Back to Journals » Cancer Management and Research » Volume 18

PET-MR Examination in Diagnosing Bone Metastases in Prostate Cancer
Authors Su X, Li K, Wang J, Jiang Z, Shan L
Received 8 October 2025
Accepted for publication 29 May 2026
Published 19 June 2026 Volume 2026:18 572865
DOI https://doi.org/10.2147/CMAR.S572865
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Yong Teng
Xiang Su, Kehan Li, Jianan Wang, Zhaoqiang Jiang, Lei Shan
Department of Urology, Henan Provincial People’s Hospital, Zhengzhou, Henan, 450000, People’s Republic of China
Correspondence: Lei Shan, Department of Urology, Henan Provincial People’s Hospital, No. 7 Weiwu Road, Jinshui District, Zhengzhou, Henan, 450000, People’s Republic of China, Email [email protected]
Background: Positron Emission Tomography-magnetic resonance (PET-MR) has the advantage of high contrast and has a high potential for diagnosing bone metastases in prostate cancer (PC). This study assesses the effectiveness of PET-MR imaging for detecting bone metastasis in PC.
Methods: A total of 212 prostate cancer patients admitted to our hospital from June 2021 to June 2024 were selected, all of whom were diagnosed with prostate cancer through pathological puncture. According to the most valuable comparative method (BVC), patients were divided into a bone metastasis group (n=40) and a non-bone metastasis group (n=172). General information such as age was collected and compared between the two groups of patients. PET-MR examination was performed on all patients, and the number of lesions was recorded (a total of 95 bone metastases were detected). Among them, BVC confirmed 58 metastatic lesions (due to the presence of multiple site metastases in some patients). The Gleason score, SUVmax, and ADCmin levels were compared between groups. ROC curve analysis determined the AUC, sensitivity, and specificity. Multivariate Logistic regression identified influencing factors.
Results: Among patients with bone metastases, 38 patients with positive PET-MR (95.00%) and 169 patients with non-bone metastases (79.72%) were PET-MR negative. The sensitivity of PET-MR in diagnosing prostate cancer bone metastasis was 95.00% (95% CI: 83.5% - 99.4%), the specificity was 79.72% (95% CI: 73.1% - 85.3%), the positive predictive value was 92.68% (95% CI: 80.1% - 98.4%), and the negative predictive value was 98.83% (95% CI: 95.8% - 99.9%). The proportion of PET-MR diagnosed prostate cancer bone metastases with pelvic, spinal, extremity, rib, and scapular lesions were 31.03%, 44.83%, 8.62%, 3.45%, and 87.93%, respectively. Compared with the non-metastatic group, the proportion of patients with Gleason score > 9, the proportion of tPSA > 100 ng/mL, ALP level and SUVmax and SUVmax/ADCmin levels were significantly higher in the metastatic group. ADCmin levels were significantly lower, and the differences were statistically significant (P < 0.05). Factors such as PET-MR positivity, Gleason score > 9, tPSA > 100 ng/mL, ALP level, SUVmax, ADCmin and SUVmax/ADCmin were significant risk factors for bone metastasis (P< 0.05). The AUC of SUVmax, ADCmin and SUVmax/ADCmin in the diagnosis of bone metastasis of prostate cancer were 0.756, 0.777 and 0.864, respectively. SUVmax, ADCmin and SUVmax/ADCmin were abnormally expressed in bone metastases of PC by PET-MR examination.
Conclusion: SUVmax, ADCmin, and SUVmax/ADCmin are significantly abnormally expressed in patients with prostate cancer bone metastases during PET-MR examination. The sensitivity and specificity of PET-MR in diagnosing prostate cancer bone metastasis are 95.00% and 79.72%, respectively. Among them, the SUVmax/ADCmin ratio has the best diagnostic efficacy (AUC = 0.864, sensitivity 76.74%, specificity 82.50%). PET-MR has certain value in the diagnosis of prostate cancer bone metastasis and can be used as a reference indicator for clinical auxiliary evaluation.
Keywords: PET-MR, prostate cancer, bone metastasis, clinical value
Background
Prostate cancer (PC) refers to the malignant tumor occurring in the prostate epithelium, which is caused by the canceration of the epithelial cells of the Prostate to form a mass. PC is a male malignant tumor with a high incidence worldwide, accounting for the first incidence of male malignant tumor in the world and the second mortality rate.1,2 At present, the prevalence of PC in China is lower than that in western countries. However, with the aggravation of population aging and changes in eating and living habits in recent years, the number of PCa patients in China has increased year by year, and it has become one of the common diseases that threaten the normal life of men. The metastasis rate of PC is high, and cancer metastasis is the main cause of death in advanced PC. Bone is the main site of PC metastases. After bone metastases, patients may experience skeletal events such as pain, pathological fractures, and bone compression, which also seriously affect the prognosis of patients. Recent studies have found that the 1-year and 5-year survival rates of PC patients without bone metastases are 87% and 56%, respectively, while the 1-year and 5-year survival rates are only 47% and 3% in PC patients with bone metastases. Early diagnosis of PC bone metastases and effective intervention can greatly improve the quality of life of patients and reduce the suffering of patients.3,4
Electron emission tomography (Positron Emission Tomography, PET) is a non-invasive imaging method. It can reflect the metabolic activity of lesions and has obvious advantages in monitoring early malignant lesions and recurrent and metastatic lesions, but it has certain limitations in displaying tissue anatomy when the spatial resolution is low. Magnetic resonance (MR) has more advantages in the imaging of soft tissue, and can detect early lesions before they appear osteogenic burning shadows. With the rapid development of imaging technology in recent years, PET-MR has been gradually applied in clinical practice. PET-MR integrates the human physiological metabolism and molecular information provided by PET, and the anatomical and morphological information provided by MR. It has the advantage of high contrast and has a high potential for diagnosing bone metastases in PC.4,5
In this study, 212 patients with PC who were treated in our hospital from June 2021 to June 2024 were selected as the observation objects. The purpose of this study was to analyze the evaluation value of PET-MR in bone metastasis of PC.
Materials and Methods
General Information
A total of 212 PC patients admitted to our hospital from June 2021 to June 2024 were selected. Inclusion criteria: (1) All patients met the relevant diagnostic criteria for PC in the European Society of Urogenital Radiology.6 All patients were diagnosed as PC by pathological puncture, and the tumor was visible and clearly displayed. (2) PET-MR examination was performed before the pathological puncture, and the image data was intact and the image quality was good. (3) No related operations such as surgical resection, chemotherapy, radiotherapy, etc. (4) The patients and their families were informed, had good compliance, and could cooperate with the examination and treatment. All signed the informed consent.
Exclusion criteria: (1) The patient has previously received treatment related to prostate cancer (including surgery, radiotherapy, chemotherapy, endocrine therapy, etc). The treatment history has been confirmed through medical records and the patient’s own account. (2) Patients with other malignant tumors. (3) Patients with severe dysfunction of vital organs. (4) Incomplete clinical data of the patient, or poor image quality. (5) Existing bone-related diseases in the past. (6) The patients were hospitalized with severe systemic infection. To control for confounding factors, this study ensured the homogeneity of the study population through strict inclusion and exclusion criteria. All patients were newly diagnosed and untreated prostate cancer patients, and those with previous treatments or related diseases that might affect the imaging manifestations were excluded.
Based on the Best Valid Comparator (BVC) method, the patients were divided into the bone metastasis group (n=40) and the non-bone metastasis group (n=172). The BVC was defined as a composite reference standard, and the specific criteria for determination were as follows: (1) The pathological examination of bone biopsy revealed cancer cells (a total of 12 patients underwent CT-guided bone puncture biopsy due to suspected lesions. The biopsy sites included the spine, pelvis, etc. The pathological report indicated that that cancer cell infiltration was judged as bone metastasis). (2) A comprehensive judgment was made based on the combined assessment of imaging follow-up and clinical data in case of no pathological results. The requirements for imaging follow-up were as follows: a whole-body bone imaging or the same site CT/MRI was conducted at six months (±2 weeks) after the PET-MR examination. If any of the following progression manifestations occur in the original suspicious lesion - an expansion of bone destruction area, new osteolytic or osteoblastic lesions, a significant increase in the radioactive nuclide concentration compared to before (a visual score increase of ≥ 2 levels), or the appearance of new bone metastases - it was determined as bone metastasis.
Clinical comprehensive judgment criteria: at least two of the following three conditions were met simultaneously: (a) Pain symptoms consistent with the site of bone metastasis (visual analogue score ≥ 4 points and excluding other causes); (b) Serum alkaline phosphatase (ALP) level exceeds the upper limit of normal by 1.5 times, and there was no other explanation such as liver or gallbladder diseases; (c) Prostate-specific antigen (PSA) was increased by ≥ 25% compared to the previous value and the absolute value was ≥ 2 ng/mL (in line with the definition of prostate cancer progression).
Judgment process: Two senior physicians (one from the nuclear medicine department and the other from the orthopedics department, with over 10 years of experience each) independently evaluated all patients’ pathological, imaging follow-up, and clinical data without knowing the PET-MR results. They compared and determined whether each case was a bone metastasis according to the above standards item by item. They reached a consensus through negotiation when the opinions were not in agreement. The final decision was made by the third chief physician (radiology department, with over 15 years of experience in diagnosing bone tumors through imaging). After confirmation by BVC, there were a total of 58 metastatic lesions in 40 patients with bone metastasis (some patients had multiple metastases, with an average of 1.45 metastatic lesions per patient), and no clear signs of bone metastasis were observed in 172 patients without bone metastasis.
General data selection was displayed in Figure 1. Initially, a total of 256 prostate cancer patients were screened, of which 44 were excluded (including 12 who had received previous treatment, 18 with incomplete imaging data, 8 with other malignant tumors, and 6 who refused to participate), and ultimately 212 were included.
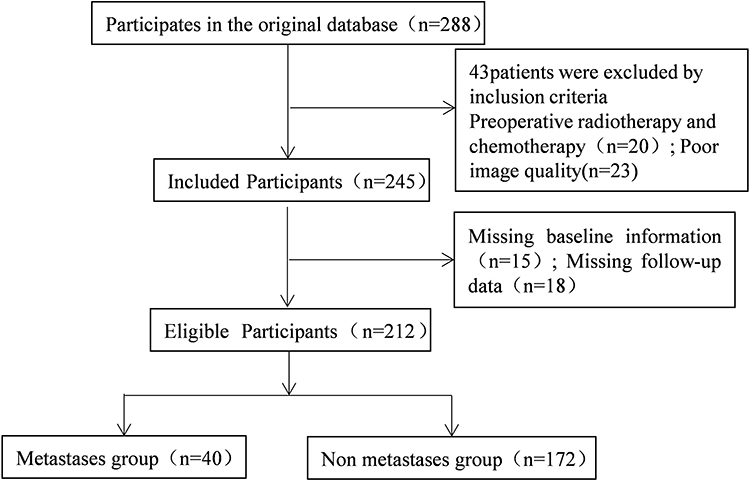 |
Figure 1 Flowchart of general data selection. |
Methods
All patients were examined by PET-MR with Siemens Biograph mMR PET-MR integrated machine in Germany. This device integrated a 3.0 T superconducting MR scanner with a PET detection system according to the protocol. The PET imaging used the tracer 18F-FDG (fluorodeoxyglucose), with a radiochemical purity of over 95%. The dose was administered at 3.7 MBq/kg via the elbow vein, and collection was made at 60 minutes after injection. During this period, speaking, chewing, and vigorous activities were avoided to minimize physiological uptake. The patient fasted for 4 hours before the examination, rested quietly for 10 minutes, and took a supine position after emptying the bladder. Whole body PET-MR imaging scans were performed, including four segments of head and neck, chest, abdomen and pelvis, followed by T2WI and DWI examinations. The MR scanning sequences including: coronal T1WI, DWI (b values = 0, 800, 1000 s/mm2), fat-suppression T2WI imaging of the pelvis and vertebral bodies, and contrast-enhanced scan. The collection was performed using the 3D List mode. The collection time was 3 minutes per bed, and a total of 6–7 beds were collected (covering from the head to the middle section of the thighs). The image reconstruction used the OSEM algorithm (3 iterations, 172×172 matrix, 21 subsets).
Using Siemens Syngo True D workstation to fuse PET and ADC images. Then, regions of Interest (ROI) were selected, and the maximum standard uptake values for localized prostate lesions (SUVmax) and the minimum apparent diffusion coefficient of the prostate (Apparent diffusion coefficient min, ADC min) were calculated. Calculate the SUVmax/ADCmin ratio. See Table 1 for detailed parameters.
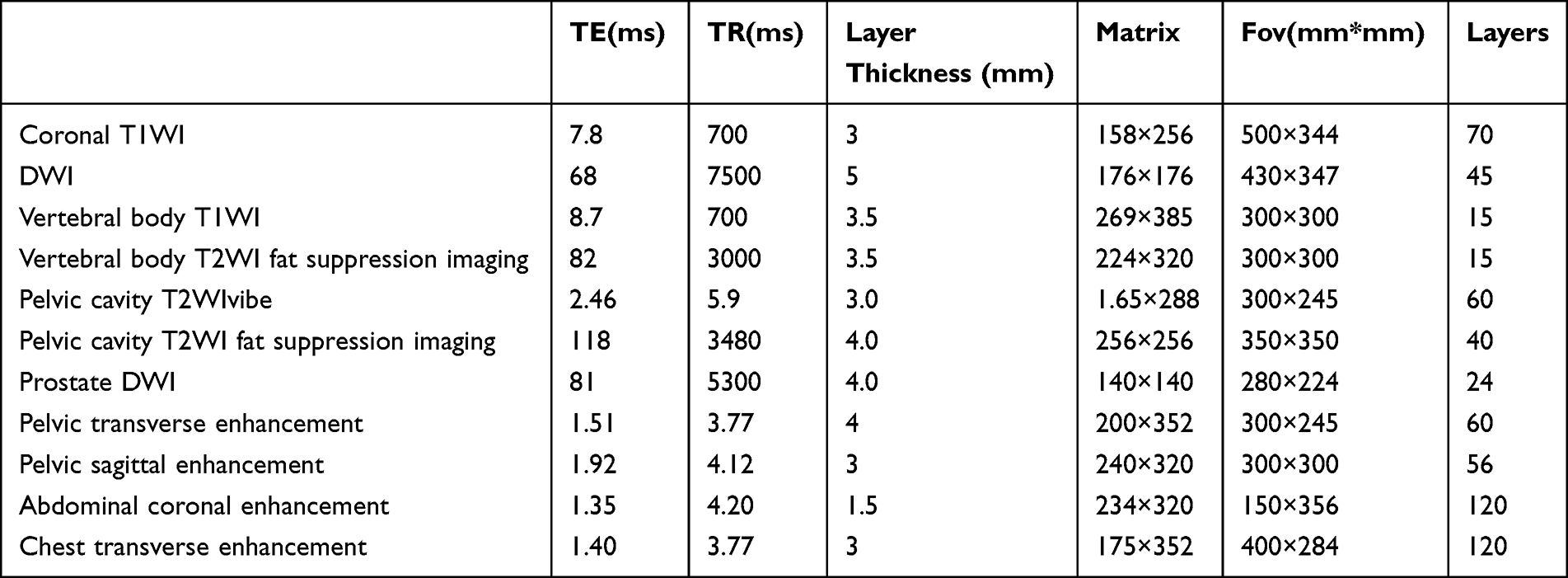 |
Table 1 PET-MR Examination of Sequences and Related Parameters |
Precautions: diabetic patients need to control blood glucose < 11.1 mmol/L before examination. After the injection of the tracer, patients were advised to drink plenty of water and urinate frequently to minimize the interference of bladder radioactivity on pelvic images.
Image interpretation was independently conducted by two nuclear medicine physicians, both of whom were unaware of the BVC results and clinical data (including pathology and laboratory tests). In case of inconsistent interpretations, consensus was reached through consultation. The final decision was made by the third senior physician (chief physician) when there was still inconsistency. The Kappa coefficient was used to assess the inter-observer consistency in the judgment of PET-MR positive/negative, with a Kappa value of 0.86 (95% CI: 0.79–0.93). The intraclass correlation coefficient (ICC) was used to evaluate the consistency of continuous variable measurements such as SUVmax and ADCmin, with an ICC value of 0.91 (95% CI: 0.86–0.94).
Observation Indicators
- Collect the fasting venous blood of the patients in the morning, and use an automatic biochemical analyzer to detect the levels of total prostate-specific antigen (t-PSA), alkaline phosphatase (ALP), and hemoglobin (Hb). All operations were carried out in accordance with the instructions.
- Gleason score: Two deputy chief physicians from the pathology department performed Gleason scores on the HE-stained specimens of histopathological sections of all patients. Due to the morphological heterogeneity of prostate cancer, multiple histological structures were common in the same specimen, therefore, the Gleason score (2–10) was calculated from the sum of the primary tissue score (1–5) and the secondary tissue score (1–5). The score was negotiated when the two physicians have any dispute over the results.
Statistical Methods
SPSS 20.0 software was used to analyze the experimental data. The measurement data such as age, BMI value, SUVmax, ADCmin, SUVmax/ADCmin were expressed as (x±s). The comparison between the two groups was performed using an independent sample t test. The indicators that did not conform to the normal distribution were expressed as [median (interquartile range)], and the rank sum test was taken to compare the differences between groups. Gleason score, PET-MR positive, PET-MR negative and other count data were expressed as frequency or percentage. Comparisons between groups were performed using the χ2 test or Fisher’s exact test. Multivariate logistic regression was applied to analyze the influencing factors of PC bone metastasis. All diagnostic efficacy indicators (AUC, sensitivity, specificity) were calculated with 95% confidence intervals. Results were considered statistically significant at P < 0.05.
Results
Analysis of PET-MR in the Diagnosis of PC Bone Metastases
Among the patients with bone metastases, 38 patients were PET-MR positive, accounting for 95.00%. Besides, among the non-bone metastases, 169 patients were PET-MR negative, accounting for 79.72% (Table 2). The sensitivity of PET-MR in diagnosing bone metastasis of prostate cancer was 95.00% (95% CI: 83.5–99.4%), the specificity was 79.72% (95% CI: 73.1–85.3%), the positive predictive value was 92.68% (38/41), and the negative predictive value was 98.83% (169/171, Table 2).
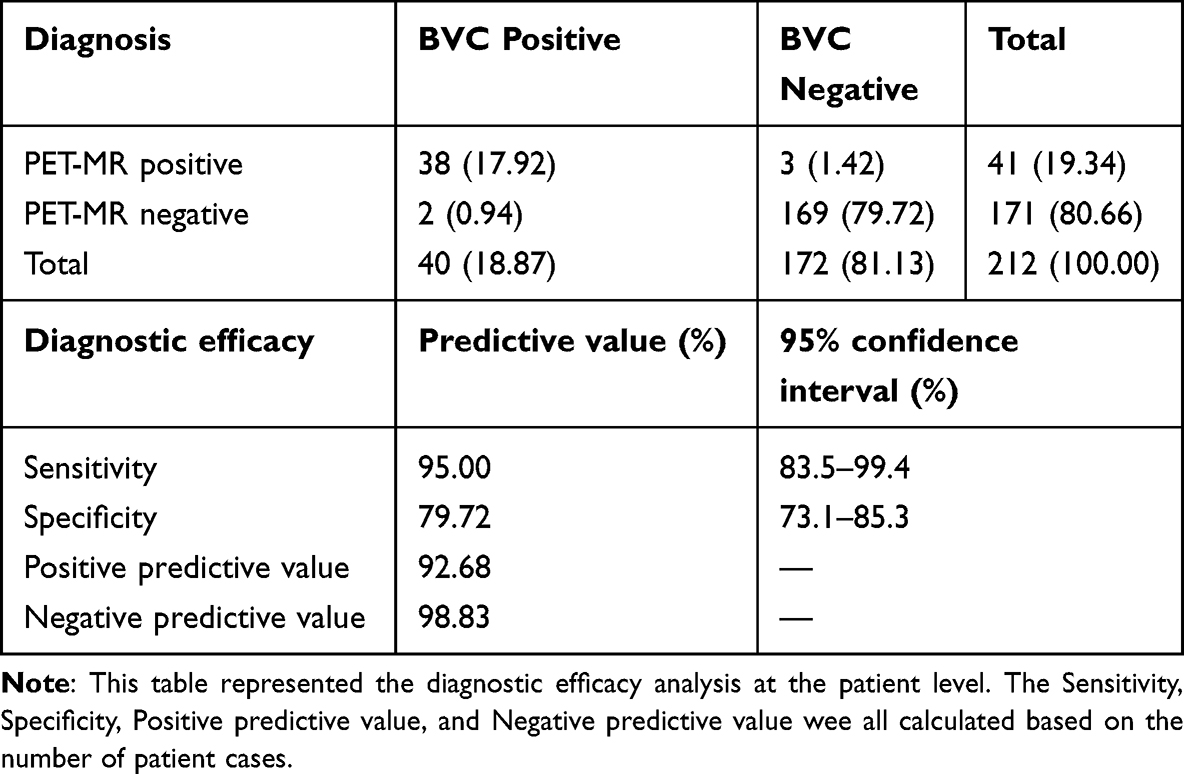 |
Table 2 Analysis of PET-MR in Diagnosis of PC Bone Metastases (Cases, %) |
Analysis of Detected Lesions in PET-MR Diagnosis of PC Bone Metastases
Among the 40 patients with bone metastasis, 18 cases (45.00%) had multiple site metastases. 58 bone metastases were detected by BVC. The proportions of pelvis, spine, limbs, ribs, and scapula lesions diagnosed by PET-MR were 31.03%, 44.83%, 8.62%, 3.45%, and 87.93%, respectively, accounting for 87.93% in total. The difference between the two inspection methods was observable (P<0.05). Among them, spinal metastasis was the most common, followed by pelvic metastasis (Table 3).
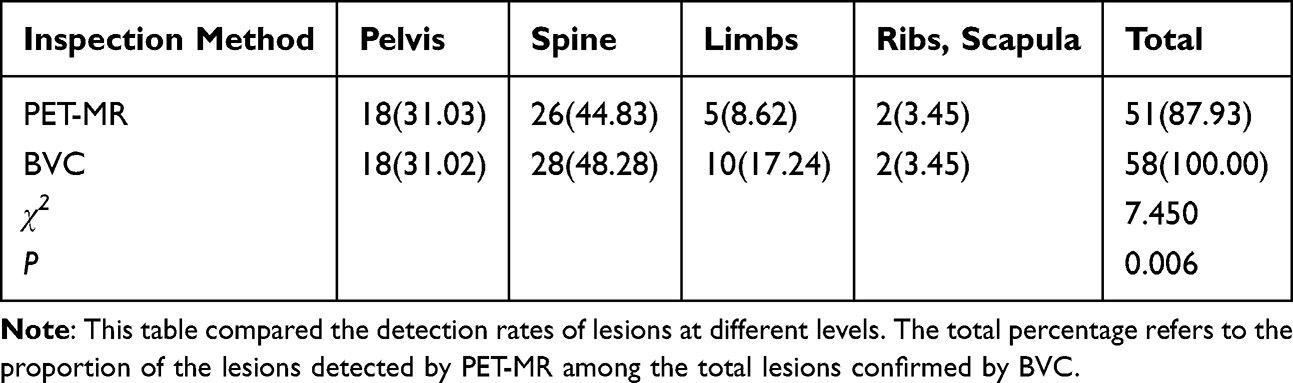 |
Table 3 Analysis of Lesions Detected by PET-MR in Diagnosis of PC Bone Metastases (Cases, %) |
The Value of PET-MR in the Diagnosis of PC Bone Metastasis
ROC curve analysis exhibited that the AUC of PET-MR in the diagnosis of PC bone metastases was 0.851, the sensitivity was 95.00%, and the specificity was 79.72% (Table 4 and Figure 2).
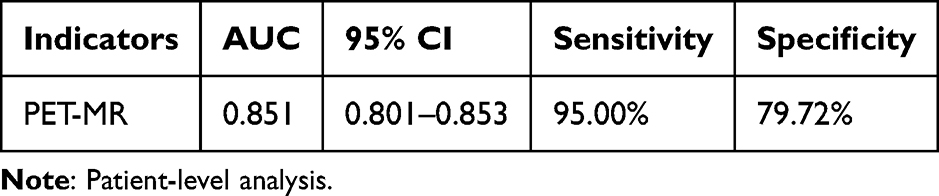 |
Table 4 Value of PET-MR in the Diagnosis of PC Bone Metastases |
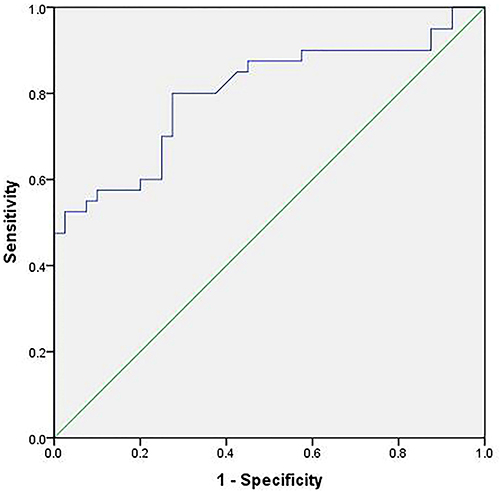 |
Figure 2 ROC curve of PET-MR in the diagnosis of bone metastases from PC patients (at the patient level). |
Univariate Analysis of the Influencing Factors of PC Bone Metastasis
Compared with the non-metastatic group, the proportion of Gleason score>9 points (62.50% vs. 30.81%), the proportion of tPSA>100 ng/mL (92.50% vs. 56.98%), the ALP level (236.15 (98.56–349.86) U/L vs. 78.50 (53.56–125.33) U/L), SUVmax (6.89±0.38 vs. 5.86±0.51), SUVmax/ADCmin level (14.06±1.63 vs. 8.75±2.05) of the patients in the metastatic group were evidently increased, and the ADCmin level ((0.49±0.12 vs. 0.67±0.08)×10−3 mm2/s) was strongly decreased. The differences were memorably significant (P <0.05, Table 5).
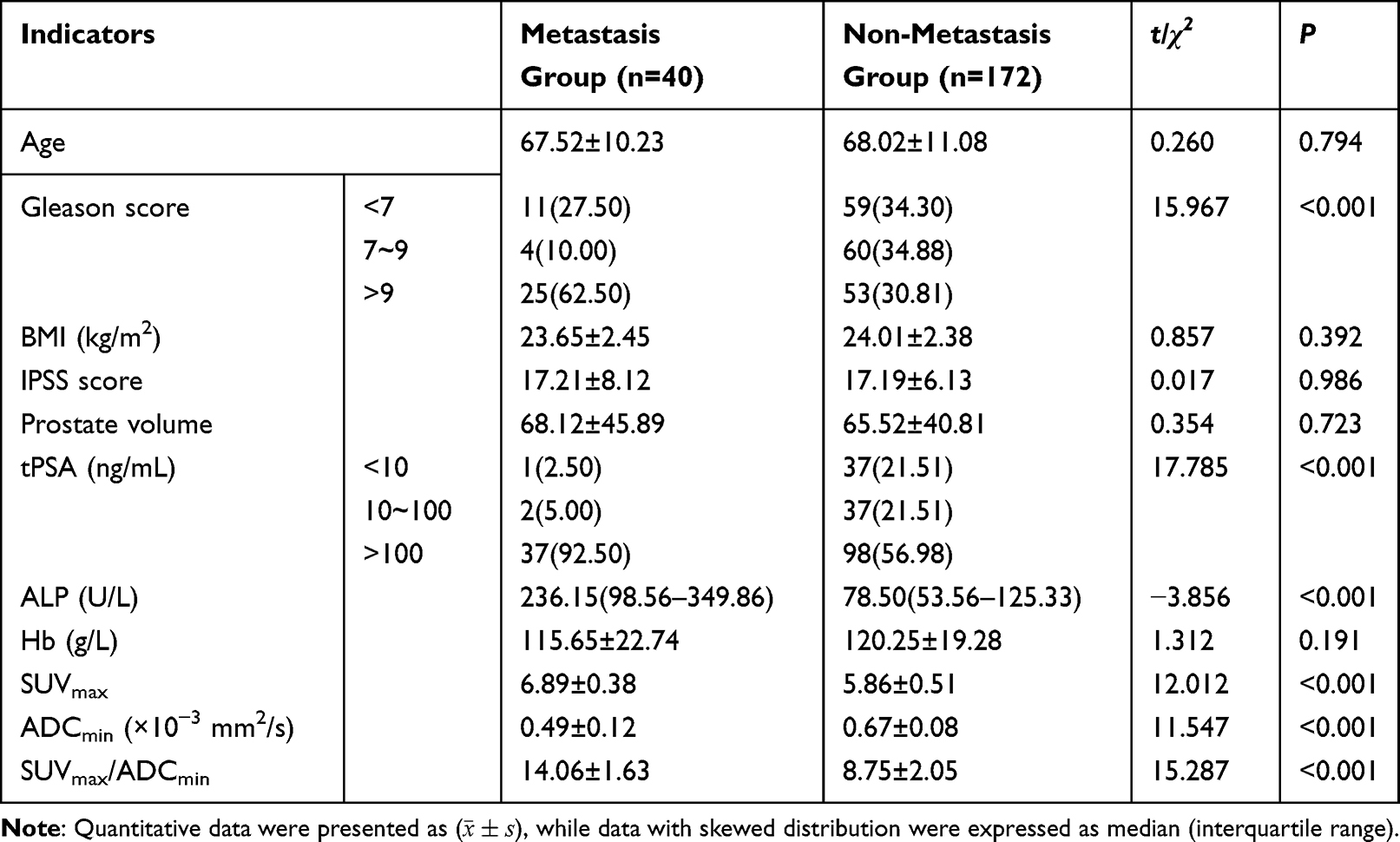 |
Table 5 Comparison of Clinical Data and PET-MR Indexes Between the Two Groups of Patients (x±s) |
Multivariate Logistic Regression Analysis
The 7 factors with statistical significance in the univariate analysis were subjected to multivariate logistic regression analysis. The results demonstrated that the PET-MR positive, proportion of Gleason score>9 points, the proportion of tPSA>100 ng/mL, ALP level, SUVmax and SUVmax/ADCmin and ADCmin value were the main risk factors affecting PC bone metastasis (P < 0.05, Table 6).
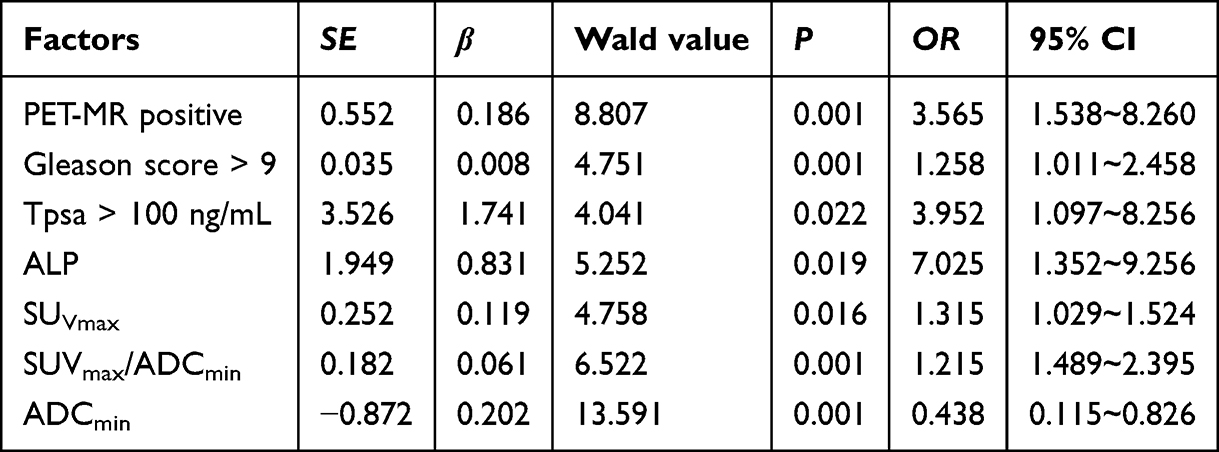 |
Table 6 Results of Multivariate Logistic Regression Analysis |
ROC Curve Analysis
The results of the ROC curve analysis showed that the optimal cutoff value for SUVmax in diagnosing bone metastasis of prostate cancer was 6.25, with an AUC of 0.756 (95% CI: 0.667–0.826), a sensitivity of 77.91%, and a specificity of 67.50%. The optimal cutoff value for ADCmin was 0.58×10−3 mm2/s, with an AUC of 0.777 (95% CI: 0.690–0.864), a sensitivity of 68.02%, and a specificity of 77.50%. The optimal cutoff value for SUVmax/ADCmin was 11.35, with an AUC of 0.864 (95% CI: 0.810–0.918), a sensitivity of 76.74%, and a specificity of 82.50% (Table 7 and Figure 3).
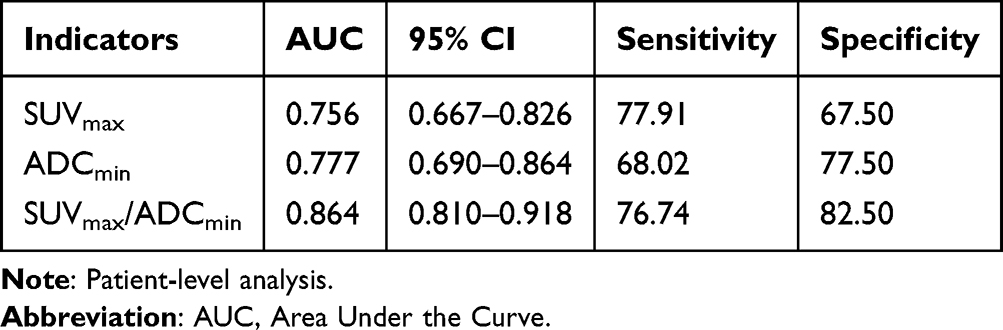 |
Table 7 ROC Curve Analysis |
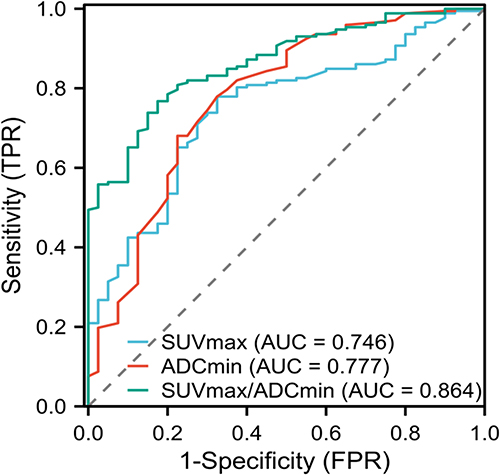 |
Figure 3 ROC curve analysis of SUVmax, SUVmax/ADCmin and ADCmin in the diagnosis of bone metastases from PC patients (at the patient level). |
Discussion
PC is the male malignant tumor with the highest clinical incidence. It has the characteristics of high metastasis rate and high mortality rate. With the change of work style and the aggravation of population aging in recent years, the number of patients with PC is increasing year by year. PC not only brings inconvenience and great pain to patients, but also consumes medical resources.7,8 Therefore, how to reduce the incidence of PC and improve the prognosis of PC patients has become the focus of medical scholars all over the world.
The early symptoms of PC are not obvious, most patients are already in the middle and late stages when they are diagnosed, and they are often accompanied by bone metastases.9 Previous statistics showed that metastatic and invasive PC patients who survived for 5 years accounted for only 25% of all PC patients. Early diagnosis of PC, tumor staging, metastasis prediction, and targeted intervention are beneficial to improve the cure rate, and are of great significance in prolonging the life of patients and improving the quality of life of patients. At present, the methods of clinical diagnosis of bone metastases include ultrasound-guided needle biopsy, bone ECT, MEI, single photon emission computed tomography, and PET-MR, etc.10,11 However, ultrasound-guided puncture biopsy is a puncture examination, which is invasive and causes certain damage to the patient’s body. Bone ECT is the main method for the traditional diagnosis of bone metastases in PC patients with high sensitivity, but its specificity is poor. MRI requires multiple examinations and can accurately evaluate various parts of the body, which not only consumes a long time, but also has high detection costs. Multiple imaging examinations also cause greater radiation damage to patients.12 Single-photon emission computed tomography is more susceptible to the influence of the body itself. The tissue degeneration and inflammatory response can also affect the inspection results.13,14 PET-MR is an emerging imaging technology that can scan directly from the head to the middle of the thigh, with a wide scanning range. A single examination can effectively evaluate and predict the metastatic lesions, and the radiation damage is small. At the same time, PET-MR can also accurately provide information on the morphology and function of lesions, which is helpful for the diagnosis of PCa bone metastases and the guidance of treatment plans.15,16 In this study, compared with the non-metastatic group, the proportion of Gleason score≥9 points, SUVmax and SUVmax/ADCmin levels in the metastatic group were notably elevated, and the ADCmin level was markedly decreased. These results suggest that SUVmax, ADCmin, and SUVmax/ADCmin are significantly abnormally expressed in PC bone metastases detected by PET-MR, which were similar to the results of Wilk’s study. They pointed out that SUVmax value can well differentiate PC from BPH, which can improve the sensitivity and specificity of PC bone metastases diagnosis.17 The reason may be related to the large number of tumor tissue cells, high density, obvious glucose metabolism, and limited diffusion of water molecules in PC complicated with bone metastases.
PC has a high probability of bone metastasis, and bone metastasis is the main cause of death in PC patients. Early identification of whether PC complicated with bone metastasis is of great significance for effective targeted therapy and improvement of patient prognosis.18 In this study, 95.00% of patients with bone metastases were positive by PET-MR, and 79.72% of patients without bone metastases were negative by PET-MR. 87.93% of PC bone metastases were diagnosed by PET-MR. Among them, the detection of scapula lesions accounted for the highest proportion, accounting for 87.93%. It is suggested that PET-MR examination has good potential in diagnosing bone metastases and bone metastases in PC patients. However, Buckup et al3 believed that PC bone metastases mostly occurred in the spine and pelvis, and then gradually transferred to other bone tissues throughout the body. Therefore, we speculate that scapula lesions are often accompanied by metastases to the spine and/or pelvis. PC is a kind of osteophilic tumor. 30% of patients have bone metastases at the time of treatment, and the early symptoms are not typical. Therefore, identify the presence or absence of bone metastases at early time has become the focus of andrology medical staff. This study found that the proportion of Gleason score >9 points, the proportion of tPSA >100 ng/mL, ALP level, SUVmax, SUVmax/ADCmin were the risk factors for bone metastasis of PC. These findings suggest PET-MR examination has certain clinical value in diagnosing bone metastasis of PC, which can help doctors in early diagnosis and give targeted treatment, and is helpful in improving the prognosis of patients and prolonging the life of patients.
In this study, the average SUVmax value of the metastasis group was 6.89 ± 0.38, the average ADCmin value was 0.49 ± 0.12 × 10−3 mm2/s, and the average SUVmax/ADCmin value was 14.06 ± 1.63. ROC analysis showed that the AUC of SUVmax/ADCmin for diagnosing bone metastasis was 0.864, the optimal cut-off value was 11.35, the sensitivity was 76.74%, and the specificity was 82.50%. Compared with previous studies, the prospective study conducted by Zacho et al19 showed that the AUC of DWI-MRI for diagnosing bone metastasis of prostate cancer was 0.59–0.62, which was lower than the AUC of ADCmin in this study (0.777). The difference might be related to the selection of b value (in this study, b = 600 s/mm2), field strength, and patient population (biochemical recurrence vs. initial diagnosis). Liu et al20 conducted a network Meta-analysis involving 45 studies, and the results showed that the sensitivity and specificity of 3.0T high-quality MRI in diagnosing bone metastasis of prostate cancer at the patient level were both 0.94, which was close to the efficacy of PSMA PET/CT, supporting the good diagnostic value of the quantitative parameters of PET-MR in this study (especially the AUC of the ratio of SUVmax/ADCmin = 0.864). The above results indicated that the quantitative parameters of PET-MR had good consistency and repeatability in differentiating bone metastases. Additionally, in this study, only 40 cases were included in the metastasis group, resulting in a relatively small sample size. This may affect the stability and extrapolation ability of the obtained critical values. A smaller sample size may lead to a large sampling error in the estimation of cut-off values, thereby reducing their diagnostic accuracy in external populations. Therefore, the optimal cut-off value proposed in this study (such as SUVmax/ADCmin = 11.35) still needs to be verified in larger-scale multicenter studies. The tracer used in this study was 18F-FDG. Its application in prostate cancer has certain limitations. The uptake of FDG is related to the glucose metabolic activity of tumor cells. In low-grade prostate cancer (Gleason score ≤ 6) or hormone-sensitive prostate cancer, the metabolic activity is often low, and the FDG uptake is not significant, which may lead to false-negative results.21,22 Therefore, the conclusions based on SUVmax in this study are mainly applicable to patients with intermediate or high-grade (Gleason score ≥ 7) or castration-resistant prostate cancer. But their general applicability is limited for low-grade or hormone-sensitive patients. A comprehensive judgment is required based on the patient’s pathological grade and hormone status in clinical applications.
This study has the following limitations: this study is a single-center retrospective design, with a single source of cases, which may introduce selection bias and limit the external validity of the results. The research conclusions should be used with caution when generalized to other populations. PSMA PET was not included as a control. PSMA PET/CT is currently the standard method for prostate cancer staging and bone metastasis detection,23 with higher tumor specificity. Due to the fact that PSMA PET was not routinely performed in our hospital during the study period, a direct comparison could not be made, which limited the comparability between the results of this study and current clinical standards. The sample size of the metastasis group was small (n=40), which may affect the statistical power and subgroup analysis. Future studies should include PSMA PET as a control and conduct prospective, multi-center research to further verify the accuracy and clinical application value of PET-MR in the diagnosis of prostate cancer bone metastasis.
Conclusion
In conclusion, the indicators (SUVmax, ADCmin, and SUVmax/ADCmin) examined by PET-MR were notably abnormal in PC bone metastases. The sensitivity of PET-MR in diagnosing bone metastasis of prostate cancer was 95.00%, and the specificity was 79.72%. Among them, the diagnostic efficacy of the SUVmax/ADCmin ratio was the best, with an AUC of 0.864, a sensitivity of 76.74%, and a specificity of 82.50%. This suggests that PET-MR has certain value in the diagnosis of bone metastasis of prostate cancer and can be used as a reference indicator for clinical auxiliary assessment. In this study, a total of 95 PET-MR positive lesions were detected in 40 patients with bone metastases, of which 58 metastatic lesions were confirmed by BVC. The difference was due to the presence of multiple site metastases in some patients (such as spinal cord combined with pelvic metastasis). In the future, prospective and multi-center studies should be conducted and directly compared with the PSMA-PET criteria, which perform better in prostate cancer staging, to further validate the conclusions of this study.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
This research was approved by the Ethics Review Committees of Henan Provincial People’s Hospital.
Consent to Participate
Informed consent was obtained from every human participant in the study and the patients participating in the study all agree to publish the research results.
Funding
No funding was received.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Akoto T, Saini S. Role of exosomes in prostate cancer metastasis. Int J Mol Sci. 2021;22(7):3528. doi:10.3390/ijms22073528
2. Zhang X. Interactions between cancer cells and bone microenvironment promote bone metastasis in prostate cancer. Cancer Commun. 2019;39(1):76. doi:10.1186/s40880-019-0425-1
3. Buckup M, Rice MA, Hsu EC, et al. Plectin is a regulator of prostate cancer growth and metastasis. Oncogene. 2021;40(3):663–11. doi:10.1038/s41388-020-01557-9
4. Chu C, Alshalalfa M, Sjstrm M, et al. Characterization of PSMA and 18F-fluciclovine transporter gene expression in localized prostate cancer. J Clin Oncol. 2020;38(6):295. doi:10.1200/JCO.2020.38.6_suppl.295
5. Weber W. Clinical PET/MR. Recent Results Cancer Res. 2020;216:747–764.
6. Mottet N, van den Bergh RCN, Briers E, et al. EAU-EANM-ESTRO-ESUR-SIOG guidelines on prostate cancer-2020 update. part 1: screening, Diagnosis, and Local Treatment with Curative Intent. Eur Urol. 2021;79(2):243–262. doi:10.1016/j.eururo.2020.09.042
7. Göbel A, Dell’Endice S, Jaschke N, et al. The role of inflammation in breast and prostate cancer metastasis to bone. Int J Mol Sci. 2021;22(10):5078. doi:10.3390/ijms22105078
8. Boevé LMS, Hulshof MCCM, Vis AN, et al. Effect on survival of androgen deprivation therapy alone compared to androgen deprivation therapy combined with concurrent radiation therapy to the prostate in patients with primary bone metastatic prostate cancer in a prospective randomised clinical trial: data from the HORRAD trial. Eur Urol. 2019;75(3):410–418. doi:10.1016/j.eururo.2018.09.008
9. Kwatra NS, Lim R, Gee MS, States LJ, Vossough A, Lee EY. PET/MR imaging:: current updates on pediatric applications. Magn Reson Imaging Clin N Am. 2019;27(2):387–407. doi:10.1016/j.mric.2019.01.012
10. Domachevsky L, Bernstine H, Goldberg N, et al. Comparison between pelvic PSMA-PET/MR and whole-body PSMA-PET/CT for the initial evaluation of prostate cancer: a proof of concept study. Eur Radiol. 2020;30(1):328–336. doi:10.1007/s00330-019-06353-y
11. Weber M, Kurek CE, Barbato F, et al. PSMA-Ligand PET for early castration-resistant prostate cancer: a retrospective single-center study. J Nucl Med. 2020;62(1):
12. Glicksman R, Metser U, Vines D, et al. Primary analysis of a Phase II study of metastasis-directed ablative therapy to PSMA (18 F-DCFPyL) PET-MR/CT defined oligorecurrent prostate cancer. J clin oncol. 2020;38(15):5553. doi:10.1200/JCO.2020.38.15_suppl.5553
13. Glicksman R, Metser U, Vines D, et al. Preliminary results of a two stage phase II study of 18F-DCFPyL PET-MR for enabling oligometastases ablative therapy in subclinical prostate cancer. Int J Radiation Oncol Biol Physics. 2019;105(1):276. doi:10.1016/j.ijrobp.2019.06.1901
14. Sb A, Raw B, Spr C, et al. PET imaging for prostate cancer. Radiologic Clin North Ame. 2021;59(5):801–811. doi:10.1016/j.rcl.2021.05.008
15. Wen X, Jiang CY, Jiang X, Chen Y, Li M. Comparative diagnostic performance of 68Ga-PSMA-11 PET/CT and 68Ga-PSMA-11 PET/MRI in detecting biochemical recurrent bone metastasis in prostate cancer: a systematic review and meta-analysis. Acta Radiol. 2025;66(3):312–327. doi:10.1177/02841851241307336
16. Glicksman R, Metser U, Vines D, et al. Preliminary results of a two stage phase II study of 18F-DCFPyL PET-MR for enabling oligometastases ablative therapy in subclinical prostate cancer. J Clin Oncol. 2019;37(7):250. doi:10.1200/JCO.2019.37.7_suppl.250
17. Wilk B, Wisenberg G, Dharmakumar R, Thiessen JD, Goldhawk DE, Prato FS. Hybrid PET/MR imaging in myocardial inflammation post-myocardial infarction. J Nucl Cardiol. 2020;27(6):2083–2099. doi:10.1007/s12350-019-01973-9
18. Bh A, Kh B. Re: prostate-specific membrane antigen PET-CT in patients with high-risk prostate cancer before curative-intent surgery or radiotherapy (proPSMA): a prospective, randomised, multi-centre study. Europ urol. 2020;78(3):470–471. doi:10.1016/j.eururo.2020.04.051
19. Zacho HD, Nielsen JB, Afshar-Oromieh A, et al. Prospective comparison of 68Ga-PSMA PET/CT,18F-sodium fluoride PET/CT and diffusion weighted-MRI at for the detection of bone metastases in biochemically recurrent prostate cancer. Eur J Nucl Med Mol Imaging. 2018;45(11):1884–1897. doi:10.1007/s00259-018-4058-4
20. Liu F, Dong J, Shen Y, et al. Comparison of PET/CT and MRI in the diagnosis of bone metastasis in prostate cancer patients: a network analysis of diagnostic studies. Front Oncol. 2021;11:736654. doi:10.3389/fonc.2021.736654
21. Sutherland DEK, Azad AA, Murphy DG, Eapen RS, Kostos L, Hofman MS. Role of FDG PET/CT in management of patients with prostate cancer. Semin Nucl Med. 2024;54(1):4–13. doi:10.1053/j.semnuclmed.2023.06.005
22. Iacovitti CM, Cuzzocrea M, Rizzo A, et al. Diagnostic value of dual-tracer PET/CT with [18F]FDG and PSMA ligands in prostate cancer: an updated systematic review. Front Med Lausanne. 2025;12:1607227. doi:10.3389/fmed.2025.1607227
23. Fendler WP, Eiber M, Beheshti M, et al. 68Ga-PSMA PET/CT: joint EANM and SNMMI procedure guideline for prostate cancer imaging: version 1.0. Eur J Nucl Med Mol Imaging. 2017;44(6):1014–1024. doi:10.1007/s00259-017-3670-z
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Exosome-Derived miRNAs as Potential Biomarkers for Prostate Bone Metastasis
Lu Z, Hou J, Li X, Zhou J, Luo B, Liang S, Lo RK, Wong TM, Kuang GM
International Journal of General Medicine 2022, 15:5369-5383
Published Date: 1 June 2022
Prostate Cancer Bone Metastasis: Molecular Mechanisms of Tumor and Bone Microenvironment
Jiang H
Cancer Management and Research 2025, 17:219-237
Published Date: 1 February 2025
Geriatric Nutritional Risk Index (GNRI) and Prognostic Nutritional Index (PNI) Before Treatment as the Predictive Indicators for Bone Metastasis in Prostate Cancer Patients
Chen L, Rao H, Chen N, Li R, Chen D, Jiang H
International Journal of General Medicine 2025, 18:2703-2713
Published Date: 24 May 2025