Back to Journals » ImmunoTargets and Therapy » Volume 6
Phase I clinical trial of sipuleucel-T combined with escalating doses of ipilimumab in progressive metastatic castrate-resistant prostate cancer
Authors Scholz M, Yep S, Chancey M, Kelly C, Chau K, Turner J, Lam R ![]() , Drake CG
, Drake CG
Received 16 September 2016
Accepted for publication 30 November 2016
Published 20 March 2017 Volume 2017:6 Pages 11—16
DOI https://doi.org/10.2147/ITT.S122497
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Michael Shurin
Video abstract presented by Mark Scholz.
Views: 125
Mark Scholz,1 Sabrina Yep,1 Micah Chancey,1 Colleen Kelly,1 Ken Chau,1 Jeffrey Turner,1 Richard Lam,1 Charles G Drake,2,3
1Prostate Oncology Specialists, Inc., Marina del Rey, CA, 2The Sidney Kimmel Cancer Center, 3The James Buchanan Brady Urological Institute, John Hopkins Medical Institutions, Baltimore, MD, USA
Background: Sipuleucel-T (SIP-T), which functions by stimulating cancer-specific dendritic cells, prolongs survival in men with prostate cancer. Ipilimumab (IPI) achieved a borderline survival advantage in a large randomized trial. SIP-T and IPI are potentially synergistic.
Patients and Methods: Nine men with progressive metastatic castrate-resistant prostate cancer (mCRPC) were treated prospectively with SIP-T followed immediately by IPI with one of the following doses of IPI: 1 mg/kg at 1 week after SIP-T; 1 mg/kg at 1 and 4 weeks after SIP-T; or 1 mg/kg at 1, 4, and 7 weeks after SIP-T. Three patients were evaluated at each level. Cancer-specific immunoglobulins directed at granulocyte-macrophage-colony-stimulating factor/prostatic acid phosphatase (PAP) fusion protein (PA2024) and PAP were measured prior to SIP-T, after SIP-T, 1 week after IPI, every other month for 5 months, then every 3 months for an additional 12 months.
Results: Adverse events of SIP-T were consistent with previous reports. IPI only caused a transient grade 1 rash in one patient. Median age, Gleason score, and number of previous hormonal interventions were 77 years, 8, and 3, respectively. Eight men had bone metastases and one had lymph node metastasis. Statistically significant increases in serum immunoglobulin G (IgG) and IgG-IgM specific for PA2024 and PAP occurred after SIP-T. An additional statistically significant increase in the aforementioned immunoglobulins – above the levels achieved by SIP-T – occurred after IPI. Median clinical follow-up was 36 months (range: 26–40). Three patients died from progressive disease after 9, 18, and 20 months. Out of the remaining six patients, five of them needed further treatment that included abiraterone acetate, enzalutamide, radium-223 dichloride, and spot radiation. One patient had an undetectable PSA, who did not receive any other treatment except spot radiation. Median PSA at last follow-up for the surviving patients was 3.8 (range: 0.6–7.47).
Conclusion: In this small trial, the addition of IPI to SIP-T was well tolerated. IPI increased immunoglobulins specific for the PA2024 protein and PAP above the level achieved with SIP-T alone.
Keywords: sipuleucel-T, ipilimumab, prostate cancer, immune therapy
Introduction
The number of new therapies for castrate-resistant prostate cancer (CRPC) is increasing. In the past 5 years sipuleucel-T (SIP-T), cabazitaxel, enzalutamide, abiraterone, and radium-223 have been United States Food and Drug Administration (US FDA)-approved for prolonging survival. Some of these agents have also demonstrated an improvement in quality of life. Minimizing treatment-related side effects in this elderly, testosterone-deprived population is important. In the enzalutamide trial, for example, a meaningful 17-month delay in the time to the initiation of chemotherapy was achieved.1
With all these new, clinically active agents, research is now being focused on methods for maximizing efficacy through combination therapy and gene sequencing. The publication of CHAARTED results also draws attention to the benefit of leveraging existing therapies by starting treatment at earlier stage of the disease’s natural history.2,3
Cytotoxic T-lymphocyte antigen-4 (CTLA-4) is a negative regulator of T-cell activation; ipilimumab (IPI) specifically blocks CTLA-4, thus enhancing T-cell activation. Based on this mechanism of action, we and others have hypothesized that IPI synergizes with SIP-T. In 2013, Prostate Oncology Specialists, a private medical oncology practicing center that specializes in prostate cancer, initiated a Phase I trial combining SIP-T with mini-dose IPI (SIPIPI). Nine patients were accrued, and preliminary results have previously been reported in abstract form.4 This study reports the impact of SIPIPI on immunoglobulin levels at baseline, after SIP-T, and after IPI administration. We also report the intermediate-term clinical outcome in terms of toxicity as well as PSA kinetics.
Patients and methods
Patients and inclusion criteria
Patients with confirmed metastatic adenocarcinoma of the prostate and castrate levels of testosterone with sequentially rising PSA levels were eligible for this study. The eligible patients had to meet the following criteria for inclusion: adequate renal, hepatic, and bone marrow function (defined as a creatinine <2× the upper limit of normal, total bilirubin and serum aspartate aminotransferase <2× the upper limit of normal, white blood cells (WBC) ≥2500/µL, an absolute neutrophil count of ≥1000, and a platelet count >100,000). All patients signed an institutional review board (IRB) approved informed consent. Patients with prior immune therapy; patients simultaneously undergoing treatment with any chemotherapy or hormonal therapy besides luteinizing hormone-releasing hormone (LHRH) agonist; patients with any history of autoimmune diseases; patients with clinically significant cardiac or pulmonary disease, uncontrolled infection, diseases of the central nervous system, active secondary malignancy, HIV, hepatitis, or those currently receiving corticosteroids were excluded from this study. This study was approved by Aspire IRB. The Clinical Trial Identifier for this study is NCT01832870.
Treatment
Treatment was administered on an outpatient basis. On weeks 0, 2, and 4, commercially available SIP-T was infused. Patients received a minimum of 50 million autologous CD54+ cells activated with PA2024. All patients received a total of three doses of SIP-T. Patients were pre-medicated with 650 mg acetaminophen and 50 mg diphenhydramine orally. Subsequently, 1 mg/kg IPI was infused over 90 minutes starting 1 week after the last dose of SIP-T. The first three participants had a single infusion of IPI. Three additional participants received two doses of 1 mg/kg IPI at 1 and 4 weeks after the last dose of SIP-T. Three more additional participants received 1 mg/kg IPI at 1, 4, and 7 weeks after the last dose of SIP-T (Figure 1). After completion of SIPIPI, all patients were treated as per the standard of care for men with metastatic progressive CRPC.
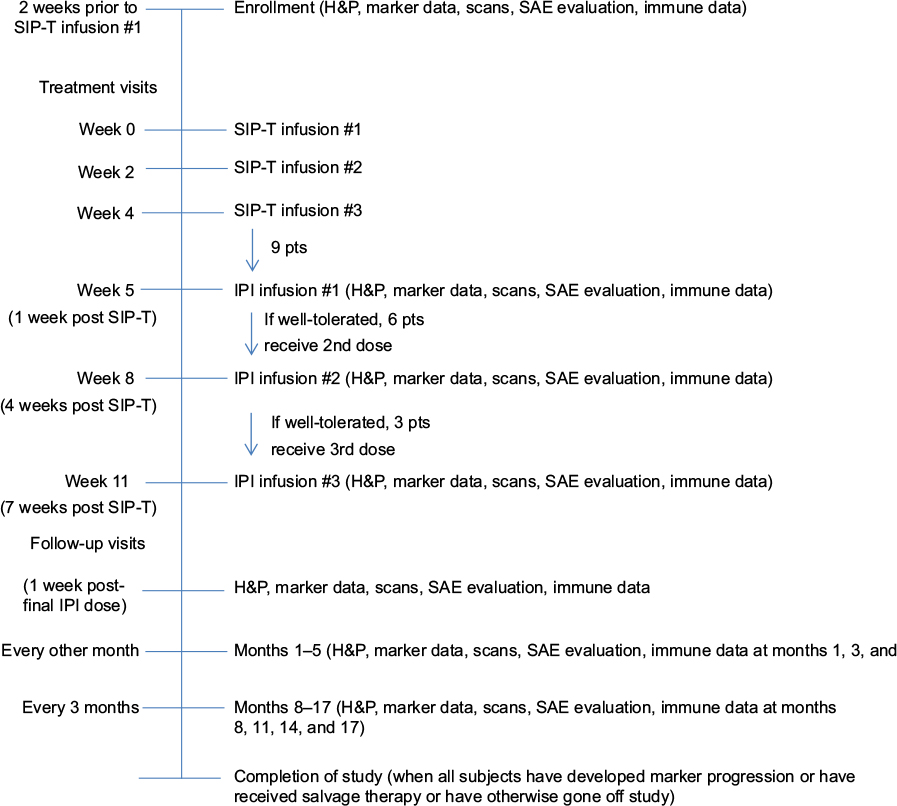 | Figure 1 Study schematic time schedule. Abbreviations: IPI, ipilimumab; SAE, serious adverse event; SIP-T, sipuleucel-T; F/U, follow up; pts, patients; H&P, history and physical |
Immune correlates
Immunoglobulin G (IgG) and IgG-IgM immunoglobulins directed toward PA2024 or to prostatic acid phosphatase (PAP) were measured prior to SIP-T, after SIP-T, 1 week after IPI, every other month for 5 months, then every 3 months for an additional 12 months (Figure 2).
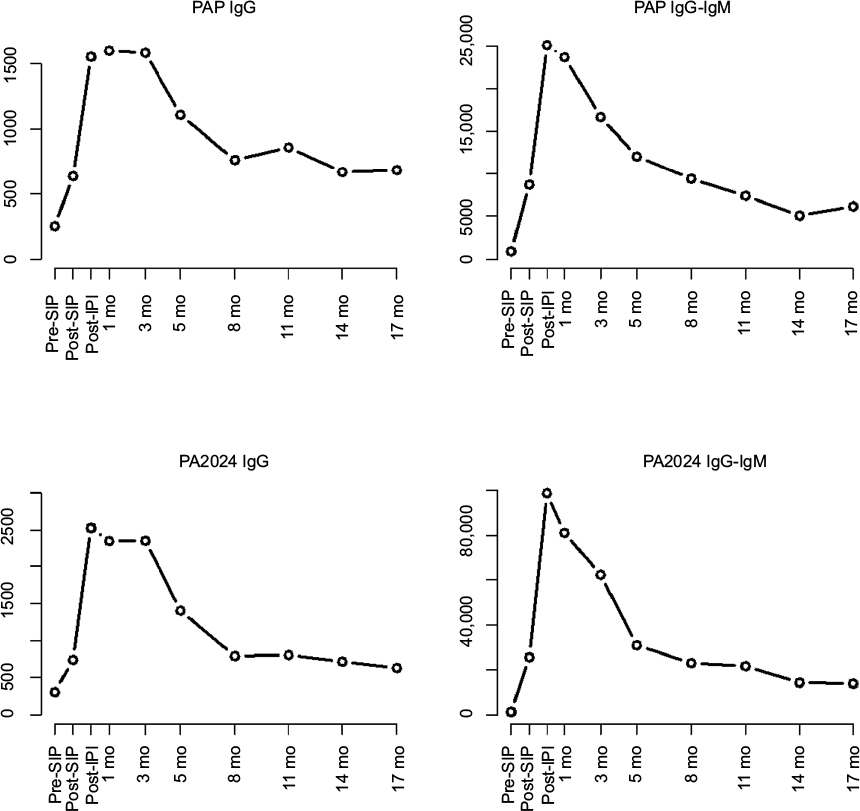 | Figure 2 Immunoglobulin titers at pre-SIP, post-SIP, and post-IPI. Abbreviations: IgG, immunoglobulin G; IPI, ipilimumab; mo, months; PAP, prostatic acid phosphatase; SIP, sipuleucel. |
Clinical monitoring
Clinically stable patients had medical office visits supervised by an MD in accordance with the aforementioned treatment and blood monitoring schedule. Subsequent to completion of all the scheduled immune testing, stable patients were followed up every 3 months. All visits included a standard medical history and physical evaluation as well as analysis of hepatic panel, complete blood count, renal panel, and PSA. Computed tomography and bone scans were performed every 6 months or more frequently if clinically indicated. No patient was lost during the follow-up period.
Study duration
Treatment was initiated on April 2013 for patient #1 and on April 2014 for patient #9. The last clinical analysis of the surviving patients was performed in September 2016.
Statistical methodology
IgG and IgG-IgM titers were log-transformed and then analyzed in a mixed-effects repeated-measures linear model. Time was treated as a categorical variable. Effects of time and dosage and the interaction of time and dosage were included in the model. The repeated-measures design included an auto-regressive correlation structure (AR(1)). Presumably due to the small number of samples in each dosage group, there were no statistically significant differences between the three doses overall (main effect of dosage: p-value >0.05; interaction of time and dosage: p-value >0.05) or at any time point (all p-values >0.05) for any of the four immune responses. In three of the four analyzed immune responses, however, the titers were greatest for three doses, somewhat smaller for two doses and the smallest for a single dose. All three dosage levels were, therefore, combined to compare mean titers at different time points. In the combined data set (n = 9 patients), main effects of time were included in the model. The repeated-measures design included a first-order AR(1). Missing data were imputed with a missing-completely-at-random assumption.
Results
Patients
All nine patients had metastatic CRPC (mCRPC) with a rising PSA. Median age was 77 years. Median baseline PSA and Gleason score were 1.7 and 8, respectively. The median number of previous hormonal interventions was 3. Three patients underwent previous local radiation therapy and four patients underwent surgery plus radiation therapy. Two patients did not undergo previous radiation therapy or surgery. Eight patients had bone metastases, and one patient had metastases limited to lymph nodes. One patient underwent previous treatment with docetaxel in the adjuvant setting, and three had previously received abiraterone acetate (Table 1).
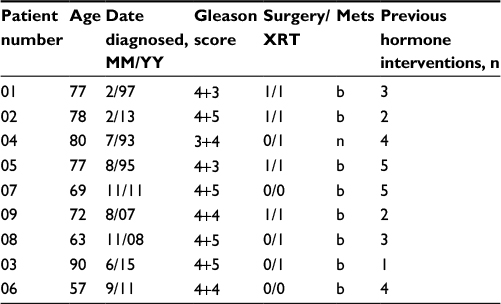 | Table 1 Patient characteristics Abbreviations: XRT, radiation therapy; Mets, metastases. |
Safety and tolerability
All patients received full amounts of the scheduled doses of SIP-T and IPI. There were no unexpected toxicities from SIP-T. IPI caused a transient grade 1 rash in one patient. The rash resolved without treatment. This patient was accrued to the trial at the lowest dose level of IPI and therefore only received one dose of IPI.
Correlative immune studies
The mean PAP IgG titer increased significantly (p-value <0.001) from baseline to post-SIP-T from 252 to 636, a relative increase of 253% (Figure 2). The mean PAP IgG titer also increased significantly (p-value <0.001) from post-SIP-T to post-IPI from 636 to 1554, a relative increase of 244%. The mean PAP IgG titer reached a maximum of 1600 at month 1 post-IPI follow up, a relative increase of 252% over post-SIP-T. The mean PAP IgG titer at month 3 remained high with a mean of 1584, a relative increase of 249% over post-SIP-T. At no time point did the mean titer decrease significantly from the apex at 1 month (all p-values >0.05).
The mean PAP IgG-IgM titer increased significantly (p-value <0.0001) from baseline to post-SIP-T from 920 to 8709, a relative increase of 947%. The mean PAP IgG-IgM titer also increased significantly (p-value = 0.002) from post-SIP-T to post-IPI from 8709 to 25,117, a relative increase of 288% (Figure 2). The mean PAP IgG-IgM titer reached a maximum of 25,117 post-IPI. The mean PAP IgG-IgM titer at month 1 remained high with a mean of 23,702, a relative increase of 272% over post-SIP-T. At 11 months, the mean titer decreased significantly from the maximum post-IPI (and was less than the post-SIP-T mean); months 14 and 17 also had significantly lower titers than the apex.
The mean PA2024 IgG titer increased significantly (p-value = 0.0001) from baseline to post-SIP-T from 307 to 741, a relative increase of 241%. The mean PA2024 IgG titer also increased significantly (p-value <0.0001) from post-SIP-T to post-IPI from 741 to 2528, a relative increase of 341% (Figure 2). The mean PA2024 IgG titer reached a maximum at post-IPI. The mean PA2024 IgG titer at month 1 remained high with a mean of 2352, a relative increase of 317% over post-SIP-T. At month 8, the mean titer decreased significantly from the maximum at post-IPI and remained significantly lower at months 11–17 (p-value <0.05).
The mean PA2024 IgG-IgM titer increased significantly (p-value <0.0001) from baseline to post-SIP-T from 1317 to 25,600, a relative increase of 1943%. The mean PA2024 IgG-IgM titer also increased significantly (p-value = 0.001) from post-SIP-T to post-IPI from 25,600 to 98,944, a relative increase of 386% (Figure 2). The mean PA2024 IgG-IgM titer reached a maximum at post-IPI. The mean PA2024 IgG-IgM titer at month 1 remained high with a mean of 81,275, a relative increase of 317% over post-SIP-T. At month 5, the mean titer decreased significantly from the maximum at post-IPI and remained significantly lower at months 8–17 (p-value <0.05).
Clinical outcomes
Three patients died of progressive disease after 9, 18, and 20 months, respectively. Two of those underwent aggressive treatment with chemotherapy, radium 223, palliative radiation, and secondary hormonal maneuvers. The third patient refused subsequent therapy and expired after 9 months. Baseline PSA levels in the three patients who expired were 2.2, 66, and 81, respectively; median baseline PSA for the group as a whole was 1.7 (Table 1). Six patients remain alive, with a median post-treatment follow-up of 36 months. Post-study treatments were typical of those used in men with mCRPC (Table 2). Individual patient data are summarized in Table 2.
 | Table 2 Experimental and subsequent treatment outcome Note: Dates are represented in the format “month/year”. Abbreviations: IPI, ipilimumab; SIPIPI, sipuleucel-T with mini-dose ipilimumab; Rx, treatment; SIR, selective internal radiation; Tax, Taxotere; Carb, Carboplatin; Jev, Jevtana; Xel, Xeloda; XRT, radiation therapy |
Discussion
SIP-T is a US FDA-approved treatment that prolongs survival in men with mCRPC.5 This autologous cellular vaccine utilizes antigen-presenting cells activated by ex vivo exposure to a recombinant PAP granulocyte-macrophage-colony-stimulating factor fusion protein (PA2024). We hypothesized that low doses (1 mg/kg) of anti-CTLA-4 would be well tolerated post-SIP-T and would result in an augmented immune response to the vaccine. This was indeed the case; up to three doses of IPI at 1 mg/kg were not associated with significant adverse events. The discrepancy between this and published Phase I6 and Phase III data7 on IPI in prostate cancer likely reflect the higher doses used in prior studies. It has been reported that men receiving SIP-T who develop augmented immunoglobulin levels to PA2024 and PAP have improved survival.8 Studies of the pattern of rise in immunoglobulin levels after SIP-T show a maximal increase 2 weeks after the third infusion of SIP-T, which was continuously maintained without any further augmentation.9 A similar pattern of maximal immunoglobulin rise soon after the third dose of SIP-T without any further subsequent increase was also observed in the STAND trial.10 This pattern of maximal immunoglobulin increase after three cycles of SIP-T has been consistent in all the reported trials. In our study, the pattern of an additional statistically significant increase in immunoglobulin levels after mini-dose IPI indicates that there are additive or synergistic effects between SIP-T and IPI.
Serum immunoglobulin levels declined to the post-SIP-T/pre-IPI level 5–14 months after the completion of SIPIPI. The significant augmentation of immunoglobulin levels seen after IPI in conjunction with their subsequent decline to baseline after a median of 8 months suggests the possibility that periodic redosing with low-dose IPI might maintain higher immunoglobulin levels and possibly further augment the anticancer effects of the SIPIPI combination. The fact that there was a statistically nonsignificant trend toward higher immunoglobulin levels with two or three doses of IPI (compared to one dose of IPI) also provides some evidence that an even more prolonged increase in immunoglobulin levels might occur with higher or repeated doses of IPI.
Firm conclusions about the clinical efficacy of SIPIPI in such a small series such as ours are difficult to derive. Retrospective analysis showed a potentially greater benefit of SIP-T in men with lower baseline PSA values.11 Applying this principle to our data, it is noteworthy that the median baseline PSA prior to SIPIPI of the three men who expired was 66, whereas for the six other surviving men, the median baseline PSA was 1.7. The potential dichotomy between these two groups, from a survival perspective, is even more sharply defined as the median PSA of the surviving participants at last follow-up remained low at 3.8.
Conclusion
In summary, SIPIPI was well tolerated and resulted in cancer-specific immunoglobulin titers that increased above the pretreatment baseline with SIP-T and were further elevated after the administration of IPI. Over the ensuing 12 months of measurements, these elevated levels were maintained and then began to decline after 5–11 months. At the last clinical follow-up, 36 months after completing treatment, the six surviving patients had a median PSA of 3.8. These data support ongoing trials of SIPIPI in mCRPC with larger patient numbers, albeit with higher doses of IPI.
Acknowledgment
This trial was funded by Dendreon.
Disclosure
Mark Scholz received direct support from Dendreon for conducting this trial. He is a paid consultant of Dendreon, as is Charles Drake. Charles Drake has received research funding from Bristol Myers Squibb (BMS). He has received consulting fees from BMS, Merck, Astra Zeneca (AZ), and Medimmune. He has patents licensed to AZ, BMS, and Medimmune. The authors report no other conflicts of interest in this work.
References
Beer TM, Armstrong AJ, Rathkopf DE, et al; PREVAIL Investigators. Enzalutamide in metastatic prostate cancer before chemotherapy. N Engl J Med. 2014;371(5):424–433. | ||
Suzman D, Eisenberger M. Beyond approval: what is the most appropriate way to use the expanding armamentarium in metastatic castration-resistant prostate cancer and how do we move forward? Eur Urol. 2014;66(5):826–828. | ||
Sweeney CJ, Chen YH, Carducci M, et al. Chemohormonal therapy in metastatic hormone-sensitive prostate cancer. N Engl J Med. 2015;373(8):737–746. | ||
Scholz M. Sipuleucel-T in combination with mini-dose ipilimumab for metastatic, castrate-resistant prostate cancer. J Clin Oncol. 2015;33(Suppl):e22104. | ||
Kantoff PW, Higano CS, Shore ND, et al; IMPACT Study Investigators. Sipuleucel-T immunotherapy for castration-resistant prostate cancer. N Engl J Med. 2010;363(5):411–422. | ||
Slovin SF, Higano CS, Hamid O, et al. Ipilimumab alone or in combination with radiotherapy in metastatic castration-resistant prostate cancer: results from an open-label, multicenter phase I/II study. Ann Oncol. 2013;24(7):1813–1821. | ||
Kwon ED, Drake CG, Scher HI, et al; CA184-043 Investigators. Ipilimumab versus placebo after radiotherapy in patients with metastatic castration-resistant prostate cancer that had progressed after docetaxel chemotherapy (CA184-043): a multicentre, randomised, double-blind, phase 3 trial. Lancet Oncol. 2014;15(7):700–712. | ||
Sheikh NA, Petrylak D, Kantoff PW, et al. Sipuleucel-T immune parameters correlate with survival: an analysis of the randomized phase 3 clinical trials in men with castration-resistant prostate cancer. Cancer Immunol Immunother. 2013;62(1):137–147. | ||
Small EJ, Lance RS, Gardner TA, et al. A randomized phase II trial of sipuleucel-T with concurrent versus sequential abiraterone acetate plus prednisone in metastatic castration-resistant prostate cancer. Clin Cancer Res. 2015;21(17):3862–3869. | ||
Antonarakis ES, Kibel AS, Adams GW, et al. Sequencing of Sipuleucel-T and Androgen Deprivation Therapy in Men with Hormone-Sensitive Biochemically-Recurrent Prostate Cancer: A Phase II Randomized Trial. Clin Cancer Res. 2016. | ||
Schelhammer PF, Chodak G, Whitmore JB, Sims R, Frohlich MW, Kantoff PW. Lower baseline prostate-specific antigen is associated with a greater overall survival benefit from sipuleucel-T in the Immunotherapy for Prostate Adenocarcinoma Treatment (IMPACT) trial. Urology. 2013;81(6):1297–1302. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.