Back to Journals » International Journal of General Medicine » Volume 16
Peripheral Mononuclear Cells Surface Markers Evaluation in Different Stages of Hepatocellular Carcinoma; in a Trial for Early and Accurate Diagnosis in Patients with Post-Hepatitis Liver Cirrhosis and Unremarkable Raised AFP
Authors Osman HA ![]() , Nafady-Hego H
, Nafady-Hego H ![]() , Nasif KA, Ahmed HA
, Nasif KA, Ahmed HA ![]() , Mahmoud EAR, Abass NM, Rayan A
, Mahmoud EAR, Abass NM, Rayan A ![]() , Mahmoud MA, Nafady A
, Mahmoud MA, Nafady A
Received 17 January 2023
Accepted for publication 7 March 2023
Published 22 March 2023 Volume 2023:16 Pages 1047—1058
DOI https://doi.org/10.2147/IJGM.S404914
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Heba Ahmed Osman,1 Hanaa Nafady-Hego,2 Khalid Ali Nasif,3,4 Heba A Ahmed,5 Ekram Abdel-Rahman Mahmoud,6 Noher Mohamad Abass,7 Amal Rayan,8 Marwa Ahmed Mahmoud,9 Asmaa Nafady10
1Department of Tropical Medicine and Gastroenterology, Qena Faculty of Medicine, South Valley University, Qena, Egypt; 2Department of Microbiology and Immunology, Faculty of Medicine, Assiut University, Assiut, Egypt; 3Department of Clinical Biochemistry, College of Medicine, King Khalid University, Abha, Kingdom of Saudi Arabia; 4Department of Biochemistry, Faculty of Medicine, Minia University, Minia, Egypt; 5Department of Clinical and Chemical Pathology Sohag Faculty of Medicine Sohag University, Sohag, Egypt; 6Department of Medical Microbiology & Immunology, Faculty of Medicine, Sohag University, Sohag, Egypt; 7Department of Internal Medicine, Faculty of Medicine, Sohag University, Sohag, Egypt; 8Department of Clinical Oncology, Faculty of Medicine, Assiut University, Assiut, Egypt; 9Department of Medical Physiology, Faculty of Medicine, Sohag University, Sohag, Egypt; 10Department of Clinical and Chemical Pathology, Qena Faculty of Medicine, South Valley University, Qena, Egypt
Correspondence: Heba Ahmed Osman, Tropical Medicine and Gastroenterology, Qena Faculty of Medicine, South Valley University, Qena, Egypt, Email [email protected]; [email protected]
Introduction: HCC is frequently diagnosed late, when only palliative treatment is available. So, we try to use different immunological markers to identify early HCC in patients with unremarkable raised AFP.
Methods: This study was conducted on 112 participants divided into two equal groups: Group I, 56 patients with liver cirrhosis and different stages of HCC; Group II, 56 patients with liver cirrhosis. The diagnosis of HCC was based on AASLD guidelines. TNM and BCLC classification systems are used for staging of HCC.
Results: A significant reduction in the median percentage of lymphocyte subset (CD3+, CD4+, CD8+, CD19+) and NK cell percentage (CD56+) has been detected in HCC patients (all P < 0.001). In the HCC group the median monocyte subpopulations CD14+ CD16− Classical, CD14++ CD16+ Intermediate, and CD14−+ CD16++ Non-Classical were 11.7, 4.0, and 3.5, respectively, with marked reduction compared with liver cirrhosis group (all P < 0.001). Patients with advanced stages (BCLC C and D) were more likely to have significantly higher median CD33+ than patients with early stages (BCLC A and B) (P = 0.05); also, the median levels of HLA DR+ lymphocytes % in the HCC case group were 21.8 in patients with advanced disease (BCLC C and D) and 13.1 in patients with early stages of the disease (P = 0.04). Patients with late stage (TNM III) were more likely to have significantly higher median CD14+ CD16− Classical monocyte subset, CD36+ HLA DR+, and CD36+ CD16− than patients with early stages (TNM I and II).
Conclusion: Patients with HCC with unremarkable raised AFP showed marked reduction in lymphocytes, natural killer cells, and all monocyte subpopulations. In addition, patients with advanced HCC showed increased CD33+ and HLA DR+ lymphocytes %, CD14+ CD16− Classical monocyte subset, CD36+ HLA DR+, and CD36+ CD16− compared with patients with early stages of HCC.
Keywords: monocyte subpopulation, lymphocyte subset, hepatocellular carcinoma, Barcelona clinic liver cancer, tumor (T), nodes (N), metastases (M)
Introduction
Hepatocellular carcinoma (HCC) is a primary tumor of the liver, develops on top of chronic liver disease especially alcoholic cirrhosis, and can also be developed on top of chronic hepatitis B or C virus infections, or nonalcoholic steatohepatitis.1,2
HCC is the fourth leading cause of cancer-related deaths worldwide.3,4 Unfortunately, HCC still carries a poor prognosis, with a five-year survival rate that does not exceed 20%.5
Many immune cell types penetrate HCC and influence the tumor’s microenvironment. Major participants in the inflammation process and in reducing the anti-tumor response are thought to be tumor-associated macrophages. These macrophages produce immunomodulatory cytokines that can suppress anti-tumor immunity, such as interleukin (IL)-10 and transforming growth factor (TGF).6
Tumor-associated macrophages are not the only immune cell types seen in tumor tissue. Innate immune cells like natural killer (NK) cells and adaptive immune cells like CD8+ T cells can also be found there. These immune cells can kill altered cells by releasing cytolytic enzymes like perforins and granzymes.7
The ease with which peripheral immune indicators may be tested in plasma or serum using very simple interface technology makes them an appealing choice. The ability of leucocytes to recognize tumor cells, which is crucial for oncogenesis, makes them one of the immune markers that offers hope for the early diagnosis of HCC.8
HCC is frequently diagnosed late in its course, mainly due to the absence of symptoms in patients with early disease.9
The aim of the diagnosis of HCC is for the early detection of the mass when its size is ≤2 cm, at which point different treatment modalities are available.10
The diagnosis of HCC is difficult; it may require two imaging modalities. Serum AFP level can be helpful for diagnosis when it is markedly elevated; however, it is detected in less than 50% of diagnosed patients at the time of diagnosis.11 Confirmation by liver biopsy can be performed only in certain situations when the diagnosis of HCC is unclear.12
No single international guideline for the diagnosis of HCC exists due to marked differences in the diagnostic approach between Eastern and Western countries.13
Surgical excision of HCC provides a chance of cure for patients. Regrettably, less than one-third of patients meet the criteria for HCC resection at the time of diagnosis.14
So, in this study, we focused on using different immunological markers using flow cytometry to identify early HCC defined by size of tumor, number of lesions, and stage of the tumor, using different HCC classification scoring systems in patients with unremarkable raised AFP.
Patients and Methods
This prospective randomized case-control study was conducted on 112 participants divided into two equal groups: Group I, 56 patients with liver cirrhosis and different stages of HCC who were admitted to the Tropical Medicine and Gastroenterology Department, Qena Faculty of Medicine, South Valley University, and the Internal Medicine Department, Sohag University, during the period from January 1, 2021, to October 30, 2022; Group II, 56 patients with liver cirrhosis with different degrees of liver disease severity according to the Child score.
All patients were subjected to complete history-taking and a full clinical examination. The diagnosis of HCC was based on the AASLD (American Association for the Study of Liver Diseases) guideline.15 The Child–Pugh score was used to determine the severity of liver disease,16 and the Tumor (T), Nodes (N), and Metastases (M) (TNM)17 and Barcelona Clinic Liver Cancer (BCLC) classification systems18 were used for staging of HCC.
Investigatory Workup
Multiphasic CT for HCC Diagnosis
Multiphasic CT was conducted with a 64-MDCT scanner (Aquilion 64, Toshiba Medical, Otawara, Japan). Following intravenous non-ionic iodinated contrast infusion, HCC tumors receive blood mainly from the hepatic artery, while the surrounding hepatic parenchyma obtains its blood mainly via the portal vein. The presence of arterial enhancement 30–40 seconds after infusion of the contrast agent for a hepatic focal lesion ≥2 cm in size with subsequent washout (hypodense HCC compared with the surrounding hepatic parenchyma) on portal phases (which began 70 seconds after the injection of the contrast material) and equilibrium phases started 180 seconds after contrast injection is considered to be the definitive CT feature of HCC by different associations for liver diseases guidelines.15,19–21
Biochemical Assays
A 10 mL blood sample was obtained from all patients and control groups under sterile conditions; 5 mL on EDTA were investigated for CBC by hematology analyzer (CELL-DYN Ruby System; Abbott Diagnostics, Chicago, IL, USA). The absolute counts of peripheral white blood cells were calculated from peripheral blood films and for flow cytometry with detection of lymphocytes subgroups, and the other 5 mL serum sample was used for evaluation of blood urea, serum creatinine, alanine aminotransferase (ALT), aspartate aminotransferase (AST), albumin, alkaline phosphatase (ALP), and total and direct bilirubin using a Beckman AU 480 fully automated biochemistry analyzer.
Citrated plasma samples were used to assay prothrombin time (PT), prothrombin concentration (PC), and international normalized ratio (INR) using a Sysmex CS-1600 Automated Blood Coagulation Analyzer. Serum alpha-fetoprotein (AFP) assessment was carried out by the AIA-360 Automated Immunoassay Analyzer - Tosoh Bioscience. Hepatitis B surface antigen (HBsAg) estimation, HCV antibody detection, and HCV quantitative PCR assay for patients with positive HCV antibodies were performed using the automated ARCHITECT i1000SR immunoassay analyzer.
Flow Cytometry with Detection of Lymphocytes Subgroups
The types of lymphocytes were measured by CD4 fluorescein isothiocyanate (FITC), CD8 phycoerythrin (PE), CD3 peridinin-chlorophyll-protein (PerCP), CD19 fluorescein isothiocyanate (FITC), and CD56 phycoerythrin (PE). HLADR peridinin-chlorophyll-protein (PerCP) binding assay was done according to the manufacturer’s instructions (BD Biosciences, San Jose, CA, USA). A 100 μL aliquot of whole blood was stained with 10 μL of each monoclonal antibody, washed twice with 2 mL of phosphate-buffered saline (PBS), and red blood cells were lysed by BD FACS lysing solution. The cells were washed and resuspended in 100 μL of PBS. Analysis was done using FACS Calibur flow cytometry. Anti-human IgG was used as an isotype-matched negative control with each sample. A forward and side scatter histogram was used to identify the lymphocyte population. Then, the percentages of CD3+, CD4+, CD8+, CD19+, CD56+, and HLADR+ lymphocytes were assessed in the lymphocyte population, and the total percentages were then calculated among the lymphocytes (Figure 1).
 |
Figure 1 Lymphocyte gating with CD3+ T-cells and subdivided T helper CD4+ and cytotoxic CD8+ cells. |
Ethical Approval
The study was done in accordance with Helsinki guidelines. The Institutional Review Board, Qena Faculty of Medicine, Egypt, approved this study (code number: SVU-MED-GIT023-4-22-9-446), and all participants gave an informed consent to join the study.
Results
Patient Characteristics and Clinical Outcomes
A total of 56 patients with accidentally discovered HCC were included in our study. The baseline characteristics of the HCC patients are shown in Table 1. The HCC patient group includes 41 (73.2%) males and 15 (26.8%) females. They ranged in age from 50 to 65 years, and the median age was 58 years. All HCC patients have post-hepatitis, liver cirrhosis. Hepatitis B and hepatitis C were diagnosed in 8 (14.3%) and 48 (85.7%) patients, respectively; 33 (58.9%) of the latter received DAAs therapy and achieved SVR. On admission, 12 (21.4%) were Child–Pugh class A, 22 (39.3%) were Child–Pugh class B, and 22 (39.3%) were Child–Pugh class C. Median α-fetoprotein (AFP) was ≥21.9 ng/mL (IQR 6.3–61.25). A total of 13 (23.2%), 10 (17.9%), 14 (25%), and 19 (33.9%) patients were classified as Barcelona Clinic Liver Cancer (BCLC) stages A, B, C, and D, respectively. On admission, 16 (28.6%) were TNM stage I, 3 (5.4%) were TNM stage II, and 37 (66.1%) were TNM stage III; 38 (67.9%) patients had a single tumor. Right lobe hepatic focal lesion was found in 30 (52.6%), left lobe involvement in 18 (32.1%), and both right and left lobe involvement in 8 (14.3%) patients. The single hepatic focal lesion was diagnosed in 38 (67.9%), and multiple hepatic focal lesions were detected in 18 (32.1%) of patients. Portal vein thrombosis was observed in 30 (53.6%) patients.
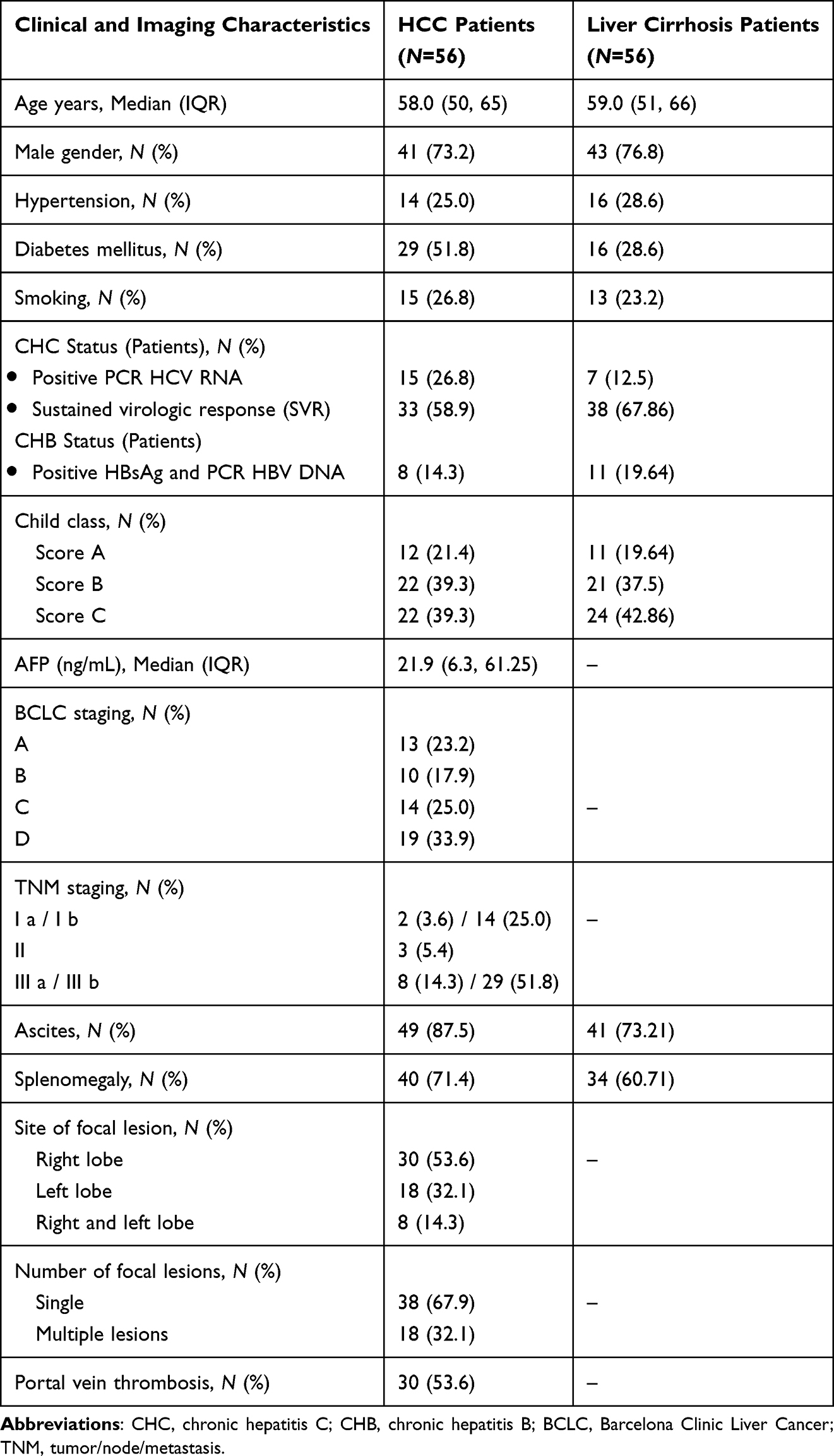 |
Table 1 Clinical and Imaging Characteristics of the Included HCC and Liver Cirrhosis Patients |
The demographics of the liver cirrhosis group were as follows: 43 (76.8%) males and 13 (23.21%) females. They ranged in age from 51 to 66 years, and the median age was 59 years. All liver cirrhosis patients have post-hepatitis liver cirrhosis. Hepatitis B and hepatitis C were diagnosed in 11 (19.64%) and 46 (82.14%) patients, respectively, and 38 (67.86%) of the latter received DAAs therapy and achieved SVR. At presentation, 11 (19.64%) were Child–Pugh class A, 21 (37.5%) were Child–Pugh class B, and 24 (42.86%) were Child–Pugh class C (Table 1).
Comparison of Routine Laboratory Data Between Studied Groups
As shown in Table 2, the median levels of hemoglobin, platelets, total white blood cell count, total lymphocyte count, monocytic count, and serum albumin all tended to be lower in the HCC group than in the patients with liver cirrhosis; however, the median INR, ALT, AST, total bilirubin, and alkaline phosphatase (ALP) levels were significantly higher in the HCC groups than in the liver cirrhosis group.
 |
Table 2 Routine Laboratory Data of the Study Groups |
Immunological Data of the Study Groups
Immunological measurements for the study groups are shown in Table 3. In the HCC group the median (IQR) lymphocyte subset and NK cell proportions CD3%, CD4%, CD8%, CD19%, and CD56% were 50.4 (8.6, 61.1), 13.9 (4.3, 36.4), 14.9 (8.3, 27.8), 5.4 (2.4, 14.6), and 14.3 (9.3, 21.1), respectively. In the liver cirrhosis group, the median (IQR) CD3%, CD4%, CD8%, CD19%, and CD56% were 50.9 (32.5, 77.0), 24.2 (16.0, 49.2), 26.9 (16.3, 36.4), 34.8 (11.1, 59.6), and 24.0 (16.6, 58.0), respectively (all P < 0.001).
 |
Table 3 Immunological Data of the Study Groups (All Data are Presented as Percentage) |
In the HCC group the median (IQR) monocyte subpopulation CD14+ CD16− Classical, CD14++CD16+ Intermediate, and CD14−+ CD16++ Non-Classical were 11.7 (5.1, 20.5), 4.0 (2.1, 9.5), and 3.5 (0.5, 9.0), respectively. In the liver cirrhosis group, the median (IQR) CD14+ CD16− Classical, CD14++ CD16+ Intermediate, and CD14−+ CD16++ Non-Classical were 38.4 (17.9, 55.7), 18.3 (14.0, 33.5), and 39.9 (19.8, 68.7), respectively (all P < 0.001) (Figure 2).
 |
Figure 2 Monocyte subsets (classical, intermediate, and non-classical monocytes) on gated monocytes. The upper part of the figure shows marked increase in non-classical monocytes. The lower part of the figure shows decreased intermediate and absent non-classical monocytes. |
With regard to the median (IQR) level of CD16+ CD36+, CD36+ HLA DR+, HLA DR+ lymphocytes%, and CD16+ HLA DR+ in the HCC case group, they were 6.0 (3.8, 7.6), 10.0 (7.7, 23.7), 15.1 (7.3, 26.0), and 3.6 (2.5, 12.3), respectively. Their median (IQR) level in the liver cirrhosis group were 46.9 (38.2, 71.2), 60.4 (30.0, 78.8), 32.9 (19.0, 36.9), and 58.1 (37.4, 77.7), respectively (all P < 0.001).
Association of Immune Cell Counts with BCLC Stage in HCC Group
Table 4 shows the associations between immune cell count and BCLC stages, and patients with advanced stages (BCLC stage C and D) were more likely to have significantly higher percentage of CD33+ than patients with early stages (BCLC stage A and B): 83.9 (74.9, 88.7) and 74.9 (60.0, 85.6), respectively (P = 0.05).
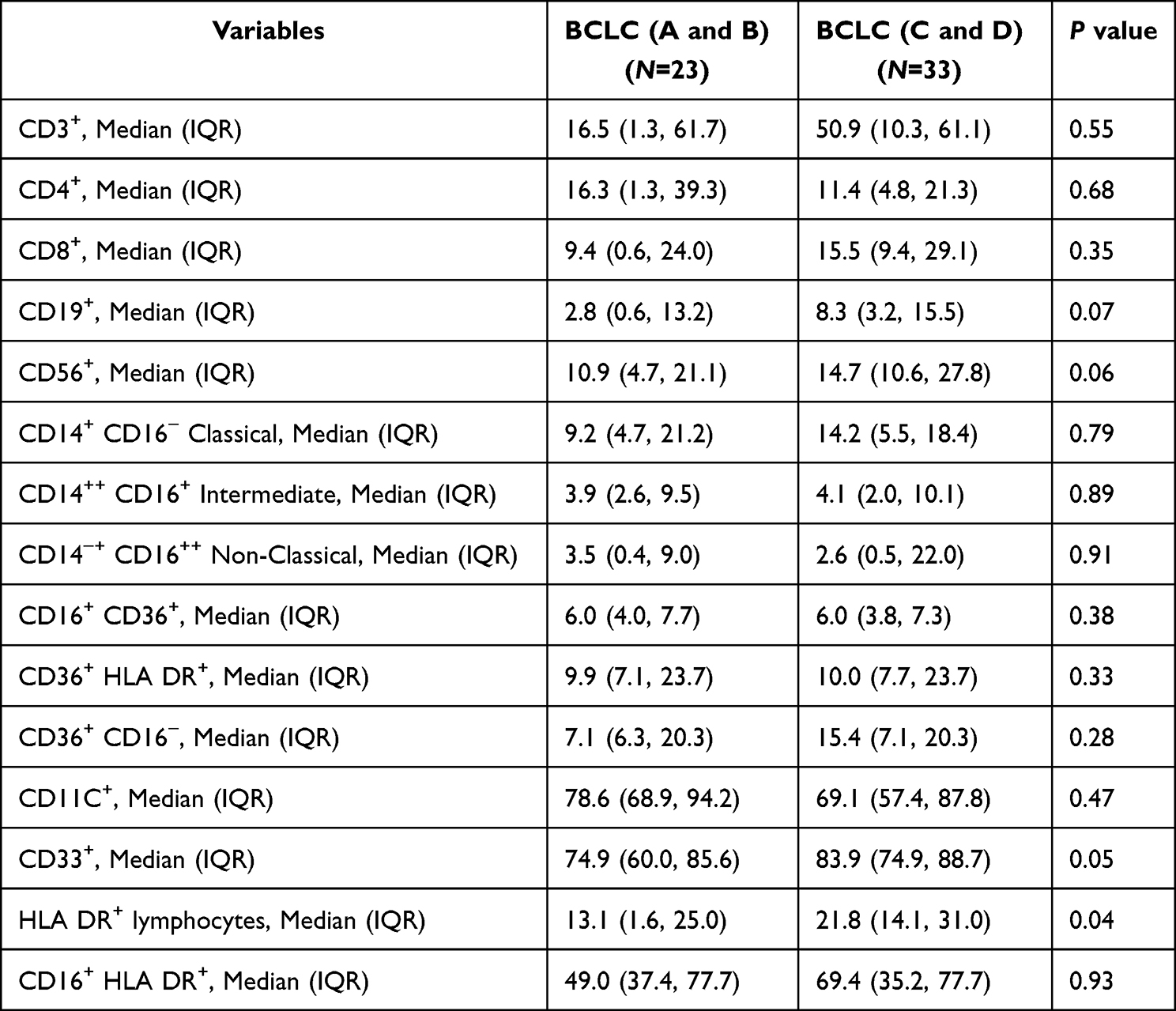 |
Table 4 Immunological Data of the Different Barcelona Clinic Liver Cancer (BCLC) Scoring Systems of HCC (All Data are Presented as Percentage) |
With regard to the median (IQR) level of HLA DR+ lymphocytes % in the HCC case group, they were 21.8 (14.1, 31.0) in patients with more advanced disease (BCLC stage C and D) and 13.1 (1.6, 25.0) in patients with early stages of the disease. High HLA DR expression on lymphocytes was associated with HCC progression (P = 0.04).
Comparing immunological parameters for the HCC study group and TNM staging, patients with early stages (TNM stage I and II) were more likely to have significantly lower median (IQR) CD14+ CD16− Classical monocyte subset, CD36+ HLA DR+, and CD36+ CD16− than patients with advanced stages (TNM stage III); the former were 9.1 (1.6, 15.0), 7.7 (6.4, 12.1), and 7.1 (1.7, 15.4), respectively, while the latter were 14.9 (7.2, 40.3), 10.0 (7.7, 23.7), and 15.4 (6.8, 20.3), respectively (P = 0.04), (P = 0.04), and (P = 0.03), respectively (Table 5).
 |
Table 5 Immunological Data of the Different TNM Scoring Systems of HCC (All Data are Presented as Percentage) |
Discussion
Both cellular and humoral immune responses work together to kill tumor cells, with a more important role of the cellular than the humoral immune response.22 The three categories of lymphocytes (T lymphocytes, B lymphocytes, and natural killer cells) are of great importance in the immune system by maintaining immunological balance through suppressing a great number of immune responses.23,24 Disruption in lymphocyte function is associated with disturbance of the immune system.25 It is widely accepted that the occurrence and progression of HCC is associated with the condition of the adaptive immunity; in addition, a normally functioning immune system can serve as therapeutic antitumor.26,27
As far as we are aware, only a few studies have examined the part played by a subset of monocytes in the initiation and progression of HCC. In view of the important activities of these cells, we detected the levels of peripheral blood monocytes and different lymphocyte subsets in patients with accidentally discovered HCC, and we found a marked reduction in total white blood cell count and total lymphocyte count in HCC patients compared with the group of patients with liver cirrhosis which is in agreement with Fujiwara et al, who found reductions in total white blood cell count and lymphocyte count in patients with HCC and considered that a raised white blood cell count correlated with advanced HCC and worse survival.28
Monocytes play an important role in innate immunity and exhibit prognostic value in cancers.29 Classical (CD14+ CD16−), intermediate (CD14++ CD16+), and non-classical (CD14−+ CD16++) monocytes are the three subsets of human monocytes that are distinguished by their CD14 and CD16 expressions.30
As opposed to patients with liver cirrhosis, patients with HCC in our study displayed a significantly lower level of each of the three monocyte subpopulations.
This is in line with the findings of Cardoso et al, 2021, who discovered a rise in monocyte subsets in their liver cirrhosis patients, with a higher rise in monocyte subsets in patients with decompensated cirrhosis.31
To our knowledge no study has evaluated mononuclear cell count as a diagnostic marker for early diagnosis. However, a few studies have evaluated the role of mononuclear cells as a prognostic marker and correlated low cell count with HCC recurrence and poor outcome.32–34
In this study a significant reduction in CD3, CD4 (helper T-cell marker), CD8 (cytotoxic T-cell marker), and CD19 (B-lymphocyte marker) lymphocytic count was detected in patients with HCC compared with patients with liver cirrhosis.
More than 80% of our cirrhotic patients had decompensated cirrhosis, and Buch et al’s study indicated that peripheral lymphocyte count can increase along with liver cirrhosis progression. Moreover, Wang et al discovered that patients with liver cirrhosis had an increase in peripheral blood lymphocytes, and that this increase was directly correlated with the severity of the disease and a bad prognosis.35,36
Regarding peripheral reduction of all lymphocyte subsets in our HCC patients, our results agree with those of Liu et al, who found in their study on HCC patients a marked reduction of all lymphocyte subsets except CD8+, which showed marked elevation, and considered it related to the fact that more than 80% of their patients were HBV carriers, which alters the proportions of the peripheral blood lymphocytes.37
In our opinion, in the current study, a marked reduction of all lymphocyte subsets in patients with HCC compared with patients with liver cirrhosis could be related to the functional depletion of lymphocytes during both HBV and HCV infections in the trial to clear the infection.
In this study, a marked increase of CD56+ (NK cells markers) was detected in patients with liver cirrhosis compared with healthy controls.
This could be related to both chronic HBV infection and chronic HCV infection being associated with increases in peripheral blood NK cells.38
Otherwise, a marked reduction in CD56+ (NK cell markers) was detected in this study in the HCC patient group compared with the liver cirrhosis group.
The same finding was detected by Liu et al and Heiberg et al in their studies, where a marked reduction of NK cells was seen in HCC patients.37–39
This could be related to antiviral and antitumor functions of NK cells, and the reduced number of NK cells in patients with post-hepatitis liver cirrhosis suggests that NK cells may be involved in the development of HCC.
In our study CD16+ CD36+, CD36+ HLA DR+, CD11C+, HLA DR+ lymphocytes percentage, and CD16+ HLA DR+ showed marked reduction in patients with HCC compared with patients with liver cirrhosis.
It is known that CD16+ is expressed on monocytes, lymphocytes, and NK cells in addition to being able to stimulate strong cytotoxicity and cytokine production.40 Most probably its reduction is linked with impairment of function of the immune system. At the same time, the low CD36 expression has been linked with highly aggressive malignancy, tumor metastasis, and a poor prognosis.41 CD36 being expressed on hepatocytes, its reduced level may play a great role in HCC development and early progression. Also, the HLA DR reduction indicates impairment of both adaptive and innate immunity in patients with hepatocellular carcinoma.
CD11c+ is expressed on monocytes, granulocytes, B cells, dendritic cells, and macrophages with abundant expression in monocytes. So, its level is reduced in patients with HCC compared with patients with liver cirrhosis related to monocytopenia in patients with HCC.42
It has been found by multiple previous studies that HCC triggers an intrinsic inflammatory reaction.43 In addition, oncogenes such as RAS and MYC family members induce the recruitment of leukocytes and lymphocytes.44 The subsequent inflammatory response stimulates neo-angiogenesis and elicits immune cells that can provide growth factors to malignant cells.45
In this study, CD33+ (as a neutrophil marker of inflammation) was higher in patients with advanced liver HCC as classified by the BCLC staging system.
This is in agreement with Liu et al, who found that the CD33+ marker was significantly associated with aggressive HCC and poor survival rates.46
Also, in this study we found that the HLA DR+ lymphocytes % in the HCC case group (as a marker of lymphocyte activation) was higher in patients with more advanced HCC disease (BCLC stage C and D).
This is in agreement with Mossanen et al, who concluded that the immune system, especially lymphocytes, has a great role in HCC development and progression.47
In our study we found that patients with HCC and advanced TNM staging (TNM stage III) have obvious higher CD14+ CD16− Classical monocyte subset, CD36+ HLA DR+, and CD36+ CD16− than patients with early TNM stages (TNM stage I and II).
This agrees with Sasaki et al, who found that a higher peripheral blood monocyte count was associated with a poor prognosis in patients with hepatocellular carcinoma.48 Also, Luo et al found that CD36 has a stimulatory effect on HCC growth and metastasis, by aerobic glycolysis through the Src/PI3K/AKT/mTOR signaling pathway.49
Conclusion
Patients with HCC with unremarkable raised AFP showed marked reduction in lymphocytes, natural killer cells, and all monocyte subpopulations, and increased CD33% as a neutrophil marker and HLA DR+ lymphocytes %, CD14+ CD16− Classical monocyte subset, CD36+ HLA DR+, and CD36+ CD16− in patients with advanced stages of HCC.
Funding
We don’t receive any financial support in this work.
Disclosure
The authors declare that there are no competing interests associated with this work.
References
1. Ganne-Carrié N, Nahon P. Hepatocellular carcinoma in the setting of alcohol-related liver disease. J Hepatol. 2019;70:284.
2. Mahmud N, Fricker Z, Hubbard RA, et al. Risk prediction models for post-operative mortality in patients with cirrhosis. Hepatology. 2021;73:204. doi:10.1002/hep.31558
3. Llovet JM, Villanueva A, Marrero JA, et al. Trial design and endpoints in hepatocellular carcinoma: AASLD consensus conference. Hepatology. 2021;73(Suppl 1):158. doi:10.1002/hep.31327
4. Kanwal F, Singal AG. Surveillance for hepatocellular carcinoma: current best practice and future direction. Gastroenterology. 2019;157:54. doi:10.1053/j.gastro.2019.02.049
5. Villanueva A. Hepatocellular carcinoma. N Engl J Med. 2019;380:1450.
6. Biswas SK, Mantovani A. Macrophage plasticity and interaction with lymphocyte subsets: cancer as a paradigm. Nat Immunol. 2010;11(10):889–896. PMID: 20856220. doi:10.1038/ni.1937
7. Morvan MG, Lanier LL. NK cells and cancer: you can teach innate cells new tricks. Nat Rev Cancer. 2016;16(1):7–19. PMID: 26694935. doi:10.1038/nrc.2015.5
8. Guillerey C, Smyth MJ. NK cells and cancer immunoediting. Curr Top Microbiol Immunol. 2016;395:115–145. PMID: 26025472. doi:10.1007/82_2015_446
9. Atkins D, Ross D, Kelley M. Acting in the face of uncertainty. Ann Intern Med. 2014;161:300.
10. Wolf E, Rich NE, Marrero JA, et al. Use of hepatocellular carcinoma surveillance in patients with cirrhosis: a systematic review and meta-analysis. Hepatology. 2021;73(2):713. doi:10.1002/hep.31309
11. Koteish A, Thuluvath PJ. Screening for hepatocellular carcinoma. J Vasc Interv Radiol. 2002;13(9 Pt 2):S185–S190. doi:10.1016/S1051-0443(07)61785-0
12. Borzio M, Borzio F, Macchi R, et al. The evaluation of fine-needle procedures for the diagnosis of focal liver lesions in cirrhosis. J Hepatol. 1994;20:117–121. doi:10.1016/S0168-8278(05)80477-5
13. Torzilli G, Belghiti J, Makuuchi M. Differences and similarities in the approach to hepatocellular carcinoma between Eastern and Western institutions. Liver Transpl. 2004;10(2 Suppl 1):S1–S2. doi:10.1002/lt.20032
14. Bismuth H, Majno PE, Adam R. Liver transplantation for hepatocellular carcinoma. Semin Liver Dis. 1999;19:311–322. doi:10.1055/s-2007-1007120
15. Heimbach JK, Kulik LM, Finn RS, et al. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology. 2018;67(1):358–380. doi:10.1002/hep.29086
16. Child CG, Turcotte JG. Surgery and portal hypertension. Major Probl Clin Surg. 1964;1:1–85. doi:10.1016/S0011-3840(64)80003-4
17. Kamarajah S, Frankel T, Sonnenday C, Cho C, Nathan H. Critical evaluation of the American Joint Commission on Cancer (AJCC) 8th edition staging system for patients with Hepatocellular Carcinoma (HCC): a Surveillance, Epidemiology, End Results (SEER) analysis. J Surg Oncol. 2017;117. doi:10.1002/jso.24908
18. Llovet JM, Brú C, Bruix J. Prognosis of hepatocellular carcinoma: the BCLC staging classification. Semin Liver Dis. 1999;19(3):329–338. doi:10.1055/s-2007-1007122
19. Hwang J, Kim SH, Lee MW, Lee JY. Small (≤ 2 cm) hepatocellular carcinoma in patients with chronic liver disease: comparison of gadoxetic acid-enhanced 3.0 T MRI and multiphasic 64-multirow detector CT. Br J Radiol. 2012;85(1015):e314–e322. doi:10.1259/bjr/27727228
20. Omata M, Lesmana LA, Tateishi R, et al. Asian Pacific association for the study of the liver consensus recommendations on hepatocellular carcinoma. Hepatol Int. 2010;4:439–474. PMID:20827404. [PMC free article]. doi:10.1007/s12072-010-9165-7
21. Forner A, Vilana R, Ayuso C, et al. Diagnosis of hepatic nodules 20 mm or smaller in cirrhosis: prospective validation of the noninvasive diagnostic criteria for hepatocellular carcinoma. Hepatology. 2008;47:97–104. PMID: 18069697. doi:10.1002/hep.21966
22. Fouts TR, Bagley K, Prado IJ, et al. Balance of cellular and humoral immunity determines the level of protection by HIV vaccines in rhesus macaque models of HIV infection. Proc Natl Acad Sci U S A. 2015;112:E992–E999. doi:10.1073/pnas.1423669112
23. Uehata T, Iwasaki H, Vandenbon A, et al. Malt1-induced cleavage of regnase-1 in cd4(+) helper t cells regulates immune activation. Cell. 2013;153:1036–1049. doi:10.1016/j.cell.2013.04.034
24. Whiteside TL. Immune modulation of t-cell and nk (natural killer) cell activities by texs (tumour-derived exosomes). Biochem Soc Trans. 2013;41:245–251. doi:10.1042/BST20120265
25. Pearce EL, Poffenberger MC, Chang CH, Jones RG. Fueling immunity: insights into metabolism and lymphocyte function. Science. 2013;342:1242454. doi:10.1126/science.1242454
26. Qin S, Ma S, Huang X, Lu D, Zhou Y, Jiang H. Th22 cells are associated with hepatocellular carcinoma development and progression. Chin J Cancer Res. 2014;26:135–141. doi:10.3978/j.issn.1000-9604.2014.02.14
27. Makarova-Rusher OV, Medina-Echeverz J, Duffy AG, Greten TF. The yin and yang of evasion and immune activation in HCC. J Hepatol. 2015;62:1420–1429. doi:10.1016/j.jhep.2015.02.038
28. Fujiwara Y, Shiba H, Furukawa K, et al. Perioperative change in white blood cell count predicts outcome of hepatic resection for hepatocellular carcinoma. J Hepatobiliary Pancreat Sci. 2010;17(6):892–897. PMID: 20449611. doi:10.1007/s00534-010-0290-4
29. Sajadieh A, Mouridsen MR, Selmer C, Intzilakis T, Nielsen OW, Haugaard SB. Monocyte number associated with incident cancer and mortality in middle-aged and elderly community-dwelling danes. Eur J Cancer. 2011;47(13):2015–2022. doi:10.1016/j.ejca.2011.02.015
30. Cros J, Cagnard N, Woollard K, et al. Human CD14dim monocytes patrol and sense nucleic acids and viruses via TLR7 and TLR8 receptors. Immunity. 2010;33:375–386. doi:10.1016/j.immuni.2010.08.012
31. Cardoso CC, Matiollo C, Pereira CHJ, et al. Patterns of dendritic cell and monocyte subsets are associated with disease severity and mortality in liver cirrhosis patients. Sci Rep. 2021;11(1):5923. PMID: 33723292; PMCID: PMC7960697. doi:10.1038/s41598-021-85148-y
32. Hong YM, Yoon KT, Hwang TH, et al. Pretreatment peripheral neutrophils, lymphocytes and monocytes predict long-term survival in hepatocellular carcinoma. BMC Cancer. 2020;20:937. doi:10.1186/s12885-020-07105-8
33. Shen SL, Fu SJ, Huang XQ, et al. Elevated preoperative peripheral blood monocyte count predicts poor prognosis for hepatocellular carcinoma after curative resection. BMC Cancer. 2014;14:744. doi:10.1186/1471-2407-14-744
34. Jeon SH, Lee YJ, Kim HD, et al. Dynamic changes in peripheral blood monocytes early after anti-PD-1 therapy predict clinical outcomes in hepatocellular carcinoma. Cancer Immunol Immunother. 2022. doi:10.1007/s00262-022-03258-6
35. Buch AC, Patil A, Haldar N, et al. Relation of lymphocyte subsets and cytokines in different grades of alcoholic cirrhosis. J Clin Diagn Res. 2019;13(1):8–11. 4.
36. Wang F, Sun W, Xiao Q, et al. Peripheral T lymphocytes predict the severity and prognosis in patients with HBV-related acute-on-chronic liver failure. Medicine. 2021;100(5):e24075. doi:10.1097/MD.0000000000024075
37. Liu HZ, Deng W, Li JL, et al. Peripheral blood lymphocyte subset levels differ in patients with hepatocellular carcinoma. Oncotarget. 2016;7(47):77558–77564. PMID: 27813499; PMCID: PMC5363604. doi:10.18632/oncotarget.13041
38. Buch A, Kulkarni RS, Kulkarni SS, Bhandari P. Journey of natural killer cells and their role in liver diseases. J Clin Diagn Res. 2022;16(4):EE01–EE05.
39. Heiberg IL, Pallett LJ, Winther TN, Hogh B, Maini MK, Peppa D. Defective natural killer cell anti-viral capacity in paediatric HBV infection. Clin Exp Immunol. 2015;179:466–476. doi:10.1111/cei.12470
40. Jun W, Lewis L. Natural killer cells and cancer. Adv Cancer Res. 2003;90:127–156.
41. Abumrad N, Storch J. Role of membrane and cytosolic fatty acid binding proteins in lipid processing by the small intestine. Chapter 66. In: Physiology of the Gastrointestinal Tract. Vol. 2.
42. Alvin W. Martin, Diagnostic Immunohistochemistry.
43. Mantovani A, Allavena P, Sica A, Balkwill F. Cancer-related inflammation. Nature. 2008;454(7203):436–444. doi:10.1038/nature07205
44. Soucek L, Lawlor ER, Soto D, Shchors K, Swigart LB, Evan GI. Mast cells are required for angiogenesis and macroscopic expansion of Myc-induced pancreatic islet tumors. Nat Med. 2007;13:1211–1218. doi:10.1038/nm1649
45. Karin M. Nuclear factor-kappaB in cancer development and progression. Nature. 2006;441:431–436. doi:10.1038/nature04870
46. Liu M, Zhou J, Liu X, et al. Targeting monocyte-intrinsic enhancer reprogramming improves immunotherapy efficacy in hepatocellular carcinoma. Gut. 2020;69(2):365–379. PMID: 31076403. doi:10.1136/gutjnl-2018-317257
47. Mossanen JC, Tacke F. Role of lymphocytes in liver cancer. Oncoimmunology. 2013;2(11):e26468. PMID: 24498546; PMCID: PMC3906418. doi:10.4161/onci.26468
48. Sasaki A, Iwashita Y, Shibata K, Matsumoto T, Ohta M, Kitano S. Prognostic value of preoperative peripheral blood monocyte count in patients with hepatocellular carcinoma. Surgery. 2006;139(6):755–764.
49. Luo X, Zheng E, Wei L, et al. The fatty acid receptor CD36 promotes HCC progression through activating Src/PI3K/AKT axis-dependent aerobic glycolysis. Cell Death Dis. 2021;12(4):328. PMID: 33771982; PMCID: PMC7997878. doi:10.1038/s41419-021-03596-w
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prognostic Significance of Elevated Platelet Count (>200 x 10^9 per L) in BCLC Stages B and C of Hepatocellular Carcinoma: A Retrospective Multicenter Analysis
Munker S, Rodriguez I, Bernhart K, Ben Khaled N, Findik M, Siegmund LK, Ye L, Reiter FP, Roessler D, Nasseh D, Balcar L, Pomej K, Scheiner B, Weiss C, Pinter M, Seidensticker M, Mayerle J, Philipp AB, De Toni EN
Journal of Hepatocellular Carcinoma 2025, 12:855-864
Published Date: 5 May 2025