")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 19
Perspectives on Ensifentrine and Its Therapeutic Potential in the Treatment of COPD: Evidence to Date
Authors Faruqi MA, Khan MMKS, Mannino DM
Received 31 October 2023
Accepted for publication 21 December 2023
Published 3 January 2024 Volume 2024:19 Pages 11—16
DOI https://doi.org/10.2147/COPD.S385811
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Russell
Muhammad Asad Faruqi,1 Malik M Khurram S Khan,1 David M Mannino1,2
1University of Kentucky College of Medicine, Lexington, KY, USA; 2COPD Foundation, Miami, FL, USA
Correspondence: David M Mannino, Department of Medicine, University of Kentucky College of Medicine, 800 Rose Street, Lexington, KY, 40536, USA, Email [email protected]
Abstract: Ensifentrine is a novel inhalational phosphodiesterase (PDE)3 and PDE4 inhibitor which improves bronchodilation and decreases inflammatory markers by acting locally on the bronchial tissue, with minimal systemic effects. Both preclinical and clinical trials have demonstrated benefits of this therapy, including improvement in lung function and reduction in exacerbations. This therapy is currently under review by the US Food and Drug Administration with a decision expected in 2024.
Keywords: chronic obstructive pulmonary disease, therapy, phosphodiesterase inhibitor
Introduction
Chronic obstructive pulmonary disease (COPD) is a progressive inflammatory disorder of the respiratory system which is characterized by irreversible airflow obstruction, remodeling of the airways and acute exacerbations leading to lung function decline, progressive dyspnea, and cough.1 Treatment of COPD is aimed towards reducing symptoms like shortness of breath and mucous production, preventing flare-ups, slowing disease progression and improving survival. COPD therapies involve both non-pharmacological and pharmacological interventions. Some patients on maximal therapies, including inhaled bronchodilators and steroids and oral phosphodiesterase 4 (PDE4) inhibitors, can still be symptomatic. Thus, new therapies are needed that can improve lung function and airway inflammation when used in addition to existing therapies.2,3 In addition, current inhaled therapies may not be tolerated by all patients. Thus, therapies with alternative mechanisms of action are needed. In this article, we review the literature available on ensifentrine, a novel phosphodiesterase inhibitor that has the potential to be an add-on therapy for patients with COPD.
Mechanism of Action
Ensifentrine (RPL554) is a novel drug that works by dual inhibition of phosphodiesterase (PDE) 3 and 4 enzymes (PDE3, PDE4) and is designed to be delivered via inhalation.4 Inhibitors of PDE3 and PDE4 target multiple respiratory functions at the cellular and tissue level (Figure 1). PDE3 regulates cyclic adenosine monophosphate (cAMP) and cyclic guanosine monophosphate (cGMP) levels in the airway smooth muscles, which mediates bronchial tone.5 PDE4 regulates cAMP levels in the airway cells associated with inflammation and is involved in activation of these cells.6 PDE4 inhibitors can also activate the Cystic Fibrosis Transmembrane Conductance Regulator (CFTR) and improve bronchial epithelial cell ciliary movements.7 Evidence has recently emerged that dual inhibition of PDE3 and PDE4 enzymes results in a synergistic effect of decreased inflammation and improved bronchodilation as both iso-forms of PDE are expressed in the inflammatory cells and airway smooth muscles.8,9 This article explores the evidence to date regarding ensifentrine as a novel therapeutic option for the treatment of COPD.
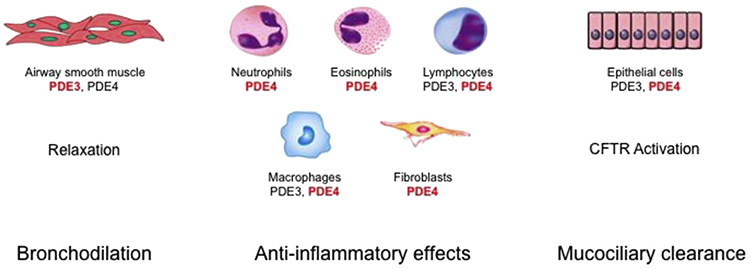 |
Figure 1 Combined inhibition of phosphodiesterase (PDE) 3 and PDE4 has additive and synergistic anti-inflammatory and bronchodilatory effects versus inhibition of either PDE3 or PDE4 alone. Furthermore, it increases mucociliary clearance. In red, the main PDE involved in the activity of the specific cell. With permission, from Current Opinion in Pharmacology. Notes: Reprinted from Current Opinion in Pharmacology, Volume 56, Matera MG, Cazzola M, Page C, Prospects for COPD treatment. pages 74–84, copyright 2021, with permission from Elsevier.3 |
Preclinical Findings
Several in vitro and in vivo studies evaluated the effect of PDE3/4 inhibitors on airway smooth muscles and degree of inflammation.
One study investigated the effects of ensifentrine (RPL554) on the tone of isolated human airway smooth muscles and its synergistic actions when used in conjunction with other bronchodilators including muscarinic antagonists and beta-adrenergic agonists. The study demonstrated that ensifentrine caused relaxation of the bronchial smooth muscles and had a synergistic effect when used with muscarinic antagonists.10
Ensifentrine’s effect on bronchial epithelial cell cultures obtained from normal and Cystic Fibrosis (CF) patients with F508del genotype has also been evaluated.11 It stimulates CFTR-dependent chloride ion secretion across bronchial epithelial cells and increases cilia beat frequency in primary human bronchial epithelial cells. It also decreases the production of monocyte chemoattractant protein-1 and granulocyte monocyte colony-stimulating factor (GM-CSF) in interleukin 1-b stimulated CF bronchial epithelial cells. This anti-inflammatory effect was primarily due to inhibition of the PDE4 enzyme.12 These findings encouraged further investigation into the role of this drug in treatment of patients with COPD where mucociliary clearance was abnormal with increased mucous production and cough.13
Ensifentrine produces sustained relaxant effects on contractions in isolated airway tissue preparations induced by compounds like histamine and carbachol and by electrical field stimulation (EFS).4 Another study investigated the isolated and combined effect of ensifentrine and glycopyrronium on medium and small human isolated bronchi. It demonstrated that small doses of these compounds induced maximal relaxation of bronchi for about 4 hours. When used in conjunction with bronchodilators, the relaxant effect lasted for about 6 hours, suggesting this could be an add-on therapy in patients with asthma or COPD.14
Inhaled ensifentrine showed bronchoprotective properties against airway constriction induced by spasmogens and antigens in guinea pigs. It caused a dose-dependent relaxation of the airways (7–65% reduction in obstruction) and had a synergistic effect when used with atropine (42–82% reduction in obstruction) and salbutamol (64–78% reduction in obstruction) in vivo.15
Another pre-clinical study demonstrated anti-inflammatory effects of ensifentrine in the respiratory system of guinea pigs. It produced inhibition of the recruitment of all cell numbers in the bronchoalveolar lavage (BAL) fluid 6 hours after antigen challenge. It also showed a dose-dependent inhibition of ovalbumin-induced eosinophil and total cell recruitment into the nasal passages, thereby reducing inflammation.16
Clinical Findings
Promising data from pre-clinical trials led to four separate small clinical studies done between 2009 and 2013 in Europe. Ensifentrine was found to be an effective bronchodilator and an anti-inflammatory drug when used alone or in conjunction with existing standard of care therapies, without significant side effects. Of note, these small studies included healthy volunteers, asthmatics and patients with COPD.17 One of the trials showed that inhaled ensifentrine solution, administered for 6 days, caused a decrease in inflammatory cells of sputum samples collected 6 hours after the lipopolysaccharide (LPS) challenge (neutrophils by 40%, macrophages by 27%, eosinophils by 44% and lymphocytes by 67%). Bronchodilator effects, overall safety and adverse events were similar across all studied populations.17
A phase IIb randomized, double-blind, placebo controlled, dose-ranging, parallel group trial was conducted in patients with COPD who were randomized to receive nebulized ensifentrine at increasing doses or placebo. At week 4, results showed increased bronchodilation (improvement in forced expiratory volume in one second (FEV1)) and improvement in patient symptoms for the ensifentrine group compared to placebo. It also showed a dose-dependent response from 0.75mg to 3mg of nebulized drug.18 Although this study had promising results, the major limitation was the short duration of treatment (4 weeks) which was not long enough to fully evaluate anti-inflammatory effects or distinguish between bronchodilator and anti-inflammatory effects.
Pharmacokinetic properties of ensifentrine when used in conjunction with other bronchodilators have been evaluated in short-term trials. One trial was a single dose, double-blind, placebo-controlled six-way crossover study on 33 COPD patients where they received single doses of nebulized Ensifentrine (6mg) or placebo, inhaled salbutamol (200 mg) or placebo and inhaled ipratropium (40 mg) or placebo. Ensifentrine (6mg) alone led to a statistically significant increase in FEV1 initially and up to 8 hours after administration. When used in conjunction with salbutamol or ipratropium, the magnitude of FEV1 increase was greater. Statistically significant reduction in residual lung volume and airway resistance was also noted when ensifentrine was used as monotherapy or along with salbutamol or ipratropium.19
A 3-day randomized, double-blind, placebo controlled, 3 way cross-over trial in 29 human subjects with COPD having moderate to severe obstruction was conducted where they were randomized to receive nebulized ensifentrine (1.5mg and 6mg) or placebo twice a day with a baseline treatment with tiotropium once daily. Ensifentrine plus tiotropium increased peak FEV1 measured by day 3, relative to placebo plus tiotropium. Ensifentrine plus tiotropium similarly reduced residual volume and airway resistance compared to placebo plus tiotropium.19 Key limitations of this study include short duration, narrow population studied and lack of determination of long-term anti-inflammatory effects of ensifentrine in COPD patients.
Most recently, Phase III randomized, double-blind, placebo-controlled multicenter trials (the Ensifentrine as a Novel Inhaled Nebulized COPD Therapy [ENHANCE] trials) were done to evaluate the efficacy of ensifentrine on patients with COPD (Table 1). Lung function, symptoms, quality of life and exacerbations were evaluated. ENHANCE-1 trial had 760 patients, and ENHANCE-2 had 789 patients enrolled with moderate to severe symptomatic COPD. Patients were randomized to receive nebulized ensifentrine or placebo. More than half of patients in both trials were receiving long-acting muscarinic antagonist or long-acting beta-2 agonist bronchodilator therapy. Results of these trials showed statistically significant improvement (P < 0.001) from baseline in week 12 average FEV1 after treatment with ensifentrine, compared to placebo. The ensifentrine group also had statistically significantly improved symptoms and quality of life vs placebo group at week 24 in both ENHANCE-1 and ENHANCE-2 studies. Mean scores in the ensifentrine group exceeded the minimally important clinical difference (MCID) for E-RS and SGRQ scores in both ENHANCE trials. The improvement in FEV1, however, did not exceed the commonly accepted MCID of 100 mL, which might question the efficacy of this therapy as a bronchodilator. Both studies showed reduced rate of COPD exacerbations and increased time to first exacerbation in the ensifentrine group. These trials demonstrated that ensifentrine ought to be considered for the treatment of diverse COPD populations as it reduces exacerbations, when used either alone or in combination with standard maintenance therapy.20
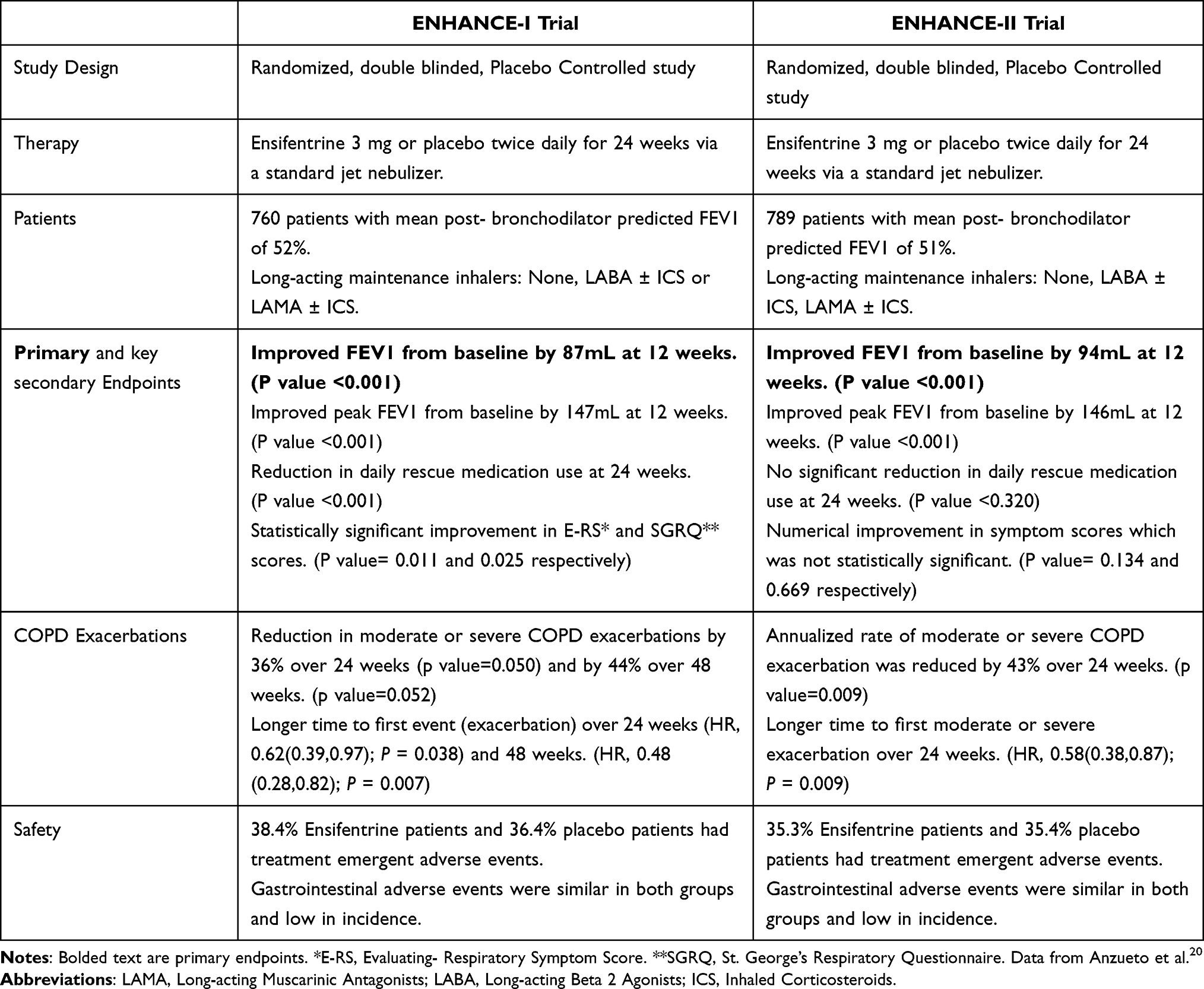 |
Table 1 Summary of Ensifentrine as a Novel Inhaled Nebulized COPD Therapy (ENHANCE) I and ENHANCE II Phase 3 Trials |
Safety Profile
The safety profile of ensifentrine in healthy individuals and patients with COPD has been evaluated in Phase II and phase III trials that have been conducted to date. A 2013 study of ensifentrine in healthy volunteers and asthma or COPD patients showed that nebulized drug (1.5mg) was well tolerated with a side effect profile similar to placebo.17
One Phase 1 study evaluated the effects of nebulized ensifentrine on cardiac conduction with doses of 3mg and 9mg in healthy volunteers. It showed that ensifentrine did not prolong QT interval or had any significant effect on PR and QRS intervals.21
Clinical safety of this drug over a wide range of doses in patients with COPD has not shown any serious adverse events related to different organ symptoms. In the dose ranging study of inhaled ensifentrine, doses up to 6mg twice a day for 4 weeks did not show any serious cardiovascular or gastrointestinal side effects.18 Side effects of diarrhea, nausea and vomiting as seen with some oral PDE4 inhibitors have not been commonly observed with nebulized therapy.
In the phase II trials of nebulized ensifentrine, which were done over 4 weeks, reported side effects in the treatment group were headaches in 5% (vs 2.5% in placebo), COPD symptoms in 3.6% (vs 3.7% in placebo), cough in 4.2% (vs 1.2% in placebo) and dyspnea in 1.8% (vs 3.1% in placebo). Overall, side effect profile in both groups was similar and no serious adverse events were reported.22
In the ENHANCE trials, safety profile of ensifentrine was similar to placebo (Table 1) and reported diarrhea did not have a temporal association with therapy. Overall incidence of pneumonia was also low and similar between both groups.20 As more data get published, it will be imperative to evaluate for any long-term side effects or potential complications of ensifentrine. Post-hoc analysis of current clinical trials will add more to the safety data and efficacy of the drug.
Discussion
Different therapies for COPD have been utilized to treat and manage symptoms including maintenance inhaled bronchodilators and inhaled corticosteroids.23
Ensifentrine is a novel inhalational PDE3/4 inhibitor which improves bronchodilation and decreases inflammatory markers by acting locally on the bronchial tissue, with minimal systemic effects.9 Ensifentrine’s inhibition of PDE isoenzymes translates into modulation of cAMP and cGMP levels in the bronchial tissues and decreased recruitment of inflammatory cells.6 Multiple in-vitro and in-vivo studies have demonstrated dose-dependent bronchodilator, bronchoprotective and anti-inflammatory effects of ensifentrine.15,16
Multiple clinical studies have demonstrated similar effects of this drug when tested on healthy individuals and patients with asthma or COPD. In 4-week, phase II clinical trials, nebulized drug given twice a day alone or in combination with other bronchodilators, showed sustained bronchodilation and improvement in FEV1, improvement in symptoms judged by questionnaires, improvement in residual volumes and COPD symptoms.19,24
Finally, the ENHANCE trials are phase III randomized, double-blinded prospective trials evaluating the effects of ensifentrine on patients with moderate to severe COPD. Treatment with ensifentrine demonstrated statistically significant improvement in FEV1 (although just short of the MCID threshold of 100 mL), improved symptoms of COPD, reduction in exacerbations, while not causing any serious adverse events. Importantly, inhaled PDE3/4 inhibitor administration did not cause major side effects of an oral PDE4 inhibitor (roflumilast) like nausea, vomiting and diarrhea.20
Conclusion
Currently, there are no inhaled phosphodiesterase inhibitors approved for maintenance therapy of chronic obstructive pulmonary disease (COPD). Ensifentrine has undergone phase III clinical trials (the ENHANCE trials) which have shown promising results in terms of improvement in lung function, improved symptom control and potential reduction in exacerbations and no increased side effects, when used alone or in combination with standard of care. Ensifentrine, in inhalational nebulized formulation, shows promise as a novel maintenance treatment for patients who are on maximal therapy with treatments like inhaled bronchodilators, inhaled corticosteroids, oral antibiotics or oral PDE4 inhibitors. This therapy is currently under review by the US Food and Drug Administration with a decision expected in 2024.25
Ensifentrine’s strong clinical profile, combined with very few side effects and overall good tolerance, makes it a promising addition to the current treatment regimens available for COPD management. In addition, it may be therapy that reduces exposure to bronchodilators or inhaled steroids in selected patients.
Disclosure
Drs. Faruqi and Khan report no conflicts of interest. Dr. Mannino is a consultant to GlaxoSmithKline, AstraZeneca, Regeneron, Genentech and The COPD Foundation, receives royalties from Up to Date, and is an expert witness on behalf of people suing the tobacco and vaping industries.
References
1. Agusti A, Celli BR, Criner GJ, et al. Global Initiative for Chronic Obstructive Lung Disease 2023 Report: GOLD Executive Summary. Eur Respir J. 2023;61(4):2300239. doi:10.1183/13993003.00239-2023
2. Cazzola M, Rogliani P, Matera MG. The future of bronchodilation: looking for new classes of bronchodilators. Eur Respir Rev. 2019;28(154):190095. doi:10.1183/16000617.0095-2019
3. Matera MG, Cazzola M, Page C. Prospects for COPD treatment. Curr Opin Pharmacol. 2021;56:74–84. doi:10.1016/j.coph.2020.11.003
4. Boswell-Smith V, Spina D, Oxford AW, Comer MB, Seeds EA, Page CP. The pharmacology of two novel long-acting phosphodiesterase 3/4 inhibitors, RPL554 [9,10-dimethoxy-2(2,4,6-trimethylphenylimino)-3-(n-carbamoyl-2-aminoethyl)-3,4,6,7-tetrahydro-2H-pyrimido[6,1-a]isoquinolin-4-one] and RPL565 [6,7-dihydro-2-(2,6-diisopropylphenoxy)-9,10-dimethoxy-4H-pyrimido[6,1-a]isoquinolin-4-one]. J Pharmacol Exp Ther. 2006;318(2):840–848. doi:10.1124/jpet.105.099192
5. Abbott-Banner KH, Page CP. Dual PDE3/4 and PDE4 inhibitors: novel treatments for COPD and other inflammatory airway diseases. Basic Clin Pharmacol Toxicol. 2014;114(5):365–376. doi:10.1111/bcpt.12209
6. Calverley PM, Rabe KF, Goehring UM, et al. Roflumilast in symptomatic chronic obstructive pulmonary disease: two randomised clinical trials. Lancet. 2009;374(9691):685–694. doi:10.1016/S0140-6736(09)61255-1
7. Dransfield M, Rowe S, Vogelmeier CF, et al. Cystic Fibrosis Transmembrane Conductance Regulator: roles in Chronic Obstructive Pulmonary Disease. Am J Respir Crit Care Med. 2022;205(6):631–640. doi:10.1164/rccm.202109-2064TR
8. Banner KH, Press NJ. Dual PDE3/4 inhibitors as therapeutic agents for chronic obstructive pulmonary disease. Br J Pharmacol. 2009;157(6):892–906. doi:10.1111/j.1476-5381.2009.00170.x
9. Zuo H, Cattani-Cavalieri I, Musheshe N, Nikolaev VO, Schmidt M. Phosphodiesterases as therapeutic targets for respiratory diseases. Pharmacol Ther. 2019;197:225–242. doi:10.1016/j.pharmthera.2019.02.002
10. Calzetta L, Page CP, Spina D, et al. Effect of the mixed phosphodiesterase 3/4 inhibitor RPL554 on human isolated bronchial smooth muscle tone. J Pharmacol Exp Ther. 2013;346(3):414–423. doi:10.1124/jpet.113.204644
11. Turner MJ, Matthes E, Billet A, et al. The dual phosphodiesterase 3 and 4 inhibitor RPL554 stimulates CFTR and ciliary beating in primary cultures of bronchial epithelia. Am J Physiol Lung Cell Mol Physiol. 2016;310(1):L59–70. doi:10.1152/ajplung.00324.2015
12. Turner MJ, Dauletbaev N, Lands LC, Hanrahan JW. The Phosphodiesterase Inhibitor Ensifentrine Reduces Production of Proinflammatory Mediators in Well Differentiated Bronchial Epithelial Cells by Inhibiting PDE4. J Pharmacol Exp Ther. 2020;375(3):414–429. doi:10.1124/jpet.120.000080
13. Turner MJ, Abbott-Banner K, Thomas DY, Hanrahan JW. Cyclic nucleotide phosphodiesterase inhibitors as therapeutic interventions for cystic fibrosis. Pharmacol Ther. 2021;224:107826. doi:10.1016/j.pharmthera.2021.107826
14. Calzetta L, Cazzola M, Page CP, Rogliani P, Facciolo F, Matera MG. Pharmacological characterization of the interaction between the dual phosphodiesterase (PDE) 3/4 inhibitor RPL554 and glycopyrronium on human isolated bronchi and small airways. Pulm Pharmacol Ther. 2015;32:15–23. doi:10.1016/j.pupt.2015.03.007
15. Keir S, Page C. RPL554, a dual phosphodiesterase (PDE) 3/4 inhibitor acts synergistically with muscarinic receptor antagonists and beta-adrenoceptor agonists to produce bronchodilation in vivo. C32 ASTHMA: PRE-CLINICAL STUDIES. Am Thorac Soc. 2014;A4218–A4218.
16. Rheault T, MacDonald-Berko M. Antiinflammatory pharmacology of ensifentrine. Chest. 2020;158(4):A2284. doi:10.1016/j.chest.2020.08.1936
17. Franciosi LG, Diamant Z, Banner KH, et al. Efficacy and safety of RPL554, a dual PDE3 and PDE4 inhibitor, in healthy volunteers and in patients with asthma or chronic obstructive pulmonary disease: findings from four clinical trials. Lancet Respir Med. 2013;1(9):714–727. doi:10.1016/S2213-2600(13)70187-5
18. Singh D, Martinez FJ, Watz H, Bengtsson T, Maurer BT. A dose-ranging study of the inhaled dual phosphodiesterase 3 and 4 inhibitor ensifentrine in COPD. Respir Res. 2020;21(1):47. doi:10.1186/s12931-020-1307-4
19. Singh D, Abbott-Banner K, Bengtsson T, Newman K. The short-term bronchodilator effects of the dual phosphodiesterase 3 and 4 inhibitor RPL554 in COPD. Eur Respir J. 2018;52(5):1801074. doi:10.1183/13993003.01074-2018
20. Anzueto A, Barjaktarevic IZ, Siler TM, et al. Ensifentrine, a Novel Phosphodiesterase 3 and 4 Inhibitor for the Treatment of Chronic Obstructive Pulmonary Disease: randomized, Double-Blind, Placebo-controlled, Multicenter Phase III Trials (the ENHANCE Trials). Am J Respir Crit Care Med. 2023;208(4):406–416. doi:10.1164/rccm.202306-0944OC
21. Rickard K, Darpo B, Xue H, Bengtsson T, Rheault T. The Dual Phosphodiesterase (PDE) 3 and 4 Inhibitor Ensifentrine Does Not Prolong QT Interval in Healthy Volunteers. B39 COPD MANAGEMENT: FROM PHARMACOLOGIC TREATMENT TO NOVEL THERAPIES. Am Thorac Soc. 2022;A5605–A5605.
22. Rickard K, Bengtsson T, Rheault T. Cardiovascular Safety Profile of Ensifentrine in Patients with COPD: results from Two Four-Week, Dose-Ranging, Randomized, Placebo-Controlled Trials. TP40 TP040 COPD CLINICAL TRIALS AND THERAPIES. Am Thorac Soc. 2021;A2256–A2256.
23. Terry PD, Dhand R. Inhalation Therapy for Stable COPD: 20 Years of GOLD Reports. Adv Ther. 2020;37(5):1812–1828. doi:10.1007/s12325-020-01289-y
24. Martin C, Burgel PR, Roche N. Inhaled Dual Phosphodiesterase 3/4 Inhibitors for the Treatment of Patients with COPD: a Short Review. Int J Chron Obstruct Pulmon Dis. 2021;16:2363–2373. doi:10.2147/COPD.S226688
25. Drugs.com. Ensifentrine FDA Approval Status. Available from: https://www.drugs.com/history/ensifentrine.html.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.