Back to Journals » Drug Design, Development and Therapy » Volume 20
Pharmacological Mechanisms and Clinical Applications of Oxycodone in Cancer Pain Management: A Narrative Review
Received 9 January 2026
Accepted for publication 29 March 2026
Published 11 April 2026 Volume 2026:20 594973
DOI https://doi.org/10.2147/DDDT.S594973
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Muzammal Hussain
Yuanlin Xia, Guihua Huang
Department of Anesthesiology, Guizhou Hospital of Beijing Jishuitan Hospital, Guiyang, Guizhou Province, 550014, People’s Republic of China
Correspondence: Guihua Huang, Email [email protected]
Abstract: Cancer pain significantly impairs quality of life in oncology patients and remains inadequately managed globally. This narrative review examines the pharmacokinetic and pharmacodynamic properties of oxycodone, the impact of CYP2D6 genetic polymorphism on its metabolism, and the EGFR-dependent bidirectional effects of oxycodone on cancer cell biology. Critically, these bidirectional tumor cell effects were observed exclusively under supraphysiological in vitro concentrations (0.01– 10 μM), far exceeding clinical therapeutic plasma levels (nM range), and are insufficient to alter current clinical guidelines. We further evaluate oxycodone’s effects on tumor angiogenesis and immune function, and summarize clinical evidence from postoperative analgesia studies in breast, colorectal, gastric, lung, and liver cancer patients, supporting oxycodone as a preferred option for perioperative analgesia in abdominal and thoracic cancer surgery. The limitations of oxycodone in chronic neuropathic and bone metastasis pain are discussed, alongside recent advances in oxycodone formulation development and novel analgesics in China. Individualized treatment strategies integrating pharmacogenomic profiles and multimodal approaches are encouraged.
Keywords: oxycodone, cancer pain, postoperative analgesia, pharmacological effects, mechanism of action, drug comparison
Introduction
Pain in cancer patients represents a global public health concern that significantly impairs quality of life and treatment adherence. Cancer-related pain may arise from direct tumor invasion of soft tissues or bone and is frequently among the presenting symptoms at cancer diagnosis.1 A 2022 systematic study revealed an overall pain prevalence of 44.5% among cancer patients, with moderate-to-severe pain affecting 30.6%.2 A European multicenter survey involving 5000 cancer patients demonstrated that 72% experienced pain, of whom 90% reported moderate-to-severe intensity.3 These data indicate that despite substantial advances in oncology and pain management, cancer pain control remains a formidable challenge. Notably, recent research has shown that fewer than half of all deceased cancer patients had been prescribed potent opioids, with a median treatment duration of only nine weeks before death,4 suggesting significant inadequacies in cancer pain treatment.
Oxycodone is a potent opioid analgesic indicated for the management of moderate-to-severe chronic pain, including cancer pain.5 Since its initial clinical application in 1917, oxycodone has been widely adopted for moderate-to-severe pain management owing to its excellent analgesic efficacy, low incidence of adverse effects, and favorable oral bioavailability.6 Oxycodone exerts its analgesic effects primarily by binding to μ-opioid receptors in the spinal dorsal horn and brain, thereby inhibiting pain signal transmission.7 This receptor binding suppresses neuronal calcium channel opening, consequently reducing the release of excitatory neurotransmitters such as glutamate and blocking pain signal conduction.8 Notably, unlike morphine and fentanyl—the most widely used opioids in oncology—oxycodone demonstrates clinically meaningful κ-opioid receptor agonist activity in animal models, which may confer advantages in alleviating visceral pain and refractory neuropathic pain.7 In addition, accumulating evidence suggests that oxycodone produces relatively milder immunosuppressive effects than morphine,9 a distinction of particular clinical relevance given the already compromised immune status of cancer patients. These pharmacological features justify dedicated analysis of oxycodone as a distinct entity rather than treating it interchangeably with other opioids.
The review aims to elucidate the pharmacokinetic and pharmacodynamic characteristics of oxycodone, with particular emphasis on CYP2D6 genetic polymorphism; to analyze the bidirectional effects of oxycodone on cancer cell biology in relation to EGFR expression levels; to summarize clinical evidence across multiple cancer types; and to discuss limitations in chronic cancer pain management and advances in novel analgesic development in China, with the aim of providing evidence-based guidance for individualized cancer pain treatment strategies.
Search Strategies and Inclusion and Exclusion Criteria
This review is a narrative review of the published literature on oxycodone in cancer pain management. We conducted a systematic literature search of PubMed, Embase, and the Cochrane Library using the following search terms: “oxycodone,” “cancer pain,” “postoperative analgesia,” “pharmacokinetics,” “pharmacodynamics,” “tumor biology,” “EGFR,” and “immune function,” covering publications from January 2000 to December 2025, supplemented by seminal earlier studies. Inclusion criteria were: original research articles, randomized controlled trials, cohort studies, registry-based analyses, and high-quality reviews addressing oxycodone use in adult cancer patients. Non-English publications without English abstracts and case reports were excluded.
Analgesic Mechanisms of Oxycodone and Its Pharmacokinetic and Pharmacod-Ynamic Characteristics in Cancer Patients
The pharmacokinetic (PK) and pharmacodynamic (PD) profiles of oxycodone in cancer patients are influenced by multiple factors, primarily including metabolic enzyme genetic polymorphisms, routes of administration, hepatic function status, and interindividual variability. The following section systematically summarizes advances in PK and PD research on oxycodone and provides an in-depth discussion of recent findings, such as the utility of population PK models in cancer patients—which facilitate individualized dose adjustments to prevent both overdosing and underdosing.
Pharmacokinetics of Oxycodone in Cancer Patients
Studies have demonstrated that oxycodone exhibits high oral bioavailability (approximately 87%). The volume of distribution is approximately 200–250 L following oral administration and 190–210 L following intravenous injection; plasma clearance is approximately 45–50 L/h, with an elimination half-life of approximately 3–4 hours.10 For intravenous administration, peak plasma concentration (Cmax) is achieved rapidly within 5–15 minutes (Tmax: ~5–15 min); for immediate-release oral formulations, Cmax occurs at approximately 1–1.5 hours (Tmax: ~60–90 min); and for controlled-release formulations, Cmax is reached at approximately 3 hours (Tmax: ~3 h) with more gradual absorption and attenuated peak concentrations.8,11 Controlled-release formulations exhibit a delayed absorption phase of approximately 1 hour, with plasma concentrations rising rapidly thereafter.12 Following absorption, oxycodone is primarily metabolized via CYP3A4 (producing noroxycodone) and CYP2D6 (producing oxymorphone) (Figure 1), with approximately 45–50% metabolized through CYP3A enzymes and 10–19% through CYP2D6.13,14 Although variations in metabolic pathways (eg., CYP2D6 metabolizer phenotypes) may affect metabolite concentrations, current evidence suggests minimal impact on analgesic efficacy and adverse effects.15,16
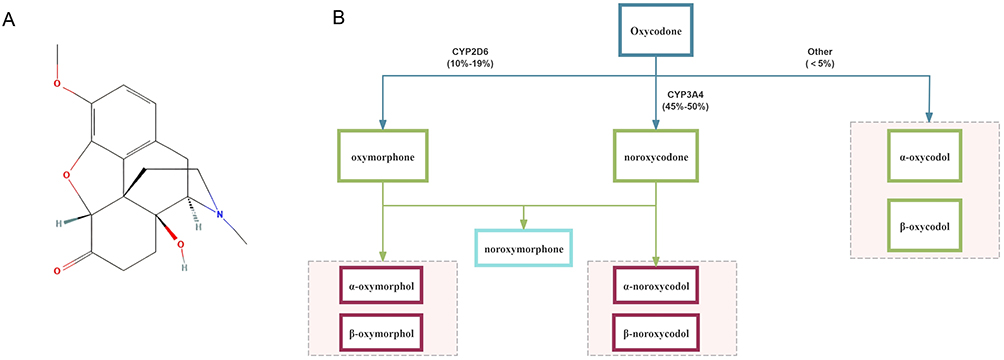 |
Figure 1 Metabolites and metabolic pathways of oxycodone. (A) Chemical structure of oxycodone; (B) Metabolic pathway of oxycodone showing major metabolic enzymes and their corresponding metabolic percentages: CYP3A4 (45–50%, producing noroxycodone) and CYP2D6 (10–19%, producing oxymorphone), with minor pathways producing α-oxycodol and β-oxycodol. |
Notably, PK characteristics differ in special populations. In patients with hepatic impairment (eg., Child-Pugh class B), oxycodone clearance may be significantly reduced, resulting in approximately 1.5-fold higher plasma concentrations and necessitating dose adjustments.12 In patients with renal dysfunction, reduced renal clearance of oxymorphone and other metabolites may lead to accumulation; a dose reduction of 25–50% or extended dosing intervals is advisable in patients with creatinine clearance below 30 mL/min.17 In elderly patients (≥75 years), polypharmacy-related drug interactions (eg., co-administration of CYP3A4 inhibitors) and reduced renal/hepatic reserve may prolong mean half-life and increase exposure; careful dose titration starting at the lower end of the dosing range is recommended.18 In patients with metastatic disease, disease burden and cachexia-related changes in protein binding and volume of distribution may further alter PK parameters; individualized population PK modeling is particularly valuable in this setting.19 In immunocompromised patients (eg., post-chemotherapy), altered drug disposition may result from hepatotoxicity or renal impairment induced by cytotoxic agents, underscoring the importance of therapeutic drug monitoring when feasible.20
Plasma clearance of oxycodone is 48.6 ± 26.5 L/h, with an elimination half-life of 3.01 ± 1.37 hours (intravenous) or 3.51 ± 1.43 hours (oral).10 The drug is predominantly hepatically metabolized, with minor amounts excreted renally as unchanged drug and metabolites.21 Under steady-state conditions (10 mg every 4 hours), trough plasma concentrations are 34.6 ± 10.3 μg/L, with no apparent drug accumulation.10 Table 1 summarizes the principal pharmacokinetic parameters of oxycodone.
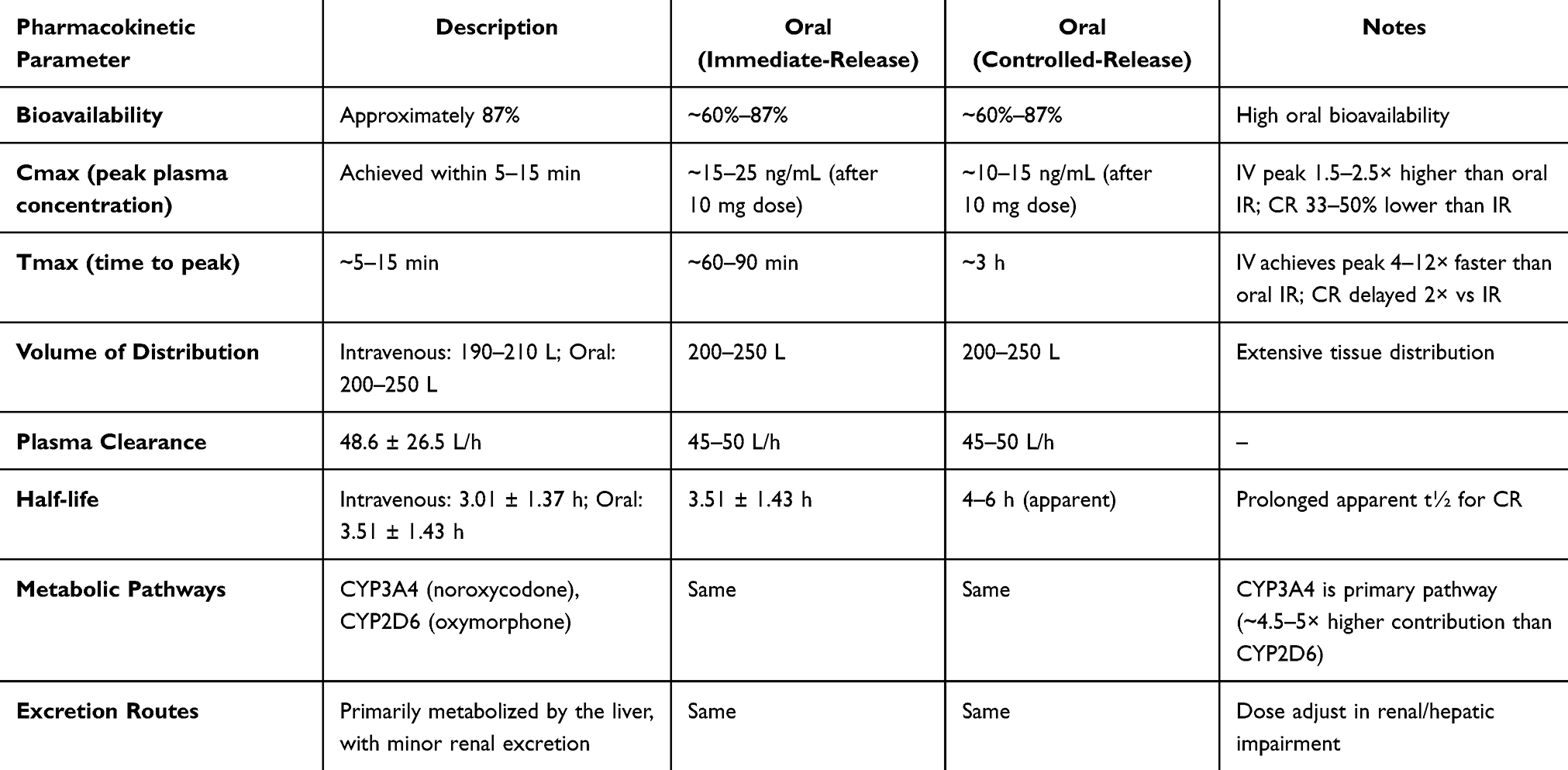 |
Table 1 Summary of Oxycodone Pharmacokinetic Parameters |
A recent population pharmacokinetic study demonstrated that in cancer patients, exposure to major oxycodone metabolites (eg., noroxycodone and noroxymorphone) varies according to CYP2D6 genotype; however, these metabolites contribute only 10–20% to the overall analgesic effect.22 For prodrug opioids that depend on CYP2D6 activation (particularly codeine and tramadol), dose escalation alone cannot compensate for deficient enzyme activity in CYP2D6 poor metabolizers (PMs); instead, it may compromise therapeutic outcomes due to inadequate analgesia coupled with increased adverse effects. Current evidence-based guidelines recommend switching such patients directly to opioids that do not rely on CYP2D6 metabolism (eg., morphine, hydromorphone, fentanyl) rather than simply increasing doses.23 For drugs only partially dependent on CYP2D6 metabolism (eg., oxycodone, hydrocodone), limited evidence suggests that increasing total doses or employing patient-controlled analgesia (PCA) may achieve comparable analgesic effects;24 however, the evidence remains limited with substantial interindividual variability. Currently, guidelines from both the Clinical Pharmacogenetics Implementation Consortium (CPIC) and the Dutch Pharmacogenetics Working Group (DPWG) conclude that existing evidence is insufficient to support CYP2D6 genotype-based dose adjustments for oxycodone, although they recommend considering alternative agents independent of CYP2D6 metabolism for patients with inadequate analgesia.25
Pharmacodynamics of Oxycodone in Cancer Patients
Oxycodone exerts its analgesic effects by agonizing μ-, κ-, and δ-opioid receptors in the spinal cord and brain.26 The signaling pathway mediated by the mu-opioid receptor (MOR) constitutes the core mechanism underlying oxycodone’s analgesic action, while κ-and δ-receptors may play auxiliary potentiating roles under specific circumstances, although their precise clinical significance remains to be elucidated.27 Upon MOR activation, the G protein complex (Gαβγ) dissociates. The Gα subunit (predominantly Gi/o subtypes) binds to GTP and inhibits adenylyl cyclase (AC) activity, resulting in decreased intracellular cyclic adenosine monophosphate (cAMP) levels. Meanwhile, the Gβγ dimer acts directly on ion channels to mediate membrane-associated signal transduction, particularly voltage-gated calcium channels and G protein-coupled inwardly rectifying potassium (GIRK) channels.27 Opening of GIRK channels increases potassium efflux, causing neuronal hyperpolarization and thereby reducing excitability. Concurrently, voltage-gated calcium channels are inhibited, reducing calcium influx and subsequently suppressing neurotransmitter release to block pain signal transmission.11 Thus, the direct analgesic action of oxycodone is primarily achieved through Gβγ subunit-mediated regulation of calcium and potassium ion channels (Figure 2).28 Additionally, MOR signaling has been reported to recruit specific signal transduction proteins via β-catenin, including Src kinase, phosphatidylinositol 3-kinase (PI3K), and mitogen-activated protein kinases (MAPKs, including ERK1/2 and JNK1–3), thereby participating in more complex signaling network regulation.29 However, the contribution of these pathways to analgesic effects is relatively minor, with the principal mechanism remaining centered on Gi/o-mediated ion channel modulation.
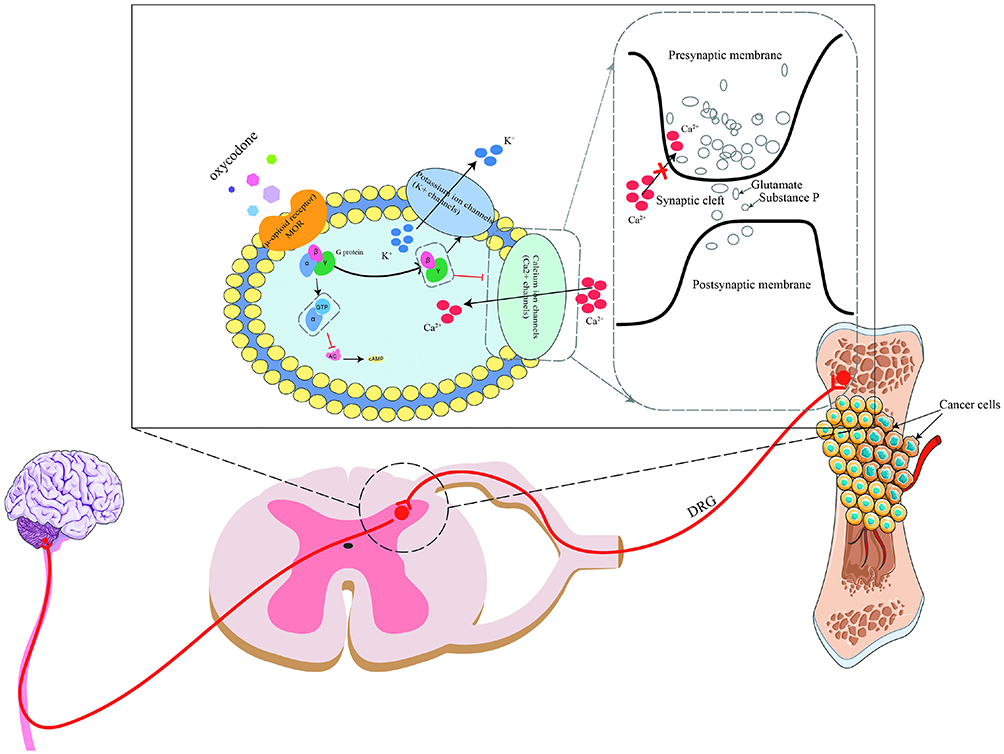 |
Figure 2 Mechanism by which oxycodone relieves pain through activation of μ-opioid receptors (MOR). |
Regarding clinical efficacy, oxycodone demonstrates analgesic effects comparable to morphine and hydromorphone in cancer patients.30 A meta-analysis revealed no significant difference in pain scores between oxycodone and morphine (P = 0.8).31 Compared with hydromorphone, oxycodone showed slightly lower pain scores, although the difference did not reach statistical significance. Studies indicate that oxycodone has a faster onset of action (approximately 1 hour for controlled-release formulations) compared to morphine, and its metabolism is more predictable, facilitating clinical dose titration.26
Concerning onset of action, a study by Leow et al32 conducted in 1995 demonstrated that intravenous oxycodone has an onset time of 5–8 minutes. This study evaluated PK and PD characteristics in 12 adult patients with moderate-to-severe cancer pain following single-dose intravenous and rectal administration. A comparative study in 2017 confirmed that the analgesic onset time for intravenous oxycodone is 2–3 minutes.33 Oral oxycodone has an onset time of 10–30 minutes, while controlled-release formulations require approximately 1 hour.32 Notably, although intravenous administration provides more rapid onset, it is associated with a relatively higher incidence of adverse effects.34 Other studies have failed to identify significant correlations between oxycodone plasma concentrations and pain scores or adverse effects, possibly attributable to limited sample sizes or data collection methodology constraints.35
Regarding genetic polymorphism, a multicenter study enrolling 450 cancer patients revealed that 6% were poor metabolizers (PMs), 92% were extensive metabolizers (EMs), and 2% were ultra-rapid metabolizers (URMs).15 Oxymorphone concentrations in the PM group (0.2 nM) were significantly lower than those in the EM group (1.6 nM) and URM group (2.3 nM) (P < 0.001). However, no significant differences were observed among the three groups in pain intensity, fatigue levels, nausea incidence, or cognitive function, further suggesting that oxymorphone contributes minimally to overall analgesic efficacy. Table 2 summarizes the pharmacodynamic characteristics of oxycodone.
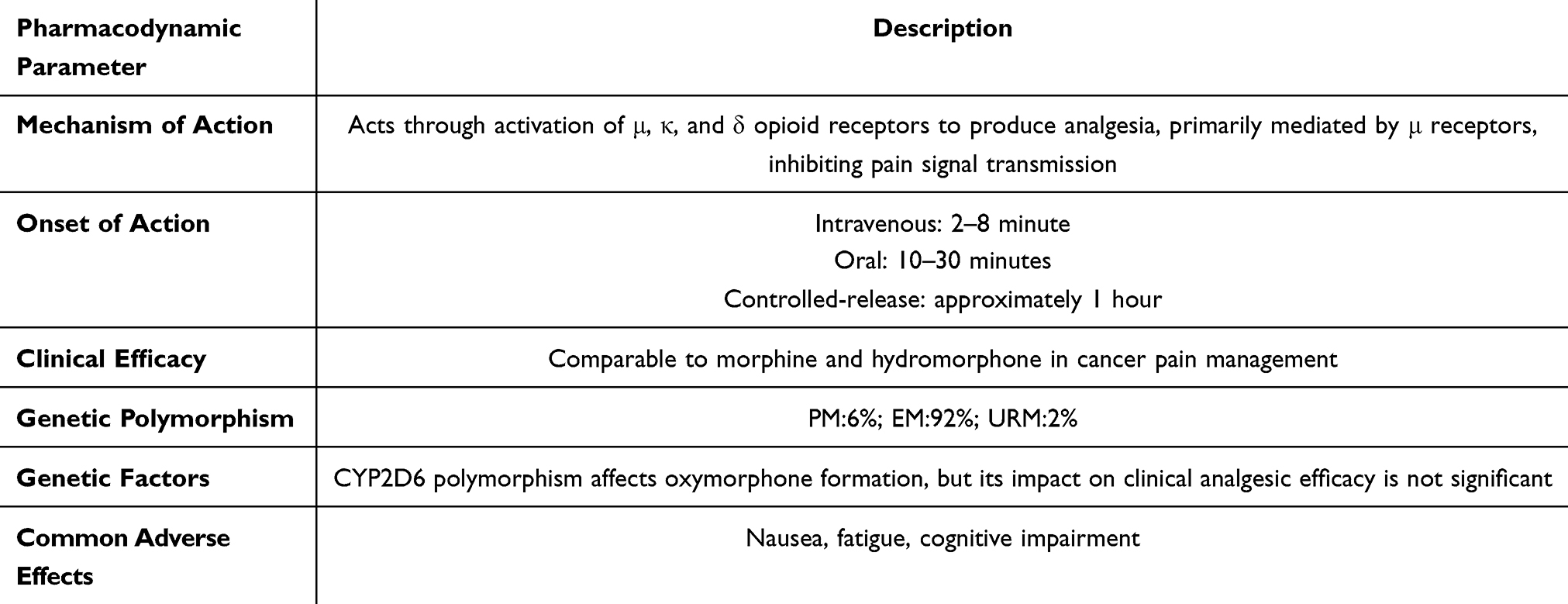 |
Table 2 Summary of Oxycodone Pharmacodynamic Parameters |
Regarding use in special populations, a recent review highlighted the pharmacodynamic characteristics of oxycodone in special populations such as pregnant women and pediatric cancer patients:36 the elimination half-life is prolonged by approximately 20% in pregnant patients, necessitating dose reduction to prevent neonatal withdrawal syndrome. Additionally, drug-drug interactions (DDIs) warrant attention: concomitant use with rifampicin (a CYP3A4 inducer) can reduce oxycodone’s analgesic efficacy by up to 50%. These findings support the adoption of individualized pharmacodynamic modeling strategies to optimize therapeutic outcomes in cancer patients.
Oxycodone Formulation Types and Clinical Application Strategies
Oxycodone is currently available in multiple formulation types, primarily including immediate-release (IR), extended-release/controlled-release (ER/CR), and combination products.6
Immediate-release (IR) formulations, encompassing oral solutions and conventional tablets, are primarily indicated for rapid relief of acute pain or breakthrough cancer pain. IR formulations have a rapid onset of action (10–30 minutes), provide analgesia lasting 3–6 hours, and are typically administered every 4–6 hours.37 Despite their relatively high oral bioavailability (60%–87%), the requirement for frequent dosing may increase the risk of drug abuse.38 In cancer pain management, IR formulations are commonly used for immediate control of breakthrough pain but are unsuitable as maintenance therapy for chronic pain.34
Extended-release/controlled-release (ER/CR) formulations (eg., OxyContin®) employ specialized drug-release technologies to provide stable plasma concentrations with twice-daily dosing, effectively minimizing peak-trough fluctuations. ER/CR formulations exhibit overall absorption rates similar to IR formulations but with more gradual drug release, making them suitable for maintenance therapy of chronic cancer pain.39 Studies have demonstrated no significant difference in analgesic efficacy between CR and IR formulations;40 however, CR formulations significantly improve patient adherence by reducing the inconvenience associated with frequent dosing.41
Combination products achieve synergistic efficacy with reduced toxicity by combining agents with different mechanisms of action. Common types include: (1) oxycodone/acetaminophen: enhances analgesic efficacy through combination with a non-opioid analgesic while reducing opioid requirements;37 (2) oxycodone/naloxone: naloxone blocks peripheral μ-receptors, effectively reducing gastrointestinal adverse effects such as constipation;42 and (3) oxycodone/naltrexone: naltrexone serves as an abuse-deterrent component to reduce abuse behaviors such as intranasal administration.43 In cancer patients, opioid combination products have been shown to reduce the incidence of opioid-related adverse effects, including a reduction in bowel obstruction risk, as supported by multiple studies.44 Table 3 provides a comparison of the characteristics of different oxycodone formulations.
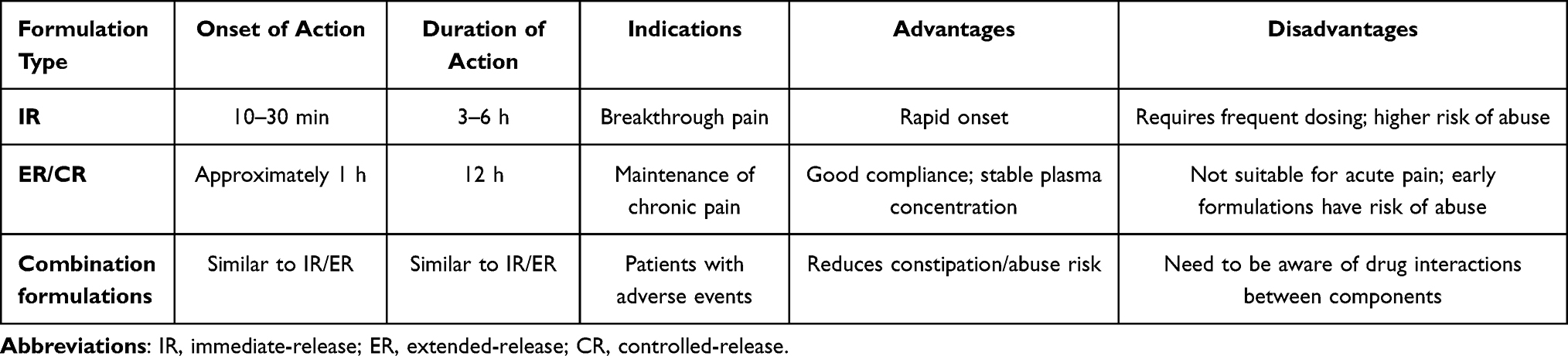 |
Table 3 Comparison of Oxycodone Formulations |
Regarding clinical application strategies, the American Society of Clinical Oncology (ASCO) and European Society for Medical Oncology (ESMO) guidelines recommend the following:45 (1) Initial therapy: titration with low-dose IR formulations (5–15 mg every 4 hours); (2) Maintenance therapy: once pain control is stabilized, conversion to ER formulations (administered every 12 hours, with each dose representing half the total daily dose); (3) Special populations: dose reduction of 25%–50% in patients with renal impairment; (4) Inadequate response: consideration of opioid rotation; and (5) Advanced-stage patients: preferential use of ER formulations to reduce caregiver burden, with IR formulations as supplemental analgesia for breakthrough pain episodes. These recommendations align with the WHO analgesic ladder framework, which provides the foundational three-step approach (non-opioid → weak opioid → strong opioid) that underpins cancer pain management internationally.46
Beyond standard oral and intravenous routes, novel delivery technologies have expanded options for patients with impaired oral absorption (eg., bowel obstruction, severe mucositis) or refractory pain. Transdermal oxycodone patches offer sustained, non-oral delivery suitable for patients with gastrointestinal dysfunction; subcutaneous infusion provides a flexible alternative for palliative care settings where intravenous access is impractical;47 and intrathecal oxycodone, while less established than intrathecal morphine, may be considered for selected cases of refractory cancer pain requiring high systemic doses.48,49 The integration of oxycodone within ERAS protocols also merits attention: oxycodone can be effectively combined with non-opioid analgesics (NSAIDs, gabapentinoids such as gabapentin and pregabalin), regional anesthesia (intercostal nerve block, epidural analgesia, transversus abdominis plane block), and non-pharmacological interventions (psychological support, physical therapy) as part of opioid-sparing multimodal strategies in cancer surgery.50
Regarding pharmacoeconomics, oxycodone’s overall cost profile compared with other opioids depends on formulation type, duration of use, and regional healthcare systems. In many settings, immediate-release oxycodone is cost-competitive with equivalent morphine formulations; however, controlled-release oxycodone (eg., OxyContin®) carries a higher acquisition cost, which may be offset by reduced adverse event management costs (eg., lower constipation burden with oxycodone/naloxone combinations) and improved adherence.51,52 In low- and middle-income countries (LMICs), availability and affordability are significant barriers: oxycodone is not universally included on national essential medicines lists, and regulatory restrictions on opioid prescribing limit access in parts of Asia, Africa, and South America.51 Prescribing practices also vary substantially by region: Asian countries (particularly China, Japan, and South Korea) have historically exhibited lower per-capita opioid consumption, partly due to regulatory constraints and cultural attitudes toward opioid use, while North American and European centers follow more liberal opioid prescribing frameworks.53 These disparities highlight the need for international policy advocacy alongside clinical guideline development.
Beyond objective pain metrics, patient-reported outcomes (PROs) represent an increasingly recognized dimension of analgesic effectiveness. Several studies included in this review assessed quality of life (QoL), physical function, sleep quality, and patient satisfaction, consistently demonstrating that oxycodone’s combination of effective analgesia and milder adverse effect profile contributes positively to overall PROs. However, standardized PRO instruments (such as the BPI, FACT-G, or PGIC) were not uniformly employed across studies, limiting cross-study comparability. Future trials should incorporate validated PRO measures as co-primary endpoints.54
However, substantial interindividual variability exists in clinical practice, and guideline recommendations cannot address all patients. Individualized treatment regimens require comprehensive consideration of each patient’s pain type, comorbidities, organ function, genetic background, and access to medications.
In summary, oxycodone possesses favorable pharmacokinetic characteristics and well-defined analgesic mechanisms, playing a significant role in cancer pain management. However, as an opioid analgesic, whether oxycodone exerts effects on tumor cells themselves beyond its actions on the nervous system remains an important—and as yet unresolved—question with implications for long-term medication safety in cancer patients. The following section systematically explores the potential effects of oxycodone on cancer cell biological behavior, tumor angiogenesis, and immune function.
Effects of Oxycodone on Tumor Cells and the Tumor Microenvironment
Oxycodone is an opioid analgesic widely used for the management of moderate-to-severe cancer pain. Recent studies have demonstrated that the effects of oxycodone extend beyond the nervous system, potentially directly influencing cancer cell biological behavior and exerting regulatory effects on the hematopoietic system and immune function.55,56 These findings have sparked academic interest and debate regarding whether long-term opioid use may affect tumor progression. The following sections systematically address three aspects: the direct effects of oxycodone on cancer cells, its impact on tumor angiogenesis, and its modulation of the immune system.
Oxycodone Exhibits Bidirectional Effects in Cancer Cells with Different EGFR Expression Levels
Critical note on concentration: All in vitro studies summarized in this section used oxycodone concentrations in the μM range (0.01–10 μM). Clinical therapeutic plasma concentrations of oxycodone are typically in the low nM range.57 The in vitro concentrations thus exceed physiological levels by approximately 100- to 1000-fold. Accordingly, the bidirectional effects described below should be interpreted as hypothesis-generating observations under supraphysiological conditions; they have not been validated by prospective clinical studies and are insufficient to alter current clinical guidelines.
Epidermal growth factor receptor (EGFR) expression levels vary significantly across different cancer cell types,58 and the effects of oxycodone on cancer cells may be associated with EGFR expression levels, potentially manifesting as either pro-tumorigenic or anti-tumorigenic effects under specific in vitro conditions. In cancer cells with high EGFR expression, oxycodone may demonstrate pro-tumorigenic effects. Using breast cancer MDA-468 cells as an example, Yu et al55 found that oxycodone at concentrations ranging from 0.01 to 10 μM (supraphysiological relative to clinical plasma levels) appeared to stimulate cell proliferation and migration without appreciably affecting cell survival. Further mechanistic investigation suggested that these effects may be mediated through activation of the EGFR/ERK/Akt signaling pathway and may depend on opioid receptor involvement. The opioid receptor antagonist naloxone (500 nM) reversed these stimulatory effects of oxycodone, suggesting that its actions may be associated with opioid receptor binding.59
In cancer cells with low EGFR expression, oxycodone may exhibit anti-tumorigenic effects under high-concentration conditions. In breast cancer SKBR3 cells and colon cancer Caco2 cells, Hu et al56 demonstrated that oxycodone (5 μM, approximately 100-fold above clinical plasma concentrations) appeared to inhibit cell growth and survival through induction of apoptosis and oxidative stress, without appreciably affecting cell migration. The apoptotic mechanism involves activation of caspase-8 and caspase-9, as well as elevated reactive oxygen species (ROS) levels.60 Oxycodone-induced oxidative stress may be mediated through the mitochondrial pathway and can be reversed by the pan-caspase inhibitor Z-VAD-fmk (50 μM)61 and the antioxidant N-acetylcysteine (NAC, 10 mM),62 but is unaffected by α-tocopherol (10 mM).63 Furthermore, under conditions of oxidative damage, Z-VAD-fmk and NAC can synergistically restore mitochondrial function and reduce cell death by inhibiting apoptosis and scavenging ROS, respectively.61
In hematopoietic stem/progenitor cells, oxycodone may exhibit pro-proliferative and pro-self-renewal effects.56 Studies suggest that oxycodone increases colony-forming capacity and self-renewal ability in both normal bone marrow (NBM) and acute myeloid leukemia (AML) stem/progenitor cells in a dose-dependent manner, while also promoting proliferation of AML somatic cells. Notably, normal bone marrow stem/progenitor cells appear to exhibit greater sensitivity to oxycodone than AML cells. Additionally, oxycodone may attenuate the cytotoxic effects of chemotherapeutic agents on AML stem/progenitor cells. These effects may be mediated through activation of the Wnt/β-catenin signaling pathway and are reportedly independent of opioid receptors. Table 4 summarizes the biological behaviors and associated signaling pathways of oxycodone across different cancer cell types, including the drug concentrations used in each study.
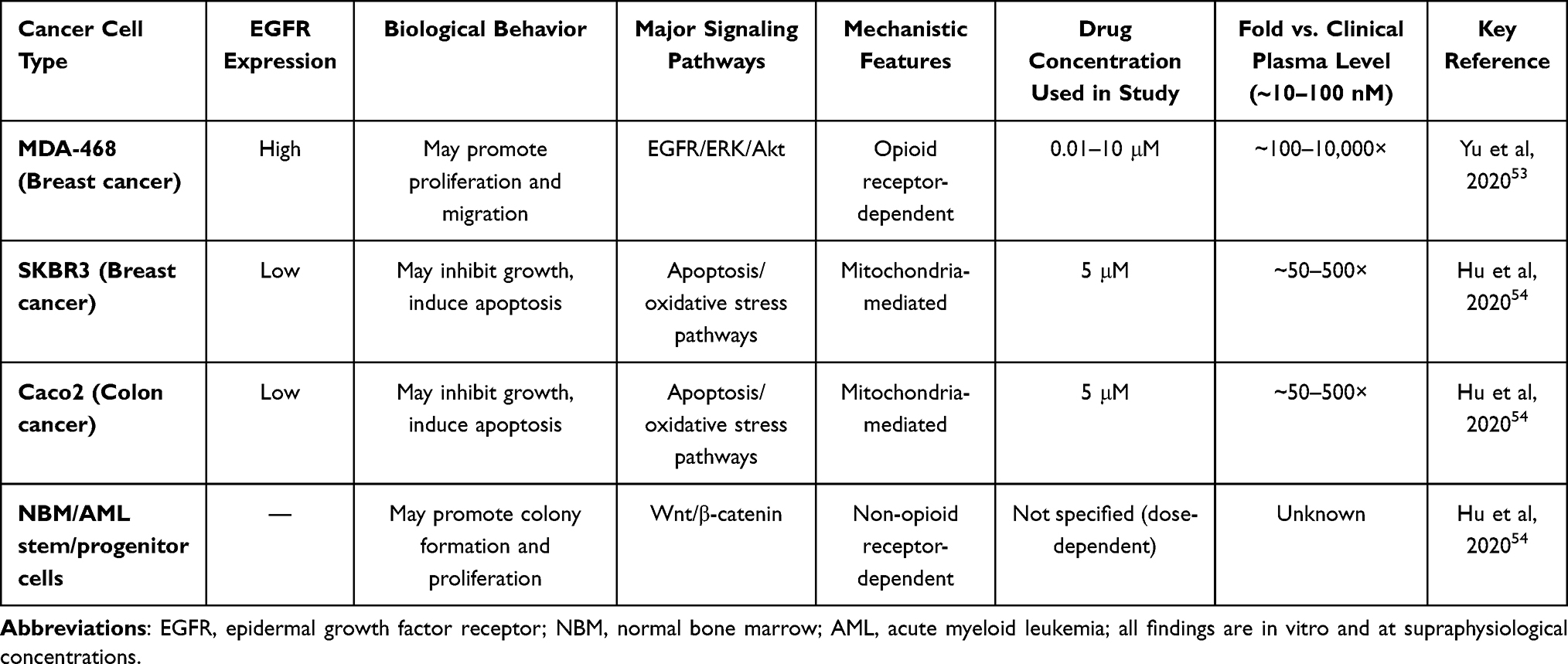 |
Table 4 Biological Behavior and Signaling Pathways of Oxycodone in Different Cancer Cell Types |
The interactions between oxycodone and chemotherapeutic agents also vary according to cancer cell type. In high EGFR-expressing MDA-468 cells, oxycodone (1 μM) attenuates the antitumor efficacy of paclitaxel (50 nM) and 5-fluorouracil (5-FU, 100 nM);55 conversely, in low EGFR-expressing SKBR364 and Caco265 cells, oxycodone enhances the anticancer effects of these chemotherapeutic agents. This bidirectional modulatory effect suggests that comprehensive evaluation of oxycodone’s potential impact on chemotherapy efficacy is warranted in clinical practice.
Regarding the potential pro-tumorigenic risks of opioids, in vitro experiments and animal model studies have demonstrated that oxycodone may promote tumor growth and metastasis through μ-receptor-mediated mechanisms, including promotion of angiogenesis, induction of immunosuppression, and metabolic reprogramming (such as elevated ROS levels). For instance, Opioids have been shown in some studies to potentially promote tumor growth.66 However, clinical evidence remains inconsistent: some retrospective studies (eg., a 2020 study) demonstrated that long-term opioid use increases cancer recurrence risk (HR = 1.5), particularly in breast cancer patients;67 yet other meta-analyses have failed to identify significant associations, suggesting that such findings may be confounded by factors such as pain severity.68 A 2023 pan-cancer analysis indicated that tumors overexpressing the μ-opioid receptor (MOR) have poorer prognosis and exhibit diminished response to PD-L1 immunotherapy;69 however, validation through prospective randomized controlled trials is still lacking. Based on the totality of current evidence, short-term oxycodone use (<3 months) carries relatively low safety risks;45 for long-term use, however, careful weighing of analgesic benefits against potential risks is warranted, with active consideration of non-opioid alternative therapeutic approaches.
Oxycodone Exerts Dual Effects on Tumor Angiogenesis
Tumor angiogenesis is an essential prerequisite for tumor growth and metastasis.70,71 Regarding the effects of oxycodone on angiogenesis, existing studies have yielded contradictory results, suggesting that its actions may be dose- and tumor type-dependent. With respect to angiogenesis inhibition, Tian et al72 demonstrated that oxycodone at a concentration of 40 μg/mL (approximately 127 μM) significantly reduced vascular endothelial growth factor (VEGF) expression levels in A549 lung cancer cells. Compared with morphine, oxycodone also decreased the expression of urokinase-type plasminogen activator (uPA) and intercellular adhesion molecule-1 (ICAM-1) in A549 cells, suggesting that oxycodone may possess superior anti-angiogenic properties compared to morphine. Regarding angiogenesis promotion, Feng et al73 found that oxycodone at doses ranging from 0.1 to 100 μM promoted endothelial cell tube formation and proliferation in a dose-dependent manner. Although this study observed increased mitogen-activated protein kinase (MAPK) phosphorylation levels in both morphine- and oxycodone-treated cells, rescue experiments demonstrated that only the pro-angiogenic effects of morphine could be reversed by specific MAPK inhibitors, while those of oxycodone remained unaffected. These findings carry important mechanistic implications: despite both morphine and oxycodone being opioid analgesics capable of activating the MAPK pathway, their regulatory mechanisms governing angiogenesis are not entirely identical. Morphine’s promotion of angiogenesis directly depends on the MAPK pathway, with MAPK activation serving as its core mechanistic component.74,75 In contrast, the mechanism of action of oxycodone requires further elucidation, with current studies suggesting potential involvement of signaling pathways other than MAPK.76,77
Regarding possible explanations for these dual effects, the bidirectional regulation of angiogenesis by oxycodone may be related to drug concentration and tumor type: at low concentrations, it tends to inhibit VEGF expression, whereas at high concentrations, it may activate endothelial cell proliferation.55,78 Some animal studies suggest that oxycodone may indirectly influence neuroinflammatory responses through immunomodulatory or metabolic pathways;79 however, there is currently no direct evidence demonstrating that it promotes tumor metastasis in animal models, and human studies are even more lacking.
Based on the above evidence, to minimize the risks of drug abuse and dependence in clinical practice, low-dose controlled-release oxycodone (ER formulations) is recommended as the preferred initial treatment strategy.80 This approach may also help circumvent the potential pro-angiogenic risks associated with high doses.
Differential Effects of Oxycodone and Morphine on Immune Function in Cancer Patients
Immune function status significantly influences prognosis in cancer patients. The immunomodulatory effects of opioid analgesics have garnered increasing attention, and differences in immunomodulatory effects may exist among different opioid agents.
Regarding comparison of immunosuppressive effects between oxycodone and morphine, a study by Cui et al81 in patients undergoing radical colorectal cancer surgery demonstrated that postoperative administration of either oxycodone or morphine resulted in decreased CD4⁺T cell, CD8⁺T cell, and natural killer (NK) cell counts in both groups; however, the oxycodone group exhibited significantly higher counts of these cell populations at all observation time points compared to the morphine group, suggesting that oxycodone exerts relatively milder immunosuppressive effects. Research by Wodehouse et al82 utilizing gene expression profiling further confirmed that compared with morphine, oxycodone produces less immunosuppression of CD4⁺, CD8⁺ T cells, and NK cells in the early postoperative period, with cytokine expression profile analysis similarly supporting the relative immunoprotective properties of oxycodone. Regarding infection risk with long-term use, a retrospective study by Suzuki et al83 found that cancer pain patients receiving long-term morphine therapy had significantly higher infection rates compared to those receiving oxycodone (OR = 3.60), suggesting that the stronger immunosuppressive effects of morphine may contribute to elevated infection risk. In a systematic review, Li et al9 summarized the immunomodulatory mechanisms of opioid analgesics, noting that morphine produces potent immunosuppressive effects through μ-receptor and Toll-like receptor 4 (TLR4) pathways, whereas oxycodone exhibits relatively weaker immunosuppressive activity. In summary, current evidence consistently indicates that compared with morphine, oxycodone produces milder immunosuppressive effects during perioperative analgesia in cancer patients, conferring certain immunoprotective advantages. This characteristic holds important clinical implications for cancer patients whose immune function is already compromised.
Regarding the anti-inflammatory effects of oxycodone, recent studies have revealed that oxycodone possesses significant anti-inflammatory properties, capable of downregulating the expression of inflammatory mediators such as interleukin-6 (IL-6), with some mechanisms potentially operating independently of the classical TLR4 pathway. For example, Tan et al84 demonstrated that oxycodone can suppress neuroinflammatory responses through the CREB/miR-181c/PDCD4 axis; Wang et al85 found that oxycodone can attenuate myocardial inflammatory injury by activating the Nrf2/HO-1 signaling pathway. In immunocompromised patients, the anti-inflammatory effects of oxycodone may confer protective benefits; however, it should be noted that long-term use may still increase infection risk, necessitating comprehensive evaluation in clinical applications.
Clinical Evidence for Postoperative Oxycodone Use in Cancer Patients
The aforementioned basic research has revealed the multiple effects of oxycodone on tumor cells and the tumor microenvironment at cellular and molecular levels, providing important references for rational clinical drug use. However, conclusions from basic research require validation through clinical evidence. The following section systematically reviews clinical studies on oxycodone use in postoperative acute pain management across different cancer types, providing an evidence base for clinical practice.
Postoperative Analgesia in Breast Cancer
Regarding oxycodone use for postoperative analgesia in breast cancer, Kampe et al86 conducted a prospective, randomized, double-blind, placebo-controlled study. This study enrolled 40 female patients (ASA I–III) undergoing breast cancer surgery, employing controlled-release oxycodone 20 mg every 12 hours. Results demonstrated that compared with the placebo group, the oxycodone group had significantly lower intravenous PCA opioid consumption (P = 0.01), required smaller intravenous opioid loading doses (P < 0.001), and exhibited significantly lower area under the curve for VAS scores at rest (P = 0.05). Notably, there was no significant difference in nausea incidence between groups (P = 0.34), suggesting that perioperative prophylactic oral controlled-release oxycodone can effectively improve postoperative pain control without increasing the risk of gastrointestinal adverse effects.86
Clinical Studies on Postoperative Oxycodone Use in Colorectal Cancer
Multiple randomized controlled trials have evaluated the efficacy of oxycodone for postoperative analgesia in colorectal cancer surgery. Yang et al87 randomized 40 patients undergoing laparoscopic colorectal cancer resection to receive either oxycodone or sufentanil for PCIA, finding that VAS scores during coughing in the oxycodone group were significantly lower than in the sufentanil group at 24 and 72 hours postoperatively (P < 0.001), while VAS scores at rest showed no significant difference between groups. Studies by Han et al88 and Wan et al89 further confirmed that oxycodone provides non-inferior analgesic efficacy compared to sufentanil for postoperative colorectal cancer surgery, with certain advantages in time to consciousness recovery, incidence of respiratory depression, and immune function preservation. Collectively, these studies indicate that oxycodone used for postoperative PCIA in colorectal cancer surgery provides excellent dynamic analgesia, making it particularly suitable for enhanced recovery after surgery (ERAS) protocols requiring early ambulation.
Clinical Studies on Postoperative Oxycodone Use in Gastric Cancer
For elderly gastric cancer patients, Lao et al90 conducted a randomized controlled trial comparing oxycodone (0.1 mg/kg) versus sufentanil (0.1 μg/kg) combined with parecoxib for postoperative analgesia following laparoscopic gastrectomy. This study enrolled 60 patients aged 65 years and older, demonstrating that the oxycodone group had lower visceral pain NRS scores at all observation time points compared to the sufentanil group, with incisional pain scores also lower at 6 and 24 hours postoperatively. Additionally, the oxycodone group exhibited lower incidence of postoperative nausea and vomiting, and changes in inflammatory cytokine levels (IL-6, IL-10) suggested superior anti-inflammatory effects. These results indicate that oxycodone may be superior to sufentanil in alleviating postoperative visceral pain, consistent with its pharmacological properties as a κ-receptor agonist.
Clinical Studies on Postoperative Oxycodone Use in Lung Cancer
Lung cancer surgery involves substantial surgical trauma, making postoperative pain management crucial for patient recovery. A retrospective analysis by Wang et al91 enrolled 135 elderly patients undergoing radical lung cancer resection to evaluate the effects of intercostal nerve block (INB) combined with oxycodone on postoperative cognitive function. Results showed that the combination therapy group had significantly higher postoperative MMSE scores compared to controls, with lower adverse event rates and VAS scores, and higher postoperative analgesia satisfaction rates. Studies by Cheng et al,92 Sun et al,93 and Zhang et al94 further confirmed that oxycodone effectively reduces inflammatory cytokine release, attenuates stress responses, and protects cognitive function following lung cancer surgery (see Table 5). These findings suggest that oxycodone combined with regional block techniques may be the preferred postoperative analgesic regimen for elderly lung cancer patients, particularly for those at high risk of postoperative delirium.
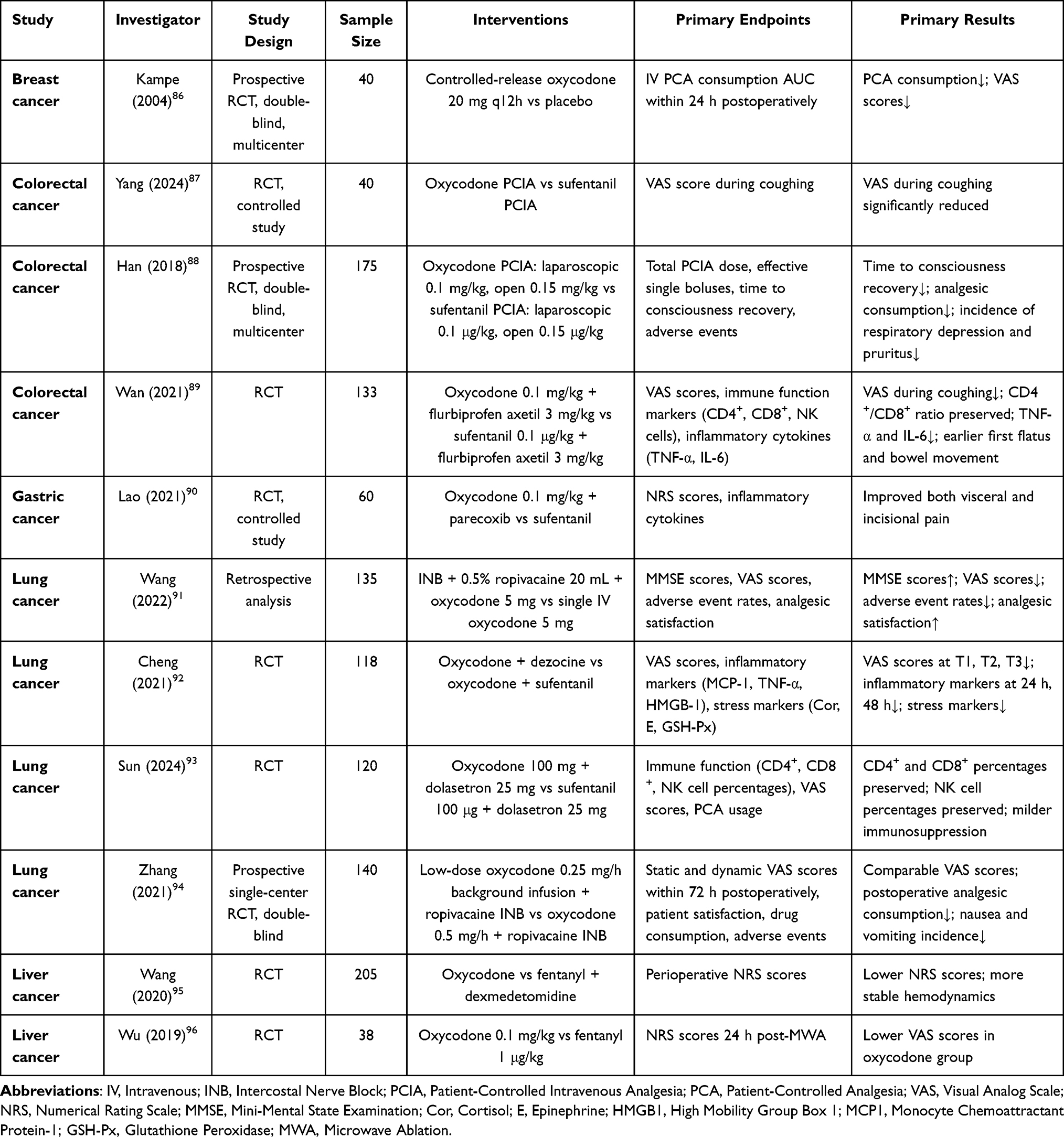 |
Table 5 Summary of Clinical Studies on the Use of Oxycodone Following Cancer Surgery |
Clinical Studies on Postoperative Oxycodone Use in Liver Cancer
Interventional treatments for liver cancer require patients to maintain spontaneous respiration and hemodynamic stability, imposing specific requirements for analgesic drug selection. Wang et al95 compared oxycodone with fentanyl during percutaneous radiofrequency ablation for liver cancer, demonstrating that the oxycodone group had lower intraoperative and postoperative NRS scores, smaller heart rate fluctuations, and significantly lower incidences of respiratory depression and adverse limb movements compared to the fentanyl group. A study by Wu et al96 similarly showed that oxycodone provides superior analgesia for hepatic microwave ablation, reduces postoperative opioid rescue requirements, and maintains more stable hemodynamics. This evidence supports oxycodone as the preferred analgesic for interventional liver cancer treatments.
Cross-Cancer Synthesis and Limitations of Oxycodone in Chronic Cancer Pain Management
A cross-cancer comparison of the clinical evidence reveals important distinctions in how oxycodone performs across surgical contexts. When comparing colorectal and lung cancer surgical settings—the two cancer types with the largest evidence base in this review—oxycodone’s advantages are complementary but distinct. In colorectal cancer surgery, three RCTs consistently demonstrated superior visceral pain control (particularly during dynamic activities such as coughing), faster gastrointestinal recovery, and immunoprotective effects, consistent with oxycodone’s κ-receptor activity.97 In lung cancer surgery, the dominant benefit shifts toward cognitive protection and attenuation of the neuroinflammatory response associated with major thoracic trauma, where oxycodone combined with regional anesthesia (intercostal nerve block) produced the most robust effects.98 For gastric cancer, oxycodone’s κ-receptor agonism similarly underpins its visceral pain advantage, with anti-inflammatory cytokine modulation as an additional benefit in elderly patients.99 For hepatic ablation procedures, the defining advantage is hemodynamic stability and minimal respiratory depression, which are critical for patients who must maintain spontaneous ventilation during interventional procedures.100 For breast cancer, the primary benefit is a reduction in overall opioid consumption during the perioperative period, consistent with the less visceral character of the pain.101 The clinical evidence largely derives from Asian (predominantly Chinese) single- and multi-center RCTs; additional studies from diverse geographical regions would be required to confirm generalizability across healthcare systems with different patient populations, surgical practices, and co-analgesic protocols.102 A comparison of oxycodone application characteristics across cancer types is summarized in Table 6.
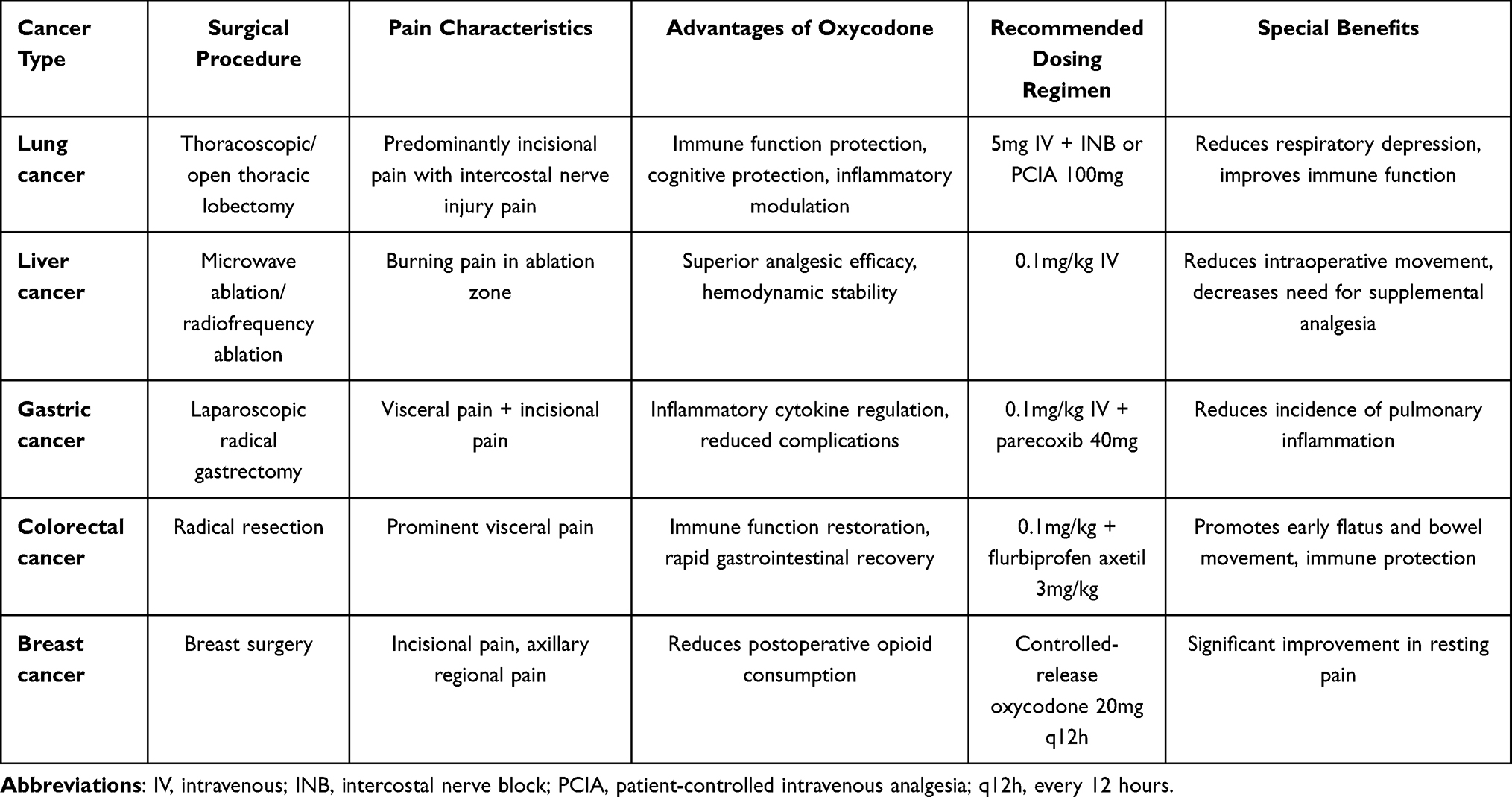 |
Table 6 Comparison of Oxycodone Application Characteristics in Different Cancer Types |
Unlike postoperative acute pain, the management of chronic cancer pain (particularly neuropathic cancer pain) is more complex, and opioids such as oxycodone alone often fail to achieve satisfactory pain relief. In clinical practice, adjuvant analgesics (such as gabapentin, pregabalin, and methadone) are frequently required in combination to achieve optimal analgesia.103 For persistent cancer pain associated with bone metastases, oxycodone provides analgesic efficacy comparable to morphine and other potent opioids and can serve as a first-line treatment option. However, for breakthrough cancer pain, the efficacy of oxycodone is relatively limited; such pain typically requires rapid-onset formulations or transmucosal delivery routes (such as transmucosal immediate-release fentanyl) for control.104 Furthermore, long-term oxycodone use may lead to drug tolerance and opioid-induced hyperalgesia (OIH),105 further limiting its long-term utility in chronic cancer pain. For patients with refractory cancer pain, multimodal analgesia strategies are recommended, incorporating opioid rotation, adjuvant analgesics, interventional treatments (such as nerve blocks and intrathecal drug delivery), and non-pharmacological approaches (such as psychological interventions and physical therapy) within an interdisciplinary comprehensive management framework. A summary comparison of oxycodone with other opioid analgesics across included studies is presented in Table 7.
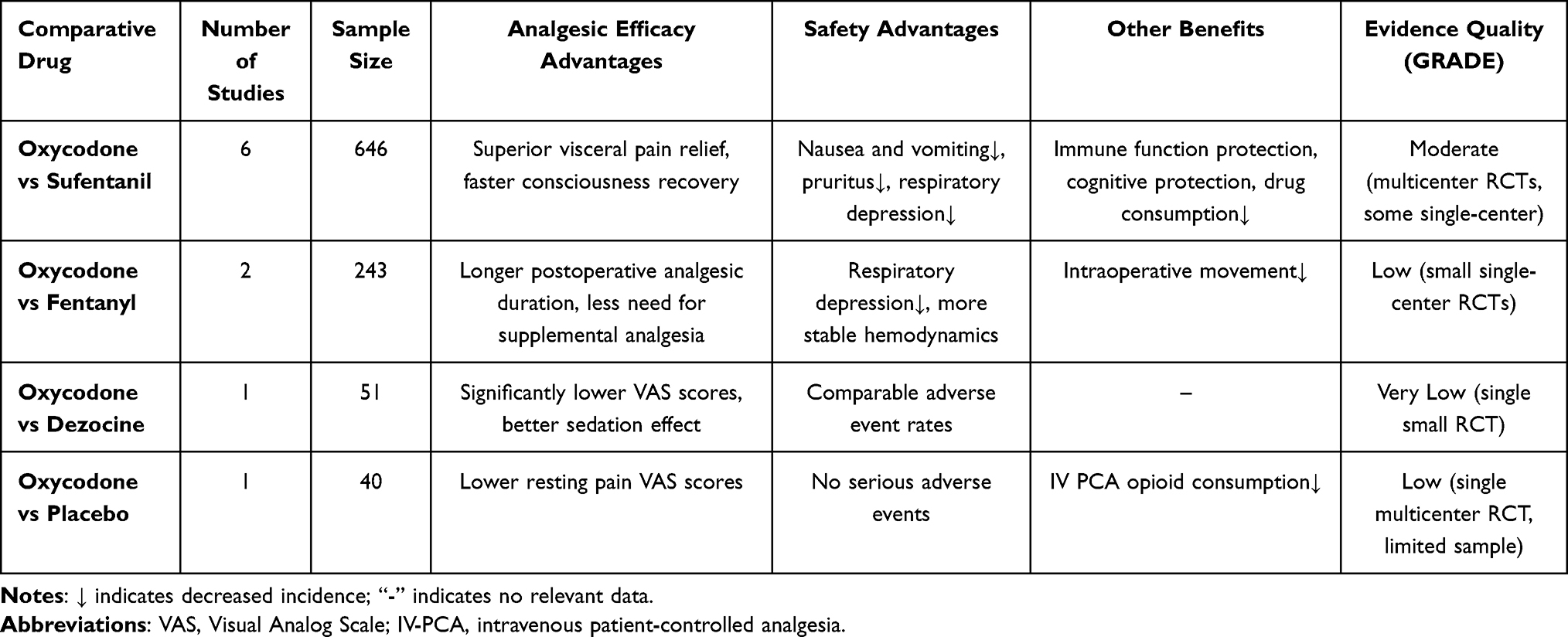 |
Table 7 Summary Comparison of Oxycodone with Other Opioid Analgesics |
In summary, oxycodone has accumulated substantial evidence for postoperative acute pain management in cancer patients, demonstrating favorable analgesic efficacy and safety profiles across various cancer surgeries. However, its application in chronic cancer pain management has limitations, necessitating integration with multimodal analgesia strategies and individualized treatment plans. With the development of novel analgesics and drug delivery systems, options for cancer pain management will continue to expand.
Discussion
This review systematically examines the pharmacological foundation, tumor biological effects, and clinical evidence for oxycodone in cancer pain management. Comprehensive analysis indicates that the clinical value of oxycodone extends beyond reliable analgesic efficacy to encompass potential advantages conferred by its unique pharmacological properties.
κ-receptor agonism confers advantages in visceral pain relief. Unlike morphine and fentanyl, oxycodone demonstrates κ-receptor agonist activity in animal models. This pharmacological characteristic may explain its superior performance in postoperative analgesia following gastrointestinal surgery: three RCTs in colorectal cancer and one in gastric cancer consistently demonstrated that oxycodone groups exhibited significantly lower visceral pain scores compared to sufentanil groups, with this advantage being particularly pronounced during dynamic activities such as coughing and turning. For patients undergoing abdominal tumor surgery, especially radical resections involving extensive visceral manipulation, oxycodone may represent a more rational analgesic choice. However, the precise contribution of κ-receptors in humans remains unclear, as existing evidence derives primarily from animal studies, and its clinical translational value warrants further validation.
Immune-protective properties have potential clinical significance. Six RCTs encompassing 646 patients demonstrated that compared with sufentanil or morphine, oxycodone exerted less suppression on CD4⁺T cells, CD8⁺T cells, and NK cells. This finding holds potential importance for cancer patients whose immune function is already compromised. Preservation of immune surveillance may help reduce postoperative infection risk and maintain antitumor immunity, although no studies have directly confirmed that oxycodone’s immune-protective effects translate into improved clinical outcomes (such as reduced infection rates or survival benefits). This hypothesis merits verification in future prospective studies.
Clinical impact of CYP2D6 genetic polymorphism is limited. Although CYP2D6 genotype significantly affects plasma concentrations of the active metabolite oxymorphone, multicenter studies indicate no significant differences in analgesic efficacy or adverse event rates among patients with different genotypes. This finding challenges the traditional concept of adjusting oxycodone dosing based on CYP2D6 genotype, suggesting that oxycodone’s analgesic action is primarily mediated by the parent compound, with limited contribution from metabolites (approximately 10–20%). Therefore, for patients with inadequate analgesia, opioid rotation may be more reasonable than simple dose escalation.
Regarding the bidirectional effects of oxycodone on tumor cells. The in vitro studies compiled in this review reveal a noteworthy phenomenon: oxycodone may promote proliferation in cancer cells with high EGFR expression while inducing apoptosis in those with low EGFR expression under supraphysiological concentration conditions. This finding mechanistically suggests that tumor molecular characteristics may influence the biological effects of opioid analgesics. However, direct extrapolation of these laboratory findings to clinical practice requires extreme caution for the following reasons.
First, and most critically, drug concentrations used in in vitro studies (0.01–10 μM) far exceed clinical therapeutic plasma concentrations (approximately 10–100 nM), a discrepancy of up to 1000-fold. This raises a fundamental question as to whether the bidirectional regulatory effects described could meaningfully occur in the human physiological environment. The lack of evidence for such effects at physiologically relevant concentrations constitutes a major limitation of the current preclinical data. Second, intratumoral EGFR expression exhibits significant spatiotemporal heterogeneity, and a single molecular marker may be insufficient to predict complex in vivo effects. Third, no prospective clinical studies have confirmed a causal association between oxycodone use and tumor progression or recurrence. Based on current evidence, the EGFR-dependent bidirectional effects of oxycodone have been observed only in high-concentration laboratory settings, remain unvalidated by clinical prospective studies, and are insufficient to alter current clinical guidelines for cancer pain management. We do not recommend using tumor EGFR status as a criterion for selecting analgesic medications.
Regarding pro-carcinogenic risks of opioid analgesics. This longstanding controversy remains unresolved. Some retrospective studies have reported associations between long-term opioid use and increased cancer recurrence risk, but these observational studies suffer from insurmountable confounding bias: patients requiring higher opioid doses often have more severe illness, more intense pain, and greater tumor burden—factors that are themselves predictors of poor prognosis. To date, no prospective randomized controlled trials have directly evaluated the impact of opioid selection on cancer outcomes.
Synthesizing available data, we conclude that: evidence adequately supports the safety of short-term oxycodone use (<3 months) for acute cancer pain management; for patients requiring long-term opioid therapy, multimodal analgesic strategies should be employed to minimize opioid exposure, accompanied by individualized risk-benefit assessment.
Conclusion
Oxycodone has earned substantial evidence-based support for postoperative acute cancer pain management. Its κ-receptor agonist activity confers advantages in visceral pain relief, its milder immunosuppressive profile benefits immunocompromised patients, and the limited clinical impact of CYP2D6 polymorphism simplifies prescribing decisions.
The bidirectional effects of oxycodone on tumor cells—observed only in high-concentration in vitro settings (0.01–10 µM), far exceeding clinical plasma concentrations (nM range)—should not influence analgesic selection. Current evidence does not support using tumor EGFR status to guide opioid choice, and short-term use (<3 months) is supported as safe; oncological implications of long-term use require prospective clarification.
For chronic cancer pain, oxycodone monotherapy shows limited efficacy against neuropathic and bone metastasis pain.57,106 It should be integrated within multimodal strategies—aligned with the WHO analgesic ladder—combining NSAIDs, gabapentinoids, regional anesthesia, novel delivery modalities, and non-pharmacological interventions.107,108 Future trials should incorporate standardized patient-reported outcomes and pharmacogenomic stratification across diverse global populations.
To assist practitioners in translating the above evidence into daily clinical decisions, concise scenario-specific recommendations are provided in Table 8.
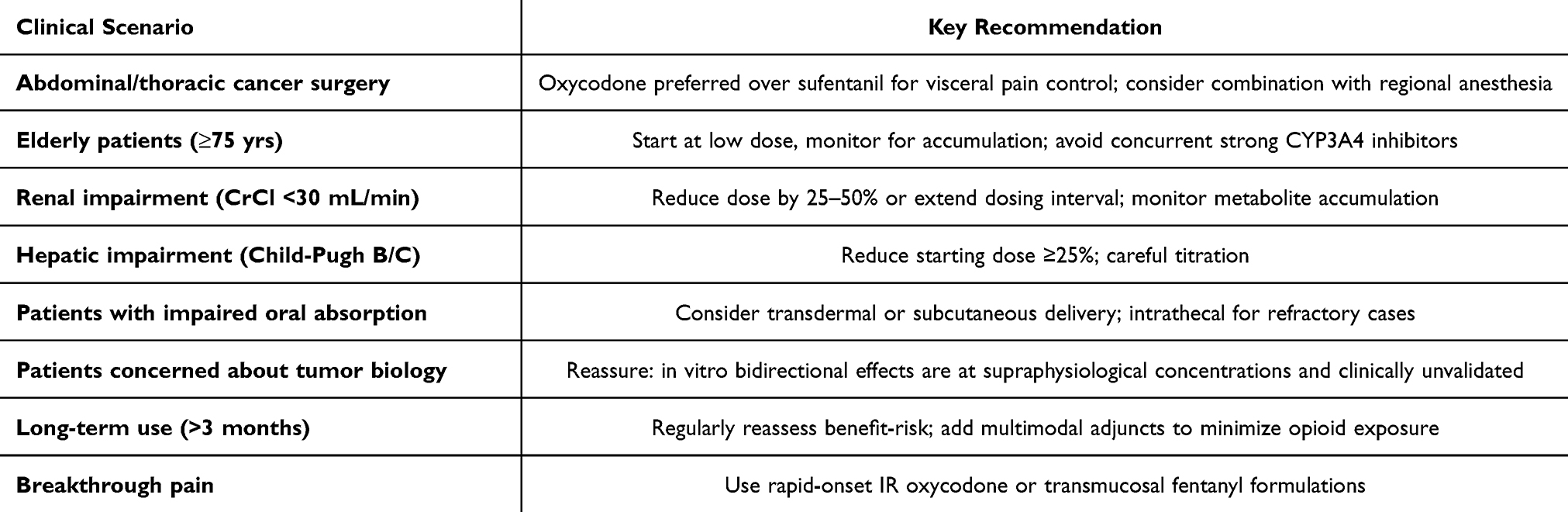 |
Table 8 Clinical Recommendations for Oxycodone Use in Cancer Pain Management |
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Wang WL, Hao YH, Pang X, Tang YL. Cancer pain: molecular mechanisms and management. Mol Biomed. 2025;6(1):45. doi:10.1186/s43556-025-00289-0
2. Snijders RAH, Brom L, Theunissen M, van den Beuken-van Everdingen MHJ. Update on Prevalence of Pain in Patients with Cancer 2022: a Systematic Literature Review and Meta-Analysis. Cancers. 2023;15(3). doi:10.3390/cancers15030591
3. Breivik H, Cherny N, Collett B, et al. Cancer-related pain: a pan-European survey of prevalence, treatment, and patient attitudes. Ann Oncol. 2009;20(8):1420–19. doi:10.1093/annonc/mdp001
4. Ziegler L, Mulvey M, Blenkinsopp A, Petty D, Bennett MI. Opioid prescribing for patients with cancer in the last year of life: a longitudinal population cohort study. Pain. 2016;157(11):2445–2451. doi:10.1097/j.pain.0000000000000656
5. Brefel-Courbon C, Harroch E, Marques A, et al. Oxycodone or Higher Dose of Levodopa for the Treatment of Parkinsonian Central Pain: OXYDOPA Trial. Mov Disord. 2024;39(9):1533–1543. doi:10.1002/mds.29878
6. Kalso E. Oxycodone. Reactions Weekly. 2023;1944(1):464. doi:10.1007/s40278-023-33983-4
7. Riley J, Eisenberg E, Muller-Schwefe G, Drewes AM, Arendt-Nielsen L. Oxycodone: a review of its use in the management of pain. Curr Med Res Opin. 2008;24(1):175–192. doi:10.1185/030079908X253708
8. Thibault K, Calvino B, Rivals I, et al. Molecular mechanisms underlying the enhanced analgesic effect of oxycodone compared to morphine in chemotherapy-induced neuropathic pain. PLoS One. 2014;9(3):e91297. doi:10.1371/journal.pone.0091297
9. Li Y, Sun L, Zhou Q, et al. Effects of opioid drugs on immune function in cancer patients. Biomed Pharmacother. 2024;175:116665. doi:10.1016/j.biopha.2024.116665
10. Leow KP, Smith MT, Williams B, Cramond T. Single-dose and steady-state pharmacokinetics and pharmacodynamics of oxycodone in patients with cancer. Clin Pharmacol Ther. 1992;52(5):487–495. doi:10.1038/clpt.1992.176
11. Berecki G, Motin L, Adams DJ. Voltage-Gated R-Type Calcium Channel Inhibition via Human mu-, delta-, and kappa-opioid Receptors Is Voltage-Independently Mediated by Gbetagamma Protein Subunits. Mol Pharmacol. 2016;89(1):187–196. doi:10.1124/mol.115.101154
12. Komatsu T, Kokubun H, Suzuki A, et al. Population Pharmacokinetics of Oxycodone in Patients With Cancer-Related Pain. J Pain Palliative Care Pharmacother. 2012;26(3):220–225. doi:10.3109/15360288.2012.702200
13. Kane M. Oxycodone Therapy and CYP2D6 Genotype. In: Pratt VM, Scott SA, Pirmohamed M, Esquivel B, Kattman BL, Malheiro AJ, editors. Medical Genetics Summaries. Bethesda (MD): National Center for Biotechnology Information (US); 2012.
14. DePriest AZ, Puet BL, Holt AC, Roberts A, Cone EJ. Metabolism and Disposition of Prescription Opioids: a Review. Forensic Sci Rev. 2015;27(2):115–145.
15. Andreassen TN, Eftedal I, Klepstad P, et al. Do CYP2D6 genotypes reflect oxycodone requirements for cancer patients treated for cancer pain? A cross-sectional multicentre study. Eur J Clin Pharmacol. 2012;68(1):55–64. doi:10.1007/s00228-011-1093-5
16. Gronlund J, Saari TI, Hagelberg NM, Neuvonen PJ, Olkkola KT, Laine K. Exposure to oral oxycodone is increased by concomitant inhibition of CYP2D6 and 3A4 pathways, but not by inhibition of CYP2D6 alone. Br J Clin Pharmacol. 2010;70(1):78–87. doi:10.1111/j.1365-2125.2010.03653.x
17. Liu S, Sands MB, Kerferd JW, et al. Opioid Analgesic Use among Patients with Kidney Disease: a Systematic Review. Kidney Blood Press Res. 2024;49(1):495–512. doi:10.1159/000538258
18. Gronich N. Central Nervous System Medications: pharmacokinetic and Pharmacodynamic Considerations for Older Adults. Drugs Aging. 2024;41(6):507–519. doi:10.1007/s40266-024-01117-w
19. Thakir TM, Wang AR, Decker-Farrell AR, et al. Cancer therapy and cachexia. J Clin Invest. 2025;135(15). doi:10.1172/JCI191934.
20. Salau VF, Erukainure OL, Olofinsan KA, Schoeman RLS, Matsabisa MG. Lippia javanica (Burm. F.) Herbal Tea: modulation of Hepatoprotective Effects in Chang Liver Cells via Mitigation of Redox Imbalance and Modulation of Perturbed Metabolic Activities. Front Pharmacol. 2023;14:1221769. doi:10.3389/fphar.2023.1221769
21. Lehmann A, Geburek I, Hessel-Pras S, et al. PBTK model-based analysis of CYP3A4 induction and the toxicokinetics of the pyrrolizidine alkaloid retrorsine in man. Arch Toxicol. 2024;98(6):1757–1769. doi:10.1007/s00204-024-03698-2
22. Agema BC, Oosten AW, Sassen SDT, et al. Population Pharmacokinetics of Oxycodone and Metabolites in Patients with Cancer-Related Pain. Cancers. 2021;13(11):2768. doi:10.3390/cancers13112768
23. Dowell D, Ragan KR, Jones CM, Baldwin GT, Chou R. CDC Clinical Practice Guideline for Prescribing Opioids for Pain - United States, 2022. MMWR Recomm Rep. 2022;71(3):1–95. doi:10.15585/mmwr.rr7103a1
24. Stamer UM, Zhang L, Book M, Lehmann LE, Stuber F, Musshoff F. CYP2D6 genotype dependent oxycodone metabolism in postoperative patients. PLoS One. 2013;8(3):e60239. doi:10.1371/journal.pone.0060239
25. Crews KR, Monte AA, Huddart R, et al. Clinical Pharmacogenetics Implementation Consortium Guideline for CYP2D6, OPRM1, and COMT Genotypes and Select Opioid Therapy. Clin Pharmacol Ther. 2021;110(4):888–896. doi:10.1002/cpt.2149
26. Ordonez Gallego A, Gonzalez Baron M, Espinosa Arranz E. Oxycodone: a pharmacological and clinical review. Clin Transl Oncol. 2007;9(5):298–307. doi:10.1007/s12094-007-0057-9
27. Che T, Roth BL. Molecular basis of opioid receptor signaling. Cell. 2023;186(24):5203–5219. doi:10.1016/j.cell.2023.10.029
28. Al-Hasani R, Bruchas MR. Molecular mechanisms of opioid receptor-dependent signaling and behavior. Anesthesiology. 2011;115(6):1363–1381. doi:10.1097/ALN.0b013e318238bba6
29. Gamble MC, Williams BR, Singh N, et al. Mu-opioid receptor and receptor tyrosine kinase crosstalk: implications in mechanisms of opioid tolerance, reduced analgesia to neuropathic pain, dependence, and reward. Front Syst Neurosci. 2022;16:1059089. doi:10.3389/fnsys.2022.1059089
30. Schmidt-Hansen M, Bennett M, Arnold S, et al. Oxycodone for cancer-related pain. Cochrane Database Syst Rev. 2022;6:1.
31. Reid CM, Martin RM, Sterne JAC, Davies AN, Hanks GW. Oxycodone for Cancer-Related Pain: meta-analysis of Randomized Controlled Trials. Archives of Internal Medicine. 2006;166(8):837–843. doi:10.1001/archinte.166.8.837
32. Leow KP, Cramond T, Smith MT. Pharmacokinetics and Pharmacodynamics of Oxycodone When Given Intravenously and Rectally to Adult Patients with Cancer Pain. Anesthesia Analg. 1995;80(2):296–302.
33. Kim NS, Lee JS, Park SY, et al. Oxycodone versus fentanyl for intravenous patient-controlled analgesia after laparoscopic supracervical hysterectomy: a prospective, randomized, double-blind study. Medicine. 2017;96(10):e6286. doi:10.1097/MD.0000000000006286
34. Hiramatsu K, Fukaya M, Aoba T, Arimoto A, Yamashita H, Nakashima Y. Early introduction of intravenous oxycodone injection followed by quick titration to oral oxycodone in outpatient cancer pain treatment in opioid-naive patients: “oxycodone bridge method”. Nagoya J Med Sci. 2025;87(2):272–284. doi:10.18999/nagjms.87.2.272
35. Agema B, Oosten A, Sassen S, et al. Population Pharmacokinetics of Oxycodone and Metabolites in Patients with Cancer-Related Pain. Cancers. 2021;14(1):13. doi:10.3390/cancers14010013
36. Kinnunen M, Piirainen P, Kokki H, Lammi P, Kokki M. Updated Clinical Pharmacokinetics and Pharmacodynamics of Oxycodone. Clin Pharmacokinet. 2019;58(6):705–725. doi:10.1007/s40262-018-00731-3
37. De Santis S, Simone MD, Mercadante S, et al. Oxycodone/Acetaminophen: the Tailoring Combination Treatment for Specific Clinical Profile of Opioid Well-Responsive Cancer Pain. Cancer Manag Res. 2021;13:1747–1756. doi:10.2147/CMAR.S290551
38. Kawana M, Miyasato A, Funato M, et al. Comparison of Analgesic Efficacy and Safety of Low-Dose Transdermal Fentanyl and Oral Oxycodone in Opioid-Naive Patients with Cancer Pain. Biol Pharm Bull. 2023;46(10):1444–1450. doi:10.1248/bpb.b23-00331
39. McGann M, Sacco A, Barnachea L. Evaluation of Extended-Release Oxycodone Administered through Enteral Tubes for the Management of Pain in Patients with Head and Neck Cancer: a Case Series. J Pain Palliat Care Pharmacother. 2021;35(4):240–245. doi:10.1080/15360288.2020.1830224
40. Schmidt-Hansen M, Bennett MI, Arnold S, Bromham N, Hilgart JS. Efficacy, tolerability and acceptability of oxycodone for cancer-related pain in adults: an updated Cochrane systematic review. BMJ Support Palliat Care. 2018;8(2):117–128. doi:10.1136/bmjspcare-2017-001457
41. Ameh S, Asogwau K, Awojulu T, Oturu O, Ezeani J. Extended-Release Formulations of Safer Opioids: improving Adherence and Reducing Mental Health Burdens. Int J Med All Body Health Res. 2022;3(1):83–86. doi:10.54660/IJMBHR.2022.3.1.83-86
42. Le BH, Aggarwal G, Douglas C, Green M, Nicoll A, Ahmedzai S. Oxycodone/naloxone prolonged-release tablets in patients with moderate-to-severe, chronic cancer pain: challenges in the context of hepatic impairment. Asia Pac J Clin Oncol. 2022;18(1):13–18. doi:10.1111/ajco.13561
43. McIntyre RS, Harris ME, Todtenkopf MS, Akerman S, Burgett J. Opioid antagonists: clinical utility, pharmacology, safety, and tolerability. CNS Spectr. 2024;29(6):542–548. doi:10.1017/S1092852924002189
44. Hamano J, Higashibata T, Kessoku T, et al. Naldemedine for Opioid-Induced Constipation in Patients With Cancer: a Multicenter, Double-Blind, Randomized, Placebo-Controlled Trial. J Clin Oncol. 2024;42(35):4206–4217. doi:10.1200/JCO.24.00381
45. Paice JA, Bohlke K, Barton D, et al. Use of Opioids for Adults With Pain From Cancer or Cancer Treatment: ASCO Guideline. J Clin Oncol. 2023;41(4):914–930. doi:10.1200/JCO.22.02198
46. Fallon M, Dierberger K, Leng M, et al. An international, open-label, randomised trial comparing a two-step approach versus the standard three-step approach of the WHO analgesic ladder in patients with cancer. Ann Oncol. 2022;33(12):1296–1303. doi:10.1016/j.annonc.2022.08.083
47. Fu Q, Han N, Li N, et al. Guidelines for Rational Clinical Use of Fentanyl Transdermal Patch. Drug Des Devel Ther. 2024;18:233–255. doi:10.2147/DDDT.S414318
48. Li Q, Long YL, He YW, et al. Intrathecal morphine delivery at prepontine cistern to control refractory cancer-related pain: a case report of extensive metastatic and refractory cancer pain. BMC Anesthesiol. 2024;24(1):77. doi:10.1186/s12871-024-02426-8
49. Kenfield M, Zacharias N, Abd-Elsayed A. Intrathecal Drug Delivery for the Treatment of Cancer-Associated Chronic Pain in Children. Neuromodulation. 2023;26(6):1153–1163. doi:10.1111/ner.13535
50. Hwang W. Evolution of pain management in lung cancer surgery: from opioid-based to personalized analgesia. Anesthesia and Pain Medicine. 2025;20(2):109–120. doi:10.17085/apm.25240
51. Barrett JE, Shekarabi A, Inan S. Oxycodone: a Current Perspective on Its Pharmacology, Abuse, and Pharmacotherapeutic Developments. Pharmacol Rev. 2023;75(6):1062–1118. doi:10.1124/pharmrev.121.000506
52. Yimer BB, Soomro M, McBeth J, et al. Comparative risk of severe constipation in patients treated with opioids for non-cancer pain: a retrospective cohort study in Northwest England. BMC Med. 2025;23(1):288. doi:10.1186/s12916-025-04118-7
53. Chan AYL, Bahmanyar S, Beyene K, et al. International Trends in Opioid Prescribing by Age and Sex from 2001 to 2019: an Observational Study Using Population-Based Databases from 18 Countries and One Special Administrative Region. CNS Drugs. 2025;39(11):1173–1185. doi:10.1007/s40263-025-01215-2
54. Waterhouse DM, Rothschild S, Dooms C, et al. Patient-reported outcomes in CodeBreaK 200: sotorasib versus docetaxel for previously treated advanced NSCLC with KRAS G12C mutation. Lung Cancer. 2024;196:107921. doi:10.1016/j.lungcan.2024.107921
55. Yu Y, Li D, Duan J, et al. The pro- and anti-cancer effects of oxycodone are associated with epithelial growth factor receptor level in cancer cells. Biosci Rep. 2020;40(2). doi:10.1042/BSR20193524.
56. Hu N, Yu T, Chen J, Zheng S, Yan H, Duan J. Oxycodone stimulates normal and malignant hematopoietic progenitors via opioid-receptor-independent-beta-catenin activation. Biochem Biophys Res Commun. 2020;533(4):1457–1463. doi:10.1016/j.bbrc.2020.10.031
57. De Rosa F, Giannatiempo B, Charlier B, et al. Pharmacological Treatments and Therapeutic Drug Monitoring in Patients with Chronic Pain. Pharmaceutics. 2023;15(8):2088. doi:10.3390/pharmaceutics15082088
58. Liu S, Li M, Liu Y, Geng R, Ji J, Zhang R. Pan-cancer Comprehensive Analysis Identified EGFR as a Potential Biomarker for Multiple Tumor Types. Appl Biochem Biotechnol. 2025;197(2):1055–1072. doi:10.1007/s12010-024-05060-9
59. Costanzo G, Turnaturi R, Parenti C, et al. New Insights into the Opioid Analgesic Profile of cis-(-)-N-Normetazocine-derived Ligands. Molecules. 2023;28(12):4827. doi:10.3390/molecules28124827
60. Wu Y, Zhao D, Zhuang J, Zhang F, Xu C. Caspase-8 and Caspase-9 Functioned Differently at Different Stages of the Cyclic Stretch-Induced Apoptosis in Human Periodontal Ligament Cells. PLoS One. 2016;11(12):e0168268. doi:10.1371/journal.pone.0168268
61. Zakharova IO, Bayunova LV, Zorina II, Sokolova TV, Shpakov AO, Avrova NF. Insulin and alpha-Tocopherol Enhance the Protective Effect of Each Other on Brain Cortical Neurons under Oxidative Stress Conditions and in Rat Two-Vessel Forebrain Ischemia/Reperfusion Injury. Int J Mol Sci. 2021;22(21):11768. doi:10.3390/ijms222111768
62. Meulmeester FL, Luo J, Martens LG, Mills K, van Heemst D, Noordam R. Antioxidant Supplementation in Oxidative Stress-Related Diseases: what Have We Learned from Studies on Alpha-Tocopherol? Antioxidants. 2022;11(12). doi:10.3390/antiox11122322
63. Camillo L, Grossini E, Farruggio S, et al. Alpha-Tocopherol Protects Human Dermal Fibroblasts by Modulating Nitric Oxide Release, Mitochondrial Function, Redox Status, and Inflammation. Skin Pharmacol Physiol. 2022;35(1):1–12. doi:10.1159/000517204
64. Weinberg F, Peckys DB, de Jonge N. EGFR Expression in HER2-Driven Breast Cancer Cells. Int J Mol Sci. 2020;21(23):9008. doi:10.3390/ijms21239008
65. Berg KCG, Eide PW, Eilertsen IA, et al. Multi-omics of 34 colorectal cancer cell lines - a resource for biomedical studies. Mol Cancer. 2017;16(1):116. doi:10.1186/s12943-017-0691-y
66. Wang J, Guo P, Bian Y, et al. Morphine and treatment of cancer -related pain-risk or benefit? J Toxicol Environ Health B Crit Rev. 2025;28(8):570–576. doi:10.1080/10937404.2025.2509920
67. Oh TK, Song IA. Chronic Opioid Use and Risk of Cancer in Patients with Chronic Noncancer Pain: a Nationwide Historical Cohort Study. Cancer Epidemiol Biomarkers Prev. 2020;29(10):1962–1967. doi:10.1158/1055-9965.EPI-20-0206
68. Constance JE, McFarland MM, Casucci T, et al. Mapping the Evidence for Opioid-Mediated Changes in Malignancy and Chemotherapeutic Efficacy: protocol for a Scoping Review. JMIR Res Protoc. 2023;12:e38167. doi:10.2196/38167
69. Sun W, Zhuang S, Cheng M, Qiu Z. Mu opioid receptor mRNA overexpression predicts poor prognosis among 18 common solid cancers: a pan-cancer analysis. Front Oncol. 2023;13:1134744. doi:10.3389/fonc.2023.1134744
70. Qin L, Zeng X, Qiu X, Chen X, Liu S. The role of N6-methyladenosine modification in tumor angiogenesis. Front Oncol. 2024;14:1467850. doi:10.3389/fonc.2024.1467850
71. Kaur G, Roy B. Decoding Tumor Angiogenesis for Therapeutic Advancements: mechanistic Insights. Biomedicines. 2024;12(4):827. doi:10.3390/biomedicines12040827
72. Tian M, Jin L, Li R, Zhu S, Ji M, Li W. Comparison of oxycodone and morphine on the proliferation, apoptosis and expression of related molecules in the A549 human lung adenocarcinoma cell line. Exp Ther Med. 2016;12(2):559–566. doi:10.3892/etm.2016.3346
73. Feng T, Zeng S, Ding J, et al. Comparative analysis of the effects of opioids in angiogenesis. BMC Anesthesiol. 2021;21(1):257. doi:10.1186/s12871-021-01475-7
74. Yang Z, Zhang F, Abdul M, et al. Tumor necrosis factor-alpha-induced protein 8-like 2 alleviates morphine antinociceptive tolerance through reduction of ROS-mediated apoptosis and MAPK/NF-kappaB signaling pathways. Neuropharmacology. 2023;238:109667. doi:10.1016/j.neuropharm.2023.109667
75. Tang Y, Li NQ, Ye LQ, et al. Nalbuphine attenuates morphine-induced scratching by inhibiting PKCbeta-dependent microglial activation and p38 phosphorylation in male mice. J Neurosci Res. 2023;101(8):1289–1304. doi:10.1002/jnr.25189
76. Haines E, Burke M, Catterall R, et al. Abstract PR10: IK-595, a MEK-RAF complex inhibitor, obviates CRAF mediated resistance resulting in superior RAS/MAPK pathway inhibition and anti-tumor activity in RAS/RAF altered cancers. Mol Cancer Res. 2023;21(5_Supplement):PR10–PR10. doi:10.1158/1557-3125.RAS23-PR10
77. Khawar IA, Wei Q, Chen TH-P, Lin L, Grierson PM, Lim K-H. Abstract 3870: TNF-MK2 signaling drives protective autophagy following MAPK pathway inhibition in pancreatic cancer. Cancer Res. 2023;83(7_Supplement):3870. doi:10.1158/1538-7445.AM2023-3870
78. Szczepaniak A, Fichna J, Zielinska M. Opioids in Cancer Development, Progression and Metastasis: focus on Colorectal Cancer. Curr Treat Options Oncol. 2020;21(1):6. doi:10.1007/s11864-019-0699-1
79. Lynch WB, Miracle SA, Goldstein SI, et al. Validation studies and multi-omics analysis of Zhx2 as a candidate quantitative trait gene underlying brain oxycodone metabolite (oxymorphone) levels and behavior. bioRxiv. 2024;2024:1.
80. Shen MR, Waljee JF. Enhanced Recovery After Surgery Protocols: can They Reduce Postoperative Opioid Use? Ann Surg. 2019;270(6):e72. doi:10.1097/SLA.0000000000003475
81. Cui JH, Jiang WW, Liao YJ, Wang QH, Xu M, Li Y. Effects of oxycodone on immune function in patients undergoing radical resection of rectal cancer under general anesthesia. Medicine. 2017;96(31):e7519. doi:10.1097/MD.0000000000007519
82. Wodehouse T, Demopoulos M, Petty R, et al. A randomized pilot study to investigate the effect of opioids on immunomarkers using gene expression profiling during surgery. Pain. 2019;160(12):2691–2698. doi:10.1097/j.pain.0000000000001677
83. Suzuki M, Sakurada T, Gotoh K, Watanabe S, Satoh N. Correlation between the administration of morphine or oxycodone and the development of infections in patients with cancer pain. Am J Hosp Palliat Care. 2013;30(7):712–716. doi:10.1177/1049909112469823
84. Tan Q, Zhang K, Wang Q, Zang R. Oxycodone alleviates LPS-induced neuroinflammation by regulating the CREB/miR-181c/PDCD4 axis. J Toxicol Sci. 2024;49(10):435–446. doi:10.2131/jts.49.435
85. Wang Y, Feng W, Li S, et al. Oxycodone attenuates lipopolysaccharide-induced myocardial injury by inhibiting inflammation, oxidation and pyroptosis via Nrf2/HO-1 signalling pathway. Clin Exp Pharmacol Physiol. 2024;51(9):e13910. doi:10.1111/1440-1681.13910
86. Kampe S, Warm M, Kaufmann J, Hundegger S, Mellinghoff H, Kiencke P. Clinical efficacy of controlled-release oxycodone 20 mg administered on a 12-h dosing schedule on the management of postoperative pain after breast surgery for cancer. Curr Med Res Opin. 2004;20(2):199–202. doi:10.1185/030079903125002874
87. Yang GW, Cheng H, Song XY, et al. Effect of Oxycodone-Based Multimodal Analgesia on Visceral Pain After Major Laparoscopic Gastrointestinal Surgery: a Randomised, Double-Blind, Controlled Trial. Drug Des Devel Ther. 2024;18:1799–1810. doi:10.2147/DDDT.S464518
88. Han L, Su Y, Xiong H, et al. Oxycodone versus sufentanil in adult patient-controlled intravenous analgesia after abdominal surgery: a prospective, randomized, double-blinded, multiple-center clinical trial. Medicine. 2018;97(31):e11552. doi:10.1097/MD.0000000000011552
89. Wan Z, Chu C, Zhou R, Que B. Effects of Oxycodone Combined With Flurbiprofen Axetil on Postoperative Analgesia and Immune Function in Patients Undergoing Radical Resection of Colorectal Cancer. Clin Pharmacol Drug Dev. 2021;10(3):251–259. doi:10.1002/cpdd.818
90. Lao WL, Song QL, Jiang ZM, Chen WD, Zheng XH, Chen ZH. The Effect of Oxycodone on Post-operative Pain and Inflammatory Cytokine Release in Elderly Patients Undergoing Laparoscopic Gastrectomy. Front Med Lausanne. 2021;8:700025. doi:10.3389/fmed.2021.700025
91. Wang Q, Guo J, Hou M. Effect of intercostal nerve block combined with oxycodone on the postoperative cognitive ability in elderly patients undergoing radical resection of lung cancer. Am J Transl Res. 2022;14(9):6277–6285.
92. Cheng X, Han L. Effect of Oxycodone and Dezocine on Postoperative Analgesic Effect and Inflammatory Stress State of Patients with Lung Cancer. Pract Cancer J. 2021;36(10):1648–1651.
93. Sun J, Zheng J, Yang F, Xie W. The Effects of Oxycodone Patient-Controlled Intravenous Analgesia on Immune Function and Analgesic Efficacy in Patients After Lung Cancer Surgery. J Fujian Med Univ. 2024;58(03):188–192.
94. Zhang Y, Yan W, Chen Y, Fan Z, Chen J. Lower Background Infusion of Oxycodone for Patient-Controlled Intravenous Analgesia, Combined with Ropivacaine Intercostal Nerve Block, in Patients Undergoing Thoracoscopic Lobectomy for Lung Cancer: a Randomized, Double-Blind, Controlled Clinical Trial. Drug Des Devel Ther. 2021;15:3535–3542. doi:10.2147/DDDT.S316583
95. Wang J, Yuan X, Guo W, et al. Sedation and Analgesia for Liver Cancer Percutaneous Radiofrequency Ablation: fentanyl and Oxycodone Comparison. Int J Med Sci. 2020;17(14):2194–2199. doi:10.7150/ijms.47067
96. Wu WT, Jia ZY, Chen Y, et al. The Safety and Efficacy of Oxycodone Versus Fentanyl in Percutaneous Microwave Ablation of a Liver Tumour Abutting the Capsule. Cardiovasc Intervent Radiol. 2019;42(1):87–94. doi:10.1007/s00270-018-1980-6
97. Formenti P, Umbrello M, Pignataro M, et al. Managing Severe Cancer Pain with Oxycodone/Naloxone Treatment: a Literature Review Update. J Pers Med. 2024;14(5). doi:10.3390/jpm14050483.
98. Wang Y, Wu G, Liu Z, et al. Effect of oxycodone combined with ultrasound-guided thoracic paravertebral nerve block on postoperative analgesia in patients with lung cancer undergoing thoracoscopic surgery: protocol for a randomised controlled study. BMJ Open. 2023;13(10):e074416. doi:10.1136/bmjopen-2023-074416
99. Xu S, Wu N, Liu X, Zhu J, Liu Z. The Catechol‐O‐Methyltransferase (COMT) Val158Met Polymorphism Is Associated with Oxycodone Requirements, Adverse Effects, and Pain Sensitivity in Cancer Patients. J Clin Pharm Therapeutics. 2024;2024(1). doi:10.1155/2024/9990112
100. Copik MM, Sadowska D, Smereka J, Czyzewski D, Misiolek HD, Bialka S. Assessment of feasibility of opioid-free anesthesia combined with preoperative thoracic paravertebral block and postoperative intravenous patient-controlled analgesia oxycodone with non-opioid analgesics in the perioperative anesthetic management for video-assisted thoracic surgery. Anaesthesiol Intensive Ther. 2024;56(2):98–107. doi:10.5114/ait.2024.141279
101. Sah D, Shoffel-Havakuk H, Tsur N, Uhelski ML, Gottumukkala V, Cata JP. Opioids and Cancer: current Understanding and Clinical Considerations. Curr Oncol. 2024;31(6):3086–3098. doi:10.3390/curroncol31060235
102. Mamiya K, Iida H, Iseki M, et al. Consensus statement on chronic pain treatment in cancer survivors. J Anesth. 2025;39(2):161–181. doi:10.1007/s00540-024-03427-0
103. Ragaban F, Purohit O, Del Fabbro E. Methadone in Cancer-Related Neuropathic Pain: a Narrative Review. Curr Oncol. 2024;31(12):7613–7624. doi:10.3390/curroncol31120561
104. Brant JM, Rodgers BB, Gallagher E, Sundaramurthi T. Breakthrough Cancer Pain: a Systematic Review of Pharmacologic Management Clin. J Oncol Nurs. 2017;21(3 Suppl):71–80. doi:10.1188/17.CJON.S3.71-80
105. Higgins C, Smith BH, Matthews K. Evidence of opioid-induced hyperalgesia in clinical populations after chronic opioid exposure: a systematic review and meta-analysis. Br J Anaesth. 2019;122(6):e114–e126. doi:10.1016/j.bja.2018.09.019
106. Abdel Shaheed C, Hayes C, Maher CG, et al. Opioid analgesics for nociceptive cancer pain: a comprehensive review. CA Cancer J Clin. 2024;74(3):286–313. doi:10.3322/caac.21823
107. Mestdagh F, Steyaert A, Lavand’homme P. Cancer Pain Management: a Narrative Review of Current Concepts, Strategies, and Techniques. Curr Oncol. 2023;30(7):6838–6858. doi:10.3390/curroncol30070500
108. Varrassi G, Paladini A, Tran YV, et al. Advances in the Pathophysiology and Management of Cancer Pain: a Scoping Review. Cancers. 2026;18(2):259. doi:10.3390/cancers18020259
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Oxycodone versus Sufentanil for Postoperative Recovery in Obese Patients Undergoing Laparoscopic Bariatric Surgery: A Randomized Controlled Trial
Yao X, Wang Z, Zhang Y, Jia W, Sheng X, Zhou Y, Xu C, Jiao H
Drug Design, Development and Therapy 2025, 19:9387-9397
Published Date: 17 October 2025