Back to Journals » Drug Design, Development and Therapy » Volume 17
Pharmacokinetic Study of Enteric-Coated Sustained-Release Aspirin Tablets in Healthy Chinese Participants
Authors Cong D, Qi W, Liu X, Xu X ![]() , Dong L, Xue W, Li K
, Dong L, Xue W, Li K
Received 29 March 2023
Accepted for publication 5 August 2023
Published 18 August 2023 Volume 2023:17 Pages 2421—2429
DOI https://doi.org/10.2147/DDDT.S409524
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Yan Zhu
Duanduan Cong,1 Wenyuan Qi,1 Xiaohui Liu,1 Xiaoyu Xu,1 Lingyun Dong,2 Wei Xue,1,* Kexin Li1,*
1Clinical Trial Center, Beijing Hospital, National Center of Gerontology, Institute of Geriatric Medicine, Chinese Academy of Medical Sciences, Beijing Key Laboratory of Drug Clinical Risk and Personalized Medication Evaluation, Beijing, People’s Republic of China; 2Beijing Yeedozencom Healthcare Science & Technology Co., Ltd, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wei Xue; Kexin Li, Clinical Trial Centre (The North Building B4), Beijing Hospital, No. 1 Dahua Road, Dongdan, Dongcheng District, Beijing, 100730, People’s Republic of China, Tel +861085133632, Email [email protected]; [email protected]
Purpose: To study and compare the pharmacokinetic characteristics of enteric-coated sustained-release (EcSr) aspirin tablets with enteric-coated (Ec) aspirin tablets (Bayer S.p.A) in healthy Chinese participants.
Patients and Methods: In this open, randomized, single-dose, three-way, crossover study, 18 healthy participants randomly received 100 mg EcSr tablets pre-prandially (a.c.), EcSr tablets post-prandially (p.c.), or Ec tablets a.c. in each period. The concentrations of acetylsalicylic acid (ASA) and salicylic acid (SA) in plasma were determined by the LC-MS/MS method, and the pharmacokinetic parameters were calculated using WinNonlin (version 8.1).
Results: The essential PK parameters under the three treatment conditions (ie Ec a.c., EcSr a.c. and EcSr p.c.) were as follows: Cmax, ASA: 758.38± 455.34, 222.77± 98.04 and 194.54± 61.19 ng, Tmax, ASA: 6.75(2,16), 4.5(2,11) and 8.25(5,11) h, T1/2, ASA: 0.43± 0.08, 1.44± 0.59 and 4.32± 10.04 h, AUC0-t, ASA: 1008.88± 452.27, 918.04± 238.40 and 845.55± 183.25 h·ng/mL; Cmax, SA: 6409.38± 2098.52, 2863.53± 679.73 and 2913.75± 853.27ng/mL, Tmax, SA: 7.25(2,24), 10(3.5– 14) and 10(7,14) h, T1/2, SA: 2.21± 0.46, 2.69± 0.72 and 3.51± 2.06h, AUC0–t, SA: 29,131.41± 9376.23, 27,243.97± 7465.16, 27,240.25± 7444.67 h·ng/mL. When taking EcSr aspirin tablets, the 90% confidence intervals of the geometric mean ratios (pre-prandial/post-prandial) of AUC0-t, ASA and AUC0–∞, ASA, Cmax, SA, AUC0-t, SA and AUC0–∞, SA were within the range of 80.00%– 125.00%.
Conclusion: EcSr aspirin tablets showed less inter-individual variation in release and absorption than Ec aspirin tablets, which was well reflected by comparing essential PK parameters. Furthermore, meals had no significant effect on the pharmacokinetics of EcSr aspirin tablets.
Keywords: acetylsalicylic acid, salicylic acid, enteric-coated sustained-release, pharmacokinetics
Introduction
Aspirin (acetylsalicylic acid) is a classic non-steroidal anti-inflammatory drug which can be rapidly hydrolysed to salicylic acid after oral administration. It exerts various pharmacological effects depending on the dose, with low doses of 75–100 mg usually used to prevent and treat cardiovascular diseases. In that case, aspirin works mainly by irreversibly inhibiting the function of cyclooxygenase in platelets, preventing them from aggregation and thrombosis.1 However, in recent years, studies have found that taking very low doses of aspirin (daily or every other day ≤100mg) could still significantly increase the risk of major gastrointestinal bleeding and haemorrhagic stroke. Especially in the primary prevention of cardiovascular diseases, the benefits of aspirin therapy do not significantly outweigh the risk of bleeding.2
Aspirin enteric-coated (EC) tablets are currently the dosage form with the highest market share. This dosage form reduces direct irritation to the gastric mucosa by avoiding decomposition in the stomach. However, apart from directly stimulating the gastric mucosa, aspirin can still produce systemic effects that inhibit the synthesis of gastric mucosal protective factors prostacyclin (prostaglandin I2, PGI2) and prostaglandin E2 (Prostaglandin E2, PGE2). Consequently, in clinical practice, enteric-coated tablets cannot effectively reduce the risk of gastric mucosal damage, ulcers and bleeding.3 Therefore, there is still an unmet clinical need to develop novel aspirin dosage forms with better benefit-risk profiles to treat and prevent cardiovascular and cerebrovascular diseases.
Another unique aspirin dosage form, aspirin enteric-coated sustained-release (EcSr) tablets developed by Shandong Xinhua Pharmaceutical Co., Ltd. (Brand name: JieNing®), has been on the market for many years. This dosage form is designed to have a more stable and long-lasting therapeutic effect through sustained-release technology, compared to those enteric-coated dosage forms. However, there is limited information on the pharmacokinetics of this particular dosage form. Besides, although the package insert of JieNing® says that this dosage form should only be taken after meals, patients rarely follow this instruction. In clinical practice, it is not uncommon to take JieNing® on an empty stomach.
Therefore, this study aims to understand the pharmacokinetic characteristics of JieNing® in healthy Chinese subjects when taken pre-prandially (a.c.) or post-prandially (p.c.) and to determine if it is appropriate to use JieNing® on an empty stomach. In addition, the pharmacokinetics of Jiening® and aspirin enteric-coated tablets developed by Bayer S.p.A, were compared.
Materials and Methods
Study Medications and Instruments
Study Medications
Aspirin enteric-coated sustained-release tablets, strength: 50mg/tablet, batch number: 1909170, produced by Shandong Xinhua Pharmaceutical Co., Ltd; Aspirin enteric-coated tablets, strength: 100 mg/tablet, batch number: BJ42198, produced by Bayer S.p.A.
Instruments
HPLC 20-AD ultra-fast liquid phase system from Shimadzu Corporation; Tandem quadrupole mass spectrometer API 5500 and 5500 QTRAP mass spectrometer, both from Applied Biosystems.
Subjects
All participants were given detailed oral and written information about the trial and voluntarily provided written informed consent before entering the trial. Eligible subjects were between the ages of 18–45 and had a body mass index between 19.0 and 26.0kg/m2. Male participants had to weigh at least 50kg, while female participants had to weigh at least 45kg. All subjects enrolled had to be deemed healthy during the screening period, with no clinically significant medical history, unremarkable vital signs and no obvious abnormalities in their physical examination, 12-lead electrocardiogram, chest X-ray and laboratory tests (including blood routine, urine routine, blood biochemistry, HIV/Syphilis/HBV/HCV tests, etc.). Exclusion criteria included a history of drug allergy, long-term smoking, drinking or drug abuse, a history of dysmenorrhea within 3 months, and any prescription and over-the-counter drug use within four weeks before the trial. Participants with toothache, headache, neuralgia, and muscle pain within 4 weeks prior to the trial, a history of recurrent acute or chronic pain or excessive consumption of coffee were also excluded from the trial. From a week before taking the study medication to the end of the trial, skincare or cosmetic products with salicylic acid were prohibited. Additionally, diets containing large amounts of salicylic acid were not allowed during the trial.
Grouping, Administration and Blood Sample Collection
This study strictly complied with the requirements of the Declaration of Helsinki, the Good Clinical Practice for Drugs and related laws and regulations. The study protocol and informed consent form were approved by the Ethics Committee of Beijing Hospital (identifier:2020BJYYEC-004-01,02&03). This study was also approved by Center for Drug Evaluation, National Medical Products Administration and registered at both www.chinadrugtrials.org.cn (identifier: CTR20201753, Date: 2020-09-01) and www.chictr.org.cn (identifier: ChiCTR2300069889, Date: 2023-03-28). The study was conducted between September 15, 2020, and March 15, 2021.
This study adopted an open-label, randomized, three-sequence, three-period single-dose study design. A total of 18 healthy Chinese participants were enrolled and randomly divided into three dosing sequences. According to the respective sequences, they received two 50mg aspirin EcSr tablets 30 minutes before or after having a high-calorie and high-fat breakfast or a 100mg aspirin EC tablet 30 minutes before having a high-calorie and high-fat breakfast. The administration time of each period was the same, and the tablets were taken with 240mL of water each time. The washout period between each administration was no less than 7 days.
During each period, blood samples were collected within 1 hour pre-dose (as 0 hours) and at 1, 2, 2.5, 3, 3.5, 4, 4.5, 5, 5.5, 6, 6.5, 7, 7.5, 8, 8.5, 9, 10, 11, 12, 14, 16, 24, and 36 hours post-dose (4mL each time). The blood samples were centrifuged (2000g at 4°C) for 10min to separate the plasma and the blood cells. The plasma was transferred into a test tube and a backup tube, and then stored in a −80°C ultra-low temperature refrigerator before testing.
Sample Testing and Analysis
Sample testing and analysis of this study were performed by Jiangsu Wanlue Pharmaceutical Technology Co., Ltd. The plasma concentrations of ASA and SA were measured simultaneously using a high-performance liquid chromatography (LC-20AD; Shimadzu MD, USA) coupled with tandem mass spectrometry (Qtrap 5500; AB Sciex, Foster City, CA, USA) method.
A 50 μL plasma sample was spiked with 20 μL internal standard (IS, 100 ng/mL ASA-d3) and 600 μL acetonitrile. After vortexing for 3 minute and centrifugation for 5 minutes, 300 μL supernatant were evaporated to dryness (room temperature, N2 flow), and the residue was reconstituted in 150 μL of 80% aqueous acetonitrile containing 1% trifluoroacetic acid.
Each sample in a volume of 5 μL was injected onto an ACE Excel 3 Super C18 column (50 × 2.1 mm, 3 µm) for chromatographic separation. Mobile phases A and B were H2O with 0.1% formic acid and 100% methanol, respectively. Gradient elution was performed using a flow rate of 0.5 mL/min as follows: 0–0.2 min, 40% B; 0.2–0.5 min, 40% −55%B; 0.5–2 min, 55% B; 2–2.2 min, 55%–100% B; 2.2–2.7min, 100% B; 2.7–3.0 min, 100%–40% B; 3.0–4.0 min, 40% B. The column and autosampler temperatures were set at 45 and 4 °C, respectively.
The MS system was operated in negative ion electrospray mode with multiple-reaction monitoring. Ion pairs from m/z 179.0 → 137.0 for ASA, from m/z 137.0 → 65.0 for SA, and from m/z 182.1 → 138.0 for IS were selected for quantitation. The mass spectrometry parameters were set as follows: ESI source voltage, −4.5 kV; source temperature, 500 °C; nebulizer gas, 50 psi; turbo gas, 50 psi; curtain gas, 20 psi; and collision activated dissociation gas, 9 psi; dwell time, 100 ms. The data were acquired with Analyst version 1.6.1 software (Applied Biosystems SCIEX).
The above method was validated for selectivity, specificity, matrix effect, recovery, sensitivity, linearity, precision, accuracy, carryover, dilution integrity and stability according to the Chinese Pharmacopoeia (2020) to ensure that the research data were accurate and reliable.
Statistics
Demographics were summarized descriptively as per dosing sequence groups. The non-compartmental model module of Phoenix WinNonlin (version 8.1) was used to estimate and analyse the pharmacokinetic parameters for each individual in each period, including the key pharmacokinetic parameters of acetylsalicylic acid and salicylic acid, such as maximum plasma concentration (Cmax), the area under the plasma concentration–time curve (AUC) from zero extrapolated to infinity (AUC0–∞), the AUC from time 0 hour to the last quantifiable concentration (AUC0-t), half-life (T1/2), time to Cmax (Tmax) and the mean residence time (MRT0-t). PK parameters under each treatment condition were summarized as mean±standard deviation (coefficient of variation [CV] %) or median (minimum, maximum).
Essential PK parameters, including the Cmax, AUC0-t and AUC0–∞ of acetylsalicylic acid and salicylic acid, were subjected to analysis of variance (ANOVA) after natural log transformation. When comparing the PK characteristics of EC tablets and EcSr tablets administered before meals, sequence, study medication, and period were assigned as fixed effects in the variance analysis model, while subjects (order) were treated as random effects. When comparing the PK characteristics of EcSr tablets administered before and after meals, sequence, feeding status, and period were assigned as fixed effects, while subjects (order) were treated as random effects. The 90% confidence intervals of essential PK parameters’ geometric mean ratios (GMRs) were calculated for each comparison.
Results
Subjects
Eighteen participants, out of 59 participants screened, were enrolled in this study, including 12 males and 6 females. Fifteen of them were Han Chinese and 3 were from other ethnic groups. The average age of these participants was 34.6 ± 6.10 years old. Their average body weight was 63.68 ± 8.21 kg. Two participants withdrew due to COVID-19 lockdown, with one completing only the first period of the study and the other missing only one period. Another female participant only completed the first period of the study due to compliance problems. The remaining 15 participants completed the trial. The detailed demographic characteristics of the enrolled participants are shown in Table 1.
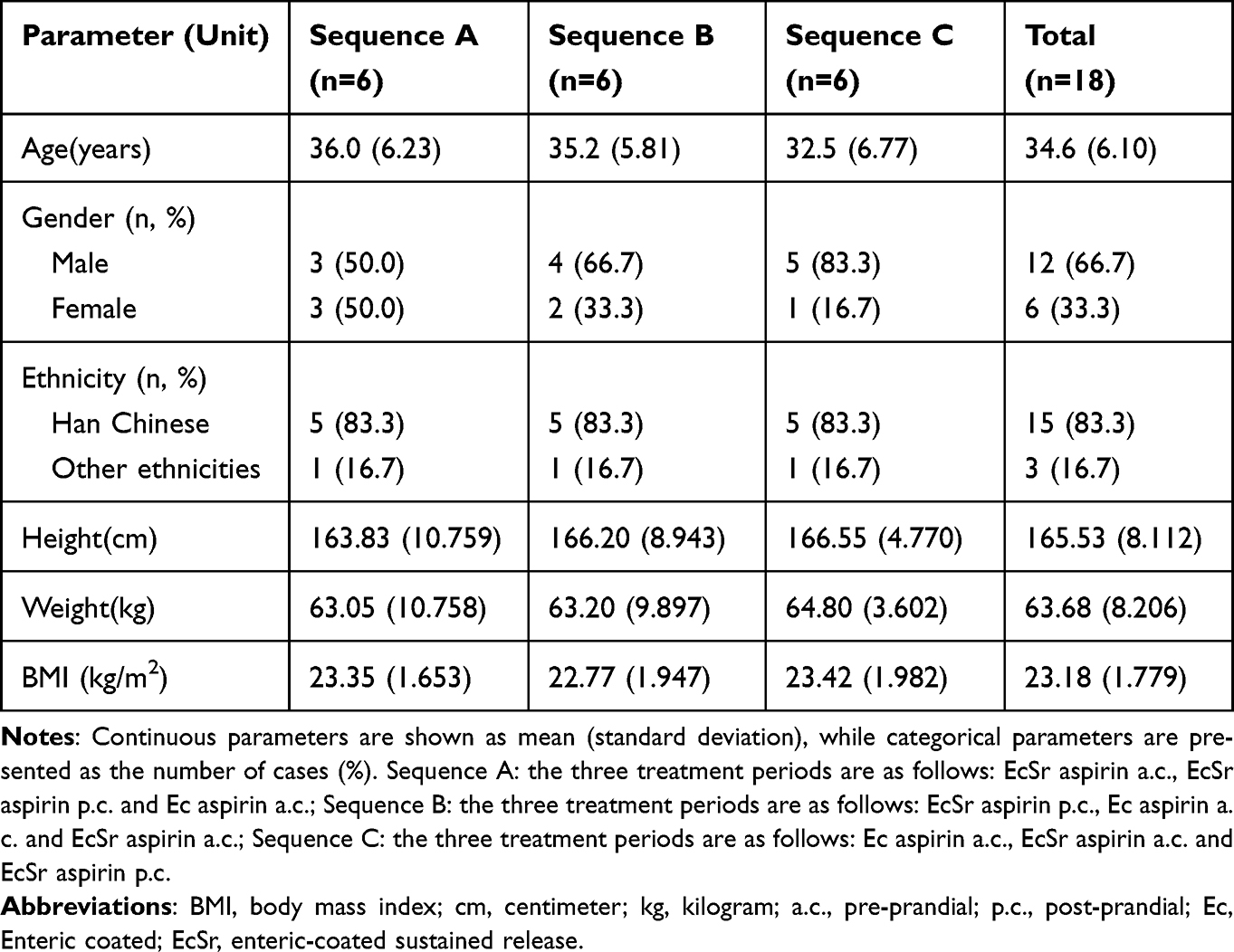 |
Table 1 Summary of Demographic Data |
Pharmacokinetics
Plasma Concentration–Time Curves
Participants received a single oral dose of 100 mg aspirin EC tablets (pre-prandial) or EcSr tablets (pre-prandial/post-prandial). The mean plasma concentration–time curves of acetylsalicylic acid and its metabolite salicylic acid are shown in Figure 1A and b, respectively.
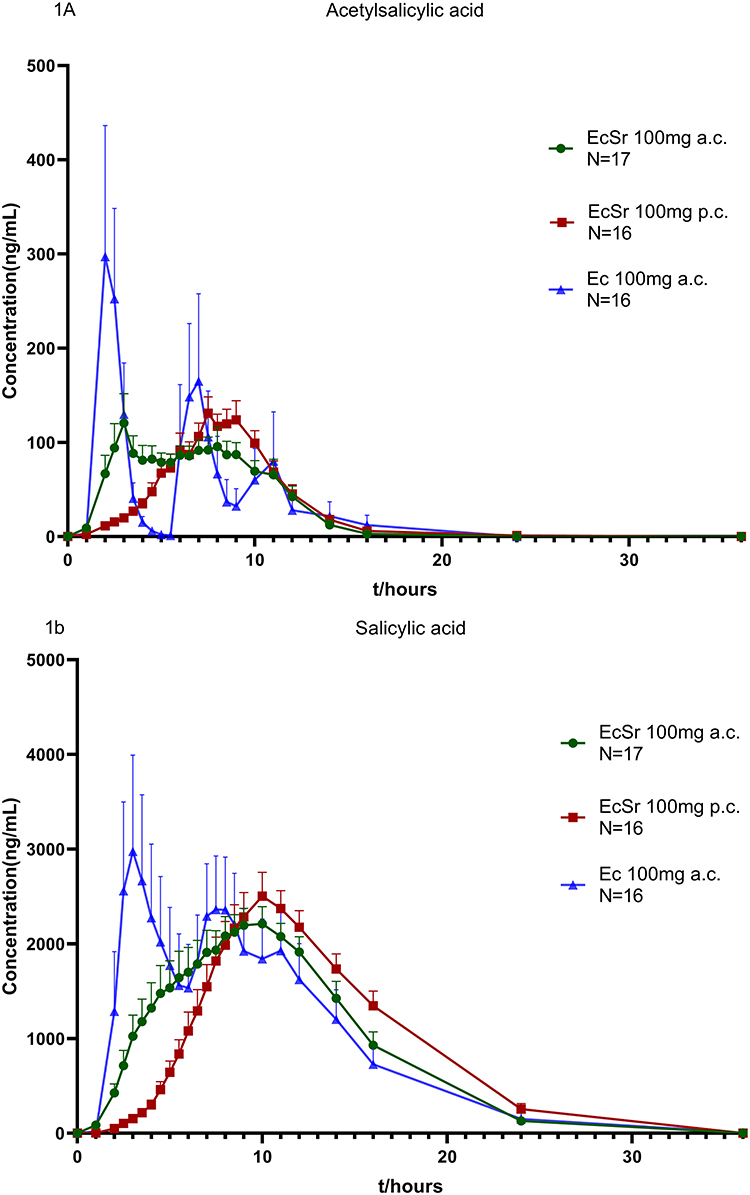 |
Figure 1 Mean plasma concentration–time profiles of acetylsalicylic acid (A) and salicylic acid (b) after a single preprandial dose of a 100-mg tablet of enteric-coated aspirin (Ec a.c.), a single preprandial dose of two 50-mg tablets of enteric-coated sustained release aspirin (EcSr a.c.) and a single postprandial dose of two 50-mg tablets of enteric-coated sustained release aspirin (EcSr p.c.). |
The time frame of acetylsalicylic acid being detectable in plasma varied after participants received a single 100 mg pre-prandial dose of EC tablets. Acetylsalicylic acid was detected in plasma 1–5.5 hours post-dose in 6 participants, 5.5–11 hours post-dose in 5 participants, and 5–16 hours post-dose in the remaining 5 participants. The peak plasma concentrations of these three groups of participants correspond to the three peaks presented on the mean plasma concentration–time curves in Figure 1A. Significant differences in time to peak plasma concentrations were also observed. Acetylsalicylic acid is rapidly hydrolysed to salicylic acid in the body, with concentrations dropping below the detection limit within 2.5–4 hours of the first detection.
However, when a single dose of EcSr tablets 100 mg was taken before or after meals, the mean plasma concentration–time curve of acetylsalicylic acid was flatter than that of enteric-coated tablets. Moreover, the time to peak plasma concentration of each subject was relatively similar. Acetylsalicylic acid can be detected in the blood 1–2 hours after taking the EcSr tablet. The last time point at which the concentration of acetylsalicylic acid can be detected is within 9–24h after taking medicine (ie, 9–16h post-dose for EcSr tablet a.c. and 11–24h post-dose for EcSr tablet p.c.). After taking EcSr tablets, acetylsalicylic acid can be continuously detected for more than 10 hours, which conforms to the characteristics of sustained-release preparations that continuously release active pharmaceutical ingredients for an extended period of time.
Pharmacokinetic Parameters
After a single oral dose of 100mg EC aspirin a.c., 100mg EcSr aspirin a.c. or 100mg EcSr p.c., essential pharmacokinetic parameters of acetylsalicylic acid and metabolite salicylic acid are presented in Table 2.
 |
Table 2 Pharmacokinetic Parameters of Acetylsalicylic Acid and Salicylic Acid Following a Single Oral Dose of Enteric-Coated Aspirin 100mg a.c., Enteric-Coated Sustained Release Aspirin 100mg a.c. or Enteric-Coated Sustained Release Aspirin 100mg p.c |
For participants taking 100mg EC aspirin a.c., the Tmax of acetylsalicylic acid ranges from 2 to 16 hours, whereas the mean t1/2 is about 0.43h. The coefficient of variation of Cmax, AUC0-t and AUC0–∞ are relatively large, suggesting significant inter-individual differences in the absorption of acetylsalicylic acid.
In contrast, whether the EcSr tablets were taken before or after meals, the coefficient of variation of the essential PK parameters of these participants was much less than that after the EC tablets was taken. In addition, compared with taking EcSr before meals, when subjects took EcSr tablets after meals, the time to reach the peak plasma concentration of acetylsalicylic acid was delayed (median Tmax: 8.25h vs 4.5h), whereas the median Tmax of salicylic acid were both around 10h.
Comparison of PK Characteristics of Aspirin EC and EcSr Tablets When Taking Pre-Prandial
The essential plasma PK parameters of acetylsalicylic acid and salicylic acid were compared following a single pre-prandial oral administration of 100mg aspirin EC or EcSr tablets. The point estimates of GMRs (EcSr/Ec) for key parameters Cmax, ASA, AUC0-t, ASA, and AUC0–∞, ASA were 26.97%, 81.40%, and 83.75%, respectively. The corresponding 90% confidence intervals of these GMRs were 21.89–33.24%, 71.22–93.04% and 71.86–97.61%, respectively. The point estimates of GMRs (EcSr/Ec) for key parameters Cmax, SA, AUC0–t, SA, and AUC0–∞, SA were 44.63%, 93.42% and 92.67%, respectively, with corresponding 90% confidence intervals of 39.52–50.39%, 86.90–100.43% and 86.02–99.82%. The 90% confidence intervals of GMRs (EcSr/Ec) for key parameters (ie, AUC0–t, SA, and AUC0–∞, SA) fell between 80% and 125%.
Comparison of PK Characteristics of Aspirin EcSr Tablets After Pre- and Post-Prandial Administration
The essential plasma PK parameters of acetylsalicylic acid and salicylic acid were compared following a single pre-prandial or post-prandial oral administration of 100mg aspirin EcSr tablets. The point estimates of GMRs (pre-prandial/post-prandial) for key parameters Cmax, ASA, AUC0-t, ASA, and AUC0–∞, ASA were 109.11%, 108.11% and 100.20%, respectively. The corresponding 90% confidence intervals of these GMRs were 92.15–129.19%, 95.92–121.84% and 97.72–122.03%, respectively. The point estimates of GMRs (pre-prandial/post-prandial) for key parameters Cmax, SA, AUC0-t, SA, and AUC0–∞, SA were 97.99%, 99.35% and 98.10%, respectively, with corresponding 90% confidence intervals of 91.02–105.49%, 93.72–105.32% and 91.23–105.48%. The 90% confidence intervals of GMRs (pre-prandial/post-prandial) for key parameters nearly all fell between 80% and 125%, except for Cmax, ASA.
Safety Evaluation
5 of 18 subjects experienced seven adverse events throughout the trial. All were mild in intensity. Two adverse events (epistaxis and hypophosphatemia) that occurred after taking EcSr tablet p.c. were also considered to be adverse drug reactions and were fully resolved by the end of the study. No serious adverse events were observed in this trial. Overall, both aspirin EC tablets and EcSr tablets have good safety profiles.
Discussion
There are few human pharmacokinetic data regarding Bayaspirin tablets in the literature, particularly in the Chinese population. In this preliminary study, we explored the pharmacokinetic characteristics of a single pre-prandial oral dose of the 100mg Bayaspirin tablet (ie aspirin EC tablet) in healthy Chinese participants. The results showed significant inter-individual differences in the absorption rate and extent of acetylsalicylic acid in healthy Chinese participants. The plasma concentration–time curves exhibited a burst release of acetylsalicylic acid, and the duration of acetylsalicylic acid in plasma was no more than 4 hours. These findings were similar to a recent PK study of Bayaspirin tablets in healthy Italian participants.4 Compared to the currently available pharmacokinetic data, the exposure to acetylsalicylic acid in healthy Chinese subjects was slightly higher than that in Italian and Japanese healthy subjects after a single pre-prandial oral dose of 100 mg of Bayaspirin tablet.4,5
The antiplatelet effect of aspirin mainly depends on the concentration of acetylsalicylic acid in the circulation and the turnover rate of platelets. Previous studies have shown that after a single dose of aspirin, platelet cyclooxygenase activity could recover approximately 10% per day, along with the continuous renewal of platelets in the circulation. Platelets with intact cyclooxygenase activity could appear in circulation as early as 4–6 hours after a single dose of 100 mg aspirin. Besides, 10–20% of platelets with intact cyclooxygenase activity were considered sufficient to counteract aspirin’s inhibitory effect on platelet aggregation.6,7 Additionally, in specific clinical settings which are characterized by a high atherothrombosis risk (eg smoking, diabetes, metabolic syndrome, undergoing cardiac surgery, etc.), the turnover rate of platelets and the recovery rate of cyclooxygenase activity are significantly increased than usual.7 Due to the short maintenance of acetylsalicylic acid in circulation after taking aspirin EC tablets, the once-daily regimen may not be sufficient to exert an antiplatelet aggregation effect over 24 hours continuously. In patient populations with a higher platelet turnover rate, some individuals might even experience the phenomenon of “aspirin resistance or non-response”.8,9 Furthermore, due to the significant inter-individual variability in the absorption of acetylsalicylic acid, individuals with reduced or delayed absorption may not be able to achieve their benefit when cardiovascular events occur (eg, in the early morning).
This study also explored the pharmacokinetic characteristics of aspirin EcSr tablets produced by Shandong Xinhua Pharmaceutical Co., Ltd. in healthy Chinese subjects. The results revealed that EcSr tablets had both enteric-coated and sustained-release properties. After consuming EcSr tablets either before or after meals, the release and absorption of acetylsalicylic acid lasted for a significantly longer period of time in comparison to Ec tablets, and the inter-individual variation was significantly less. Whether the EcSr tablets were taken before or after a meal, acetylsalicylic acid could always be detected in the blood 1–2 hours after administration, and its duration was more than 10 hours. Although the peak concentrations of acetylsalicylic acid and salicylic acid were lower than those of the EC tablets, the AUC0-t and AUC0–∞ of acetylsalicylic acid and salicylic acid were similar between aspirin EC and EcSr tablets. Therefore, we speculated that the above PK characteristics of EcSr tablets might enable them to continuously inhibit platelet aggregation (including daily platelet renewal) after administration and reduce the gastrointestinal tract bleeding risk by decreasing the peak acetylsalicylic acid concentration. Intriguingly, a recent multi-centre randomized controlled clinical study in China also found that the preventive use of aspirin EcSr tablets 50–100 mg per day in the elderly had a similar inhibitory effect on platelet aggregation rate as the aspirin EC tablets. However, the short-term safety of EcSr tablets seemed to be better than EC tablets.10
In addition, although the [Dosage and Administration] section of the package insert for aspirin EcSr tablets states that “this product should be taken with warm water after meals, not on an empty stomach”, AUC0-t, ASA, AUC0–∞, ASA and other essential PK parameters of salicylic acid in this study were almost the same when EcSr tablets were taken before or after a meal, suggesting that feeding status had no significant effect on the pharmacokinetic characteristics of aspirin EcSr tablets. Therefore, this may allow the conditions of use to be appropriately broadened.
One potential limitation of our study is that we only examined the PK characteristics of JieNing® after a single administration. To gain a more thorough understanding of JieNing®, further studies investigating its PK characteristics after repeated administration and how they affect PD markers would be beneficial. We are now actively planning another study to address these important questions.
Conclusion
The duration of release and absorption of acetylsalicylic acid was significantly longer and the inter-individual variation was much less when EcSr aspirin tablets were taken with or after meals, compared with Ec aspirin tablets. Furthermore, meals had no significant effect on the pharmacokinetics of EcSr aspirin tablets.
Data Sharing Statement
The raw data of this study will not be shared because of confidentiality.
Acknowledgments
The study was financially supported by Shandong Xinhua Pharmaceutical Co., Ltd, Shandong, China and National Key R&D Program of China [grant number:2020YFC2008303]. The authors thank all the participants who participated in this study, as well as all the investigators, site staff, and operations staff who participated in the study. Additionally, the authors thank Jiangsu Wanlue Pharmaceutical Technology Co., Ltd. for performing sample testing and analysis of this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Christiansen M, Grove EL, Hvas AM. Contemporary Clinical Use of Aspirin: Mechanisms of Action, Current Concepts, Unresolved Questions, and Future Perspectives. Semin Thromb Hemost. 2021;47(7):800–814. doi:10.1055/s-0041-1726096
2. Davidson KW, Barry MJ, Mangione CM, et al. Aspirin use to prevent cardiovascular disease: US Preventive Services Task Force recommendation statement. JAMA. 2022;327:1577–1584. doi:10.1001/jama.2022.5207
3. Kedir HM, Sisay EA, Abiye AA. Enteric-coated aspirin and the risk of gastrointestinal side effects: a systematic review. Int J Gen Med. 2021;14:4757. doi:10.2147/IJGM.S326929
4. Dei Cas M, Rizzo J, Scavone M, et al. In-vitro and in-vivo metabolism of different aspirin formulations studied by a validated liquid chromatography tandem mass spectrometry method. Sci Rep. 2021;11(1):10370. doi:10.1038/s41598-021-89671-w
5. Pharmaceuticals and Medical Devices Agency, PMDA.医薬品インタビューフォーム——バイアスピリンⓇ錠100mg[EB/OL]. (2022-05)[2022-06-20] [Pharmaceutical Interview Form ——Bayaspirin® Tablets]. http://www.pmda.go.jp/PmdaSearch/iyakuSearch/.
6. Di Minno G. Aspirin resistance and platelet turnover: a 25-year old issue. Nutr Metab Cardiovasc Dis. 2011;21(8):542–545. doi:10.1016/j.numecd.2011.04.002
7. Altman R, Luciardi HL, Muntaner J, et al. The antithrombotic profile of aspirin. Aspirin resistance, or simply failure? Thromb J. 2004;2(1):1–8. doi:10.1186/1477-9560-2-1
8. Grosser T, Fries S, Lawson JA, et al. Drug resistance and pseudoresistance: an unintended consequence of enteric coating aspirin. CIRCULATION. 2013;127(3):377–385. doi:10.1161/CIRCULATIONAHA.112.117283
9. Bhatt DL, Grosser T, Dong J, et al. Enteric coating and aspirin nonresponsiveness in patients with type 2 diabetes mellitus. J AM COLL CARDIOL. 2017;69:603–612. doi:10.1016/j.jacc.2016.11.050
10. Chen XH, Liu ML, Qin MF, et al. Anti-aggregation effect and short-term safety evaluation of low-dose aspirin therapy in the elderly Chinese population: a multicenter randomized controlled clinical trial. Chin Circ J. 2018;33:457–462.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.