Back to Journals » Clinical Ophthalmology » Volume 18
Phacoemulsification versus Laser Peripheral Iridotomy for Treating Primary Angle Closure Glaucoma: A Systematic Review and Meta-Analysis
Authors Sharif RK, Aljahdali FF ![]() , Aljabri HM, Alomari LK
, Aljabri HM, Alomari LK ![]() , Sagim RA, Alamri DM, Alshehri MA, Alshigari RA
, Sagim RA, Alamri DM, Alshehri MA, Alshigari RA
Received 5 December 2023
Accepted for publication 11 March 2024
Published 4 April 2024 Volume 2024:18 Pages 1023—1032
DOI https://doi.org/10.2147/OPTH.S446285
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Rahaf K Sharif,1 Faisal F Aljahdali,1 Hind M Aljabri,1 Lugean K Alomari,1 Renad A Sagim,1 Duaa M Alamri,1 Merai A Alshehri,2 Rayan Abdullah Alshigari3
1College of Medicine, King Saud Bin Abdulaziz University for Health Sciences, Jeddah, Saudi Arabia; 2Department of Surgery, College of Medicine, University of Bisha, Bisha, Saudi Arabia; 3Department of Glaucoma Section, King Khaled Eye Specialist Hospital, Riyadh, Saudi Arabia
Correspondence: Faisal F Aljahdali, College of Medicine, King Saud bin Abdulaziz University for Health Sciences, Jeddah, Saudi Arabia, Email [email protected]
Background: Primary Angle Closure Glaucoma (PACG), is caused by narrowing the iridocorneal angle and increases the risk of blockage in the trabecular meshwork. Phacoemulsification and laser peripheral iridotomy (LPI) effectively control IOP elevation and widen the angle. This systematic review and meta-analysis compared Phacoemulsification and LPI Effectiveness for PACG.
Methods: We searched Medline, Embase, and CENTRAL. We included randomized controlled trials (RCTs) that compared Phacoemulsification and LPI for individuals with PACG. We sought to evaluate the following outcomes: mean IOP, number of glaucoma medications, visual acuity (VA), visual field (VF) progression, peripheral anterior synechiae (PAS), Shaffer gonioscopy grading, central corneal thickness (CCT), central endothelial cell density (CECD), and poor response to surgery. The standardized mean difference (SMD) was used to represent continuous outcomes, while the risk ratio (RR) was used to represent dichotomous outcomes.
Results: 5 RCTs that enrolled 917 participants were deemed eligible. The phacoemulsification group showed statistically significance lower mean CCT and CECD and lower risk of poor response to surgery compared to LPI (SMD = − 1.10; 95% − 1.50, − 0.70; P< 0.001, SMD − 366.12; 95% − 652.59, − 79.65; P=0.01, and RR 0.35; 95% 0.23, 0.54; P< 0.001 respectively). There were no significant improvement in IOP and number of medications between both groups (SMD = − 0.74; 95% CI = − 2.26, 0.78; P=0.34, and SMD − 17.58; 95% CI = − 50.28, 15.12; P=0.29 respectively). Finally, there were also no significant differences in VA, VF progression, PAS, and mean Shaffer gonioscopy grading between both groups.
Conclusion: Phacoemulsification showed statistically significant lower mean corneal thickness, central endothelial cell density, and lower risk of poor response to surgery compared to LPI. However, there were no significant differences in mean IOP, number of medications, VA, VF progression, PAS, and mean Shaffer gonioscopy grading between Phacoemulsification and LPI.
Keywords: phacoemulsification, laser, iridotomy, glaucoma
Introduction
Primary angle closure glaucoma (PACG) is typically caused by a sudden blockage of the trabecular meshwork, which is in the anterior chamber angle of the eye. This blockage leads to a rapid increase in the pressure inside the eye.1 High intraocular pressure (IOP) can cause irreversible damage to the optic nerve. If the elevated pressure persists for hours or days, it can lead to blindness.2 Glaucoma is a major cause of blindness worldwide. In 2013, it was estimated that there were 64.3 million individuals between the ages of 40 and 80 who had glaucoma globally. By 2020, this number had risen to 76.0 million, and it is projected to increase to 111.8 million by 2040.3 PACG may lead to emergencies that require urgent treatment, but it can be managed and controlled if the angle closure process is diagnosed early.4
The primary objective of treating primary angle closure glaucoma (PACG) is to rapidly lower the intraocular pressure (IOP) to alleviate pain, reduce corneal edema, and prevent optic nerve damage. Lowering IOP can typically be achieved using topical or oral medications, and this can enable more definitive treatments such as laser peripheral iridotomy (LPI) or lens removal.4 Laser iridotomy (LI) is a well-established procedure for treating and preventing acute primary angle closure glaucoma (APACG). By equalizing the pressure gradient between the anterior and posterior chambers of the eye, LI reduces the risk of angle closure and subsequent elevation of intraocular pressure.5 However, the role of the crystalline lens in the onset of PACG is significant, and some experts propose that early removal of the lens through Phacoemulsification may improve IOP management and potentially reduce the need for medication and subsequent glaucoma surgery.6 These procedures have demonstrated effectiveness in controlling IOP elevation and widening the angle.4 Recently, several RCTs comparing the efficacy of LPI and Phacoemulsification in managing PACG have been published in the literature.
Two previous systematic reviews investigated the impact of phacoemulsification and LPI in patients with PACG. The first review included both randomized controlled trials and non-randomized controlled studies.7 The second systematic review did not assess several important outcomes such as the number of medications, visual field (VF) progression, central corneal thickness (CCT), peripheral anterior synechiae (PAS), and poor response to surgery.8
This systematic review aimed to compare the effectiveness of laser peripheral iridotomy to early lens extraction in the management of primary angle closure glaucoma (PACG), with respect to intraocular pressure (IOP), Shaffer gonioscopy grading, PAS, best-corrected visual acuity (BCVA), visual field (VF), central endothelial cell density (CECD), CCT, number of glaucoma medications, and poor response to treatment.
Methods
This systematic review and meta-analysis were conducted following a predetermined protocol and reported following the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines.
Eligibility Criteria
Patients: Individuals with Primary Angle Closure Glaucoma; intervention: Phacoemulsification; Comparison: Laser Peripheral Iridotomy; Outcomes: Prevalence of IOP rise above 21 mmHg and the number of glaucoma medications, Shaffer gonioscopy grading, visual acuity (VA), visual field (VF), central endothelial cell density (CECD), central corneal thickness (CCT), peripheral anterior synechiae (PAS) and poor response to treatment.
Search Strategy
The systematic search was performed on Medline, Embase, and Cochrane Central Register of Controlled Trials (CENTRAL) starting from their inception until February 15th, 2023. There were no restrictions on the publication dates, but we only included studies published in English. Additionally, we searched for ongoing or recently completed trials by checking ClinicalTrials.gov, UMIN Clinical Trials Registry, Australian New Zealand Clinical Trials Registry, ISRCTN registry, and MetaRegister of Controlled Trials. We reviewed the reference lists of the included RCTs in our study to identify any potentially relevant RCTs that might have been missed during the systematic search.
Study Selection and Data Extraction
Two reviewers independently and in duplicate screened the titles and abstracts of eligible trials, assessed the full text, and extracted data. In cases of disagreement, a consensus was reached, or a third reviewer was consulted for discussion.
Risk of Bias Assessment
Two reviewers performed the risk of bias assessment for the included RCTs using the Revised Cochrane Risk of Bias Assessment Tool independently and in duplicate. This tool is composed of seven items: random sequence generation, allocation concealment (selection bias), blinding of participants and personnel performance bias), blinding of outcome assessment (detection bias), incomplete outcome data (attrition bias), selective reporting (reporting bias), and other possible causes of bias.9
Meta-Analysis
We performed the meta-analysis using Review Manager version 5.4 (Cochrane Collaboration) and Comprehensive Meta-Analysis v3 software.10,11 We used 95% as a confidence level and P <0.05 as a threshold. Statistical heterogeneity was assessed using the Higgins I2 statistic and the Cochrane Q (Chi2 test) at the value of p < 0.10, using the random-effects model.12 The continuous outcomes, IOP, BCVA, Shaffer gonioscopy grading, PAS, VF, CECD, CCT, and number of the medications were represented as standardized mean difference (SMD) and pooled using the inverse variance weighting method. The dichotomous outcomes poor response to surgery was represented as risk ratio (RR) and pooled using the inverse variance weighting method. The mean change from the baseline was calculated based on the equations reported in the Cochrane Handbook for systematic reviews of intervention.13 Data reported in median and range or mean and range were converted to mean and standard deviation (SD) based on Hozo et al, 2005 equations.14
Results
Figure 1 shows the flowchart and study inclusion in this review. The literature search yielded 962 articles, of which 238 duplicates were excluded. 711 articles were excluded after title and abstract screening, leaving 16 articles for full text assessment. Ultimately, 5 RCTs were deemed eligible.
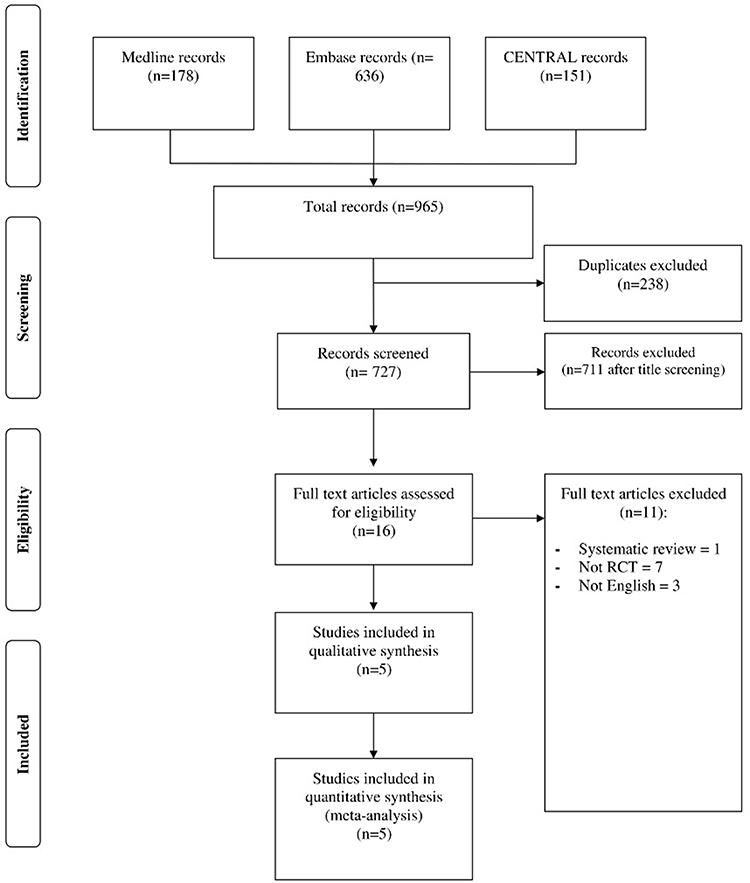 |
Figure 1 Shows the flowchart and study inclusion in this review. |
Demographic Characteristics of the Included Studies
A total of 917 participants were included in this review. Of them, 455 were subjected to Phacoemulsification, whereby 462 were treated with Laser Peripheral Iridotomy. Thirty-four patients received Phacoemulsification with intraocular lens Implantation. The average age of the included patients ranged from 65.1 to 72.3 years and from 66.1 to 69 years among the Phacoemulsification and Laser Peripheral Iridotomy groups, respectively. There were 155 females in the phacoemulsification group and 153 in the Laser Peripheral Iridotomy group. The average IOP ranged from 15.07 to 59.7 mm Hg among the phacoemulsification group and 19.93 to 57.9 mm Hg among the Laser Peripheral Iridotomy group. The average axial length ranged from 22.42 to 22·5 and 22.46 to 22.7 among the Phacoemulsification and Laser Peripheral Iridotomy groups shown in Supplementary Table 1.
Risk of Bias Assessment
All the 5 included RCTs showed a low risk of random sequence generation selection bias.15–19 Where Chan et al, 202116 showed a low risk of allocation concealment bias, the remaining articles showed unclear risk.7,9–11 All the included articles showed a low risk of performance bias, while three articles showed a high risk of attribution bias.15,16,19 All the included articles showed a low risk of reporting bias15–19 see Figure 2.
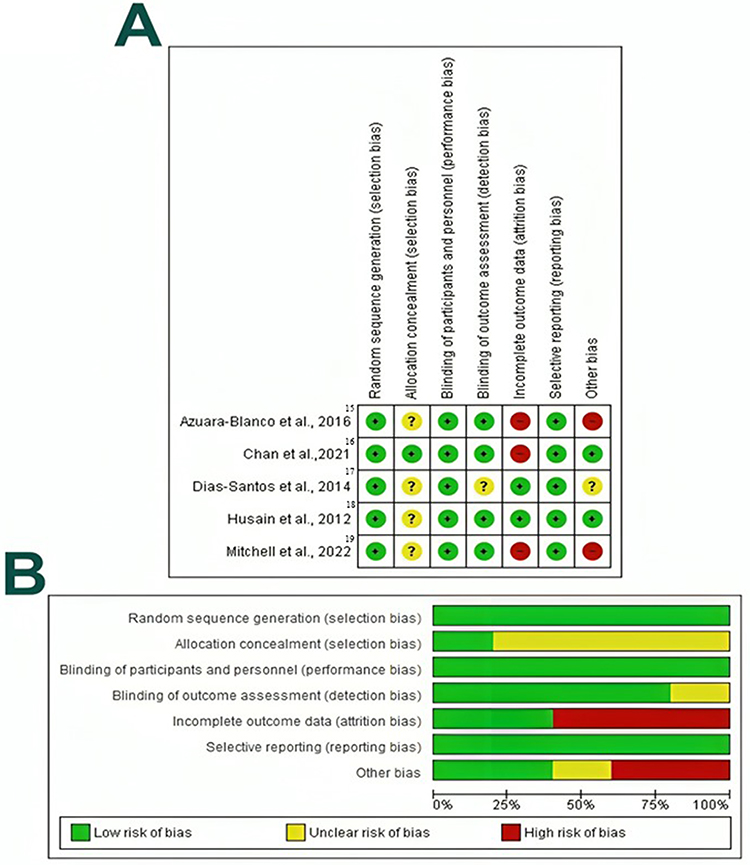 |
Figure 2 (A) Risk of bias graph (B) Risk of bias summary: review authors’ judgements about each risk of bias item presented as percentages across all included studies. |
Study Outcomes
Intraocular Pressure (Mm Hg)
Four articles included 471 patients with primary angle glaucoma and reported the mean change from baseline among the Phacoemulsification and laser peripheral iridotomy groups.15–18 In the random-effects model (I2=15%, P=0.32), there was no statistically significant difference between both groups (SMD −0.74; 95% CI= −2.26, 0.78; P=0.34) see Figure 3.
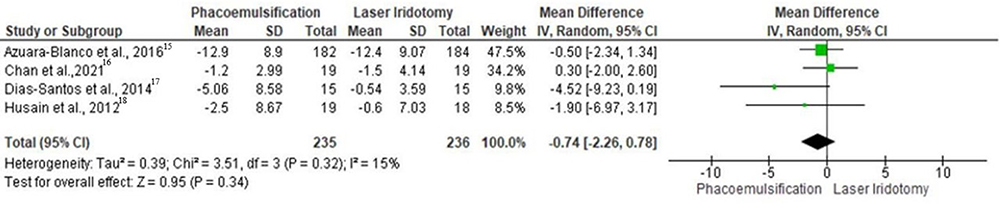 |
Figure 3 Forest plot of summary analysis of the Mean Difference (MD) and 95% CI of mean change from baseline of the intraocular pressure between the phacoemulsification and laser peripheral iridotomy groups. Size of the green squares is proportional to the statistical weight of each trial. The grey diamond represents the pooled point estimate. The positioning of both diamonds and squares (along with 95% CIs) beyond the vertical line (unit value) suggests a significant outcome (IV = inverse variance). |
Medications Usage
The difference in mean change from the baseline of the medication usage was assessed within two articles, including 443 patients with primary angle glaucoma.15,17 Of them, 219 patients were treated with Phacoemulsification, while 224 were subjected to laser peripheral iridotomy. There was no statistically significant difference between both groups (SMD −17.58; 95% CI= −50.28, 15.12; P=0.29) in the random-effects model (I2=100%, P<0.001) see Figure 4.
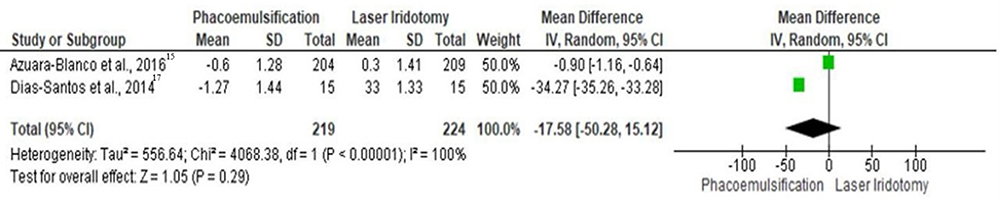 |
Figure 4 Forest plot of summary analysis of the Mean Difference (MD) and 95% CI of mean change from baseline of the medications usage between the phacoemulsification and laser peripheral iridotomy groups. Size of the green squares is proportional to the statistical weight of each trial. The grey diamond represents the pooled point estimate. The positioning of both diamonds and squares (along with 95% CIs) beyond the vertical line (unit value) suggests a significant outcome (IV = inverse variance). |
Visual Field
Two trials, including 382 patients, evaluated the difference in the visual field score after Phacoemulsification and laser peripheral iridotomy.15,16 Pooling the data in the random-effects model (I2=0%, P=0.68), revealed no statistically significant difference between Phacoemulsification and laser peripheral iridotomy groups with a SMD of −0.01 and 95% CI ranging from −0.21 to 0.19 (P=0.89) see Figure 5.
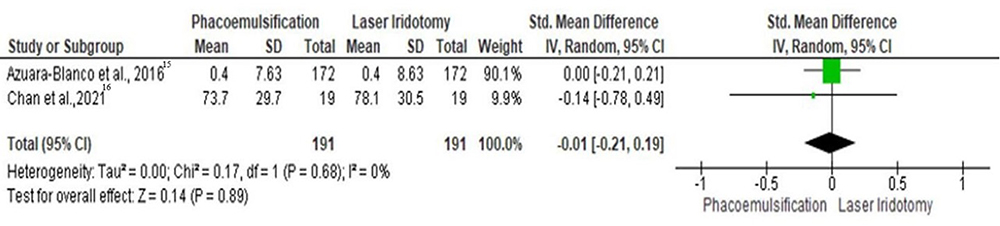 |
Figure 5 Forest plot of summary analysis of the Standardized Mean Difference (SMD) and 95% CI of the mean score of visual field between the phacoemulsification and laser peripheral iridotomy groups. Size of the green squares is proportional to the statistical weight of each trial. The grey diamond represents the pooled point estimate. The positioning of both diamonds and squares (along with 95% CIs) beyond the vertical line (unit value) suggests a significant outcome (IV = inverse variance). |
Visual Acuity
Three studies, including 422 patients with primary angle glaucoma assessed the difference in the visual acuity scores between the Phacoemulsification and laser peripheral iridotomy groups.15,16,18 There was no statistically significant difference between both groups (SMD 0.08; 95% CI= −0.29, 0.45; P=0.67) in the random-effects model (I2=41%, P=0.18) shown in Figure 6.
 |
Figure 6 Forest plot of summary analysis of the Standardized Mean Difference (SMD) and 95% CI of the mean score of visual acuity between the phacoemulsification and laser peripheral iridotomy groups. Size of the green squares is proportional to the statistical weight of each trial. The grey diamond represents the pooled point estimate. The positioning of both diamonds and squares (along with 95% CIs) beyond the vertical line (unit value) suggests a significant outcome (IV = inverse variance). |
Central Corneal Thickness (μm)
Two articles included 378 patients and evaluated the difference in central corneal thickness between the Phacoemulsification and laser peripheral iridotomy groups.15,16 Patients treated with Phacoemulsification achieved a statistically significant lower mean thickness of the central cornea with a SMD of −1.10 (95% CI= −1.50, −0.70; P<0.001), in the random-effects model (I2=41%, P=0.19) see Figure 7.
 |
Figure 7 Forest plot of summary analysis of the Standardized Mean Difference (SMD) and 95% CI of the mean central corneal thickness between the phacoemulsification and laser peripheral iridotomy groups. Size of the green squares is proportional to the statistical weight of each trial. The grey diamond represents the pooled point estimate. The positioning of both diamonds and squares (along with 95% CIs) beyond the vertical line (unit value) suggests a significant outcome (IV = inverse variance). |
Central Endothelial Cell Density
The difference between the Phacoemulsification and laser peripheral iridotomy groups in terms of central endothelial cell density was reported in two articles, including 77 patients.16,18 Pooling the data in the random-effects model (I2=0%, P=0.47), revealed a statistically significant lower central endothelial cell density among the Phacoemulsification (MD −366.12; 95% CI= −652.59, −79.65; P=0.01), relative to the laser peripheral iridotomy group Figure 8.
 |
Figure 8 Forest plot of summary analysis of the Mean Difference (MD) and 95% CI of the mean central endothelial cell density between the phacoemulsification and laser peripheral iridotomy groups. Size of the green squares is proportional to the statistical weight of each trial. The grey diamond represents the pooled point estimate. The positioning of both diamonds and squares (along with 95% CIs) beyond the vertical line (unit value) suggests a significant outcome (IV = inverse variance). |
Peripheral Anterior Synechiae
Two studies included 77 patients with primary angle glaucoma and assessed the difference in the peripheral anterior synechiae level between the Phacoemulsification and laser peripheral iridotomy groups.16,18 There was no statistically significant difference between both groups with a SMD of −0.39 and 95% CI ranging from −1.47, 0.69 (P=0.48), in the random-effects model (I2=82%, P=0.02) see Figure 9.
 |
Figure 9 Forest plot of summary analysis of the Standardized Mean Difference (SMD) and 95% CI of the mean peripheral anterior synechiae between the phacoemulsification and laser peripheral iridotomy groups. Size of the green squares is proportional to the statistical weight of each trial. The grey diamond represents the pooled point estimate. The positioning of both diamonds and squares (along with 95% CIs) beyond the vertical line (unit value) suggests a significant outcome (IV = inverse variance). |
Mean Shaffer Gonioscopy Grading
The mean difference in Shaffer gonioscopy grading between the Phacoemulsification and laser peripheral iridotomy groups was assessed within three articles, including 139 patients.16–18 There was no statistically significant difference between both groups (MD −0.04; 95% CI = −0.41, 0.33; P=0.83) in the random-effects model (I2=51%, P=0.13) see Figure 10.
 |
Figure 10 Forest plot of summary analysis of the Mean Difference (MD) and 95% CI of the mean Shaffer gonioscopy grading between the phacoemulsification and laser peripheral iridotomy groups. Size of the green squares is proportional to the statistical weight of each trial. The grey diamond represents the pooled point estimate. The positioning of both diamonds and squares (along with 95% CIs) beyond the vertical line (unit value) suggests a significant outcome (IV = inverse variance). |
Poor Response to Surgery/Failure
Three studies included 94 patients with primary angle glaucoma and assessed the risk of poor Response to Phacoemulsification and laser peripheral iridotomy interventions.15,18,19 Patients treated with the Phacoemulsification were at a statistically significant lower risk of poor response to surgery, in contrast to patients treated with laser peripheral iridotomy(RR 0.35; 95% CI = 0.23, 0.54; P<0.001) without significant heterogeneity between the included studies (I2=48%, P=0.15) see Figure 11.
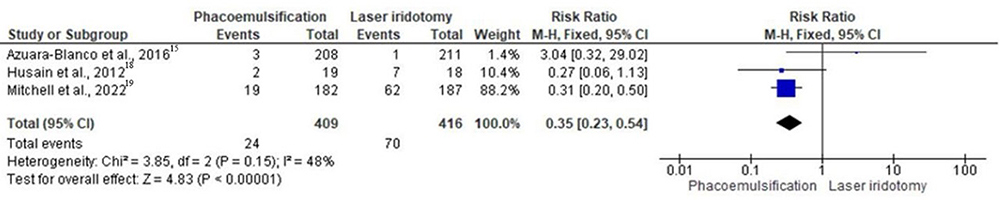 |
Figure 11 Forest plot of summary analysis of the risk ratio (RR) and 95% CI of the risk of poor response to surgery between the phacoemulsification and laser peripheral iridotomy groups. Size of the blue squares is proportional to the statistical weight of each trial. The grey diamond represents the pooled point estimate. The positioning of both diamonds and squares (along with 95% CIs) beyond the vertical line (unit value) suggests a significant outcome (IV = inverse variance). |
Discussion
This systematic review and meta-analysis of 5 RCTs included 917 participants compared phacoemulsification and peripheral laser iridotomy for primary angle closure glaucoma. The analysis showed statistically significant lower CCT, CECD, and risk of poor Response to surgery in Phacoemulsification compared to LPI. On the other hand, no significant differences in IOP, number of medication usage, VF, PAS, mean Shaffer gonioscopy grading, and VA.
Glaucoma is a neurodegenerative disease that may lead to progressive visual loss. It can be divided into open-angle and closed-angle glaucoma.20 When certain signs suggest that the peripheral iris is blocking the trabecular meshwork in the eye, it indicates the presence of primary angle closure (PAC). This can lead to elevated IOP, PAS, iris whorling, glaucomfleken, lens opacities, or excessive pigment deposition on the trabecular meshwork.21 The primary objective is to control IOP and prevent further damage to the optic nerve while monitoring the angle, which can be achieved by revising the angle configuration through LPI or lens extraction.4,22 The current standard considered LPI for the initial intervention of PACG as its role in decreased IOP. It caused the iris to become flatter and the ciliary body to move slightly towards the back.22 On the other hand, the phacoemulsification role still needs to be fully understood in the management of PACG.23 Numerous studies suggest that performing Phacoemulsification, aspiration, and implantation of intraocular lenses in eyes with acute angle closure has led to widening the chamber angle and reducing intraocular pressure.23–26 RCTs included in this analysis demonstrated that lens extraction is more effective than LRI in controlling IOP. These studies revealed significant differences in both IOP levels and the number of medications required to control it.15–18 Interestingly, our meta-analysis showed no significant differences in the mean IOP and number of medications between the lens extraction and LPI groups.
The position of the lens is an important factor in the development of PAC, as lenses located more toward the front of the eye result in a higher degree of curvature of the iris.27 According to Lowe’s research in 1975 and 1976, an increase in lens thickness results in a shallowing of the anterior chamber by approximately 0.35 millimeters, while a more anteriorly positioned lens causes an even greater degree of shallowing, approximately 0.65 millimeters. Studies showed that lens extraction increases the anterior chamber depth and eliminates the angle closure.26–30 Dias-Santos et al trial also showed statistical significance in anterior chamber depth, volume, and angle favoring lens extraction over LPI.17 In his trial, Chan et al demonstrate that lens extraction is superior to LPI for having less extensive PAS and greater Shaffer grad.16 In his trial, Husain et al revealed that LPI has lesser PAS and greater mean Shaffer score. He explained that the decrease in PAS in lens extraction Group related to their injection protocol, which involved administering viscoelastic substance all around the front chamber, led to the PAS breakage.18 Our analysis showed no significant differences in mean Shaffer Gonioscopy grading and PAS in both groups.
Performing surgery on patients with angle closure presents greater challenges compared to regular surgery due to the following factors: a shallow anterior chamber and a lack of muscle tone in the pupil resulting from a recent acute attack, as well as persistent corneal swelling. However, Tarongoy et al reviewed reports on the use of lensectomy as a treatment for angle closure glaucoma; it is stated that lensectomy, whether performed through extracapsular cataract extraction (ECCE) or Phacoemulsification (PHACO), has the potential to be a safe procedure when performed by an experienced cataract surgeon.23,31–37 In their trial, Husain and Mitchell et al mention that LPI has more common complications than lens extraction. CECD was measured in two RCTs and showed no significant difference between the two groups.16,18 This meta-analysis revealed a significantly lower CECD, CCT, and risk of poor response to surgery among Phacoemulsification than the LPI group. Moreover, VA and VF measured the visual impermeant and the severity of PACG in this analysis. Many trials stated no significant difference in VA and VF between the two groups, and our meta-analysis supports their conclusion.15,16,18
Our review included RCTs with a high level of evidence and a large sample size. Despite the variation in the follow-up period, the outcomes of these RCTs demonstrate a low rate of heterogeneity. Additionally, our review provides a comprehensive comparison of Phacoemulsification and LRI, encompassing a wide range of outcomes. Up to our knowledge, this is the only systematic review that has specifically examined and compared phacoemulsification to LPI with respect to number of medications, VF progression, central CCT, PAS, and poor response to surgery that was not evaluated in previous systematic reviews.
We acknowledge that our review has several limitations. Firstly, the variation in follow-up periods among the RCTs hinders our ability to compare intraocular pressure (IOP) at different time points. Additionally, there is a lack of long-term follow-up data, with only one RCT having a ten-year follow-up period. Secondly, there is a need for more data comparing the cost-effectiveness of the two interventions, as only one RCT addresses this aspect. Finally, it is important to note that our inclusion criteria focused solely on RCTs published in the English language.
Conclusions
This systematic review and meta-analysis showed that lens extraction and LPI are effective treatments for PACG. Phacoemulsification demonstrated a statistically significant reduction in average central corneal thickness and central endothelial cell density when compared to LPI. Moreover, Phacoemulsification exhibited a lower likelihood of an inadequate response in the treatment of PACG compared to the LPI group. Nevertheless, there were no notable differences between Phacoemulsification and LPI in terms of average intraocular pressure, medication usage, visual acuity, visual field progression, peripheral anterior synechiae, and average Shaffer gonioscopy grading.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sun X, Dai Y, Chen Y, et al. Primary angle closure glaucoma: what we know and what we don’t know. Prog Retin Eye Res. 2017;57:26–45. doi:10.1016/j.preteyeres.2016.12.003
2. Flores-Sánchez BC, Tatham AJ. Acute angle closure glaucoma. Br J Hosp Med. 2019;80(12):C174–C179. doi:10.12968/hmed.2019.80.12.C174
3. Tham Y-C, Li X, Wong TY, Quigley HA, Aung T, Cheng C-Y. Global prevalence of glaucoma and projections of glaucoma burden through 2040. Ophthalmology. 2014;121(11):2081–2090. doi:10.1016/j.ophtha.2014.05.013
4. Chan PP, Pang JC, Tham CC. Acute primary angle closure–treatment strategies, evidences and economical considerations. EYE. 2019;33(1):110–119. doi:10.1038/s41433-018-0278-x
5. Wang PX, Koh VTC, Loon SC. Laser iridotomy and the corneal endothelium: a systemic review. Acta Ophthalmol. 2014;92(7):604–616. doi:10.1111/aos.12367
6. Javanbakht M, Azuara-Blanco A, Burr JM, et al. Early lens extraction with intraocular lens implantation for the treatment of primary angle closure glaucoma: an economic evaluation based on data from the EAGLE trial. BMJ Open. 2017;7(1):e013254. doi:10.1136/bmjopen-2016-013254
7. Rahmasari AZ, Indri Wahyuni I, Djuari L. Comparison of Intraocular Pressure after Phacoemulsification Compared to Laser Peripheral Iridotomy (LPI) in Acute Primary Angle Closure (APAC) Patients: a Systematic Review. J Curr Med Res Opin. 2022;5(12):1510–1519.
8. Xie J, Li P, Han B, Patel S. Meta-analysis of phacoemulsification and laser peripheral iridotomy in the treatment of primary angle-closure glaucoma. J Ophthalmol. 2023;2023:6732424. doi:10.1155/2023/6732424
9. Higgins JPT, Altman DG, Gøtzsche PC, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343(2):d5928. doi:10.1136/bmj.d5928
10. Borenstein M Comprehensive meta-analysis V2 [Computer software and manual]; 2005:24.
11. Copenhagen J. D.T.N.C.C., Cochrane Collaboration, Review manager. (version 5.3)[computer software].2014.
12. Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557–560. doi:10.1136/bmj.327.7414.557
13. Cumpston M, Li T, Page MJ, et al. Updated guidance for trusted systematic reviews: a new edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Libr. 2019;10:10.
14. Hozo SP, Djulbegovic B, Hozo I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med Res Methodol. 2005;5(1). doi:10.1186/1471-2288-5-13
15. Azuara-Blanco A, Burr J, Ramsay C, et al. Effectiveness of early lens extraction for the treatment of primary angle-closure glaucoma (EAGLE): a randomised controlled trial. Lancet. 2016;388(10052):1389–1397. doi:10.1016/S0140-6736(16)30956-4
16. Chan PP, Tang FY, Leung DY, Lam TC, Baig N, Tham CC. Ten-year clinical outcomes of acute primary angle closure randomized to receive early phacoemulsification versus laser peripheral iridotomy. J Glaucoma. 2021;30(4):332–339. doi:10.1097/IJG.0000000000001799
17. Dias-Santos A, Ferreira J, Abegão Pinto L, et al. Phacoemulsification versus peripheral iridotomy in the management of chronic primary angle closure: long-term follow-up. Int Ophthalmol. 2015;35(2):173–178. doi:10.1007/s10792-014-9926-8
18. Husain R, Gazzard G, Aung T, et al. Initial management of acute primary angle closure: a randomized trial comparing phacoemulsification with laser peripheral iridotomy. Ophthalmology. 2012;119(11):2274–2281. doi:10.1016/j.ophtha.2012.06.015
19. Mitchell WG, Azuara-Blanco A, Foster PJ, et al. Predictors of long-term intraocular pressure control after lens extraction in primary angle closure glaucoma: results from the EAGLE trial. Br J Ophthalmol. 2023;107(8):1072–1078. doi:10.1136/bjophthalmol-2021-319765
20. Bissing A, Rivier D, Zaninetti M, Shaarawy T, Mermoud A, Roy S. Ten years follow-up after deep sclerectomy with collagen implant. J Glaucoma. 2008;17(8):680–686. doi:10.1097/IJG.0b013e318182ed9e
21. Amerasinghe N, Aung T. Angle-closure: risk factors, diagnosis and treatment. In: Progress in Brain Research. Elsevier; 2008:31–45.
22. Wright C, Tawfik MA, Waisbourd M, Katz LJ. Primary angle-closure glaucoma: an update. Acta Ophthalmol. 2016;94(3):217–225. doi:10.1111/aos.12784
23. Tarongoy P, Ho CL, Walton DS, et al. Changes in the anterior chamber configuration after small-incision cataract surgery with posterior chamber intraocular lens implantation. Am J Ophthalmol. 1997;54(2):775–780.
24. Yang CH, Hung PT. Intraocular lens position and anterior chamber angle changes after cataract extraction in eyes with primary angle-closure glaucoma. J Cataract Refract Surg. 1997;23(7):1109–1113. doi:10.1016/S0886-3350(97)80089-2
25. Roberts TV, Francis IC, Lertusumitkul S, Kappagoda MB, Coroneo MT. Primary phacoemulsification for uncontrolled angle-closure glaucoma. J Cataract Refract Surg. 2000;26(7):1012–1016. doi:10.1016/S0886-3350(00)00358-8
26. Jacobi PC, Dietlein TS, Lüke C, Engels B, Krieglstein GK. Primary phacoemulsification and intraocular lens implantation for acute angle-closure glaucoma. Ophthalmology. 2002;109(9):1597–1603. doi:10.1016/S0161-6420(02)01123-5
27. Wyatt H, Ghosh J. Behaviour of an iris model and the pupil block hypothesis. Br J Ophthalmol. 1970;54(3):177–185. doi:10.1136/bjo.54.3.177
28. Lowe RF. Aetiology of the anatomical basis for primary angle-closure glaucoma. Biometrical comparisons between normal eyes and eyes with primary angle-closure glaucoma. Br J Ophthalmol. 1970;54(3):161–169. doi:10.1136/bjo.54.3.161
29. Lowe RF. Causes of shallow anterior chamber in primary angle-closure glaucoma: ultrasonic biometry of normal and angle-closure glaucoma eyes. Am J Ophthalmol. 1969;67(1):87–93. doi:10.1016/0002-9394(69)90012-9
30. Ming Zhi Z, Lim ASM, Yin Wong T. A pilot study of lens extraction in the management of acute primary angle-closure glaucoma. Am J Ophthalmol. 2003;135(4):534–536. doi:10.1016/S0002-9394(02)02108-6
31. Kubota T, Toguri I, Onizuka N, Matsuura T. Phacoemulsi- fication and intraocular lens implantation for angle closure glaucoma after the relief of pupillary block. Ophthalmologica. 2003;217(5):325–328. doi:10.1159/000071346
32. Wang J-K, Lai P-C. Unusual presentation of angle-closure glaucoma treated by phacoemulsification. J Cataract Refract Surg. 2004;30(6):1371–1373. doi:10.1016/j.jcrs.2003.10.027
33. Harasymowycz PJ, Papamatheakis DG, Ahmed I, et al. Phacoemulsification and goniosynechialysis in the management of unresponsive primary angle closure. J Glaucoma. 2005;14(3):186–189. doi:10.1097/01.ijg.0000159131.38828.85
34. Nonaka A, Kondo T, Kikuchi M, et al. Cataract surgery for residual angle closure after peripheral laser iridotomy. Ophthalmology. 2005;112(6):974–979. doi:10.1016/j.ophtha.2004.12.042
35. Lai JSM, Tham CCY, Chan JCH. The clinical outcomes of cataract extraction by phacoemulsification in eyes with primary angle-closure glaucoma (PACG) and co-existing cataract: a prospective case series. J Glaucoma. 2006;15(4):346. doi:10.1097/01.ijg.0000212231.65545.9a
36. Liu CJ-L, Cheng C-Y, Wu CW, Lau L-I, Chou JC, Hsu W-M. Factors predicting intraocular pressure control after phacoemulsification in angle-closure glaucoma. Arch Ophthalmol. 2006;124(10):1390–1394. doi:10.1001/archopht.124.10.1390
37. Imaizumi M, Takaki Y, Yamashita H. Phacoemulsification and intraocular lens implantation for acute angle closure not treated or previously treated by laser iridotomy. J Cataract Refract Surg. 2006;32(1):85–90. doi:10.1016/j.jcrs.2005.11.014
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.