Back to Journals » Journal of Pain Research » Volume 15
Perineural Methylprednisolone Depot Formulation Decreases Opioid Consumption After Total Knee Arthroplasty
Authors Del Toro-Pagán NM, Dai F, Banack T, Berlin J, Makadia SA, Rubin LE, Zhou B, Huynh P, Li J ![]()
Received 14 June 2022
Accepted for publication 15 August 2022
Published 27 August 2022 Volume 2022:15 Pages 2537—2546
DOI https://doi.org/10.2147/JPR.S378243
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ellen Soffin
Nicole M Del Toro-Pagán,1,2 Feng Dai,3 Trevor Banack,4 Jill Berlin,4 Satya A Makadia,4 Lee E Rubin,5 Bin Zhou,3 Phu Huynh,6 Jinlei Li4
1Department of Pharmacy, Yale New Haven Health - Bridgeport Hospital, Bridgeport, CT, USA; 2Applied Precision Pharmacotherapy Institute, Tabula Rasa HealthCare, Moorestown, NJ, USA; 3Department of Biostatistics, Yale University School of Public Health, New Haven, CT, USA; 4Department of Anesthesiology, Yale School of Medicine, New Haven, CT, USA; 5Department of Orthopedics and Rehabilitation, Yale School of Medicine, New Haven, CT, USA; 6Department of Pharmacy, Yale New Haven Hospital, New Haven, CT, USA
Correspondence: Jinlei Li, Department of Anesthesiology, Yale University School of Medicine, 333 Cedar Street, PO Box 208051, New Haven, CT, 06520-8051, USA, Tel + 1 475 434 4038, Email [email protected]
Purpose: Opioid consumption after total knee arthroplasty (TKA) remains a challenge with single injection nerve blocks even with common local anesthetic adjuvants dexamethasone (DEX). This study aimed to investigate the effects of adding methylprednisolone acetate (MPA) to adductor canal blocks (ACB) and interspace between the popliteal artery and capsule of the posterior knee (iPACK) blocks on postoperative opioid consumption.
Methods: A retrospective analysis was conducted on 100 consecutive TKA patients equally assigned into two groups, with one group receiving DEX through ACB and iPACK block and the other group receiving DEX and methylprednisolone acetate (DEX/MPA) through the same nerve blocks. The primary outcome was cumulative opioid consumption (oral milligram morphine equivalent, OME) during hospitalization for up to three days. Secondary outcomes included daily opioid consumption, highest rest and active pain scores, prosthetic knee joint active range of motion (AROM), laboratory studies including fasting serum glucose (FSG) and white blood cell count (WBC) on each postoperative day (POD), and length of hospital stay.
Results: Cumulative opioid consumption was significantly lower in the DEX/MPA group vs DEX group (median difference (95% CI) = − 45.3 (− 80.5 to − 10), P = 0.011). The highest rest and active pain scores were both significantly lower in the DEX/MPA group than in DEX group on POD 2 (least square mean difference (95% CI) = − 1.3 (− 2.3 to − 0.4), P = 0.005 and − 0.9 (− 1.8 to − 0.1), P = 0.031, respectively). Except on POD 1, FSG values were significantly lower in the DEX/MPA group (median difference (95% CI) = − 22.5 (− 36 to − 8.9), P = 0.001). AROM, WBC, and length of stay were comparable between both groups.
Conclusion: Compared to perineural DEX alone, the addition of MPA further decreases postoperative opioid consumption without clinically significant changes on FSG and WBC.
Level of Evidence: III.
Keywords: perineural, arthroplasty, glucocorticoids, total knee arthroplasty, TKA, peripheral nerve block, PNB, methylprednisolone acetate
Introduction
The United States is currently experiencing an opioid epidemic and consumes more narcotics than any other nation in the world.1 Among surgical specialties, orthopedic surgery represents the third highest group of opioid prescribers, which underscores the newfound urgency to maximize non-opioid analgesic regimens to control surgical pain.2 Numerous opioid-sparing methods have been used for total knee arthroplasty (TKA) with acute and subacute pain management to facilitate effective physical therapy, including peripheral nerve blockade (PNB), local infiltration analgesia, non-opioid adjunct analgesics, as well as transcutaneous electrical nerve stimulation.3–6 PNB has been shown to improve pain management, reduce perioperative complications, enhance early outcomes, and increase patient satisfaction while decreasing opioid use following TKA.7 Glucocorticoids are among the most common additives to local anesthetics to prolong nerve block duration. Dexamethasone sodium phosphate (DEX) is hydrophilic and thought to prolong nerve blockade for about 6–8 hours.8 In comparison, Methylprednisolone acetate (MPA) is a lipophilic glucocorticoid that is commonly used in chronic pain procedures with good safety record and can last from days to weeks.9 The use of MPA in peripheral nerve blocks for acute and subacute pain management is under-investigated and promising.10,11
Here, we presented a hypothesis-generating retrospective study assessing the analgesic effects of adding MPA depot formulation to the commonly used DEX and ropivacaine in adductor canal blocks (ACB) and interspace between the popliteal artery and capsule of the posterior knee (iPACK) blocks for patients undergoing TKA, with the hypothesis that the addition of MPA to the PNB “cocktail” will result in less opioid consumption during hospitalization by further augmenting the analgesic effects generated from DEX and ropivacaine alone.
Materials and Methods
With Yale University institutional review board approval and exempt informed consent to this retrospective cohort study, a single-center electronic chart review was conducted on consecutive patients who underwent inpatient TKA at a tertiary care academic medical center in the United States from September 5, 2018 backwards until 50 patients were reached in each group, with the ending date being November 17, 2017. A total of 218 TKA patients were screened, 118 were excluded, and 100 patients were analyzed. All data were immediately de-identified once the initial data collection were complete to maintain patient data confidentiality and compliance with the Declaration of Helsinki. Inclusion criteria consisted of elective primary unilateral TKA patients who received preoperative ACB and iPACK blocks, and spinal anesthesia intraoperatively with plain 0.5% bupivacaine. Exclusion criteria: (1) bilateral TKA; (2) revision TKA or surgical history on the ipsilateral knee; (3) on opioids or pregabalin/gabapentin prior to surgery; (4) intraoperative primary anesthesia was general anesthesia or spinal anesthesia with non-plain-bupivacaine agents; (5) patients intubated for any reason or admitted to locations other than routine post anesthesia care unit (PACU) at the end of the surgery.
Participants were categorized into two groups based on the peripheral nerve block regimen placed in preoperative holding area with standard American Society of Anesthesiologists (ASA) monitors under direct ultrasound guidance. The DEX group received 5 mg of DEX through single-injection ACB with 30 mL of 0.2% ropivacaine, and the same mixture was administered through iPACK per standard protocol at this institution (N = 50). The DEX/MPA group received 40 mg MPA depot formulation in addition to DEX in each nerve block (N = 50). All patients subsequently received spinal anesthesia with 0.5% plain bupivacaine and were transferred to PACU at the end of the surgery. The standard surgical techniques for total knee replacement at the study institute were through a medial parapatellar incision, and implants of both cruciate retaining and sacrificing designs were fixed with methyl methacrylate cementation. All patient data was retrospectively collected from the electronic medical record from the day of surgery up to 3 months postoperatively. The CT state Prescription Monitoring Program profile of each patient was also reviewed to assess opioid consumption at 6 weeks and 3 months.
The primary outcome was cumulative opioid consumption (oral milligram morphine equivalent, OME) during hospitalization. Secondary outcomes investigated include postoperative daily rest and active pain scores (right before and after physical therapy, respectively), daily opioid consumption, prosthetic joint range of motion assessed by physical therapists (using a goniometer per institutional standard of care), laboratory studies on potential systemic effects of perineural glucocorticoid on FSG and WBC, as well as length of hospital stay and adverse events or complications (severe hyperglycemia, nerve injury, revision surgery, intensive care unit admission, fall, wound infection, or delayed wound healing, emergency room visit, hospital readmission, etc, and mortality) for 12 weeks.
Statistical Analysis
Data were summarized as number of observations (%) for categorical variables, mean values ± standard deviation (SD) or median and interquartile range (IQR) for continuous variables. For the univariate analyses, categorical variables between two groups were compared using the Chi-Square test or the Fisher’s exact test as appropriate. Continuous variables were compared using two-sample Welch's t-test with unequal variances for normal data, for which the mean difference and 95% confidence interval (CI) were calculated. For non-normal data, Wilcoxon rank sum test was used in statistical comparison, and the median difference (95% CI) between two groups was estimated by the Hodges-Lehmann approach.
Linear Mixed Model Repeated measures (MMRM) analysis was utilized to evaluate the change in the postoperative day (POD) pain score (or opioid consumption), in which its baseline value, time (eg, POD 1, 2, 3), group (ie, DEX/MPA vs DEX), and time by group interaction were adjusted as covariates, with an unstructured variance-covariance matrix specified to account for within-subject correlation of repeatedly measured values. This method assumes that outcomes are missing values at random, and patients were kept in the MMRM analysis if they had any outcome value collected at any postoperative day and there was no missing data in preoperative value. As there was no significant imbalance in patient characteristics between two groups suggested by univariate analyses (p > 0.05), no other covariates were included in the MMRM analysis. For the MMRM analysis of FSG and WBC, as no baseline lab values were available, only time, group, and time by group interaction terms were included as the fix effects. To quantitate the magnitude of estimated effect size between two groups, least square mean (LSM) and 95% CI of repeatedly measured outcomes were reported at each time point.
All the statistical analyses were performed using the SAS v9.4 (Cary, NC) and a p-value of less than 0.05 was considered to be statistically significant.
Results
A total of 218 patients were screened for eligibility, and 100 were included in the final analysis shown in the STROBE flow chart (Figure 1). There were no statistically significant differences between the DEX and DEX/MPA groups in most baseline characteristics including age, sex, ethnicity, cigarette or alcohol usage, active diabetes, preoperative baseline laboratory data, ASA status, percentage of cases that received additional periarticular injection by surgeon intraoperatively, surgical duration, tourniquet time, PACU stay, and length of hospital stay (Table 1). A few noted differences between the groups included the use of anxiolytics or anti-depressive medication prior to surgery, with more patients in the DEX group under medical treatment for anxiety or depression disorders, 32% vs 14% (P = 0.032). In light of the current difficulty in pain assessment, the authors incorporated patient factor such as acceptable/comfort level of pain (ACLP) into the analysis of pain. Our results indicated the preoperative ACLP in the study patients was representative of the general population, right at the junction between minor and moderate pain categories, approximately 4/10; although the DEX/MPA group had a lower level, mean ± SD, 4.05 ± 1.29 vs 3.51 ± 0.82 (P = 0.028) (Tables 1 and 2).
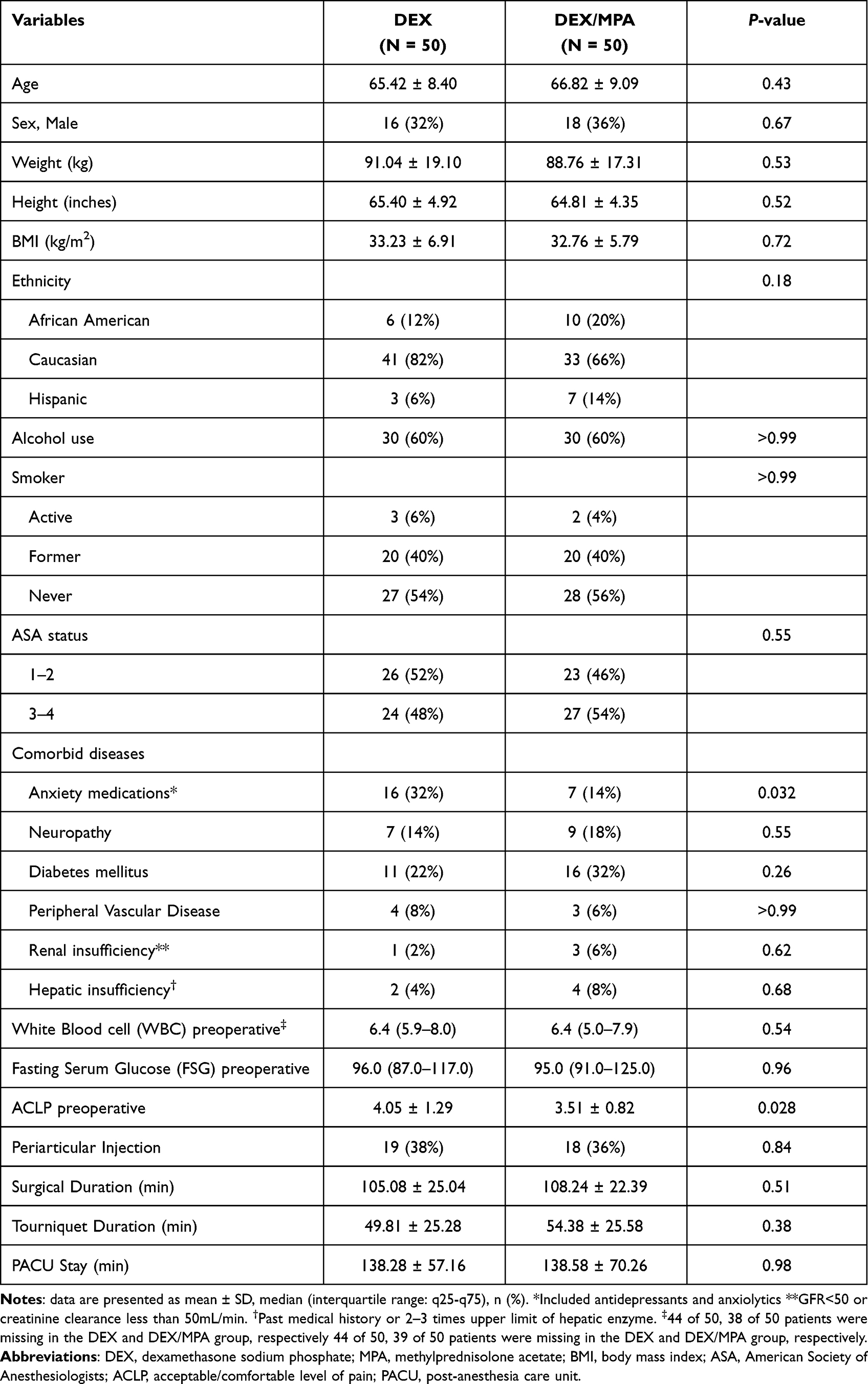 |
Table 1 Patient Demographics and Clinical Characteristics |
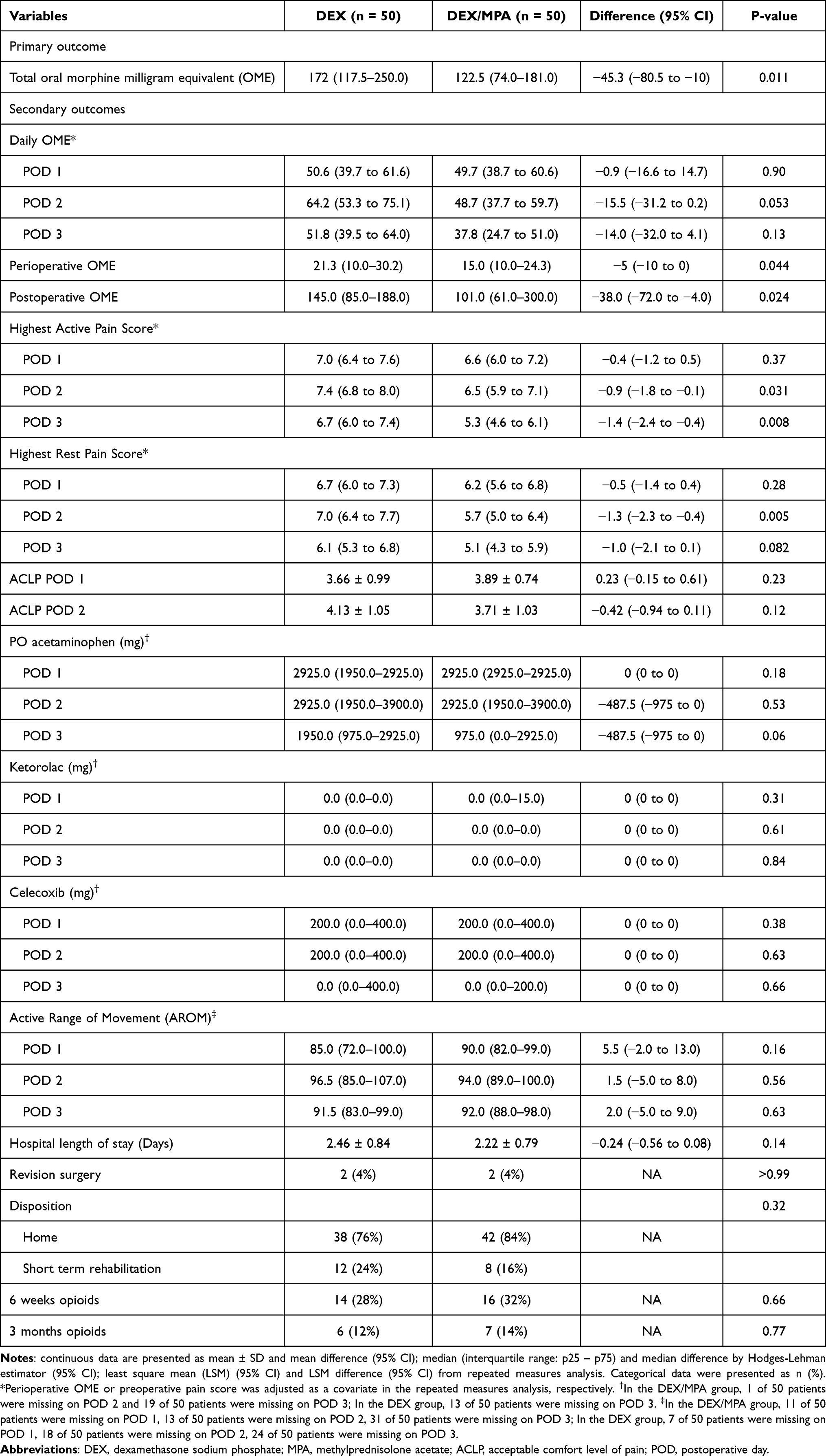 |
Table 2 Summary of Postoperative Outcomes |
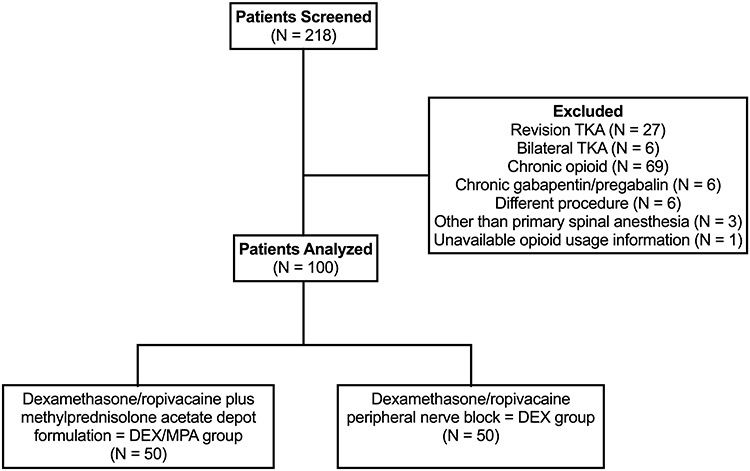 |
Figure 1 This STROBE flowchart shows patient inclusion. Abbreviation: STROBE, Strengthening the Reporting of Observational studies in Epidemiology. |
Total opioid consumption (oral milligram morphine equivalent, OME) during the entire hospitalization was significantly lower in the DEX/MPA group (median (IQR) 122.5 (74.0–181.0)) than (172 (117.5–250.0)) in the DEX group, with a median difference (95% CI) of −45.3 (−80.5 to −10), p = 0.011 (Table 2). Opioid consumption was also significantly different between groups during the immediate perioperative phase, which included preoperative (for peripheral nerve block placement), intraoperative, and post-anesthesia care unit (PACU), with a lower value in the DEX/MPA group vs in the DEX group (15.0 (10.0–24.3) vs 21.3 (10.0–30.2), median difference (95% CI) = −5 (−10 to 0), P = 0.044). A significantly lower opioid consumption was also seen for the postoperative phase, starting at the departure from PACU until hospital discharge, with a median (IQR) value of 101.0 (61.0–300.0) in the DEX/MPA group vs 145.0 (85.0–188.0) in the DEX group, resulting in a median difference (95% CI) of −38.0 (−72.0 to −4.0), P = 0.024 (Table 2). The progression of opioid consumption on each POD is plotted in Figure 2, even though the DEX/MPA group showed a similar percentage (over 20%) of reduction in opioid consumption on POD 2 and POD 3 as that of the postoperative phase or the entire hospitalization, no statistical significance in daily opioid consumption was found after adjusting for the perioperative opioid. Consumption of non-opioids analgesics including acetaminophen, ketorolac, and celecoxib throughout the hospital stay was similar between the two groups (Table 2).
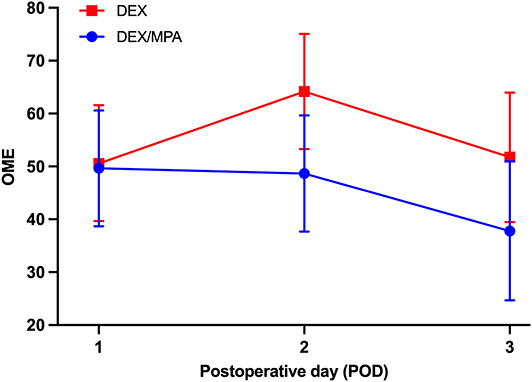 |
Figure 2 Progression of opioid consumption throughout the immediate postoperative period in DEX and DEX/MPA group. Abbreviations: POD, postoperative day; OME, oral milligram morphine equivalent. |
There were no statistically significant differences in highest rest or active pain scores on POD 1 between the two groups. Highest pain scores on POD 2 was significantly different both at rest and with activity (Table 2). At rest (right before physical therapy), the least square mean difference (95% CI) between the DEX/MPA and DEX groups was −1.3 (−2.3 to −0.4), P = 0.005. During activity (immediately after physical therapy), the mean difference (95% CI) in highest pain score was −0.9 (−1.8 to −0.1), P = 0.031. A statistically significant difference was seen in pain scores on POD 3 during activity (P = 0.008), but not at rest (P = 0.082).
The AROM (including both flexion and extension of the prosthetic knee joint) was comparable on each POD. No difference was observed in disposition, 84% in the DEX/MPA group vs 76% in the DEX group, P = 0.32. Length of stay in the DEX/MPA group vs the DEX group was Mean ± SD, 2.22 ± 0.79 days vs 2.46 ± 0.84 days, P = 0.14. In addition, there was no significant difference in the cost of stay (specific data not shown due to hospital policy), P = 0.18.
Laboratory results including FSG and WBC values reported throughout the admission were mostly comparable between the groups (Table 3). The only noted significant difference was on POD 1, where FSG values were significantly lower in the DEX/MPA group (median difference (95% CI) = −22.5 (−36 to −8.9). P = 0.001).
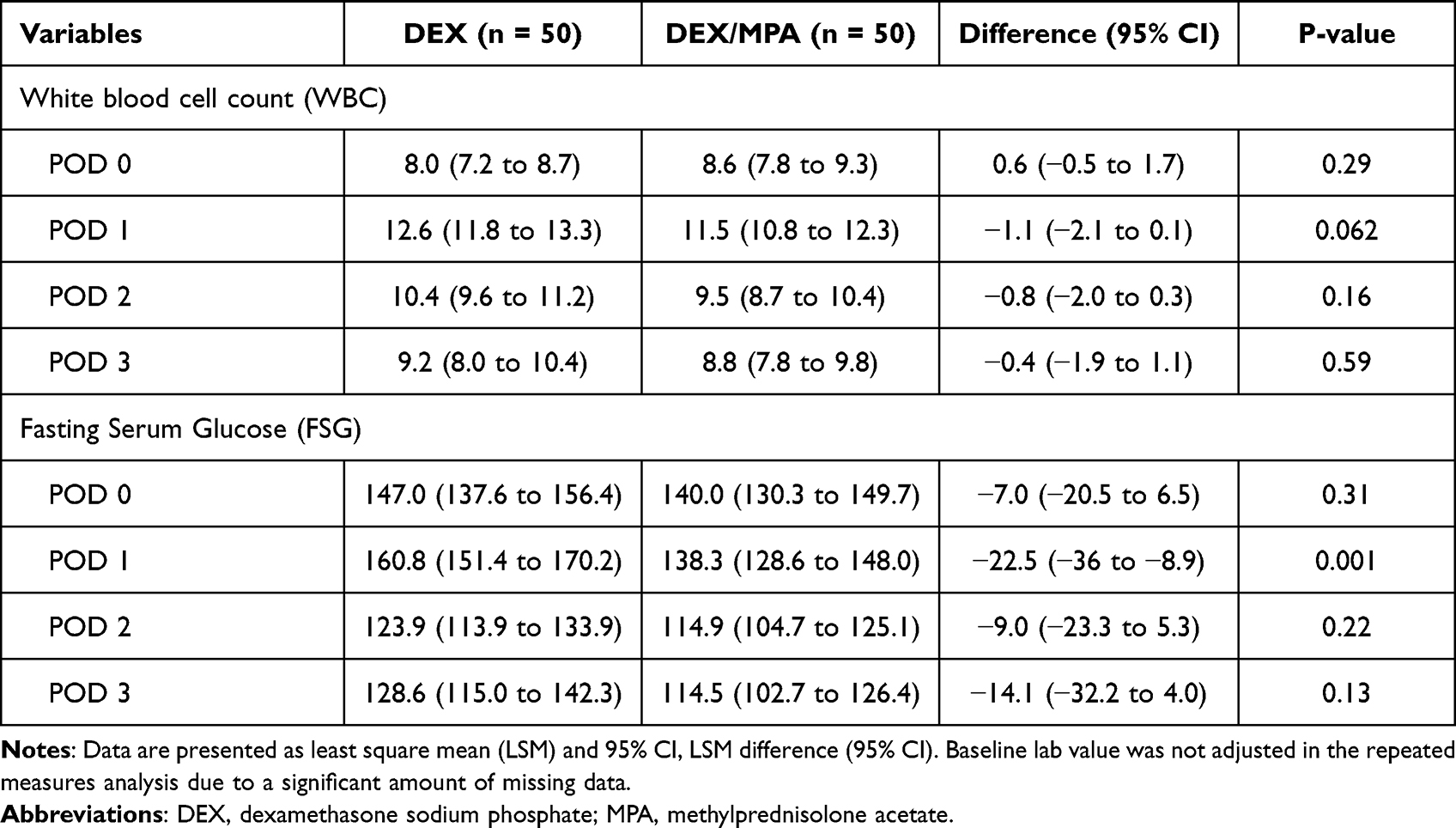 |
Table 3 Summary of Results for Laboratory Values |
Discussion
This single center study comparing the analgesic effects of DEX vs DEX/MPA through ACB and iPACK blocks for TKA demonstrated that patients who received MPA in addition to DEX consumed statistically significantly less opioids postoperatively and during the hospitalization. Similarly, patients in the DEX/MPA group experienced lower highest pain scores at rest or during physical therapy on POD 2 and POD 3, but not on POD 1. To the best of our knowledge, this is the first study that demonstrated the analgesic advantage of adding depot formulation MPA to DEX for acute pain DEX in TKA, with lower pain scores and opioid reduction when compared to DEX alone. The reduction of opioids postoperatively and during the entire hospitalization are clinically relevant, both are approximately 30%. This reduction was also calculated in the setting of detailed analysis of commonly used non-opioid adjunct analgesics including acetaminophen, NSAIDs by the hospital pharmacy department, therefore effectively minimized confounding factors during opioid consumption analysis.
Glucocorticoids are among the most used local anesthetic adjuvants in regional anesthesia, based on a few postulated mechanisms of analgesic properties of perineural glucocorticoids that include potent anti-inflammatory effects,12 inhibition of peripheral phospholipase thereby decreasing inflammatory mediators from the cyclooxygenase and lipoxygenase pathways,13 and blockade of nociception and immune modulation.14 DEX is the most popular water-soluble choice of glucocorticoids, but prolongs the duration sensory and motor block by merely 6 hours.15 MPA is one of the most commonly used long-acting glucocorticoids for treatment of chronic pain conditions via epidural anesthesia, intrathecal injection, and paravertebral routes in addition to intravenous and perineural administration.8,16–19 Currently, there are limited studies evaluating MPA in the perioperative setting for acute and subacute pain control,19 presumably due to its lipophilicity and slow onset, therefore not being able to provide reliable analgesia in the immediate postoperative period without a bridging agent such as DEX between local anesthetics and MAP.20,21 Combining two glucocorticoids with different onsets and duration of actions such as Celestone Soluspan® (betamethasone sodium phosphate and betamethasone acetate combination) has been proven effective and is approved for use by the United States Food and Drug Administration (FDA) for chronic conditions in tenosynovitis, rheumatoid arthritis, osteoarthritis, and multiple sclerosis.22
Data on the systemic effects of perineurally glucocorticoids is limited. In this study, none of the patients experienced any complications such as severe hyperglycemia, nerve injury related to the nerve block, wound infection, or delayed wound healing postoperatively. In addition, no differences were observed between the groups in FSG and WBC, which is consistent with current evidence in the literature where perioperative administration of glucocorticoids did not lead to increased rates of infection, symptomatic hyperglycemia, or wound healing complications in TKA and total hip arthroplasty.18,23
Limitations of this study include its retrospective design, with confounding factors that are not completely matched between groups, notably preoperative acceptable pain level and the percentage of patients with anxiety or depression disorders. The retrospective design also limited our ability to assess adverse events and specific follow-up data, especially if patients were lost to follow-up or moved out of our health system for further care. Missing data increased with each POD, most significantly on POD 3, because a portion of patients were discharged on POD 2. The timing of discharge affected our ability to observe the exact duration of analgesic effects from the nerve blocks. In addition, the follow-up period of 12-week was relatively short and may have missed potential long term adverse events and complications. DEX/MPA combination has been recently used in several other types of nerve blocks, including paravertebral block for breast surgery,24 femoral nerve block and lateral femoral cutaneous nerve block for total hip arthroplasty,9 and quadratus lumborum and lateral femoral cutaneous nerve block for total hip25 that the analgesic duration lasted from at least 3 days to one week. In addition, selection of DEX vs DEX/MPA was based on individual attending anesthesiologist preference, even though the number of patients with diabetes and ASA status were comparable between groups. A certain percentage of patients, nonetheless comparable between the groups, 38% in the DEX group and 36% in the DEX/MPA group, had received additional intraoperative periarticular injections by surgeons using medications at their discretion, but without additional glucocorticoids.
Nonetheless, we demonstrated an effective regimen using perineural DEX/MPA for analgesia following TKA that significantly decreased postoperative opioid consumption as compared to perineural use of DEX alone. Our institutional experience can certainly be considered in centers when other long duration of opioid-sparing pain control modalities is not readily available for TKA due to practical limitations such as prohibitory cost of patented medication or staffing restriction limiting the use of continuous nerve block catheters. A randomized controlled trial with longer duration of follow-up will be beneficial to systemically validate the utility and assess the safety of DEX and MPA combination in peripheral nerve block in the perioperative arena.
Conclusions
The addition of MPA to DEX and ropivacaine in adductor canal and iPACK blocks in TKA patients decreased opioid consumption and lowered pain scores immediate postoperatively, without causing apparent adverse events during a 12-week follow-up period.
Disclosure
Dr Lee Rubin reports personal fees from DePuy Synthes, personal fees from ConvaTec, personal fees from SLACK, Inc., outside the submitted work. The authors report no conflicts of interest in this work.
References
1. Manchikanti L, Helm S 2nd, Fellows B, et al. Opioid epidemic in the United States. Pain Physician. 2012;15(3 Suppl):Es9–38. doi:10.36076/ppj.2012/15/ES9
2. Volkow ND, McLellan TA, Cotto JH, Karithanom M, Weiss SR. Characteristics of opioid prescriptions in 2009. J Am Med Assoc. 2011;305(13):1299–1301. doi:10.1001/jama.2011.401
3. Rakel BA, Zimmerman MB, Geasland K, et al. Transcutaneous electrical nerve stimulation for the control of pain during rehabilitation after total knee arthroplasty: a randomized, blinded, placebo-controlled trial. Pain. 2014;155(12):2599–2611. doi:10.1016/j.pain.2014.09.025
4. Ramamoorthy KG. Local infiltration analgesia following total knee arthroplasty. Indian J Anaesth. 2012;56(2):208–209. doi:10.4103/0019-5049.96320
5. Szczukowski MJ
6. Gortemoller MA, Allen B, Forsyth R, Theiss K, Cunningham K, Tucker C. Comparison of oral and intravenous tranexamic acid for prevention of perioperative blood loss in total knee and total hip arthroplasty. Ann Pharmacother. 2018;52(3):246–250. doi:10.1177/1060028017735859
7. Joshi G, Gandhi K, Shah N, Gadsden J, Corman SL. Peripheral nerve blocks in the management of postoperative pain: challenges and opportunities. J Clin Anesth. 2016;35:524–529. doi:10.1016/j.jclinane.2016.08.041
8. Kirkham KR, Jacot-Guillarmod A, Albrecht E. Optimal dose of perineural dexamethasone to prolong analgesia after brachial plexus blockade: a systematic review and meta-analysis. Anesth Analg. 2018;126(1):270–279. doi:10.1213/ANE.0000000000002488
9. Li J, Perese F, Rubin LE, Carlyle D. Effective pain management after total Hip arthroplasty in a sickle cell patient emphasizing dexamethasone sodium phosphate/methylprednisolone acetate administered via a peripheral nerve blockade: a case report. A a Pract. 2019;12(5):171–175. doi:10.1213/XAA.0000000000000877
10. Puledda F, Goadsby PJ, Prabhakar P. Treatment of disabling headache with greater occipital nerve injections in a large population of childhood and adolescent patients: a service evaluation. J Headache Pain. 2018;19(1):5. doi:10.1186/s10194-018-0835-5
11. Evaluation of methylprednisolone or ibuprofen on efficacy of nerve blocks with symptomatic irreversible pulpitis; 2020. Available from: https://clinicaltrials.gov/ct2/show/NCT04157036.
12. Rhen T, Cidlowski JA. Antiinflammatory action of glucocorticoids–new mechanisms for old drugs. N Engl J Med. 2005;353(16):1711–1723. doi:10.1056/NEJMra050541
13. Shen S, Gao Z, Liu J. The efficacy and safety of methylprednisolone for pain control after total knee arthroplasty: a meta-analysis of randomized controlled trials. Int J Surg. 2018;57:91–100. doi:10.1016/j.ijsu.2018.07.009
14. Johansson A, Hao J, Sjölund B. Local corticosteroid application blocks transmission in normal nociceptive C-fibres. Acta Anaesthesiol Scand. 1990;34(5):335–338. doi:10.1111/j.1399-6576.1990.tb03097.x
15. Pehora C, Pearson AM, Kaushal A, Crawford MW, Johnston B. Dexamethasone as an adjuvant to peripheral nerve block. Cochrane Database Syst Rev. 2017;11(11):Cd011770. doi:10.1002/14651858.CD011770.pub2
16. Lunn TH, Kehlet H. Perioperative glucocorticoids in Hip and knee surgery - benefit vs. harm? A review of randomized clinical trials. Acta Anaesthesiol Scand. 2013;57(7):823–834. doi:10.1111/aas.12115
17. Wylde V, Beswick A, Bruce J, Blom A, Howells N, Gooberman-Hill R. Chronic pain after total knee arthroplasty. EFORT Open Rev. 2018;3(8):461–470. doi:10.1302/2058-5241.3.180004
18. Bedard NA, Pugely AJ, Westermann RW, Duchman KR, Glass NA, Callaghan JJ. Opioid use after total knee arthroplasty: trends and risk factors for prolonged use. J Arthroplasty. 2017;32(8):2390–2394. doi:10.1016/j.arth.2017.03.014
19. Toner AJ, Ganeshanathan V, Chan MT, Ho KM, Corcoran TB. Safety of perioperative glucocorticoids in elective noncardiac surgery: a systematic review and meta-analysis. Anesthesiology. 2017;126(2):234–248. doi:10.1097/ALN.0000000000001466
20. Abrishamkar S, Rafiei AR, Sabouri M, et al. The effect of impregnated autogenous epidural adipose tissue with bupivacaine, methylprednisolone acetate or normal saline on postoperative radicular and low back pain in lumbar disc surgery under spinal anesthesia; A randomized clinical trial study. J Res Med Sci. 2011;16(5):621–626.
21. Autefage A, Alvinerie M, Toutain PL. Synovial fluid and plasma kinetics of methylprednisolone and methylprednisolone acetate in horses following intra-articular administration of methylprednisolone acetate. Equine Vet J. 1986;18(3):193–198. doi:10.1111/j.2042-3306.1986.tb03594.x
22. Shering C. Celestone Soluspan® [package insert]. U.S: Food and Drug Administration; 2008. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2008/014602s047lbl.pdf.
23. Hartman J, Khanna V, Habib A, Farrokhyar F, Memon M, Adili A. Perioperative systemic glucocorticoids in total Hip and knee arthroplasty: a systematic review of outcomes. J Orthop. 2017;14(2):294–301. doi:10.1016/j.jor.2017.03.012
24. Li J, Lee K, Chang D, Boominathan P, Banack T. A breast cancer survivor’s self-controlled case report: methylprednisolone acetate provided a week longer analgesia than dexamethasone sodium phosphate via thoracic paravertebral blockade. Cureus. 2019;11(11):e6085. doi:10.7759/cureus.6085
25. Li J, Dai F, Ona Ayala KE, Zhou B, Schonberger RB, Sharma A. Transmuscular quadratus lumborum and lateral femoral cutaneous nerve block in total hip arthroplasty. Clin J Pain. 2021;37:366.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.