Back to Journals » Neuropsychiatric Disease and Treatment » Volume 16
Pharmacological Intervention in Children with Autism Spectrum Disorder with Standard Supportive Therapies Significantly Improves Core Signs and Symptoms: A Single-Center, Retrospective Case Series
Authors Alsayouf HA ![]() , Talo H, Biddappa ML
, Talo H, Biddappa ML ![]() , Qasaymeh M
, Qasaymeh M ![]() , Qasem S
, Qasem S ![]() , De Los Reyes E
, De Los Reyes E ![]()
Received 16 August 2020
Accepted for publication 27 October 2020
Published 16 November 2020 Volume 2020:16 Pages 2779—2794
DOI https://doi.org/10.2147/NDT.S277294
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 6
Editor who approved publication: Dr Roger Pinder
Hamza A Alsayouf,1 Haitham Talo,1 Marisa L Biddappa,1 Mohammad Qasaymeh,2 Shadi Qasem,3 Emily De Los Reyes4
1Kids Neuro Clinic and Rehab Center, Dubai, United Arab Emirates; 2Pediatric Neurology, Dent Neurological Institute, Amherst, NY, USA; 3Pathology and Laboratory Medicine, University of Kentucky College of Medicine, Lexington, KY, USA; 4Pediatric Neurology, Nationwide Children’s Hospital and Ohio State University, Columbus, OH, USA
Correspondence: Hamza A Alsayouf
Kids Neuro Clinic and Rehab Center, Dubai Healthcare City, Dubai, United Arab Emirates
Tel +97 145570326
Email [email protected]
Purpose: Autism spectrum disorder (ASD) is a debilitating neurodevelopmental disorder with high heterogeneity and no clear common cause. Several drugs, in particular risperidone and aripiprazole, are used to treat comorbid challenging behaviors in children with ASD. Treatment with risperidone and aripiprazole is currently recommended by the Food and Drug Administration (FDA) in the USA for children aged 5 and 6 years and older, respectively. Here, we investigated the use of these medications in younger patients aged 4 years and older.
Patients and Methods: This retrospective case series included 18 children (mean age, 5.7 years) with ASD treated at the Kids Neuro Clinic and Rehab Center in Dubai. These patients began treatment with risperidone or aripiprazole at the age of 4 years and older, and all patients presented with comorbid challenging behaviors that warranted pharmacological intervention with either risperidone or aripiprazole.
Results: All 18 children showed objective improvement in their ASD core signs and symptoms. Significant improvement was observed in 44% of the cases, and complete resolution (minimal-to-no-symptoms) was observed in 56% of the cases as per the Childhood Autism Rating Scale 2-Standard Test (CARS2-ST) and the Clinical Global Impression (CGI) scales.
Conclusion: Our findings indicate that the chronic administration of antipsychotic medications with or without ADHD medications is well tolerated and efficacious in the treatment of ASD core and comorbid symptoms in younger children when combined with standard supportive therapies. This is the first report to suggest a treatment approach that may completely resolve the core signs and symptoms of ASD. While the reported outcomes indicate significant improvement to complete resolution of ASD, pharmacological intervention should continue to be considered as part of a multi-component intervention in combination with standard supportive therapies. Furthermore, the findings support the critical need for double-blind, placebo-controlled studies to validate the outcomes.
Keywords: risperidone, aripiprazole, antipsychotic, comorbid challenging behaviors
Plain Language Summary
ASD is a chronic neurodevelopmental disorder that is increasing in prevalence worldwide.
There are no FDA-approved medications to treat the core symptoms even though ASD shares many signs and symptoms with other neuropsychiatric diseases.
FDA-approved pharmacological therapies are currently only indicated for the treatment of comorbid irritability and severe behavioral issues in children with ASD aged 5 years and older.
In this study, antipsychotic medications, with or without ADHD medications, were found to significantly improve ASD core symptoms when used in combination with standard supportive therapies.
We observed complete resolution of core ASD symptoms in 56% of our patient cohort, which is unprecedented in the medical literature.
Dose optimization for each patient and chronic use are key to resolving core signs and symptoms.
The potential benefits and risks must be weighed on a case-by-case basis when considering further optimization of medications to target core symptoms in children with ASD and comorbid behavioral issues.
Introduction
Autism spectrum disorder (ASD) is a complex neurodevelopmental disorder with high heterogeneity.1 In 2013, the Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-5), consolidated the four previously separate categories of autism under the single umbrella of “autism spectrum disorder.”1 These categories were autistic disorder, Asperger’s syndrome, childhood disintegrative disorder, and pervasive developmental disorder not otherwise specified.1,2 While the symptoms of ASD can manifest before 2 years of age, they usually become more apparent between 2 and 3 years of age.1,3 Patients with ASD are all unique in their presentation; however, the disorder is characterized by core symptoms that include impairments in social interaction and communication, as well as the presence of restricted and repetitive behaviors.1 These symptoms are universal regardless of culture, race, ethnicity, or socioeconomic group.1 All children with ASD experience difficulty in developing social, speech, and behavioral skills. Therefore, early intervention with behavioral therapy affords these children with the best opportunity to support healthy development and to deliver benefits across their life span.2 Pharmacological interventions, where needed, are used as an adjunct to support patients’ function in their daily activities and to treat comorbid irritability and difficult behaviors.4,5
ASD impairs social skills and autonomy to a variable and sometimes severe extent. A longitudinal study over 40 years has shown general improvement in symptoms in young adulthood but poor outcomes in later adulthood.6 Although core domains may improve across the life span, some symptom subdomains, such as limited interests or facial expressions, may remain unchanged over time.7,8 The impact of these long-term deficits on functioning is severe, with manifestations that can become increasingly complex later in life.9 In 2018, the Centers for Disease Control and Prevention (CDC) in the USA determined that approximately 1 in 59 children is diagnosed with ASD (1 in 37 boys and 1 in 151 girls), with increasing prevalence year after year.10
Unfortunately, the current evidence-based pharmacological treatment approach for ASD is limited to the treatment and control of comorbid challenging behaviors only.11 Risperidone and aripiprazole were approved by the FDA in 2006 and 2009, respectively, to treat irritability associated with ASD.12,13 The recommended age to initiate treatment with these medications is 5 years and above for risperidone and 6 years and above for aripiprazole. In randomized controlled trials, risperidone and aripiprazole have been found to improve irritability and agitation in children with ASD.14,15 The majority of children with ASD show improvements in challenging comorbid behaviors such as irritability, agitation, aggression, self-injury, and disruptive behaviors when using these medications.16 Both drugs are classified as atypical antipsychotics, and this class of medication can potentially cause significant side effects such as sedation, weight gain, and metabolic disturbances; therefore, close follow-up and monitoring by a physician with special expertise are required when using these medications.17 To mitigate medication-induced weight gain, metformin can be prescribed if needed.17,18 Several medications typically used to treat children with attention-deficit hyperactivity disorder (ADHD), including methylphenidate, atomoxetine, guanfacine, and bupropion, have been reported to also improve hyperactivity and attention symptoms in children with ASD.19–22
In this retrospective report, we present our single-center experience in treating 18 children with ASD and comorbid behavioral issues. These children were treated from the age of 4 years and older with risperidone or aripiprazole, either with or without atomoxetine or methylphenidate, combined with standard supportive therapies. A significant clinical and statistical improvement in the patients’ core signs and symptoms, in addition to improvements in their behavioral issues, was observed as per the Childhood Autism Rating Scale 2-Standard Test (CARS2-ST) and the Clinical Global Impression (CGI) scales.23,24 The Clinical Global Impression-Severity (CGI-S) and CARS2-ST scale were performed at baseline, and serial Clinical Global Impression-Improvement (CGI-I) scores were obtained to monitor improvement. Once a patient attained a CGI-I score of 1 or 2 we repeated the CGI-S and CARS2-ST to further confirm improvement, in addition to serial clinical evaluations and follow-up.
Patients and Methods
Patients
This is a retrospective case series report of all patients, aged 4 years or older, who were diagnosed with autism spectrum disorder and comorbid behavioral issues and treated at our center (Kids Neuro Clinic and Rehab Center, Dubai) from 2017 to 2020, and for whom informed consent was obtained from the parents or legal guardians to participate in this study. The cohort comprised 18 children in total. The children’s parents and legal guardians were duly notified of the off-label use and potential side effects of the antipsychotic medications used in this study. The data collected for each patient included: age at presentation, age of initiation of the first medication, medications used, starting dose, time to reach the maximum dose, current medications, medication side effects, analyses performed, initial signs and symptoms, initial formal diagnosis as per the DSM-5 criteria and CARS2-ST, baseline CGI-S score before starting medications, Clinical Global Impression-Improvement (CGI-I) score, and their repeat CARS2-ST as per their last visit to our clinic.
To supplement the CGI-I scale, we also used the CGI-S score in addition to CARS2-ST at baseline against which we marked each patient’s severity prior to starting medications. Condition severity was scored on the following seven-point CGI-S scale: 1 = normal, not at all ill; 2 = borderline mentally ill; 3 = mildly ill; 4 = moderately ill; 5 = markedly ill; 6 = severely ill; 7 = among the most extremely ill patients.23
CGI-I is scored on a seven-point scale that compares the patient’s current condition to their baseline condition before treatment initiation: 1 = very much improved since the initiation of treatment; 2 = much improved; 3 = minimally improved; 4 = no change from baseline (the initiation of treatment); 5 = minimally worse; 6 = much worse; 7 = very much worse since the initiation of treatment.23
CARS2-ST can be used for children aged 2 years and older and classifies patients into three ASD severity groups based on a 15-category scoring system: minimal-to-no symptoms of ASD, mild-to-moderate symptoms of ASD, and severe symptoms of ASD.5,24,25
This retrospective observational case series was approved by an independent Institutional Review Board (IRB), the Pearl IRB Committee, which is fully accredited by the Association for the Accreditation of Human Research Protection Program (AAHRPP; approval no. 20-KNRC-101). This study was also approved locally by the Dubai Healthcare City Regulatory Ethics Committee (DHCR; approval no. KNCRC-01)
Diagnosis
When a patient with signs and symptoms suggestive of ASD presented at our clinic, we performed a thorough history and physical examination. In addition, we performed an electroencephalogram (EEG) with a sleep sample to evaluate for electrical status epilepticus in sleep or epileptic encephalopathy, as well as an auditory brainstem response (ABR) test to assess for hearing loss. These tests were conducted to exclude potentially treatable conditions requiring different treatment approaches.26–29 Pharmacological treatment was recommended if the individual had a normal ABR, normal EEG, no findings suggestive of a genetic disorder (such as dysmorphic features, a family history of genetic disorders, or an abnormal genetic test), no global developmental delay, and a confirmed ASD diagnosis as per the DSM-5 criteria and CARS2-ST, and a CGI-S score ≥ 4 with comorbid behavioral issues. In each case, the diagnosis was obtained by both a pediatric neurologist and a clinical psychologist following a multidisciplinary assessment and diagnostic approach. A flowchart of the diagnosis and medication schedule is depicted in Figure 1.
 |
Figure 1 Flowchart of the diagnosis and medication schedule. |
Treatment
Based on previous safety and efficacy studies recommending atypical antipsychotics for the treatment of the comorbid behavioral symptoms of ASD, patients were prescribed either risperidone or aripiprazole.12,13 Risperidone treatment was usually initiated with 0.25 mg orally at night, and this dose was increased gradually every 1 to 2 weeks until reaching either a maximum dose of 2 mg in the morning and 0.5 mg at night or the maximum dose tolerated by each patient within these limits (see Table 1 for each patient’s dosing schedule). This regimen was adhered to as long as the patient showed improvement with each dose increment and no side effects. This approach was followed for 8/18 (44%) cases (cases 1, 6, 7, 9, 10, 14, 17, and 18). Aripiprazole was started at 1 mg at night, and this dose was increased gradually every 1 to 2 weeks until reaching a maximum dose of 15 mg at night or the maximum tolerated dose for the patient (Table 1). This regimen was adhered to as long as an improvement was observed with no side effects. This approach was followed for 10/18 (56%) cases (cases 2, 3, 4, 5, 8, 11, 12, 13, 15, and 16). The clinical data for all of the patients are provided in Table 1.
 | 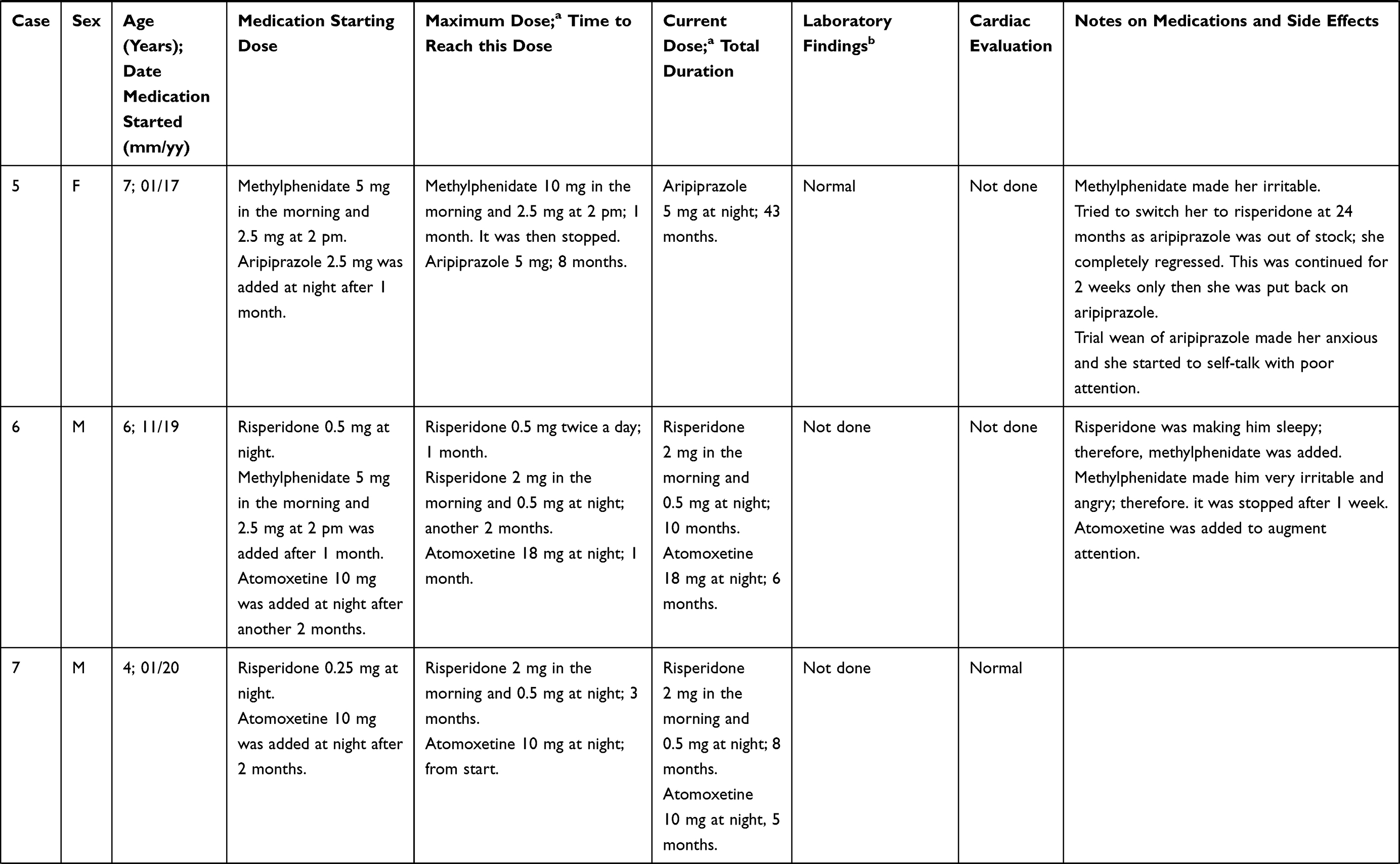 | 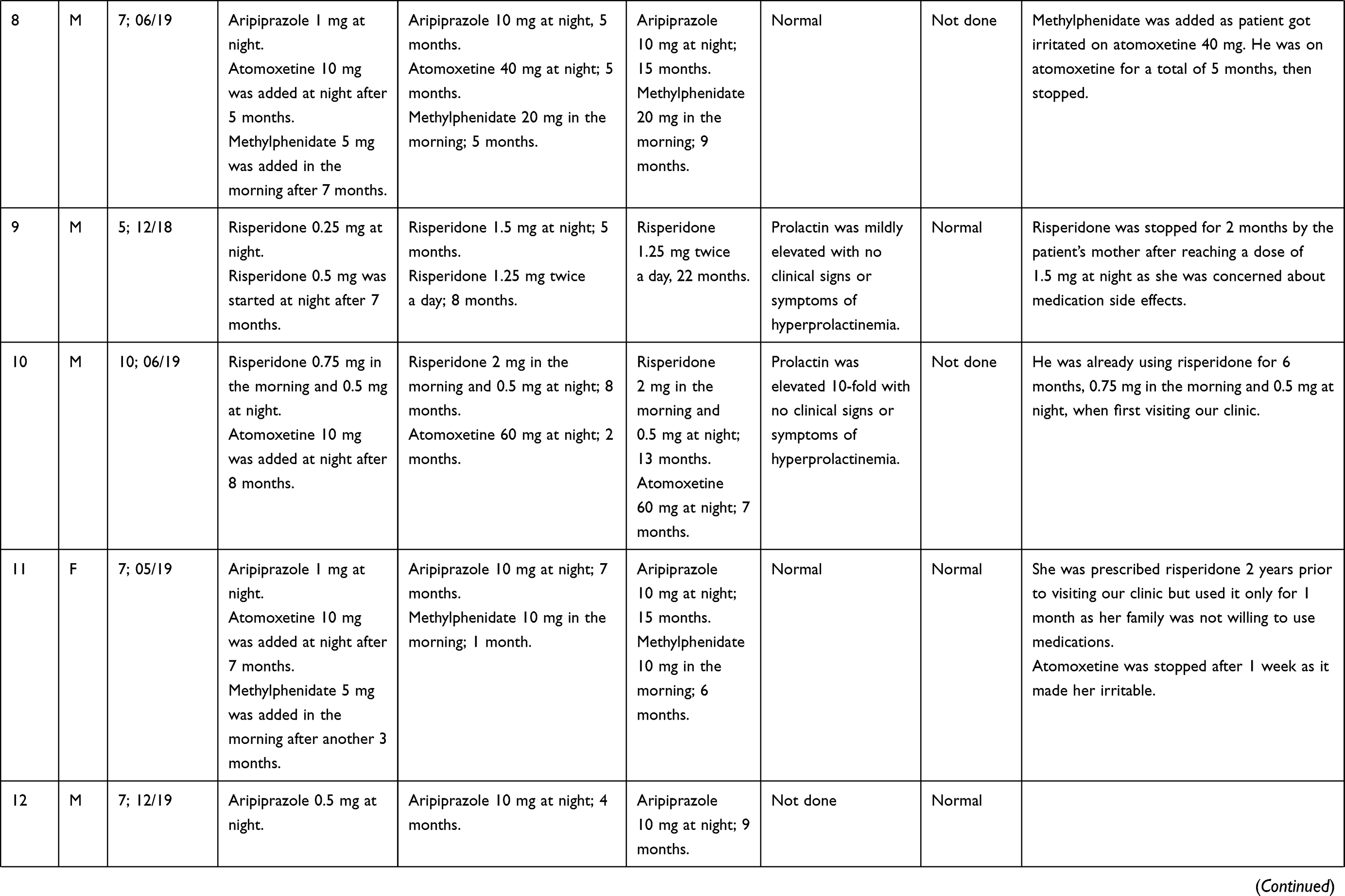 | 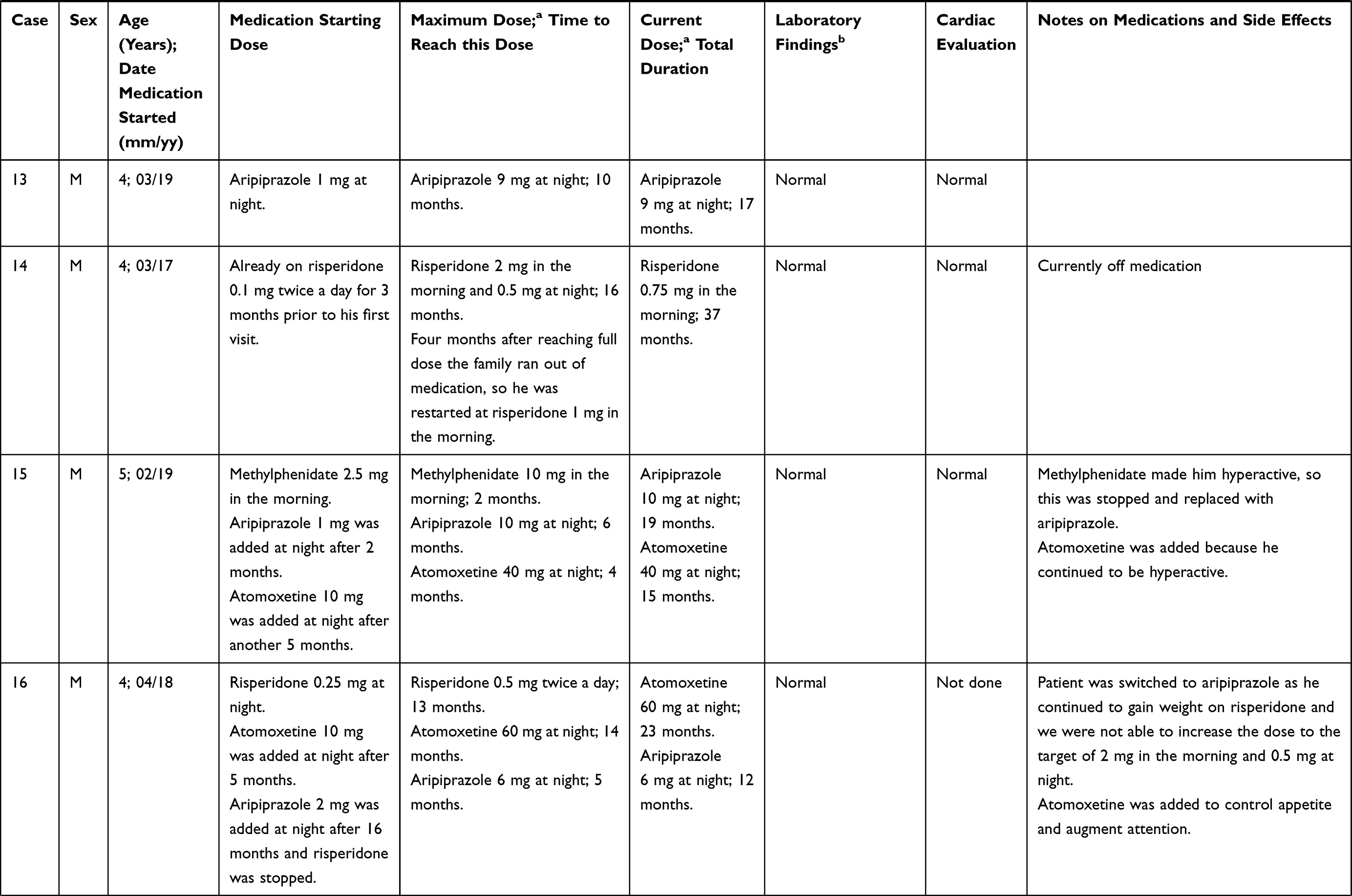 |
Table 1 Clinical Characteristics of All Patients in the Case Series |
When a patient tolerated risperidone or aripiprazole with no side effects and showed progressive improvement to a CGI-I score of 1 or 2, the child was continued on that medication. If the CGI-I score plateaued at 2 or higher, or the patient started to gain excessive weight and still exhibited hyperactivity or an inadequate attention span, methylphenidate or atomoxetine was added in an effort to augment improvement to a CGI-I score of 1, improve their attention span, and control excessive weight gain (these classes of medication are known to suppress appetite). All children with progressive weight gain were also referred to a nutritionist since progressive weight gain can cause serious health issues and may affect compliance with therapy and lead to the premature tapering of the medication.
Methylphenidate was usually added at 2.5 mg in the morning and increased gradually to a maximum dose of 20 mg in the morning or less as tolerated. Atomoxetine was usually added at 10 mg at night and increased gradually to a maximum dose of 60 mg at night or less as tolerated, as long as no side effects were observed and an improvement was seen with each dose increment (Table 1). Once a patient reached a CGI-I score of 1 and a repeat CARS2-ST score of minimal-to-no symptoms of ASD, we continued the medications for an additional 6 months before trying to wean the child very slowly off the medications (Figure 1 describes the process used for weaning).
Before the initiation of therapy, a complete blood count, kidney function test, and lipid panel were performed, and the levels of electrolytes, liver enzymes, hemoglobin A1c, and prolactin were determined to provide a baseline for monitoring any metabolic side effects of the antipsychotic medications.30–34 The tests were repeated 3 to 6 months after initiating medication, followed by subsequent yearly checkups. Similarly, cardiac evaluations to monitor for any adverse medication effects, including an echocardiogram and electrocardiogram, were obtained by a fully trained pediatric cardiologist for half of the patients 9/18 (50%) when the maximum dose was reached or earlier if clinically indicated.35–37 Serial measurements of weight, body mass index (BMI), height, and vital signs were obtained for each patient at every office visit.
The initial presenting and current signs and symptoms of each patient, initial and current CARS2-ST scores, initial diagnosis as per the DSM-5 criteria, baseline CGI-S score, and current CGI-S and CGI-I scores are described in Supplementary Table S1.
All patients were strongly advised to continue the standard supportive therapies, such as applied behavior analysis (ABA) therapy, speech therapy, and occupational therapy. Where a family could not afford these therapies, the parents and caregivers were provided practical support and guidance as per our center’s practice. All parents and caregivers were strongly encouraged to maximize their child’s opportunity for social interactions by attending a daycare, nursery, or playgroups, as well as strongly advised to limit their child’s screen time where applicable.
Statistical Analysis
The statistical significance of the differences between the mean pre- and post-treatment CGI-S and CARS2-ST scores was determined with the Wilcoxon signed-rank test. A P-value < 0.05 was considered statistically significant. Data were analyzed using the VassarStats online suite of statistical tools (www.vassarstats.net).
Results
In total, 18 cases of ASD were included in this study, comprising 14 males and 4 females with a 3.5:1 male-to-female ratio. The age of the patients at presentation ranged from 4 to 10 years (mean age 5.7 years). The duration of treatment ranged from 6 to 43 months (mean 18.3 months). Eight patients (44%) were started on risperidone and 10 patients (56%) were started on aripiprazole. Efficacy of treatment was based on the changes in the CGI-I score from baseline, the repeat CARS2-ST score, family reports, and clinical observations of the treating physician.
In total, 10/18 (56%) patients attained a CGI-I score of 1 and had minimal-to-no symptoms of ASD (ie, complete resolution of ASD symptoms) when reassessed with the CARS2-ST, while the remaining 8/18 (44%) patients attained a CGI-I of 2 and a reassessment using CARS2-ST showed significant improvement from their baseline score. The differences in the mean CGI-S and CARS2-ST scores pre- and post-treatment in our cohort were statistically significant (Z = 3.71, P < 0.001 for both) using the Wilcoxon signed-ranked test, with pre- and post-treatment median values of 5 and 1 for CGI-S, respectively, and 35 and 22 for CARS2-ST, respectively.
Among the eight patients who were treated with risperidone with or without methylphenidate or atomoxetine in this case series, 5/8 patients (62%) achieved a CGI-I score of 1 and minimal-to-no-symptoms of ASD when reassessed on the CARS2-ST (cases 1, 9, 10, 14, and 18). The other 3/8 patients (38%) achieved a CGI-I score of 2 and their repeat CARS2-ST showed significant improvement from baseline (cases 6, 7, and 17). Two of the eight patients (25%) continued with risperidone only and did not require any adjunct therapy for attention issues (cases 9 and 14).
Among the 10 patients who were treated with aripiprazole with or without atomoxetine or methylphenidate in this case series, 6/10 patients (60%) achieved a CGI-I score of 1 with a normal repeat CARS2-ST (cases 2, 3, 4, 5, 8, and 13), and 4/10 patients (40%) achieved a CGI-I score of 2 and their repeat CARS2-ST showed significant improvement from baseline (cases 11, 12, 15, and 16). The remaining 3/10 patients (30%) did not require any adjunct therapy to aid attention (cases 3, 12, and 13).
Three patients (cases 2, 16, and 17) showed clear improvement on monotherapy with risperidone or aripiprazole to a CGI-I score of 1 or 2 but started to exhibit excessive weight gain (BMI > 25) with attention deficit; therefore, atomoxetine or methylphenidate was added. One patient (case 4) continued to be inattentive on aripiprazole 15 mg and atomoxetine 40 mg at night; therefore, long-acting methylphenidate was added in the morning and the dose was increased to 36 mg. This combination improved his attention greatly and further improved his CGI-I score from 2 to 1 with minimal-to-no symptoms of ASD on his repeat CARS2-ST. One patient (case 16) started to gain excessive weight with no clear improvement with risperidone dose increments; therefore, he was switched to aripiprazole with clear improvement. Two patients (cases 1 and 11) did not tolerate or did not show clear clinical improvement with atomoxetine as an adjunct therapy and were switched to methylphenidate with superior results. Three patients (cases 6, 15, and 17) who did not show clear improvement on methylphenidate as an adjunct therapy or who started to be irritable were switched to atomoxetine with clear improvement. One patient attained a CGI-I score of 1 and had minimal-to-no-symptoms of ASD when reassessed on the CARS2-ST, and he is currently off all medications after being on risperidone for a total of 37 months (case 14). One patient is on a maintenance dose only to control symptoms of anxiety and self-talking, currently attends regular school, and had minimal-to-no-symptoms of ASD when reassessed on the CARS2-ST (case 5). All medication regimens are presented in Table 1.
One family stopped risperidone prematurely due to concerns about medication side effects, and this resulted in a clear regression of the patient (case 9) to his original status. Risperidone was then restarted. The parents of one patient (case 14) ran out of medication 20 months after starting risperidone and 4 months after reaching the full dose of 2 mg in the morning and 0.5 mg at night. The family noted that during the 4 weeks that he was off medication, the child became hyperactive again and inattentive but did not relapse to his initial ASD symptoms. That he did not completely relapse may be explained by the fact that he had already been on risperidone for 20 months, in comparison with case 13, who had only been on risperidone for 5 months. Of note, one patient (case 5) completely regressed when she was switched to risperidone from aripiprazole when aripiprazole was out of stock, and she was, therefore, placed back on aripiprazole as soon as it became available again. Another patient (case 18) was already on risperidone and atomoxetine for almost a year when she presented to us but was still showing signs and symptoms of ASD. Once the doses were optimized, she attained a CGI-I score of 1 and had minimal-to-no-symptoms of ASD when reassessed on the CARS2-ST.
Laboratory results for our patients (complete blood count, electrolytes, liver enzymes, kidney function test, lipid panel, and hemoglobin A1c) were all within normal limits for their age. Three patients (17%; cases 9, 10, and 14) developed asymptomatically elevated prolactin levels and were treated conservatively as per the recommendations of a pediatric endocrinologist. Cardiac monitoring did not reveal any adverse effects. Some families were unable to afford cardiac evaluation or unwilling to undergo it, in which case the patients were monitored clinically for any signs or symptoms of cardiac issues, but none showed any adverse cardiac effects.
Discussion
Altered neuronal connectivity and plasticity in the brain cortex are reported to be the underlying cause for the signs and symptoms observed in ASD patients.38–41 In mice with ASD, the prefrontal cortex appears to be the main site of brain pathology.42–45 Aman et al reported a considerable improvement in irritability and maladaptive behavior in comparison to the baseline, including core symptoms associated with ASD, in ASD patients who had been treated with risperidone for an average of 21 months.46 Recent studies in mice have shown that the chronic administration of risperidone or aripiprazole improves valproic acid-induced social interaction deficits and recognition memory impairment, with reductions observed in dendritic spine density in the prefrontal cortex and hippocampus.47 In addition, methylphenidate and atomoxetine were both found to improve valproic acid-induced social deficits and recognition memory impairment in mice.48
The financial and social burden of ASD is huge and expected to rise substantially in the coming years.10 For example, intensive behavioral interventions for children with ASD cost from $40,000 to $60,000 per child in the USA in 2011.49 The lifelong cost of supporting an individual with ASD and intellectual disability is estimated to be $2.4 million in the USA and £1.5 million ($2.2 million) in the UK.50 Residential care or supportive living accommodation during adulthood and individual productivity loss both contribute to these high costs.50 Caring for Americans with ASD cost society a staggering $268 billion in 2015, a number that has increased more than six-fold since 2006 and is expected to rise to $461 billion by 2025 in the absence of more effective interventions and support across patients’ life spans.10,51 Therefore, finding a successful treatment for ASD is a global necessity.
For this case series, children who presented with ASD and comorbid challenging behaviors at our center were started on the antipsychotics risperidone or aripiprazole provided their parents or legal guardians agreed with the treatment plan and understood the off-label use of such medications. We titrated medication doses to also target core symptoms and not just control challenging behaviors. We combined two proven therapeutic approaches, namely non-biological (eg, ABA therapy) and biological therapies (risperidone and aripiprazole), to treat children with ASD in a region where the vast majority cannot afford full supportive therapies. We added ADHD medications as needed to further augment attention as attention is crucial in the learning process. This intervention approach is based on our initial observations that these medications improved many aspects of ASD symptoms when used to control comorbid behavior as indicated by the FDA. We noted that treating difficult comorbid behavior, anxiety, poor attention, and hyperactivity made ASD patients a lot more responsive and receptive to supportive therapies. In addition, many previous studies and reports support the use of these medications in young children with ASD.14–17,19,20 Several studies have shown improvements in the core symptoms of children with ASD when using risperidone or aripiprazole, including language impairment, maladaptive behaviors, social withdrawal, stereotypy, sensory motor issues, inappropriate speech, and ADHD.52–58 Troost et al, in their placebo discontinuation study, reported that risperidone helped prevent relapses in problem behaviors in children with ASD when used for 6 months, and the authors concluded that these results provide a rationale for the continued use of risperidone beyond 6 months with close observation for weight gain.59
Here, the medication doses were slowly increased to the maximum dose tolerated and this regimen was maintained as long as the patient continued to show improvement and the maximum allowed dose had not been reached. If the patient did not respond to risperidone, the patient was shifted to aripiprazole or vice versa. Patients who responded initially but then plateaued over subsequent dose increments were supplemented with atomoxetine or methylphenidate to help increase attention, control hyperactivity, and attain further improvement. Patients who continued to improve with risperidone or aripiprazole increments but started to experience side effects, such as excessive weight gain along with attention deficit and/or hyperactivity, were also supplemented with atomoxetine or methylphenidate to control their weight and further improve their attention span. Our goal was to achieve a low CGI-I score with minimal-to-no-symptoms of ASD as per the CARS2-ST and clinical evaluation.
We used the DSM-5 criteria and CARS2-ST to confirm the diagnosis of ASD. The CGI scale and CARS2-ST were used to measure baseline severity and to monitor improvement. The American Academy of Child and Adolescent Psychiatry (AACAP), in its 2014 ASD practice parameters, emphasized that the most important diagnostic step is clinical diagnosis based on careful consideration of the DSM-5 criteria.4 These guidelines further emphasize that while there are many assessment instruments for ASD, including the childhood autism rating scale (CARS) and the autism diagnostic observation scale (ADOS) among others, these instruments, if needed, should only supplement and not replace informed clinical judgment based on the DSM-5 criteria. The American Academy of Pediatrics (AAP), in its latest ASD clinical report published in 2020, emphasized the importance of using the DSM-5 criteria and definitions for the clinical diagnosis of ASD.5 Severity ratings of DSM-5 criteria do not provide a quantifiable score and are based on the extent of the patient’s social communication impairments, their restricted and repetitive patterns of behavior, and the resultant level of care the individual requires; thus, these ratings often reflect the impact of cognitive limitations.5,60 In contrast, the CGI-I scale offers an objective, readily understood, and practical measurement tool that can be easily applied even in a very busy clinical setting. It has two main features that make it suitable for ASD patients and treatment trials: there is scope for cross-comparison with the many other trials in which the CGI-I rating scale has been used in psychiatry, and it reflects general severity and clinical improvement even in small ASD studies, especially when combined with a standard ASD test like CARS2-ST.60,61 Therefore, in addition to clinical diagnosis based on the DSM-5 criteria, which also provides a severity scale, we included CARS2-ST and the CGI scales to try to maximize sensitivity and specificity in diagnosis and when monitoring for improvement among our patients.5,7,60 Diagnosis in each case was made by a team comprising both a pediatric neurologist and clinical psychologist.
In this case series, while risperidone or aripiprazole was started at an earlier age than that recommended by the FDA to primarily control behavioral issues, the off-label use of risperidone, aripiprazole, and other psychotropic medications is well described in common practice with a trend of increasing use in recent years, especially in preschool children with ASD.62–68 Treating our patients with early and chronic administration of risperidone or aripiprazole along with standard supportive therapies, supplemented with methylphenidate or atomoxetine as needed to augment attention, resulted in marked and statistically significant clinical improvement with minimal-to-no-symptoms (resolution of symptoms) of ASD in 56% of these patients as per the CGI-S scale, CARS2-ST, and clinical evaluation.
This is a single-center case series of children with ASD who were treated successfully with the antipsychotic drugs risperidone and aripiprazole in combination with atomoxetine or methylphenidate along with standard supportive therapies. These medications have been available on the market for over a decade and have been used to treat psychiatric disorders that share many features with ASD.69,70 Recent meta-analyses concluded that patients with ASD have a high burden of comorbid neuropsychiatric disorders such as anxiety disorders, depressive disorders, bipolar and mood disorders, schizophrenia spectrum, suicidal behavior disorders, attention-deficit/hyperactivity disorder, as well as disruptive, impulse-control, and conduct disorders and may share underlying brain circuit disruption or pathology.69,70 The improvements in symptoms in our patient cohort are likely due to the following: initiating risperidone or aripiprazole as soon as a diagnosis was made and as young as 4 years to control challenging behavior that can be a major barrier for learning, prescribing medications to control challenging behavior and target the core symptoms under the assumption that all ASD core symptoms are neuropsychiatric in nature and need to be treated the same way, and slowly increasing the medication doses to the maximum tolerated or highest dose allowed to achieve significant clinical improvement with an individualized treatment plan. These medications need to be used for many months to result in minimal-to-no-symptoms of ASD signs and symptoms, and treatment requires combining antipsychotic drugs with medications used for attention deficit hyperactivity as needed, to augment attention and control hyperactivity. This must be performed in a manner that is tailored to each patient’s response, as attention plays a critical role in the learning process. Unfortunately, all double-blind, placebo-controlled studies performed to date on ASD were of short duration, used medications to primarily control challenging behaviors in children with ASD, did not combine antipsychotic medications with ADHD medications, and did not include cross-over design for non-responders.14,15,56,71–78
The main side effects noted were weight gain, sedation, drooling, and irritability. Sedation and drooling were noted mainly when first initiating the medications, were mild in nature, and disappeared with continuation of the medications. This could be related to the very slow titration schedule we used for our patients. Weight gain was excessive, uncontrollable (BMI > 25), and required further intervention in only five patients (17%).
A major challenge we faced in our approach was to convince the families to start or continue using the medications once they were duly informed about the side effects of the medications and their FDA-approved uses.
The findings of this case series are limited because of the small sample size and retrospective nature of the data collection. These factors might have caused an inherent bias in the results. Cardiac evaluations were not performed for all patients, mainly because of affordability issues or the families being unwilling.
Conclusions
Our study showed clinically and statistically significant improvement of ASD patients’ core signs and symptoms as per the CGI scales and CARS2-ST with early and chronic administration of risperidone or aripiprazole, with or without ADHD medications, and combined with standard supportive therapy. Our findings suggest that a notable proportion of patients with ASD can be successfully treated and potentially cured this way. Early intervention with behavioral therapy and pharmacological medications provide the best opportunity to support normal development in children with ASD. No one medication works for all children, and a trial of other antipsychotic medications should be used if a patient fails to respond to the first medication tried. While reported outcomes indicate significant improvement in the core signs and symptoms of ASD, pharmacological intervention should continue to be considered as part of a multi-component intervention in combination with standard supportive therapies. The potential benefits and risks must be weighed on a case-by-case basis when considering the use of medications to target core symptoms in children with ASD. Double-blind, placebo-controlled studies should be conducted to verify the findings of our study. Finding an effective treatment for ASD is of utmost importance because of its increasing prevalence, its poorly understood causes and pathology, and its devastating consequences.
Data Sharing Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
This retrospective observational case series was deemed by an independent Institutional Review Board (IRB), the Pearl IRB Committee, which is fully accredited by the Association for the Accreditation of Human Research Protection Program (AAHRPP), as exempt according to FDA 21 CFR 56.104 and 45CFR46.104(b)(4): (4) Secondary Research Uses of Data or Specimens on 06/01/2020 (approval no. 20-KNRC-101). This study was also approved locally by the Dubai Healthcare City Regulatory Ethics Committee (DHCR; approval no. KNCRC-01). Informed consent to participate in this study and publish the case details was obtained from the parents or legal guardians of all patients.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests.
References
1. American Psychiatric Association. DSM-5 Task Force. Diagnostic and Statistical Manual of Mental Disorders: DSM-5.
2. Zwaigenbaum L, Bauman ML, Choueiri R, et al. Early intervention for children with autism spectrum disorder under 3 years of age: recommendations for practice and research. Pediatrics. 2015;136(Suppl 1):S60–81. doi:10.1542/peds.2014-3667E
3. Carbone PS, Campbell K, Wilkes J, et al. Primary care autism screening and later autism diagnosis. Pediatrics. 2020;146(2):e20192314. doi:10.1542/peds.2019-2314
4. Volkmar F, Siegel M, Woodbury-Smith M, King B, McCracken J, State M. Practice parameter for the assessment and treatment of children and adolescents with autism spectrum disorder. J Am Acad Child Adolesc Psychiatry. 2014;53(2):237–257. doi:10.1016/j.jaac.2013.10.013
5. Hyman SL, Levy SE, Myers SM. For council on children with disabilities, section on developmental and behavioral pediatrics. Identification, evaluation, and management of children with autism spectrum disorder. Pediatrics. 2020;145(1):e20193447. doi:10.1542/peds.2019-3447
6. Magiati I, Tay XW, Howlin P. Cognitive, language, social and behavioural outcomes in adults with autism spectrum disorders: a systematic review of longitudinal follow-up studies in adulthood. Clin Psychol Rev. 2014;34(1):73–86. doi:10.1016/j.cpr.2013.11.002
7. Esbensen AJ, Seltzer MM, Lam KS, Bodfish JW. Age-related differences in restricted repetitive behaviors in autism spectrum disorders. J Autism Dev Disord. 2009;39(1):57–66.
8. Bal VH, Kim SH, Fok M, Lord C. Autism spectrum disorder symptoms from ages 2 to 19 years: implications for diagnosing adolescents and young adults. Autism Res. 2019;12(1):89–99. doi:10.1002/aur.2004
9. Militerni R, Bravaccio C, Falco C, Fico C, Palermo MT. Repetitive behaviors in autistic disorder. Eur Child Adolesc Psychiatry. 2002;11(5):210–218.
10. Centers for Disease Control. Data & statistics on autism spectrum disorder; 2018. Available from: https://www.cdc.gov/ncbddd/autism/data.html.
11. Lord C, Elsabbagh M, Baird G, Veenstra-Vanderweele J. Autism spectrum disorder. Lancet. 2018;392(10146):508–520. doi:10.1016/S0140-6736(18)31129-2
12. Food and Drug Administration. Approval for risperdal (risperidone) in the treatment of irritability associated with autistic disorder; 2006. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2006/020272Orig1s036,s041,020588Orig1s024,s028,s029,21444Orig1s008,s015.pdf.
13. Squibb BM. U.S. Food and Drug Administration approves ABILIFY® (aripiprazole) for the treatment of irritability associated with autistic disorder in pediatric patients (ages 6 to 17 years); 2009. Available from: http://news.bms.com/press-release/rd-news/us-food-and-drug-administration-approves-abilify-aripiprazole-treatment-irrita.
14. Kent JM, Kushner S, Ning X, et al. Risperidone dosing in children and adolescents with autistic disorder: A double-blind, placebo-controlled study. J Autism Dev Disord. 2013;43(8):1773–1783. doi:10.1007/s10803-012-1723-5
15. Owen R, Sikich L, Marcus RN, et al. Aripiprazole in the treatment of irritability in children and adolescents with autistic disorder. Pediatrics. 2009;124(6):1533–1540. doi:10.1542/peds.2008-3782
16. Fung LK, Mahajan R, Nozzolillo A, et al. Pharmacologic treatment of severe irritability and problem behaviors in autism: A systematic review and meta-analysis. Pediatrics. 2016;137(Suppl 2):S124–135. doi:10.1542/peds.2015-2851K
17. Politte LC, McDougle CJ. Atypical antipsychotics in the treatment of children and adolescents with pervasive developmental disorders. Psychopharmacology. 2014;231(6):1023–1036. doi:10.1007/s00213-013-3068-y
18. Anagnostou E, Aman MG, Handen BL, et al. Metformin for treatment of overweight induced by atypical antipsychotic medication in young people with autism spectrum disorder: A randomized clinical trial. JAMA Psychiatry. 2016;73(9):928–937. doi:10.1001/jamapsychiatry.2016.1232
19. Sturman N, Deckx L, van Driel ML. Methylphenidate for children and adolescents with autism spectrum disorder. Cochrane Database Syst Rev. 2017;11(11):CD011144.
20. Handen BL, Aman MG, Arnold LE, et al. Atomoxetine, parent training, and their combination in children with autism spectrum disorder and attention-deficit/hyperactivity disorder. J Am Acad Child Adolesc Psychiatry. 2015;54(11):905–915. doi:10.1016/j.jaac.2015.08.013
21. Scahill L, McCracken JT, King BH, et al. Extended-release guanfacine for hyperactivity in children with autism spectrum disorder. Am J Psychiatry. 2015;172(12):1197–1206. doi:10.1176/appi.ajp.2015.15010055
22. Ng QX. A systematic review of the use of bupropion for attention-deficit/hyperactivity disorder in children and adolescents. J Child Adolesc Psychopharmacol. 2017;27(2):112–116. doi:10.1089/cap.2016.0124
23. Busner J, Targum SD. The clinical global impressions scale: applying a research tool in clinical practice. Psychiatry. 2007;4(7):28–37.
24. Dawkins T, Meyer AT, Van Bourgondien ME. The relationship between the childhood autism rating scale: second edition and clinical diagnosis utilizing the DSM-IV-TR and the DSM-5. J Autism Dev Discord. 2016;46(10):3361–3368. doi:10.1007/s10803-016-2860-z
25. Schopler E, Van Bourgondien ME, Wellman GJ, Love SR. Childhood Autism Rating Scale.
26. Yilmaz S, Serdaroglu G, Akcay A, Gokben S. Clinical characteristics and outcome of children with electrical status epilepticus during slow wave sleep. J Pediatr Neurosci. 2014;9(2):105–109. doi:10.4103/1817-1745.139266
27. Hergüner MO, Incecik F, Altunbaşak S, Kiriş N. Clinical characteristics of 10 patients with continuous spikes and waves during slow sleep syndrome. Pediatr Neurol. 2008;38(6):411–414. doi:10.1016/j.pediatrneurol.2008.02.007
28. Brian JA, Zwaigenbaum L, Ip A. Standards of diagnostic assessment for autism spectrum disorder. Paediatr Child Health. 2019;24(7):444–551. doi:10.1093/pch/pxz117
29. Nachshen J, Garcin N, Moxness K, et al. Screening, Assessment, and Diagnosis of Autism Spectrum Disorders in Young Children: Canadian Best Practice Guidelines. Montreal, Quebec: Miriam Foundation; 2008.
30. American Diabetes Association, American Psychiatric Association, American Association of Clinical Endocrinologists, North American Association for the Study of Obesity. Consensus development conference on antipsychotic drugs and obesity and diabetes. Diabetes Care. 2004;27(2):596–601. doi:10.2337/diacare.27.2.596
31. Ho J, Panagiotopoulos C, McCrindle B. for Canadian Alliance for Monitoring Effectiveness and Safety of Antipsychotics in Children (CAMESA) guideline group. Management recommendations for metabolic complications associated with second generation antipsychotic use in children and youth. Paediatr Child Health. 2011;16(9):575–580.
32. Kimura G, Kadoyama K, Brown JB, et al. Antipsychotics-associated serious adverse events in children: an analysis of the FAERS database. Int J Med Sci. 2015;12(2):135–140. doi:10.7150/ijms.10453
33. Roke Y, van Harten PN, Boot AM, Buitelaar JK. Antipsychotic medication in children and adolescents: A descriptive review of the effects on prolactin level and associated side effects. J Child Adolesc Psychopharmacol. 2009;19(4):403–414. doi:10.1089/cap.2008.0120
34. Haddad PM, Wieck A. Antipsychotic-induced hyperprolactinaemia: mechanisms, clinical features and management. Drugs. 2004;64(20):2291–2314. doi:10.2165/00003495-200464200-00003
35. Correll CU, Manu P, Olshanskiy V, Napolitano B, Kane JM, Malhotra AK. Cardiometabolic risk of second-generation antipsychotic medications during first-time use in children and adolescents. JAMA. 2009;302(16):1765–1773. doi:10.1001/jama.2009.1549
36. Jensen KG, Juul K, Fink-Jensen A, Correll CU, Pagsberg AK. Corrected QT changes during antipsychotic treatment of children and adolescents: A systematic review and meta-analysis of clinical trials. J Am Acad Child Adolesc Psychiatry. 2015;54(1):25–36. doi:10.1016/j.jaac.2014.10.002
37. Rizzo R, Gulisano M, Cali PV, Di Pino A. Mandatory electrocardiographic monitoring in young patients treated with psychoactive drugs. Eur Child Adolesc Psychiatry. 2013;22(9):577–579. doi:10.1007/s00787-013-0413-y
38. Hashemi E, Ariza J, Rogers H, Noctor SC, Martínez-Cerdeño V. The number of parvalbumin-expressing interneurons is decreased in the prefrontal cortex in autism. Cereb Cortex. 2017;27(3):1931–1943.
39. Camacho J, Ejaz E, Ariza J, Noctor SC, Martínez-Cerdeño V. RELN-expressing neuron density in layer I of the superior temporal lobe is similar in human brains with autism and in age-matched controls. Neurosci Lett. 2014;579:163–167. doi:10.1016/j.neulet.2014.07.031
40. Nair A, Treiber JM, Shukla DK, Shih P, Müller RA. Impaired thalamocortical connectivity in autism spectrum disorder: A study of functional and anatomical connectivity. Brain. 2013;136(Pt 6):1942–1955. doi:10.1093/brain/awt079
41. Cheon KA, Kim YS, Oh SH, et al. Involvement of the anterior thalamic radiation in boys with high functioning autism spectrum disorders: A diffusion tensor imaging study. Brain Res. 2011;1417:77–86. doi:10.1016/j.brainres.2011.08.020
42. Testa-Silva G, Loebel A, Giugliano M, de Kock CP, Mansvelder HD, Meredith RM. Hyperconnectivity and slow synapses during early development of medial prefrontal cortex in a mouse model for mental retardation and autism. Cereb Cortex. 2012;22(6):1333–1342. doi:10.1093/cercor/bhr224
43. Rinaldi T, Perrodin C, Markram H. Hyper-connectivity and hyper-plasticity in the medial prefrontal cortex in the valproic acid animal model of autism. Front Neural Circuits. 2008;2:4. doi:10.3389/neuro.04.004.2008
44. Kalmbach BE, Johnston D, Brager DH. Cell-type specific channelopathies in the prefrontal cortex of the fmr1-/y mouse model of fragile X syndrome. eNeuro. 2015;2(6):
45. Brumback AC, Ellwood IT, Kjaerby C, et al. Identifying specific prefrontal neurons that contribute to autism-associated abnormalities in physiology and social behavior. Mol Psychiatry. 2018;23(10):2078–2089. doi:10.1038/mp.2017.213
46. Aman M, Rettiganti M, Nagaraja HN, et al. Tolerability, safety, and benefits of risperidone in children and adolescents with autism: 21-month follow-up after 8-week placebo-controlled trial. J Child Adolesc Psychopharmacol. 2015;25(6):482–493. doi:10.1089/cap.2015.0005
47. Hara Y, Ago Y, Taruta A, et al. Risperidone and aripiprazole alleviate prenatal valproic acid-induced abnormalities in behaviors and dendritic spine density in mice. Psychopharmacology. 2017;234(21):3217–3228. doi:10.1007/s00213-017-4703-9
48. Hara Y, Ago Y, Taruta A, et al. Improvement by methylphenidate and atomoxetine of social interaction deficits and recognition memory impairment in a mouse model of valproic acid-induced autism. Autism Res. 2016;9(9):926–939. doi:10.1002/aur.1596
49. Amendah D, Grosse SD, Peacock G, Mandell DS. The economic costs of autism: A review. In: Amaral D, Geschwind D, Dawson G, editors. Autism Spectrum Disorders. Oxford: Oxford University Press; 2011:1347–1360.
50. Buescher AV, Cidav Z, Knapp M, Mandell DS. Costs of autism spectrum disorders in the United Kingdom and the United States. JAMA Pediatr. 2014;168(8):721–778. doi:10.1001/jamapediatrics.2014.210
51. Autism Speaks. New research finds annual cost of autism has more than tripled to $126 billion in the U.S. and reached £34 billion in the U.K; 2012. Available from: https://www.autismspeaks.org/press-release/new-research-finds-annual-cost-autism-has-more-tripled-126-billion-us-and-reached.
52. Lamberti M, Siracusano R, Italiano D, et al. Head-to-head comparison of aripiprazole and risperidone in the treatment of ADHD symptoms in children with autistic spectrum disorder and ADHD: A pilot, open-label, randomized controlled study. Pediatr Drugs. 2016;18(4):319–329. doi:10.1007/s40272-016-0183-3
53. Gencer O, Emiroglu FN, Miral S, Baykara B, Baykara A, Dirik E. Comparison of long-term efficacy and safety of risperidone and haloperidol in children and adolescents with autistic disorder. An open label maintenance study. Eur Child Adolesc Psychiatry. 2008;17(4):217–225. doi:10.1007/s00787-007-0656-6
54. Scahill L, McDougle CJ, Aman MG, et al. Effects of risperidone and parent training on adaptive functioning in children with pervasive developmental disorders and serious behavioral problems. J Am Acad Child Adolesc Psychiatry. 2012;51(2):136–146. doi:10.1016/j.jaac.2011.11.010
55. Akhondzadeh S, Fallah J, Mohammadi MR, et al. Double-blind placebo-controlled trial of pentoxifylline added to risperidone: effects on aberrant behavior in children with autism. Prog Neuropsychopharmacol Biol Psychiatry. 2010;34(1):32–36. doi:10.1016/j.pnpbp.2009.09.012
56. McDougle CJ, Scahill L, Aman MG, et al. Risperidone for the core symptom domains of autism: results from the study by the autism network of the research units on pediatric psychopharmacology. Am J Psychiatry. 2005;162(2):1142–1148. doi:10.1176/appi.ajp.162.6.1142
57. Ghaeli P, Nikvarz N, Alaghband-Rad J, Alimadadi A, Tehrani-Doost M. Effects of risperidone on core symptoms of autistic disorder based on childhood autism rating scale: an open label study. Indian J Psychol Med. 2014;36(1):66–70.
58. Williams SK, Scahill L, Vitiello B, et al. Risperidone and adaptive behavior in children with autism. J Am Acad Child Adolesc Psychiatry. 2006;45(4):431–439. doi:10.1097/01.chi.0000196423.80717.32
59. Troost PW, Lahuis BE, Steenhuis MP, et al. Long-term effects of risperidone in children with autism spectrum disorders: a placebo discontinuation study. J Am Acad Child Adolesc Psychiatry. 2005;44(11):1137–1144. doi:10.1097/01.chi.0000177055.11229.76
60. Mazurek MO, Lu F, Macklin EA, Handen BL. Factors associated with DSM-5 severity level ratings for autism spectrum disorder. Autism. 2019;23(2):468–476. doi:10.1177/1362361318755318
61. Brugha TS, Doos L, Tempier A, Howlin P. Outcome measures in intervention trials for adults with autism spectrum disorders; a systematic review of assessments of core autism features and associated emotional and behavioural problems. Int J Methods Psychiatr Res. 2015;24(2):99–115. doi:10.1002/mpr.1466
62. Lòpez-de Fede A, Vyavaharkar M, Bellinger JD. Antipsychotic prescriptions for children aged 5 years or younger: do we need policy oversight standards? SAGE Open. 2014;4(4):1–7. doi:10.1177/2158244014555116
63. Chirdkiatgumchai V, Xiao H, Fredstrom BK, et al. National trends in psychotropic medication use in young children: 1994–2009. Pediatrics. 2013;132(4):615–623. doi:10.1542/peds.2013-1546
64. Pringsheim T, Stewart DG, Chan P, Tehrani A, Patten SB. The pharmacoepidemiology of psychotropic medication use in Canadian children from 2012 to 2016. J Child Adolesc Psychopharmacol. 2019;29(10):740–745. doi:10.1089/cap.2019.0018
65. Fanton J, Gleason MM. Psychopharmacology and preschoolers: A critical review of current conditions. Child Adolesc Psychiatr Clin N Am. 2009;18(3):753–771. doi:10.1016/j.chc.2009.02.005
66. Gleason MM, Egger HL, Emslie GJ, et al. Psychopharmacological treatment for very young children: contexts and guidelines. J Am Acad Child Adolesc Psychiatry. 2007;46(12):1532–1572. doi:10.1097/chi.0b013e3181570d9e
67. Brophy S, Kennedy J, Fernandez-Gutierrez F, et al. Characteristics of children prescribed antipsychotics: analysis of routinely collected data. J Child Adolesc Psychopharmacol. 2018;28(3):180–191. doi:10.1089/cap.2017.0003
68. Luby J, Mrakotsky C, Stalets MM, et al. Risperidone in preschool children with autistic spectrum disorders: an investigation of safety and efficacy. J Child Adolesc Psychopharmacol. 2006;16(5):575–587. doi:10.1089/cap.2006.16.575
69. Hossain MM, Khan N, Sultana A, et al. Prevalence of comorbid psychiatric disorders among people with autism spectrum disorder: an umbrella review of systematic reviews and meta-analyses. Psychiatry Res. 2020;287:112922. doi:10.1016/j.psychres.2020.112922
70. Lai MC, Kassee C, Besney R, et al. Prevalence of co-occurring mental health diagnoses in the autism population: a systematic review and meta-analysis. Lancet Psychiatry. 2019;6(10):819–829. doi:10.1016/S2215-0366(19)30289-5
71. Nagaraj R, Singhi P, Malhi P. Risperidone in children with autism: randomized, placebo-controlled, double-blind study. J Child Neurol. 2006;21(6):450–455. doi:10.1177/08830738060210060801
72. McDougle CJ, Holmes JP, Carlson DC, Pelton GH, Cohen DJ, Price LH. A double-blind, placebo-controlled study of risperidone in adults with autistic disorder and other pervasive developmental disorders. Arch Gen Psychiatry. 1998;55(7):633–641. doi:10.1001/archpsyc.55.7.633
73. Pandina GJ, Bossie CA, Youssef E, Zhu Y, Dunbar F. Risperidone improves behavioral symptoms in children with autism in a randomized, double-blind, placebo-controlled trial. J Autism Dev Disord. 2007;37(2):367–373. doi:10.1007/s10803-006-0234-7
74. Aman MG, Hollway JA, McDougle CJ, et al. Cognitive effects of risperidone in children with autism and irritable behavior. J Child Adolesc Psychopharmacol. 2008;18(3):227–236. doi:10.1089/cap.2007.0133
75. Shea S, Turgay A, Carroll A, et al. Risperidone in the treatment of disruptive behavioral symptoms in children with autistic and other pervasive developmental disorders. Pediatrics. 2004;114(5):e634–641. doi:10.1542/peds.2003-0264-F
76. Ichikawa H, Mikami K, Okada T, et al. Aripiprazole in the treatment of irritability in children and adolescents with autism spectrum disorder in Japan: A randomized, double-blind, placebo-controlled study. Child Psychiatry Hum Dev. 2017;48(5):796–806. doi:10.1007/s10578-016-0704-x
77. Marcus RN, Owen R, Kamen L, et al. A placebo-controlled, fixed-dose study of aripiprazole in children and adolescents with irritability associated with autistic disorder. J Am Acad Child Adolesc Psychiatry. 2009;48(11):1110–1119. doi:10.1097/CHI.0b013e3181b76658
78. Finding RL, Mankoski R, Timko K, et al. A randomized controlled trial investigating the safety and efficacy of aripiprazole in the long-term maintenance treatment of pediatric patients with irritability associated with autistic disorder. J Clin Psychiatry. 2014;75(1):22–30. doi:10.4088/JCP.13m08500
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.