (Table 4), corroborating the potent efficacy of this combination.17–19 Our study adds to these by providing preliminary data on the subsequent application of diverse consolidation strategies. The comparable 2-year PFS rates observed among patients consolidated with ASCT, WBRT, or orelabrutinib maintenance suggest that orelabrutinib may represent a viable, less invasive consolidation option, though this observation is hypothesis-generating due to the non-randomized allocation and small subgroup sizes.
Despite these promising results, BTK inhibitors have certain risks, including an increased susceptibility to neutropenia and pneumonia (≥ Grade 3), as was observed in 13.6% and 9.0% of patients in the present study.23,35 Overall, the regimen was well-tolerated throughout the 6 induction cycles. Only 1 patient, who had achieved a PR after 2 cycles of induction, died of severe pneumonia. The patient’s pneumonia existed before initiation of therapy and exacerbated during treatment. Although no evidence of fungal infection was identified, antifungal therapy with voriconazole was applied.
Several limitations of our study must be acknowledged. First, the single-arm design and small sample size limit the power for robust subgroup analyses and definitive conclusions regarding the comparative efficacy of consolidation therapies. Second, the selection of consolidation therapy was based on patient and physician preference rather than randomization, introducing potential confounding by indication. Third, the median follow-up of 22.3 months is sufficient for early efficacy signals but remains too short to evaluate long-term outcomes and the risk of late relapse. Extended follow-up in larger, randomized trials is needed to assess the durability of response and the efficacy of the induction regimen and subsequent consolidation strategies.
Conclusion
This study provided evidence supporting the combination of orelabrutinib, HD-MTX, and rituximab as a promising and tolerable therapeutic strategy for newly diagnosed PCNSL. Due to the modest sample size and the non-randomized design, we cannot conclude with its superiority or parity to established standards like MATRix and R-MPV. Larger randomized controlled clinical trials are warranted to validate these observations and further optimize the management of PCNSL in clinical practice.
Data Sharing Statement
The individual deidentified participant data used and/or analyzed during the current study are available from the corresponding author Ji Ma (Email: [email protected]) upon reasonable request.
Ethics Statement
The study was approved by the ethics committees of Qilu Hospital of Shandong University, Shandong Cancer Hospital and Institute, and Shengli Oilfield Central Hospital according to the Helsinki Principles. Written informed consent was obtained from all the patients upon enrollment.
Acknowledgment
An unauthorized version of the Chinese MMSE was used by the study team without permission, however this has now been rectified with PAR. The MMSE is a copyrighted instrument and may not be used or reproduced in whole or in part, in any form or language, or by any means without written permission of PAR (www.parinc.com).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the National Natural Science Foundation of China (Grant No. 82170123), the Natural Science Foundation of Shandong Province (ZR2021MH132), and Young Taishan Scholar Foundation of Shandong Province (Grant/Award No. tsqn202312325). China Zhongguancun Precision Medicine Science and Technology Foundation (Grant No. GXZDH48).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Shao L, Xu C, Wu H, et al. Recent progress on primary central nervous system lymphoma-from bench to bedside. Front Oncol. 2021;11:689843. doi:10.3389/fonc.2021.689843
2. Li W. The 5(Th) Edition of the World Health Organization Classification of Hematolymphoid Tumors. Li W, editor. Brisbane (AU): Leukemia; 2022.
3. Ferreri AJ, Cwynarski K, Pulczynski E, et al. Chemoimmunotherapy with methotrexate, cytarabine, thiotepa, and rituximab (MATRix regimen) in patients with primary CNS lymphoma: results of the first randomisation of the International Extranodal Lymphoma Study Group-32 (IELSG32) Phase 2 trial. Lancet Haematol. 2016;3(5):e217–27. doi:10.1016/S2352-3026(16)00036-3
4. Morris PG, Correa DD, Yahalom J, et al. Rituximab, methotrexate, procarbazine, and vincristine followed by consolidation reduced-dose whole-brain radiotherapy and cytarabine in newly diagnosed primary CNS lymphoma: final results and long-term outcome. J Clin Oncol. 2013;31(31):3971–3979. doi:10.1200/JCO.2013.50.4910
5. Sieg N, Naendrup JH, Godel P, et al. Treatment patterns and disease course of previously untreated primary central nervous system lymphoma: feasibility of MTX-based regimens in clinical routine. Eur J Haematol. 2021;107(2):202–210. doi:10.1111/ejh.13639
6. Omuro A, Correa DD, DeAngelis LM, et al. R-MPV followed by high-dose chemotherapy with TBC and autologous stem-cell transplant for newly diagnosed primary CNS lymphoma. Blood. 2015;125(9):1403–1410. doi:10.1182/blood-2014-10-604561
7. Lee JY, Paik JH, Suh KJ, et al. R-MPV followed by high-dose chemotherapy with thiotepa-based and autologous stem cell transplantation for newly diagnosed primary central nervous system lymphoma: a single-center experience. Blood Res. 2021;56(4):285–292. doi:10.5045/br.2021.2021073
8. Scordo M, Wang TP, Ahn KW, et al. Outcomes associated with thiotepa-based conditioning in patients with primary central nervous system lymphoma after autologous hematopoietic cell transplant. JAMA Oncol. 2021;7(7):993–1003. doi:10.1001/jamaoncol.2021.1074
9. Calimeri T, Anzalone N, Cangi MG, et al. Molecular diagnosis of primary CNS lymphoma in 2024 using MYD88(Leu265Pro) and IL-10. Lancet Haematol. 2024;11(7):e540–e549. doi:10.1016/S2352-3026(24)00104-2
10. Zhang Z, Zhang D, Liu Y, et al. Targeting Bruton’s tyrosine kinase for the treatment of B cell associated malignancies and autoimmune diseases: preclinical and clinical developments of small molecule inhibitors. Arch Pharm. 2018;351(7):e1700369. doi:10.1002/ardp.201700369
11. Chalmers SA, Garcia SJ, Webb D, et al. BTK inhibition modulates multiple immune cell populations involved in the pathogenesis of immune mediated nephritis. Clin Immunol. 2021;223:108640. doi:10.1016/j.clim.2020.108640
12. Schaff L, Nayak L, Grommes C. Bruton’s tyrosine kinase (BTK) inhibitors for the treatment of primary central nervous system lymphoma (PCNSL): current progress and latest advances. Leuk Lymphoma. 2024;65(7):882–894. doi:10.1080/10428194.2024.2333985
13. Zhang Y, Li Y, Zhuang Z, et al. Preliminary evaluation of zanubrutinib-containing regimens in DLBCL and the cerebrospinal fluid distribution of zanubrutinib: a 13-case series. Front Oncol. 2021;11:760405. doi:10.3389/fonc.2021.760405
14. Yonezawa H, Narita Y, Nagane M, et al. Three-year follow-up analysis of Phase 1/2 study on tirabrutinib in patients with relapsed or refractory primary central nervous system lymphoma. Neurooncol Adv. 2024;6(1):vdae037. doi:10.1093/noajnl/vdae037
15. Shen J, Liu J. Bruton’s tyrosine kinase inhibitors in the treatment of primary central nervous system lymphoma: a mini-review. Front Oncol. 2022;12:1034668. doi:10.3389/fonc.2022.1034668
16. Wu JJ, Wang WH, Dong M, et al. Orelabrutinib-bruton tyrosine kinase inhibitor-based regimens in the treatment of central nervous system lymphoma: a retrospective study. Invest New Drugs. 2022;40(3):650–659. doi:10.1007/s10637-022-01219-5
17. Sheng L, Liu H, Zhang X, et al. Prospective phase II trial of first-line rituximab, methotrexate, and orelabrutinib (R-MO) in primary central nervous system lymphoma. Blood Cancer J. 2025;15(1):81. doi:10.1038/s41408-025-01278-w
18. Xiao XB, Weng YQ, Jiang HW, et al. Orelabrutinib combined with rituximab and high-dose methotrexate as induction therapy in newly diagnosed primary central nervous system lymphoma. Invest New Drugs. 2025;43(3):679–686. doi:10.1007/s10637-025-01548-1
19. Zhao SH, Zhu ZM, Yang T, et al. Rituximab, high-dose methotrexate plus orelabrutinib as induction therapy in newly diagnosed primary central nervous system lymphoma. Leukemia. 2025;39(8):2035–2038. doi:10.1038/s41375-025-02658-8
20. Abrey LE, Batchelor TT, Ferreri AJ, et al. Report of an international workshop to standardize baseline evaluation and response criteria for primary CNS lymphoma. J Clin Oncol. 2005;23(22):5034–5043. doi:10.1200/JCO.2005.13.524
21. Cheson BD, Pfistner B, Juweid ME, et al. Revised response criteria for malignant lymphoma. J Clin Oncol. 2007;25(5):579–586. doi:10.1200/JCO.2006.09.2403
22. Kansara R, Shenkier TN, Connors JM, et al. Rituximab with high-dose methotrexate in primary central nervous system lymphoma. Am J Hematol. 2015;90(12):1149–1154. doi:10.1002/ajh.24204
23. Deng LJ, Zhou KS, Liu LH, et al. Orelabrutinib for the treatment of relapsed or refractory MCL: a phase 1/2, open-label, multicenter, single-arm study. Blood Adv. 2023;7(16):4349–4357. doi:10.1182/bloodadvances.2022009168
24. Langner-Lemercier S, Houillier C, Soussain C, et al. Primary CNS lymphoma at first relapse/progression: characteristics, management, and outcome of 256 patients from the French LOC network. Neuro Oncol. 2016;18(9):1297–1303. doi:10.1093/neuonc/now033
25. Grommes C, Rubenstein JL, DeAngelis LM, Ferreri AJM, Batchelor TT. Comprehensive approach to diagnosis and treatment of newly diagnosed primary CNS lymphoma. Neuro Oncol. 2019;21(3):296–305. doi:10.1093/neuonc/noy192
26. Grommes C, Tang SS, Wolfe J, et al. Phase 1b trial of an ibrutinib-based combination therapy in recurrent/refractory CNS lymphoma. Blood. 2019;133(5):436–445. doi:10.1182/blood-2018-09-875732
27. Lionakis MS, Dunleavy K, Roschewski M, et al. Inhibition of B cell receptor signaling by ibrutinib in primary CNS lymphoma. Cancer Cell. 2017;31(6):833–843e5. doi:10.1016/j.ccell.2017.04.012
28. Grommes C, Pastore A, Palaskas N, et al. Ibrutinib unmasks critical role of bruton tyrosine kinase in primary CNS lymphoma. Cancer Discov. 2017;7(9):1018–1029. doi:10.1158/2159-8290.CD-17-0613
29. Shirley M. Bruton tyrosine kinase inhibitors in B-cell malignancies: their use and differential features. Target Oncol. 2022;17(1):69–84. doi:10.1007/s11523-021-00857-8
30. Dhillon S. Orelabrutinib: first approval. Drugs. 2021;81(4):503–507. doi:10.1007/s40265-021-01482-5
31. Holdhoff M, Ambady P, Abdelaziz A, et al. High-dose methotrexate with or without rituximab in newly diagnosed primary CNS lymphoma. Neurology. 2014;83(3):235–239. doi:10.1212/WNL.0000000000000593
32. Yu H, Wang X, Li J, et al. Addition of BTK inhibitor orelabrutinib to rituximab improved anti-tumor effects in B cell lymphoma. Mol Ther Oncolytics. 2021;21:158–170. doi:10.1016/j.omto.2021.03.015
33. Freeman T, Legasto CS, Schickli MA, et al. High-dose methotrexate-based regimens with or without vincristine for the treatment of primary central nervous system lymphoma. Neurooncol Adv. 2020;2(1):vdaa077. doi:10.1093/noajnl/vdaa077
34. Yang C, Cui Y, Ren X, et al. Orelabrutinib combined with lenalidomide and immunochemotherapy for relapsed/refractory primary central nervous system lymphoma: a retrospective analysis of case series. Front Oncol. 2022;12:901797. doi:10.3389/fonc.2022.901797
35. Lipsky A, Lamanna N. Managing toxicities of Bruton tyrosine kinase inhibitors. Hematology Am Soc Hematol Educ Program. 2020;2020(1):336–345. doi:10.1182/hematology.2020000118
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.