")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 18
Pharmacological Management of Core Symptoms and Comorbidities of Autism Spectrum Disorder in Children and Adolescents: A Systematic Review
Authors Maniram J , Karrim SBS, Oosthuizen F, Wiafe E
Received 15 April 2022
Accepted for publication 21 July 2022
Published 7 August 2022 Volume 2022:18 Pages 1629—1644
DOI https://doi.org/10.2147/NDT.S371013
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Roger Pinder
Jennal Maniram,1 Saira BS Karrim,1 Frasia Oosthuizen,1 Ebenezer Wiafe1,2
1School of Health Sciences, University of KwaZulu-Natal, Durban, South Africa; 2Clinical Pharmacy Services Unit, Directorate of Pharmacy, Ho Teaching Hospital, Ho, Ghana
Correspondence: Jennal Maniram, School of Health Sciences, University of KwaZulu-Natal, Durban, South Africa, Tel +27718931508, Email [email protected]
Purpose: The pharmacological management of Autism Spectrum Disorder (ASD) in children remains a challenge due to limited effective management options and the absence of approved drugs to manage the core symptoms. This review aims to describe and highlight effective pharmacological management options employed in managing the core symptoms and comorbidities of ASD from eligible studies over the past decade.
Methods: A search of databases; PubMed, Scopus, Science Direct, and PsychInfo for pharmacotherapeutic options for ASD was conducted in this systematic review. Duplicate studies were removed by utilizing the EndNote citation manager. The studies were subsequently screened independently by two authors. Eligible studies from 01 January 2012 to 01 January 2022 were included based on established eligibility criteria. A narrative synthesis was used for data analysis.
Results: The systematic review provides a comprehensive list of effective management options for ASD comorbidities and core symptoms from 33 included studies. The management options for ASD comorbidities; insomnia, hyperactivity, irritability and aggression, gastrointestinal disturbances, and subclinical epileptiform discharges, were reviewed. Risperidone, aripiprazole, methylphenidate, guanfacine, levetiracetam, and atomoxetine are examples of effective pharmacological drugs against ASD comorbidities. Additionally, this review identified various drugs that improve the core symptoms of ASD and include but are not limited to, bumetanide, buspirone, intranasal oxytocin, intranasal vasopressin, and prednisolone.
Conclusion: This review has successfully summarized the pharmacological advancements made in the past decade to manage ASD. Although there is still no pharmacological cure for ASD core symptoms or additional drugs that have obtained regulatory approval for use in ASD, the availability of promising pharmacological agents are under evaluation and study.
Keywords: pharmacotherapy, therapeutic agent, effectiveness, outcome measure, randomized clinical trial, narrative synthesis
Introduction
Autism spectrum disorder (ASD) refers to a neurodevelopment disorder that is characterized by difficulties with social communication, social interaction, and restricted and repetitive patterns in behaviors, interests, and activities. By definition, the symptoms are present early on in development and affect daily functioning. The term “spectrum” is used because of the heterogeneity in the presentation and severity of ASD symptoms.1 The core symptoms of ASD include persistent deficits in social communication and social interaction across multiple contexts, as manifested by deficits in social-emotional reciprocity, nonverbal communicative behaviors, and developing, maintaining, and understanding relationships. Restricted, repetitive patterns of behavior, interests, or activities are also identified as core symptoms of ASD and manifest as insistence on sameness and inflexible adherence to routines, highly restricted, fixated interests that are abnormal in intensity or focus, hyper or hypo reactivity to sensory input and stereotyped or repetitive motor movements, use of objects, or speech.2 Most children who present with ASD, also experience a range of medical comorbidities. Common underlying medical conditions include anxiety, depression, epilepsy, gastrointestinal and immune function disorders, metabolic disorders, and sleep disorders.3
According to a recent systematic review update on the global prevalence of ASD, approximately 1/100 children are diagnosed with ASD around the world.4 While various medications are undergoing clinical trials for use in relieving ASD symptoms, some of the commonly prescribed medications include second-generation antipsychotics, selective serotonin reuptake inhibitors (SSRIs), stimulants, and alpha-2 adrenergic agonists.5 Risperidone and aripiprazole are currently the only medications that the Food and Drug Administration (FDA) has approved for symptoms associated with ASD, targeting the irritability often associated with this medical condition.6 Medicines for treating the core symptoms of ASD have long represented an area of unmet need since few drugs effectively relieve these symptoms, and none of the options currently used, work well for every individual. The FDA has also yet to approve a medicine for treating ASD core characteristics.7
Considering the triad of symptoms experienced by individuals with ASD and the increasing number of children diagnosed with the condition, it is apparent that additional therapeutic agents become readily available and accessible. This study aims to systematically review potential options for the pharmacological management of ASD in children and adolescents by identifying successful therapeutic agents against the core symptoms and comorbidities of ASD.
Materials and Methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines (2020) for systematic reviews were followed from design to reporting.8
Study Objectives
- To develop a comprehensive list of pharmaceutical agents that are in use for the management of the core symptoms of ASD.
- To identify available pharmacological options for the management of ASD-related comorbidities.
- To review and discuss therapeutic outcomes for all included studies.
Study Eligibility
Inclusion Criteria
The PICO framework was used to determine the eligibility of studies for this review;
- P – Population/participants: Children and adolescents (male and female) diagnosed with ASD (Autistic Disorder, Asperger’s Syndrome, or Pervasive Development Disorder) and between the ages of 2 and 18 years old.
- I–Intervention: Pharmacological agents for the management of ASD, including vitamins and dietary supplements when used for medicinal purposes to manage the core symptoms and/or the comorbidities of ASD.
- C – Comparison: Placebo, different pharmaceutical agents, or non-pharmacological therapeutic options to which ASD management agents of focus were compared.
- O – Outcome: An outcome measure that resulted in an improvement in the core symptoms of ASD and/or ASD comorbidity.
Exclusion Criteria
- Non-English studies.
- Studies that do not have the outcome of interest.
- Studies before the year 2012 and after 01 January 2022.
- Studies that there were not randomized control trials due to the large volume of studies available and the accuracy and reduction of bias in results in this type of study design.9
- Studies that involved individuals who were not diagnosed with ASD.
- Studies with individuals under the age of 2 and over the age of 18.
Information Sources and Search Strategy
A comprehensive search of 4 databases, PubMed, Scopus, Science Direct, and Psych-Info, was conducted by J.M and E.W. A triple stage approach to searching published literature was utilized in the development of the search strategy. Firstly, PubMed was searched for relevant articles. Secondly, the search strategy was adopted to Scopus, Science Direct, and Psych-Info. Thirdly, the citation list of the selected studies was further scanned for additional studies. Text words, keywords, and MESH terms such as pharmacological, drugs, medicine, treatment, drug therapy, ASD, autism, autism spectrum disorder, comorbidity, core symptoms, and children were used in each database. The search terms were combined using the Boolean operators “AND” and “OR” as indicated in Appendix 1.
Screening and Selection of Studies
Titles and Abstract Screening
Four databases, PubMed, Scopus, Science Direct, and PsychInfo were searched independently by two authors (J.M & E.W) according to the search strategy designed. The duplicate results and those studies with titles and abstracts that did not meet eligibility criteria were removed. There were no disagreements between J.M and E.W.
Full-Text Screening
After the removal of duplicates and results with irrelevant titles and abstracts, the remaining studies went through full-text screening. This step was also done independently by two authors (J.M & E.W). Additional articles that did not meet the inclusion criteria due to ineligible study design, study population, and target age group, were removed. Review articles and studies without the desired outcome of interest were also removed. The remaining studies were selected for final inclusion in the review. There were no disagreements between J.M and E.W.
Quality Assessment
The Joanna Briggs Critical Appraisal tool, Checklist for Randomized Controlled Trials10 was utilized to assess the quality of each study. This appraisal tool contained questions related to true randomization, concealment of allocation to treatment groups, blinding at all stages, the use of reliable outcome measures, and the performance of appropriate statistical analysis. The quality appraisal stage was done independently by two authors (J.M & E.W). The articles were then scored based on their quality scores and classified as less than 50% (low-quality studies), 50% to 75% (moderate-quality studies), or greater than 75% (high-quality studies). There were no disagreements between J.M and E.W.
Data Extraction
A data extraction tool (Appendix 2) was utilized to obtain the data required for this systematic review. The tool was designed by J.M to record data related to the therapeutic agent, study reference, sample size, and country. For ASD comorbidities, the name of the comorbidity and treatment effectiveness from the study were recorded. For ASD core symptoms, the improved outcome measure and treatment effectiveness were recorded. There was a greater emphasis on improved outcome measures and treatment effectiveness for ASD core symptoms due to the absence of a cure and no approved pharmacological treatments.11
Data Synthesis
Extracted data from the studies were analyzed through a narrative synthesis for the management options of core symptoms and ASD-related comorbidities. For narrative synthesis, the quantitative data was converted into “qualitised data”. This involved the transformation into thematic descriptions of the quantitative results from the selected studies in a manner that would answer the review questions. The collected data were categorized and pooled together based on similarity in meaning to produce a set of integrated results. It was not possible to perform a meta-analysis on the effectiveness of management options since the studies had different outcome measures and different drugs therefore an overall quantitative estimate could not be performed.12
Results
Search Results
The data collection process began in February 2022 by J.M and E.W. Based on the search of 4 databases there were a total of 1655 citations (PubMed = 71, Science Direct = 854, Scopus = 522, PsychInfo = 208; Figure 1). Upon removal of duplicate results, the articles were reduced to 904. These articles were screened by title and abstract according to eligibility criteria and a further 819 results were removed. A total of 84 articles were then subjected to full-text assessment. A further 51 studies were excluded for reasons indicated in the PRISMA flow diagram (Figure 1); 33 studies were included in the systematic review. There were no disagreements between J.M and E.W.
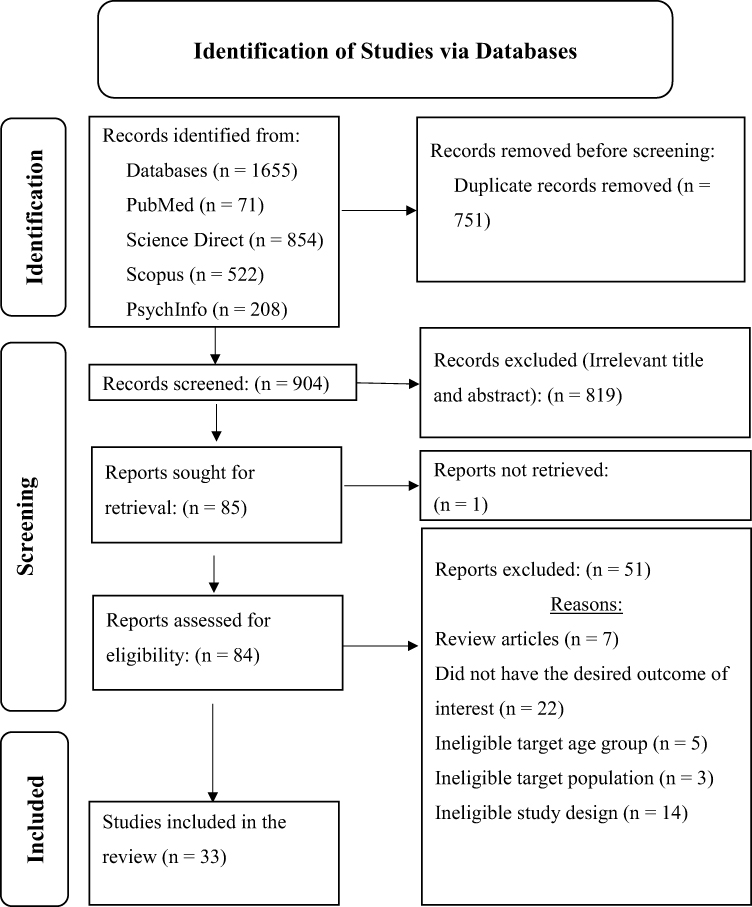 |
Figure 1 A summary of the study selection procedure which is presented on a PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram. Notes: Based on the search of 4 databases (PubMed, Scopus, Science Direct and PyschInfo), a total of 1655 citations were available. After removing duplicate results [n (number of studies) = 751] and excluding studies with irrelevant title and abstract (n = 819), the results were reduced to 85. An additional study was not retrievable. The rest of the studies were assessed for eligibility and a further 51 studies were excluded for reasons indicated in the PRISMA flow diagram and 33 studies were included in the systematic review. PRISMA figure adapted from Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews.8 |
Quality Assessment
The 33 selected studies were appraised for quality by utilizing the Johanna Briggs Institute (JBI) critical appraisal checklist for randomized control trials.10 Appraisal of individual studies using the JBI appraisal method is shown as supplementary information (Appendix 3).10 The majority of the studies (52%) were of the highest quality scoring (100%) and 48% of studies were of a high-quality (score > 75%). None of the studies were eliminated based on methodological quality evaluation outcomes as the authors wanted to compile a comprehensive list of all potentially effective therapeutic agents. There were no disagreements between J.M and E.W.
Study Characteristics
The data extracted from the 33 studies are detailed in Table 1: Summary of Study Characteristics and Management Effectiveness of ASD Comorbidities, and Table 2: Summary of Study Characteristics and Management Effectiveness of ASD Core Symptoms. The articles selected were published from the year 2012 up to and including the year 2021. This produced a set of results that describe current trends in the pharmacological management of ASD over the past decade. The study design of all selected articles included in this review was randomized control trials. The sample size of participants across all studies ranged from 13 to 166 participants.
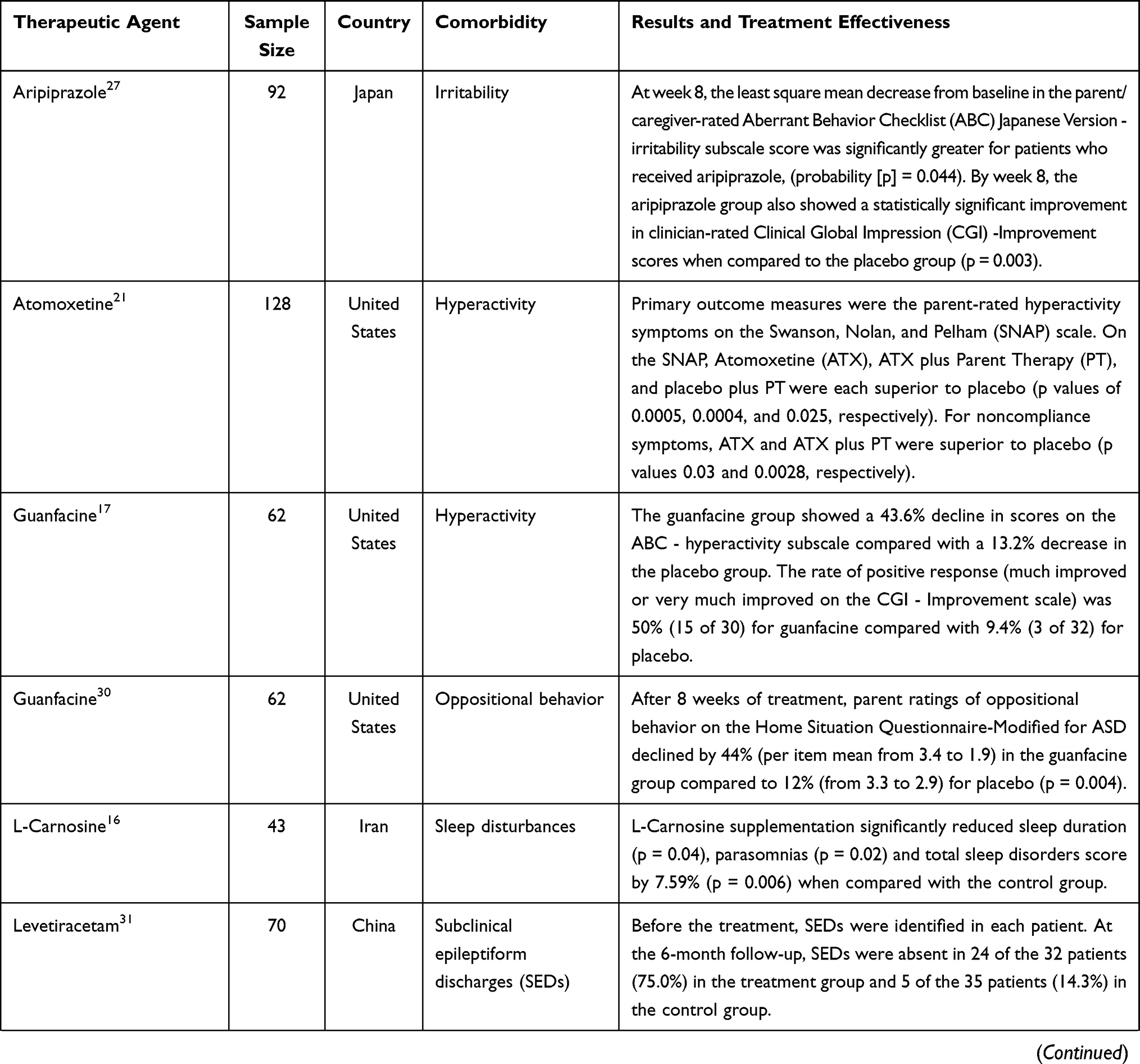 |  | 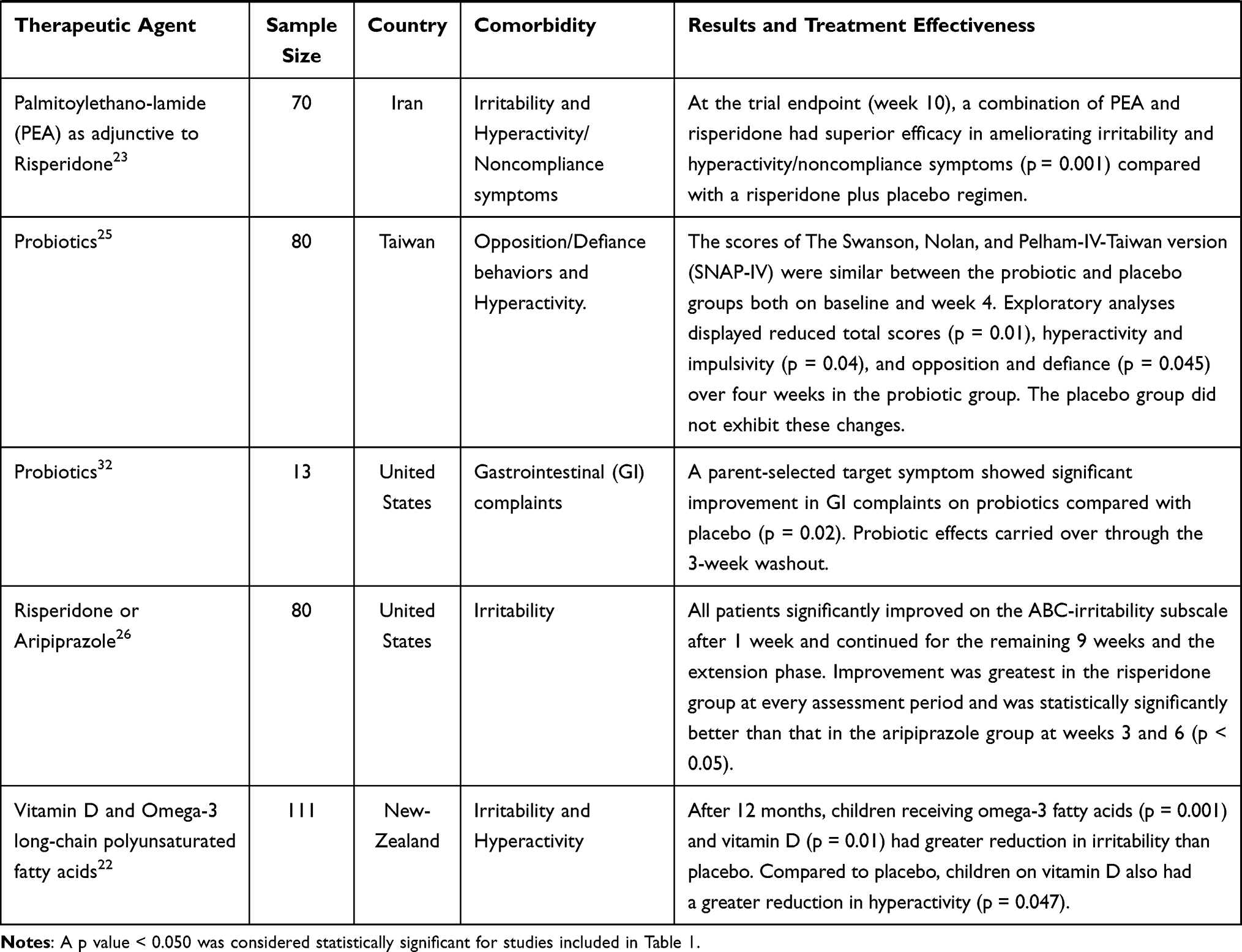 |
Table 1 Characteristics of Studies for the Treatment of ASD Comorbidities |
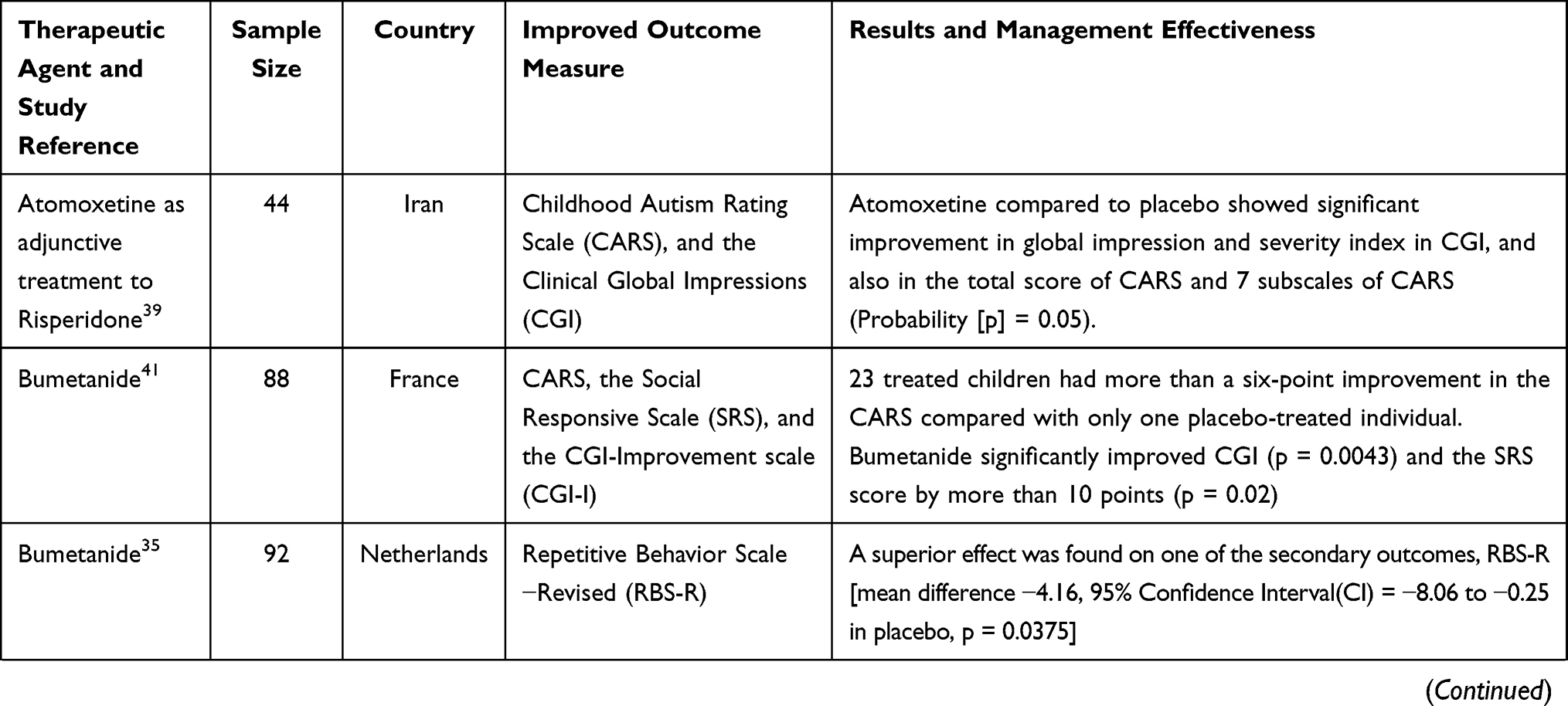 | 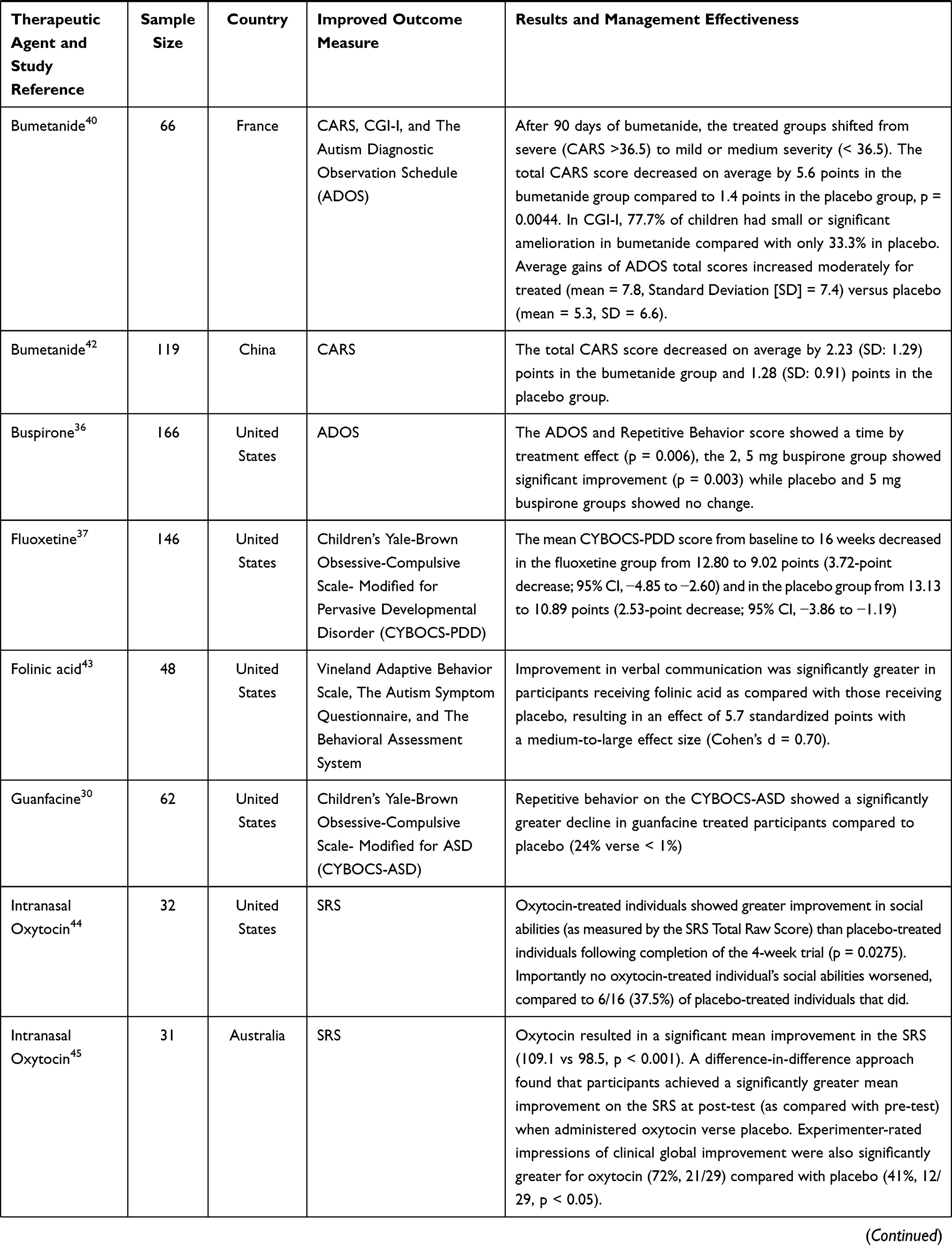 | 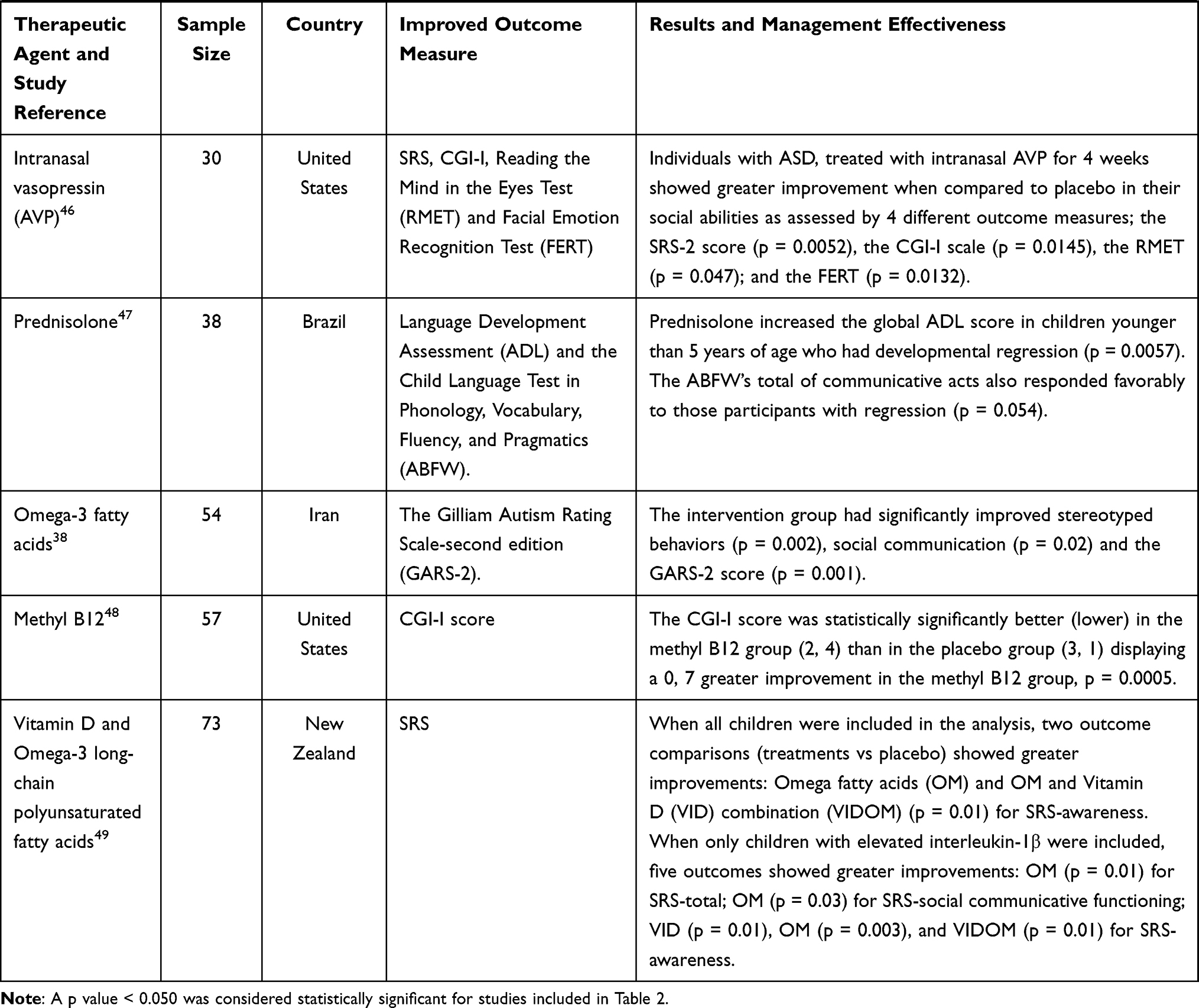 |
Table 2 Summary of Study Characteristics and Management Effectiveness of ASD Core Symptoms |
Demographic and Participant’s Characteristics
Of the selected studies, 52% (n = 17) were conducted in the USA and 18% (n = 6) were conducted in Iran. The rest of the studies were conducted in New Zealand (n = 2), Asia (n = 4), France (n = 2), Australia (n = 1) and Brazil (n = 1). Interestingly, there were no studies conducted in Africa. The main objective of all studies was to examine the effect of a pharmacological intervention compared to a placebo when used to manage an ASD comorbidity or core symptom. All studies included male and/or female children and/or adolescents diagnosed with ASD. The population age group for the included studies ranged between 2 and 18 years.
Review Findings
Management Options for ASD Comorbidities
Insomnia and Sleep Disturbances
Melatonin - Melatonin is a hormone produced in response to darkness that assists with the timing of circadian rhythms (24-hour internal clock) and with sleep.13 According to a randomized control trial,14 melatonin illustrated improved sleep duration and onset when compared to placebo.
L- Carnosine - Carnosine, a substance produced naturally by the body is classified as a dipeptide, a compound made up of two linked amino acids and is highly concentrated in muscle tissue and the brain.15 A randomized control trial16 indicated that carnosine supplementation in ASD individuals (4–16 years old) could be effective in improving sleep disturbances, in particular, sleep duration and parasomnias subscales when compared to placebo.
Hyperactivity
Guanfacine - In a multisite, randomized clinical trial, extended-release guanfacine was compared with placebo in children with ASD. The guanfacine group displayed a significant decline in scores on the Aberrant Behavior Checklist (ABC)-hyperactivity subscale when compared to the placebo group. Results indicated that extended-release guanfacine was safe and effective for reducing hyperactivity, impulsiveness, and distractibility in children with ASD.17
Methylphenidate - Three randomized control trials displayed the effectiveness of methylphenidate for the treatment of hyperactivity. A multisite, 4-week, randomized crossover trial compared three dose levels (low, medium, and high) of methylphenidate with placebo. On the primary outcome measure, the ABC-hyperactivity subscale, the medium and high-dose levels were superior to placebo.18 Similar results were seen in a second study where methylphenidate treatment was associated with significant declines in hyperactive and impulsive behavior at both home and school.19 Additionally, a within-subject, crossover, placebo-controlled design study revealed that methylphenidate treatment was associated with significant performance gains on cognitive tasks tapping sustained attention, selective attention, and impulsivity/inhibition in children with ASD.20
Atomoxetine - In a double-blind trial of atomoxetine (ATX) and parent therapy (PT), 128 children (ages 5–14 years) with ASD and Attention Deficit Hyperactivity Disorder (ADHD) symptoms were randomized to ATX, ATX plus PT, placebo plus PT, or placebo. Primary outcome measures indicated that both ATX and PT resulted in significant improvement in ADHD symptoms, whereas ATX (both alone and combined with PT) was associated with significant decreases in measures of noncompliance. The study concluded that subsequent research should include a comparison of atomoxetine with other psychopharmacological treatments for ADHD along with the impact of psychosocial interventions.21
Additionally, vitamin D,22 Palmitoylethanolamide (PEA) as adjunctive to risperidone,23 memantine as adjunctive to risperidone,24 and probiotics25 also displayed effectiveness in reducing hyperactivity compared to placebo.
Irritability, Aggression, Aberrant Behavior, Anxiety, and Maladaptive Behaviors
Aripiprazole and Risperidone - Both these agents have FDA approval for the aggression and irritability seen in children with ASD. A randomized double-blind parallel-group study of risperidone or aripiprazole was conducted in three academic medical centers and a single private pediatric practice. Pharmacotherapy (treatment with risperidone or aripiprazole) of patients with ASD resulted in behavioral improvement within 1 week and lasted at least 22 weeks. A trend was observed for greater improvement in the risperidone group at all assessment points, but the difference compared to aripiprazole reached statistical significance only at weeks 3 and 6. This trial supports previous results of drug effectiveness and safety in patients with ASD from other trials and extends the evidence-based support for choosing an FDA-approved drug for initial pharmacotherapy for ASD.26
Aripiprazole - A randomized, double-blind, placebo-controlled 8-week study in Japan evaluated the effectiveness and safety of aripiprazole in the treatment of irritability in children and adolescents (6–17 years) with ASD. Aripiprazole produced a significant improvement in the mean parent/caregiver-rated ABC Japanese Version-irritability subscale score relative to placebo. Aripiprazole displayed effectiveness, safety, and tolerability in the treatment of irritability associated with ASD in Japanese children and adolescents.27
PEA, N-Acetylcysteine (NAC), or Memantine as Adjunctive Treatment to Risperidone - Three studies conducted in Iran investigated the addition of PEA, NAC, or memantine to risperidone for enhanced therapeutic effect when treating irritability and other aberrant behaviors seen in ASD. A randomized, parallel-group, double-blind placebo-controlled trial was conducted to investigate the effectiveness of co-management with risperidone and PEA in children with ASD. At the trial endpoint (week 10), the combination of PEA and risperidone had superior effectiveness in ameliorating the irritability and hyperactivity/noncompliance symptoms compared with a risperidone plus placebo regimen.23 Similar results were seen with NAC as adjunctive management for ASD as risperidone plus NAC decreased irritability more than risperidone plus placebo in children and adolescents with ASD.28 Additionally, a study utilizing risperidone and memantine illustrated differences between the two management arms as the group that received memantine had a greater reduction in irritability, stereotypic behavior, and hyperactivity.24
NAC - A study of NAC as monotherapy also produced effective results as NAC resulted in significant improvements on the ABC-irritability subscale compared with placebo.29
Additionally, other randomized controlled trials included in this review that utilize vitamin D and omega-3 long-chain polyunsaturated fatty acids,22 probiotics,25 guanfacine,30 and levetiracetam31 also demonstrated significant improvements in irritability, maladaptive or oppositional behaviors seen in children and adolescents with ASD.
Gastrointestinal Disturbances
Probiotics – This therapeutic agent was effective against common gastrointestinal (GI) symptoms seen in children with ASD. In a study conducted in the United States, thirteen children, 3–12 years of age with ASD and GI symptoms were randomized into a probiotic crossover trial of 8 weeks each on VISBIOME (a probiotic that contains eight probiotic species, mostly Lactobacillus and Bifidobacterium) and placebo separated by a 3-week washout. A parent-selected target symptom showed significant improvement in GI complaints on probiotics compared with placebo. The probiotic formulation was safe and suggested a health benefit in children with ASD and GI symptoms who retained lactobacillus.32 Additionally, two open-label studies,33,34 not included in this review due to the study design, also supported the improvement of gastrointestinal comorbidities attributed to the use of probiotics in children with ASD.
Subclinical Epileptiform Discharges (SEDs)
Levetiracetam - SEDs are common in pediatric patients with ASD. A physician-blinded, randomized controlled trial investigated an association between the anticonvulsant drug levetiracetam and SEDs in children with ASD. Levetiracetam was effective for controlling SEDs in pediatric patients with ASD and was also associated with improved behavioral and cognitive functions. The rate of electroencephalographic normalization was also significantly higher in the treatment group.31
Management Options for ASD Core Symptoms
Therapeutic Agents for Restricted and Repetitive Behaviors or Interests
Bumetanide - Although a study conducted in the Netherlands for bumetanide displayed no superior effectiveness for the trial’s primary outcome measures, it did result in an improvement on a secondary outcome measure; The Repetitive Behavior Scale-Revised (RBS-R), and the observed effect was more explicit in female participants.35
Buspirone - A study involving the use of buspirone concluded that buspirone treatment may be considered for further exploration as a useful adjunct therapy to target restrictive and repetitive behavior in conjunction with early behavioral intervention, to provide therapeutic coverage for the full range of ASD core features and adaptive skills in young children with ASD.36
Fluoxetine - In a multicenter, randomized, placebo-controlled clinical trial, participants aged 7.5–18 years with ASD and a total score of 6 or higher on the Children’s Yale-Brown Obsessive Compulsive Scale, modified for pervasive developmental disorder (CYBOCS-PDD) were recruited from 3 tertiary health centers across Australia. Treatment with fluoxetine compared with placebo resulted in significantly lower scores for obsessive-compulsive behaviors at 16 weeks.37
Guanfacine - Repetitive behavior showed a significantly greater decline in guanfacine-managed participants compared to placebo. Results from this study concluded that guanfacine can be considered a first-line treatment for children with ASD who exhibit hyperactivity, as well as oppositional behavior, or repetitive behavior. Future studies could focus on repetitive behavior or anxiety, symptoms with limited treatment options.30
Omega-3 fatty acids - Stereotype behaviors significantly improved by intervention with omega-3 fatty acids according to the Gilliam Autism Rating Scale – second edition (GARS-2).38
Therapeutic Agents for Social Communication and Social Interaction Challenges
Atomoxetine as Adjunctive Treatment to Risperidone - A study done in Iran illustrated that the addition of atomoxetine to risperidone displayed improvements for 7 subscales on the Childhood Autism Rating Scale (CARS) which included relationship to people, emotional response, body use, listening response, fear and nervousness, nonverbal communication, and activity level. The study concluded that the addition of atomoxetine to risperidone resulted in significant improvements compared to placebo and risperidone.39
Bumetanide – A study conducted in France that examined the effects of bumetanide on the core symptoms of ASD indicated that bumetanide reduced significantly the CARS, Clinical Global Impressions (CGI), and The Autism Diagnostic Observation Schedule (ADOS) values when the most severe cases were removed. Several qualitative comments from the parents of children in the study attested to bumetanide’s positive effects, including a greater presence of the child, facilitated visual communication, and social exchanges. Results suggested a promising novel therapeutic approach to treating ASD children.40 An additional study conducted in France suggested that bumetanide was effective in improving ASD-related symptoms across the pediatric age range as assessed by CARS, the CGI-Improvement scale (CGI-I), and the Social Responsive Scale (SRS). Interestingly, responders were found in all subpopulations, ages, and ASD severity according to CARS scores suggesting that the treatment was not restricted to a particular group.41 Thirdly, a randomized, double-blind, placebo-controlled trial of bumetanide in a large group of children with ASD, aged 3−6 years, found that bumetanide at a dose of 0.5 mg twice daily significantly improved the core symptoms of ASD as measured by the primary clinical outcome (CARS total score). It was concluded that bumetanide is safe and effective in improving disease severity, attenuating social impairment, and improving the activity level of children with ASD, and therefore provides a viable alternative therapeutic option for young patients in addition to behavioral interventions.42
Folinic acid - Improvement in verbal communication was significantly greater in participants receiving folinic acid as compared with those receiving placebo according to three different subscales: Vineland Adaptive Behavior Scale, The Autism Symptom Questionnaire, and The Behavioral Assessment System. Folate receptor-α autoantibody (FRAA) status was predictive of response to treatment. For FRAA-positive participants, improvement in verbal communication was significantly greater in those receiving folinic acid as compared with those receiving placebo, indicating that folinic acid treatment may be more efficacious in children with ASD who are FRAA positive.43
Intranasal Oxytocin - Two studies included in the review demonstrated the effectiveness of intranasal oxytocin on social communication and social interaction challenges. In the study conducted in the United States, the efficacy and tolerability of intranasal oxytocin treatment (24 International Units, twice daily) were tested in 32 children with ASD, aged 6–12 years old. When pretreatment neuropeptide measures were included in the statistical model, oxytocin compared with placebo treatment significantly enhanced social abilities in children with ASD. Importantly, pretreatment blood oxytocin concentrations also predicted treatment response, such that individuals with the lowest pretreatment oxytocin concentrations showed the greatest social improvement.44 Additionally, a study in Australia also resulted in a significant mean improvement on the SRS parent report when oxytocin was compared to placebo. The study was the first clinical trial to support the potential of oxytocin as an early intervention for young children with ASD to help improve social interaction deficits.45
Intranasal Vasopressin (AVP) - A study conducted in the USA indicated that individuals managed with intranasal AVP for 4 weeks showed greater improvement in their social abilities as assessed by the primary outcome measure, the Social Responsive Scale-2 (SRS-2). AVP-managed individuals also showed greater clinician-evaluated improvement in social communication abilities as assessed by the CGI-I scale. Similarly, child participants managed with intranasal AVP versus placebo showed enhanced theory of mind abilities, as assessed by the Reading the Mind in the Eyes Test (RMET), and increased facial emotion recognition abilities as assessed by the Facial Emotion Recognition Test (FERT).46
Prednisolone - A study conducted in Brazil that aimed to describe the effect of prednisolone on the language of children with ASD resulted in positive therapeutic outcomes as indicated by the Language Development Assessment (ADL) and the Child Language Test in Phonology, Vocabulary, Fluency, and Pragmatics (ABFW). The benefit of prednisolone for language scores was more evident in participants who were younger than five years, with a history of developmental regression. The prednisolone dose of 1 mg/kg/day used during the first eight weeks of the trial was low therefore the study concluded that a higher dose would have achieved more favorable intervention outcomes.47
Additionally, studies that utilize non-pharmacological agents; methyl B1248 and vitamin D and omega-3 long-chain polyunsaturated fatty acids49 also displayed effectiveness for social communication and social interaction challenges as indicated numerically in Table 2.
Discussion
This review highlights and describes the effectiveness of various therapeutic agents for ASD comorbidities and core symptoms through thirty-three randomized control trial studies conducted over the past decade. As indicated above, a meta-analysis to perform a quantitative estimate of drug effectiveness was not possible due to the heterogeneous nature of the selected studies.12 Various trends could be observed from the included studies in this review. Firstly, the addition of therapeutic agents to risperidone improved the effectiveness in the management of ASD comorbidities as seen in the following studies.23,24,28 A similar observation was found with atomoxetine as adjunctive treatment to risperidone and produced improved results on the core symptoms compared to placebo and risperidone.39 All four of these studies were conducted in Iran and therefore it would be interesting to observe results from similar studies conducted elsewhere internationally. Bumetanide was the agent of choice for improvement in the core symptoms of ASD since it produced effective results in four different randomized control trials.35,40–42 The results also indicated that bumetanide improved both core symptoms (restricted and repetitive behaviors or interests and social communication and social interaction challenges). The geographical distribution of the studies with bumetanide also spanned across three different countries: France,40,41 Netherlands,35 and China.42 Intranasal dosage preparations observed in the form of oxytocin44,45 and vasopressin46 produced effective results for social communication and social interaction challenges. Intranasal vasopressin as a pharmacological treatment option produced positive results on the core symptoms according to four improved outcome measures from a single study.46 Future studies involving intranasal vasopressin should be conducted by utilizing the same target population and greater sample size to determine if the same replication of results is observed. A study involving the use of prednisolone displayed promising effectiveness against social communication deficits and this was the first prospective study in medical literature based on a double-blinded, randomized, placebo-controlled clinical trial on the treatment of ASD with corticosteroids.47 Two pharmacological agents, atomoxetine and guanfacine which are both indicated for use in ADHD, resulted in positive outcomes on the core symptoms and comorbidities of ASD. Guanfacine in some studies resulted in improvements in hyperactivity,17 oppositional behavior,30 and core symptoms.30 Similarly, studies involving the use of atomoxetine resulted in improvements in hyperactivity21 and core symptoms.39 A study in Japan involving the use of aripiprazole produced results that were in line with FDA approval of this pharmacological agent for the management of irritability and aggression seen in ASD individuals.27 Methylphenidate produced effective results from three different clinical trials for the management of hyperactivity in ASD.18–20 Epilepsy is a common comorbidity experienced by children with ASD. However, the only antiepileptic drug that appeared in this review was levetiracetam for the effective management of subclinical epileptiform discharges.31 Non-pharmacological agents in the form of dietary and vitamin supplements produced effective results for the management of ASD comorbidities and/or core symptoms. According to this review, there were no pharmacological agents available for the management of insomnia and gastric symptoms. However, dietary supplements in the form of melatonin14 and L-carnosine16 were effective in the management of insomnia while probiotics produced effective results for gastrointestinal complications.32 Omega-3 fatty acids displayed effectiveness in irritability,22 repetitive behavior,38 and social communication and social interaction challenges.49 Additionally, folinic acid,43 vitamin D,49 and methyl B1248 produced effective results for the core symptoms of ASD. An important observation, based on this review and the inclusion criteria, is the complete absence of any randomized control trials from South Africa or Africa as a continent. This is an area of concern considering the prediction that 40% of the world’s children will live on the continent of Africa by the year 2050 and 1–2% of them are likely to have ASD.50 Previous international systematic reviews regarding the pharmacological management of ASD in children either involved an investigation of pharmacological interventions for the core symptoms of ASD only example51,52 or involved a systematic review of psychotropic drug use for ASD comorbidities.53 Additional systematic reviews included pharmacological management options for severe irritability54 and ADHD55 in individuals diagnosed with ASD. To our knowledge, this systematic review could be the only or possibly one of the limited studies that describe effective management options for both ASD core symptoms and comorbidities in children and adolescents over the past ten years.
Limitations
The review was limited to full-text studies from four databases. Also, due to the large volume of studies available on the pharmacological management of ASD, the eligibility criteria for study design were limited to randomized control trials since randomization reduces bias and provides a rigorous tool to examine cause-effect relationships between an intervention and outcome.9 This indicates the availability of the same or additional therapeutic agents from this review that display effectiveness through open-label trials, case reports, case studies, and other types of study designs. Data analysis was limited to narrative synthesis due to the heterogeneous nature of the studies retrieved. However, a meta-analysis in the future should not be ruled out if additional studies are conducted for individual drug effectiveness. To ensure results were current trends in the pharmacological management of ASD, eligible studies were selected from 01 January 2012 to 01 January 2022 only.
Conclusion
Since the FDA approval of risperidone and aripiprazole,6 there are still no additional pharmacological agents that have gained a similar therapeutic status for the treatment of ASD core symptoms or comorbidities. However, based on the results of this review, it can be concluded that various drugs are available and it is apparent that sufficient progress has been made over the past decade related to effective management options for ASD core symptoms and comorbidities. Although none of the therapeutic agents included in this review provided a complete resolution or cure of ASD core symptoms, they did display positive outcomes and improved management effectiveness compared to placebo. In the future, based on results from additional effective studies conducted internationally, there is a possibility that certain drugs especially bumetanide and possibly other therapeutic agents included in this review, would be in a position to obtain regulatory approval for use in ASD.
Data Sharing Statement
Most of the data used in this systematic review are publicly available.
Ethical Considerations
Ethical approval was not required since no individual data was used. The results will be disseminated for publication in a reputable medical journal.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare they have no conflicts of interest.
References
1. American Psychological Association. Autism spectrum disorder; 2022. Available from: https://www.apa.org/topics/autism-spectrum-disorder.
2. Centers for Disease Control and Prevention. Autism spectrum disorder; 2020. Available from: https://www.cdc.gov/ncbddd/autism/hcp-dsm.html.
3. Autism Research Institute. Comorbidities of autism; 2021. Available from: https://www.autism.org/comorbidities-of-autism/.
4. Zeidan J, Fombonne E, Scorah J, et al. Global prevalence of autism: a systematic review update. Autism Res. 2022;15(5):778–790. doi:10.1002/aur.2696
5. MedicineNet. Types of autism medications and treatments; 2021. Available from: https://www.medicinenet.com/types_of_autism_medications_and_treatments/drug-class.htm.
6. DeFilippis M, Wagner KD. Treatment of autism spectrum disorder in children and adolescents. Psychopharmacol Bull. 2016;46(2):18–41.
7. Autism Speaks. Medicines for treating autism’s core symptoms; 2022. Available from: https://www.autismspeaks.org/medicines-treating-autisms-core-symptoms.
8. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Br Med J. 2021;372:n71. doi:10.1136/bmj.n71
9. Hariton E, Locascio JJ. Randomized controlled trials - the gold standard for effectiveness research: study design: randomized controlled trials. Int J Obstetr Gynaecol. 2018;125(13):1716. doi:10.1111/1471-0528.15199
10. Aromataris E, Munn Z. Joanna Briggs Institute Reviewers Manual. 2017. Available from: https://joannabriggs.org/. Accessed August 5, 2022.
11. National Institute of Child Health and Human Development. Medication treatment for autism; 2021. Available from: https://www.nichd.nih.gov/health/topics/autism/conditioninfo/treatments/medication-treatment#.
12. Ioannidis JPA, Patsopoulos NA, Rothstein HR. Reasons or excuses for avoiding meta-analysis in forest plots. Br Med J. 2008;336(7658):1413–1415. doi:10.1136/bmj.a117
13. National Center for Complementary and Integrative Health. Melatonin: what you need to know; 2021. Available from: https://www.nccih.nih.gov/health/melatonin-what-you-need-to-know.
14. Gringras P, Nir T, Breddy J, Frydman-Marom A, Findling RL. Efficacy and safety of pediatric prolonged-release melatonin for insomnia in children with autism spectrum disorder. J Am Acad Child Adolesc Psychiatry. 2017;56(11):948–957.e944. doi:10.1016/j.jaac.2017.09.414
15. Wong C. What is carnosine?; 2021. Available from: https://www.verywellhealth.com/the-benefits-of-carnosine-89430.
16. Mehrazad-Saber Z, Kheirouri S, Noorazar SG. Effects of l-carnosine supplementation on sleep disorders and disease severity in autistic children: a randomized, controlled clinical trial. Basic Clin Pharmacol Toxicol. 2018;123(1):72–77. doi:10.1111/bcpt.12979
17. Scahill L, McCracken JT, King BH, et al. Extended-release guanfacine for hyperactivity in children with autism spectrum disorder. Am J Psychiatry. 2015;172(12):1197–1206. doi:10.1176/appi.ajp.2015.15010055
18. Scahill L, Bearss K, Sarhangian R, et al. Using a patient-centered outcome measure to test methylphenidate versus placebo in children with autism spectrum disorder. J Child Adolesc Psychopharmacol. 2017;27(2):125–131. doi:10.1089/cap.2016.0107
19. Pearson DA, Santos CW, Aman MG, et al. Effects of extended release methylphenidate treatment on ratings of attention-deficit/hyperactivity disorder (ADHD) and associated behavior in children with autism spectrum disorders and ADHD symptoms. J Child Adolesc Psychopharmacol. 2013;23(5):337–351. doi:10.1089/cap.2012.0096
20. Pearson DA, Santos CW, Aman MG, et al. Effects of extended-release methylphenidate treatment on cognitive task performance in children with autism spectrum disorder and attention-deficit/hyperactivity disorder. J Child Adolesc Psychopharmacol. 2020;30(7):414–426. doi:10.1089/cap.2020.0004
21. Handen BL, Aman MG, Arnold LE, et al. Atomoxetine, parent training, and their combination in children with autism spectrum disorder and attention-deficit/hyperactivity disorder. J Am Acad Child Adolesc Psychiatry. 2015;54(11):905–915. doi:10.1016/j.jaac.2015.08.013
22. Mazahery H, Conlon CA, Beck KL, et al. A randomized controlled trial of vitamin D and omega-3 long chain polyunsaturated fatty acids in the treatment of irritability and hyperactivity among children with autism spectrum disorder. J Steroid Biochem Mol Biol. 2019;187:9–16. doi:10.1016/j.jsbmb.2018.10.017
23. Khalaj M, Saghazadeh A, Shirazi E, et al. Palmitoylethanolamide as adjunctive therapy for autism: efficacy and safety results from a randomized controlled trial. J Psychiatr Res. 2018;103:104–111. doi:10.1016/j.jpsychires.2018.04.022
24. Ghaleiha A, Asadabadi M, Mohammadi MR, et al. Memantine as adjunctive treatment to risperidone in children with autistic disorder: a randomized, double-blind, placebo-controlled trial. Int J Neuropsychopharmacol. 2013;16(4):783–789. doi:10.1017/S1461145712000880
25. Liu YW, Liong MT, Chung YE, et al. Effects of lactobacillus plantarum PS128 on children with autism spectrum disorder in Taiwan: a randomized, double-blind, placebo-controlled trial. Nutrients. 2019;11(4):820. doi:10.3390/nu11040820
26. DeVane CL, Charles JM, Abramson RK, et al. Pharmacotherapy of autism spectrum disorder: results from the randomized BAART clinical trial. Pharmacotherapy. 2019;39(6):626–635. doi:10.1002/phar.2271
27. Ichikawa H, Mikami K, Okada T, et al. Aripiprazole in the treatment of irritability in children and adolescents with autism spectrum disorder in Japan: a randomized, double-blind, placebo-controlled study. Child Psychiatry Hum Dev. 2017;48(5):796–806. doi:10.1007/s10578-016-0704-x
28. Ghanizadeh A, Moghimi-Sarani E. A randomized double blind placebo controlled clinical trial of N-Acetylcysteine added to risperidone for treating autistic disorders. BMC Psychiatry. 2013;13. doi:10.1186/1471-244X-13-196
29. Hardan AY, Fung LK, Libove RA, et al. A randomized controlled pilot trial of oral N-acetylcysteine in children with autism. Biol Psychiatry. 2012;71(11):956–961. doi:10.1016/j.biopsych.2012.01.014
30. Politte LC, Scahill L, Figueroa J, McCracken JT, King B, McDougle CJ. A randomized, placebo-controlled trial of extended-release guanfacine in children with autism spectrum disorder and ADHD symptoms: an analysis of secondary outcome measures. Neuropsychopharmacology. 2018;43(8):1772–1778. doi:10.1038/s41386-018-0039-3
31. Wang M, Jiang L, Tang X. Levetiracetam is associated with decrease in subclinical epileptiform discharges and improved cognitive functions in pediatric patients with autism spectrum disorder. Neuropsychiatr Dis Treat. 2017;13:2321–2326. doi:10.2147/NDT.S143966
32. Arnold LE, Luna RA, Williams K, et al. Probiotics for gastrointestinal symptoms and quality of life in autism: a placebo-controlled pilot trial. J Child Adolesc Psychopharmacol. 2019;29(9):659–669. doi:10.1089/cap.2018.0156
33. Niu M, Li Q, Zhang J, et al. Characterization of intestinal microbiota and probiotics treatment in children with autism spectrum disorders in China. Front Neurol. 2019;10. doi:10.3389/fneur.2019.01084
34. Shaaban SY, El Gendy YG, Mehanna NS, et al. The role of probiotics in children with autism spectrum disorder: a prospective, open-label study. Nutr Neurosci. 2018;21(9):676–681. doi:10.1080/1028415X.2017.1347746
35. Sprengers JJ, van Andel DM, Zuithoff NPA, et al. Bumetanide for core symptoms of autism spectrum disorder (BAMBI): a single center, double-blinded, participant-randomized, placebo-controlled, phase-2 superiority trial. J Am Acad Child Adolesc Psychiatry. 2021;60(7):865–876. doi:10.1016/j.jaac.2020.07.888
36. Chugani DC, Chugani HT, Wiznitzer M, et al. Efficacy of low-dose buspirone for restricted and repetitive behavior in young children with autism spectrum disorder: a randomized trial. J Pediatr. 2016;170:
37. Reddihough DS, Marraffa C, Mouti A, et al. Effect of fluoxetine on obsessive-compulsive behaviors in children and adolescents with autism spectrum disorders: a randomized clinical trial. JAMA. 2019;322(16):1561–1569. doi:10.1001/jama.2019.14685
38. Doaei S, Bourbour F, Teymoori Z, et al. The effect of omega-3 fatty acids supplementation on social and behavioral disorders of children with autism: a randomized clinical trial. Pediatr Endocrinol Diabetes Metab. 2021;27(1):12–18. doi:10.5114/pedm.2020.101806
39. Eslamzadeh M, Hebrani P, Behdani F, et al. Assessment the efficacy of atomoxetine in autism spectrum disorders: a randomized, double-blind, placebo-controlled trial. Iran J Psychiatry Behav Sci. 2018;12(2). doi:10.5812/ijpbs.10596
40. Lemonnier E, Degrez C, Phelep M, et al. A randomised controlled trial of bumetanide in the treatment of autism in children. Transl Psychiatry. 2012;2(12):e202. doi:10.1038/tp.2012.124
41. Lemonnier E, Villeneuve N, Sonie S, et al. Effects of bumetanide on neurobehavioral function in children and adolescents with autism spectrum disorders. Transl Psychiatry. 2017;7(3):e1056. doi:10.1038/tp.2017.10
42. Dai Y, Zhang L, Yu J, et al. Improved symptoms following bumetanide treatment in children aged 3−6 years with autism spectrum disorder: a randomized, double-blind, placebo-controlled trial. Sci Bull. 2021;66(15):1591–1598. doi:10.1016/j.scib.2021.01.008
43. Frye RE, Slattery J, Delhey L, et al. Folinic acid improves verbal communication in children with autism and language impairment: a randomized double-blind placebo-controlled trial. Mol Psychiatry. 2018;23(2):247–256. doi:10.1038/mp.2016.168
44. Parker KJ, Oztan O, Libove RA, et al. Intranasal oxytocin treatment for social deficits and biomarkers of response in children with autism. Proc Natl Acad Sci USA. 2017;114(30):8119–8124. doi:10.1073/pnas.1705521114
45. Yatawara CJ, Einfeld SL, Hickie IB, Davenport TA, Guastella AJ. The effect of oxytocin nasal spray on social interaction deficits observed in young children with autism: a randomized clinical crossover trial. Mol Psychiatry. 2016;21(9):1225–1231. doi:10.1038/mp.2015.162
46. Parker KJ, Oztan O, Libove RA, et al. A randomized placebo-controlled pilot trial shows that intranasal vasopressin improves social deficits in children with autism. Sci Transl Med. 2019;11(491). doi:10.1126/scitranslmed.aau7356
47. Brito AR, Vairo GPT, Dias A, Olej B, Nascimento OJM, Vasconcelos MM. Effect of prednisolone on language function in children with autistic spectrum disorder: a randomized clinical trial. J Pediatr (Rio J). 2021;97(1):22–29. doi:10.1016/j.jped.2019.10.012
48. Hendren RL, James SJ, Widjaja F, Lawton B, Rosenblatt A, Bent S. Randomized, placebo-controlled trial of methyl B12 for children with autism. J Child Adolesc Psychopharmacol. 2016;26(9):774–783. doi:10.1089/cap.2015.0159
49. Mazahery H, Conlon CA, Beck KL, et al. Inflammation (IL-1β) modifies the effect of vitamin D and omega-3 long chain polyunsaturated fatty acids on core symptoms of autism spectrum disorder-an exploratory pilot study(‡). Nutrients. 2020;12(3):661. doi:10.3390/nu12030661
50. Centre for Autism Research in Africa. Autism in an African context; 2017. Available from: http://www.cara.uct.ac.za/news/autism-african-context.
51. Clevenger S, Palffy A, Popescu R. Pharmacological treatments for the core symptoms of autism spectrum disorder: a systematic review. J Am Acad Child Adolesc Psychiatry. 2021;60(10):161–162. doi:10.1016/j.jaac.2021.09.085
52. Yu Y, Chaulagain A, Pedersen SA, et al. Pharmacotherapy of restricted/repetitive behavior in autism spectrum disorder: asystematic review and meta-analysis. BMC Psychiatry. 2020;20(1):121. doi:10.1186/s12888-020-2477-9
53. Persico AM, Ricciardello A, Lamberti M, et al. The pediatric psychopharmacology of autism spectrum disorder: a systematic review - Part I: the past and the present. Prog Neuropsychopharmacol Biol Psychiatry. 2021;110:110326. doi:10.1016/j.pnpbp.2021.110326
54. Fung LK, Mahajan R, Nozzolillo A, et al. Pharmacologic treatment of severe irritability and problem behaviors in autism: a systematic review and meta-analysis. Pediatrics. 2016;137(Suppl 2):S124–135. doi:10.1542/peds.2015-2851K
55. Rodrigues R, Lai MC, Beswick A, et al. Practitioner review: pharmacological treatment of attention-deficit/hyperactivity disorder symptoms in children and youth with autism spectrum disorder: a systematic review and meta-analysis. J Child Psychol Psychiatry. 2021;62(6):680–700. doi:10.1111/jcpp.13305
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.