")
Back to Journals » OncoTargets and Therapy » Volume 12
Perioperative Targeted Therapy Or Immunotherapy In Non-Small-Cell Lung Cancer
Authors Sa H, Song P , Ma K, Gao Y, Zhang L, Wang D
Received 10 July 2019
Accepted for publication 20 September 2019
Published 3 October 2019 Volume 2019:12 Pages 8151—8159
DOI https://doi.org/10.2147/OTT.S222412
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sanjay Singh
Huanlan Sa,1,* Peng Song,2,* Kewei Ma,3 Yong Gao,1 Li Zhang,2 Deqiang Wang1
1Department of Pain Management, Affiliated Hospital of Binzhou Medical University, Binzhou 256603, People’s Republic of China; 2Department of Respiratory Medicine, Peking Union Medical College Hospital, Chinese Academy of Medical Science & Peking Union Medical College, Beijing 100010, People’s Republic of China; 3Department of Oncology, Cancer Center, The First Hospital of Jilin University, Changchun, 130021, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Li Zhang
Department of Respiratory Medicine, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing 100730, People’s Republic of China
Tel +8618811630866
Email [email protected]
Deqiang Wang
Department of Pain Management, Affiliated Hospital of Binzhou Medical University, Binzhou 256603, People’s Republic of China
Tel +8615066918983
Email [email protected]
Abstract: Targeted therapy and immunotherapy have changed the treatment modes for advanced non-small cell lung cancer (NSCLC), moving from second-line to first-line treatment and significantly extending patients’ survival. Surgery and chemoradiotherapy remain the main treatment options for patients with locally advanced lung cancer, but recurrence and metastasis still occur in some patients. The survival rates of conventional perioperative chemotherapy among NSCLC patients have increased by only 5%. Therefore, more studies have begun to explore targeted and immune neoadjuvant/adjuvant therapies in early-stage and locally advanced NSCLC, and the relevant clinical research data have shown good efficacy and safety profiles. This article summarizes several clinical studies of critical importance.
Keywords: non-small-cell lung cancer, targeted therapy, immunotherapy
Introduction
Lung cancer has the highest incidence and mortality among all cancers worldwide. According to the GLOBOCAN2018 report released in 2018, approximately 2.09 million new cases and 1.76 million deaths from lung cancer are estimated to occur globally each year, accounting for 11.6% and 18.4%, respectively.1 Non-small cell lung cancer (NSCLC) accounts for approximately 80%–85% of lung cancer cases. NSCLC is the most common lung cancer, and approximately one third of the patients are at the local progressive stage (stage III) at the time of diagnosis.2 The 5-year survival rates for stage IA and III lung cancer patients are 80% and 20%, respectively, and most patients have postoperative recurrence. Surgical resection combined with postoperative adjuvant chemoradiotherapy remains the primary treatment mode for locally advanced NSCLC. However, a meta-analysis revealed that the 5-year survival rate of patients with perioperative platinum-based chemotherapy was only 5% higher than that of the surgery-only group, and more than 60% of patients experienced grade 3–4 toxic reactions, causing delayed treatment and drug withdrawal.3–6 Therefore, novel neoadjuvant/adjuvant therapies to improve patient prognoses are urgently needed. In recent years, the high efficacy and low toxicity of targeted therapy and immunotherapies have provided novel avenues for lung cancer treatment, especially advanced lung cancer, and have achieved continuous improvement from second-line to first-line treatment. To improve the survival rate of patients in early-stage and locally advanced NSCLC, appropriate clinical studies are being conducted. Continuous publication of research data has opened a new chapter regarding treatment modes for early-stage and locally advanced lung cancer. This article reviews clinical research on targeted therapy and immunotherapy for perioperative lung cancer.
Targeted Therapy
Epidermal growth factor receptor (EGFR)-tyrosine kinase inhibitors (TKIs) have significantly extended progression-free survival (PFS) in advanced EGFR-positive NSCLC patients, compared with platinum-based chemotherapy.7,8 The EGFR mutation rate of NSCLC patients in the United States is 10%, and is as high as 35% in eastern Asian patients9,10 The EGFR-TKI-targeted therapy mode may clinically benefit these patients. Case reports and small-scale non-randomized clinical trials have demonstrated the potential efficacy of neoadjuvant EGFR-TKI in treating resectable NSCLC.11–15 However, the efficacy and safety of EGFR-TKI in neoadjuvant/adjuvant therapy for NSCLC remain unclear. The following is a brief overview of several recent clinical studies on perioperative targeted therapy for lung cancer.
Neoadjuvant Targeted Therapy
Neoadjuvant therapy is mainly targeted at patients in the IIIA-N2 stage, but owing to the heterogeneity of IIIA-N2 NSCLC, the overall prognosis is poor, and selecting a treatment regimen is controversial in clinical practice. In one study, 50 patients with stage I/II NSCLC who received Gefitinib for 3 weeks prior to surgery were included in a clinical trial related to tumor regression after oral Gefitinib treatment. The objective remission rate was 42%, and treatment was effective in 21 patients, including 17 with EGFR mutations and 4 with wild-type EGFR. Imaging assessment showed that tumor size was reduced by approximately 25%.16
EMERGING (CTONG1103)17 was a randomized phase II clinical trial led by Yilong Wu and Wenzhao Zhong of Guangdong Province People’s Hospital, which was the first to apply randomized controlled research methods to compare the efficacy and safety of neoadjuvant EGFR-TKI with platinum-based double-medicine chemotherapy in stage IIIA N2 NSCLC patients. After eight years, the findings were published in the Journal of Clinical Oncology on June 13, 2019. The treatment reduced the risk of recurrence of stage IIIA N2 NSCLC by 61%, and progression-free survival (PFS) was extended by 10.1 months. In this study, 72 patients with stage IIIA-N2 who were confirmed as EGFR-mutation-positive before surgery were included and randomly divided into two groups: one group received Erlotinib treatment (42 days neoadjuvant+1 year adjuvant therapy), while the other group received Gemcitabine + Cisplatin chemotherapy (2 cycles of neoadjuvant/adjuvant therapy) and surgical treatment after induction therapy. The primary endpoint was the objective response rate (ORR) of the preoperative induction therapy, and despite the fact that the ORR value in the Erlotinib group was objectively better to that of the chemotherapy group (54.1% vs 34.3%), there was no statistical significance (P=0.092). After neoadjuvant therapy, the rates of complete resection in the Erlotinib and chemotherapy groups were 73% and 63%, and the rates of descending lymph nodes were 10.8% and 2.9%, respectively. No patient in either group achieved pathological complete remission (pCR). Compared with the chemotherapy group, the Erlotinib group had significantly prolonged PFS (11.4 and 21.5 months, respectively; hazard ratio [HR] 0.39; 95% confidence interval [95% CI, 0.23–0.67; P<0.001). The median overall survival (OS) was 32.5 months, and the median OS of the Erlotinib and chemotherapy groups were 45.8 and 39.2 months, respectively (HR 0.77; 95% CI. 0.41–1.45, P=0.417). These results were not statistically significant, but conclusions can be reached only after follow up. In terms of safety, the incidence of grade 3–4 adverse reactions in the Erlotinib group was much lower than that in the chemotherapy group.
The ESTERN study18 was a single-arm, single-center, phase II study evaluating the efficacy and safety of Erlotinib as neoadjuvant treatment in patients with Endobronchial ultrasonography (EBUS) confirmed stage IIIA N2 NSCLC with an activated EGFR mutation on exon 19 or 21. The primary endpoint of the study was radical resection rate. Patients received Erlotinib at 150 mg/day. Treatment was continued for 8 weeks or until disease progression or unacceptable toxicities. Sixteen patients underwent radical surgery, and the complete resection rate was 93.8% (15/16).
The FLAURA study19 found that in advanced first-line treatment of EGFR-positive NSCLC, Osimertinib significantly extended PFS by 8.7 months (18.9 vs 10.2, HR=0.46) compared with the standard treatment EGFR-TKI (Erlotinib or Gefitinib). The median treatment time for Osimertinib and the standard treatment were 16.2 months and 11.5 months respectively. The toxicity and adverse effects of the two were similar, and Osimertinib was better tolerated. We plan to explore the efficacy of Osimertinib in neoadjuvant therapy of early-stage NSCLC (ChiCTR1800016948,20 NCT0343346921 [Table1]).
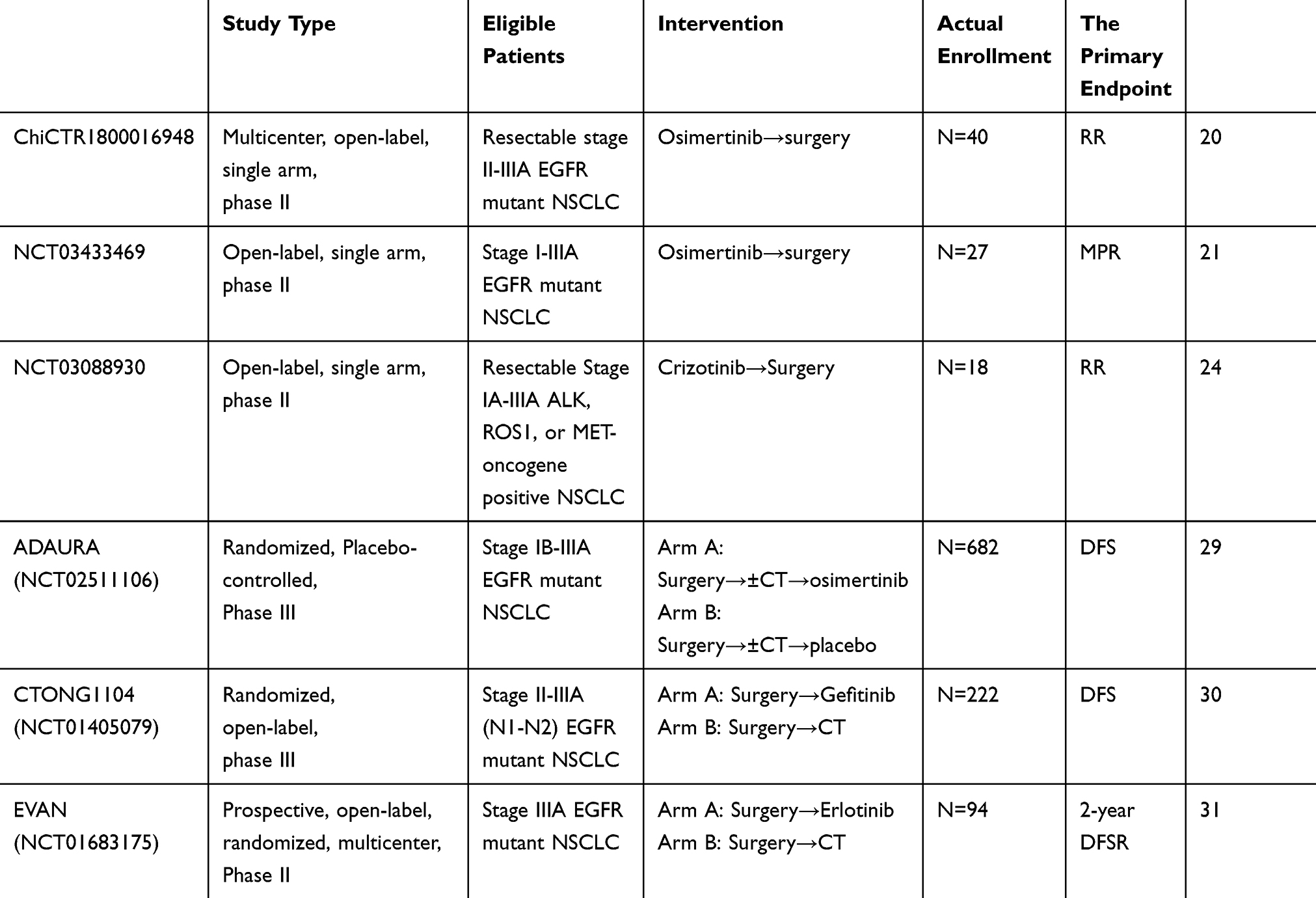 |
Table 1 The Major Trials Of Neoadjuvant/Adjuvant Targeted Therapies In Early-Stage And Locally Advanced NSCLC |
Anaplastic lymphoma kinase (ALK) is another important driver gene in NSCLC, with a mutation incidence of 3%–7%.22 ALK inhibitors can significantly improve the prognoses of patients with advanced ALK-positive NSCLC, but as a neoadjuvant therapy, high-level evidence is lacking. Wenzhao Zhong’s team at Guangdong Province People’s Hospital reviewed the curative effect of neoadjuvant therapy in patients with locally advanced ALK-positive NSCLC,23 including 11 patients diagnosed with locally advanced ALK-positive NSCLC, including 10 cases of partial response (PR), 2 cases of pathologic complete response (pCR), and 3 cases that reached the lymph node pathological drop period. All patients successfully underwent surgery after neoadjuvant therapy. In addition, 5 patients with recurrence achieved good results after continued treatment with Crizotinib. Although the sample size of this study was small, the study still suggests that Crizotinib is effective for neoadjuvant therapy.
A phase II trial is currently evaluating the efficacy of Crizotinib for induction therapy in participants with surgically resectable ALK rearrangement, ROS1 rearrangement, or MET exon 14 mutation-positive stage IA-IIIA NSCLC (NCT03088930)24 (Table 1). This neoadjuvant treatment will last 6 weeks, and on the last day that Crizotinib is administered, participants will undergo surgical resection, followed by 5 years of follow up.
Perioperative neoadjuvant-targeted therapy for NSCLC still faces many problems that require further exploration, such as the duration of treatment and length of time from drug withdrawal to surgery, how the optimum timing of surgery and mode of postoperative adjuvant therapy should be chosen, recurrence of postoperative problems and biomarker selection (NCT02804776)25 require further study. Therefore, further clinical trials regarding neoadjuvant-targeted therapy are needed.
Adjuvant-Targeted Therapy
The first randomized controlled study for postoperative EGFR-TKI was the BR19 study26 launched in 2002. However, because of the irrationality of the enrolled population, the trial was closed early, and no significant differences were found in either DFS or OS between the Gefitinib and placebo groups. The RADIANT study27 in 2006 randomized 973 patients with stage IB–IIIA NSCLC at a ratio of 2:1 into Erlotinib or placebo groups respectively, with the Erlotinib group receiving 150 mg/d with a 2-year treatment cycle. All enrolled patients were tested for EGFR mutations via immunohistochemistry or fluorescence in situ hybridization (FISH) and were stratified according to stage, pathological type, smoking status, EGFR expression status, early adjuvant chemotherapy, and country. The primary study endpoint was DFS, and the secondary study endpoint was DFS and OS of patients with positive EGFR mutations. No statistically significant differences were found in median DFS between the Erlotinib and placebo groups (HR=0.90, 95% CI: 0.74–1.10, P=0.324). In addition, subgroup analysis of EGFR-positive patients showed that DFS in the Erlotinib group was significantly longer than that of the placebo group (HR=0.61, 95% CI: 0.38–0.98, P=0.039), but no benefit was observed in OS (HR=1.09, 95% CI: 0.55–2.16). The main reasons for the negative results in this study were similar to those of the BR19 study, which included staging of the enrolled population and failure to detect EGFR mutations by currently recommended PCR or second-generation sequencing methods. However, analysis of these two studies reveals that only when an advantageous population is selected for adjuvant-targeted therapy can the greatest clinical benefit be obtained.
Subsequently, the SELECT study,28 launched in 2008, was the first TKI-adjuvant therapy study conducted in EGFR-mutant NSCLC patients, and the 2-year DFS rate of Erlotinib treatment reached 89%, confirming the efficacy of post-operative adjuvant-targeted therapy. The median follow-up time was 3.4 years. However, this was a one-arm study and as such efficacies cannot be compared. However, the duration of drug administration remains undefined, and prolonged drug administration reduces the recurrence rate but correspondingly increases the adverse effects caused by accumulated drug toxicity. The ADAURA study (NCT02511106)29 (Table 1) is expected to reveal the optimal EGFR-TKI duration.
In 2018, the ADJUVANT trial (CTONG 1104) (Table 1),30 led by Wu Yilong, was the first to compare targeted adjuvant treatment and post-operative adjuvant chemotherapy in a randomized controlled phase III clinical study. Participants included 222 patients with EGFR-mutation-positive stage II-IIIA NSCLC, who were randomly assigned, at a 1:1 ratio, into targeted therapy and chemotherapy groups. The targeted therapy groups received Gefitinib 250 mg/d for 2 years. The chemotherapy group received 25 mg/m2 Vinorelbine on days 1 and 8 and 75 mg/m2 Cisplatin on day 1, then every 21 days to conclude 1 cycle, for a total of 4 cycles. The median follow-up time was 36.5 months. Compared with the chemotherapy group, the median DFS in the targeted therapy group increased from 18.0 months to 28.7 months (HR=0.60, 95% CI: 0.42–0.87, P=0.0054). More importantly, the subgroup analysis found that N2 patients showed a significant benefit in DFS (HR=0.52, 95% CI, 0.34–0.80, P=0.003 2), while N1 patients showed no benefit (HR=0.89, 95% CI, 0.45–1.76, P=0.743). Moreover, the toxic and adverse effects in the Gefitinib group were significantly less than those of the chemotherapy group. Therefore, ADJUVANT demonstrated for the first time that post-operative adjuvant therapy can significantly improve the efficacy and reduce adverse effects in patients compared to traditional chemotherapy and confirmed that N2 patients benefit the most, which is a significant milestone.
EVAN research31 (Table 1) was the first randomized phase II study to compare the efficacy and safety of adjuvant treatment and chemotherapy in patients with EGFR mutations in stage IIIA NSCLC. The 2-year DFS rate of the Erlotinib group increased significantly (81.35% vs 44.62%, P<0.001) compared with that of the chemotherapy group, and the median DFS was extended from 21.0 to 42.4 months (HR=0.27, 95% CI, 0.14–0.53, P<0.001). OS data are not yet available. Six (12%) of the 50 patients in the Erlotinib group had grade 3 or more serious adverse events, while 11 (26%) of the 43 patients in the chemotherapy group had grade 3 or more serious adverse events. No treatment related deaths were reported. Most importantly, of all patients in EVAN who were in stage IIIA, only 3 patients did not have N2. Thus, the results of this study equaled those of the IIIAN2 period in patients with available test data. Therefore, patients in stage IIIAN2 will receive the most benefit from targeted therapy, which is consistent with the ADJUVANT trial results. Insufficient evidence exists for giving adjuvant-targeted therapy to N0 and N1 patients.
The ADJUVANT and EVAN studies opened a new chapter for adjuvant therapy for NSCLC and confirmed that adjuvant targeted therapy can benefit patients with EGFR-mutation-positive stage IIIA N2 NSCLC and provides the highest level of evidence for targeted therapy. Based on these studies, adjuvant targeted therapy of EGFR-TKI provides IB evidence for resectable EGFR-mutation-positive stage IIIA/IIIB (T3N2M0) NSCLC patients, and these are included in the latest targeted therapy for NSCLC in the Consensus of Chinese Thoracic Surgeons. However, no clear conclusions have been reached regarding targeted-adjuvant therapy for 1) selecting the optimum beneficiaries, 2) the appropriate research endpoint (DFS or OS), 3) the patients who will receive clinical benefits from DFS, and 4) duration of the targeted therapy. These questions must be continuously addressed.
Immunotherapy
Immunotherapy has moved from second-line to first-line treatment in advanced NSCLC. The current research focus has shifted to early-stage and locally advanced resectable NSCLC, and relevant studies have shown good efficacy and safety. Here, we review the relevant clinical studies in detail.
Neoadjuvant Immunotherapy
The CheckMate-159 study (Table 2),32 published in the New England Journal of Medicine in 2018, first explored the efficacy and safety of neoadjuvant immunotherapy for NSCLC. Twenty-one patients with untreated and resectable stage I–IIIA were included. The primary endpoints were safety and feasibility. Two patients were in PR, and 18 had stable disease (SD). All 20 underwent surgery and R0 resection, and 9 (45%) achieved major pathological remission (MPR; residual surviving tumor cells in postoperative specimens <10%). During follow up, the 20 patients who underwent radical surgery had a recurrence rate of 73% within 18 months, and an overall survival rate of 95%. MPR was significantly correlated with tumor mutation burden (TMB) before treatment but not with PD-L1 expression. Although this study had a small sample study, it showed the safety of neoadjuvant immunotherapy for NSCLC, in which the pCR of early-stage NSCLC after neoadjuvant chemotherapy increased from 4% to 15%, and the MPR increased from 20% to 45%, setting a precedent for neoadjuvant immunotherapy for lung cancer.32–34 The relevant data were updated again at the 2019 American Society of Clinical Oncology (ASCO) conference, with the median follow-up time standing at 34.6 months, but the median relapse-free survival (RFS) and OS have not yet been ascertained. Fifteen of the 20 surgically treated patients maintained DFS, and Kaplan-Meier analysis estimated a 24-month RFS rate of 69% (95% CI, 51%–93%). Compared with the untreated population, ctDNA clearance and peripheral blood T-cell amplification may be potential predictive markers for treatment response and monitoring recurrence.35 The long-term follow-up safety data further confirmed the feasibility and safety of Nivolumab for neoadjuvant therapy of resectable NSCLC.
 |
Table 2 Five Major Trials Of Neoadjuvant Immunotherapy In Early-Stage And Locally Advanced NSCLC |
The LCMC3 study is evaluating the safety and efficacy of neoadjuvant therapy with Atezolizumab in resectable stage IB-IIIB NSCLC patients, with MPR as the main study endpoint. Patients with the EGFR mutation or ALK fusion were excluded. Midterm analysis results were orally reported at the 2019 ASCO meeting (Table 2).36 Seventy-seven patients were included in the main efficacy observation data, and 101 patients were included in the safety data analysis. The MPR was 19% (15/77, 95% CI, 11%–30%), and the pCR was 5% (4/77). RECIST criteria were used to evaluate the results: 7% of patients had PR, and 89% had SD. MPR was associated with changes in tumor volume, which were not correlated with PD-L1 expression levels or TMB. Atezolizumab as neoadjuvant therapy was safe and well-tolerated, and the incidence of immune-related adverse reactions was 6% for ≥grade 3 patients.
NEOSTAR37 (Table 2) was another neoadjuvant phase II trial to compare the efficacy of Nivolumab and Nivolumab + Ipilumab in resectable NSCLC patients. Forty-four patients were enrolled (23 patients receiving Nivolumab alone and 21 receiving Nivolumab + Ipilumab). The results showed that the overall MPR rate was 24%, the overall MPR + pCR rate was 25% (monotherapy vs combination: 17% vs 33%), and 8 patients (18%) achieved pCR (monotherapy vs combination: 9% vs 29%). The overall ORR (CR+PR) of the RESICT study reached 20% (9/44; monotherapy vs combination: 22% vs 19%), and the ORR was positively correlated with the MPR (P<0.001). Subgroup analysis found that the PD-L1 expression level was related to ORR and MPR (P=0.024). Higher PD-L1 expression yielded greater benefits (which was inconsistent with the subgroup analysis results for Atezolizumab in the LCMC3 study). Combined immunotherapy increased the CD3+ cell frequency in tumor-infiltrating lymphocytes and enhanced intraoperative T-cell infiltration, diversity and reactivity-related functions. The study found no unacceptable toxicity or increased perioperative morbidity/mortality. Thus, Nivolumab + Ipilumab combined with immunotherapy was more effective than Nivolumab alone.
The NADIM study38 (Table 2) was the first clinical study to explore the efficacy of immune-combined chemotherapy in patients with stage IIIA NSCLC by observing the efficacy and safety of Nivolumab combined with Paclitaxel + Carboplatin neoadjuvant/adjuvant therapy in patients with resectable stage IIIA NSCLC. Forty-six patients were included, and 41 underwent surgery and achieved R0 resection. The MPR reached 85.36% (95% CI, 71%–95%), and the pCR reached 71.4% (95% CI, 54%–87%). In the RECIST study, PR was 72%, and CR was 6.5%. In 93% of patients, neoadjuvant immunotherapy combined with chemotherapy was down staged. No patients withdrew from the study before surgery because of PD or safety reasons.
ChiCTR-OIC-17013726 (Table 2) is an open, single-center, IB phase of the study to evaluate Sintilimab for resectable NSCLC neoadjuvant therapy.39 Twenty-two patients with biopsy-proven stage IB-IIIA squamous NSCLC were included and received two preoperative cycles of Sintilimab and PET-CT examinations, then radical surgery. The results of this study were published as a poster at the 2019 ASCO conference. Compared with PET-CT before and after neoadjuvant therapy, 9 patients’ tumor metabolism uptake (TMU) decreased by 30%, and 8 of these achieved MPR. No MPR was found in 11 patients whose TMU dropped below 30% or whose TMU increased. Postoperative pathological results showed that 10 patients (45.5%) achieved MPR, and 4 patients (18.2%) achieved pCR. Decreases in MPR and TMU were correlated with decreases in TMU on PET-CT after neoadjuvant therapy, which may predict the postoperative MPR status. In summary, Sintilimab has shown good safety in neoadjuvant therapy for resectable NCSLC.
The above data reveal good efficacy and safety profiles for immunotherapy in neoadjuvant therapy for NSCLC, but many decisions remain, such as 1) whether the immunotherapy regimen should be a single-drug or combination; 2) how the joint treatment plan should be chosen (immunotherapy combination chemotherapy, radiotherapy, anti-VEGFR or immunotherapy); 3) whether the joint timing should be synchronous or sequential; and 4) whether immunotherapy will affect the timing of the surgery. The Checkmate-159 study was 1 to 2 cycles of neoadjuvant immunotherapy before surgery. NEOSTAR was studied approximately 3 cycles before surgery. The NADIM study involved 3 cycles before surgery until 3 or 4 weeks after the last immunotherapy. The final results do not affect the timing of the surgery, but more research is needed. For example, should biomarkers such as PD-L1 or TMB be tested? Can MPR, pCR, or MPR criteria predict survival? How should the pseudo-progress of neoadjuvant immunotherapy be evaluated? Much research is still needed to determine how best to apply checkpoint inhibitors to neoadjuvant therapy for NSCLC. However, the progress made thus far represents an important step toward longer-term survivalin early treatment. Phase III studies of neoadjuvant immunotherapy are ongoing, including CheckMate-816,40 IMpower03041 and KEYNOTE67142 (Table 3). The release of these research data will help develop more beneficial treatments for NSCLC patients.
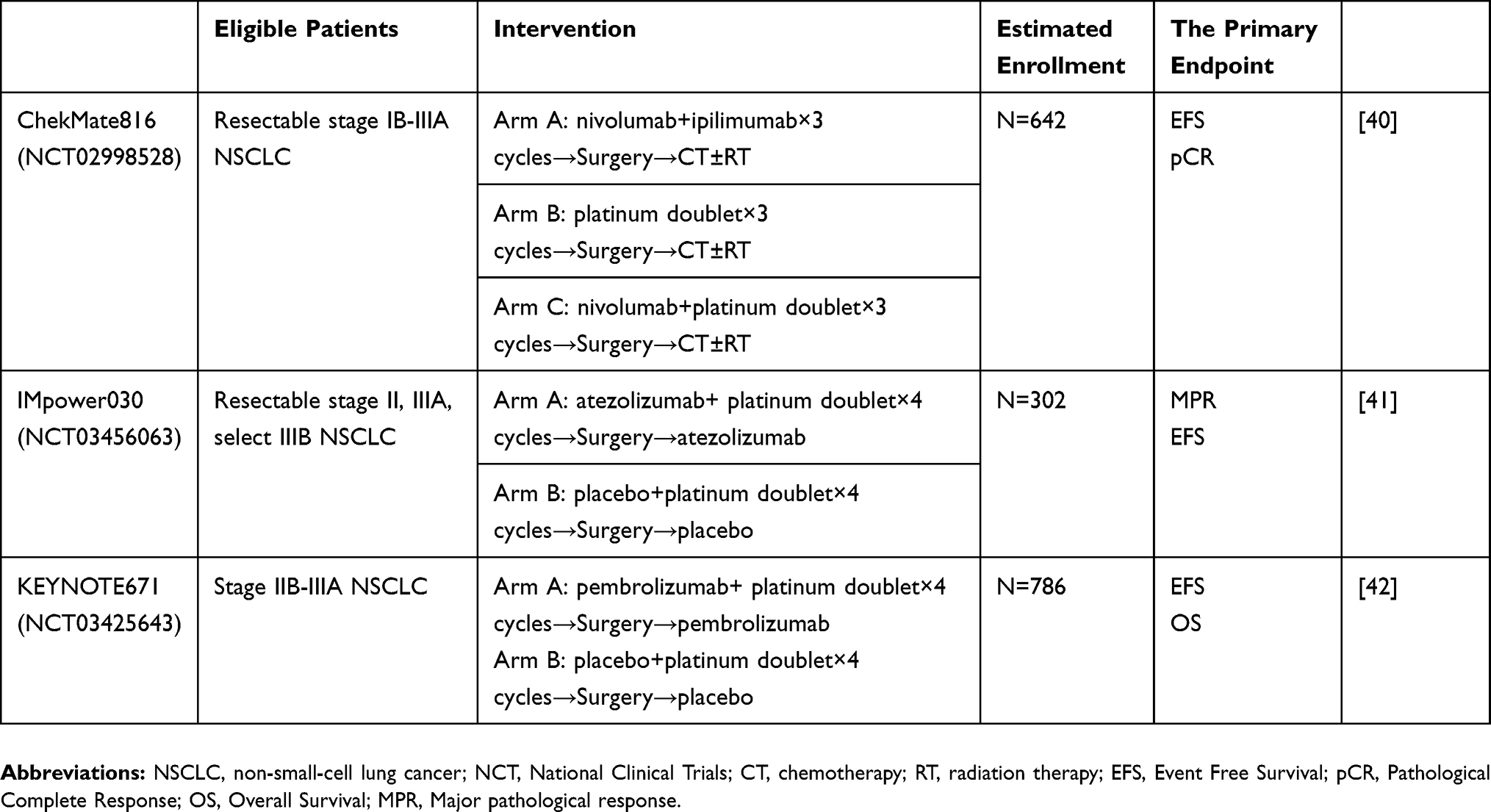 |
Table 3 Ongoing Randomized Phase III Trials Of Neoadjuvant Immunotherapy In Early-Stage And Locally Advanced NSCLC |
Adjuvant Immunotherapy
Phase III studies of adjuvant therapy for NSCLC, including ANVIL,43 IMpower010,44 PEARLS,45 KEYNOTE671,42 and IFCT-1401,46 are ongoing (Table 4). Phase III studies remain in the exploration stage and are faced with many challenges, such as how to choose the beneficiaries, how to choose the immunotherapy regimen, and the timing and duration of the immunotherapy. More clinical findings will help to answer these questions.
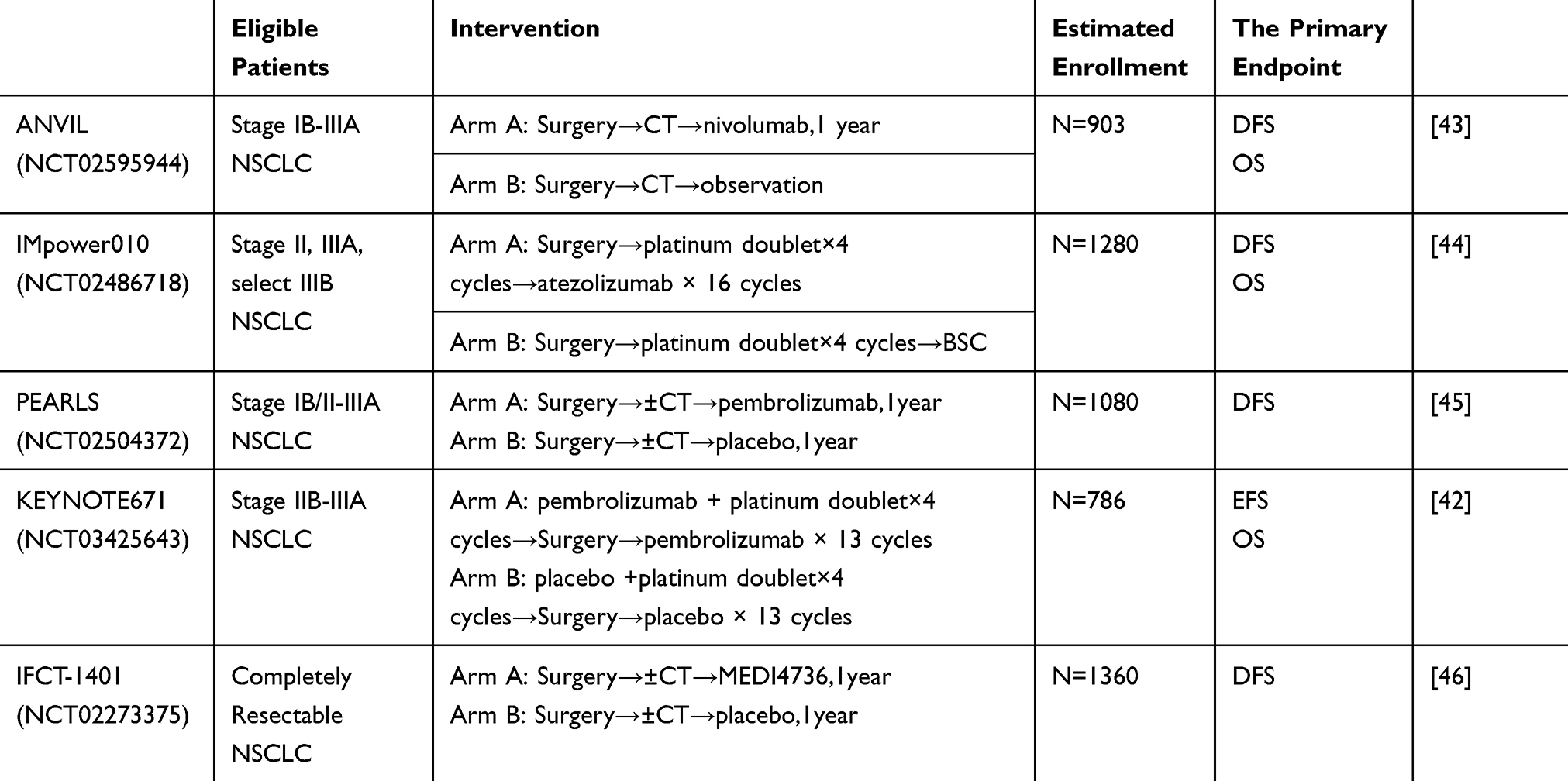 |
Table 4 Ongoing Randomized Phase III Trials Of Adjuvant Immunotherapy In Early-Stage And Locally Advanced NSCLC |
Summary And Prospects
Advanced lung cancer treatment has entered the era of precision treatment, and treatment plans are relatively clear, but early-stage and locally advanced NSCLC perioperative treatment remain controversial. Initial studies have found targeted therapy and immunotherapy to be very effective and safe. However, several problems persist, such as identifying the patients suitable for perioperative treatment, timing and duration of perioperative treatment, choice of treatment regimens and biomarkers, prediction criteria for efficacy, and whether MPR can be used as an alternative endpoint. To achieve better clinical benefits, accurate and individualized treatment is needed, but more and larger clinical studies are needed in evidence-based medicine to formulate optimal treatment strategies.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018:GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. doi:10.3322/caac.21492
2. Yang P, Allen MS, Aubry MC, et al. Clinical features of 5,628 primary lung cancer patients: experience at mayo clinic from 1997 to 2003. Chest. 2005;128(1):452–462. doi:10.1378/chest.128.1.452
3. Burdett S, Pignon JP, Tierney J, et al. Adjuvant chemotherapy for resected early-stage non-small cell lung cancer. Cochrane Database Syst Rev. 2015;(3):CD011430. doi:10.1002/14651858.CD011430
4. Arriagada R, Auperin A, Burdett S, et al. Adjuvant chemotherapy, with or without postoperative radiotherapy, in operable non-small-cell lung cancer: two meta-analyses of individual patient data. Lancet. 2010;375(9722):1267–1277. doi:10.1016/S0140-6736(10)60059-1
5. Pignon JP, Tribodet H, Scagliotti GV, et al. Lung adjuvant cisplatin evaluation: a pooled analysis by the LACE collaborative group. J Clin Oncol. 2008;26(21):3552–3559. doi:10.1200/JCO.2007.13.9030
6. Meta-Analysis Collaborative NSCLC Group. Preoperative chemotherapy for non⁃small-cell lung cancer: a systematic review and meta-analysis of individual participant data. Lancet. 2014;383(9928):1561–1571. doi:10.1016/S0140-6736(13)62159-5
7. Fukuoka M, Wu YL, Thongprasert S, et al. Biomarker analyses and final overall survival results from a phase III, randomized, open-label, first-line study of gefitinib versus carboplatin/paclitaxel in clinically selected patients with advanced non-small-cell lung cancer in Asia (IPASS). J Clin Oncol. 2011;29(21):2866–2874. doi:10.1200/jco.2010.33.4235
8. Wu YL, Zhou C, Hu CP, et al. Afatinib versus cisplatin plus gemcitabine for first-line treatment of Asian patients with advanced non-small-cell lung cancer harbouring EGFR mutations (LUX-Lung 6): an open-label, randomised phase 3 trial. Lancet Oncol. 2014;15(2):213–222. doi:10.1016/S1470-2045(13)70604-1
9. Slamon DJ. Activating mutations in the epidermal growth factor receptor underlying responsiveness of non-small-cell lung cancer to gefitinib. N Engl J Med. 2004;350(350):2129–2139. doi:10.1056/NEJMoa040938
10. Paez JG, Janne PA, Lee JC, et al. EGFR mutations in lung cancer: correlation with clinical response to gefitinib therapy. Science. 2004;304(5606):1497–1500. doi:10.1126/science.1099314
11. Zhong W, Yang X, Yan H, et al. Phase II study of biomarker-guided neoadjuvant treatment strategy for IIIA-N2 non-small cell lung cancer based on epidermal growth factor receptor mutation status. J Hematol Oncol. 2015;8(1):54. doi:10.1186/s13045-015-0151-3
12. Lara-Guerra H, Chung CT, Schwock J, et al. Histopathological and immunohistochemical features associated with clinical response to neoadjuvant gefitinib therapy in early stage non-small cell lung cancer. Lung Cancer. 2017;76(2):235–241. doi:10.1016/j.lungcan.2011.10.020
13. Lara-Guerra H, Waddell TK, Salvarrey MA, et al. Phase II study of preoperative gefitinib in clinical stage I non-small-cell lung cancer. J Clin Oncol. 2009;27(36):6229–6236. doi:10.1200/jco.2009.22.3370
14. Hishida T, Nagai K, Mitsudomi T, et al. Salvage surgery for advanced non-small cell lung cancer after response to gefitinib. J Thorac Cardiovasc Surg. 2010;140(5):e69–e71. doi:10.1016/j.jtcvs.2010.06.035
15. Schaake EE, Kappers I, Codrington HE, et al. Tumor response and toxicity of neoadjuvant erlotinib in patients with early-stage non-small-cell lung cancer. J Clin Oncol. 2012;30(22):2731–2738. doi:10.1200/JCO.2011.39.4882
16. Rizvi NA, Rusch V, Pao W, et al. Molecular characteristics predict clinical outcomes: prospective trial correlating response to the EGFR tyrosine kinase inhibitor gefitinib with the presence of sensitizing mutations in the tyrosine binding domain of the EGFR gene. Clin Cancer Res. 2011;17(10):3500–3506. doi:10.1158/1078-0432.CCR-10-2102
17. Zhong WZ, Chen KN, Chen C, et al. Erlotinib versus gemcitabine plus cisplatin as neoadjuvant treatment of stage IIIA-n2-mutant non-small-cell lung cancer (EMERGING-CTONG 1103): a randomized phase II study. J Clin Oncol. 2019:JCO1900075. doi:10.1200/JCO.19.00075
18. Han B, Xiong L, Sun J, et al. Erlotinib as neoadjuvant treatment in endobronchial ultrasound confirmed stage IIIA-N2 non⁃small cell lung cancer (NSCLC) patients with epidermal growth factor receptor (EGFR) mutation (exon 19 or 21) (NCT01217619,ESTERN): A prospective, single arm, phase II clinical trial. Ann Oncol. 2015;26(1S):i24. doi:10.1093/annonc/mdv383
19. Soria JC, Ohe Y, Vansteenkiste J, et al. Osimertinib in untreated EGFR-mutated advanced non-small-cell lung cancer. N Engl J Med. 2018;378(2):113–125. doi:10.1056/NEJMoa1713137
20. Chictr.org. A multicenter, open-label, single arm pilot study: osimertinib as neoadjuvant treatment for resectable stage II-IIIA EGFR mutant lung adenocarcinoma. Available from: http://www.chictr.org.cn/showproj.aspx?proj=28760.
21. ClinicalTrials.gov. Osimertinib in treating participants with stage I-IIIA EGFR-mutant non-small cell lung cancer before surgery. Available from: https://clinicaltrials.gov/ct2/show/NCT03433469.
22. Lin JJ, Riely GJ, Shaw AT. Targeting ALK: precision medicine takes on drug resistance. Cancer Discov. 2017;7(2):137–155. doi:10.1158/2159-8290.CD-16-1123
23. Zhang C, Li SL, Nie Q, et al. Neoadjuvant crizotinib in resectable locally advanced non-small cell lung cancer with ALK rearrangement. J Thorac Oncol. 2019;14:726–731. doi:10.1016/j.jtho.2018.10.161
24. ClinicalTrials.gov. Evaluating crizotinib in the neoadjuvant setting in patients with non-small cell lung cancer. Available from: https://clinicaltrials.gov/ct2/show/NCT03088930.
25. ClinicalTrials.gov. Pre-operative gefitinib in resectable EGFR mutation positive lung cancer with sector sequencing for biomarker discovery (PROGRESS). Available from: https://clinicaltrials.gov/ct2/show/NCT02804776.
26. Goss GD, O’Callaghan C, Lorimer I, et al. Gefitinib versus placebo in completely resected non-small-cell lung cancer: results of the NCIC CTG BR19 study. J Clin Oncol. 2013;31(27):3320–3326. doi:10.1200/JCO.2013.51.1816
27. Kelly K, Altorki NK, Eberhardt WE, et al. Adjuvant erlotinib versus placebo in patients with stage IB-IIIA non-small-cell lung cancer (RADIANT): A randomized, double-blind, phase III trial. J Clin Oncol. 2015;33(34):4007–4014. doi:10.1200/JCO.2015.61.8918
28. Pennell NA, Neal JW, Chaft JE, et al. SELECT: A multicenter phase II trial of adjuvant erlotinib in resected early-stage EGFR mutation-positive NSCLC. J Clin Oncol. 2014;32(15_suppl):7514. doi:10.1200/jco.2014.32.15_suppl.7514
29. ClinicalTrials.gov. AZD9291 versus placebo in patients with stage IB-IIIA non-small cell lung carcinoma, following complete tumour resection with or without adjuvant chemotherapy. (ADAURA). Available from: https://clinicaltrials.gov/ct2/show/NCT02511106.
30. Zhong WZ, Wang Q, Mao WM, et al. Gefitinib versus vinorelbine plus cisplatin as adjuvant treatment for stage II-IIIA (N1-N2) EGFRmutant NSCLC (ADJUVANT/CTONG1104): A randomised, open-label, phase 3 study. Lancet Oncol. 2018;19(1):139–148. doi:10.1016/S1470-2045(17)30729-5
31. Yue D, Xu S, Wang Q, et al. Erlotinib versus vinorelbine plus cisplatin as adjuvant therapy in Chinese patients with stage IIIA EGFR ⁃⁃⁃mutation-positive non-small-cell lung cancer (EVAN): a randomised, open-label, phase 2 trial. Lancet Respir Med. 2018;6(11):863–873. doi:10.1016/S2213-2600(18)30277-7
32. Forde PM, Chaft JE, Smith KN, et al. Neoadjuvant PD⁃1 blockade in resectable lung cancer. N Engl J Med. 2018;378(21):1976–1986. doi:10.1056/nejmoa1716078
33. Reck M, Rodriguez-Abreu D, Robinson AG, et al. Pembrolizumab versus chemotherapy for PD-L1–positive non–small-cell lung cancer. N Engl J Med. 2016;375(19):1823–1833. doi:10.1056/NEJMoa1606774
34. Gandhi L, Rodriguez-Abreu D, Gadgeel S, et al. Pembrolizumab plus chemotherapy in metastatic non–small cell lung cancer. N Engl J Med. 2018;378(22):2078–2092. doi:10.1056/nejmoa1801005
35. Reuss JE, Smith KN, Anagnostou V, et al. Neoadjuvant nivolumab in resectable non-small cell lung cancer: extended follow-up and molecular markers of response. J Clin Oncol. 2019;37(suppl):abstr 8524.
36. Kwiatkowski DJ, Rusch VW, Chaft JE, et al. Neoadjuvant atezolizumab in resectable non-small cell lung cancer (NSCLC): interim analysis and biomarker data from a multicenter study (LCMC3). J Clin Oncol. 2019;37(suppl):abstr 8503.
37. Cascone T, William WN, Weissferdt A, et al. Neoadjuvant nivolumab (N) or nivolumab plus ipilimumab (NI) for resectable non-small cell lung cancer (NSCLC): clinical and correlative results from the NEOSTAR study. J Clin Oncol. 2019;37(suppl):abstr 8504.
38. Provencio M, Nadal E, Insa A, et al. Neoadjuvant chemo-immunotherapy for the treatment of stage IIIA resectable non-small-cell lung cancer (NSCLC): A phase II multicenter exploratory study—final data of patients who underwent surgical assessment. J Clin Oncol. 2019;37(suppl):abstr 8509.
39. Li N, J M Y, Tao XL, et al. Efficacy and safety of neoadjuvant PD-1 blockade with sintilimab in resectable squamous non-small cell lung cancer (sqNSCLC). J Clin Oncol. 2019;37(suppl):abstr 8531.
40. ClinicalTrials.gov. A neoadjuvant study of nivolumab plus ipilimumab plus chemotherapy versus chemotherapy alone in early stage non-small cell lung cancer (NSCLC) (CheckMate 816). Available from: https://clinicaltrials.gov/ct2/show/NCT02998528.
41. ClinicalTrials.gov. A study of neoadjuvant atezolizumab plus chemotherapy versus placebo plus chemotherapy in patients with resectable stage II, IIIA, or select IIIB non-small cell lung cancer (IMpower030). Available from: https://clinicaltrials.gov/ct2/show/NCT03456063.
42. ClinicalTrials.gov. Efficacy and safety of pembrolizumab (MK-3475) with platinum doublet chemotherapy as neoadjuvant/adjuvant therapy for participants with resectable stage IIB or IIIA non-small cell lung cancer (MK-3475-671/KEYNOTE-671). Available from: https://clinicaltrials.gov/ct2/show/NCT03425643.
43. ClinicalTrials.gov. nivolumab after surgery and chemotherapy in treating patients with stage IB-IIIA non-small cell lung cancer (An ALCHEMIST Treatment Trial) (ANVIL). Available from: https://clinicaltrials.gov/ct2/show/NCT02595944.
44. ClinicalTrials.gov. Study to assess safety and efficacy of atezolizumab (MPDL3280A) compared to best supportive care following chemotherapy in patients with lung cancer [IMpower010]. Available from: https://clinicaltrials.gov/ct2/show/NCT02486718.
45. ClinicalTrials.gov. Study of pembrolizumab (MK-3475) vs placebo for participants with non-small cell lung cancer after resection with or without standard adjuvant therapy (MK-3475-091/KEYNOTE-091) (PEARLS). Available from: https://clinicaltrials.gov/ct2/show/NCT02504372.
46. ClinicalTrials.gov. Double-blind placebo controlled study of adjuvant MEDI4736 in completely resected NSCLC. Available from: https://clinicaltrials.gov/ct2/show/NCT02273375.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.