Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 11
Periodontal services rendered by general dental practitioners in Saudi Arabia
Authors Alblowi JA, Zahid TM ![]()
Received 18 October 2018
Accepted for publication 30 January 2019
Published 6 March 2019 Volume 2019:11 Pages 53—60
DOI https://doi.org/10.2147/CCIDE.S191252
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Christopher E. Okunseri
Jazia A Alblowi, Talal M Zahid
Periodontology Department, Faculty of Dentistry, King Abdulaziz University, Jeddah, Saudi Arabia
Purpose: The study aimed to determine the types of periodontal services rendered by general dental practitioners (GDPs) in Saudi Arabia.
Subjects and methods: A cross-sectional survey was performed on a convenience sample of 340 licensed GDPs practicing within Saudi Arabia. GDPs were asked several questions regarding the types of periodontal services offered, the level of training and education received in periodontics and the periodontal referral processes.
Results: Two hundred and ninety GDPs responded to the survey. The most commonly rendered periodontal services by the GDPs were oral hygiene instructions (84.1%; 244/290), mouthwash prescribing (82.7%; 240/290) and scaling and root planing (72.4%; 210/290). Only 21% (59/282) of the GDPs surveyed reported providing periodontal surgical services. The most frequently rendered surgical procedures included gingivectomy, functional crown lengthening and single posterior implant. Also, 76% (220/290) of the GDPs had no continuing education (CE) credit relating to periodontics. The level of training received in the dental school seemed to be an important factor that influenced a GDP’s decision to provide periodontal services. Also, 64% (184/286) of the GDPs were not routinely performing periodontal screening exams. The most common reason for not referring patients to a periodontist was practice setting’s policy.
Conclusion: Periodontal services commonly rendered by the GDPs of this survey were mostly nonsurgical in nature. The results indicate a need for formal advanced training in periodontics. GDPs should be encouraged to take periodontic CE courses.
Keywords: periodontology, periodontics, periodontal services, periodontal therapy, general dentist, general dental practitioner
Introduction
Periodontology or periodontics is the branch of dentistry that deals with the supporting hard and soft tissue structures of the teeth. With the newer advances in the diagnosis and treatment of periodontal diseases, periodontal therapy has become an essential part of today’s dental practice. Basic knowledge and practice of periodontal therapy is currently a component of most dental school curriculums. In addition, there has been an increase in demand for periodontal services in many developed countries1,2 and even in Saudi Arabia.3,4 However, contrary to the expected rise in the referral from general dental practitioners (GDPs) to periodontal specialists, a decreasing trend has been observed in several countries.5–7 It has been reported that this scenario is largely due to the rendering of more periodontal services by GDPs. Nevertheless, it is not yet investigated whether the referral from GDPs to periodontists is declining in Saudi Arabia.
There are limited reports in the dental literature regarding the types of periodontal services rendered in the general dental office. Lanning et al5 found that the types of services provided by GDPs were mostly nonsurgical, such as scaling, root planing and periodontal maintenance. Ghiabi and Matthews6 reported that around 95% of the GDPs in Nova Scotia, Canada were providing nonsurgical periodontal treatment. While <30% of them were performing surgical procedures, the majority of procedures were limited to crown lengthening, frenectomy and gingivectomy. Furthermore, Darby et al8 conducted a survey to evaluate the confidence level of GDPs in handling periodontal patients. They found that the majority of the GDPs were confident in diagnosing and treating gingivitis and initial periodontitis, whereas <50% of dentists were confident in treating aggressive periodontitis.
In general, the knowledge of GDPs in the diagnosis and management of periodontal diseases is often limited to what is taught as part of their graduation curriculum. However, certain factors may affect the practice patterns of GDPs. Betof et al9 reported that the age of dentist and years of practice affected the likelihood of providing periodontal services. In contrast, Zemanovich et al10 reported that periodontal referrals by GDPs were not affected by their age or years of practice, but by the proximity of a periodontist. Darby et al8 suggested that the level of training might influence the decision of dentists to provide periodontal services. In addition, Lanning et al5 found that variables such as year of graduation, the availability of dental hygienists in practice and recent continuing education (CE) earned on periodontics affected the types of services rendered by GDPs.
To date, no study has been conducted to determine the periodontal services commonly provided by GDPs in Saudi Arabia. Such information is critical to have a clear understanding of the periodontal procedures expected from GDPs and to help establish a good referral system. Therefore, the aim of this study was to investigate the types of periodontal services rendered by Saudi GDPs.
Subjects and methods
Study design
The present study was designed as a cross-sectional survey. The approval of this investigation was obtained from the Research Ethics Committee at the Faculty of Dentistry, King Abdulaziz University, Jeddah, Saudi Arabia. The survey was conducted from January 2017 to April 2017 using a structured questionnaire that was developed after a thorough literature review. The questionnaire was independently reviewed by a team of experts (a periodontist and three GDPs). This team also evaluated the clarity and comprehensibility of the questions. A pilot study was later conducted on 20 GDPs to evaluate the efficiency of the survey questionnaire. Any discrepancies observed were modified by the team of experts.
Subject selection
The survey was carried out on a convenience sample of 340 GDPs with dental licensure to practice within Saudi Arabia. The email addresses of this sample were obtained from the database of the Saudi Dental Society. A web-based version of the questionnaire was used for data collection. An introductory cover letter was sent directly to dentists’ email addresses. The respondents were provided with informed consent accompanying the questionnaire. Participants who received the questionnaire link via emails were able to read the rationale of the study before participation. The inclusion criteria for the participants were as follows: having a dental license and 1 year professional experience from either a private or a government dental clinic. However, because the aim of this survey was to gain an insight on the periodontal services rendered by GDPs and their perceptions toward the therapy, we excluded dentists with Master’s degree or higher certification. Informed consent was obtained from each subject beforehand, assuring anonymity and confidentiality of their responses.
The questionnaire
The questionnaire of this survey consisted of five parts. The first part was planned to collect demographics of the participating GDPs, such as type and years of dental practice and the total number of working hours per week. The second part collected information regarding their periodontal knowledge and training including dental school training and CE courses on periodontics. The third part asked the participants about the nature of periodontal services rendered in their practice. The fourth part contained questions addressing the confidence level of GDPs in the diagnosis and treatment of periodontal diseases. In the final part, GDPs were asked to give their opinion regarding the training and education that a dental school graduate should have for periodontal management. In addition, they were also asked about the referral of patients to a periodontist.
Data analysis
Data analysis was performed using R Studio software (version 3.4; RStudio Inc., Boston, MA, USA). This was primarily a descriptive study conducted to determine the specific nature of periodontal services offered by GDPs. Hence, data were summarized as counts and percentages. Bar plots were used to visualize the results.
Results
Of the 340 GDPs approached for this survey, 290 (85.3%) responded. Among these GDPs, 46.2% were from King Abdulaziz University; 89.3% of the GDPs graduated between 2001 and 2015, whereas only 10.7% graduated before 2000. When asked about hours of dental services provided per week, 44.1% of the participants replied that they provide >20 hours of services. A majority (64.5%) of the interviewed GDPs were in practice for <5 years. Government hospitals (53.8%) and private clinics (43.1%) were the two major practice settings for these GDPs; only 8.3% worked in teaching institutes. Furthermore, only 24.1% of the dentists had earned CE credit in periodontics in the last 5 years. The demographic and practice characteristics of the participants are summarized in Table 1.
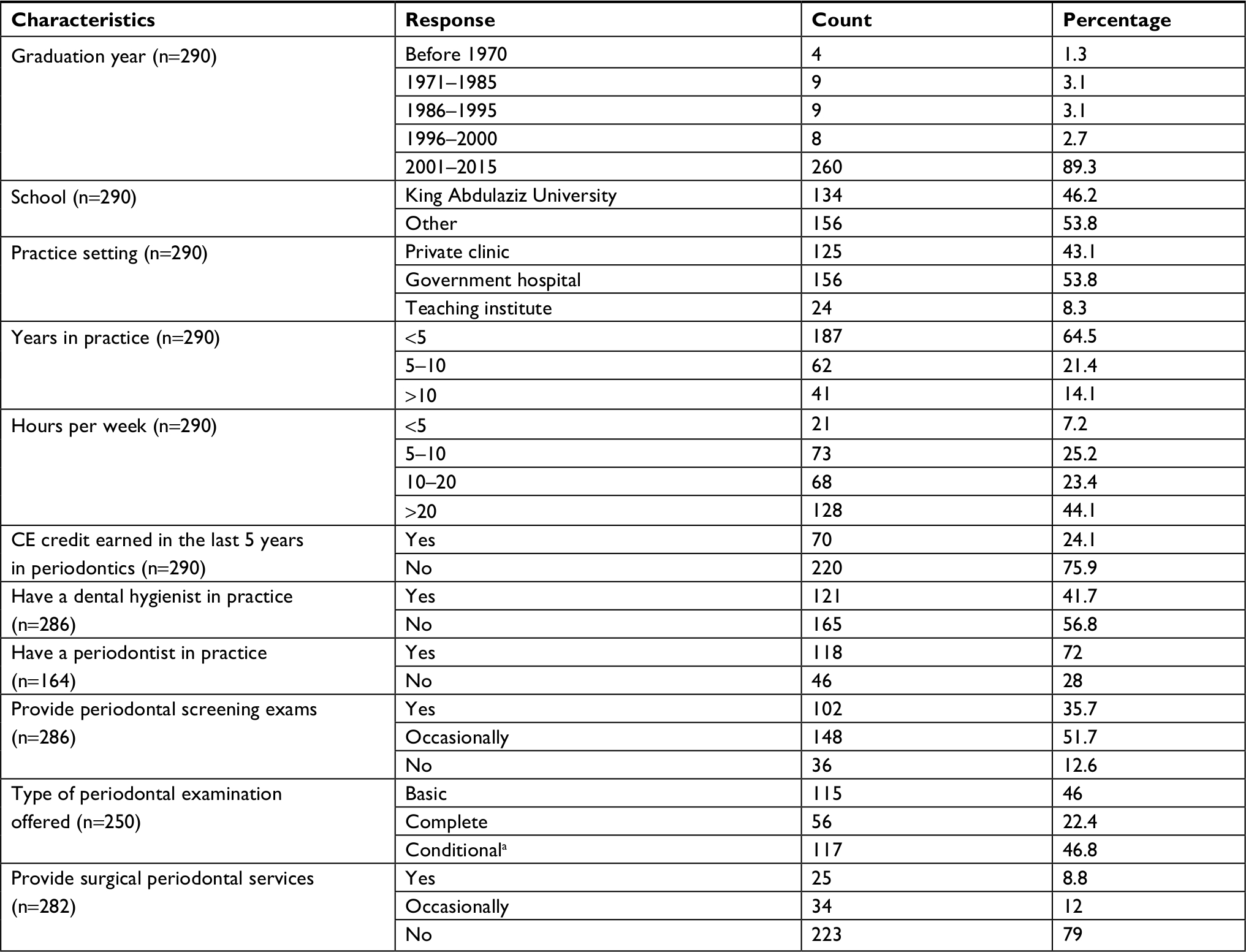 | Table 1 Demographic and practice characteristics of participating dentists Note: aDecision to perform periodontal examination depends on the severity of the condition. Abbreviation: CE, continuing education. |
Of the GDPs who responded to the survey, around 96% received training in scaling and root planing as part of their undergraduate degree. The periodontal procedures in which GDPs received the least training in school included single implant in the anterior area (8.6%), single implant in the posterior area (17.2%) and crown lengthening in the esthetic zone (12.4%). Table 2 demonstrates the participants’ level of training received regarding various periodontal procedures in their dental school.
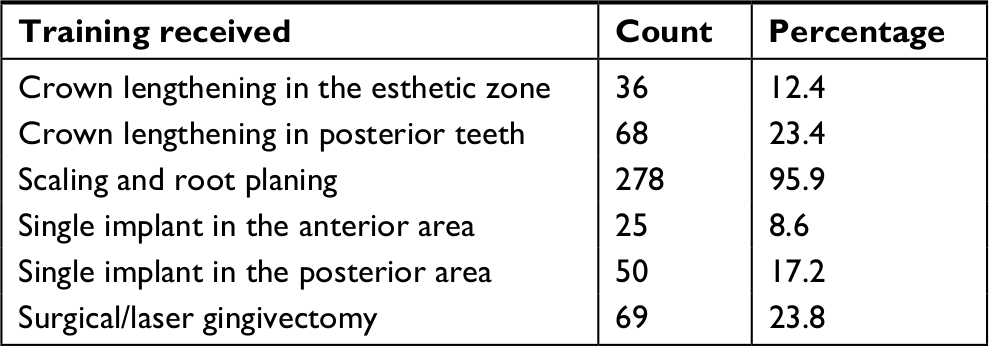 | Table 2 Periodontal training received in dental school by GDPs (N=290) Abbreviation: GDP, general dental practitioner. |
Profile of periodontal services
Of the surveyed GDPs, 250 (86.2%) were performing periodontal screening exams in their practices. Of these, 51% mentioned that they were occasionally providing such services. The basic periodontal examination was offered by around 46% of the GDPs, whereas nearly 47% were offering examination services depending on the severity of the periodontal condition; only 22% offered a complete examination (Table 1). Regarding periodontal disease diagnosis, a majority (74.8%) of the GDPs mentioned that the most commonly used diagnostic method was the clinical attachment level (CAL) calculation. Other methods that were frequently used by the participants included probing depth (PD, 64.8%), radiographs (64.4%) and bleeding gums (52.4%).
Nearly 79% of the surveyed dentists were not providing surgical periodontal services. Only 8.8% of the GDPs regularly performed surgical periodontal procedures, whereas 12% performed such procedures on an occasional basis (Table 1). The most common periodontal service rendered by GDPs in their dental office was oral hygiene instructions (84.1%, Figure 1). Other services commonly offered by the GDPs were mouthwash prescribing (82.7%), scaling and root planing (72.4%), gross debridement (51.7%) and splinting (16.9%). The most frequently rendered surgical periodontal procedures were gingivectomy (79.6%), functional crown lengthening (44%) and single posterior implant (28.8%). The least frequently performed procedures by the dentists were multiple implants (1.7%), osseous regenerative surgery (1.7%) and soft tissue graft (8.4%).
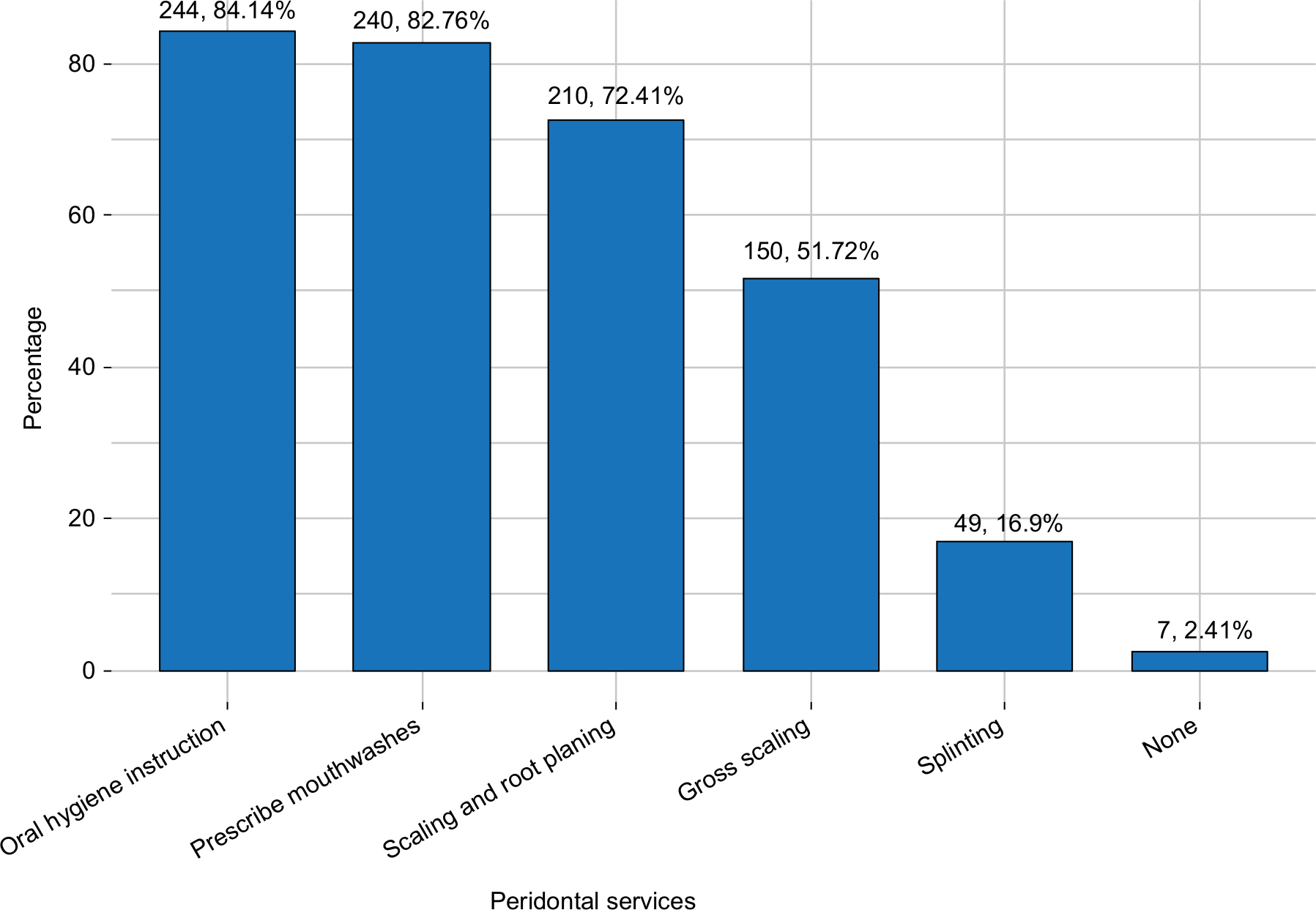 | Figure 1 Periodontal services commonly rendered by the surveyed dentists (N=290). |
Confidence level in providing periodontal services
Responses of surveyed GDPs indicated a decreasing trend in confidence with the increasing severity of the periodontal disease. Around 93% of the respondents were confident in diagnosing and treating gingivitis and initial periodontitis, whereas only 25% felt confident to diagnose and treat aggressive periodontitis. Figure 2 depicts the confidence level of GDPs to diagnose and treat various forms of periodontitis.
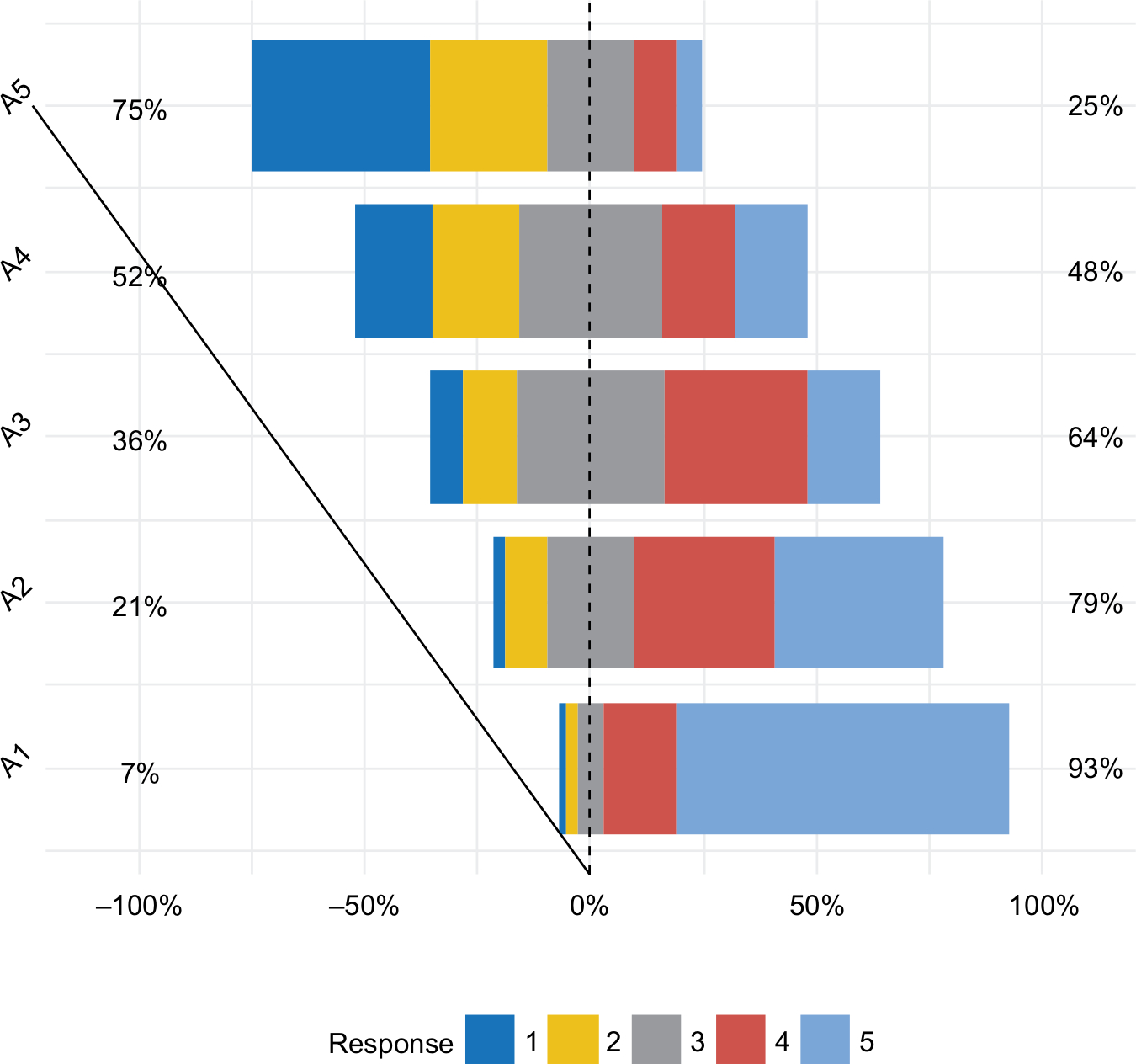 | Figure 2 Confidence level in diagnosing and treating periodontal disease. Notes: A1= gingivitis (CAL 0); A2= mild chronic periodontitis (CAL 1–2 mm or PD >3 and <5 mm); A3= moderate chronic periodontitis (CAL 3–4 mm or PD ≥5 and <7 mm); A4= severe chronic periodontitis (CAL ≥5 mm or PD ≥7 mm); A5= aggressive periodontitis. 1= Not confident; 2= neutral; 3= slightly confident; 4= confident; 5= highly confident. Abbreviations: CAL, clinical attachment loss; PD, probing depth. |
Skills that a dental school graduate should have
The surveyed dentists were asked to give their opinion about the skills and procedures that dental school graduates should learn from their institute for periodontal management. Responses of GDPs indicated that graduates from dental school should be well versed in diagnosing gingival and periodontal disease (93.7%), be able to perform scaling and root planing (86%) and know when to refer to a periodontist (85%). The interviewed GDPs also recommended some surgical procedures that dental school graduates should be familiar with, including gingivectomy (39.3%), posterior and anterior crown lengthening (36.5% and 25.8%, respectively), posterior and anterior single implant (24.5% and 14.8%, respectively) and pocket elimination surgery (18.6%).
Referral to periodontist
Only 164 (56.6%) GDPs replied to the questions related to the referral of patients to a periodontist; of these, 75% of the GDPs were referring patients to a periodontist, whereas 25% respondents replied “no” to referral to a specialist (Table 3). Around 61% of these dentists were referring patients either once a week (36%) or twice (or more) a week (25%). The most common reason for the referral to a periodontist was to ensure that the patient gets the best possible treatment, which was cited by 46.3% of participants. The second and third common reasons were lack of adequate training and complicated systemic health (42.3% and 35%, respectively). On the other hand, the biggest reason for not referring patients to a specialist by GDPs was practice setting’s policy (56.1%). Other major reasons were the unavailability of a periodontist (34.6%) and inability to motivate patients (29.2%). Three of the primary criteria reported by GDPs for selecting a periodontist were: availability in the community (39%), skills and expertise in periodontal surgery (37.4%) and previous success with the periodontist (27.6%). The least common criteria for the selection of a periodontist were friendship with the periodontist and consultation fees (6.5% and 4.8%, respectively).
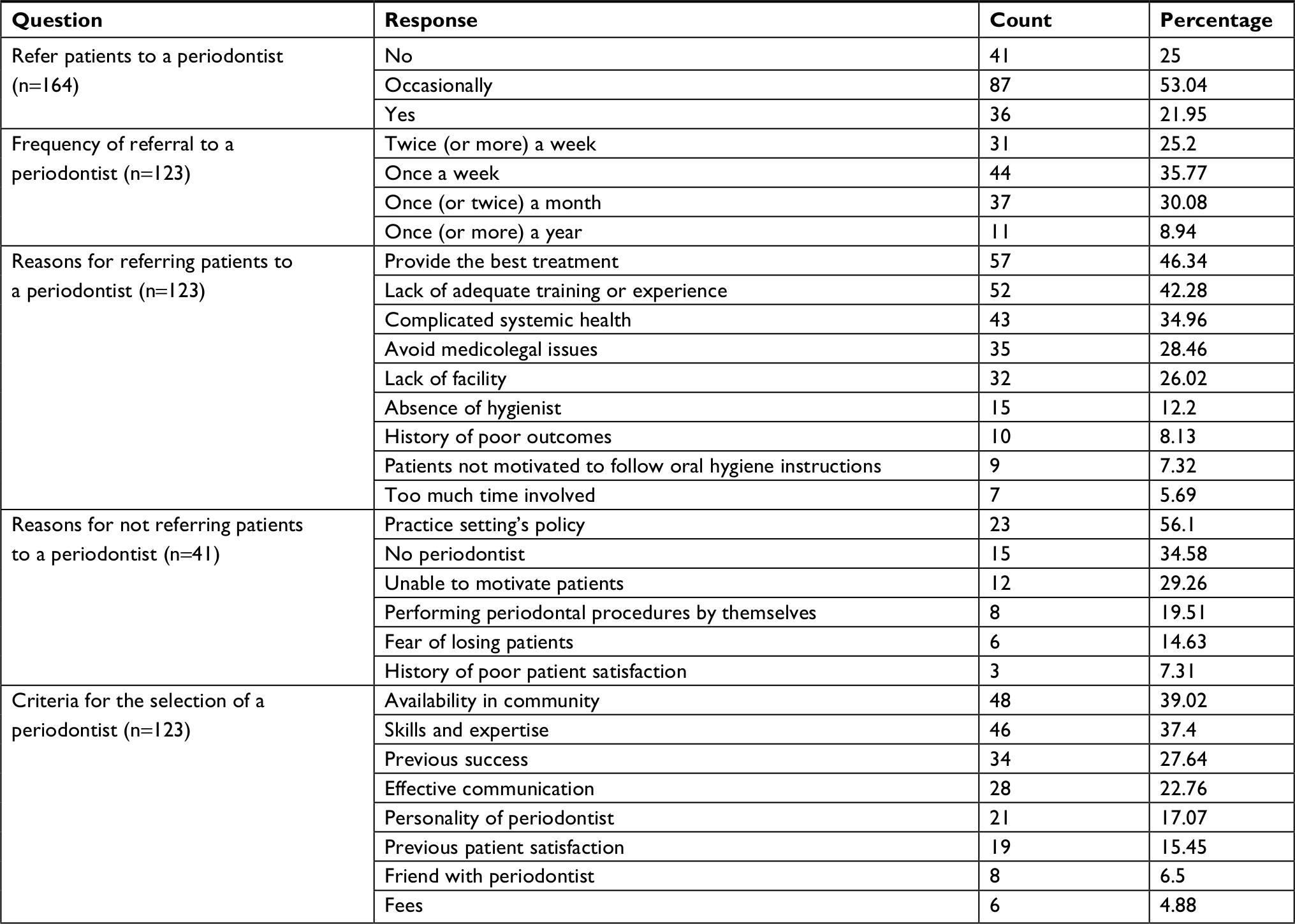 | Table 3 Reasons for and frequency of referral to a periodontist by GDPs Abbreviation: GDP, general dental practitioner. |
Discussion
There is little or no information in the dental literature about the types of periodontal services commonly rendered by GDPs practicing in Saudi Arabia. Therefore, this survey was designed to gather information regarding the periodontal services that Saudi GDPs often provide to their patients and the factors influencing their decisions to provide these services.
In the current study, a majority of the GDPs were rendering nonsurgical periodontal therapy, which is similar to the findings of earlier studies.5–7,11 Two of the most commonly rendered nonsurgical services by the surveyed GDPs were oral hygiene instructions and mouthwash prescribing. In contrast, Lanning et al5 and Ghiabi and Matthews6 reported scaling and root planing and periodontal maintenance as the most frequently rendered periodontal services. The number of GDPs providing scaling and root planing and gross debridement services was comparatively lower than the figures reported in the studies conducted in other countries. Around 98.5% of the GDPs in the Nova Scotia, Canada study6 and 100% in the Belgaum city, India study7 reported rendering gross debridement, whereas only 52% of our respondents reported providing such a procedure. Furthermore, only 21% of the respondents of this survey were offering surgical periodontal services. A similar result was reported in a few studies.5,6,8,11 However, studies by Lanning et al5 and Gilbert et al11 reported relatively higher figures (48% and 32%, respectively) than our finding, whereas Ghiabi and Matthews6 and Darby et al8 described slightly lower figures (16% and 15%, respectively).
These countrywide variations could be due to the differences in subject selection, postdental school training or education, the availability of a hygienist in practice, hours of CE credit earned, training received in undergraduate school and regulatory requirements. For example, in Gilbert et al’s11 study, around 19% of the enrolled participants were dental specialists, and 39% of respondents of the Virginia study5 reported completing a formal advanced dental training; in contrast, none of the GDPs surveyed reported receiving a formal advanced training beyond dental school. In addition, the number of dental hygienists in office has been found to impact referrals to periodontists and specific periodontal services rendered by the GDPs.5,6,10 Lanning et al5 reported that dentists who employed two or more hygienists were more likely to provide occlusal therapies in their practices than those employing fewer hygienists.
Several studies reported that hours of CE credit earned in periodontics affected the types of periodontal services offered by GDPs.5,6,12 In the Nova Scotia study, dentists who took more hours of CE courses in periodontics were more likely to provide surgical periodontal services.6 In the Virginia study, 97% of the GDPs had earned CE credit in periodontics in the last 5 years.5 The study reported a positive correlation between earning CE credit in periodontics and performing surgical procedures by dentists. However, only 24% of the GDPs in the current study earned a CE credit in periodontics in the last 5 years. The reasons behind this low percentage may be a limitation in the regulatory requirement and the preference for CE courses by GDPs. Although the regulatory body in Saudi Arabia requires that dentists must take 30 credit hours of CE courses annually to maintain their dental licensures, there are no minimum hours of CE in periodontics that must be taken annually by the GDPs.13 In addition, a recent study conducted in the Eastern Province of Saudi Arabia reported that GDPs were more interested in attending CE courses in esthetic dentistry (77.4%) than periodontics (47.9%).14
Formal training received in dental school by the GDPs of our survey was largely focused on nonsurgical periodontal therapy. Only 24% of the respondents received formal training in surgical/laser gingivectomy. A need for adequate training in surgical procedures relating to periodontics was reflected in their confidence to diagnose and treat periodontal diseases, as a decreasing trend in confidence was observed with the increasing severity of periodontitis. The need for more periodontal training was again reflected when the respondents were asked regarding the skills that dental school graduates should have. Darby et al8 and Lee et al12 also emphasized the importance of quality education in periodontics and suggested that it should be considered in the planning of undergraduate curricula. Taken together, it can be said that the level of training received in school is an important factor that influences a dentist’s decision to diagnose and treat periodontal disease.
In this study, only 36% of the GDPs reported performing periodontal examination routinely. This figure is significantly lower compared to the survey conducted by Bailey et al,15 where between 87% and 95% of the dentists reported providing routine periodontal examination to their patients. In an earlier study, Darby et al8 also reported a higher figure, where around 80% of the respondents were routinely checking the periodontal status of their patients. Such differences could be due to the countrywide variations in regulatory requirements. For example, the Dental Practice Board of Victoria requires that the periodontal status should be recorded for each presented case;16 however, it is still not a mandatory requirement in Saudi Arabia that all new patients must have their periodontal status recorded.
The parameters commonly used by GDPs surveyed to diagnose periodontal disease were CAL, PD, radiographs and bleeding gums. PD and CAL have been found to be the most commonly used parameters for periodontal diagnosis and are widely used for periodontitis case definitions.17 However, Bailey et al15 suggested CAL as a more preferable parameter, as the use of PD alone might misjudge the aggressiveness of the periodontal disease. Additionally, a basic periodontal examination involves measurement of PD, whereas a detailed calculation of PD and CAL is a mandatory component of a complete examination.18
The most common reasons for the referral to a periodontist were ensuring the best possible treatment, lack of adequate training, complicated systemic health and avoiding medicolegal problems. Our findings are quite similar to those reported in the Nova Scotia study.6 On the other hand, we identified that practice setting’s policy was the biggest reason for not referring patients to a periodontist. This is a surprising finding, but may be a reality in Saudi Arabia due to the fact that private practices may tend to have the fear of losing patients after referral. A slightly similar scenario was observed among general dentists of the Michigan Dental Association where respondents with high perception about their dental education showed less willingness to the referral and an increased desire to treat periodontal patients in their own offices.12
This survey had some limitations. First, the findings of this study cannot be generalized due to the small sample size. Second, we chose a convenience sample to conduct this study, given the difficulty in recruiting study subjects. However, a random sample would have been more appropriate here. Last, the data presented in this study could be an overestimation of the periodontal services rendered, as the survey is mainly based on self-reported data by GDPs and did not ask the respondents to show actual practice records. Further investigation is warranted with a stratified random sample to establish the findings of this study. Future studies should examine the factors affecting GDPs’ practice patterns in greater detail and investigate the regulatory steps required to overcome the barriers in referring patients to periodontists.
Conclusion
This was the first study conducted to explore the types of periodontal therapy commonly offered by GDPs in Saudi Arabia. It was found that periodontal services rendered by GDPs surveyed were mostly nonsurgical in nature. Surgical services were offered by only a small percentage of the GDPs. These findings are comparatively in line with the results of studies conducted in other countries; however, it appeared that Saudi GDPs are falling behind in three areas: hours of CE credit earned in periodontics, training received in dental school and periodontal status recording. Therefore, GDPs practicing in Saudi Arabia should be encouraged to take more CE courses in periodontics. More periodontal training, specifically relating to surgical techniques, should be considered in the undergraduate curricula. It should be made mandatory that the periodontal status of all new patients is recorded as part of their routine oral examinations. Furthermore, a thorough evaluation of periodontal referral patterns is needed to improve patient outcomes.
Acknowledgment
The authors would like to thank Dr Azhar Alanazi, Dr Nora Al Bahrani, and Dr Alanoud Alazmi who helped in data collection and entry.
Disclosure
The authors report no conflicts of interest in this work.
References
Ab-Murat N, Sheiham A, Tsakos G, Watt R. Periodontal treatment needs and workforce requirements: comparisons between the normative and sociodental approaches using different skill mix models. Community Dent Oral Epidemiol. 2015;43(2):106–115. | ||
Holtfreter B, Kocher T, Hoffmann T, Desvarieux M, Micheelis W. Prevalence of periodontal disease and treatment demands based on a German dental Survey (DMS IV). J Clin Periodontol. 2010;37(3):211–219. | ||
Farsi JM. Dental visit patterns and periodontal treatment needs among Saudi students. East Mediterr Health J. 2010;16(7):801–806. | ||
El Tantawi M, Alagl A. Disability and the impact of need for periodontal care on quality of life: a cross-sectional study. J Int Med Res. 2017;45(6):1949–1960. | ||
Lanning SK, Best AM, Hunt RJ. Periodontal services rendered by general practitioners. J Periodontol. 2007;78(5):823–832. | ||
Ghiabi E, Matthews DC. Periodontal practice and referral profile of general dentists in Nova Scotia, Canada. J Can Dent Assoc. 2012;78:c55. | ||
Halemani S, Sanikop S, Patil S, Jalli V. Perception regarding factors related to periodontal therapy among general dental practitioners of Belgaum city: a questionnaire survey. Oral Health Prev Dent. 2014;12(2):183–189. | ||
Darby IB, Angkasa F, Duong C, et al. Factors influencing the diagnosis and treatment of periodontal disease by dental practitioners in Victoria. Aust Dent J. 2005;50(1):37–41. | ||
Betof N, Salkin LM, Ferris RT. Why general dentists refer patients to periodontists. J Dent Pract Adm. 1985;2(3):106–110. | ||
Zemanovich MR, Bogacki RE, Abbott DM, Maynard JG, Lanning SK. Demographic variables affecting patient referrals from general practice dentists to periodontists. J Periodontol. 2006;77(3):341–349. | ||
Gilbert GH, Gordan VV, Korelitz JJ, et al. Provision of specific dental procedures by general dentists in the national dental practice-based research network: questionnaire findings. BMC Oral Health. 2015;15(1):11. | ||
Lee JH, Bennett DE, Richards PS, Inglehart MR. Periodontal referral patterns of general dentists: lessons for dental education. J Dent Educ. 2009;73(2):199–210. | ||
Saudi Commission for Health Specialties. Available from: https://www.scfhs.org.sa. Accessed December 28, 2018. | ||
Nazir M, Al-Ansari A, Alabdulaziz M, Alnasrallah Y, Alzain M. Reasons for and barriers to attending continuing education activities and priorities for different dental specialties. Open Access Maced J Med Sci. 2018;6(9):1716–1721. | ||
Bailey DL, Barrow S-Y, Cvetkovic B, et al. Periodontal diagnosis in private dental practice: a case-based survey. Aust Dent J. 2016;61(2):244–251. | ||
Dental Board of Australia. Dental guidelines on dental records; 2010. Available from: https://www.dentalboard.gov.au/Codes-Guidelines/Policies-Codes-Guidelines.aspx. Accessed December 28, 2018. | ||
Savage A, Eaton KA, Moles DR, Needleman I. A systematic review of definitions of periodontitis and methods that have been used to identify this disease. J Clin Periodontol. 2009;36(6):458–467. | ||
Armitage GC. The complete periodontal examination. Periodontol 2000. 2004;34(1):22–33. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.