Back to Journals » Infection and Drug Resistance » Volume 17
Peripheral Blood CD8+T Cell as a Prognostic Biomarker for Hospitalised COVID-19 Patients Without Antiviral Treatment
Authors Sun Y, Liu P, Zhang L, Lei S, Gao Q
Received 7 September 2023
Accepted for publication 14 December 2023
Published 12 January 2024 Volume 2024:17 Pages 109—117
DOI https://doi.org/10.2147/IDR.S432283
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Yuming Sun,1– 6,* Peilin Liu,7,* Lifang Zhang,8 Shaorong Lei,1 Qian Gao7
1Department of Plastic and Cosmetic Surgery, Xiangya Hospital, Central South University, Changsha, People’s Republic of China; 2National Engineering Research Centre of Personalized Diagnostic and Therapeutic Technology, Xiangya Hospital, Central South University, Changsha, People’s Republic of China; 3Furong Laboratory, Central South University, Changsha, People’s Republic of China; 4Hunan Key Laboratory of Skin Cancer and Psoriasis, Hunan Engineering Research Centre of Skin Health and Disease, Xiangya Hospital, Central South University, Changsha, People’s Republic of China; 5National Clinical Research Centre for Geriatric Disorders, Xiangya Hospital, Central South University, Changsha, People’s Republic of China; 6Department of Dermatology, Xiangya Hospital, Central South University, Changsha, People’s Republic of China; 7Clinical Laboratory Department, Xiangya Hospital, Central South University, Changsha, People’s Republic of China; 8Department of Plastic and Cosmetic Surgery, Changsha Mylike Cosmetic Hospital, Changsha, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Qian Gao; Shaorong Lei, Email [email protected]; [email protected]
Background: The status of T lymphocyte subset counts in patients with COVID-19 remains uncertain. This study aimed to assess alterations in peripheral blood CD3+CD8+T (CD8+T) cells among hospitalized COVID-19 patients who have not received antiviral treatment and to evaluate their prognostic value within this patient population.
Methods: A single-center, retrospective cohort study and a meta-analysis were conducted. The cohort study was performed at Xiangya Hospital from December 5, 2022, to January 31, 2023. We conducted a meta-analysis to explore the association between peripheral blood CD3+CD8+T cells and mortality in COVID-19 patients who did not receive antiviral therapy. All relevant studies in Embase, PubMed, Web of Science databases were systematically searched for meta-analysis.
Results: The retrospective cohort study included 201 patients. A significant decrease in peripheral blood CD8+ T cell count was found to be associated with an increased risk of mortality (adjusted odds ratio [aOR]: 13.88; 95% confidence interval [CI]: 3.15– 61.23), after adjusting for gender, age, comorbidities, severity at admission, steroid therapy, and antibiotic therapy. The threshold value for CD8+T cell counts, determined by the receiver operating characteristic (ROC) curve analysis, was 145.5 (area under the curve [AUC]: 0.828, specificity: 90.3%, sensitivity: 72.9%, P< 0.001). Additionally, A total of 7 studies with 2765 participants were included in the meta-analysis. The meta-analysis reveals a significant association between lower CD8+ T cell counts and mortality (odds ratio [OR] = 3.543, 95% CI: 1.726 to 7.272; I2=93%).
Conclusion: Peripheral blood CD8+ T cell can serve as a valuable prognostic biomarker for hospitalized patients who do not receive antiviral treatment.
Keywords: peripheral blood CD3+CD8+T cell, prognostic biomarker, hospitalised COVID-19 patients
Introduction
Since December 2019, the coronavirus disease 2019 (COVID-19) pandemic caused by the novel coronavirus SARS-CoV-2 has imposed a substantial global public health burden, resulting in over 6.89 millions deaths to data.1 As the pandemic persists, the virus undergoes continuous genome mutation and reassortments, potentially influencing its infectivity, transmission, and pathogenicity.2 Currently, the dominant variant, Omicron strain, displays the concerning ability to evade neutralizing antibodies.3 Consequently, the focus has shifted from solely presenting infections prevention to effectively reducing the incidence of severe cases and mortality rates in managing pandemic.4
The adaptive immunity response plays a crucial role in the pathogenesis, progression, and prognosis of COVID-19 patients.5,6 CD3+CD8+T (CD8+T) cells, as a fundamental component of adaptive immunity, exhibit vital functions in eliminating virus-infected cells and producing effector cytokines.6,7 However, despite three years having elapsed since the first reported COVID-19 case, with Omicron strain of the SARS-CoV-2 virus emerge and spread, it remains to be concerned regarding potential alterations in T lymphocyte subset counts in COVID-19 patients. Although the World Health Organization recommends various antiviral drugs for COVID-19 treatment,8 the global demand often surpasses the available supply. Therefore, further clinical evidence is needed to confirm the association between CD8+T cells and mortality risk, enabling the identification of high-risk COVID-19 patients for early access to antiviral treatment, ultimately improving survival rates and optimizing drug utilization.
In this study, we present a comprehensive summary of the latest clinical research data from COVID-19 patients who did not receive antiviral treatment. Additionally, we employ a meta-analysis approach to systematically investigate CD8+ T cells as potential biomarkers for predicting mortality risk in this specific patient population. The findings of this study provide valuable insights to a better understanding of COVID-19 patients and contribute guidelines for early clinical diagnosis, treatment and the improvement of patient’s prognosis.
Methods
Study Population
We performed a retrospective, single-center cohort study at Xiangya hospital from December 5, 2022 to January 31, 2023. The study was conducted with strict inclusion, included hospitalized patients who 1) were hospitalized patients with positive real-time fluorescent Polymerase Chain Reaction (RT-PCR) for SARS-CoV-2 infection; 2) age 18 years and above; 3) did not receive antiviral treatment; and 4) with outcome of peripheral blood T lymphocyte subsets test by flow cytometry (BD, USA). Patients who younger than 18 years, with oral antiviral drug and no flow cytometry measurement were excluded. Our research has been approved by the institutional review committee of Xiangya hospital, Central South University (202,002,024). No informed consent was required for this retrospective cohort, anonymized study. In addition, we conducted a meta-analysis to explore the association between peripheral blood CD3+CD8+T cells and mortality in COVID-19 patients who did not receive antiviral therapy.
Data Collection and Search Strategy
We retrieved electronic health records of COVID-19 patients from the inpatient system of Xiangya Hospital, which included demographic characteristics, admission date, time from symptom onset to admission, pre-existing conditions, prescription and drug dispensing records, laboratory tests, ICU admission, and date of discharge or death. Collected data were recorded consecutively until the planned time point. All data were anonymously collected by experienced researchers.
The meta-analysis was conducted according to the PRISMA guidelines (Preferred reporting items for systematic reviews and meta-analyses).9 We systematically searched Embase, PubMed, Web of Science databases for all related literature works. The final search was updated on November 11, 2023, using the terms “COVID-19”, “SARS-CoV-2”, “CD8-Positive T-Lymphocytes”, “CD8+T cell”. The publication language was restricted to Chinese and English. The original and review articles were manually identified, and the references that met the requirements were included in this study.
Statistical Analysis
Continuous variables were shown as median and interquartile range (IQR), and compared by the Mann–Whitney test since most laboratory data was with skewed distribution. Categorical variables were presented as counts and proportions, and compared by Chi-square test or Fisher’s exact test. The logistic regression model was used to eliminate the impact of confounding variables. We adopted ROC curve to find the warning values of CD8+ T cell to predict in-hospital death. The reference range of normal CD8+ T cell was based on the standard of Xiangya Hospital (5).
Meta Analysis
The studies were eligible if they adhered to the following criteria: (1) publication in English language, (2) studies including associations between peripheral blood CD8+T cells and mortality, (3) recruit patients with COVID-19 and without any antiviral treatment. Two authors (YM S and PL L) independently performed the literature search and data extraction according to the inclusion criteria. All disputes between the two authors were resolved by discussion with the third author (LF Z). Studies selection is based on title and abstract, with full text reviewed as necessary. The following data were extracted from studies that met the inclusion criteria: countries of the studies, number of participants, time period, the counts of peripheral blood lymphocyte and its subsets. We performed a meta-analysis to summarized the results as odds ratio and 95% confidence interval2 was used to assess heterogeneity among included studies, and we choose a random effect model to combine the results to reduce the influence of heterogeneity. All statistical analyses were performed with SPSS (version 26.0, IBM), and R (version 4.3.0). The level of significance was two-tailed 0.05 for statistical tests.
Results
Demographic and Clinical Characteristics of Hospitalized COVID-19 Patients Without Antiviral Treatment
A total of 2118 hospitalized patients with confirmed SARS-CoV-2 infection were consecutively collected, and 201 patients fulfilled the inclusion criteria and were included in the final analysis (Figure 1). Among them, there were 129 males and 72 females, with a mean age of 68.0. The most common symptoms reported by the patients were dry cough (82.1%), expectoration (68.7%) and fever (61.7%). Hypertension was the most frequent preexisting condition, observed in 42.3% of the patients. Upon admission, majority of the patients presented with a severe condition (66.7%). Moreover, 73.6% patients received nasal cannula oxygen support and antibiotics treatment. Detailed clinical characteristics are provided in Table 1.
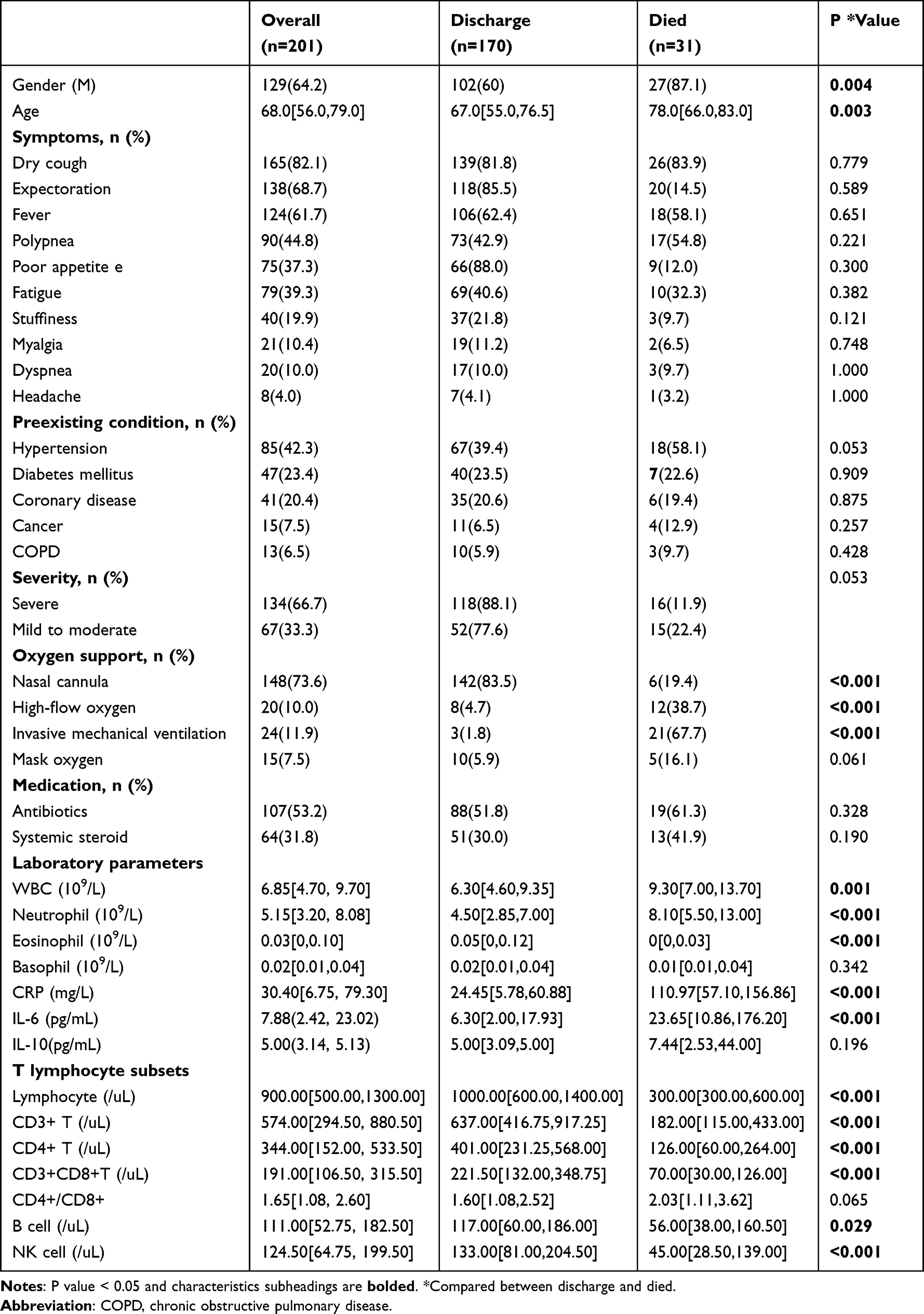 |
Table 1 Characteristics of Included Patients |
 |
Figure 1 Flowchart of patient recruitment. |
During the hospitalization period, a total of 31 patients unfortunately died. As shown in Table 1, the deceased patients were older than those who were discharged (P<0.05), and there was a higher proportion of males in the died group (P<0.05). Oxygen support via nasal cannula was more prevalent among the discharged group, whereas a greater number of patients in died group required high-flow oxygen or invasive mechanical ventilation (P<0.001). Significant difference was also observed in various laboratory parameters, including WBC, Neutrophil, Eosinophil, CRP, IL-6. The median values of Lymphocyte, CD3+ T-cell, CD4+ T-cell, CD8+ T-cell, B-cell, and NK-cell in the died group were notably lower compared to the discharged group (P<0.05). Moreover, the median concentration of CRP and IL-6 in the deceased patients was nearly four times higher than that in the discharged patients.
Correlation Between Peripheral Blood CD8+T Cell Count and Mortality Risk in Hospitalized COVID-19 Patients Without Antiviral Treatment
Next, our analysis demonstrated a significant correlation between a decrease in CD8+T cell count in peripheral blood and an increased the risk of mortality. This association was significant after adjusting for factors such as adjusted for gender, age, comorbidities, and severity at admission, steroid therapy, antibiotic therapy (adjusted odds ratio aOR: 13.88; 95% confidence interval CI: 3.15–61.23). The receiver operating characteristic (ROC) curve analysis revealed a threshold value of 145.5 for CD8+T cell counts, with an area under the curve (AUC) of 0.828, a specificity of 90.3%, and a sensitivity of 72.9% (P<0.001) (Figure 2).
 |
Figure 2 The receiver operating characteristic (ROC) curve analysis revealing the threshold value for CD8+T cell counts. |
We conducted a meta-analysis to further validate the associations between peripheral blood CD8+T cells and mortality. The latest version of the PRISMA flowchart shows the literature screening process used in our report (Figure 1). A total of 4209 potentially relevant studies were identified in the literature search, and finally seven studies were collected for further analysis.5,10–14 The basic characteristic of the included literatures is presented in Table 2. The included literatures comprise 2765 individuals, which are published between 2019 to 2023, and conducted in the China and Spain. The pooled analysis consistently demonstrated a significant association between lower CD8+T cell counts and mortality risk (odds ratio OR =3.543, 95% CI: 1.726 to 7.272; I2=93%) (Figure 3).
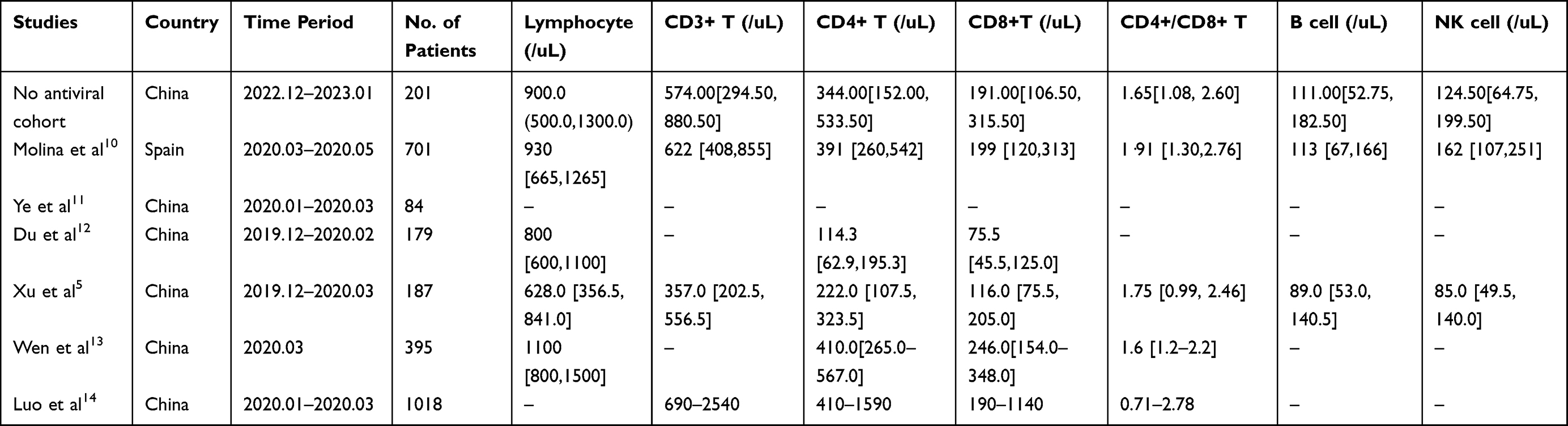 |
Table 2 Characteristics of the Included Studies |
 |
Figure 3 Forest plot showing the association of lower CD8+T cells with death in COVID-19 patients. Subheadings and significant results are bolded. |
Discussion
This study provides a concise overview of the clinical characteristics of 201 COVID-19 patients who did not receive antiviral treatment, incorporating a meta-analysis of five studies. Surprisingly, a significant decrease in peripheral blood CD8+ T cell count was observed, emerging as a significant predictor of mortality risk in COVID-19 patients without antiviral treatment.
Peripheral blood CD8+ T cell have been implicated in predicting the prognosis of various diseases, including untreated extensive small cell lung cancer, infection event in patients undergoing peritoneal dialysis, and the risk and mortality of critically ill immunocompromised patients with invasive pulmonary aspergillosis.15–18 Multiple studies have reported a significant reduction in T lymphopenia subsets, especially CD8+ T cell.19,20 In our study, both multivariate logistic regression and meta-analysis confirmed that decreased counts of peripheral blood CD8+ T cells were significantly associated with death in patients without antiviral therapy. This finding not only assigns a new role to CD8+ T cells in disease prediction but also establishes them as a new reliable peripheral blood biological marker for preventing COVID-19 death and critical illness.
Moreover, it is worth noting that CD8+ cells play a critical role in antiviral defense and targeted elimination of infected cells.21–23 Therefore, we speculate that the increased risk of death in COVID-19 patients with a low proportion of peripheral blood CD8+ T cells may be attributed to compromised immunity and reduced anti-infective ability. Further investigations, both at the cellular and molecular levels, are needed to elucidate the specific mechanism involved.
To our knowledge, this is the first study that compared the levels of T lymphocyte subsets in COVID-19 patients at different infectious periods, and through Meta-analysis to explore the association between CD8+ T cells and death in patients with COVID-19. Our research has some unavoidable limitations. First, it was a retrospective and single center study, which would affect the reliability of the data, whereas the meta-analysis outcome is consistent with our conclusion. Second, the association of other T cell subsets and laboratory indicators with COVID-19 patient outcomes was not explored. Last, the specific reason for hospitalization of mild to moderate cases of COVID-19 is not clear and lack the documentation of duration of symptoms and time of sample collection. Multi-Centre clinical studies with larger samples and long follow-up are needed in the future.
In conclusion, peripheral blood CD8+T cell can act as a prognostic biomarker for hospitalized patients without antiviral treatment, which may help physicians identify high-risk patients as soon as possible, provide early antiviral treatment and improve drug utilization.
Ethical Approval
This research was carried out in compliance with the recommendations of the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Because this study was retrospective and did not require additional medical procedures. Our research has been approved by the institutional review committee of Xiangya hospital, Central South University (202002024), and an exemption for informed consent was obtained from our Investigational Ethical Review Board.
Acknowledgments
We thank all the hospital staff members for their efforts in collecting the information that used in this study; thank the patients who participated in this study, their families, and the medical, nursing, and research staff at Xiangya Hospital of Central South University.
We appreciate Professor Jian Zhang’s support throughout the paper writing, editing, and submission process.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China (Grant Nos. 82102803, 82272849 to GD), National Natural Science Foundation of Hunan Province (Grant Nos. 2021JJ40976 to GD) and National Natural Science Foundation of China (Grant Nos. 8197081674 to SR L.).
Disclosure
The authors declare no conflicts of interest that pertain to this work.
References
1. Dong E, Ratcliff J, Goyea TDCOVID-19 Dashboard by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU). Johns Hopkins University; 2021.
2. Hirotsu Y, Maejima M, Shibusawa M, et al. Classification of omicron BA.1, BA.1.1, and BA.2 sublineages by TaqMan assay consistent with whole genome analysis data. Int J Infect Dis. 2022;122:486–491. doi:10.1016/j.ijid.2022.06.039
3. Cheung AT, Ho LLK, Li WHC, Chung JOK, Smith GD. Psychological distress experienced by nurses amid the fifth wave of the COVID-19 pandemic in Hong Kong: a qualitative study. Front Public Health. 2022;10:1023302. doi:10.3389/fpubh.2022.1023302
4. Mefsin YM, Chen D, Bond HS, et al. Epidemiology of infections with SARS-CoV-2 omicron BA.2 variant, Hong Kong, January-March 2022. Emerg Infect Dis. 2022;28(9):1856–1858. doi:10.3201/eid2809.220613
5. Xu B, Fan CY, Wang AL, et al. Suppressed T cell-mediated immunity in patients with COVID-19: a clinical retrospective study in Wuhan, China. J Infect. 2020;81(1):e51–e60. doi:10.1016/j.jinf.2020.04.012
6. Sette A, Crotty S. Adaptive immunity to SARS-CoV-2 and COVID-19. Cell. 2021;184(4):861–880. doi:10.1016/j.cell.2021.01.007
7. Rha MS, Shin EC. Activation or exhaustion of CD8(+) T cells in patients with COVID-19. Cell Mol Immunol. 2021;18(10):2325–2333. doi:10.1038/s41423-021-00750-4
8. Lamontagne F, Stegemann M, Agarwal A, et al. A living WHO guideline on drugs to prevent covid-19. BMJ. 2021;372:n526. doi:10.1136/bmj.n526
9. Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ. 2009;339:b2700.
10. Cantenys-Molina S, Fernandez-Cruz E, Francos P, Lopez Bernaldo D, Quiros JC, Munoz P. Lymphocyte subsets early predict mortality in a large series of hospitalized COVID-19 patients in Spain. Clin Exp Immunol. 2021;203(3):424–432. doi:10.1111/cei.13547
11. Ye H, Liu ZM, Zhou L, et al. Levels of peripheral IL-6 and CD4+ and CD8+ T cells and their prognostic significance in COVID-19. Eur Rev Med Pharmacol Sci. 2023;27(6):2686–2691. doi:10.26355/eurrev_202303_31806
12. Du RH, Liang LR, Yang CQ, et al. Predictors of mortality for patients with COVID-19 pneumonia caused by SARS-CoV-2: a prospective cohort study. Eur Respir J. 2020;55(5):2000524. doi:10.1183/13993003.00524-2020
13. Wen XS, Jiang D, Gao L, et al. Clinical characteristics and predictive value of lower CD4(+)T cell level in patients with moderate and severe COVID-19: a multicenter retrospective study. BMC Infect Dis. 2021;21(1):57. doi:10.1186/s12879-020-05741-w
14. Luo M, Liu J, Jiang W, Yue S, Liu H, Wei S. IL-6 and CD8+ T cell counts combined are an early predictor of in-hospital mortality of patients with COVID-19. JCI Insight. 2020;5(13). doi:10.1172/jci.insight.139024
15. Li Z, Chen G, Cai Z, et al. Genomic and transcriptional profiling of tumor infiltrated CD8(+) CD8 +T cells revealed functional heterogeneity of antitumor immunity in hepatocellular carcinoma. Oncoimmunology. 2019;8(2):e1538436. doi:10.1080/2162402X.2018.1538436
16. An N, Wang H, Jia W, et al. The prognostic role of circulating CD8(+) T cell proliferation in patients with untreated extensive stage small cell lung cancer. J Transl Med. 2019;17(1):402. doi:10.1186/s12967-019-02160-7
17. Jiao X, Cao X, Zou J, Ji J, Ding X, Yu X. The proportion of memory cd8+ t cell predicts infection event in patients with peritoneal dialysis. Kidney Blood Press Res. 2022;47(11):674–682. doi:10.1159/000526207
18. Cui N, Wang H, Long Y, Liu D. CD8(+) T-cell counts: an early predictor of risk and mortality in critically ill immunocompromised patients with invasive pulmonary aspergillosis. Crit Care. 2013;17(4):R157. doi:10.1186/cc12836
19. Mirsharif ES, Chenary MR, Bozorgmehr M, et al. Immunophenotyping characteristics of COVID-19 patients: peripheral blood CD8+ HLA-DR+ T cells as a biomarker for mortality outcome. J Med Virol. 2023;95(1):e28192. doi:10.1002/jmv.28192
20. Tan M, Liu Y, Zhou R, et al. Immunopathological characteristics of coronavirus disease 2019 cases in Guangzhou, China. Immunology. 2020;160(3):261–268. doi:10.1111/imm.13223
21. Santos-Zas I, Lemarie J, Zlatanova I, et al. Cytotoxic CD8(+) T cells promote granzyme B-dependent adverse post-ischemic cardiac remodeling. Nat Commun. 2021;12(1):1483. doi:10.1038/s41467-021-21737-9
22. Li M, Guo W, Dong Y, et al. Elevated exhaustion levels of NK and CD8(+) T cells as indicators for progression and prognosis of COVID-19 disease. Front Immunol. 2020;11:580237. doi:10.3389/fimmu.2020.580237
23. Reina-Campos M, Scharping NE, Goldrath AW. CD8(+) T cell metabolism in infection and cancer. Nat Rev Immunol. 2021;21(11):718–738. doi:10.1038/s41577-021-00537-8
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.