Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Pharmacovigilance Study on Adverse Events of Nicotine Replacement Therapy, Bupropion, and Varenicline in Patients with Chronic Obstructive Pulmonary Disease
Authors Wang YD, Wang YT, Chen HH, Bao JK, Chen SM, Chen DX
Received 24 December 2024
Accepted for publication 10 May 2025
Published 15 May 2025 Volume 2025:20 Pages 1509—1524
DOI https://doi.org/10.2147/COPD.S514133
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Richard Russell
Yi Da Wang,1,* Yan Tian Wang,1,* Hao Hui Chen,2,* Jin Ku Bao,1 Shou Ming Chen,3,4 Dong Xu Chen3,4
1Key Laboratory of BioResource and Eco-Environment of Ministry of Education, College of Life Science, Sichuan University, Chengdu, People’s Republic of China; 2West China School of Medicine, Sichuan University, Chengdu, People’s Republic of China; 3Department of Anesthesiology, West China Second University Hospital, Sichuan University, Chengdu, People’s Republic of China; 4Key Laboratory of Birth Deficits and Related Diseases of Women and Children, Sichuan University, Ministry of education, Chengdu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Shou Ming Chen, Department of Anesthesiology, West China Second University Hospital, Sichuan University, Chengdu, People’s Republic of China, Email [email protected] Dong Xu Chen, Department of Anesthesiology, West China Second University Hospital, Sichuan University, Chengdu, People’s Republic of China, Email [email protected]
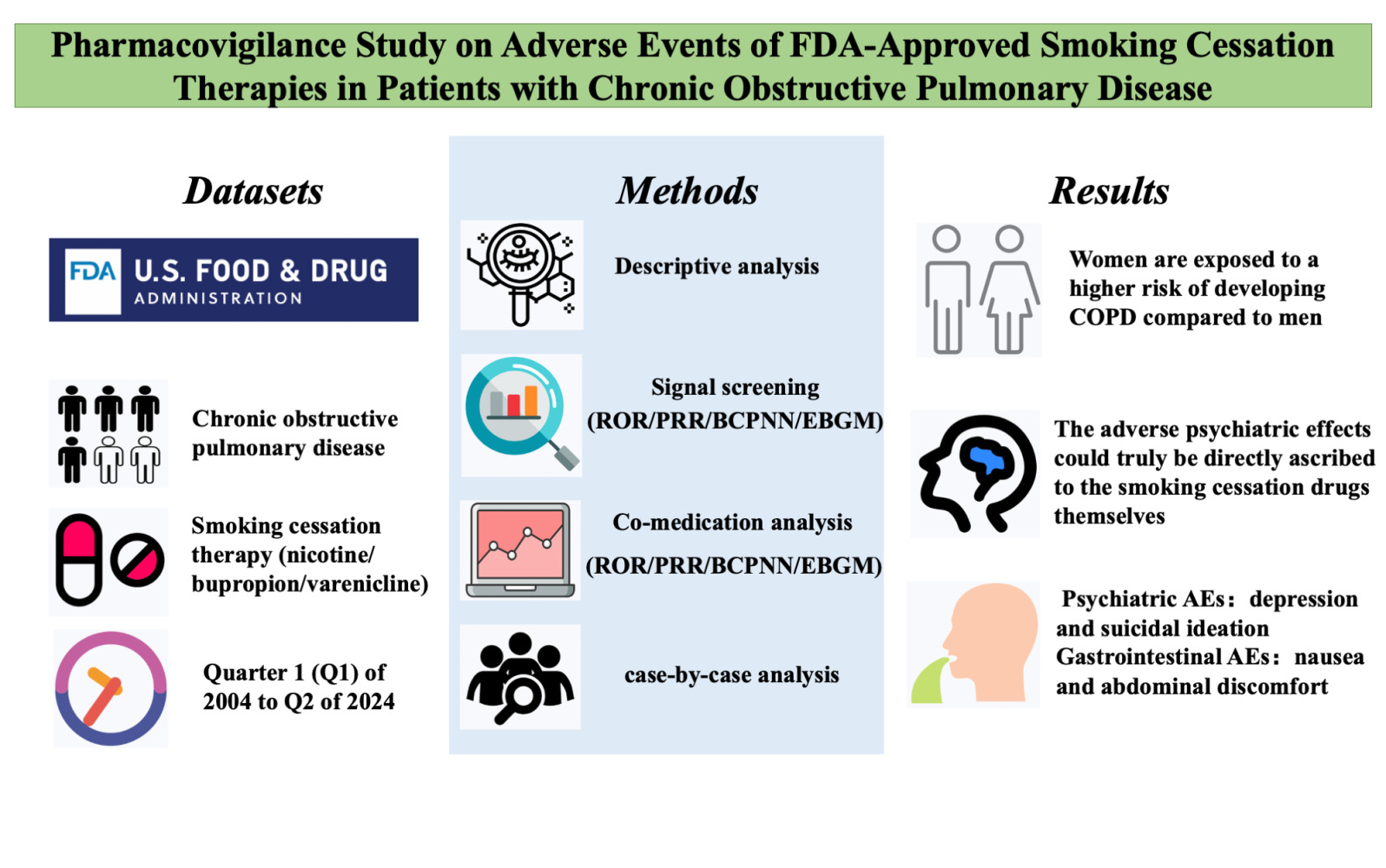
Purpose: Chronic obstructive pulmonary disease (COPD) is one of the most prevalent respiratory disorders, with smoking being a major risk factor. Smoking cessation is therefore crucial in the management of COPD. This study aimed to comprehensively evaluate the safety profiles of common cessation therapies, including nicotine replacement therapy, bupropion, and varenicline.
Patients and Methods: Using the FDA Adverse Event Reporting System (FAERS) database from Q1 2004 to Q2 2024, we analyzed adverse events (AEs) associated with bupropion, nicotine, and varenicline in COPD patients. Disproportionality analysis, case-by-case evaluation, and co-medication analysis were performed to identify positive safety signals.
Results: Eighty-eight positive safety signals were identified, primarily involving psychiatric, nervous system, and gastrointestinal disorders. Notable AEs included depression, nausea, anxiety, abnormal dreams, and insomnia. Critically, eight PTs indicated serious AEs associated with psychiatric disorders that were not present in the labeling but required Important Medical Event (IME) surveillance. Experiencing severe neuropsychiatric symptoms (eg, suicidal thoughts and suicide attempts) was the major reason for limiting the use of these drugs, especially varenicline, for which the FDA issued a black box warning in 2009. Nicotine combined with varenicline showed higher risks for skin reactions and gastrointestinal issues. Most AEs occurred within the first 30 days of therapy, with some persisting beyond a year.
Conclusion: This study highlights significant psychiatric, neurological, and gastrointestinal AEs associated with smoking cessation therapies in patients with COPD. Clinicians are advised to be particularly cautious of these risks, especially when using combination therapies or treating patients with a predisposition to psychiatric disorders.
Keywords: FAERS database, chronic obstructive pulmonary disease, bupropion, varenicline, nicotine
Graphical Abstract:
Introduction
Chronic obstructive pulmonary disease (COPD) is one of the most prevalent respiratory disorders, characterized by chronic airway inflammation, small airway lesions, emphysema, and reduced lung elasticity. These pathological changes ultimately lead to irreversible airflow obstruction and impaired ventilation function.1 COPD is among the leading causes of mortality related to chronic lung diseases, with the World Health Organization predicting that by 2030, COPD will become the third leading cause of death globally.2,3 This escalating health burden demands comprehensive healthcare strategies, particularly in developing evidence-based clinical guidelines for effective disease management.
Tobacco smoking is the primary risk factor for the development and progression of COPD, particularly in individuals with a genetic predisposition to the disease.4 In the United States, the prevalence of current smoking among patients with COPD is significantly higher than in the general adult population without COPD or other chronic illnesses (47.3% vs 20.0%).5 Smoking contributes significantly to COPD mortality, with an age-standardized mortality rate of 68.89 per 100,000 among the general population and 73.74 per 100,000 specifically from COPD-related deaths among men.6 The cessation of smoking is the most effective measure to slow the progression of COPD and reduce mortality, particularly for the approximately 50% of diagnosed patients with COPD who continue to smoke.7 The GOLD guidelines also emphasize smoking cessation as a critical component of COPD management.8 However, despite the long-lasting notion about the substantial contribution of smoking to the severity of COPD, studies have revealed lower quit rates in patients with COPD compared with “healthy” smokers, emphasizing that there may be more obstacles to quitting in patients with COPD.9,10
Pharmacological treatment for smoking cessation is designed to block the reinforcing effects of nicotine and reduce withdrawal symptoms. Treatments for smoking cessation include nicotine replacement therapy, bupropion, and varenicline.11 Nicotine replacement therapies (such as nicotine gum, inhalants, nasal sprays, transdermal patches, sublingual tablets or tablets) maintain relatively low plasma nicotine levels that ease anxiety and withdrawal symptoms by acting directly on the nicotinic cholinergic receptors α4β29. While effective in increasing long-term cessation rates compared to placebo,12 the selection of appropriate delivery forms, dosing schedules, and treatment duration requires careful consideration of individual patient factors. Bupropion, an antidepressant that stimulates noradrenergic and dopaminergic functions, has been shown to double abstinence rates even in the long term. However, the FDA’s black box warning for neuropsychiatric adverse events (AEs) necessitates particular caution in patients with psychiatric comorbidities.13 Varenicline is a partial agonist of nicotinic α4β2 cholinergic receptors, demonstrating 20 times greater affinity for these receptors compared to nicotine. This mechanism of action aids in reducing the risk of relapse in persons who smokes by inducing anhedonia associated with smoking.14 Thus, the clinical application and safety controversies of smoking cessation therapies remains in dispute.
Considering the increasing number of patients with COPD who need to receive pharmacological treatment for smoking cessation and the relatively limited subject pool in pre-marketing research, it is necessary to assess the safety profile of these drugs during the post-marketing period. The complex interplay between these medications and COPD-related pathophysiology, combined with the presence of multiple comorbidities in this patient population, creates unique challenges in medication safety management. These challenges can significantly impact treatment adherence, therapeutic outcomes, and overall quality of life. AEs frequently lead to premature treatment discontinuation, with studies showing that nausea and psychiatric symptoms are primary reasons for varenicline discontinuation, resulting in reduced smoking cessation success rates by up to 30%,15 while poor medication adherence is significantly associated with treatment failure across all smoking cessation pharmacotherapies.16 Furthermore, the impact on quality of life is substantial, with patients reporting that sleep-related AEs (including vivid dreams and insomnia) affect their daily functioning,17 while gastrointestinal symptoms such as nausea and vomiting can significantly interfere with work and social activities.18 Considering the increasing number of COPD patients requiring pharmacological intervention for smoking cessation and the limited scope of pre-marketing trials, a comprehensive assessment of these medications’ safety profiles in real-world settings is crucial for optimizing treatment strategies and improving patient outcomes.
This study aimed to investigate the adverse reactions associated with smoking cessation therapies in patients with COPD by analyzing data from the FDA Adverse Event Reporting System (FAERS). Specifically, we examined interactions between bupropion, nicotine, and varenicline, focusing on metrics such as onset time, disproportionality analysis, and co-medication analysis. Taking into account the unique challenges and requirements of COPD patients, these findings emphasize the urgent need for personalized smoking cessation strategies and shed light on potential barriers that must be addressed in clinical practice guidelines. This encompasses considerations for medication selection, monitoring protocols, as well as the establishment of comprehensive support systems aimed at improving quit rates within this vulnerable population.
Materials and Methods
Study Design and Data Source
The FAERS database plays a crucial role in post-marketing surveillance for adverse drug reactions (ADRs) and medication errors.19 It aggregates extensive data from both the FDA’s Safety Information and Adverse Event Reporting Program, contributing 5%, and the FDA’s Pharmacovigilance System, which accounts for 95%. This publicly accessible database supports the identification and analysis of signals that suggest disproportionate reporting of ADRs, aiding in the establishment of associations between particular drugs and AEs.20,21 While FAERS data is valuable for signal detection, it is important to note potential sources of bias inherent in spontaneous reporting systems, including variable reporting rates, selective reporting, and the inability to establish true incidence rates due to the lack of denominator data. Researchers frequently utilize FAERS for signal mining in post-market safety monitoring of pharmaceuticals and biologics.
The study period (Q1 2004 to Q2 2024) was selected to provide comprehensive coverage of the post-marketing period for all studied medications, ensuring adequate time for signal accumulation while maintaining data currency. At the onset of this study, the FDA had released data for the second quarter of 2024. Since the research utilized de-identified publicly available data, ethical approval was not necessary.
Cases and Drugs Definition
Within the FAERS database, AEs are classified using Preferred Terms (PTs), which are derived from the systematically structured, five-tiered Medical Dictionary for Regulatory Activities (MedDRA). PTs act as distinctive identifiers for specific medical concepts, such as symptoms, signs, and disease diagnoses. To ensure thorough research, we systematically examined the target drugs under different names (e-Supplementary material 1). Furthermore, we designated the role code Preferred Suspect (PS) to identify the drug reported as the primary suspect in AEs, enhancing the study’s reliability. To address potential confounding factors, we carefully documented and considered relevant clinical variables including COPD severity indicators, concurrent medications, and comorbidities when available in the reports.
For assessing the post-market safety of bupropion, nicotine, and varenicline in patients with COPD, data were extracted from the American Standard Code for Information Interchange (ASCII) files within the FAERS database. Our methodology followed established pharmacovigilance practices and was designed to enable replication by other researchers. Following FDA protocols, our study carefully identified and excluded duplicate reports. The most recent entry in the FDA_DT field was preferred for each CASEID, and when both CASEID and FDA_DT were identical, the entry with the higher PRIMARYID was selected to eliminate redundant data.
Descriptive Analysis
Patient demographics (age, sex, and reporter type) and clinical aspects (latency, outcome, and indication) were documented in reports of COPD with bupropion, nicotine, and varenicline.
Signal Screening and Analysis Strategy
This study aimed to investigate AEs associated with both individual smoking cessation medications (bupropion, varenicline, and nicotine) and their combinations. Our analysis strategy consisted of two main components: individual drug analysis and combination therapy analysis.
Signal Screening
Disproportionality analysis is a crucial method in pharmacovigilance for evaluating potential links between specific AEs and particular drugs.22 In this study, we compared data from the full FAERS database with four commonly used methods to identify positive safety signals: reporting odds ratio (ROR),23,24 proportional reporting ratio (PRR),25 Bayesian confidence propagation neural network (BCPNN),26 and Empirical Bayesian Geometric Mean (EBGM).27 ROR was calculated with its 95% confidence interval (CI), where a positive signal was defined as the lower bound of the 95% CI exceeding 1 with at least 3 cases reported. For PRR, a positive signal was identified when PRR ≥ 2, chi-squared ≥ 4, and the number of cases ≥ 3. BCPNN method utilized the Information Component (IC), with a positive signal defined as the lower bound of the 95% CI of IC (IC025) > 0. For EBGM, a positive signal was determined when the lower bound of the 90% CI of EBGM05 exceeded 2. These calculations were based on standard 2×2 contingency tables, where variables represented the presence or absence of the drug and AE of interest. Detailed mathematical formulas and computational procedures are provided in e-Supplementary material 2. To ensure the reliability of the results, a strong and valid association with the target drug was only considered when all four measures detected a positive safety signal for the AE under investigation. The target drugs examined in this study were bupropion, nicotine, varenicline.
We additionally inspected for unexpected PTs (uPT) absent from the target drug FDA approval documentation, which could imply undiscovered hazards linked to its administration. Additionally, we categorized PTs following the most recent edition (26.1) of the “Important medical event (IME) list” which was created by the EudraVigilance Expert Working Group. The primary standard for inclusion in the IME list is the presence of a serious AE or reaction. This includes any unfavorable medical event, irrespective of the dosage, that may result in death, be life-threatening, require hospital admission or extend an existing hospital stay, or lead to lasting or considerable disability/incapacity.
To further validate our findings and account for potential sex-based differences, we conducted additional analyses stratified by sex.
Co‑medication Analysis
We performed a combined drug analysis of bupropion, nicotine and varenicline. We also used ROR, PRR, BCPNN, and EBGM to measure drug interactions, as shown in e-Table 1. In addition, a post-hoc case-by-case analysis of 79 patients was conducted to identify combination drugs by searching for eight positive psychiatric signals associated with IME that were not listed in the official guidelines. The neuropsychiatric drugs and indications recorded in the report were retained. Data processing and statistical analyses were conducted using R (version 4.2.2).
Results
Descriptive Analysis
Figure 1 depicts the study flowchart. A total of 21,433,114 reports were present in FAERS through 2024Q2. Recorded AE reports associated with bupropion, nicotine, and varenicline spanned from 2004Q1 to 2024Q2, comprising 3882 AE reports attributed to bupropion, nicotine, and varenicline as the PS. In terms of combination drugs, bupropion and nicotine involved 23 AE reports, nicotine and varenicline involved 70 AE reports, and bupropion and varenicline involved 100 AE reports.
 |
Figure 1 Flowchart depicting the study process. Note: n represents the number of adverse events, and c represents the type of adverse events. |
From Q1 2004 to Q2 2024, there were 830 AE reports regarding bupropion, nicotine, and varenicline as the PS (Table 1). Sex distribution included 65.7% females (N =545), 31.1% males (N =258). Weight data were partly unavailable, with 31.4% (N =261) lacking this information; where provided, 54.0% weighed 50–100 kg (N =450), 8.4% over 100 kg (N =70), and 6.1% under 50 kg (N =51). Regarding patient age, 57.2% were ages 18–64 years (N = 475), 25.5% were ages 65–85 years (N =212) and 0.4% were ages over 85 years (N =3). Reports originated primarily from non-healthcare professional (such as consumer and lawyer) (69.5%, N =576) as well as healthcare professional (28.2%, N =234). Although most reports (94.2%, N =782) showed nonlethal results, 5.8% (N =48) concluded with loss of life. e-Table 2 shows the characteristics of reports associated with bupropion, nicotine and varenicline in combination from 2004Q1–2024Q2.
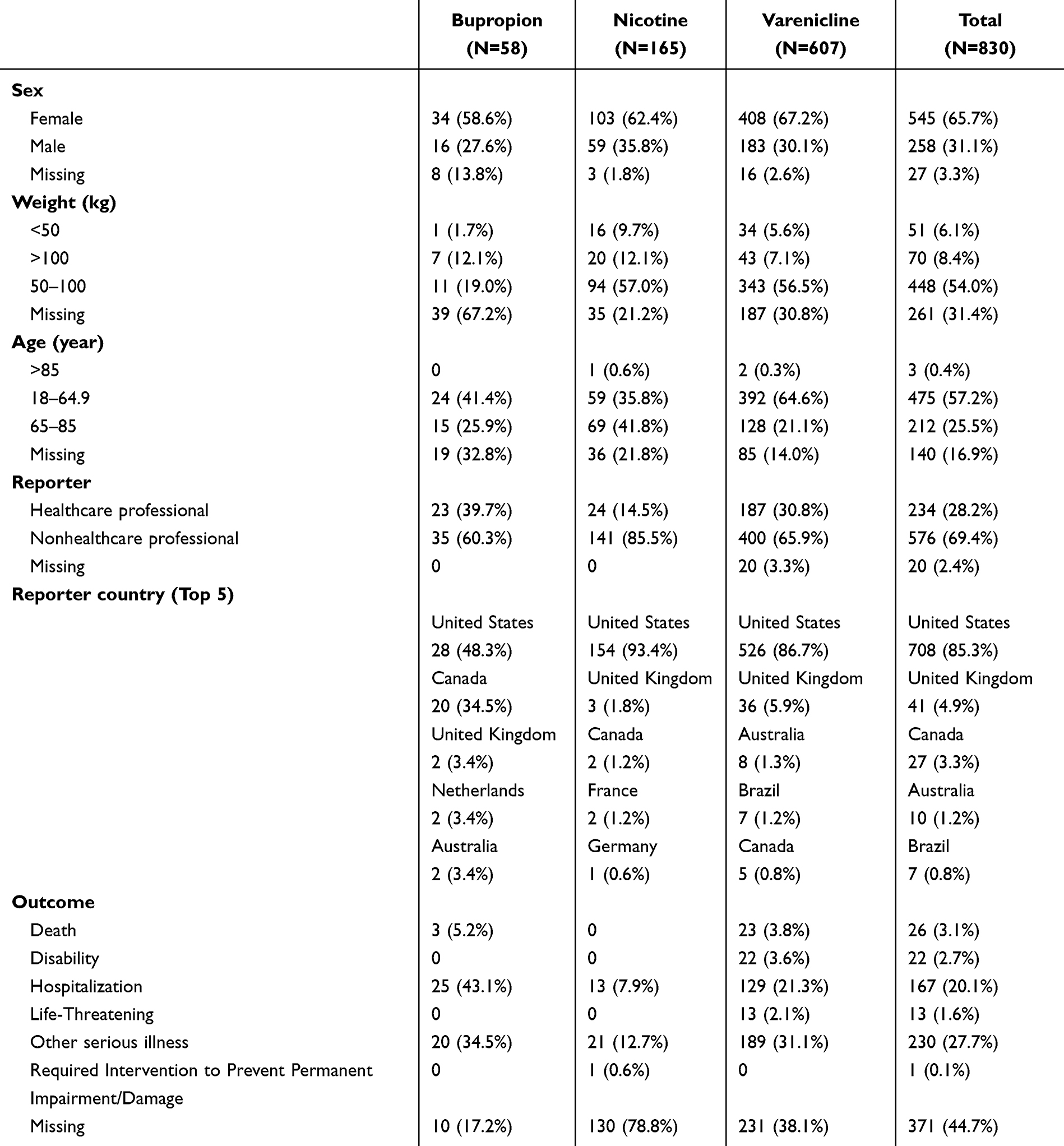 |
Table 1 Characteristics of Reports Associated with Bupropion, Nicotine and Varenicline from 2004Q1–2024Q2. Healthcare Professionals Including Reporters Such as Physicians and Pharmacists; Nonhealthcare Professionals Including Reporters Such as Consumer and Lawyer |
Figure 2A presents the yearly AE report trends for bupropion, nicotine, and varenicline from Q1 2004 to Q2 2024. Initially, very few reports were recorded between 2006 and 2009. A brief increase was observed in 2010, followed by a decline until it stabilized at around 200 AE reports per year to this day. The proportion of bupropion, nicotine, and varenicline among all AEs reported annually for COPD is shown in Figure 2B. It demonstrated that the proportion of varenicline increased year by year before 2010, then gradually decreased, and constituted many AEs of smoking cessation therapy before 2016. The proportion of nicotine has fluctuated at a low level throughout time. The proportion of bupropion increases at a slow rate and becomes dominant after 2021. Figure 2C shows the annual number of reported cases, which shows a similar trend as Figure 2A. As shown in Figure 2D, the number of AEs was mainly concentrated within 0–30 days, and then gradually decreased with the increase of the number of days, until it gradually increased after 181–360 days.
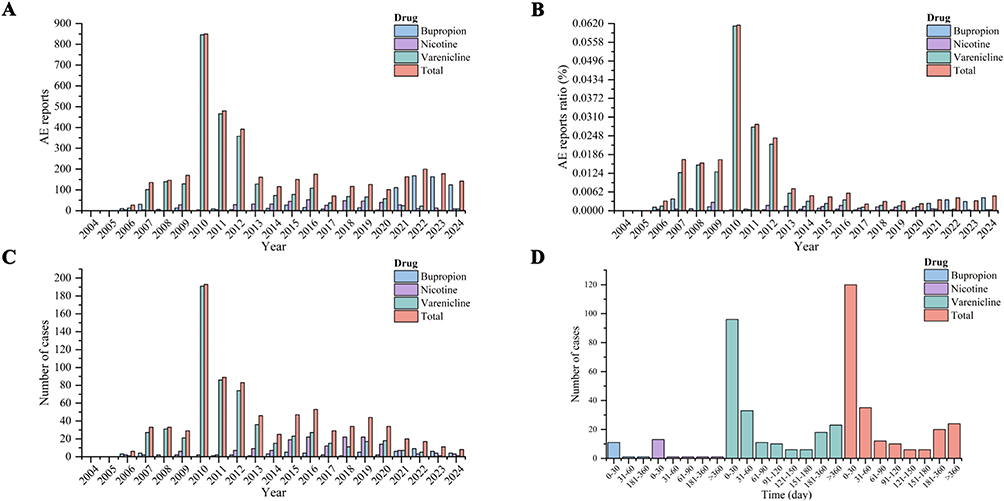 |
Figure 2 Comprehensive analysis of target drugs’ data. (A) Frequency of target drugs’ AEs in the FAERS database (2004Q1 - 2024Q2). (B) AE ratio for target drugs versus the total AE reports (2004Q1 - 2024Q2). (C) Number of target drugs’ cases in the FAERS database (2004Q1 - 2024Q2). (D) The frequency of AEs occurred in different time periods (2004Q1 - 2024Q2). |
 |
Figure 3 Classification of the AEs related to bupropion, nicotine and varenicline. |
Single-Drug Adverse Events
There were 727 AE categories of bupropion, nicotine, and varenicline recorded in FAERS database. After conducting signal screening, 639 categories were eliminated, comprising cases with fewer than 3 reports. Ultimately, 88 positive signals were identified. In addition, the signals of bupropion, nicotine and varenicline corresponding to AE were screened respectively, and 47, 13, 63 positive signals were obtained respectively. Figure 3 classifies and displays the positive signals obtained above. Results revealed that bupropion, nicotine, and varenicline involved adverse reactions mainly concentrated in psychiatric disorders, nervous system disorders, and gastrointestinal disorders. Some adverse reactions are classified as uPT, meaning they do not appear in the official FDA specification (e-Table 3).
A subsequent separate analysis found that psychiatric disorders, gastrointestinal disorders, and nervous system disorders were present in AEs in bupropion, nicotine and varenicline, but with different proportions (e-Figures 1–3). Gastrointestinal disorders (4 categories) and psychiatric disorders (7 categories) predominate in nicotine. Gastrointestinal disorders (11 categories) and psychiatric disorders (10 categories) account for the majority in bupropion, while psychiatric disorders (49 categories) dominate in varenicline.
Figure 4 presents the ROR results for the top 20 AEs. Depression, nausea, anxiety, abnormal dreams, insomnia, malaise, dizziness, feeling abnormal, suicide attempt, and suicidal ideation were the most frequently reported at the PT level. Multiple statistical measures including ROR (17.71/69.1/21.72), PRR (17.08/68.23/21.47), EBGM05 (12.81/31.14/13.86), and IC025 (2.22/3.71/2.5) indicated significantly elevated AE reporting for depression, suicide attempt, and suicidal ideation.
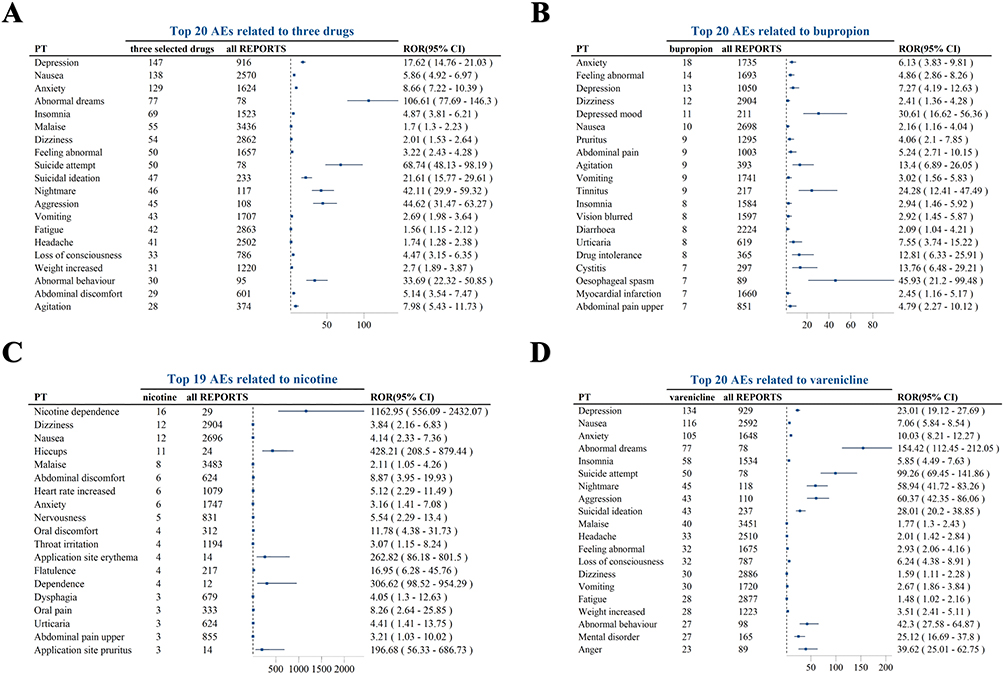 |
Figure 4 The reporting odds ratios of the top 20 AEs related to target drugs. (A) The reporting odds ratios of the top 20 AEs related to bupropion, nicotine and varenicline. (B) The reporting odds ratios of the top 20 AEs related to bupropion. (C) The reporting odds ratios of the 19 AEs related to nicotine. (D) The reporting odds ratios of the top 20 AEs related to varenicline. |
e-Figure 4 reveals that among the 149 identified bupropion, nicotine, and varenicline-related PTs, 15 PTs were recognized as IME warranting observation by the European Medicines Agency. Critically, 8 PTs indicated serious AEs not present in the labeling but requiring IME surveillance, including: bipolar disorder, completed suicide, dependence, hallucination (auditory), hallucination (visual), major depression, schizophrenia, and suicide attempt. These eight types of PTs were primarily associated with psychiatric disorders; thus, vigilant monitoring for potential AEs is necessary.
The total number of effective cases was 1808, which was analyzed for the onset time. It is worth noting that some cases only had the duration of treatment, while others only had the occurrence time of AEs (Figure 5). Among them, 14 PTs were reported between 0 to 1 years after the cessation of bupropion, nicotine and varenicline, which might be related to the delayed ADRs caused by the interested drugs. And six PTs showed up while taking the drug.
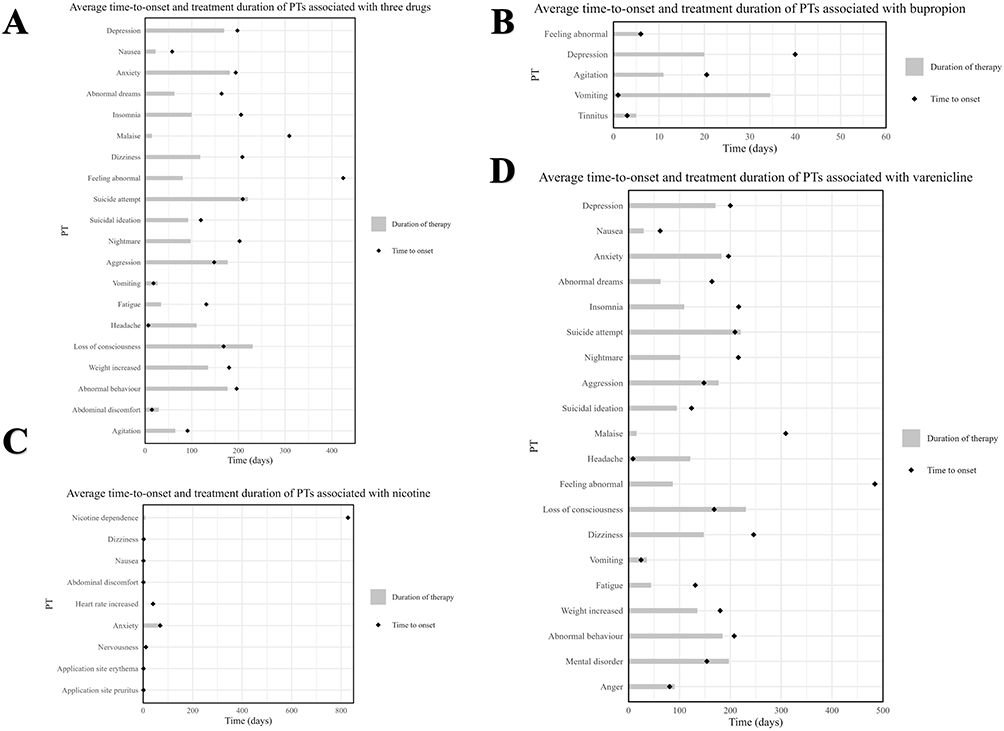 |
Figure 5 Time-to-onset analysis of the top 20 AEs reported for target drugs. Reported time-to-onset analysis and duration of treatment of the top 20 AEs with (A) bupropion, nicotine and varenicline, (B) bupropion (Only five), (C) nicotine (Only nine), (D) varenicline. |
In sex-stratified analysis of AEs across three smoking cessation medications, females constituted 65.7% of all reports, with distinct patterns emerging between sexes (e-Figure 5). While both males and females shared common primary AEs such as depression and anxiety, significant sex-specific differences were observed. Females demonstrated notably higher reporting of nausea (ROR: 6.57, 95% CI: 5.41–7.98) and abnormal dreams (ROR: 115.91, 95% CI: 77.82–172.64), while males showed increased reporting of suicidal ideation (ROR: 24.19, 95% CI: 14.99–39.02) and aggression (ROR: 39.96, 95% CI: 22.85–69.86). Drug-specific analyses revealed that females reported higher rates of nausea with varenicline (ROR: 7.78, 95% CI: 6.35–9.53) and showed distinct AE profiles with nicotine, particularly regarding dependence (ROR: 1771.34, 95% CI: 668.55–4693.21).
Combination Adverse Events
As shown in Figure 6A, nicotine combined with varenicline can produce bipolar disorder, anger, suicide attempt, weight increased, and depression as compared with nicotine alone. Nicotine combined with varenicline was associated with hallucination, dysphagia, pharyngeal oedema, dry mouth, and pneumonia compared with varenicline alone. Bipolar disorder, hypersensitivity, mental impairment, motor dysfunction, terminal insomnia, sleep terror, major depression, and schizophrenia et al were found in the combination of bupropion and varenicline compared with each on its own (Figure 6B). In the case of bupropion in combination with nicotine, nicotine dependence, and heart rate increased when using bupropion alone. Abdominal pain and agitation were observed when using nicotine alone. Thus, combining nicotine with varenicline or bupropion increases the risk of more severe adverse effects than using each drug alone. Notable risks include psychiatric (bipolar disorder, suicide attempt, hallucination, and depression et al), neurological (loss of consciousness, motor dysfunction, speech disorder and mental impairment et al), and gastrointestinal (abdominal pain, dysphagia and constipation et al) AEs.
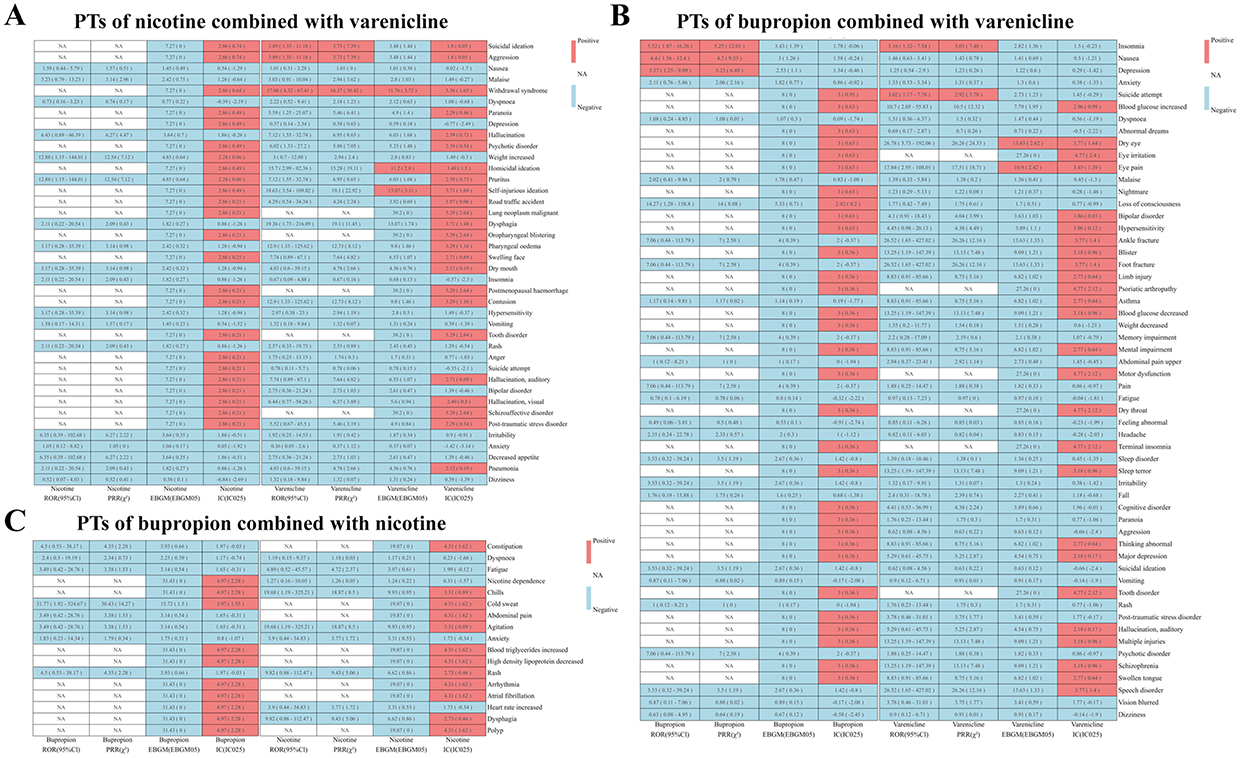 |
Figure 6 The heatmap of the AEs related to target drugs in combination. (A) PTs of nicotine combined with varenicline. (B) PTs of bupropion combined with varenicline. (C) PTs of bupropion combined with nicotine. |
Risk Management Plan‑Driven Case‑by‑Case Assessment
Eight AEs related to psychiatric disorders that were not listed in the official manual and associated with IME were also investigated case by case (e-Table 4): A range of psychiatric AEs were observed in association with psychiatric drug use, affecting patients with complex psychiatric profiles. These events included mood disorders, anxiety, substance dependence, hallucinations, schizophrenia, sleep disturbances, suicidality, and personality disorders. Common factors such as polypharmacy and pre-existing mental health conditions often exacerbated these events. Bipolar disorder was predominantly observed in females, involving psychotropic agents like lithium and antidepressants. Anxiety and depression were frequently reported, with polypharmacy contributing to adverse outcomes. Dependence on substances such as oxycodone and clonazepam was common, especially in patients with underlying anxiety and sleep disorders. Hallucinations (both auditory and visual) were linked to psychoactive drugs like gabapentin and antipsychotics. Sleep disturbances were often related to medications such as promethazine and were complicated by co-existing conditions. Instances of completed suicide and suicide attempts were particularly noted among older male patients, often involving drugs like sertraline and lorazepam. Specifically, out of the analyzed cases, 15% involved completed suicide and 20% involved suicide attempts, with several cases involving patients who had no prior psychiatric condition but experienced suicidal ideation or attempts after starting smoking cessation therapy with varenicline or bupropion. This suggests that these drugs may have a potential role in inducing suicidality, independent of any existing psychiatric conditions.
In our comprehensive case summary of psychiatric-type disorders (n=78), we identified distinct patterns between patients with and without pre-existing anti-psychotic therapy. (e-Table 4) Among the 23 patients without prior anti-psychotic therapy, only one patient (4.3%) exhibited multiple (2) positive psychiatric AE signals. In contrast, among the 55 patients with pre-existing anti-psychotic therapy, a significantly higher frequency of multiple AE signals was noted, with 15 patients (27.3%) exhibiting more than two positive signals. These findings indicate that patients with pre-existing anti-psychotic therapy may be more susceptible to experiencing multiple psychiatric AEs when using smoking cessation medications.
Patients with higher numbers of comorbidities consistently experienced more AEs, with this trend being particularly pronounced in the bupropion group where patients with 20 comorbidities exhibited approximately 25–30 AEs (e-Figure 6). Similarly, varenicline users showed a moderate increase in AEs with increasing comorbidities, though less dramatic than bupropion, while nicotine replacement therapy also demonstrated an upward trend in AEs as comorbidities increased. The aggregate data (e-Figure 6A) further supports this pattern, showing a clear escalation in AE frequency as the number of comorbidities rises, with patients having 13–15 comorbidities experiencing the highest median number of AEs. These findings strongly suggest that patients with multiple comorbidities are indeed more susceptible to experiencing AEs during smoking cessation treatment, which has important implications for clinical practice and highlights the need for more careful monitoring and potentially modified treatment approaches for patients with multiple comorbidities.
Discussion
Smoking cessation represents a critical intervention in clinical practice, particularly for COPD patients, as it remains the most effective strategy to slow disease progression and improve survival. Studies have shown that successful smoking cessation can reduce the decline in forced expiratory volume in one second (FEV1), decrease exacerbation frequency, and improve quality of life in COPD patients.28 Relatively few studies of interventions for smoking cessation have targeted patients with COPD specifically. Our study investigated the adverse reactions associated with smoking cessation therapies—specifically bupropion, nicotine, and varenicline—in patients with COPD. By analyzing data from the FAERS database, the study examined drug interactions, onset times, and signal detection, thereby providing insights into the safety profiles of these therapies in this vulnerable population.
The current findings revealed significant sex and age disparities in AE reports, with most reports coming from females and individuals aged 18–64 years. While smoking persists as the predominant cause of COPD across all genders, only a portion of the increase in COPD among women can be attributed to proportional rises in smoking.29 Even when comparing individuals with similar tobacco exposures, women are exposed to a higher risk of developing COPD compared to men.30 The aforementioned sex disparities are also evident in several theories, including the smaller lung size of women, hormonal disparities, and genetics/epigenetics, among others.31
The rate of AE reporting increased significantly from 2004 to 2010, possibly reflecting the increased prescription of pharmacotherapy in this period. However, reports decreased significantly from 2010 onwards, especially with the use of varenicline, while nicotine and bupropion have remained relatively stable This could have resulted from the FDA issuing a black box warning in 2009. The decision comes after reports of patients taking varenicline experiencing severe neuropsychiatric symptoms, including suicidal thoughts and suicide attempts. And 3.9 million US patients took the drug in 2007 versus only 1.2 million in 2012.32 More recently, in 2021, Pfizer recalled varenicline due to elevated nitrosamine levels exceeding acceptable daily intake limits, leading to its temporary market withdrawal. The distribution of AEs over time indicates that most events occur within the first 30 days of therapy, with a gradual decline thereafter, though some AEs persist or emerge even after a year. This timeline is essential for clinicians to monitor patients closely during the early stages of smoking cessation therapy and to be aware of potential delayed AEs.
The analysis of AEs at the PT level in the FAERS database revealed 88 positive safety signals for bupropion, nicotine, and varenicline. These signals predominantly clustered around psychiatric disorders, nervous system disorders, and gastrointestinal disorders. The most frequently reported AEs included depression, nausea, anxiety, abnormal dreams, and insomnia, with significant signal strength across multiple statistical measures. Sex-stratified analysis revealed distinct AE patterns, with females (65.7% of reports) experiencing higher rates of nausea and abnormal dreams, while males showed increased vulnerability to suicidal ideation and aggression. These findings highlight the psychological and neurological impact of smoking cessation therapies in patients with COPD. Anthenelli et al found that varenicline, bupropion, and nicotine patches are more effective than placebo for smoking cessation, with varenicline being the most effective. None of these treatments increased the risk of neuropsychiatric adverse effects, including suicidal thoughts or behavior, in either group.33 The high prevalence of psychiatric AEs, particularly depression and suicidal ideation, is concerning, given the already heightened vulnerability of patients with COPD to mental health issues due to chronic illness. Gastrointestinal AEs, such as nausea and abdominal discomfort, also pose a challenge, potentially affecting medication adherence. These insights underscore the need for comprehensive patient counseling and close monitoring, particularly for those with pre-existing psychiatric conditions or a history of gastrointestinal issues.
When analyzing the combination of bupropion, nicotine, and varenicline, the study identified several significant AEs. For instance, bupropion combined with varenicline was linked to a wide range of adverse effects, including blood glucose changes, bipolar disorder, hypersensitivity, mental impairment, hallucinations, and schizophrenia. The Phase III trial conducted by Ebbert et al identified anxiety (18% with bupropion and varenicline vs 8% with monotherapy) and depressive symptoms (9% with bupropion and varenicline vs 2% with monotherapy) as the only AEs occurring more commonly with combination therapy.34 In contrast, Rose et al reported no significant difference in the incidence of AEs between combination therapy (bupropion and varenicline) and monotherapy.35 When bupropion was combined with nicotine, there were increased risks of nicotine dependence, heart rate, abdominal pain, agitation, constipation, rash, arrhythmia, and dysphagia, among others. In the combination treatment group (varenicline + nicotine), there was a numerically greater incidence of nausea, sleep disturbance, skin reactions, constipation, and depression, with only skin reactions reaching statistical significance (14.4% vs 7.8%); the varenicline-alone group experienced more abnormal dreams and headaches.36 Overall, the observed increase in psychiatric, neurological, cardiovascular, and gastrointestinal AEs with certain drug combinations suggests that while combination therapy may be effective in aiding smoking cessation, it may also introduce new risks, particularly in vulnerable populations such as those with pre-existing conditions. Additionally, several patients reported experiencing depression and suicide even though they had no previous history of psychiatric disorders or use of psychotropic medications. It implies that the adverse psychiatric effects could truly be directly ascribed to the smoking cessation drugs themselves, rather than the impact of prior psychiatric conditions or other medications. Clinicians should carefully assess each patient’s comorbidity, considering the inherent risks of these medications, while also weighing the benefits of combination therapy against the potential for increased AEs to individual patient profiles to minimize risks.
Even with the most effective combination of pharmacotherapy and counseling for smoking cessation, more than 80% of persons who smoke with COPD continue smoking after one year.7 The Lung Health Study (LHS) identified potential barriers to successful quitting in patients with mild to moderate COPD, including weight gain (especially in women) and insufficient social support.37 During the first year of the LHS, women who quit smoking gained 8.4% of their baseline weight, while men gained 6.7%.38 Among those accompanied by an ex-smoker, 75% of men and 72% of women achieved abstinence after one year, compared to only 34% of men and 32% of women who were supported by a current smokers.39 Depression and anxiety are more common in individuals with COPD, with rates of 18.8% and 28.2% respectively, compared to 6.1% and 3.5% in non-COPD controls, as reported by an Italian study.40 Depression has also been identified as a significant obstacle to successful smoking cessation; individuals with current or past depression tend to have higher nicotine dependence, are more prone to experiencing negative mood changes during quit attempts, and were more likely to relapse than the general smoking population.41 A meta-analysis of randomized trials specifically targeting patients with COPD, encompassing 7,372 participants across six of eight identified trials, found that smoking cessation counseling combined with an antidepressant was the second most effective intervention, compared to counseling alone.42 Thus, studies of novel smoking cessation strategies are deserved.
Based on our findings and the critical importance of smoking cessation in clinical practice, we propose several key considerations for medication selection and patient monitoring. For patients with eating disorders, bupropion should be avoided due to its reduced manageability and potential impact on appetite and weight, while those with psychiatric history require careful monitoring when using varenicline or bupropion, particularly during the first 30 days of treatment, with nicotine replacement therapy being a potentially safer initial choice. Elderly patients should begin with lower doses and consider monotherapy before attempting combination treatments, while patients with gastrointestinal sensitivity might benefit from nicotine replacement therapy as the first-line treatment due to its lower incidence of gastrointestinal AEs. For patients who cannot tolerate or have limited access to first-line medications, cytisine represents a viable second-line treatment option, with evidence supporting its efficacy and favorable safety profile, particularly in regions where cost or availability of first-line treatments may be limiting factors.43 When considering combination therapy, clinicians should carefully evaluate the patient’s comorbidity profile, previous response to monotherapy, risk factors for specific AEs, and available support system.
The results of this study should be interpreted in light of several limitations. First, this is a descriptive study focused on characterizing AE patterns without formal statistical analyses, which limits our ability to make comparative inferences and establish causal relationships between the therapies and the reported AEs; the findings should be interpreted with caution. Second, the FAERS database relies on voluntary reporting, which introduces inherent reporting biases that significantly impact data interpretation. These biases include potential underreporting of AEs, particularly for mild or common reactions, and selective over-reporting of specific AEs, especially those that are severe or receive media attention. To address these reporting biases, we implemented a comprehensive validation approach that includes case-by-case analysis as an additional verification step, and employed multiple disproportionality analysis methods (ROR, PRR, BCPNN, and EBGM) with conservative thresholds to minimize false positives. Third, the data did not account for confounding factors such as the severity of COPD, concomitant medications, or comorbid conditions, which could influence the occurrence and reporting of AEs. Fourth, the relatively small sample size in the co-medication analyses may limit the generalizability of our findings and the ability to detect rare AEs. To mitigate this limitation, we employed a more conservative analytical approach, where only EBGM05 and IC025 were included to ensure statistical reliability, as the ROR and PRR methods were not applicable for small sample sizes. Given these limitations, further controlled studies with rigorous statistical analyses are needed to confirm the associations identified in this analysis and to better understand the underlying mechanisms of these adverse effects. Additionally, longitudinal studies would be valuable to determine the temporal relationship between drug administration and AEs, as well as their potential duration and long-term outcomes.
Conclusion
This study provided crucial insights into the safety profile of smoking cessation therapies in patients with COPD, emphasizing the notable risks associated with psychiatric, neurological, and gastrointestinal AEs, especially in psychiatric disorders. Given these findings, clinicians need to pay more attention to patients’ comorbidities and prior medication history, especially those who are predisposed to mental health disorders or who use combination therapy.
Abbreviations
COPD, Chronic obstructive pulmonary disease; FAERS, FDA Adverse Event Reporting System; ADRs, adverse drug reactions; AEs, adverse events; PTs, Preferred Terms; MedDRA, Medical Dictionary for Regulatory Activities; PS, Preferred Suspect; ASCII, Information Interchange; ROR, reporting odds ratio; PRR, proportional reporting ratio; BCPNN, Bayesian confidence propagation neural network; EBGM, Empirical Bayesian Geometric Mean; CI uPT, confidence interval; unexpected PT; LHS, The Lung Health Study.
Ethical Approval Statement
This study utilized data from a publicly available, open-source database. According to the Measures for Ethical Review of Life Science and Medical Research Involving Human Subjects (effective February 18, 2023, China), research involving publicly available datasets is exempt from additional ethical review by an Institutional Review Board or ethics committee (Article 32, Items 1 and 2).
Acknowledgments
The authors thank The FDA Adverse Event Reporting System (FAERS).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Science and Technology Department of Sichuan Province (No. 2024NSFSC1679 to Dong Xu Chen) and Chengdu Science and Technology Department - Technological Innovation R&D Project (General Project. No. 2024-YF05-00339-SN to Dong Xu Chen).
Disclosure
The authors declare no competing interests in this work.
References
1. Devadoss D, Long C, Langley RJ, et al. Long noncoding transcriptome in chronic obstructive pulmonary disease. American Journal of Respiratory Cell and Molecular Biology. 2019;61:678–688. doi:10.1165/rcmb.2019-0184TR
2. Ehteshami-Afshar S, FitzGerald JM, Doyle-Waters MM, Sadatsafavi M. The global economic burden of asthma and chronic obstructive pulmonary disease. Int J Tuberc Lung Dis. 2016;20:11–23. doi:10.5588/ijtld.15.0472
3. Sana A, Meda N, Kafando B, Badoum G, Bouland C. Prevalence of COPD among women and relation with cooking fuel choice in Ouagadougou, Burkina Faso. Int J Tuberc Lung Dis. 2020;24:928–933. doi:10.5588/ijtld.19.0609
4. Joo H, Yoon HK, Hwang Y, et al. Application of the lancet commission COPD classification to COPD cohort population in South Korea. Respir Med. 2024;230:107679. doi:10.1016/j.rmed.2024.107679
5. Schauer GL, Wheaton AG, Malarcher AM, Croft JB. Smoking prevalence and cessation characteristics among U.S. adults with and without COPD: findings from the 2011 behavioral risk factor surveillance system. COPD. 2014;11:697–704. doi:10.3109/15412555.2014.898049
6. Yin P, Wu J, Wang L, et al. The burden of COPD in China and its provinces: findings from the global burden of disease study 2019. Front Public Heal. 2022;10:859499. doi:10.3389/fpubh.2022.859499
7. Tashkin DP. Smoking cessation in chronic obstructive pulmonary disease. Semin Respir Crit Care Med. 2015;36:491–507. doi:10.1055/s-0035-1555610
8. 2024 GOLD report - global initiative for chronic obstructive lung disease - GOLD. Available from: https://goldcopd.org/2024-gold-report/.
9. Hand S, Edwards S, Campbell IA, Cannings R. Controlled trial of three weeks nicotine replacement treatment in hospital patients also given advice and support. Thorax. 2002;57:715–718. doi:10.1136/thorax.57.8.715
10. Tashkin D, Kanner R, Bailey W, et al. Smoking cessation in patients with chronic obstructive pulmonary disease: a double-blind, placebo-controlled, randomised trial Lancet. 2001;357:1571–1575. doi:10.1016/S0140-6736(00)04724-3
11. Clinical Practice Guideline Treating Tobacco Use and Dependence. 2008 update panel, liaisons and S. A clinical practice guideline for treating tobacco use and dependence: 2008 update. A U.S. public health service report. American Journal of Preventive Medicine. 2008;35:2008158. doi:10.1016/j.amepre.2008.04.009
12. Tønnesen P, Carrozzi L, Ko F, et al. Smoking cessation in patients with respiratory diseases: a high priority, integral component of therapy. Eur Respir J. 2007;29:390–417. doi:10.1183/09031936.00060806
13. US FDA. US food and drug administration public health advisory: FDA requires new boxed warnings for the smoking cessation drugs Chantix and Zyban. 2009.
14. Hurt RT, Ebbert JO, Croghan IT, Schroeder DR, Hurt RD, Hays JT. Varenicline for tobacco-dependence treatment in alcohol-dependent smokers: a randomized controlled trial. Drug Alcohol Depend. 2018;184:12–17. doi:10.1016/j.drugalcdep.2017.11.017
15. Walton KM, Herrmann ES. Medication adherence in tobacco cessation clinical trials. Available from: http://www.ncbi.nlm.nih.gov/pubmed/36817408.
16. D Drovandi A, C Chen C, D Glass B. Adverse effects cause varenicline discontinuation: a meta-analysis. Curr Drug Saf. 2015;11:78–85.
17. Ebbert J, Jimenez-Ruiz C, Dutro MP, Fisher M, Li J, Hays JT. Frequently reported adverse events with smoking cessation medications: post hoc analysis of a randomized trial. Mayo Clin Proc. 2021;96:1801–1811. doi:10.1016/j.mayocp.2020.10.046
18. Shah SD, Wilken LA, Winkler SR, Lin S-J. Systematic review and meta-analysis of combination therapy for smoking cessation. J Am Pharm Assoc. 2008;48:659–665. doi:10.1331/JAPhA.2008.07063
19. Jing Y, Liu J, Ye Y, et al. Multi-omics prediction of immune-related adverse events during checkpoint immunotherapy. Nat Commun. 2020;11:4946. doi:10.1038/s41467-020-18742-9
20. Raschi E, Fusaroli M, Giunchi V, et al. Adrenal insufficiency with anticancer tyrosine kinase inhibitors targeting vascular endothelial growth factor receptor: analysis of the FDA adverse event reporting system. Cancers. 2022;15:14. doi:10.3390/cancers15010014
21. Xia S, Gong H, Zhao Y, et al. Tumor lysis syndrome associated with monoclonal antibodies in patients with multiple myeloma: a pharmacovigilance study based on the FAERS database. Clin Pharmacol Ther. 2023;114:211–219. doi:10.1002/cpt.2920
22. Caster O, Aoki Y, Gattepaille LM, Grundmark B. Disproportionality analysis for pharmacovigilance signal detection in small databases or subsets: recommendations for limiting false-positive associations. Drug Saf. 2020;43:479–487. doi:10.1007/s40264-020-00911-w
23. Yan Y-D, Zhao Y, Zhang C, et al. Toxicity spectrum of immunotherapy in advanced lung cancer: a safety analysis from clinical trials and a pharmacovigilance system. EClinicalMedicine. 2022;50:101535. doi:10.1016/j.eclinm.2022.101535
24. Zhou C, Peng S, Lin A. Psychiatric disorders associated with immune checkpoint inhibitors: a pharmacovigilance analysis of the FDA Adverse Event Reporting System (FAERS) database. eClinicalMedicine. 2023;59:101967. doi:10.1016/j.eclinm.2023.101967
25. Zhu H, Qu Y, Du Z. Mining and analysis of adverse event signals of cariprazine based on the real-world data of FAERS database. J Affect Disord. 2024;347:45–50. doi:10.1016/j.jad.2023.11.076
26. Bate A, Lindquist M, Edwards IR. A Bayesian neural network method for adverse drug reaction signal generation. Eur J Clin Pharmacol. 1998;54:315–321. doi:10.1007/s002280050466
27. Chen C, Ding L, Fu F, Xiao J. Updated insights on dementia-related risk of sacubitril/valsartan: a real-world pharmacovigilance analysis. CNS Neurosci Ther. 2023;29:2548–2554. doi:10.1111/cns.14195
28. Pezzuto A, Ricci A, D’ascanio M, et al. Short-Term benefits of smoking cessation improve respiratory function and metabolism in smokers. Int J COPD. 2023;18:2861–2865. doi:10.2147/COPD.S423148
29. Aryal S, Diaz-Guzman E, Mannino DM. Influence of sex on chronic obstructive pulmonary disease risk and treatment outcomes. International Journal of COPD. 2014;9:1145–1154. doi:10.2147/COPD.S54476
30. Hardin M, Foreman M, Dransfield MT. Sex-specific features of emphysema among current and former smokers with COPD. Eur Respir J. 2016;47:104–112. doi:10.1183/13993003.00996-2015
31. Han MK. Chronic obstructive pulmonary disease in women: a biologically focused review with a systematic search strategy. Int J Chron Obstruct Pulmon Dis. 2020;15:711–721. doi:10.2147/COPD.S237228
32. Mohammadi D. Black-box warnings could be removed from varenicline. Lancet Respir Med. 2016;4:861. doi:10.1016/S2213-2600(16)30310-1
33. Anthenelli RM, Benowitz NL, West R. Neuropsychiatric safety and efficacy of varenicline, bupropion, and nicotine patch in smokers with and without psychiatric disorders (EAGLES): a double-blind, randomised, placebo-controlled clinical trial. Lancet. 2016;387:2507–2520. doi:10.1016/S0140-6736(16)30272-0
34. Ebbert JO, Hatsukami DK, Croghan IT. Combination varenicline and bupropion SR for tobacco-dependence treatment in cigarette smokers: a randomized trial. JAMA. 2014;311:155–163. doi:10.1001/jama.2013.283185
35. Rose JE, Behm FM. Combination treatment with varenicline and bupropion in an adaptive smoking cessation paradigm. Am J Psychiatry. 2014;171:1199–1205. doi:10.1176/appi.ajp.2014.13050595
36. Koegelenberg CFN, Noor F, Bateman ED, et al. Efficacy of varenicline combined with nicotine replacement therapy vs varenicline alone for smoking cessation: a randomized clinical trial. JAMA. 2014;312:155–161. doi:10.1001/jama.2014.7195
37. Kanner RE, Connett JE, Williams DE, Buist AS. Effects of randomized assignment to a smoking cessation intervention and changes in smoking habits on respiratory symptoms in smokers with early chronic obstructive pulmonary disease: the Lung Health Study. Am J Med. 1999;106:410–416. doi:10.1016/S0002-9343(99)00056-X
38. Nides M, Rand C, Dolce J. Weight gain as a function of smoking cessation and 2-Mg nicotine gum use among middle-aged smokers with mild lung impairment in the first 2 years of the lung health study. Heal Psychol. 1994;13:354–361. doi:10.1037/0278-6133.13.4.354
39. Tashkin DP, Murray RP. Smoking cessation in chronic obstructive pulmonary disease. Respiratory Medicine. 2009;103:2009963. doi:10.1016/j.rmed.2009.02.013
40. Di Marco F, Verga M, Reggente M, et al. Anxiety and depression in COPD patients: the roles of gender and disease severity. Respir Med. 2006;100:1767–1774. doi:10.1016/j.rmed.2006.01.026
41. Pergolizzi J, Böger RH, Budd K. Opioids and the management of chronic severe pain in the elderly: consensus statement of an international expert panel with focus on the six clinically most often used world health organization step III opioids (buprenorphine, fentanyl, hydromorphone, methadone, morphine, oxycodone). Pain Pract. 2008;8:287–313. doi:10.1111/j.1533-2500.2008.00204.x
42. Strassmann R, Bausch B, Spaar A, Kleijnen J, Braendli O, Puhan MA. Smoking cessation interventions in COPD: a network meta-analysis of randomised trials. Eur Respir J. 2009;34:634–640. doi:10.1183/09031936.00167708
43. Hajek P, McRobbie H, Myers K. Efficacy of cytisine in helping smokers quit: systematic review and meta-analysis. Thorax. 2013;68:1037–1042. doi:10.1136/thoraxjnl-2012-203035
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.