Back to Journals » Advances in Medical Education and Practice » Volume 10
Perioperative Provider and Staff Competency in Providing Culturally Competent LGBTQ Healthcare in Pediatric Setting
Authors Walia H, Banoub R ![]() , Cambier GS, Rice J, Tumin D, Tobias JD
, Cambier GS, Rice J, Tumin D, Tobias JD ![]() , Raman VT
, Raman VT ![]()
Received 24 June 2019
Accepted for publication 9 December 2019
Published 31 December 2019 Volume 2019:10 Pages 1097—1102
DOI https://doi.org/10.2147/AMEP.S220578
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Hina Walia, 1 Rita Banoub, 1, 2 Gregory S Cambier, 1, 2 Julie Rice, 1 Dmitry Tumin, 1 Joseph D Tobias, 1, 2 Vidya T Raman 1, 2
1Department of Anesthesiology & Pain Medicine, Nationwide Children’s Hospital, Columbus, OH, USA; 2Department of Anesthesiology & Pain Medicine, The Ohio State University College of Medicine, Columbus, OH, USA
Correspondence: Hina Walia
Department of Anesthesiology & Pain Medicine, Nationwide Children’s Hospital, 700 Children’s Drive, Columbus, OH 43205, USA
Tel +1614 722-3846
Fax +1614 722-4203
Email [email protected]
Introduction: Children and adolescents identifying as lesbian, gay, bisexual, transgender, or queer/questioning (LGBTQ) may feel reluctant to seek medical care due to stigma and the possibility of negative interactions with health care providers. Due to the short duration of the perioperative period, the interaction in this setting is limited and providers may not have the time to develop a rapport with the patient. It is imperative that staff are trained to address the patient and family in a culturally competent manner.
Methods: We undertook surveys before and after a 2 part educational series among the pediatric perioperative staff to understand the impact of providing education and cultural competency training regarding caring for patients who identify as LGBTQ. Providers self-reported their knowledge and comfort on a 1– 5 point scale (5 being most knowledgeable or comfortable) in 6 domains of caring for LGBTQ patients. Objective knowledge of LGBTQ issues was assessed using 7 questions based on lecture material. On objective assessment, knowledge of LGBTQ issues improved after cultural competency training.
Results: The analysis included 90 responses. Before training, median ratings of knowledge and comfort were 3 or 4 out of a maximum of 5 for each domain. The pre-training median score on the 7-item test of LGBTQ cultural competency was 5 (IQR: 4, 6). After training, knowledge and comfort self-ratings did not improve, but the score on the objective knowledge test increased to a median of 6 (IQR: 4, 7; p=0.011) of 7 possible points.
Discussion: Anesthesia providers participating in LGBTQ cultural competency training self-reported high levels of knowledge and comfort with providing care to LGBTQ patients even before formal training was provided. On objective assessment, knowledge of LGBTQ issues improved after cultural competency training.
Keywords: LGBTQ, health, concerns, competency, training, attitude
Corrigendum for this paper has been published
Introduction
In the United States, people identifying as lesbian, gay, bisexual, transgender, queer/questioning (LGBTQ) may experience numerous health disparities when compared to people identifying as heterosexual and cisgender.1 This community is among the most medically underserved groups in our society. Due to discrimination in the health care setting, patients identifying as LGBTQ may avoid or delay seeking health care.2 LGBTQ adolescents and young adults face additional challenges related to sexual orientation, evolving gender roles, peer pressure, bullying, and progression through developmental stages.3,4 Sexual minorities including the LGBTQ community are understudied with respect to health and health care inequalities.5 Due to lack of formal training when interacting with this patient population, it is imperative that pediatric health care providers are educated on caring for patients who identify as LGBTQ, including pre-adolescents and adolescents, in order to ensure a safe and comfortable hospital experience.6 The purpose is to ensure that the patient does not experience a negative interaction and lose trust in health care providers. Education and cultural competency in the health care system can facilitate a more positive experience and better health care outcomes for the LGBTQ community.7 Due to the short duration of the perioperative period, the interaction is limited and providers may not have the time to develop a rapport with the patient and family. Hence it is imperative that staff are trained to utilize this time effectively and address the patient and family in a comfortable manner. We undertook surveys before and after a 2 part educational series among the pediatric perioperative staff including anesthesia providers to gauge the impact of providing education and cultural competency training regarding caring for patients who identify as LGBTQ.
Methods
The Institutional Review Board at Nationwide Children’s Hospital waived the need for review of this project as a quality improvement initiative. A confidential survey was distributed to perioperative health care providers at a tertiary-care free-standing children’s hospital before and after a two-part lecture series presented by the director of the LGBTQ health initiative at a regional non-profit community-based health care system. The lecture series “Providing Health and Social Services to the Trans and Gender Non-conforming Community (Basic and Advanced)” addressed several topics including the differences between sexual orientation and gender identity, cultural competency, specific health disparities experienced by LGBTQ community, and culturally competent care for patients who identify as LGBTQ. Perioperative staff unable to attend the lecture were sent links to the video recordings. The survey was developed based on a previous “Gender and Sexual Minorities Cultural Competency Training” provided to a focus group of pediatric residents. The confidential survey was distributed to the perioperative staff before and after the lecture series and collected in June–December 2016. The staff reported demographic data including their age, gender, role, and whether they received prior training in cultural competency related to gender identity and sexual orientation. They also self-reported their knowledge and comfort on a 1–5 scale in 6 domains: sensitivity about their language; sensitivity about their non-verbal communication; not assuming all patients are heterosexual; not assuming all patients identify with their gender assigned at birth; awareness of multiple minority status; and non-judgmental communication. Responses were recorded on 1–5 scale with 5 being most knowledgeable or comfortable. Additionally, a series of 7 questions (graded as correct or incorrect) testing knowledge regarding LGBTQ cultural competency, with responses coded on a 0–7 scale identifying the number of correct answers (Table 1). Continuous data were summarized as medians with interquartile ranges (IQR), and compared between pre-training and post-training questionnaires using signed-rank tests. Categorical data were summarized as counts with percentages, and compared between pre- and post-training questionnaires using McNemar’s tests. Due to the exploratory nature of the assessment (ie, there was no prespecified hypothesis about which evaluated factor would change after training), no adjustment for multiple comparisons was made when calculating statistical significance.
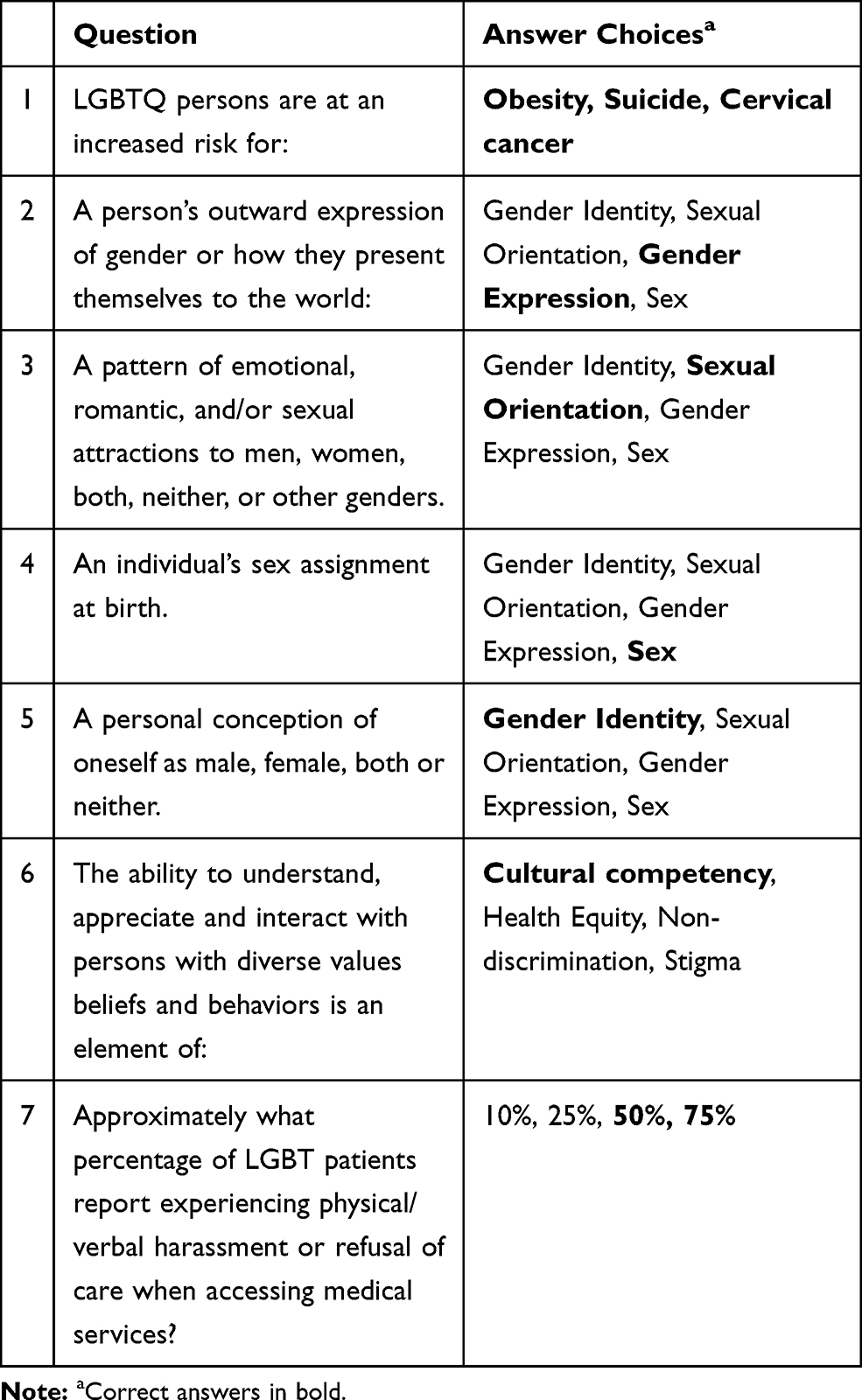 |
Table 1 Testing Knowledge Regarding the LGBTQ Community |
Results
Two hundred and fifty three responses were recorded, of which 214 responses by 169 participants were selected for analysis. Exclusions were missing age or study ID, multiple pre-responses per ID with the first response kept, multiple post-responses per ID with the first response kept, and multiple post-incomplete responses. Participants included 31 (18%) men and 138 (82%) women; 71 (42%) providers age 20–35 years, 74 (44%) providers age 35–50 years, and 24 (14%) providers age 50 years and older. The study cohort included 45 respondents who completed both pre- and post-intervention surveys. Participants included 6 (13%) men and 39 (87%) women; 16 (36%) providers aged 20–35 years, 20 (44%) providers aged 35–50 years, and 9 (20%) providers ≥50 years of age. Participant roles included medical doctor (MD) such as a faculty member or trainee (n=6, 13%), registered nurse (RN) or certified registered nurse anesthetist (n=37, 82%), and others (n=2, 4%) including patient care assistants and surgical technicians. Six respondents (13%) reported previous training in LGBTQ cultural competency, most commonly at a conference (n=2), or during medical school or residency (n=2).
The rate of low (1–2) responses for the 12 self-rated questions was 0-13%, depending on the question. Questions with higher rates of low responses related to assumptions about whether patients identified as heterosexual and whether patients identified with their gender assigned at birth. In total, 6 of 45 providers (13%) rated their knowledge or comfort as low (1–2) on at least one of these 12 questions. Self-rated knowledge and comfort (pre-training) in 6 domains of caring for LGBT patients are summarized in Table 2. The median ratings of knowledge and comfort were 3 or 4 out of 5 for each domain. The median score on the 7-item test of LGBTQ cultural competency was 5 (IQR: 5, 6). The most commonly missed questions related to health risks in the LGBTQ community and experiences with health care providers (questions 1 and 7).
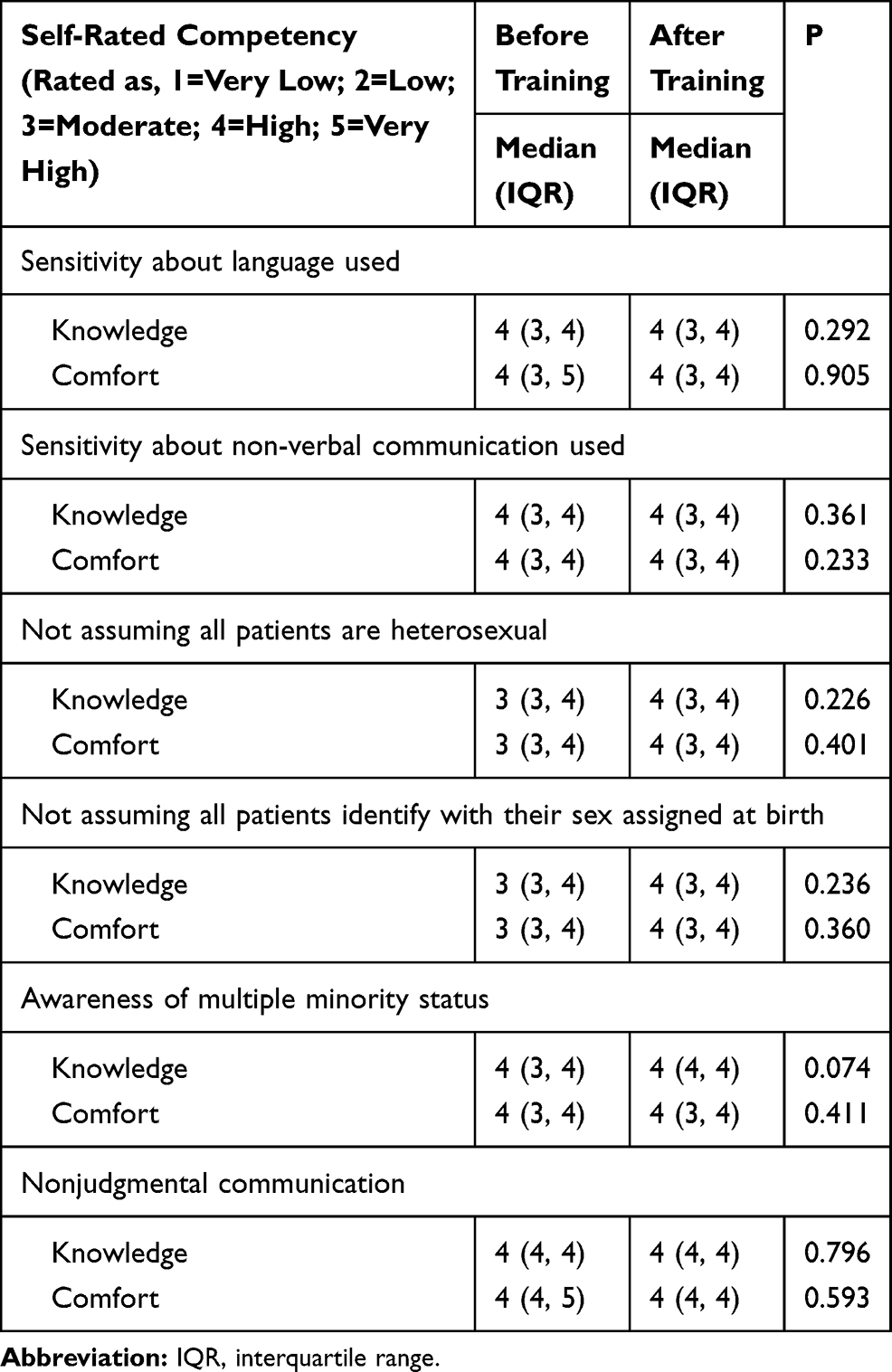 |
Table 2 Self-Rated Knowledge and Comfort with Competencies in Caring for Lesbian, Gay, Bisexual, Transgender, and Queer/Questioning (LGBTQ) Patients, Reported by Health care Providers Before and After Completing LGBTQ Cultural Competency Training (N = 45) |
After training, there were no statistically significant improvements in knowledge or comfort with the 6 domains. Median scores on the 7-item test improved by 1 point after training (pre-training median=5; IQR: 4, 6, compared to post-training median=6; IQR: 4, 7; p=0.011). Among providers with low (1–2) scores on self-rated questions, the only improved self-rating from pre-test to post-test was in knowledge of multiple minority status (from median of 3 with IQR: 3, 3 to median of 4 with IQR 3, 4; p=0.049). Three of 45 providers (7%) had an objective knowledge score ≤2 on the 0–7 scale before training. In this subgroup, the objective knowledge score increased from a median of 2 (IQR: 2, 2) to a median of 4 (IQR: 3, 6). Meanwhile, one provider had a perfect score before and after training while 14 had a perfect score after training, but not before. Improvement in the proportion of providers with a perfect score was supported by a statistically significant McNemar test (p=0.013).
Discussion
In the present study, we report our experience with providing LGBTQ cultural competency training to perioperative care providers at our institution. Whereas participants’ objectively assessed knowledge in this area improved after the intervention, self-rated knowledge and comfort with caring for LGBTQ patients were already high in the pre-intervention assessment, and did not significantly improve after the intervention. This finding suggests that future interventions to improve LGBTQ cultural competency among health care workers should not only assess knowledge but include different case studies in caring for patients who identify as LGBTQ, and target specific clinical scenarios where health care providers’ understanding, ability to ask questions and build a rapport with LGBTQ patients in clinical settings can be observed and improved.
Patients identifying as LGBTQ encounter limited access to health care and discrimination in health care settings. Medical issues in the LGBTQ community include common clinical problems, such as smoking, obesity, alcohol, and drug use; and more complex clinical issues, such as human immunodeficiency virus infection and other sexually transmitted diseases. Due to widespread stigma and discrimination, LGBTQ youth are also more likely to attempt suicide, experience homelessness, and be subject to victimization.8 Broadly, LGBTQ youth may have insufficient social support, contributing to feeling isolated and marginalized.9
Our goal in this study was to provide the perioperative health care team with information regarding how to address the unique health needs of LGBTQ patients during the perioperative period.10 The perioperative period is a very stressful time for the patients and their families. Furthermore, as health care providers involved in the perioperative period, we are frequently meeting the patient and their family for the first time and may have a limited amount of time to gain their trust during a particularly stressful situation. Such issues may contribute to LGBTQ patients avoiding medical and surgical services. Preoperative anxiety can contribute to the development of postoperative issues including emergence delirium and increased postoperative pain.11 It is important to create an affirmative, inclusive and safe clinical environment that will make the adolescent feel comfortable and facilitate a frank discussion of sexual orientation and gender identity between patients and health providers. This open and positive interaction will be a key factor in decreasing the anxiety of the patient and their family. The quality of the patient–provider relationship is also important for obtaining a truthful medical history during the short interaction in the perioperative period.
The health care needs and disparities experienced by LGBTQ patients are increasingly recognized in health care settings but, despite growing cultural acceptance of LGBTQ people, negative views of homosexuality are still prevalent.12 In 1973, the Diagnostic and Statistical Manual of Mental Disorders (DSM) removed the categorization of homosexuality as an illness, and in 2000 the American Psychiatric Association publicly stated its opposition to “conversion” therapy.13 Despite these changes, acceptance of LGBTQ patients and provision of culturally competent care to this population has not yet been fully achieved within the medical professions.14 A survey conducted among medical residents found that 71% did not ask sexually active adolescents about their sexual orientation because of their own lack of comfort with such discussions.15 This emphasizes that there is a need for continuing education in cultural competency related to LGBTQ community.
Notwithstanding initiatives to improve care provided to LGBTQ patients in health care settings, there remain broader disadvantages experienced by this population. The social characteristics of LGBTQ people including economic status, education, employment, stigma and discrimination lead to unequal access to health care, and providers with lack of knowledge and sensitivity when caring for LGBTQ patients. The inherent societal biases, and prejudice against LGBTQ people should be addressed at multiple levels, starting at schools, by protecting students identifying as LGBTQ and preventing bullying.16 Educators need to understand the diversity of families including LGBTQ parents and that children of LGBTQ parents are developing in healthy ways.17 Violence against LGBTQ adolescents whether in the form of verbal or physical assault is of a primary concern as it can lead to multiple health problems including anxiety, depression, and suicide.18 At state and government levels, policies that prevent employment discrimination and allow same sex marriage are also important steps in reducing the invisibility of LGBTQ population and securing a safe, supportive and inclusive society. It is of interest to note that lesbian and gay adolescents are looking for the future with the hope of being able to marry a same-sex partner.19 State-level same-sex marriage policies have been associated with a reduction in the proportion of high school students reporting suicide attempts, providing empirical evidence for an association between same-sex marriage policies and mental health outcomes.20
The conclusions of the present study are tempered by some limitations of the data collection and analysis. Data were collected confidentially, precluding further study of participants’ characteristics, experience, or attitudes and beliefs about patients identifying as LGBTQ. There was also a lack of follow-up for many of the intervention participants, limiting the sample available for analysis. Additionally, participants’ objective knowledge of issues in LGBTQ cultural competency was evaluated using a short questionnaire based on lecture material, which may have limited our ability to differentiate between adequate and excellent understanding of this subject matter. Further studies of LGBTQ cultural competency among health care providers should address providers’ ability to obtain a social history including adolescent sexual activity, tobacco, alcohol and other substance use. An effort should be made to ask preferred pronouns and be aware of diverse gender identities and sexual orientation when addressing patients and families. This patient information can help the health care team in providing individualized care according to each patient’s needs, and particularly help in relieving the anxiety of the preoperative period and insuring a rapid postoperative recovery.
Health care providers play a vital role during the perioperative period in easing the associated anxiety by showing compassion, acceptance and approaching patients with an open mind. The goal of this initiative was to ensure an appropriate knowledge base in our perioperative team thereby ensuring the provision of the best care to our LGBTQ patients. Health care providers need to be sensitive to the various issues surrounding the LGBTQ youth and avoid unconscious bias against those seeking medical care.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Mustanski BS, Garofalo R, Emerson EM. Mental health disorders, psychological distress, and suicidality in a diverse sample of lesbian, gay, bisexual, and transgender youths. Am J Public Health. 2010;100:2426–2432. doi:10.2105/AJPH.2009.178319
2. Clift JB, James K. Articles health care access and perceptions of provider care among individuals in same-sex couples: findings from the medical expenditure panel survey (MEPS). J Homosex. 2012;59:839–850. doi:10.1080/00918369.2012.694766
3. Arnett JJ. Emerging adulthood. A theory of development from the late teens through the twenties. Am Psychol. 2000;55:469–480. doi:10.1037/0003-066X.55.5.469
4. Park MJ, Scott JT, Adams SH, et al. Adolescent and young adult health in the United States in the past decade: little improvement and young adults remain worse off than adolescents. J Adolescent Health. 2014;55:3–16. doi:10.1016/j.jadohealth.2014.04.003
5. Strutz KL, Herring AH, Halpern CT. Health disparities among young adult sexual minorities in the U.S. Am J Prev Med. 2015;48:76–88. doi:10.1016/j.amepre.2014.07.038
6. Bosse JD, Chiodo L. It is complicated: gender and sexual orientation identity in LGBTQ youth. J Clin Nurs. 2016;25:3665–3675. doi:10.1111/jocn.2016.25.issue-23pt24
7. Dean MA, Victor E, Guidry-Grimes L. Inhospitable healthcare spaces: why diversity training on LGBTQIA issues is not enough. J Bioeth Inq. 2016;13:557–570. doi:10.1007/s11673-016-9738-9
8. Haas AP, Eliason M, Mays VM, et al. Suicide and suicide risk in lesbian, gay, bisexual, and transgender populations: review and recommendations. J Homosex. 2011;58:10–51. doi:10.1080/00918369.2011.534038
9. Peters A. Isolation or inclusion: creating safe spaces for lesbian and gay youth. Fam Soc. 2003;84:331–337. doi:10.1606/1044-3894.122
10. Remafedi G. Fundamental issues in the care of homosexual youth. Med Clin North Am. 1990;74:1169–1179. doi:10.1016/S0025-7125(16)30509-0
11. Kain ZN, Mayes LC, Caldwell-Andrews AA, Karas DE, McClain BC. Preoperative anxiety, postoperative pain, and behavioral recovery in young children undergoing surgery. Pediatrics. 2006;118:651–658. doi:10.1542/peds.2005-2920
12. Weber A, Collins SA, Robinson-Wood T, Zeko-Underwood E, Poindexter B. Subtle and severe: microaggressions among racially diverse sexual minorities. J Homosex. 2017;16:1–20.
13. American Psychiatric Association. Commission of Psychotherapy by Psychiatrists. Position statement on therapies focused on attempts to change sexual orientation (reparative or conversion therapies). Am J Psychiatry. 2000;157:1719–1721.
14. Cahill S, Makadon H. Sexual orientation and gender identity data collection in clinical settings and in electronic health records: a key to ending LGBT health disparities. LGBT Health. 2014;1:34–41. doi:10.1089/lgbt.2013.0001
15. Kitts RL. Barriers to optimal care between physicians and lesbian, gay, bisexual, transgender and questioning adolescent patient. J Homosexual. 2010;57:730–747. doi:10.1080/00918369.2010.485872
16. Daley A, Solomon S, Newman PA, Mishna F. Traversing the margins: intersectionalities in the bullying of lesbian, gay, bisexual and transgender youth. J Gay Lesbian Soc Serv. 2008;19:9–29. doi:10.1080/10538720802161474
17. Farr RH, Forsell SL, Patterson CJ. Parenting and child development in adoptive families: does parental sexual orientation matter? Appl Dev Sci. 2010;14:164–178. doi:10.1080/10888691.2010.500958
18. Pilkington N, D’Augelli AR. Victimization of lesbian, gay, and bisexual youth in community setting. J Community Psychol. 1995;23:34–56. doi:10.1002/1520-6629(199501)23:1<34::AID-JCOP2290230105>3.0.CO;2-N
19. D’ Augelli RHJ, Sinclair KO, Grossman AH. Lesbian and gay youth’s aspirations for marriage and raising children. J LGBT Issues Couns. 2006;1:77–98. doi:10.1300/J462v01n04_06
20. Raifman J, Moscoe E, Austin BS, McConnell M. Difference-in-differences analysis of the association between state same-sex marriage policies and adolescent suicide attempts. JAMA Pediatr. 2017;171:350–356. doi:10.1001/jamapediatrics.2016.4529
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.