Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 12
Personalized intervention to improve stress and sleep patterns for glycemic control and weight management in obese Emirati patients with type 2 diabetes: a randomized controlled clinical trial
Authors Mussa BM ![]() , Schauman M, Kumar V, Skaria S, Abusnana S
, Schauman M, Kumar V, Skaria S, Abusnana S ![]()
Received 10 January 2019
Accepted for publication 24 April 2019
Published 28 June 2019 Volume 2019:12 Pages 991—999
DOI https://doi.org/10.2147/DMSO.S201142
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Konstantinos Tziomalos
Bashair M Mussa,1 Mia Schauman,2 Vijay Kumar,3 Sijomol Skaria,3 Salah Abusnana4,5
1Basic Medical Science Department, College of Medicine, University of Sharjah, Sharjah, United Arab Emirates; 2Medical Research Department, Celolab, Dubai, United Arab Emirates; 3Rashid Centre for Diabetes and Research, Ajman, United Arab Emirates; 4Clinical Science Department, College of Medicine, University of Sharjah, Sharjah, United Arab Emirates; 5Diabetes and Endocrinology Department, University Hospital Sharjah, Sharjah, United Arab Emirates
Background: There is growing evidence that stress and sleep deprivation are involved in development of type 2 diabetes (T2DM). The latter is one of the most challenging health problems in the UAE. Therefore, the present study aimed to investigate the effects of personalized intervention on glycemic and weight control in Emirati patients with T2DM. The intervention involved assessment and modification of stress levels and sleep patterns.
Methods: This was a randomized controlled study conducted on 51 Emirati patients with T2DM (age 18–60 years, body-mass index (BMI) ≥25 kg/m2): those in the intervention group who completed the trial numbered 18 and those in the control group who completed the trial numbered 17. Heart-rate variability was used for real-life and long-term assessments of stress, sleep, and recovery. Body weight, BMI, HbA1c and lipid profile were included in the investigation. The National Clinical Trial identifier number is NCT03644134.
Results: Percentage change in body weight was significantly greater (P<0.05) in the intervention group (–3.2±2.9) than the control group (–0.02). Percentage change in the BMI of the intervention group was –4.50±5.9, while the control group exhibited less change in BMI (–0.0003±3.3, P<0.05). In addition, a significant reduction in HbA1c was observed in the intervention group (–5.3±15.7) and an increase of 9.9±13.1 was observed in the control group (P<0.01).
Conclusion: The findings of the present study show that personalized approaches that reduce stress levels, increase recovery levels, and promote healthy sleep habits play an important role in weight management and glycemic control in T2DM.
Keywords: diabetes mellitus, obesity, stress, recovery levels, sleep pattern, heart rate variability
Introduction
Globally, diabetes mellitus (DM) and obesity are considered the fastest-growing disorders, and their prevalence has increased dramatically over the last 20 years. These two disorders can lead to a wide range of serious complications, including heart diseases, stroke, renal failure, and autonomic neuropathy.1–4 The Middle East and North Africa region has the third-highest prevalence (9.1%) of DM, and about 14.4 million people within this region have undiagnosed DM.4 Several countries within the region, including the Gulf states, have experienced significant social and economic transformations that have led to an increase in DM, as well as obesity.5,6 Recent studies have shown that about 19% of the United Arab Emirates (UAE) population have been diagnosed with DM and 68% of UAE citizens are obese.4,7
A substantial portion of the literature has shown that prevention and treatment of DM and obesity are influenced mainly by lifestyle modifications and it has been well documented that good glycemic control involves comprehensive lifestyle approaches, including diet and nutrition advice and adequate levels of physical activity.8,9 However, William et al demonstrated that factors other than diet and exercise should be considered as key elements in the development of diabetes.10 Psychosocial adversity seems to play a role in DM and obesity, despite the fact that the direct relationship between these disorders and stressful life events is yet to proven.10 In addition, studies in animals and in patients with DM have demonstrated that stress can induce hyperglycemia.11,12 Furthermore, it has been shown that stress management can significantly improve long-term glycemic control in type 1 and type 2 DM (T2DM).13–16 In agreement with these findings, Björntorp theory has suggested that the hypothalamo–pituitary–adrenal axis is activated in response to stress. This in turn leads to endocrine abnormalities and hormonal imbalance, which contribute significantly in development of insulin resistance.17 Moreover, UAE studies in Sharjah and Al Ain populations have demonstrated a strong relationship between depressive and anxiety disorders and DM complications.18,19
Studies have shown for decades the numerous benefits of intensive lifestyle interventions for T2DM patients, including improvement in glycemic control, weight loss, quality of life, and more importantly reduction in cardiovascular mobility and mortality.20 In contrast, more recent studies have questioned the outcomes of these previous reports, highlighting the fact that the effects of intensive lifestyle interventions may vary among T2DM patients.21 It has been found that these interventions do not reduce the cardiovascular risk in obese patients with T2DM compared to control patients who receive social and educational support.21 Although lifestyle modification is an efficient way to improve the general well-being of patients with T2DM, other factors, including genetic composition and environmental inputs, seem to influence the outcomes of these modifications, emphasizing the importance of personalized lifestyle approaches.22 Recently, the latter have received much attention, due to the fact that they provide innovative solutions based on individual perception and health metrics. In addition, specific patient-oriented care and personalized action plans can be designed to implement long-term goals that prevent complications associated with chronic disorders, including T2DM.23
There is a paradox in the field of stress and DM research, and this could be due to many reasons, including different study populations, use of different types of DM as investigating model, and various stress-measurement methods and techniques.24 The latter mainly include questionnaires such as the ATT39, Questionnaire on Stress in Patients with Diabetes — Revised, Problem Areas in Diabetes, and the Diabetes Distress Scale, and measurement of stress response.25–27 Stress questionnaires have several clinical limitations, including, subjective measures, personality may affect results significantly, different types of populations may need different types of questionnaires, and the lack of a direct link to individual stress response. Therefore, recent investigations have focused on and emphasized the importance of individualized measurement of stress response. This response triggers a set of physiological reactions, and several systems and hormones are involved; however, the association between the autonomic nervous system (ANS) and cardiovascular system is considered the body’s first-line defense against stress.28,29 Several studies have confirmed the direct relationship between the ANS and heart-rate variability (HRV) and shown that activation of the former in response to stress leads to decreased HRV.30 Therefore, analysis and assessment of HRV is currently receiving much attention and considered as a powerful technique to measure stress.22 A review by Chandola et al showed the majority of studies investigating the relationship between HRV and stress strongly suggested that a greater amount of reported stress is associated with lower HRV.31
Taking into account these findings, along with the fact that T2DM and obesity are one of the most pressing health challenges in the UAE, the present study was designed to investigate the effects of stress management and improvement in sleep habits on glycemic control and weight loss in obese T2DM Emirati patients.
Methods
The present study was a randomized controlled trial conducted at Rashid Centre for Diabetes and Research (RCDR) in Ajman, which is one of the seven emirates of the UAE. The study was approved by the research ethics committee of Al Qassimi Clinical Research Centre, Al Qassimi Hospital (Ministry of Health, UAE) and conducted in accordance with the Declaration of Helsinki. The study is registered with the ClinicalTrials.gov (NCT03644134).
Study participants
The study population were Emirati individuals (n=51) attending RCDR diabetes clinics on a quarterly basis (an initial visit and three follow-up visits per annum). Participants were recruited from RCDR diabetes clinics and through different methods, including direct contact, distribution of informative flyers, and phone calls using Diamond, an electronic medical database of RCDR patients. The screening process involved 110 Emirati patients with T2DM, and 51 individuals were eligible to participate in the present trial based on the inclusion and exclusion criteria. Inclusion criteria were age 18–60 years, body-mass index (BMI) >25 kg/m2, and T2DM. Exclusion criteria were age <18 and >60 years, BMI <25 kg/m2, T1DM, diagnosis of atrial fibrillation and/or atrial flutter and/or bundle-branch block, and heart transplantation.
As shown in Figure 1, screening failure, premature withdrawal from the trial, and participation in different trials within the same site were the main reasons for the significant reduction in the number of participants. Eligible participants were randomly allocated into an intervention group (n=26) and a control group (n=25). Noncompliance was the main obstacle to maintaining the same number of randomized participants in each group, and 19% and 24% of participants in the intervention and control groups, respectively, did not attend the first visit.
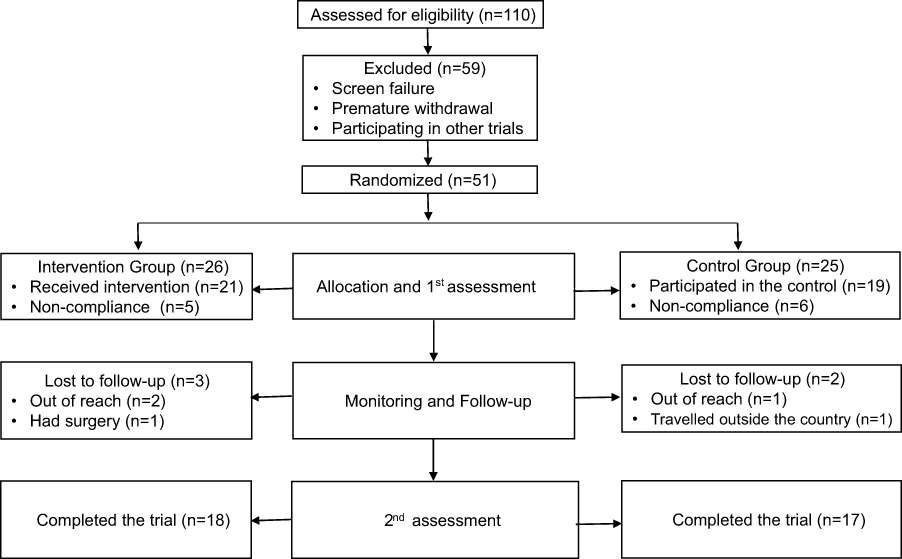 |
Figure 1 Schematic flow chart showing the selection process based on the inclusion and exclusion criteria. |
Study design
The present randomized controlled clinical trial included Emirati patients with T2DM who attended RCDR on a regular basis. Those who were interested in participating in the study were asked to sign an informed-consent form written in their native language. This form had been approved by the ethics committee prior to recruitment. All participants attended an initial information session for 45 minutes. This session was divided into four parts: background information about the study, intervention and control protocols, a demonstration of the HRV measurements, and a chance to ask questions and share points of view regarding the flowchart and timeline of the study.
Study visits
After randomization and allocation of participants into control and intervention groups, the schedule of the visits was revealed and elucidated to the participants. As shown in Figure 2, the study included seven visits: visit 1 (site visit in week 1), visit 2 (site visit in week 2), visit 3 (telephone call in week 4), visit 4 (telephone call in week 14), visit 5 (telephone call in week 21), visit 6 (site visit in week 24), and visit 7 (site visit in week 25). Site visits 1 and 2 included an assessment of medical history, collection of demographic data, and anthropometric measurements (using patient scales from SECA [Hamburg, Germany]). In addition, blood samples were collected for measurement of HBA1c and assessment of lipid profile.
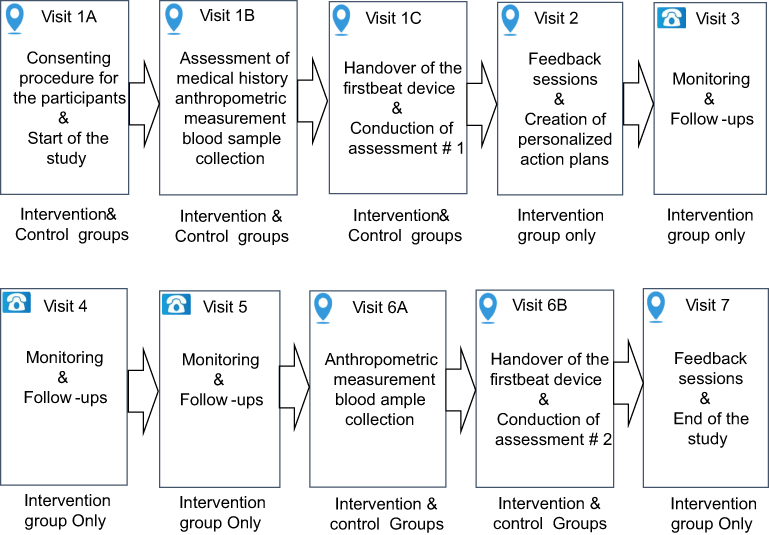 |
Figure 2 Schematic flow chart showing the site visits and telephone calls of the study. |
Monitoring of study variables
HRV was used as the main method to monitor the variables of this study, including stress levels, recovery levels, and sleep patterns. Real-life and continuous measurements were conducted using a Firstbeat Bodyguard Monitor (FB120140; Mega Electronics, Jyväskylä, Finland). The monitor allows 3 days of continuous data recording and provides a reliable overview of changes in study variables. The device is attached to the skin with two electrodes to minimize skin contact. After the recording is done, the data are downloaded and transferred to special software via a USB port.
Intervention and control protocols
The personalized intervention consisted of an information session, pre-assessment (first assessment) of stress and recovery (relaxation) levels and sleep patterns using measurement of HRV, individual feedback sessions and action plans based on the outcomes of the initial assessment, monitoring and follow-up, and post-assessment (second assessment) of stress and recovery levels and sleep patterns using measurement of HRV. The control protocol included only an information session, pre-assessment (initial assessment), and post-assessment (second assessment) of stress and recovery levels and sleep patterns using measurement of HRV.
Measurement diary
All participants were requested to fill in a measurement diary, which included questionnaires about their daily activities. Start and end time of activities were recorded: physical activity (eg, exercise), meals (eg, breakfast, lunch, snacks), mentally stressful tasks (eg, meetings, other work commitments), relaxing events (eg, reading, listening to music), and sleep details (eg, naps and night’s sleep).
Action-plan elements
Personalized action plans were created based on the outcomes of the initial assessment. The general categories of the action plans included engaging in physical activities, healthy eating and drinking, avoiding stressful experiences, enhancing leisure time, and improving the quality of sleep. More specific elements were integrated in each category, such as taking regular breaks and not dealing with work during the breaks, setting a realistic work schedule and reasonable number of goals, enhancing leisure time and activities, avoiding high-intensity exercise and heavy meals late at night, and engaging in relaxing activities prior to sleep.
Statistical analysis
All results of the present study are expressed as means ± SD for continuous variables and numbers and percentage for discrete variables. Two-tailed t-tests were used to evaluate differences in participants’ characteristics, and one-way ANOVA was used to compare means of different groups at baseline and after the 24th week. Percentage changes in body weight, BMI, HbA1c, and lipid profile were calculated at baseline and post-24 weeks for both groups. P<0.05 was considered statistically significant. IBM SPSS version 21.0 was used to manage and analyze the data presented in the study.
Results
A total of 110 Emirati patients with T2DM were invited to participate in the study, 53% were excluded, and 51 obese Emirati patients with T2DM were randomized and allocated to the control group (n=25) and intervention group (n=26). After the start of the study, six and five participants dropped out from the control and intervention groups, respectively. The main reasons for noncompliance included traveling outside the country and being out of reach.
As shown in Table 1, 35 Emirati obese patients with T2DM completed the study (intervention group 18, control group 17), with 57% females in the intervention group and 69% females in the controls. The mean age of participants was 39.0±8.0 years and 39.8±6.9 years in the intervention and control groups, respectively. Diagnosis of T2DM was confirmed at age 31.7±7.2 years (intervention group) and 28.0±7.6 years (control group). Diabetes duration in the latter was 12.3±6.9 years, whereas the intervention group had diabetes for 7.0±5.7 years.
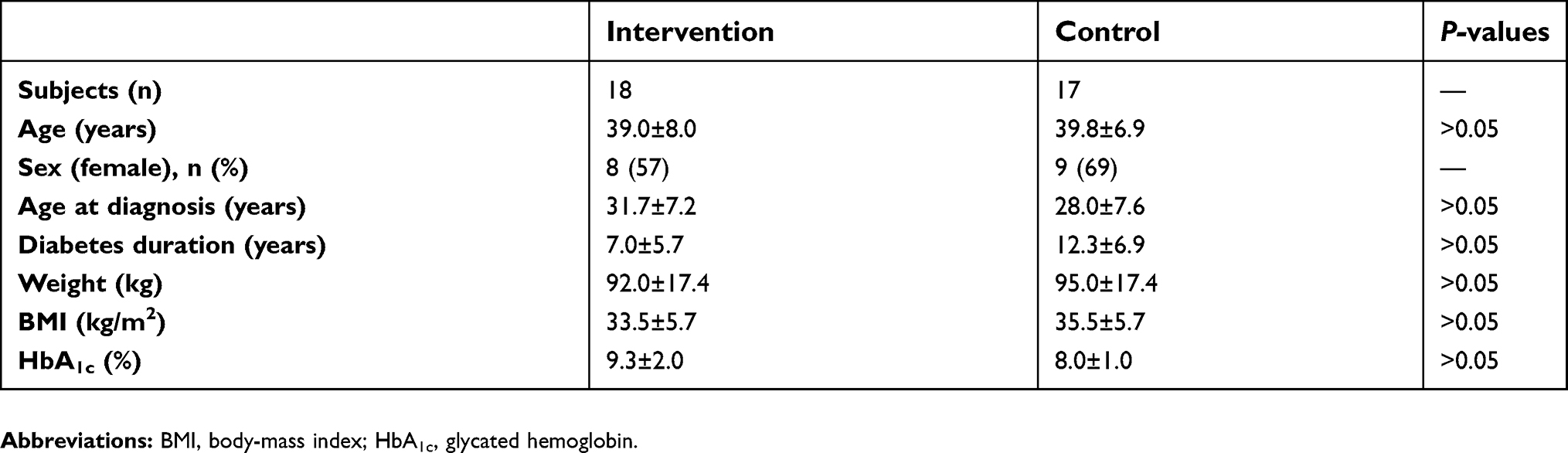 |
Table 1 Baseline demographic and clinical characteristics of the studied population (intervention and control groups) |
In addition, the baseline HbA1c, weight, and BMI were not significantly different between the two groups (P>0.05). Mean body weight and BMI in the intervention group were 92.0±17.4 kg and 33.5±5.7 kg/m2, respectively. The control group exhibited a similar range of body weight (95.0±17.4 kg) and BMI (35.5±5.7 kg/m2).
The personalized intervention led to significant reductions in weight, BMI, and HbA1c in 24 weeks (Table 2). Participants in the intervention group experienced more significant reduction in weight (–3.2±2.9) than participants in the control group (–0.02±4.5), and this outcome was statistically significant (P<0.05). Similarly, reduction in BMI was more significant in the intervention group (–4.50±5.9) than the control group (–0.0003±3.3). Although a significant (P<0.05) reduction in HbA1c (–5.3±15.7) was observed in the intervention group, an increase in HbA1c was reported in the control group (9.9±13.1).
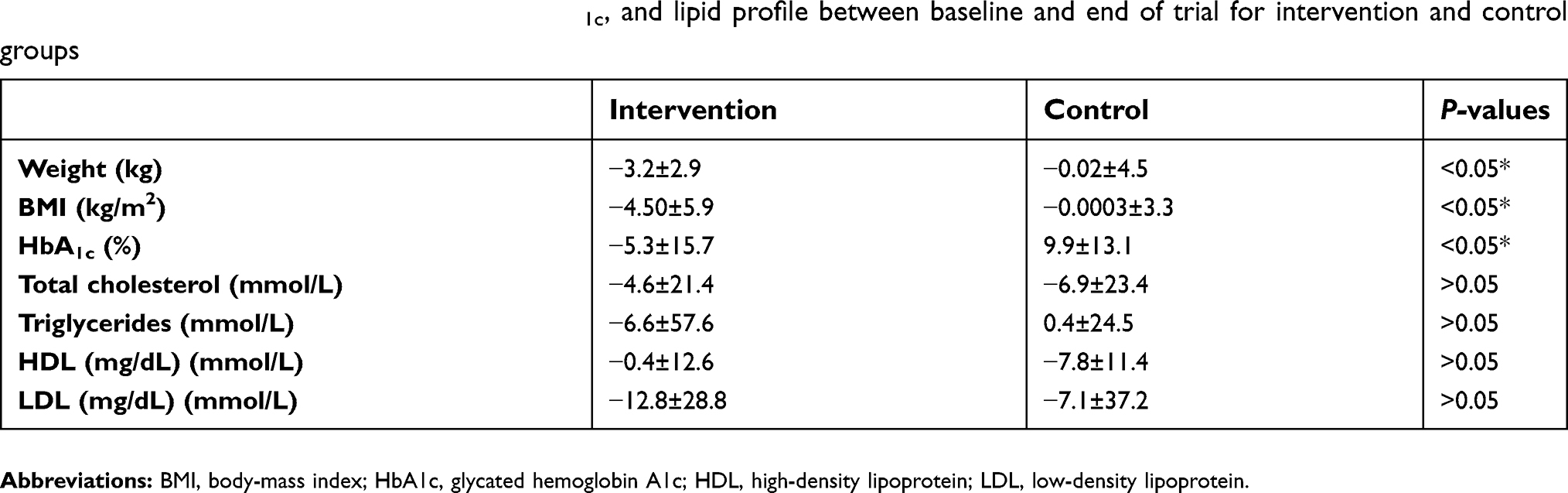 |
Table 2 Percentage change in weight, BMI, HbA1c, and lipid profile between baseline and end of trial for intervention and control groups |
Investigation of lipid profiles in the intervention and control groups showed slight differences in total cholesterol; however, there was more reduction in triglycerides in the intervention group than in the control group. These results were not statistically significant. Similarly, more reduction in low-density lipoprotein (LDL) was reported in the intervention group compared to the control group (P>0.05). In contrast, less reduction in high-density lipoprotein was reported in the intervention group compared to the control group (P>0.05; Table 2).
As shown in Table 3, a significant increase in recovery levels (P<0.001) was observed in obese Emirati patients with T2DM following the personalized intervention. Stress levels (−2.2±27.2%) and duration (−18.53±15.8 hours) were reduced in the intervention group, whereas the control group exhibited high levels (25.3±22.5) and long duration of stress (12.2±16.2 hours). However, these outcomes were not statistically significant (P>0.05).
 |
Table 3 Percentage change in recovery, stress, and sleep duration and quality between baseline and end of trial for intervention and control groups |
Participants in the intervention group tended to have longer sleep duration (9.7±23.2 hours) compared to baseline values, and those in the control group tended to experience less sleep (−3.3±29.6 hours); however, these observations were not statistically significant. In addition, the former group seemed to have better sleep quality (26.9±21.7 ms) than the control group, who experienced lower-quality sleep (−25.5±23.5 ms); however, there was no statistical significance.
Discussion
Several studies have supported the hypothesis that stress is a major contributor to the chronic hyperglycemia that is associated with T2DM.32 It seems that stress plays a dual role in T2DM as a predictor of the onset and a marker of disease severity.33 Although the relationship between stress and T2DM has recently received more attention, it is still a challenge to find the appropriate tool to make solid statements and draw precise conclusions about this relationship. The subjectivity of questionnaires and involvement of cultural beliefs in how patients with T2DM perceive the concept of stress influence the research of stress-induced and -deteriorated T2DM axis. In the present study, we attempted to tackle this challenge by using evidence-based protocols that exclude a great deal of subjectivity and give more accurate outcomes.
It is well documented that measurement of HRV is a noninvasive technique that can be used in real-life settings to provide continuous and precise recording and monitoring of different variables.34 Most of these variables are directly related to the ANS, and thus represent a key tool to identify reactions of this system to different stimuli, including stress and sleep.35
In the present study, the same approach was used, and advanced monitors were given to the participants to record comprehensive data about the physiological changes associated with stress and sleep for 72 hours. The present study used HRV measurement beyond the classical diagnostic approach and implemented a novel plan to manipulate stress and sleep.
The findings of the present study show for the first time that a personalized approach to manage stress and improve sleep quality have a positive impact on glycemic control in obese patients with T2DM. The finding is novel, but not surprising, given the fact that stress is one of the factors that can lead to hyperglycemia, as shown by previous research.36 The relationship between glycemic control and stress has been studied for a long time, but the approach has always been group- and questionnaire-based, and thus the outcomes were inconclusive.13 However, in the present study we applied a personalized approach to identify and create goals for each subject to reduce stressful events and improve the quality of sleep. This led to a significant percentage reduction in HbA1c in the intervention group, whereas the control group failed to maintain the same HbA1c level as the baseline. Interestingly, HbA1c levels showed a trend toward increase in the control group, and this could be explained by the fact that pharmacological antidiabetic treatment is not adequate to maintain fluctuations in HbA1c, and other aspects, including stress and sleep, should be considered.37,38 In addition, previous case reports suggested that increasing HbA1c despite antidiabetic medication could be due to hereditary persistence of hemoglobin F. It has been found that hemoglobin variants and elevated hemoglobin F levels can influence levels of HbA1c and lead to falsely elevated HbA1c measurements; however, with the elements investigated in the present study, it was not possible to confirm this hypothesis.39
It is noteworthy that a significant reduction in weight and BMI was observed in the intervention group compared to the control group. This emphasizes that the management of stress can improve various aspects of quality of life of T2DM patients, including glycemic control and management of weight. In agreement with this finding, Stavrou et al shown that application of stress-management interventions resulted in significant reductions in weight and BMI.40 Although these studies used different interventions to manage stress and were conducted in different populations, the outcomes seem to be consistent with the present findings.
Given the fact that the first line of antidiabetic medications, such as metformin, in combination with other therapies can produce similar effects on HbA1c levels and weight, one can argue that the present observations could have been due to therapies and not the intervention per se.41 However, both the intervention and control groups were exposed to the same spectrum of antidiabetic therapies, supporting the proposal that the present observations were most likely the outcomes of the interventions that were adopted in the present study.
It has been well documented that control of lifestyle variables has a positive impact on lipid profile, and stress is considered a key risk factor for several lipid disorders.39,42 In the present study, some improvements were observed in lipid-profile components in the intervention group compared to controls but these changes were not statistically significant. Total cholesterol, LDL, and triglycerides exhibited a tendency to decrease after the intervention. However, considering the fact that the study was conducted in patients with comorbidities and the study duration was 6 months, the differences between the intervention and control groups may have clinical significance. Previous studies have shown that the effects of multiple interventions that involve physical activities and changing of eating habits produced differential effects on lipid profile.39 Total cholesterol and triglycerides were reduced but LDL increased after these interventions. It is more likely that several factors are involved in regulation of lipid profile components, including management plans.
On the other hand, the influence of reducing stress and improving sleep quality in the present study was manifested clearly in the comparison of recovery periods between the intervention and control groups. The intervention group experienced more significant levels of recovery, and this seems to be the main reason for the improvements observed in this group.
In addition, stress levels and duration were reduced in the intervention group, whereas the control group exhibited high levels and longer duration of stress. Absence of statistical significance in the latter may have been due to the fact that study participants were exposed to different types of stress, and although the action plans were individualized, the nature of stress varied among participants. An alternative explanation is that increasing the level of recovery had more significant effects on the aforementioned variables than decreased levels of stress.
Similarly, sleep periods were longer and sleep quality improved in the intervention group compared to the control group; however, the variation in these parameters showed no statistical significance. The relationship between sleep duration and quality and T2DM has been demonstrated by previous studies, but the main assessment tool was based on self-report, and thus the present study has the advantage that these parameters were measured using a device and diary.5,21
The small sample size in this trial limited our ability to produce stronger outcomes and investigate additional variables. This was due to premature withdrawal from study and the high dropout rate. Further studies with larger samples will give more opportunities to produce concise outcomes with more powerful statistical significance.
Conclusion
The present study has shown that personalized interventions that involve management of stress, enhancement of recovery, and improvement of sleep patterns have a significant effect on glycemic control and weight management in obese patients with T2DM.
Data availability
Research data used in the preparation of the manuscript are available for sharing upon reasonable request. This includes the assessment tools and individual deidentified participant data. The data can be obtained from Dr Bashair M Mussa or https://clinicaltrials.gov.
Acknowledgments
The authors would like to acknowledge Rashid Centre for Diabetes and Research for supporting the study and providing all the required resources. Also, the authors would like to thank Celo-Lab for providing us with the monitoring devices. Furthermore, the authors would like to acknowledge all participants of the study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ginter E, Simko V. Global prevalence and future of diabetes mellitus. Adv Exp Med Biol. 2012;771:35–41.
2. Wild S, Roglic G, Green A, Sicree R, King H. Global prevalence of diabetes: estimates for the year 2000 and projections for 2030. Diabetes Care. 2004;27(5):1047–1053.
3. WHO. Obesity: preventing and managing the global epidemic. World Health Organ Tech Rep Ser. 2000;894(i–xii):1–253.
4. IDF. The IDF Diabetes Atlas.
5. Thomas D, Frankenberg E. Health, nutrition and prosperity: a microeconomic perspective. Bull World Health Organ. 2002;80(2):106–113.
6. Barakat-Haddad C. Prevalence of high blood pressure, heart disease, thalassemia, sickle-cell anemia, and iron-deficiency anemia among the UAE adolescent population. J Environ Public Health. 2013;2013:1–10. doi:10.1155/2013/680631
7. Streib L. World‘S Fattest Countries. Forbes. New York, USA: Forbes Media, LLC; 2007.
8. Imam K. Managment and treatment of diabetes mellitus. Advences Exp Med Biol. 2012;771:356–380.
9. Weitgasser R, Niebauer J. Lifestyle modification. Wien Klin Wochenschr. 2012;124(Suppl 2):7–9. doi:10.1007/s00508-012-0275-1
10. Williams ED, Magliano DJ, Tapp RJ, Oldenburg BF, Shaw JE. Psychosocial stress predicts abnormal glucose metabolism: the Australian diabetes, obesity and lifestyle study. Ann Behav Med. 2013;46(1):62–72. doi:10.1007/s12160-013-9473-y
11. Surwit RS, Schneider MS, Feinglos MN. Stress and diabetes mellitus. Diabetes Care. 1992;15:1413–1422.
12. Wales JK. Does psychological stress cause diabetes? Diabetic Med. 1995;12:109–112.
13. Surwit RS, van Tilburg MA, Zucker N, et al. Stress management improves long-term glycemic control in type 2 diabetes. Diabetes Care. 2002;25(1):30–34.
14. Koloverou E, Tentolouris N, Bakoula C, Darviri C, Chrousos G. Implementation of a stress management program in outpatients with type 2 diabetes mellitus: a randomized controlled trial. Hormones (Athens). 2014;13(4):509–518. doi:10.14310/horm.2002.1492
15. Mello D, Wiebe DJ, Barranco C, The Stress BJ. Coping context of type 1 diabetes management among latino and non-latino white early adolescents and their mothers. J Pediatr Psychol. 2017;42(6):647–656. doi:10.1093/jpepsy/jsw109
16. Saghaei M, Omidi P, Dehkordi EH, Safavi P. The effectiveness of cognitive-function stress management training in glycemic control in children and in mental health of mother caring for child with type 1 diabetes mellitus. Diabetes Metab Syndr. 2017;11(Suppl 2):S925–S928. doi:10.1016/j.dsx.2017.07.017
17. Bjőrntorp P. Body fat distribution, insulin resistence and metabolic disease. Nutrition. 1997;13:795–803.
18. Sulaiman N, Hamdan A, Tamim H, Mahmood DA, Young D. The prevalence and correlates of depression and anxiety in a sample of diabetic patients in Sharjah, United Arab Emirates. BMC Fam Pract. 2010;11. doi:10.1186/1471-2296-11-80
19. El-Rufaie OEF, Bener A, Ali TA, Abuzied MSO. Psychiatric morbidity among type II diabetic patients: a controlled primary care survey. Primary Care Psychiatry. 1997;3:189–194.
20. Group TLAR. Long term effects of a lifestyle intervention on weight and cardiovascular risk factors in individuals with type 2 diabetes: four year results of the look AHEAD trial. Arch Intern Med. 2010;170(17):1566–1575. doi:10.1001/archinternmed.2010.328
21. Pi-Sunyer X. The look AHEAD trial: a review and discussion of its outcomes. Curr Nutr Rep. 2014;3(4):387–391. doi:10.1007/s13668-014-0099-x
22. Dishman RK, Nakamura Y, Garcia ME, Thompson RW, Dunn AL, Blair SN. Heart rate variability, trait anxiety, and perceived stress among physically fit men and women. Int J Psychophysio. 2000;37(2):121–133. doi:10.1016/S0167-8760(00)00085-4
23. Minich DM, Bland JS. Personalized lifestyle medicine: relevance for nutrition and lifestyle recommendations. Sci World Jl. 2013;129841. doi:10.1155/2013/129841
24. Lloyd C, McKenna K, King R. Sources of stress experienced by occupational therapists and social workers in mental health settings. Occup Ther Int. 2005;12(2):81–94.
25. Herschbach P, Duran G, Waadt S, Zettler A, Amm C, Marten-Mittag B. Psychometric properties of the Questionnaire on Stress in Patients with Diabetes–revised (QSD-R). Health Psychol. 1997;16(2):171.
26. Wilcox CS, Welch WJ, Murad F, et al. Nitric oxide synthase in macula densa regulates glomerular capillary pressure. Proc National Acad Sci (USA). 1992;89(24):11993–11997. doi:10.1073/pnas.89.24.11993
27. Eom YS, Park HS, Kim SH, et al. Evaluation of stress in korean patients with diabetes mellitus using the problem areas in diabetes-Korea questionnaire. Diabetes Metab J. 2011;35(2):182–187. doi:10.4093/dmj.2011.35.2.182
28. Chrousos GP, Gold PW. The concepts of stress and stress system disorders. Overview of physical and behavioral homeostasis. JAMA. 1992;267(9):1244–1252.
29. Castaneda JO, Segerstrom SC. Effect of stimulus type and worry on physiological response to fear. J Anxiety Disord. 2004;18(6):809–823. doi:10.1016/j.janxdis.2003.10.003
30. Martinmäki K, Rusko H, Kooistra L, Kettunen J, Saalast S. Intraindividual validation of heart rate variability indexes to measure vagal effects on hearts. Am J Physiol Heart Circ Physiol. 2006;290(2):H640–H647. doi:10.1152/ajpheart.00054.2005
31. Chandola T, Heraclides A, Kumari M. Psychophysiological biomarkers of workplace stressors. Neurosci Biobehav Rev. 2010;35(1):51–57. doi:10.1016/j.neubiorev.2009.11.005
32. Hackett RA, Steptoe A. Type 2 diabetes mellitus and psychological stress - a modifiable risk factor. Nat Rev Endocrinol. 2017;13(9):547–560. doi:10.1038/nrendo.2017.64
33. Marik PE, Bellomo R. Stress hyperglycemia: an essential survival response! Crit Care Med. 2013;41(6):e93–e94. doi:10.1097/CCM.0b013e318283d124
34. Sztajzel J. Heart rate variability: a noninvasive electrocardiographic method to measure the autonomic nervous system. Swiss Med Wkly. 2004;134(35–36):514–522. doi:10.4414/smw.2004.10321
35. Myllymäki T, Rusko H, Syväoja H, Juuti T, Kinnunen ML, Kyröläinen H. Effects of exercise intensity and duration on nocturnal heart rate variability and sleep quality. Eur J Appl Physiol. 2012;112(3):801–809. doi:10.1007/s00421-011-2034-9
36. Faulenbach M, Uthoff H, Schwegler K, Spinas GA, Schmid C, Wiesli P. Effect of psychological stress on glucose control in patients with type 2 diabetes. Diabet Med. 2012;29(1):128–131. doi:10.1111/j.1464-5491.2011.03431.x
37. Woo MH, Park S, Woo JT, Choue R. A comparative study of diet in good and poor glycemic control groups in elderly patients with type 2 diabetes mellitus. Korean Diabetes J. 2010;34(5):303–311. doi:10.4093/kdj.2010.34.5.303
38. Asif M. The prevention and control the type-2 diabetes by changing lifestyle and dietary pattern. J Educ Health Promotion. 2014;3:1. doi:10.4103/2277-9531.127541
39. Christaki E, Kokkinos A, Costarelli V, Alexopoulos EC, Chrousos GP, Darviri C. Stress management can facilitate weight loss in Greek overweight and obese women: a pilot study. J Hum Nutr Diet. 2013;26(Suppl 1):132–139. doi:10.1111/jhn.12086
40. Stavrou S, Nicolaides N, Papageorgiou I, et al. The effectiveness of a stress-management intervention program in the management of overweight and obesity in childhood and adolescence. J Mol Biochem. 2016;5(2):63–70.
41. Wilding J, Godec T, Khunti K, et al. Changes in HbA1c and weight, and treatment persistence, over the 18 months following initiation of second-line therapy in patients with type 2 diabetes: results from the United Kingdom clinical practice research datalink. BMC Med. 2018;16(1):116. doi:10.1186/s12916-018-1085-8
42. Assadi SN. What are the effects of psychological stress and physical work on blood lipid profiles? Medicine (Baltimore). 2017;96(18):e6816. doi:10.1097/MD.0000000000006816
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.